communicable disease profile - whocommunicable disease profile for afghanistan and neighbouring...
TRANSCRIPT
WHO/CDS/2001.5 Original: English
Dist.: General
COMMUNICABLE DISEASE PROFILE
AFGHANISTAN AND NEIGHBOURING COUNTRIES
October 2001
Communicable Disease Working Group on Emergencies HQ Division of Communicable Disease Control EMRO
Communicable Diseases EURO WORLD HEALTH ORGANIZATION
© World Health Organization, 2001 This document is not a formal publication of the World Health Organization (WHO), and all rights are reserved by the Organization. The document may, however, be freely reviewed, abstracted, reproduced and translated, in part or in whole, but not for sale nor for use in conjunction with commercial purposes. The views expressed in documents by named authors are solely the responsibility of those authors.

Communicable Disease Profile for Afghanistan and Neighbouring Countries
WHO Communicable Disease WG on Emergencies/October 2001
Contents INTRODUCTION 2
FOOD OR WATER-BORNE DISEASES
1. Diarrhoeal diseases 3
2. Bacillary dysentery 6
3. Cholera 8
4. Typhoid fever 10
5. Poliomyelitis 12
RESPIRATORY-BORNE DISEASES
6. Acute Lower Respiratory Infections 14
7. Measles 17
8. Tuberculosis 20
9. Meningococcal disease 24
VECTOR-BORNE DISEASES
10. Malaria 26
11. Dengue 30
12. Crimean-Congo haemorrhagic fever 32
13. Plague 34
ZOONOTIC DISEASES
14. Rabies 36
15. Anthrax 38
ANNEXES
Annex 1 : Syndromic Approach to Diagnosis of Communicable Diseases 40 Annex 2 : Steps for Management of a Communicable Disease Outbreak 45
Annex 3 : Safe Water and Sanitation 46 Annex 4 : Injection Safety 48
Annex 5 : Key WHO Contacts for Central Asia crisis 49
Annex 6 : List of WHO Guidelines on Communicable Diseases 53
Communicable Disease Profile for Afghanistan and Neighbouring Countries
WHO Communicable Disease WG on Emergencies/October 2001 2
Introduction This document is intended to provide health professionals working in Afghanistan and neighbouring countries with information on the major epidemic and endemic disease threats faced by the displaced population. Following an emergency, resettlement in temporary locations such as refugee camps may entail high population densities, inadequate shelter, poor water and sanitation, and lack of basic health care. This poses an increased threat of communicable diseases to the population and a high risk of epidemics. The document provides data on recent outbreaks in Afghanistan and neighbouring countries, outlines the burden of communicable diseases in the region, presents disease-specific guidelines on the prevention and control of these diseases and adapts them for use in an emergency situation. The major causes of morbidity and mortality in Afghanistan and neighbouring countries are diarrhoeal diseases, acute respiratory infections and measles. Other communicable diseases such as meningococcal meningitis have caused large outbreaks among displaced populations. Malnutrition and trauma are the two main additional causes of illness and death. A systematic approach to the control of communicable diseases is a key component of humanitarian response. This profile seeks to provide local authorities, UN agencies and NGOs with a user friendly, concise summary on the prevention and control of the main communicable diseases among the emergency affected population. The list of diseases has been selected on the basis of the potential threat to the population in terms of morbidity and mortality. Additional diseases will be added as data is received from the field. The profile will be updated in three months time. This profile is a collaboration between the Communicable Disease Working Group on Emergencies (CD-WGE) at HQ, the Division of Communicable Disease Control (DCD) at EMRO and Communicable Diseases (CDS) at EURO. The CD-WGE supports the Department of Emergency and Humanitarian Action (EHA) on communicable disease control issues in emergencies and includes the Departments of Surveillance and Response (CSR), Control, Prevention and Eradication (CPE), Roll Back Malaria (RBM) and Stop TB (STB) in the Communicable Disease Cluster (CDS), the Department for Child and Adolescent Health (CAH), and the Department for Vaccines and Biologicals (VAB). Compiled by Dr Claudio Beltramello (CPE), Mr Christopher Haskew (CPE), and Dr Maire Connolly (CSR) on Communicable Disease Working Group on Emergencies. The following persons in HQ, EMRO and EURO contributed to the development of this document and their input is gratefully acknowledged: Dr Samira Aboubaker (CAH), Mr Richard Allan (RBM), Dr Ray Arthur (CSR), Dr Karen Bradbury (MAL/EURO), Dr Sylvie Briand (CSR), Dr E Capobianco (STB/EMRO), Dr Daniel Lavanchy (CSR), Dr Claire-Lise Chaignat (CSR), Ms Claire Chauvin (VAB/Polio), Dr Otorino Cosivi (CSR), Dr Charles Delacollette (RBM), Dr Mikhail Ejov (MAL/EURO), Dr Taky Gaafar (DCD/EMRO), Dr Bernadus Ganter (CDS/EURO), Dr Malgosia Grzemska (STB), Dr Max Hardiman (CSR), Dr Hamid Jafari (EPI/EMRO), Dr Faizallah Kakar (CDS/Pakistan), Dr AnaMaria Henao-Restrepo (VAB), Dr Tony Mounts (EPI/Pakistan), Mr Jose Hueb (WSH), Dr Yvan Hutin (VAB), Mr Chris Maher (VAB/Polio), Dr Francois Meslin (CSR), Dr Rudi Nowak (CSR), Dr Aafje Rietveld (RBM), Dr Mike Ryan (CSR), Dr Guido Sabatanelli (RBM/EMRO), Dr Saleh Ottmani (STB), Dr Maria Santamaria (CSR), Dr Akihiro Seita (STB/EMRO), Dr Nadia Teleb (CSR/EMRO), Dr Eugene Tikomirov (CSR), Dr Shamim Qazi (CAH). WHO would like to acknowledge the support of the Government of Ireland who funded the production of this document.
Communicable Disease Profile for Afghanistan and Neighbouring Countries
WHO Communicable Disease WG on Emergencies/October 2001 3
Food or Water-borne Diseases 1. DIARRHOEAL DISEASES
DESCRIPTION
Infectious agent Bacteria: such as Salmonellae (commonly S. enteritidis, S. typhimurium) and Escherichia coli. The bacteria that cause the most severe outbreaks are Shigella dysenteriae type 1 and Vibrio cholerae (see Bacillary dysentery and Cholera)
Protozoa: such as Giardia lamblia
Viruses: such as Rotavirus and Norwalk virus
Case definition Clinical case definition Three or more abnormally loose or fluid stools over 24 hours
Mode of transmission
Fecal-oral route, particularly contaminated water and food
Incubation Salmonella generally requires an 8-48 hour incubation period, whereas E. coli is typically longer at 2-8 days (median of 3-4 days). Both usually last between 2-5 days
The incubation period for rotavirus is about 48 hours, and symptoms may last for up to one week
Period of communicability
During the acute stage of the disease and for duration of fecal excretion. Temporary Salmonella carriers can continue to exist for several months
EPIDEMIOLOGY
Incidence in the region
No data available
Geographical distribution
Diarrhoeal diseases are endemic throughout the region
Seasonality No data available
Alert threshold An increase in the number of cases above what is expected
Recent epidemics in the region
See Bacillary dysentery and Cholera
RISK FACTORS FOR INCREASED TRANSMISSION
Population movement
Yes Importation
Overcrowding Yes Very important
Poor access to health services
Yes Early detection and containment of the cases are paramount to reduce transmission
Food shortages Yes Malnutrition increases gastrointestinal tract susceptibility to invasiveness of the organism and severity of disease
Communicable Disease Profile for Afghanistan and Neighbouring Countries
WHO Communicable Disease WG on Emergencies/October 2001 4
Lack of safe water and poor sanitation
Yes The most important risk factor. The prevention of diarrhoeal diseases depends on the provision and use of safe water, adequate sanitation and health education. The supply of adequate quantities of water should be one of the highest priorities for camp planners. The emergency requirement is 20 litres/person/day. Common sources of infection in emergency situations are:
�� polluted water sources (e.g. by fecally contaminated surface water entering an incompletely sealed well) or during storage (e.g. by contact with hands soiled by faeces)
�� shared water containers and cooking pots
Others Yes Lack of soap
Risk assessment conclusions
Diarrhoeal diseases are a major cause of morbidity and mortality in emergency situations. This is mainly due to an inadequate water supply in terms of quality and quantity; insufficient, poorly maintained sanitation facilities; and overcrowding.
In camp situations, diarrhoeal diseases have accounted for between 25% and 40% of deaths in the acute phase of the emergency. Over 80% of deaths are among children under 2 years old.
PREVENTION AND CONTROL MEASURES
Case Management �� The prevention and treatment of dehydration, using Oral Rehydration Salt (ORS) or i.v. fluids (ringer lactate) if severely dehydrated patient, is the mainstay of the management of diarrhoeal illness. Reduction of mortality due to diarrhoeal disease is primarily related to effective management of dehydration particularly in children.
�� Use of antibiotics is dependent on the infectious agent
�� Resume feeding with a normal diet when vomiting has stopped. It is important to separate those who are eating from those who are not. Food should be cooked on site. Continue breast feeding infants and young children
Epidemic control �� Inform the Health Authorities if a increase in the number of cases above what is expected is identified
�� Confirm the diagnosis and ensure prompt treatment
�� Confirm the outbreak following WHO guidelines
Prevention
Safe drinking water
�� Provision of an adequate supply, collection and storage system
�� Provision of information on the importance of clean water, also covering system maintenance and household storage
See Annex 3 : Safe Water and Sanitation
Safe disposal of human excreta
�� Provision of an adequate facilities for the disposal of human waste
�� Provision of information on the importance of human waste disposal, also covering use and maintenance of the facilities
Communicable Disease Profile for Afghanistan and Neighbouring Countries
WHO Communicable Disease WG on Emergencies/October 2001 5
Food safety
�� Provision of adequate food storage facilities, (both uncooked and cooked), cooking utensils, adequate quantity of water and fuel to allow for cooking and reheating
�� Provision of information on the importance of food safety
Hand washing with soap
�� Provision of soap, allowing for bathing and laundry
�� Provision of information on the diseases spread through lack of or poor hand washing. Demonstration of good hand washing
Breastfeeding
�� Provision of information on: the protective qualities of breast-feeding. the importance of breast feeding ill children
�� Practical support for breast feeding ill children

Communicable Disease Profile for Afghanistan and Neighbouring Countries
WHO Communicable Disease WG on Emergencies/October 2001 6
2. BACILLARY DYSENTERY (SHIGELLOSIS) DESCRIPTION
Infectious agent Bacterium: Genus Shigella, of which Shigella dysenteriae type 1 causes the most severe disease and the largest epidemics
Case definition
Clinical case definition Diarrhoea with visible blood Confirmed case Isolation of S. dysenteriae type 1 from stool
Mode of transmission
Fecal-oral route, particularly contaminated water and food
Incubation Incubation period is usually 1-3 days. May be up to one week for S. dysenteriae type 1
Period of communicability
During acute infection and until 4 weeks after illness (without treatment). With appropriate treatment 2-3 days. Asymptomatic carriers exist
EPIDEMIOLOGY
Incidence in the region
No data available
Geographical distribution
The disease is present throughout the region
Seasonality No data available
Alert threshold Five or more linked cases must be investigated further
Recent epidemics in the region
No data available
RISK FACTORS FOR INCREASED TRANSMISSION
Population movement
Yes Importation
Overcrowding Yes Very important
Poor access to health services
Yes �� Early detection and containment of the cases are paramount to reduce transmission
�� Case fatality rate is high for S. dysenteriae type 1 in children under 10 years-old (10%) in absence of a proper treatment
Food shortages Yes Malnutrition increases gastrointestinal tract susceptibility to invasiveness of the organism and severity of disease
Lack of safe water and poor sanitation
Yes The most important risk factor.
Others No
Communicable Disease Profile for Afghanistan and Neighbouring Countries
WHO Communicable Disease WG on Emergencies/October 2001 7
Risk assessment conclusions
Risk of epidemics of S. dysenteriae type 1 is high in the refugee camps (up to one third of the population at risk may be affected)
In the general population the risk is strictly related to the availability of safe water
PREVENTION AND CONTROL MEASURES
Case Management �� S. dysenteriae type 1 is often more severe or fatal in young children, the elderly, and the malnourished, and prompt treatment with antibiotics is essential
�� Appropriate antibiotic therapy is very important. Selection depends on resistance patterns of the bacteria and drug availability
�� Nalidixic acid is first choice, and ciprofloxacin second choice in the region
�� A study performed in Pakistan, in 1990, showed that all shigella isolates were susceptible to nalidixic acid, 7% susceptible to cotrimoxazole, and 3.5% to ampicillin. No recent data on strain resistance are available, and selection of antibiotics must be tailored to reflect clinical response and anti-biogramme sensitivity results
�� Dehydration prevention and case management using ORS also plays an important role
Epidemic control �� Inform the Health Authorities if one or more suspected cases are identified
�� Confirm the outbreak, following WHO guidelines. Stool samples must be taken with a rectal swab and transported in Cary Blair medium. It is recommended that 10-20 cases be used to confirm the cause, identify antibiotic sensitivity and verify the outbreak. Once confirmed, it is not necessary to obtain laboratory confirmation for every patient as this depletes laboratory supplies.
Do not wait for laboratory results before starting treatment/control activities
�� Confirm the diagnosis and ensure prompt treatment
Prevention �� See prevention of diarrhoeal diseases
See Annex 3 : Safe Water and Sanitation
See Guidelines for the Control of Epidemics due to Shigella dysenteriae type 1, WHO, 1995. Available at: http://www.who.int/emc-documents/cholera/whocdr954c.html
Communicable Disease Profile for Afghanistan and Neighbouring Countries
WHO Communicable Disease WG on Emergencies/October 2001 8
3. CHOLERA DESCRIPTION
Infectious agent Bacterium: Vibrio cholerae.
Case definition
Clinical case definition Person aged over 5 years with severe dehydration from acute watery diarrhoea. Person aged over 2 years with acute watery diarrhoea in an area where there is a cholera outbreak Confirmed case Isolation of Vibrio cholerae O1 or O139 from diarrhoeal stool sample
Mode of transmission
Fecal oral route, particularly contaminated water and food
Incubation Incubation period is usually between 1 and 5 days
Period of communicability
During the symptomatic phase until 2-3 days after recovery. Very rarely for months
EPIDEMIOLOGY
Incidence in the region
No data available
Geographical distribution
Cholera outbreaks have occurred in all the countries of the region during the past five years
Seasonality Higher risk from June until September
Alert threshold One suspected case must be investigated
Recent epidemics in the region
Afghanistan June 2001 Samangan and Baghlan provinces
4499 cases including 114 deaths (CFR 2.5%) reported Vibrio cholerae serotype Ogawa, laboratory confirmed
2000 4330 cases and 198 deaths reported to WHO Iran August 1998 Teheran, Qom, Espahan, and Sistan- Baluchistan
4300 cholera cases including 44 deaths.
May 2000 Cholera suspected In Dol Avkurt camps, Kandil Moutain 76 deaths reported in the camps in North-eastern area. Number of cases unknown. 352 cases including 3 deaths were reported in 2000
Pakistan February 2000 Cholera suspected in Khairpur district
9 deaths (all children, age: 2-10) reported. Number of cases unknown
August 2000 Cholera suspected in Muzaffarabad 4 deaths reported in north-eastern area. Number of cases unknown
Communicable Disease Profile for Afghanistan and Neighbouring Countries
WHO Communicable Disease WG on Emergencies/October 2001 9
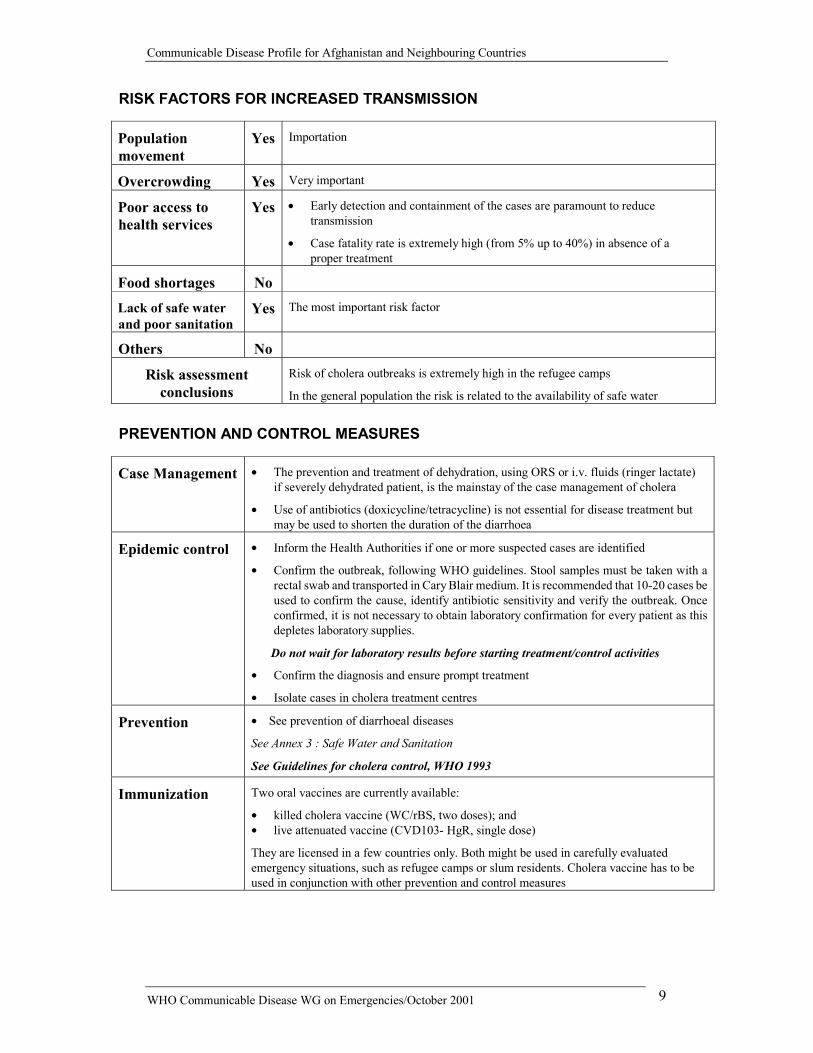
RISK FACTORS FOR INCREASED TRANSMISSION
Population movement
Yes Importation
Overcrowding Yes Very important
Poor access to health services
Yes �� Early detection and containment of the cases are paramount to reduce transmission
�� Case fatality rate is extremely high (from 5% up to 40%) in absence of a proper treatment
Food shortages No
Lack of safe water and poor sanitation
Yes The most important risk factor
Others No
Risk assessment conclusions
Risk of cholera outbreaks is extremely high in the refugee camps
In the general population the risk is related to the availability of safe water
PREVENTION AND CONTROL MEASURES
Case Management �� The prevention and treatment of dehydration, using ORS or i.v. fluids (ringer lactate) if severely dehydrated patient, is the mainstay of the case management of cholera
�� Use of antibiotics (doxicycline/tetracycline) is not essential for disease treatment but may be used to shorten the duration of the diarrhoea
Epidemic control �� Inform the Health Authorities if one or more suspected cases are identified
�� Confirm the outbreak, following WHO guidelines. Stool samples must be taken with a rectal swab and transported in Cary Blair medium. It is recommended that 10-20 cases be used to confirm the cause, identify antibiotic sensitivity and verify the outbreak. Once confirmed, it is not necessary to obtain laboratory confirmation for every patient as this depletes laboratory supplies.
Do not wait for laboratory results before starting treatment/control activities
�� Confirm the diagnosis and ensure prompt treatment
�� Isolate cases in cholera treatment centres
Prevention �� See prevention of diarrhoeal diseases
See Annex 3 : Safe Water and Sanitation
See Guidelines for cholera control, WHO 1993
Immunization Two oral vaccines are currently available:
�� killed cholera vaccine (WC/rBS, two doses); and �� live attenuated vaccine (CVD103- HgR, single dose)
They are licensed in a few countries only. Both might be used in carefully evaluated emergency situations, such as refugee camps or slum residents. Cholera vaccine has to be used in conjunction with other prevention and control measures
Communicable Disease Profile for Afghanistan and Neighbouring Countries
WHO Communicable Disease WG on Emergencies/October 2001 10
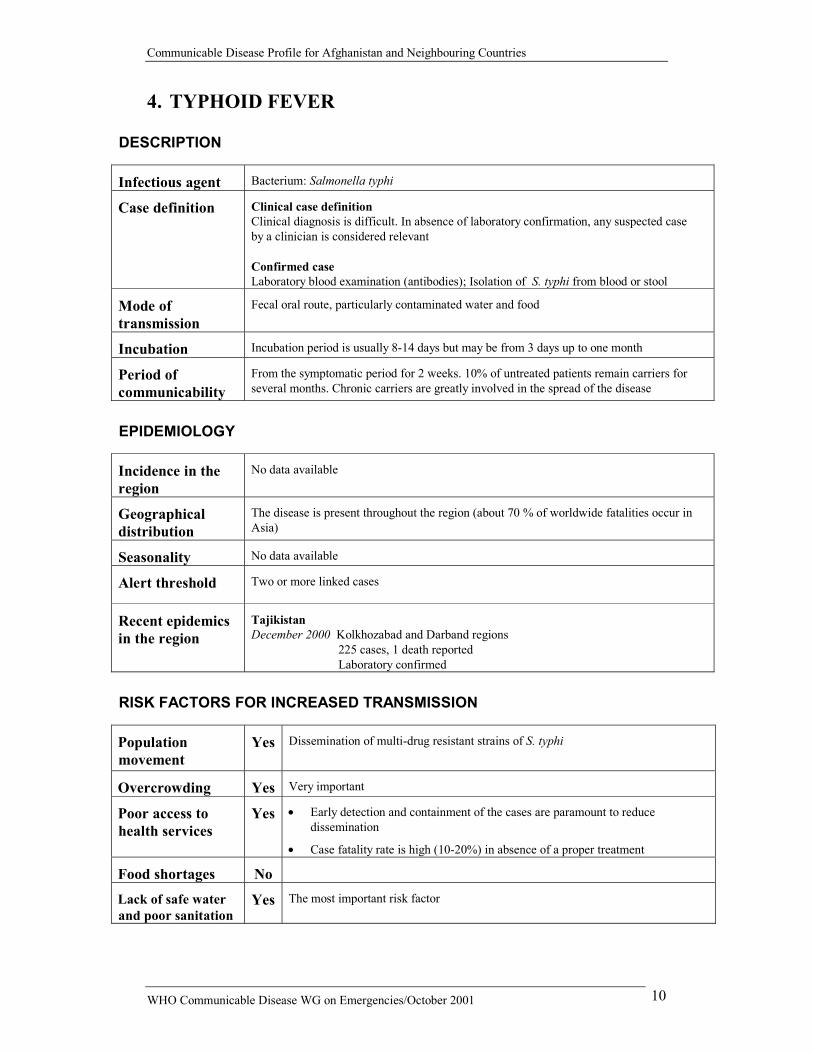
4. TYPHOID FEVER DESCRIPTION
Infectious agent Bacterium: Salmonella typhi
Case definition
Clinical case definition Clinical diagnosis is difficult. In absence of laboratory confirmation, any suspected case by a clinician is considered relevant Confirmed case Laboratory blood examination (antibodies); Isolation of S. typhi from blood or stool
Mode of transmission
Fecal oral route, particularly contaminated water and food
Incubation Incubation period is usually 8-14 days but may be from 3 days up to one month
Period of communicability
From the symptomatic period for 2 weeks. 10% of untreated patients remain carriers for several months. Chronic carriers are greatly involved in the spread of the disease
EPIDEMIOLOGY
Incidence in the region
No data available
Geographical distribution
The disease is present throughout the region (about 70 % of worldwide fatalities occur in Asia)
Seasonality No data available
Alert threshold Two or more linked cases
Recent epidemics in the region
Tajikistan December 2000 Kolkhozabad and Darband regions
225 cases, 1 death reported Laboratory confirmed
RISK FACTORS FOR INCREASED TRANSMISSION
Population movement
Yes Dissemination of multi-drug resistant strains of S. typhi
Overcrowding Yes Very important
Poor access to health services
Yes �� Early detection and containment of the cases are paramount to reduce dissemination
�� Case fatality rate is high (10-20%) in absence of a proper treatment
Food shortages No
Lack of safe water and poor sanitation
Yes The most important risk factor
Communicable Disease Profile for Afghanistan and Neighbouring Countries
WHO Communicable Disease WG on Emergencies/October 2001 11
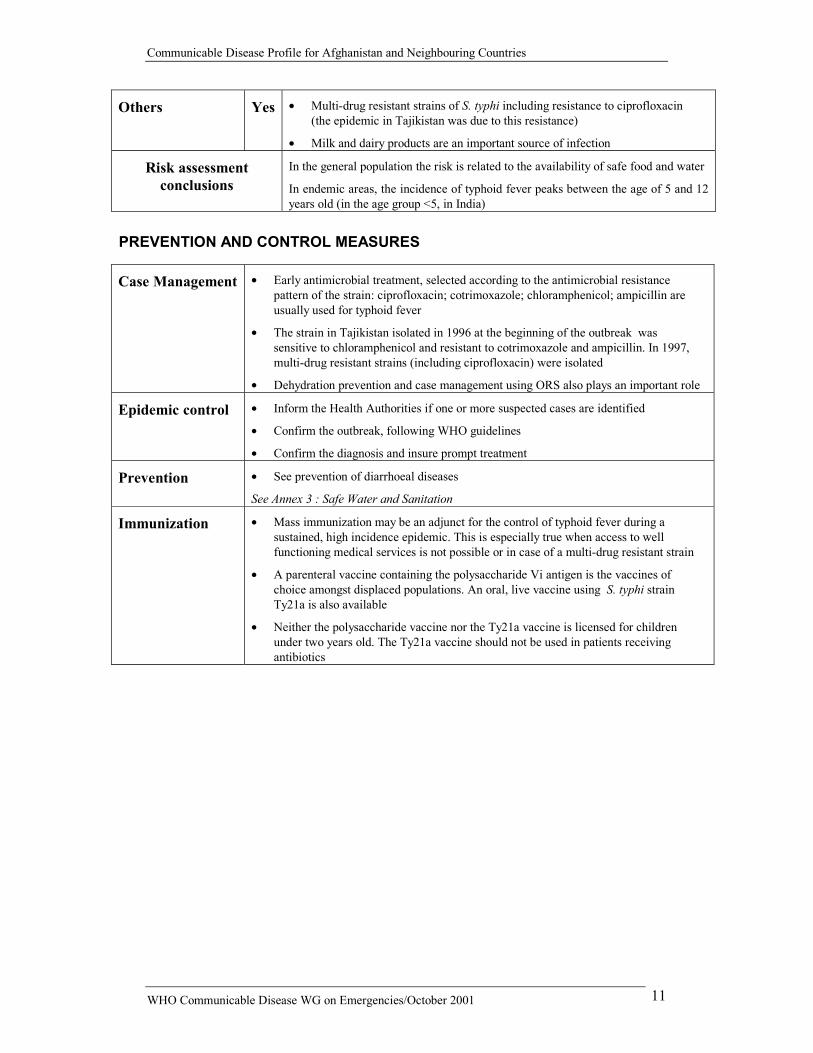
Others Yes �� Multi-drug resistant strains of S. typhi including resistance to ciprofloxacin (the epidemic in Tajikistan was due to this resistance)
�� Milk and dairy products are an important source of infection
Risk assessment conclusions
In the general population the risk is related to the availability of safe food and water
In endemic areas, the incidence of typhoid fever peaks between the age of 5 and 12 years old (in the age group <5, in India)
PREVENTION AND CONTROL MEASURES
Case Management �� Early antimicrobial treatment, selected according to the antimicrobial resistance pattern of the strain: ciprofloxacin; cotrimoxazole; chloramphenicol; ampicillin are usually used for typhoid fever
�� The strain in Tajikistan isolated in 1996 at the beginning of the outbreak was sensitive to chloramphenicol and resistant to cotrimoxazole and ampicillin. In 1997, multi-drug resistant strains (including ciprofloxacin) were isolated
�� Dehydration prevention and case management using ORS also plays an important role
Epidemic control �� Inform the Health Authorities if one or more suspected cases are identified
�� Confirm the outbreak, following WHO guidelines
�� Confirm the diagnosis and insure prompt treatment
Prevention �� See prevention of diarrhoeal diseases See Annex 3 : Safe Water and Sanitation
Immunization �� Mass immunization may be an adjunct for the control of typhoid fever during a sustained, high incidence epidemic. This is especially true when access to well functioning medical services is not possible or in case of a multi-drug resistant strain
�� A parenteral vaccine containing the polysaccharide Vi antigen is the vaccines of choice amongst displaced populations. An oral, live vaccine using S. typhi strain Ty21a is also available
�� Neither the polysaccharide vaccine nor the Ty21a vaccine is licensed for children under two years old. The Ty21a vaccine should not be used in patients receiving antibiotics
Communicable Disease Profile for Afghanistan and Neighbouring Countries
WHO Communicable Disease WG on Emergencies/October 2001 12
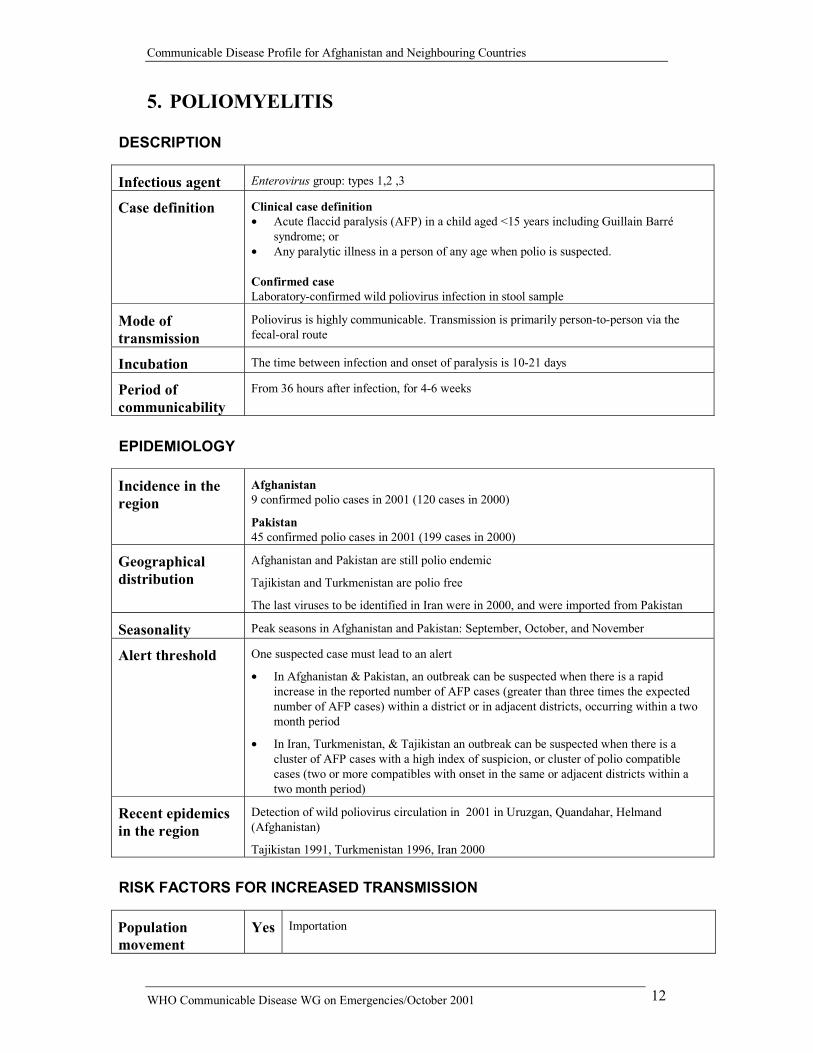
5. POLIOMYELITIS DESCRIPTION
Infectious agent Enterovirus group: types 1,2 ,3
Case definition
Clinical case definition �� Acute flaccid paralysis (AFP) in a child aged <15 years including Guillain Barré
syndrome; or �� Any paralytic illness in a person of any age when polio is suspected. Confirmed case Laboratory-confirmed wild poliovirus infection in stool sample
Mode of transmission
Poliovirus is highly communicable. Transmission is primarily person-to-person via the fecal-oral route
Incubation The time between infection and onset of paralysis is 10-21 days
Period of communicability
From 36 hours after infection, for 4-6 weeks
EPIDEMIOLOGY
Incidence in the region
Afghanistan 9 confirmed polio cases in 2001 (120 cases in 2000)
Pakistan 45 confirmed polio cases in 2001 (199 cases in 2000)
Geographical distribution
Afghanistan and Pakistan are still polio endemic
Tajikistan and Turkmenistan are polio free
The last viruses to be identified in Iran were in 2000, and were imported from Pakistan
Seasonality Peak seasons in Afghanistan and Pakistan: September, October, and November
Alert threshold One suspected case must lead to an alert
�� In Afghanistan & Pakistan, an outbreak can be suspected when there is a rapid increase in the reported number of AFP cases (greater than three times the expected number of AFP cases) within a district or in adjacent districts, occurring within a two month period
�� In Iran, Turkmenistan, & Tajikistan an outbreak can be suspected when there is a cluster of AFP cases with a high index of suspicion, or cluster of polio compatible cases (two or more compatibles with onset in the same or adjacent districts within a two month period)
Recent epidemics in the region
Detection of wild poliovirus circulation in 2001 in Uruzgan, Quandahar, Helmand (Afghanistan)
Tajikistan 1991, Turkmenistan 1996, Iran 2000
RISK FACTORS FOR INCREASED TRANSMISSION
Population movement
Yes Importation
Communicable Disease Profile for Afghanistan and Neighbouring Countries
WHO Communicable Disease WG on Emergencies/October 2001 13
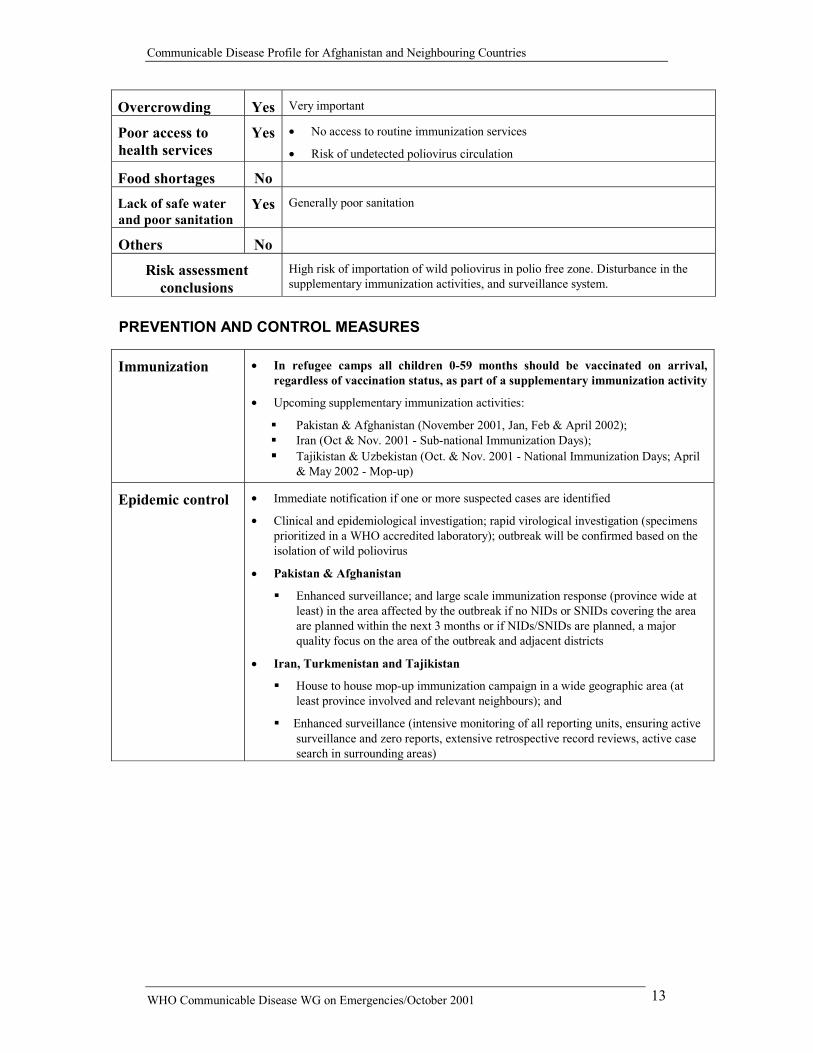
Overcrowding Yes Very important
Poor access to health services
Yes �� No access to routine immunization services
�� Risk of undetected poliovirus circulation
Food shortages No
Lack of safe water and poor sanitation
Yes Generally poor sanitation
Others No
Risk assessment conclusions
High risk of importation of wild poliovirus in polio free zone. Disturbance in the supplementary immunization activities, and surveillance system.
PREVENTION AND CONTROL MEASURES
Immunization �� In refugee camps all children 0-59 months should be vaccinated on arrival, regardless of vaccination status, as part of a supplementary immunization activity
�� Upcoming supplementary immunization activities:
�� Pakistan & Afghanistan (November 2001, Jan, Feb & April 2002); �� Iran (Oct & Nov. 2001 - Sub-national Immunization Days); �� Tajikistan & Uzbekistan (Oct. & Nov. 2001 - National Immunization Days; April & May 2002 - Mop-up)
Epidemic control �� Immediate notification if one or more suspected cases are identified
�� Clinical and epidemiological investigation; rapid virological investigation (specimens prioritized in a WHO accredited laboratory); outbreak will be confirmed based on the isolation of wild poliovirus
�� Pakistan & Afghanistan
�� Enhanced surveillance; and large scale immunization response (province wide at least) in the area affected by the outbreak if no NIDs or SNIDs covering the area are planned within the next 3 months or if NIDs/SNIDs are planned, a major quality focus on the area of the outbreak and adjacent districts
�� Iran, Turkmenistan and Tajikistan
�� House to house mop-up immunization campaign in a wide geographic area (at least province involved and relevant neighbours); and
��Enhanced surveillance (intensive monitoring of all reporting units, ensuring active surveillance and zero reports, extensive retrospective record reviews, active case search in surrounding areas)
Communicable Disease Profile for Afghanistan and Neighbouring Countries
WHO Communicable Disease WG on Emergencies/October 2001 14
Respiratory-Borne Diseases
6. ACUTE LOWER RESPIRATORY INFECTIONS (ALRI)
DESCRIPTION
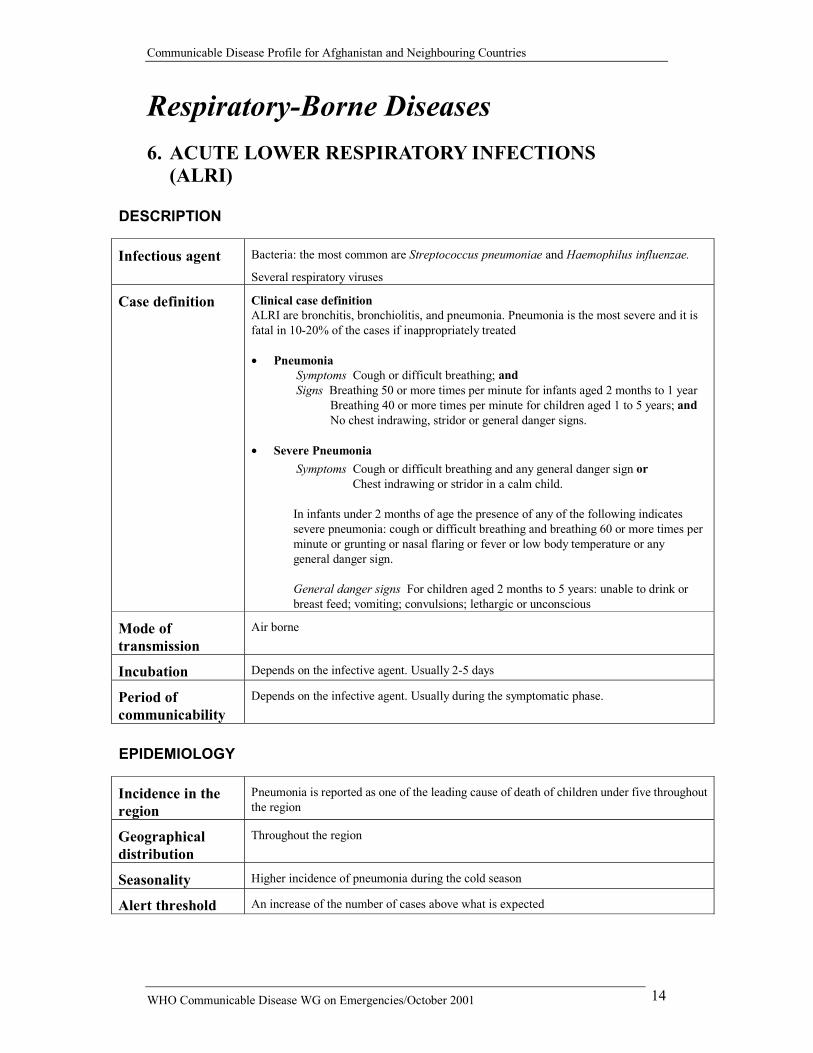
Infectious agent Bacteria: the most common are Streptococcus pneumoniae and Haemophilus influenzae.
Several respiratory viruses
Case definition
Clinical case definition ALRI are bronchitis, bronchiolitis, and pneumonia. Pneumonia is the most severe and it is fatal in 10-20% of the cases if inappropriately treated �� Pneumonia Symptoms Cough or difficult breathing; and Signs Breathing 50 or more times per minute for infants aged 2 months to 1 year
Breathing 40 or more times per minute for children aged 1 to 5 years; and No chest indrawing, stridor or general danger signs.
�� Severe Pneumonia Symptoms Cough or difficult breathing and any general danger sign or
Chest indrawing or stridor in a calm child.
In infants under 2 months of age the presence of any of the following indicates severe pneumonia: cough or difficult breathing and breathing 60 or more times per minute or grunting or nasal flaring or fever or low body temperature or any general danger sign.
General danger signs For children aged 2 months to 5 years: unable to drink or breast feed; vomiting; convulsions; lethargic or unconscious
Mode of transmission
Air borne
Incubation Depends on the infective agent. Usually 2-5 days
Period of communicability
Depends on the infective agent. Usually during the symptomatic phase.
EPIDEMIOLOGY
Incidence in the region
Pneumonia is reported as one of the leading cause of death of children under five throughout the region
Geographical distribution
Throughout the region
Seasonality Higher incidence of pneumonia during the cold season
Alert threshold An increase of the number of cases above what is expected
Communicable Disease Profile for Afghanistan and Neighbouring Countries
WHO Communicable Disease WG on Emergencies/October 2001 15
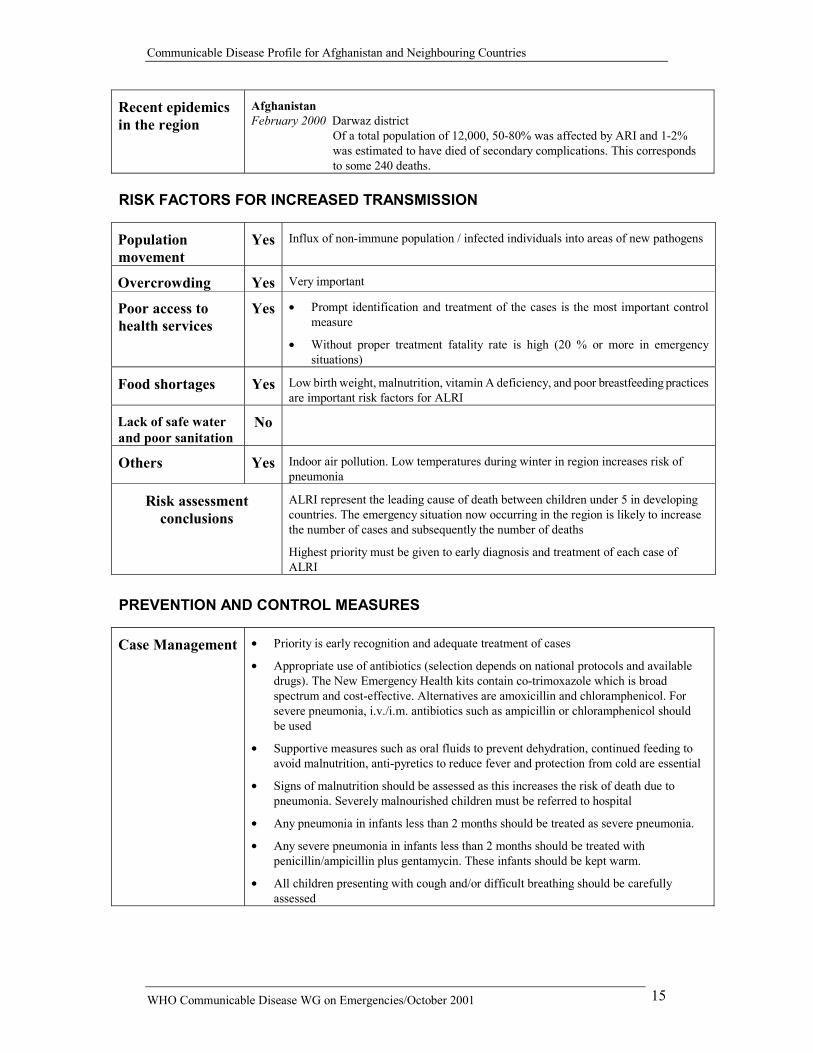
Recent epidemics in the region
Afghanistan February 2000 Darwaz district
Of a total population of 12,000, 50-80% was affected by ARI and 1-2% was estimated to have died of secondary complications. This corresponds to some 240 deaths.
RISK FACTORS FOR INCREASED TRANSMISSION
Population movement
Yes Influx of non-immune population / infected individuals into areas of new pathogens
Overcrowding Yes Very important
Poor access to health services
Yes �� Prompt identification and treatment of the cases is the most important control measure
�� Without proper treatment fatality rate is high (20 % or more in emergency situations)
Food shortages Yes Low birth weight, malnutrition, vitamin A deficiency, and poor breastfeeding practices are important risk factors for ALRI
Lack of safe water and poor sanitation
No
Others Yes Indoor air pollution. Low temperatures during winter in region increases risk of pneumonia
Risk assessment conclusions
ALRI represent the leading cause of death between children under 5 in developing countries. The emergency situation now occurring in the region is likely to increase the number of cases and subsequently the number of deaths
Highest priority must be given to early diagnosis and treatment of each case of ALRI
PREVENTION AND CONTROL MEASURES
Case Management �� Priority is early recognition and adequate treatment of cases
�� Appropriate use of antibiotics (selection depends on national protocols and available drugs). The New Emergency Health kits contain co-trimoxazole which is broad spectrum and cost-effective. Alternatives are amoxicillin and chloramphenicol. For severe pneumonia, i.v./i.m. antibiotics such as ampicillin or chloramphenicol should be used
�� Supportive measures such as oral fluids to prevent dehydration, continued feeding to avoid malnutrition, anti-pyretics to reduce fever and protection from cold are essential
�� Signs of malnutrition should be assessed as this increases the risk of death due to pneumonia. Severely malnourished children must be referred to hospital
�� Any pneumonia in infants less than 2 months should be treated as severe pneumonia.
�� Any severe pneumonia in infants less than 2 months should be treated with penicillin/ampicillin plus gentamycin. These infants should be kept warm.
�� All children presenting with cough and/or difficult breathing should be carefully assessed
Communicable Disease Profile for Afghanistan and Neighbouring Countries
WHO Communicable Disease WG on Emergencies/October 2001 16
Prevention �� Community wide awareness campaign on early danger signs
�� Adequate feeding to avoid malnutrition
�� Protection from the cold
Immunization �� Measles, diphtheria and whooping cough immunization are effective to reduce impact of ARLI
Communicable Disease Profile for Afghanistan and Neighbouring Countries
WHO Communicable Disease WG on Emergencies/October 2001 17
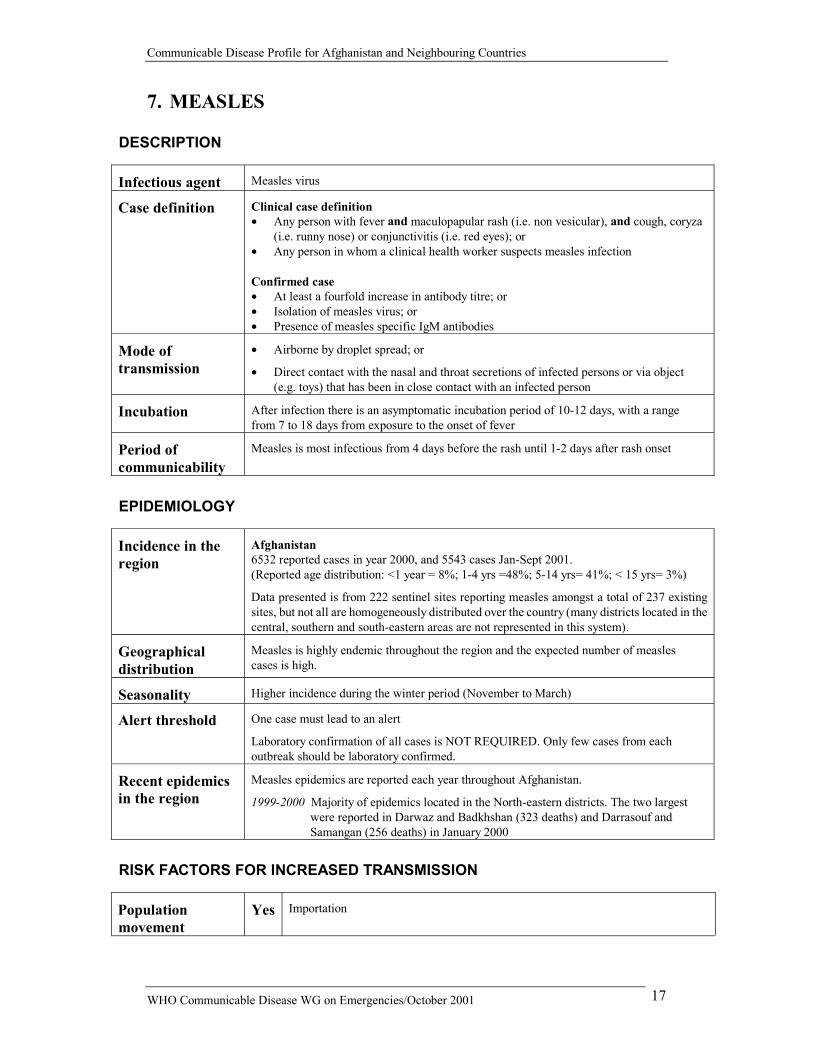
7. MEASLES DESCRIPTION
Infectious agent Measles virus
Case definition
Clinical case definition �� Any person with fever and maculopapular rash (i.e. non vesicular), and cough, coryza
(i.e. runny nose) or conjunctivitis (i.e. red eyes); or �� Any person in whom a clinical health worker suspects measles infection Confirmed case �� At least a fourfold increase in antibody titre; or �� Isolation of measles virus; or �� Presence of measles specific IgM antibodies
Mode of transmission
�� Airborne by droplet spread; or
�� Direct contact with the nasal and throat secretions of infected persons or via object (e.g. toys) that has been in close contact with an infected person
Incubation After infection there is an asymptomatic incubation period of 10-12 days, with a range from 7 to 18 days from exposure to the onset of fever
Period of communicability
Measles is most infectious from 4 days before the rash until 1-2 days after rash onset
EPIDEMIOLOGY
Incidence in the region
Afghanistan 6532 reported cases in year 2000, and 5543 cases Jan-Sept 2001. (Reported age distribution: <1 year = 8%; 1-4 yrs =48%; 5-14 yrs= 41%; < 15 yrs= 3%)
Data presented is from 222 sentinel sites reporting measles amongst a total of 237 existing sites, but not all are homogeneously distributed over the country (many districts located in the central, southern and south-eastern areas are not represented in this system).
Geographical distribution
Measles is highly endemic throughout the region and the expected number of measles cases is high.
Seasonality Higher incidence during the winter period (November to March)
Alert threshold One case must lead to an alert
Laboratory confirmation of all cases is NOT REQUIRED. Only few cases from each outbreak should be laboratory confirmed.
Recent epidemics in the region
Measles epidemics are reported each year throughout Afghanistan.
1999-2000 Majority of epidemics located in the North-eastern districts. The two largest were reported in Darwaz and Badkhshan (323 deaths) and Darrasouf and Samangan (256 deaths) in January 2000
RISK FACTORS FOR INCREASED TRANSMISSION
Population movement
Yes Importation
Communicable Disease Profile for Afghanistan and Neighbouring Countries
WHO Communicable Disease WG on Emergencies/October 2001 18
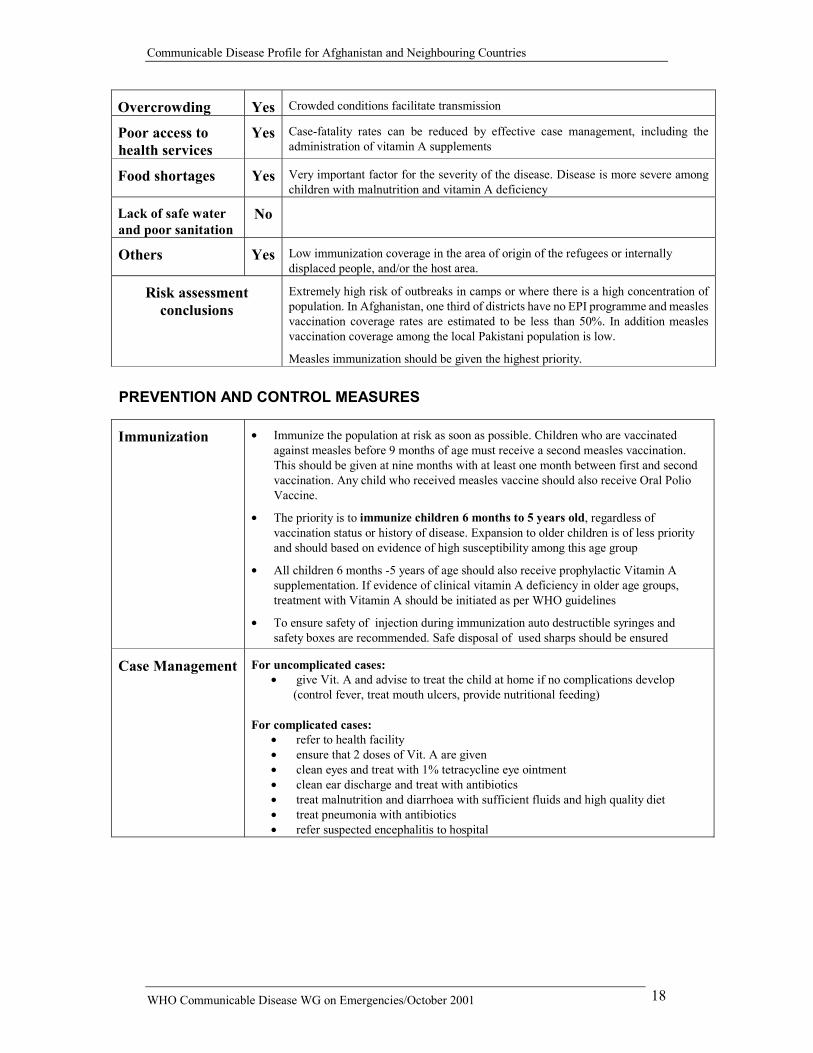
Overcrowding Yes Crowded conditions facilitate transmission
Poor access to health services
Yes Case-fatality rates can be reduced by effective case management, including the administration of vitamin A supplements
Food shortages Yes Very important factor for the severity of the disease. Disease is more severe among children with malnutrition and vitamin A deficiency
Lack of safe water and poor sanitation
No
Others Yes Low immunization coverage in the area of origin of the refugees or internally displaced people, and/or the host area.
Risk assessment conclusions
Extremely high risk of outbreaks in camps or where there is a high concentration of population. In Afghanistan, one third of districts have no EPI programme and measles vaccination coverage rates are estimated to be less than 50%. In addition measles vaccination coverage among the local Pakistani population is low.
Measles immunization should be given the highest priority.
PREVENTION AND CONTROL MEASURES
Immunization �� Immunize the population at risk as soon as possible. Children who are vaccinated against measles before 9 months of age must receive a second measles vaccination. This should be given at nine months with at least one month between first and second vaccination. Any child who received measles vaccine should also receive Oral Polio Vaccine.
�� The priority is to immunize children 6 months to 5 years old, regardless of vaccination status or history of disease. Expansion to older children is of less priority and should based on evidence of high susceptibility among this age group
�� All children 6 months -5 years of age should also receive prophylactic Vitamin A supplementation. If evidence of clinical vitamin A deficiency in older age groups, treatment with Vitamin A should be initiated as per WHO guidelines
�� To ensure safety of injection during immunization auto destructible syringes and safety boxes are recommended. Safe disposal of used sharps should be ensured
Case Management For uncomplicated cases: �� give Vit. A and advise to treat the child at home if no complications develop
(control fever, treat mouth ulcers, provide nutritional feeding) For complicated cases:
�� refer to health facility �� ensure that 2 doses of Vit. A are given �� clean eyes and treat with 1% tetracycline eye ointment �� clean ear discharge and treat with antibiotics �� treat malnutrition and diarrhoea with sufficient fluids and high quality diet �� treat pneumonia with antibiotics �� refer suspected encephalitis to hospital
Communicable Disease Profile for Afghanistan and Neighbouring Countries
WHO Communicable Disease WG on Emergencies/October 2001 19
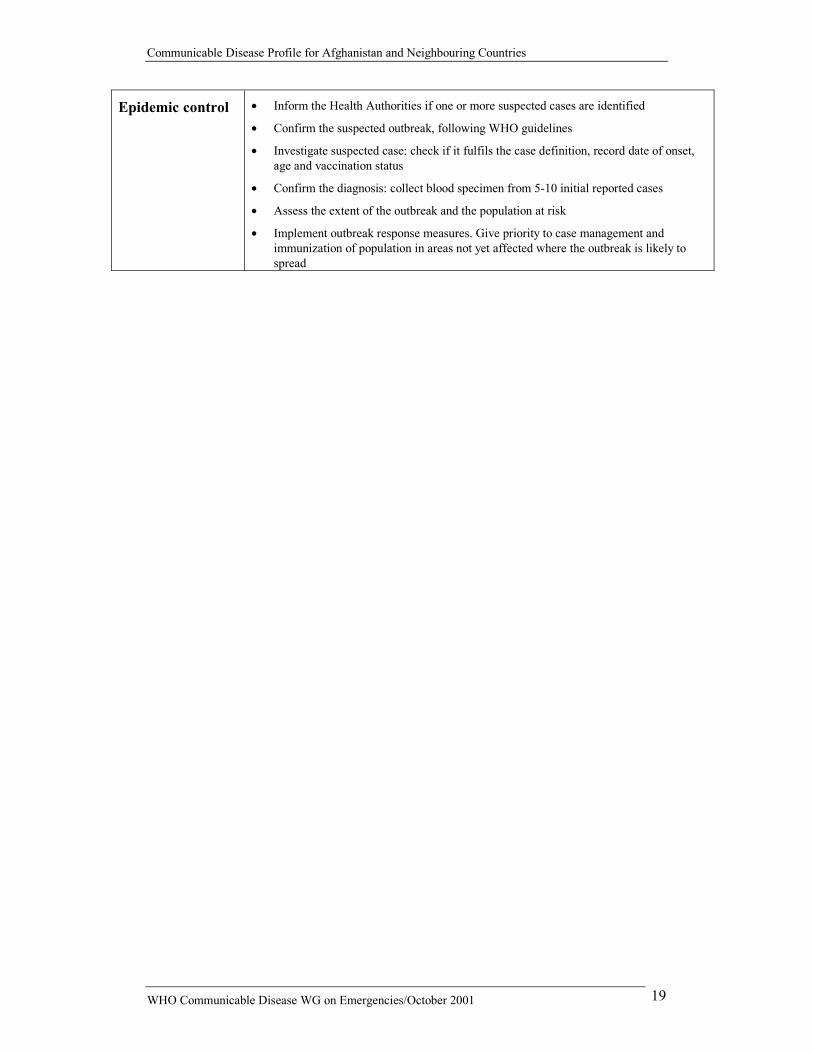
Epidemic control �� Inform the Health Authorities if one or more suspected cases are identified
�� Confirm the suspected outbreak, following WHO guidelines
�� Investigate suspected case: check if it fulfils the case definition, record date of onset, age and vaccination status
�� Confirm the diagnosis: collect blood specimen from 5-10 initial reported cases
�� Assess the extent of the outbreak and the population at risk
�� Implement outbreak response measures. Give priority to case management and immunization of population in areas not yet affected where the outbreak is likely to spread
Communicable Disease Profile for Afghanistan and Neighbouring Countries
WHO Communicable Disease WG on Emergencies/October 2001 20
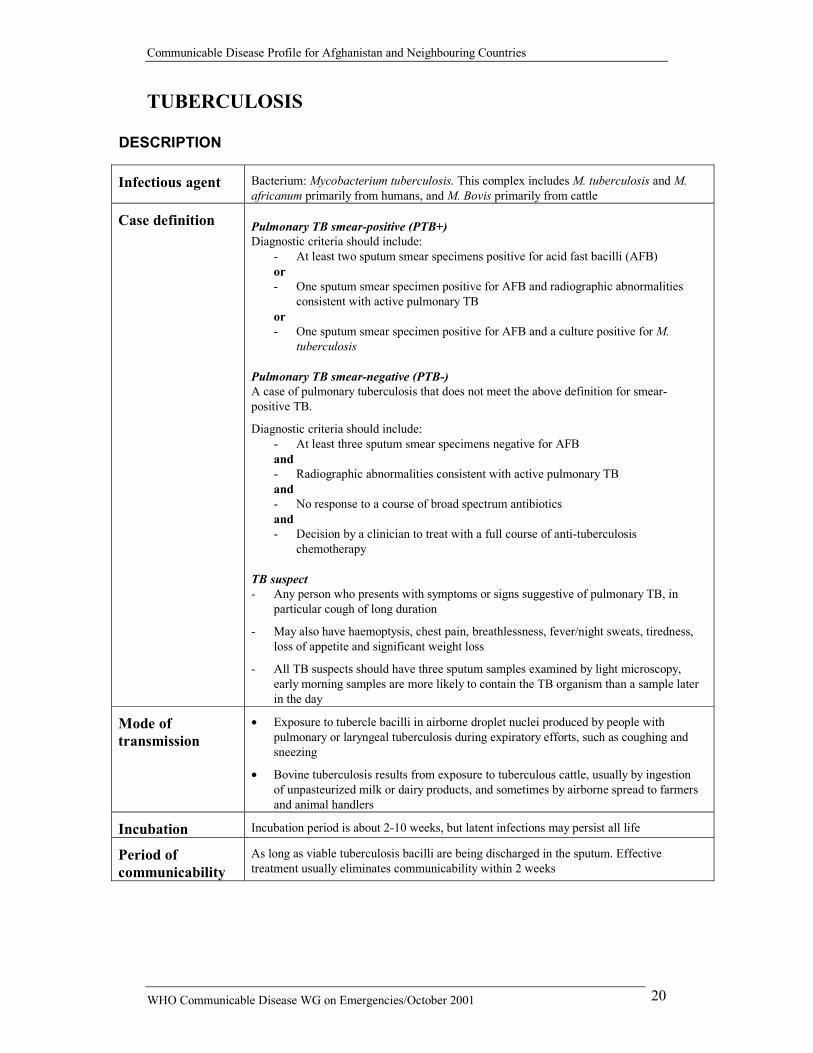
TUBERCULOSIS DESCRIPTION
Infectious agent Bacterium: Mycobacterium tuberculosis. This complex includes M. tuberculosis and M. africanum primarily from humans, and M. Bovis primarily from cattle
Case definition
Pulmonary TB smear-positive (PTB+) Diagnostic criteria should include:
- At least two sputum smear specimens positive for acid fast bacilli (AFB) or - One sputum smear specimen positive for AFB and radiographic abnormalities
consistent with active pulmonary TB or - One sputum smear specimen positive for AFB and a culture positive for M.
tuberculosis Pulmonary TB smear-negative (PTB-) A case of pulmonary tuberculosis that does not meet the above definition for smear-positive TB.
Diagnostic criteria should include: - At least three sputum smear specimens negative for AFB and - Radiographic abnormalities consistent with active pulmonary TB and - No response to a course of broad spectrum antibiotics and - Decision by a clinician to treat with a full course of anti-tuberculosis
chemotherapy TB suspect - Any person who presents with symptoms or signs suggestive of pulmonary TB, in
particular cough of long duration
- May also have haemoptysis, chest pain, breathlessness, fever/night sweats, tiredness, loss of appetite and significant weight loss
- All TB suspects should have three sputum samples examined by light microscopy, early morning samples are more likely to contain the TB organism than a sample later in the day
Mode of transmission
�� Exposure to tubercle bacilli in airborne droplet nuclei produced by people with pulmonary or laryngeal tuberculosis during expiratory efforts, such as coughing and sneezing
�� Bovine tuberculosis results from exposure to tuberculous cattle, usually by ingestion of unpasteurized milk or dairy products, and sometimes by airborne spread to farmers and animal handlers
Incubation Incubation period is about 2-10 weeks, but latent infections may persist all life
Period of communicability
As long as viable tuberculosis bacilli are being discharged in the sputum. Effective treatment usually eliminates communicability within 2 weeks
Communicable Disease Profile for Afghanistan and Neighbouring Countries
WHO Communicable Disease WG on Emergencies/October 2001 21
EPIDEMIOLOGY
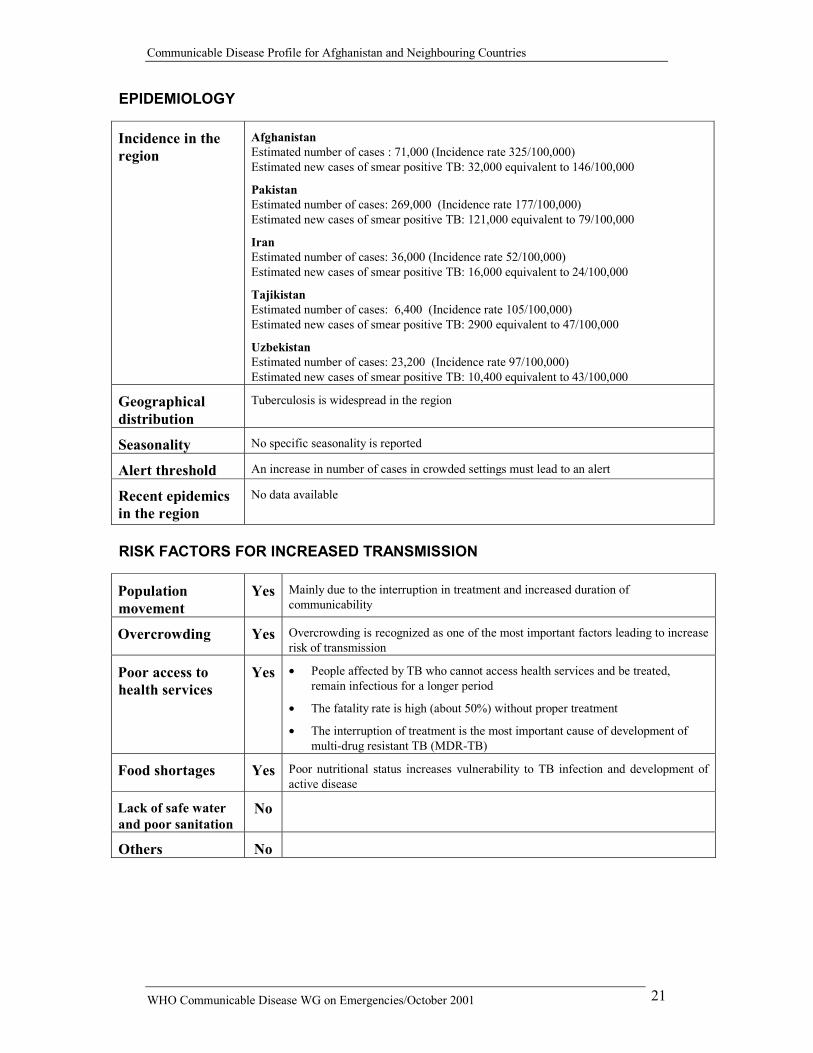
Incidence in the region
Afghanistan Estimated number of cases : 71,000 (Incidence rate 325/100,000) Estimated new cases of smear positive TB: 32,000 equivalent to 146/100,000
Pakistan Estimated number of cases: 269,000 (Incidence rate 177/100,000) Estimated new cases of smear positive TB: 121,000 equivalent to 79/100,000
Iran Estimated number of cases: 36,000 (Incidence rate 52/100,000) Estimated new cases of smear positive TB: 16,000 equivalent to 24/100,000
Tajikistan Estimated number of cases: 6,400 (Incidence rate 105/100,000) Estimated new cases of smear positive TB: 2900 equivalent to 47/100,000
Uzbekistan Estimated number of cases: 23,200 (Incidence rate 97/100,000) Estimated new cases of smear positive TB: 10,400 equivalent to 43/100,000
Geographical distribution
Tuberculosis is widespread in the region
Seasonality No specific seasonality is reported
Alert threshold An increase in number of cases in crowded settings must lead to an alert
Recent epidemics in the region
No data available
RISK FACTORS FOR INCREASED TRANSMISSION
Population movement
Yes Mainly due to the interruption in treatment and increased duration of communicability
Overcrowding Yes Overcrowding is recognized as one of the most important factors leading to increase risk of transmission
Poor access to health services
Yes �� People affected by TB who cannot access health services and be treated, remain infectious for a longer period
�� The fatality rate is high (about 50%) without proper treatment
�� The interruption of treatment is the most important cause of development of multi-drug resistant TB (MDR-TB)
Food shortages Yes Poor nutritional status increases vulnerability to TB infection and development of active disease
Lack of safe water and poor sanitation
No
Others No
Communicable Disease Profile for Afghanistan and Neighbouring Countries
WHO Communicable Disease WG on Emergencies/October 2001 22
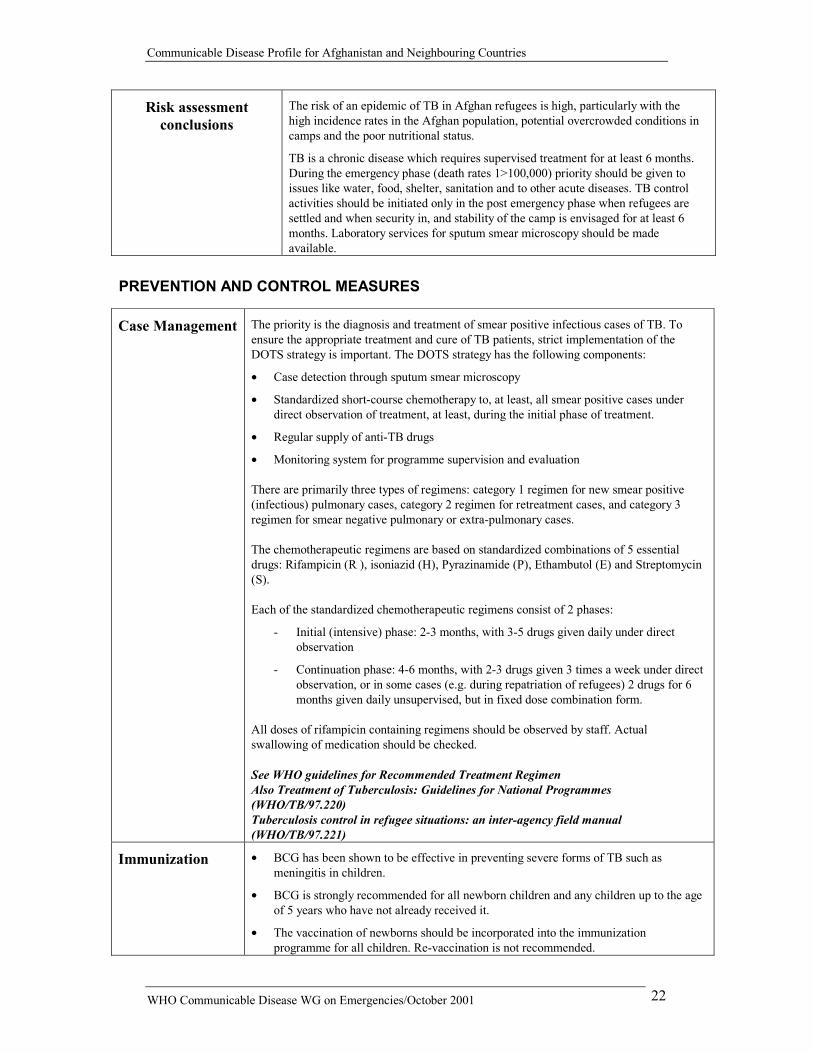
Risk assessment conclusions
The risk of an epidemic of TB in Afghan refugees is high, particularly with the high incidence rates in the Afghan population, potential overcrowded conditions in camps and the poor nutritional status.
TB is a chronic disease which requires supervised treatment for at least 6 months. During the emergency phase (death rates 1>100,000) priority should be given to issues like water, food, shelter, sanitation and to other acute diseases. TB control activities should be initiated only in the post emergency phase when refugees are settled and when security in, and stability of the camp is envisaged for at least 6 months. Laboratory services for sputum smear microscopy should be made available.
PREVENTION AND CONTROL MEASURES
Case Management The priority is the diagnosis and treatment of smear positive infectious cases of TB. To ensure the appropriate treatment and cure of TB patients, strict implementation of the DOTS strategy is important. The DOTS strategy has the following components:
�� Case detection through sputum smear microscopy
�� Standardized short-course chemotherapy to, at least, all smear positive cases under direct observation of treatment, at least, during the initial phase of treatment.
�� Regular supply of anti-TB drugs
�� Monitoring system for programme supervision and evaluation There are primarily three types of regimens: category 1 regimen for new smear positive (infectious) pulmonary cases, category 2 regimen for retreatment cases, and category 3 regimen for smear negative pulmonary or extra-pulmonary cases. The chemotherapeutic regimens are based on standardized combinations of 5 essential drugs: Rifampicin (R ), isoniazid (H), Pyrazinamide (P), Ethambutol (E) and Streptomycin (S). Each of the standardized chemotherapeutic regimens consist of 2 phases:
- Initial (intensive) phase: 2-3 months, with 3-5 drugs given daily under direct observation
- Continuation phase: 4-6 months, with 2-3 drugs given 3 times a week under direct observation, or in some cases (e.g. during repatriation of refugees) 2 drugs for 6 months given daily unsupervised, but in fixed dose combination form.
All doses of rifampicin containing regimens should be observed by staff. Actual swallowing of medication should be checked. See WHO guidelines for Recommended Treatment Regimen Also Treatment of Tuberculosis: Guidelines for National Programmes (WHO/TB/97.220) Tuberculosis control in refugee situations: an inter-agency field manual (WHO/TB/97.221)
Immunization �� BCG has been shown to be effective in preventing severe forms of TB such as meningitis in children.
�� BCG is strongly recommended for all newborn children and any children up to the age of 5 years who have not already received it.
�� The vaccination of newborns should be incorporated into the immunization programme for all children. Re-vaccination is not recommended.

Communicable Disease Profile for Afghanistan and Neighbouring Countries
WHO Communicable Disease WG on Emergencies/October 2001 23
Prevention �� Detection and treatment of smear positive TB cases is the most effective preventive measure
�� Health education to improve awareness and reduce stigma
�� Maintaining good ventilation and reducing overcrowding in health clinics, and ensuring hospitalized patients are kept in a separate ward for the first two weeks of treatment.
�� Isoniazid prophylaxis is not recommended in refugee situations, except for children being breast-fed by smear positive mothers. If the child is well, BCG vaccination should be postponed and isoniazid should be given to the child for 6 months. In the event of a sudden disruption to the programme, isoniazid may be stopped, and BCG should be given before the child leaves the refugee camp (preferably after a one week interval)

Communicable Disease Profile for Afghanistan and Neighbouring Countries
WHO Communicable Disease WG on Emergencies/October 2001 24
9. MENINGOCOCCAL DISEASE (MENINGITIS and SEPTICAEMIC FORM)
DESCRIPTION
Infectious agent Bacterium: Neisseria meningitidis serogroups A,B,C,Y,W135
Case definition
Clinical case definition Person with sudden onset of fever (>38.0 °C axillary) and one of the following:
�� neck stiffness �� altered consciousness �� other meningeal sign
or petechial or purpural rash
In patients under one year of age meningitis is suspected when fever is accompanied by a bulging fontanelle Confirmed case Positive cerebro-spinal fluid antigen detection or cerebro-spinal fluid positive culture or blood positive culture
Mode of transmission
Direct contact with respiratory droplets
Incubation Incubation period varies between 2 to 10 days, most commonly 4 days
Period of communicability
From the beginning of the symptoms till 24 hours after the institution of the therapy, but the most important source of infection are asymptomatic carriers
EPIDEMIOLOGY
Incidence in the region
No data available
Geographical distribution
Sporadic cases throughout the region
Seasonality Increase in incidence during cold months
Alert threshold Five cases per 100,000 per week or a cluster of cases in an area
Recent epidemics in the region
Afghanistan Spring 2000 Central highlands
175 cases and 7 deaths
May 2001 Kandahar 30 cases and 1 death
India 1985 New Delhi
6133 cases
Communicable Disease Profile for Afghanistan and Neighbouring Countries
WHO Communicable Disease WG on Emergencies/October 2001 25
RISK FACTORS FOR INCREASED TRANSMISSION
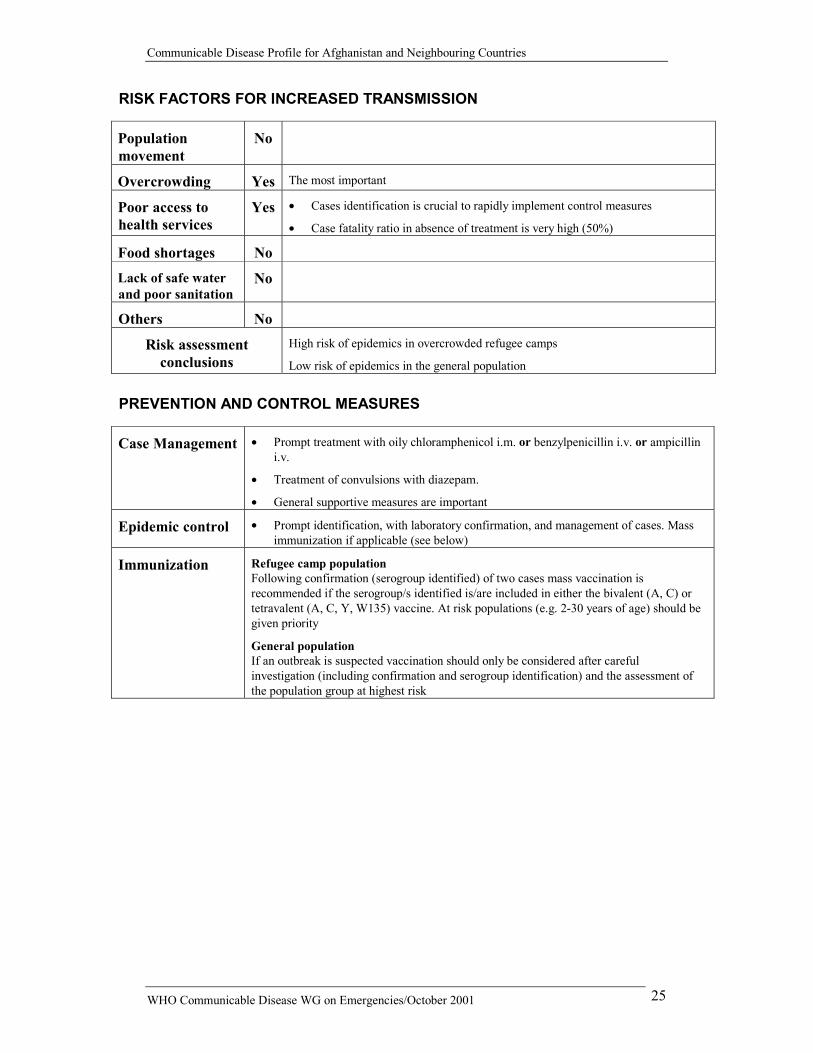
Population movement
No
Overcrowding Yes The most important
Poor access to health services
Yes �� Cases identification is crucial to rapidly implement control measures
�� Case fatality ratio in absence of treatment is very high (50%)
Food shortages No
Lack of safe water and poor sanitation
No
Others No
Risk assessment conclusions
High risk of epidemics in overcrowded refugee camps
Low risk of epidemics in the general population
PREVENTION AND CONTROL MEASURES
Case Management �� Prompt treatment with oily chloramphenicol i.m. or benzylpenicillin i.v. or ampicillin i.v.
�� Treatment of convulsions with diazepam.
�� General supportive measures are important
Epidemic control �� Prompt identification, with laboratory confirmation, and management of cases. Mass immunization if applicable (see below)
Immunization Refugee camp population Following confirmation (serogroup identified) of two cases mass vaccination is recommended if the serogroup/s identified is/are included in either the bivalent (A, C) or tetravalent (A, C, Y, W135) vaccine. At risk populations (e.g. 2-30 years of age) should be given priority
General population If an outbreak is suspected vaccination should only be considered after careful investigation (including confirmation and serogroup identification) and the assessment of the population group at highest risk
Communicable Disease Profile for Afghanistan and Neighbouring Countries
WHO Communicable Disease WG on Emergencies/October 2001 26
Vector-Borne Diseases 10. MALARIA
DESCRIPTION
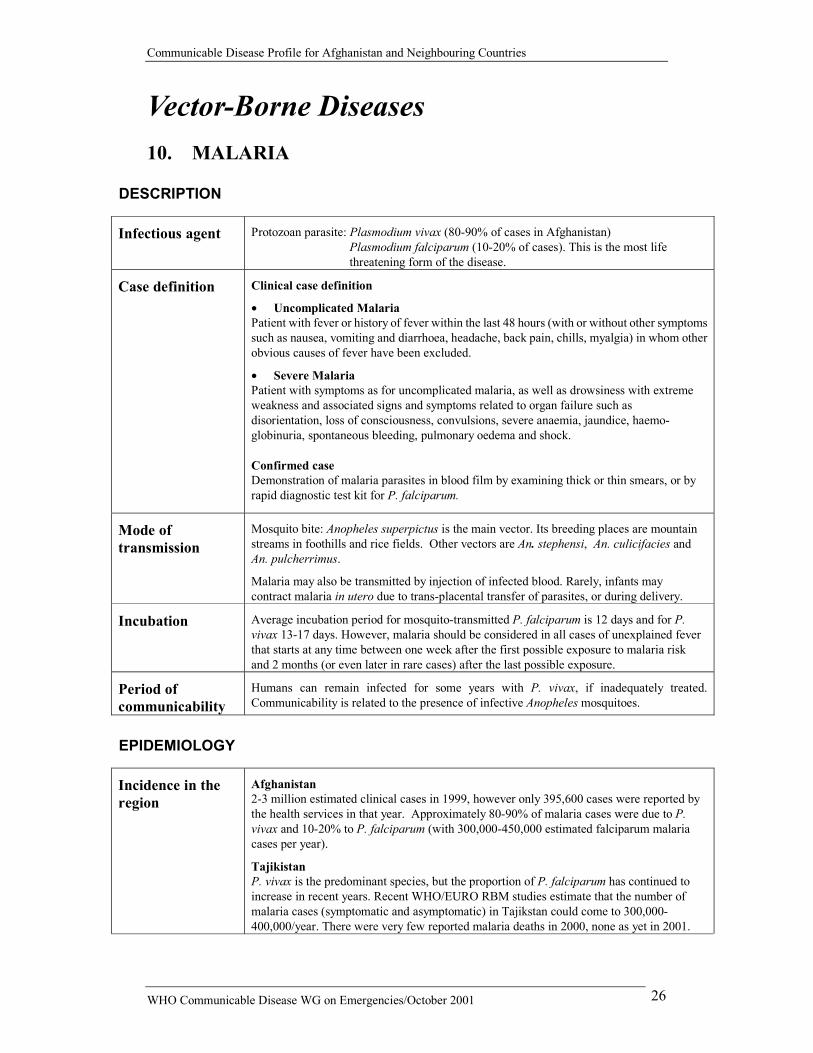
Infectious agent Protozoan parasite: Plasmodium vivax (80-90% of cases in Afghanistan) Plasmodium falciparum (10-20% of cases). This is the most life threatening form of the disease.
Case definition
Clinical case definition
�� Uncomplicated Malaria Patient with fever or history of fever within the last 48 hours (with or without other symptoms such as nausea, vomiting and diarrhoea, headache, back pain, chills, myalgia) in whom other obvious causes of fever have been excluded.
�� Severe Malaria Patient with symptoms as for uncomplicated malaria, as well as drowsiness with extreme weakness and associated signs and symptoms related to organ failure such as disorientation, loss of consciousness, convulsions, severe anaemia, jaundice, haemo-globinuria, spontaneous bleeding, pulmonary oedema and shock. Confirmed case Demonstration of malaria parasites in blood film by examining thick or thin smears, or by rapid diagnostic test kit for P. falciparum.
Mode of transmission
Mosquito bite: Anopheles superpictus is the main vector. Its breeding places are mountain streams in foothills and rice fields. Other vectors are An. stephensi, An. culicifacies and An. pulcherrimus.
Malaria may also be transmitted by injection of infected blood. Rarely, infants may contract malaria in utero due to trans-placental transfer of parasites, or during delivery.
Incubation Average incubation period for mosquito-transmitted P. falciparum is 12 days and for P. vivax 13-17 days. However, malaria should be considered in all cases of unexplained fever that starts at any time between one week after the first possible exposure to malaria risk and 2 months (or even later in rare cases) after the last possible exposure.
Period of communicability
Humans can remain infected for some years with P. vivax, if inadequately treated. Communicability is related to the presence of infective Anopheles mosquitoes.
EPIDEMIOLOGY
Incidence in the region
Afghanistan 2-3 million estimated clinical cases in 1999, however only 395,600 cases were reported by the health services in that year. Approximately 80-90% of malaria cases were due to P. vivax and 10-20% to P. falciparum (with 300,000-450,000 estimated falciparum malaria cases per year).
Tajikistan P. vivax is the predominant species, but the proportion of P. falciparum has continued to increase in recent years. Recent WHO/EURO RBM studies estimate that the number of malaria cases (symptomatic and asymptomatic) in Tajikstan could come to 300,000-400,000/year. There were very few reported malaria deaths in 2000, none as yet in 2001.
Communicable Disease Profile for Afghanistan and Neighbouring Countries
WHO Communicable Disease WG on Emergencies/October 2001 27
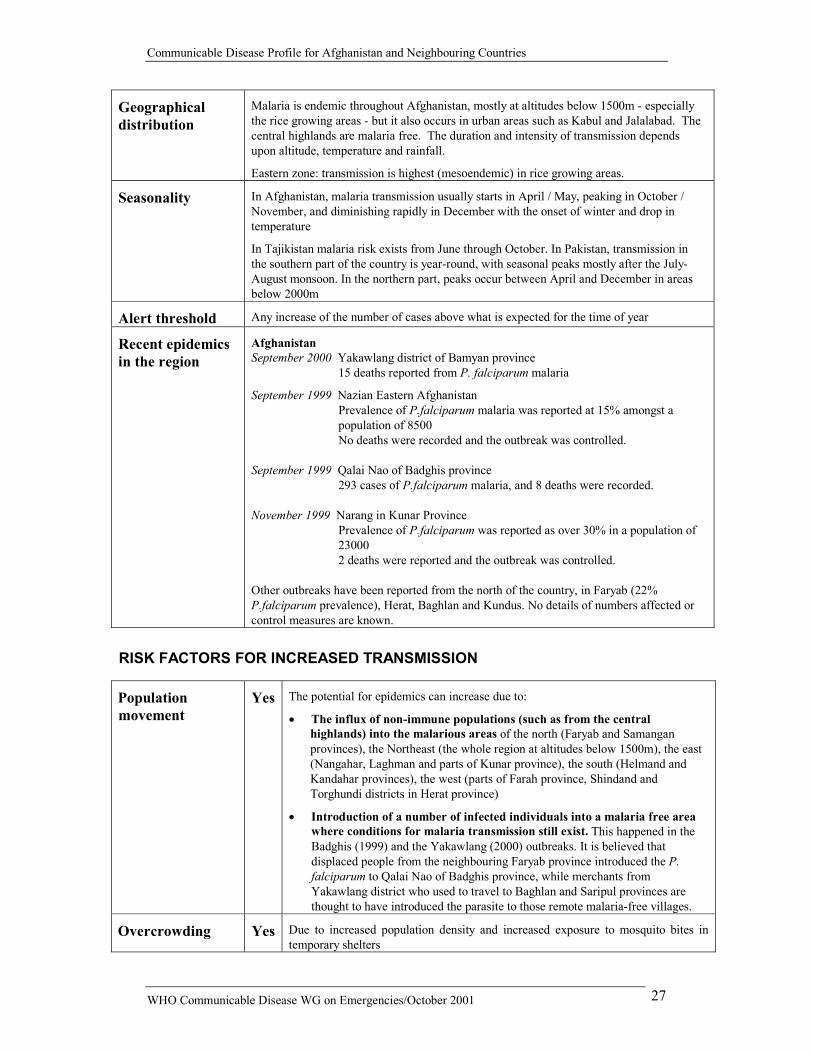
Geographical distribution
Malaria is endemic throughout Afghanistan, mostly at altitudes below 1500m - especially the rice growing areas - but it also occurs in urban areas such as Kabul and Jalalabad. The central highlands are malaria free. The duration and intensity of transmission depends upon altitude, temperature and rainfall.
Eastern zone: transmission is highest (mesoendemic) in rice growing areas.
Seasonality In Afghanistan, malaria transmission usually starts in April / May, peaking in October / November, and diminishing rapidly in December with the onset of winter and drop in temperature
In Tajikistan malaria risk exists from June through October. In Pakistan, transmission in the southern part of the country is year-round, with seasonal peaks mostly after the July-August monsoon. In the northern part, peaks occur between April and December in areas below 2000m
Alert threshold Any increase of the number of cases above what is expected for the time of year
Recent epidemics in the region
Afghanistan September 2000 Yakawlang district of Bamyan province
15 deaths reported from P. falciparum malaria
September 1999 Nazian Eastern Afghanistan Prevalence of P.falciparum malaria was reported at 15% amongst a population of 8500 No deaths were recorded and the outbreak was controlled.
September 1999 Qalai Nao of Badghis province
293 cases of P.falciparum malaria, and 8 deaths were recorded. November 1999 Narang in Kunar Province
Prevalence of P.falciparum was reported as over 30% in a population of 23000 2 deaths were reported and the outbreak was controlled.
Other outbreaks have been reported from the north of the country, in Faryab (22% P.falciparum prevalence), Herat, Baghlan and Kundus. No details of numbers affected or control measures are known.
RISK FACTORS FOR INCREASED TRANSMISSION
Population movement
Yes The potential for epidemics can increase due to:
�� The influx of non-immune populations (such as from the central highlands) into the malarious areas of the north (Faryab and Samangan provinces), the Northeast (the whole region at altitudes below 1500m), the east (Nangahar, Laghman and parts of Kunar province), the south (Helmand and Kandahar provinces), the west (parts of Farah province, Shindand and Torghundi districts in Herat province)
�� Introduction of a number of infected individuals into a malaria free area where conditions for malaria transmission still exist. This happened in the Badghis (1999) and the Yakawlang (2000) outbreaks. It is believed that displaced people from the neighbouring Faryab province introduced the P. falciparum to Qalai Nao of Badghis province, while merchants from Yakawlang district who used to travel to Baghlan and Saripul provinces are thought to have introduced the parasite to those remote malaria-free villages.
Overcrowding Yes Due to increased population density and increased exposure to mosquito bites in temporary shelters

Communicable Disease Profile for Afghanistan and Neighbouring Countries
WHO Communicable Disease WG on Emergencies/October 2001 28
Poor access to health services
Yes �� Delays in access to effective treatment increase the likelihood of severe disease and death
�� Delays in access to effective treatment also increase the pool of malaria gametocyte carriers (the mature sexual stage of the parasite in humans, that once picked up in the blood feed of a mosquito then develops into the infective stage for transmission to another human)
Food shortages Yes Malnutrition increases vulnerability to severe malaria once infected. Case management also becomes more complicated, resulting in increased mortality
Lack of safe water and poor sanitation
No However, temporary surface water bodies may increase malaria vector breeding opportunities
Others Yes �� Breakdown of control measures, and lack of preventive interventions such as insecticide treated materials (bed nets, sheeting etc.) and residual insecticide spraying of shelters
�� Sudden increase in vectorial capacity as a result of unusual weather. Many parts of the country were stricken by drought and witnessed prolonged periods of abnormally warm weather during the past two years. Unusual / unseasonal favourable meteorological conditions can increase vector capacity and subsequent malaria transmission
�� Epidemics are usually severe when rains follow unusual drought / famine periods
Risk assessment conclusions
The majority of malaria cases in Afghanistan will be caused by P. vivax, which is rarely life threatening. 10-20% of cases will be P. falciparum which can cause severe disease and death.
The peak malaria season is October / November in Afghanistan. There are estimated to be over 3 million displaced, many fleeing highland areas (with less or no malaria) and moving to, or through, areas where they are at risk of malaria transmission. This specific displaced group has low immunity to malaria and is at increased risk of severe disease if infected.
Long term drought across the country has resulted in increasing malnutrition. All malnourished are at increased risk of severe disease, particularly young children.
Those communities displaced to border regions of Pakistan and Tajikistan where malaria transmission is relatively higher are most at risk both during the remaining transmission period and from the start of the new transmission season in April/May.
Communicable Disease Profile for Afghanistan and Neighbouring Countries
WHO Communicable Disease WG on Emergencies/October 2001 29
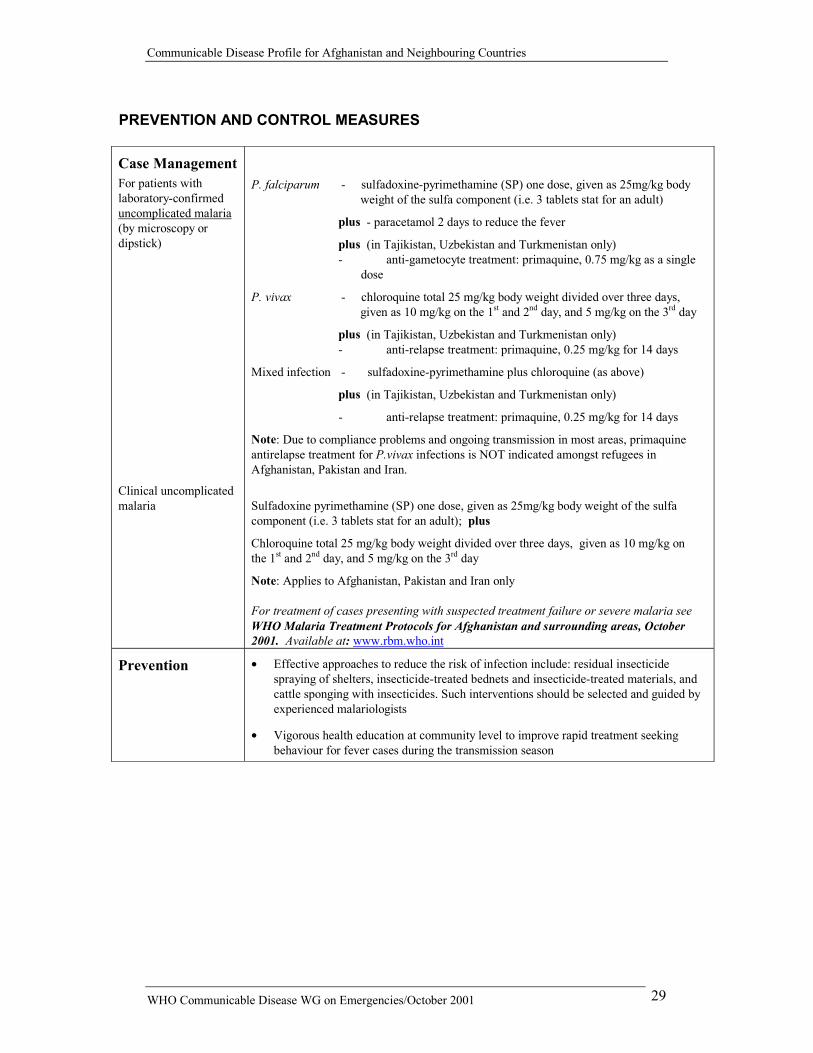
PREVENTION AND CONTROL MEASURES Case Management For patients with laboratory-confirmed uncomplicated malaria (by microscopy or dipstick)
Clinical uncomplicated malaria
P. falciparum - sulfadoxine-pyrimethamine (SP) one dose, given as 25mg/kg body weight of the sulfa component (i.e. 3 tablets stat for an adult)
plus - paracetamol 2 days to reduce the fever
plus (in Tajikistan, Uzbekistan and Turkmenistan only) - anti-gametocyte treatment: primaquine, 0.75 mg/kg as a single
dose
P. vivax - chloroquine total 25 mg/kg body weight divided over three days, given as 10 mg/kg on the 1st and 2nd day, and 5 mg/kg on the 3rd day
plus (in Tajikistan, Uzbekistan and Turkmenistan only) - anti-relapse treatment: primaquine, 0.25 mg/kg for 14 days
Mixed infection - sulfadoxine-pyrimethamine plus chloroquine (as above)
plus (in Tajikistan, Uzbekistan and Turkmenistan only)
- anti-relapse treatment: primaquine, 0.25 mg/kg for 14 days
Note: Due to compliance problems and ongoing transmission in most areas, primaquine antirelapse treatment for P.vivax infections is NOT indicated amongst refugees in Afghanistan, Pakistan and Iran.
Sulfadoxine pyrimethamine (SP) one dose, given as 25mg/kg body weight of the sulfa component (i.e. 3 tablets stat for an adult); plus
Chloroquine total 25 mg/kg body weight divided over three days, given as 10 mg/kg on the 1st and 2nd day, and 5 mg/kg on the 3rd day
Note: Applies to Afghanistan, Pakistan and Iran only
For treatment of cases presenting with suspected treatment failure or severe malaria see WHO Malaria Treatment Protocols for Afghanistan and surrounding areas, October 2001. Available at: www.rbm.who.int
Prevention �� Effective approaches to reduce the risk of infection include: residual insecticide spraying of shelters, insecticide-treated bednets and insecticide-treated materials, and cattle sponging with insecticides. Such interventions should be selected and guided by experienced malariologists
�� Vigorous health education at community level to improve rapid treatment seeking behaviour for fever cases during the transmission season
Communicable Disease Profile for Afghanistan and Neighbouring Countries
WHO Communicable Disease WG on Emergencies/October 2001 30
11. DENGUE DESCRIPTION
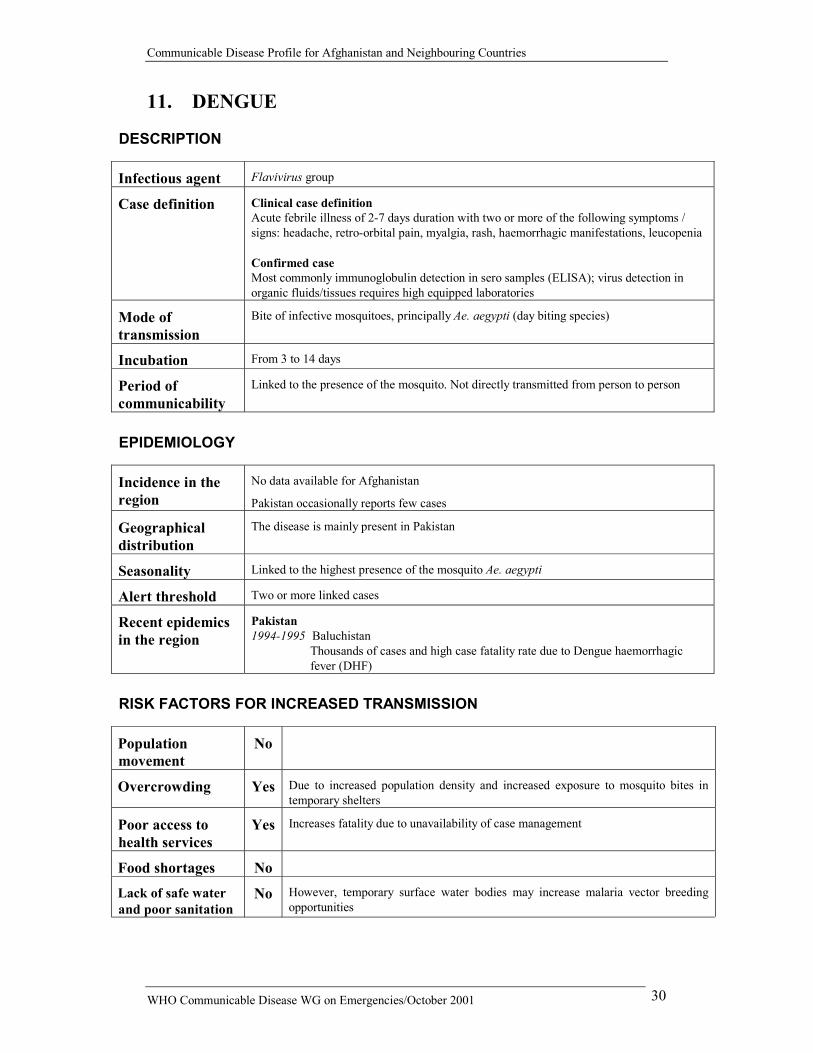
Infectious agent Flavivirus group
Case definition
Clinical case definition Acute febrile illness of 2-7 days duration with two or more of the following symptoms / signs: headache, retro-orbital pain, myalgia, rash, haemorrhagic manifestations, leucopenia Confirmed case Most commonly immunoglobulin detection in sero samples (ELISA); virus detection in organic fluids/tissues requires high equipped laboratories
Mode of transmission
Bite of infective mosquitoes, principally Ae. aegypti (day biting species)
Incubation From 3 to 14 days
Period of communicability
Linked to the presence of the mosquito. Not directly transmitted from person to person
EPIDEMIOLOGY
Incidence in the region
No data available for Afghanistan
Pakistan occasionally reports few cases
Geographical distribution
The disease is mainly present in Pakistan
Seasonality Linked to the highest presence of the mosquito Ae. aegypti
Alert threshold Two or more linked cases
Recent epidemics in the region
Pakistan 1994-1995 Baluchistan
Thousands of cases and high case fatality rate due to Dengue haemorrhagic fever (DHF)
RISK FACTORS FOR INCREASED TRANSMISSION
Population movement
No
Overcrowding Yes Due to increased population density and increased exposure to mosquito bites in temporary shelters
Poor access to health services
Yes Increases fatality due to unavailability of case management
Food shortages No
Lack of safe water and poor sanitation
No However, temporary surface water bodies may increase malaria vector breeding opportunities
Communicable Disease Profile for Afghanistan and Neighbouring Countries
WHO Communicable Disease WG on Emergencies/October 2001 31
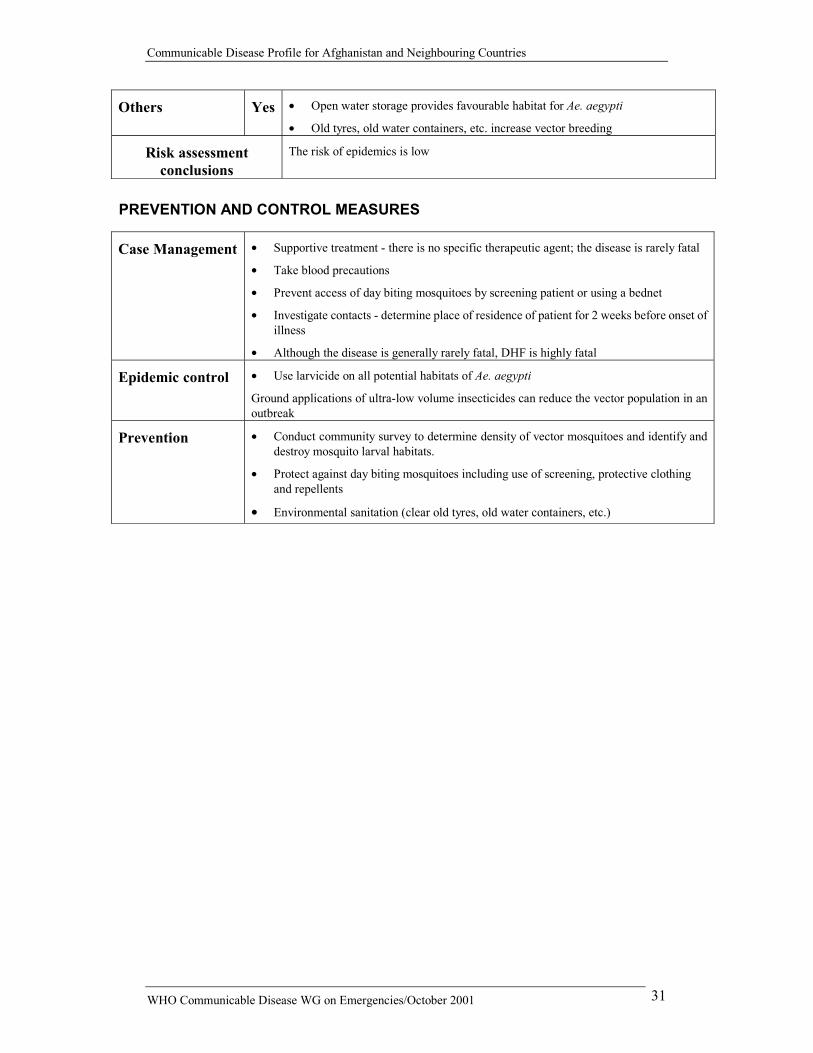
Others Yes �� Open water storage provides favourable habitat for Ae. aegypti
�� Old tyres, old water containers, etc. increase vector breeding
Risk assessment conclusions
The risk of epidemics is low
PREVENTION AND CONTROL MEASURES
Case Management �� Supportive treatment - there is no specific therapeutic agent; the disease is rarely fatal
�� Take blood precautions
�� Prevent access of day biting mosquitoes by screening patient or using a bednet
�� Investigate contacts - determine place of residence of patient for 2 weeks before onset of illness
�� Although the disease is generally rarely fatal, DHF is highly fatal
Epidemic control �� Use larvicide on all potential habitats of Ae. aegypti
Ground applications of ultra-low volume insecticides can reduce the vector population in an outbreak
Prevention �� Conduct community survey to determine density of vector mosquitoes and identify and destroy mosquito larval habitats.
�� Protect against day biting mosquitoes including use of screening, protective clothing and repellents
�� Environmental sanitation (clear old tyres, old water containers, etc.)
Communicable Disease Profile for Afghanistan and Neighbouring Countries
WHO Communicable Disease WG on Emergencies/October 2001 32
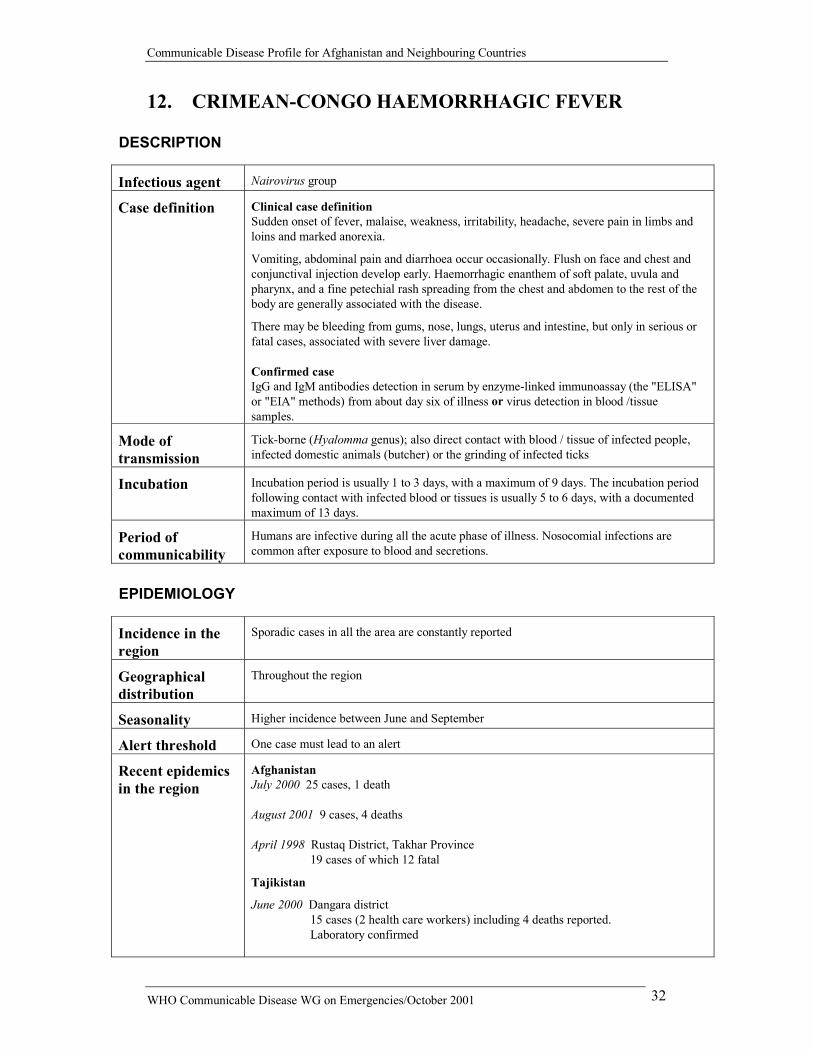
12. CRIMEAN-CONGO HAEMORRHAGIC FEVER DESCRIPTION
Infectious agent Nairovirus group
Case definition
Clinical case definition Sudden onset of fever, malaise, weakness, irritability, headache, severe pain in limbs and loins and marked anorexia.
Vomiting, abdominal pain and diarrhoea occur occasionally. Flush on face and chest and conjunctival injection develop early. Haemorrhagic enanthem of soft palate, uvula and pharynx, and a fine petechial rash spreading from the chest and abdomen to the rest of the body are generally associated with the disease.
There may be bleeding from gums, nose, lungs, uterus and intestine, but only in serious or fatal cases, associated with severe liver damage. Confirmed case IgG and IgM antibodies detection in serum by enzyme-linked immunoassay (the "ELISA" or "EIA" methods) from about day six of illness or virus detection in blood /tissue samples.
Mode of transmission
Tick-borne (Hyalomma genus); also direct contact with blood / tissue of infected people, infected domestic animals (butcher) or the grinding of infected ticks
Incubation Incubation period is usually 1 to 3 days, with a maximum of 9 days. The incubation period following contact with infected blood or tissues is usually 5 to 6 days, with a documented maximum of 13 days.
Period of communicability
Humans are infective during all the acute phase of illness. Nosocomial infections are common after exposure to blood and secretions.
EPIDEMIOLOGY
Incidence in the region
Sporadic cases in all the area are constantly reported
Geographical distribution
Throughout the region
Seasonality Higher incidence between June and September
Alert threshold One case must lead to an alert
Recent epidemics in the region
Afghanistan July 2000 25 cases, 1 death August 2001 9 cases, 4 deaths April 1998 Rustaq District, Takhar Province
19 cases of which 12 fatal
Tajikistan
June 2000 Dangara district 15 cases (2 health care workers) including 4 deaths reported. Laboratory confirmed
Communicable Disease Profile for Afghanistan and Neighbouring Countries
WHO Communicable Disease WG on Emergencies/October 2001 33
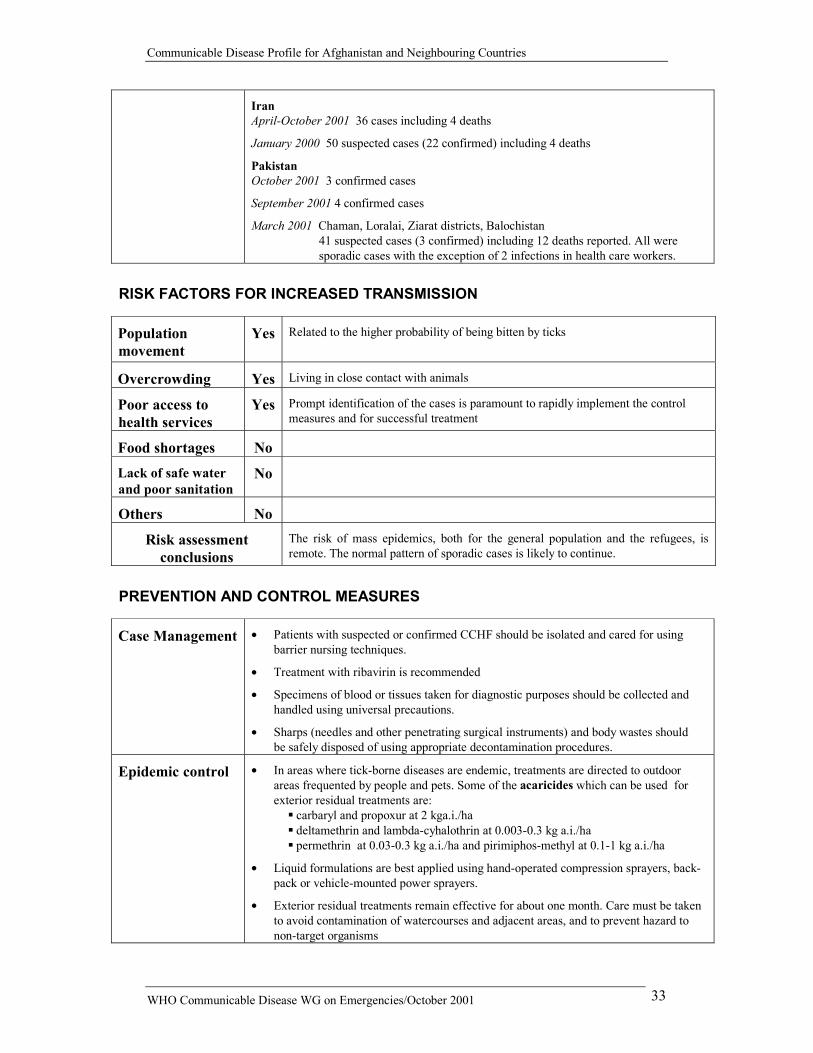
Iran April-October 2001 36 cases including 4 deaths
January 2000 50 suspected cases (22 confirmed) including 4 deaths
Pakistan October 2001 3 confirmed cases
September 2001 4 confirmed cases
March 2001 Chaman, Loralai, Ziarat districts, Balochistan 41 suspected cases (3 confirmed) including 12 deaths reported. All were sporadic cases with the exception of 2 infections in health care workers.
RISK FACTORS FOR INCREASED TRANSMISSION
Population movement
Yes Related to the higher probability of being bitten by ticks
Overcrowding Yes Living in close contact with animals
Poor access to health services
Yes Prompt identification of the cases is paramount to rapidly implement the control measures and for successful treatment
Food shortages No
Lack of safe water and poor sanitation
No
Others No
Risk assessment conclusions
The risk of mass epidemics, both for the general population and the refugees, is remote. The normal pattern of sporadic cases is likely to continue.
PREVENTION AND CONTROL MEASURES
Case Management �� Patients with suspected or confirmed CCHF should be isolated and cared for using barrier nursing techniques.
�� Treatment with ribavirin is recommended
�� Specimens of blood or tissues taken for diagnostic purposes should be collected and handled using universal precautions.
�� Sharps (needles and other penetrating surgical instruments) and body wastes should be safely disposed of using appropriate decontamination procedures.
Epidemic control �� In areas where tick-borne diseases are endemic, treatments are directed to outdoor areas frequented by people and pets. Some of the acaricides which can be used for exterior residual treatments are:
��carbaryl and propoxur at 2 kga.i./ha ��deltamethrin and lambda-cyhalothrin at 0.003-0.3 kg a.i./ha ��permethrin at 0.03-0.3 kg a.i./ha and pirimiphos-methyl at 0.1-1 kg a.i./ha
�� Liquid formulations are best applied using hand-operated compression sprayers, back-pack or vehicle-mounted power sprayers.
�� Exterior residual treatments remain effective for about one month. Care must be taken to avoid contamination of watercourses and adjacent areas, and to prevent hazard to non-target organisms
Communicable Disease Profile for Afghanistan and Neighbouring Countries
WHO Communicable Disease WG on Emergencies/October 2001 34
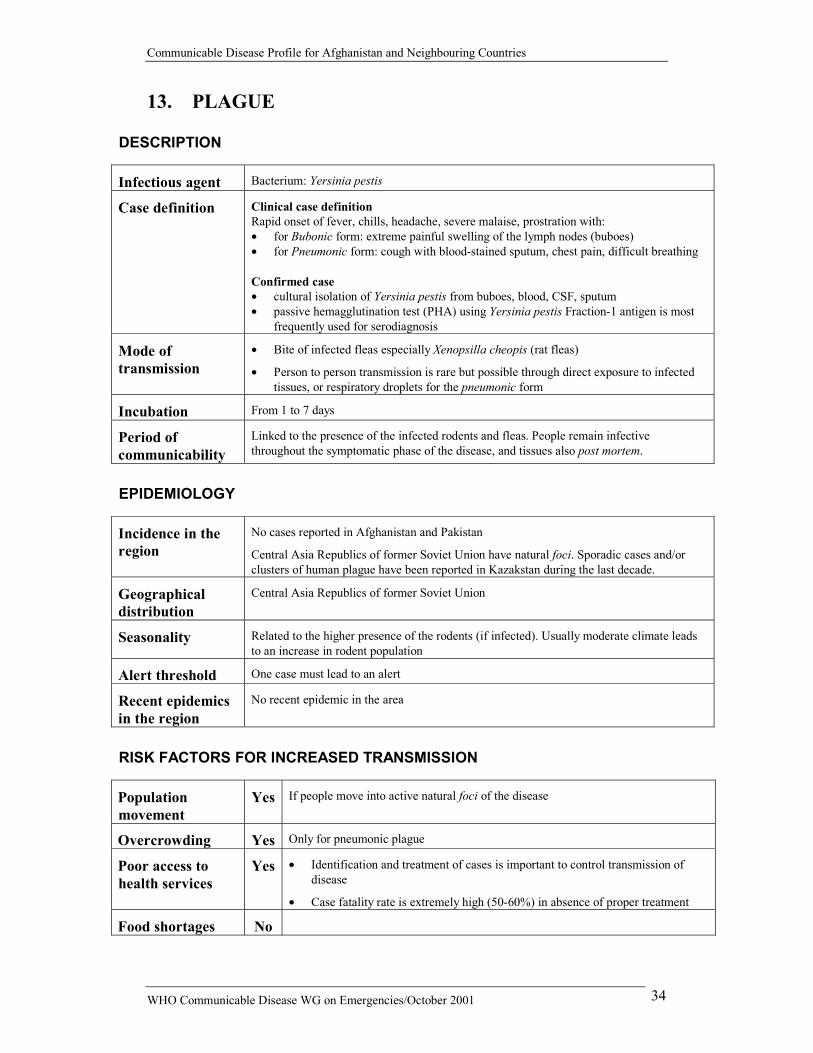
13. PLAGUE DESCRIPTION
Infectious agent Bacterium: Yersinia pestis
Case definition
Clinical case definition Rapid onset of fever, chills, headache, severe malaise, prostration with: �� for Bubonic form: extreme painful swelling of the lymph nodes (buboes) �� for Pneumonic form: cough with blood-stained sputum, chest pain, difficult breathing Confirmed case �� cultural isolation of Yersinia pestis from buboes, blood, CSF, sputum �� passive hemagglutination test (PHA) using Yersinia pestis Fraction-1 antigen is most
frequently used for serodiagnosis
Mode of transmission
�� Bite of infected fleas especially Xenopsilla cheopis (rat fleas)
�� Person to person transmission is rare but possible through direct exposure to infected tissues, or respiratory droplets for the pneumonic form
Incubation From 1 to 7 days
Period of communicability
Linked to the presence of the infected rodents and fleas. People remain infective throughout the symptomatic phase of the disease, and tissues also post mortem.
EPIDEMIOLOGY
Incidence in the region
No cases reported in Afghanistan and Pakistan
Central Asia Republics of former Soviet Union have natural foci. Sporadic cases and/or clusters of human plague have been reported in Kazakstan during the last decade.
Geographical distribution
Central Asia Republics of former Soviet Union
Seasonality Related to the higher presence of the rodents (if infected). Usually moderate climate leads to an increase in rodent population
Alert threshold One case must lead to an alert
Recent epidemics in the region
No recent epidemic in the area
RISK FACTORS FOR INCREASED TRANSMISSION
Population movement
Yes If people move into active natural foci of the disease
Overcrowding Yes Only for pneumonic plague
Poor access to health services
Yes �� Identification and treatment of cases is important to control transmission of disease
�� Case fatality rate is extremely high (50-60%) in absence of proper treatment
Food shortages No
Communicable Disease Profile for Afghanistan and Neighbouring Countries
WHO Communicable Disease WG on Emergencies/October 2001 35
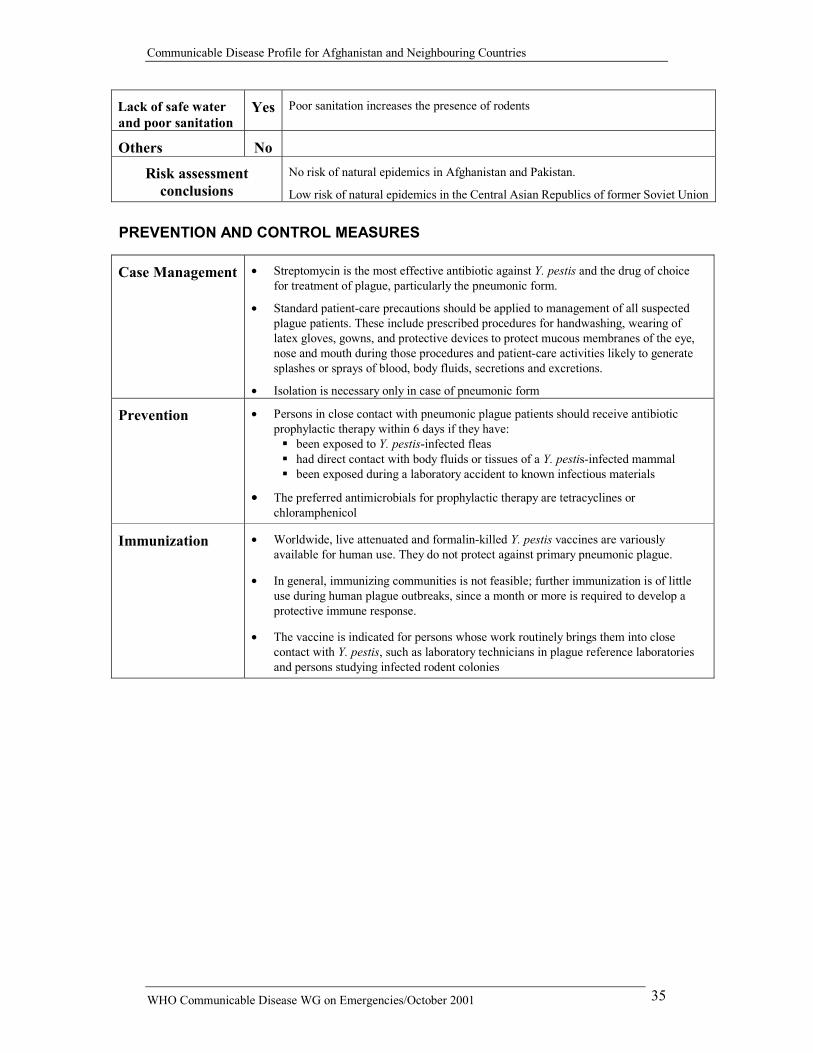
Lack of safe water and poor sanitation
Yes Poor sanitation increases the presence of rodents
Others No
Risk assessment conclusions
No risk of natural epidemics in Afghanistan and Pakistan.
Low risk of natural epidemics in the Central Asian Republics of former Soviet Union
PREVENTION AND CONTROL MEASURES
Case Management �� Streptomycin is the most effective antibiotic against Y. pestis and the drug of choice for treatment of plague, particularly the pneumonic form.
�� Standard patient-care precautions should be applied to management of all suspected plague patients. These include prescribed procedures for handwashing, wearing of latex gloves, gowns, and protective devices to protect mucous membranes of the eye, nose and mouth during those procedures and patient-care activities likely to generate splashes or sprays of blood, body fluids, secretions and excretions.
�� Isolation is necessary only in case of pneumonic form
Prevention �� Persons in close contact with pneumonic plague patients should receive antibiotic prophylactic therapy within 6 days if they have: ��been exposed to Y. pestis-infected fleas ��had direct contact with body fluids or tissues of a Y. pestis-infected mammal ��been exposed during a laboratory accident to known infectious materials
�� The preferred antimicrobials for prophylactic therapy are tetracyclines or chloramphenicol
Immunization �� Worldwide, live attenuated and formalin-killed Y. pestis vaccines are variously available for human use. They do not protect against primary pneumonic plague.
�� In general, immunizing communities is not feasible; further immunization is of little use during human plague outbreaks, since a month or more is required to develop a protective immune response.
�� The vaccine is indicated for persons whose work routinely brings them into close contact with Y. pestis, such as laboratory technicians in plague reference laboratories and persons studying infected rodent colonies
Communicable Disease Profile for Afghanistan and Neighbouring Countries
WHO Communicable Disease WG on Emergencies/October 2001 36
Zoonotic Diseases 14. RABIES
DESCRIPTION
Infectious agent Rhabdovirus, genus Lyssavirus
Case definition
Clinical case definition An acute neurological syndrome (encephalitis) dominated by forms of hyperactivity (furious rabies) or paralytic syndrome (dumb rabies) that progresses toward coma and death usually by respiratory failure within 7-10 days Confirmed case One or more of the following:
�� Detection of rabies viral antigens by direct fluorescent antibody (FA) in clinical specimens, preferably brain tissue (collected post mortem)
�� Detection by FA on skin or corneal smear (collected ante mortem)
�� FA positive after inoculation of brain tissue, saliva or CSF in cell culture, in mice or in suckling mice
�� Detectable rabies-neutralizing antibody titre in the CSF of an unvaccinated person
�� Identification of viral antigens by PCR on fixed tissue collected post mortem or in a clinical specimen (brain tissue or skin, cornea or saliva)
�� Isolation of rabies virus from clinical specimens and confirmation of rabies viral antigens by direct fluorescent antibody testing
Mode of transmission
Usually by the bite of an infected mammalian species (dog, cat, fox, etc.). No human to human transmission has been documented
Incubation Usually 3-8 weeks, occasionally shorter or longer
Period of communicability
The transmission is related to the bite of an infected animal
EPIDEMIOLOGY
Incidence in the region
Afghanistan No precise data, but on average 4 human cases are reported daily in Kabul
Iran Disease present
Pakistan Between 2000 and 5000 human deaths reported per year, over the past 5 years
Geographical distribution
The disease is present throughout the region
Seasonality No specific seasonality reported
Alert threshold One case in a susceptible animal species and /or human must lead to an alert
Communicable Disease Profile for Afghanistan and Neighbouring Countries
WHO Communicable Disease WG on Emergencies/October 2001 37
Recent epidemics in the region
Afghanistan June 1999 Kabul, Maidan Shahr
Total number of cases and deaths unknown
RISK FACTORS FOR INCREASED TRANSMISSION
Population movement
No
Overcrowding Yes An infected animal has the possibility to bite more people
Poor access to health services
Yes Prompt administration of vaccine post exposure (plus immunoglobulin if heavy exposure) is the only way to avoid death for an infected person
Food shortages No
Lack of safe water and poor sanitation
No
Others Yes �� Availability of food sources for the dogs and wild susceptible animals increases their number
�� Children of 5 to 15 years are the group at major risk
Risk assessment conclusions
Risk of epidemics for humans is significant if cases of rabies are reported in dogs or other susceptible animals in the same zone
PREVENTION AND CONTROL MEASURES
Case Management �� Immediate deep cleaning of the wound with a detergent and water. Then use a disinfectant. Wound should not be sutured, if possible. All exposure categories (I-III)
�� Prompt administration of a modern rabies vaccine (vero cell vaccine PVRV or the chick embryo cell vaccine PCECV). Exposure category II or III
�� Prompt administration of human rabies immunoglobulin, if category exposure III
�� Administration of tetanus vaccine
�� If a person develops the disease death is inevitable. Universal nursing barrier practices are necessary for the sick people.
Epidemic control �� Immediate notification if one or more suspected cases are identified
�� Confirm the outbreak, following WHO guidelines
�� Confirm diagnosis and insure prompt management
Prevention �� Identify and kill all the suspected infected animals in rabies foci
�� Identify and treat all those who have (or may have) been exposed
Immunization �� Human preventive mass vaccination is generally not recommended but can be considered under certain circumstances for the age group 5 to 15 years
Communicable Disease Profile for Afghanistan and Neighbouring Countries
WHO Communicable Disease WG on Emergencies/October 2001 38
15. ANTHRAX DESCRIPTION
Infectious agent Bacterium: Bacillus anthracis
Case definition
Clinical case definition An illness with acute onset characterized by several clinical forms:
(a) Localized form: �� Cutaneous: skin lesion evolving over 1 to 6 days from a papular through a
vesicular stage, to a depressed black eschar invariably accompanied by oedema that may be mild to extensive
(b) Systemic forms: �� Gastro-intestinal: abdominal distress characterized by nausea, vomiting, anorexia
and followed by fever �� Pulmonary (inhalation): brief prodrome resembling acute viral respiratory illness,
followed by rapid onset of hypoxia, dyspnoea and high temperature, with X-ray evidence of mediastinal widening
�� Meningeal: acute onset of high fever possibly with convulsions, loss of consciousness, meningeal signs and symptoms; commonly noted in all systemic infections
Confirmed case
�� Isolation of B anthracis from a clinical specimen (e.g., blood, lesions, discharges)
�� Demonstration of B. anthracis in a clinical specimen by microscopic examination of stained smears (vesicular fluid, blood, cerebrospinal fluid, pleural fluid, stools)
�� Positive serology (ELISA, Western blot, toxin detection, chromatographic assay, fluorescent antibody test (FAT)
Mode of transmission
�� Cutaneous infection is by contact with tissues of infected animals (cattle, sheep, goats, etc.) often during slaughter procedures or by contact with infected or contaminated animal products (e.g. hides).
�� Intestinal and oropharingeal anthrax arises from ingestion of contaminated undercooked meat
�� Pulmonary inhalation is an occupational diseases of people working with contaminated wool and hides
Incubation From 1 to 7 days, even if up to 60 days is possible
Period of communicability
Related to the presence of infected animals. Direct transmission from person to person is not recorded. Hides and soil contaminated by spores may remain infectious for decades
EPIDEMIOLOGY
Incidence in the region
Sporadic cases and outbreaks are reported
Geographical distribution
The disease is present throughout the region
Seasonality Highest incidence in the spring/summer
Alert threshold One human case must lead to an alert
Any animal outbreak must be followed up by the veterinary and health authorities
Communicable Disease Profile for Afghanistan and Neighbouring Countries
WHO Communicable Disease WG on Emergencies/October 2001 39
Recent epidemics in the region
Tajikistan July 2000 Khatlon Region
17 suspected cases. No deaths reported. Suspected source: infected cows
RISK FACTORS FOR INCREASED TRANSMISSION
Population movement
No
Overcrowding No
Poor access to health services
Yes Poor of veterinary services and lack of animal vaccination
Food shortages Yes Consumption of animals who died due to illness
Lack of safe water and poor sanitation
No
Others Yes �� Slaughter of dead animals
�� Lack of disinfection of contaminated areas
Risk assessment conclusions
If not present in animals, very low risk of epidemics in human
PREVENTION AND CONTROL MEASURES
Case Management �� Prompt antibiotic therapy with penicillin usually results in dramatic recovery of the individual or animal infected with anthrax
Epidemic control �� Following the first detection of anthrax in a herd, the remaining animals should be removed immediately from the field and checked regularly for signs of illness
Prevention �� Prevention of anthrax in both humans and animals is based on control measures in livestock in endemic areas such as the safe disposal of anthrax carcasses and vaccination of at risk herds/areas
�� The most efficient method of disposal is incineration in a manner that ensures heat sterilization of the underlying soil
Immunization �� There is a vaccine against anthrax, but it is not approved for widespread use
�� The vaccine is sometimes given to people who are likely to be exposed to anthrax through their occupation, for example, tannery workers, or to military personnel
�� It is not recommended for mass immunization
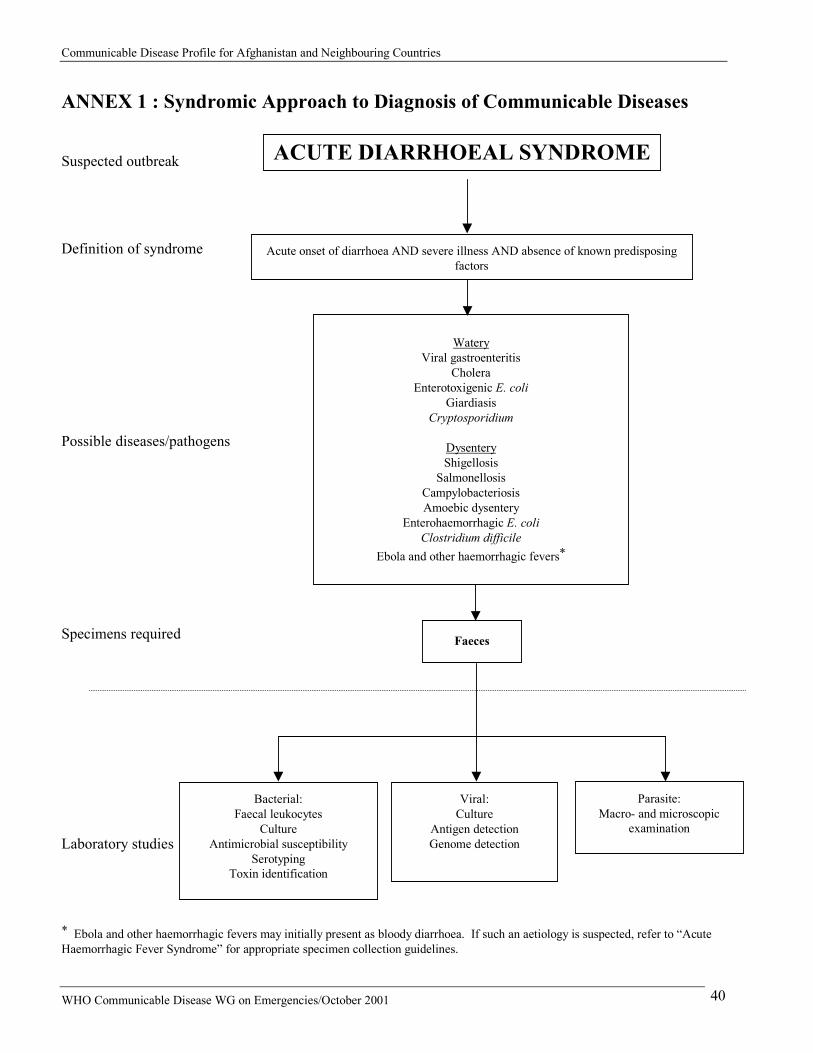
Communicable Disease Profile for Afghanistan and Neighbouring Countries
WHO Communicable Disease WG on Emergencies/October 2001 40
ANNEX 1 : Syndromic Approach to Diagnosis of Communicable Diseases Suspected outbreak Definition of syndrome Possible diseases/pathogens Specimens required Laboratory studies * Ebola and other haemorrhagic fevers may initially present as bloody diarrhoea. If such an aetiology is suspected, refer to “Acute Haemorrhagic Fever Syndrome” for appropriate specimen collection guidelines.
ACUTE DIARRHOEAL SYNDROME
Acute onset of diarrhoea AND severe illness AND absence of known predisposing factors
Faeces
Watery
Viral gastroenteritis Cholera
Enterotoxigenic E. coli Giardiasis
Cryptosporidium
Dysentery Shigellosis
Salmonellosis Campylobacteriosis Amoebic dysentery
Enterohaemorrhagic E. coli Clostridium difficile
Ebola and other haemorrhagic fevers*
Bacterial: Faecal leukocytes
Culture Antimicrobial susceptibility
Serotyping Toxin identification
Viral: Culture
Antigen detection Genome detection
Parasite: Macro- and microscopic
examination
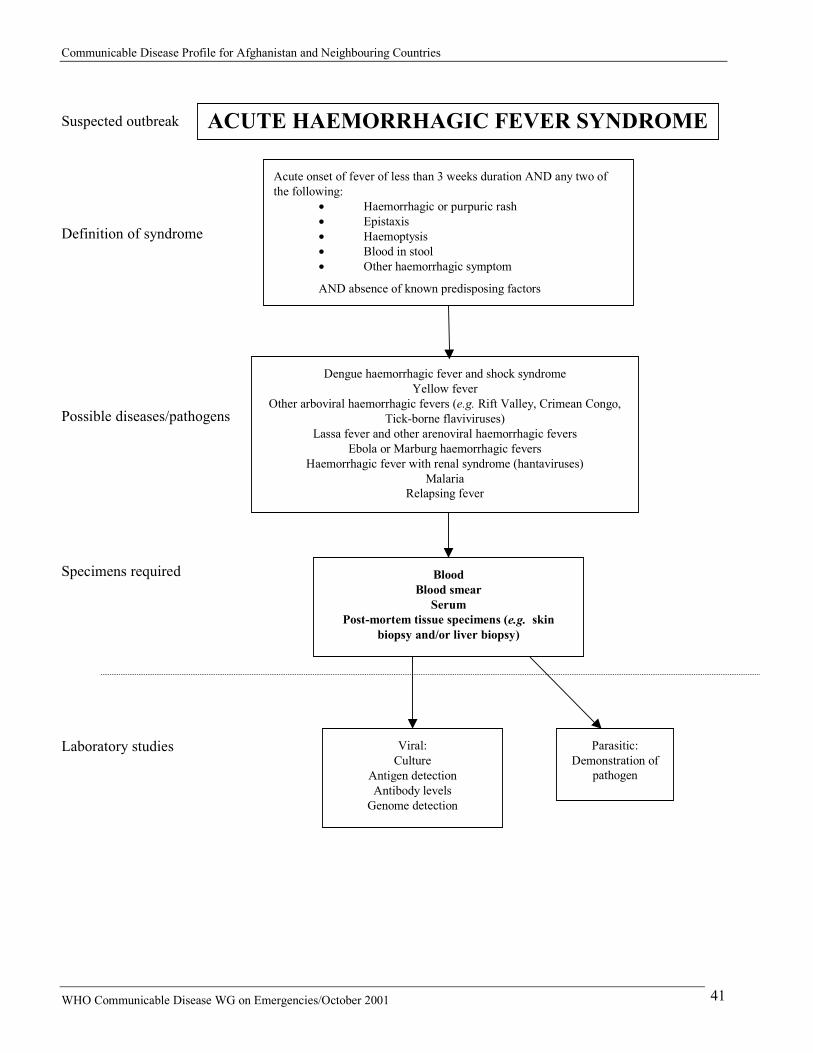
Communicable Disease Profile for Afghanistan and Neighbouring Countries
WHO Communicable Disease WG on Emergencies/October 2001 41
Suspected outbreak Definition of syndrome
Possible diseases/pathogens
Specimens required Laboratory studies
ACUTE HAEMORRHAGIC FEVER SYNDROME
Acute onset of fever of less than 3 weeks duration AND any two of the following:
�� Haemorrhagic or purpuric rash �� Epistaxis �� Haemoptysis �� Blood in stool �� Other haemorrhagic symptom
AND absence of known predisposing factors
Dengue haemorrhagic fever and shock syndrome Yellow fever
Other arboviral haemorrhagic fevers (e.g. Rift Valley, Crimean Congo, Tick-borne flaviviruses)
Lassa fever and other arenoviral haemorrhagic fevers Ebola or Marburg haemorrhagic fevers
Haemorrhagic fever with renal syndrome (hantaviruses) Malaria
Relapsing fever
Blood Blood smear
Serum Post-mortem tissue specimens (e.g. skin
biopsy and/or liver biopsy)
Viral: Culture
Antigen detection Antibody levels
Genome detection
Parasitic: Demonstration of
pathogen
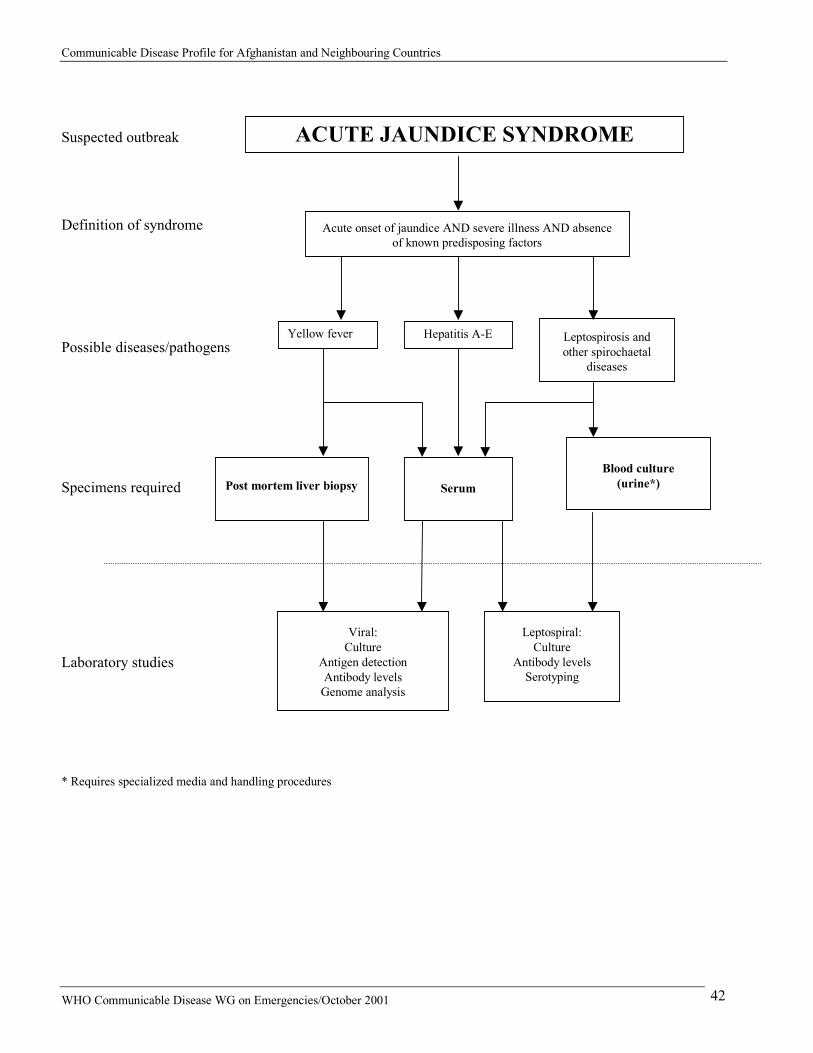
Communicable Disease Profile for Afghanistan and Neighbouring Countries
WHO Communicable Disease WG on Emergencies/October 2001 42
Suspected outbreak Definition of syndrome Possible diseases/pathogens Specimens required Laboratory studies * Requires specialized media and handling procedures
Acute onset of jaundice AND severe illness AND absence of known predisposing factors
Hepatitis A-E Leptospirosis and other spirochaetal
diseases
Blood culture
(urine*)
Serum
Leptospiral: Culture
Antibody levels Serotyping
Viral: Culture
Antigen detection Antibody levels
Genome analysis
Post mortem liver biopsy
Yellow fever
ACUTE JAUNDICE SYNDROME
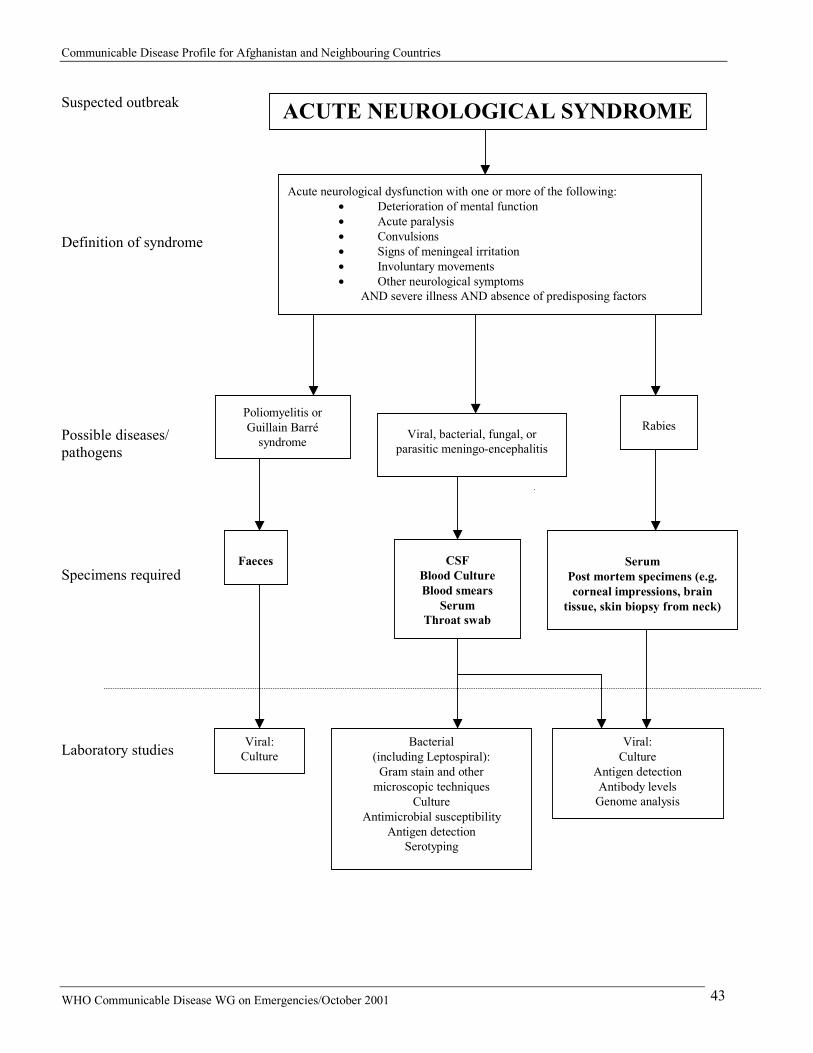
Communicable Disease Profile for Afghanistan and Neighbouring Countries
WHO Communicable Disease WG on Emergencies/October 2001 43
Suspected outbreak Definition of syndrome Possible diseases/ pathogens Specimens required Laboratory studies
ACUTE NEUROLOGICAL SYNDROME
Acute neurological dysfunction with one or more of the following: �� Deterioration of mental function �� Acute paralysis �� Convulsions �� Signs of meningeal irritation �� Involuntary movements �� Other neurological symptoms
AND severe illness AND absence of predisposing factors
Poliomyelitis or Guillain Barré
syndrome Viral, bacterial, fungal, or parasitic meningo-encephalitis
Rabies
Faeces CSF
Blood Culture Blood smears
Serum Throat swab
Serum
Post mortem specimens (e.g. corneal impressions, brain
tissue, skin biopsy from neck)
Viral: Culture
Bacterial (including Leptospiral):
Gram stain and other microscopic techniques
Culture Antimicrobial susceptibility
Antigen detection Serotyping
Viral: Culture
Antigen detection Antibody levels
Genome analysis
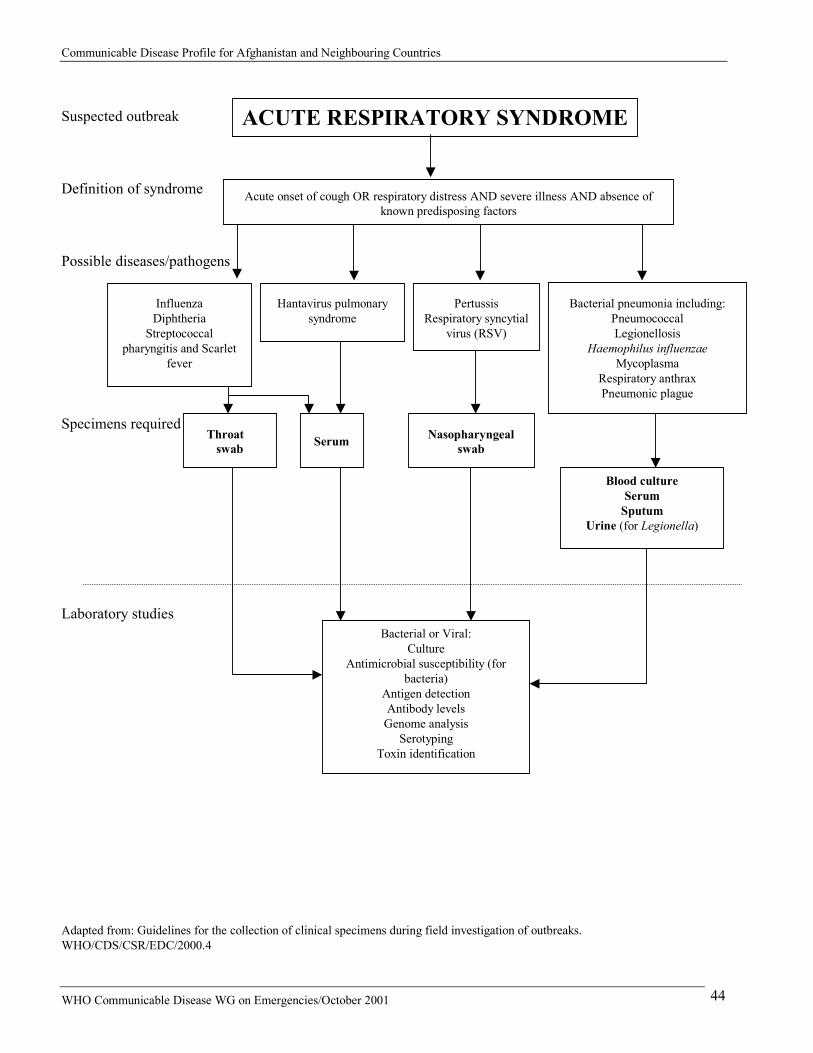
Communicable Disease Profile for Afghanistan and Neighbouring Countries
WHO Communicable Disease WG on Emergencies/October 2001 44
Suspected outbreak
Definition of syndrome
Possible diseases/pathogens
Specimens required Laboratory studies
Adapted from: Guidelines for the collection of clinical specimens during field investigation of outbreaks. WHO/CDS/CSR/EDC/2000.4
ACUTE RESPIRATORY SYNDROME
Acute onset of cough OR respiratory distress AND severe illness AND absence of known predisposing factors
Influenza Diphtheria
Streptococcal pharyngitis and Scarlet
fever
Bacterial pneumonia including: Pneumococcal Legionellosis
Haemophilus influenzae Mycoplasma
Respiratory anthrax Pneumonic plague
Throat swab
Nasopharyngeal swab
Blood culture Serum
Sputum Urine (for Legionella)
Bacterial or Viral: Culture
Antimicrobial susceptibility (for bacteria)
Antigen detection Antibody levels
Genome analysis Serotyping
Toxin identification
Hantavirus pulmonary syndrome
Pertussis Respiratory syncytial
virus (RSV)
Serum
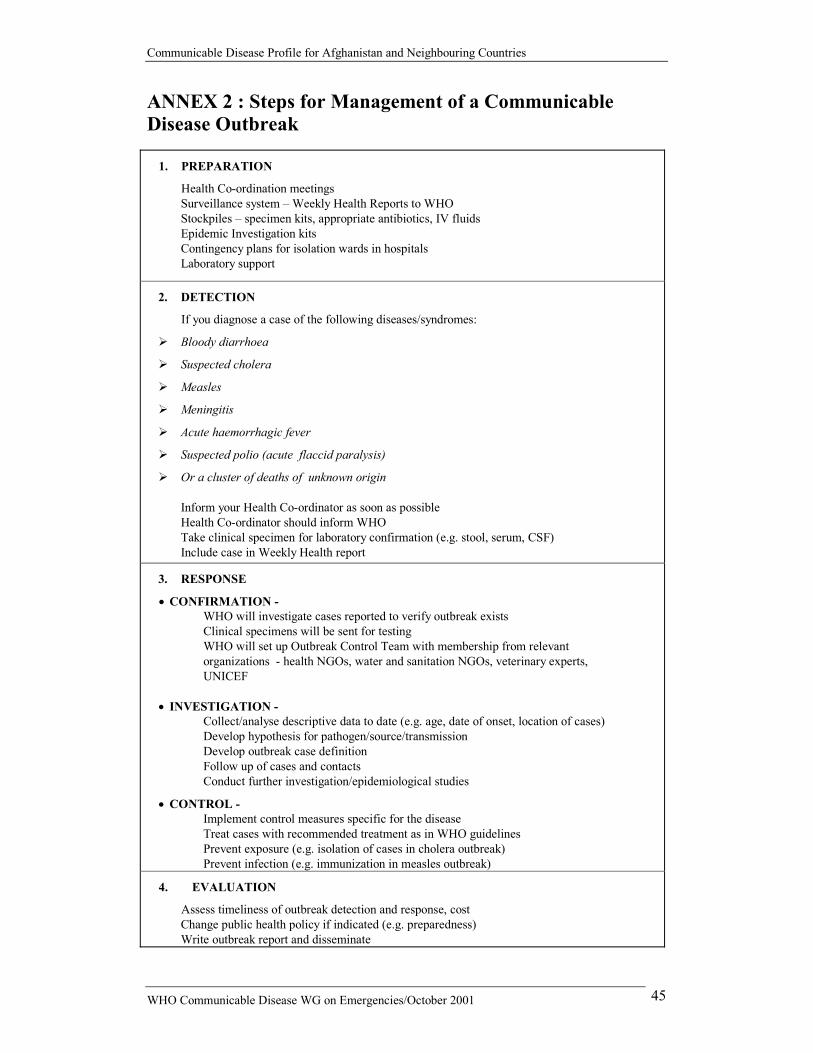
Communicable Disease Profile for Afghanistan and Neighbouring Countries
WHO Communicable Disease WG on Emergencies/October 2001 45
ANNEX 2 : Steps for Management of a Communicable Disease Outbreak
1. PREPARATION
Health Co-ordination meetings Surveillance system – Weekly Health Reports to WHO Stockpiles – specimen kits, appropriate antibiotics, IV fluids Epidemic Investigation kits Contingency plans for isolation wards in hospitals Laboratory support
2. DETECTION
If you diagnose a case of the following diseases/syndromes:
��Bloody diarrhoea
��Suspected cholera
��Measles
��Meningitis
��Acute haemorrhagic fever
��Suspected polio (acute flaccid paralysis)
��Or a cluster of deaths of unknown origin Inform your Health Co-ordinator as soon as possible Health Co-ordinator should inform WHO Take clinical specimen for laboratory confirmation (e.g. stool, serum, CSF) Include case in Weekly Health report
3. RESPONSE
��CONFIRMATION - WHO will investigate cases reported to verify outbreak exists Clinical specimens will be sent for testing WHO will set up Outbreak Control Team with membership from relevant organizations - health NGOs, water and sanitation NGOs, veterinary experts, UNICEF
�� INVESTIGATION -
Collect/analyse descriptive data to date (e.g. age, date of onset, location of cases) Develop hypothesis for pathogen/source/transmission Develop outbreak case definition Follow up of cases and contacts Conduct further investigation/epidemiological studies
�� CONTROL - Implement control measures specific for the disease Treat cases with recommended treatment as in WHO guidelines Prevent exposure (e.g. isolation of cases in cholera outbreak) Prevent infection (e.g. immunization in measles outbreak)
4. EVALUATION
Assess timeliness of outbreak detection and response, cost Change public health policy if indicated (e.g. preparedness) Write outbreak report and disseminate

Communicable Disease Profile for Afghanistan and Neighbouring Countries
WHO Communicable Disease WG on Emergencies/October 2001 46
ANNEX 3 : Safe Water and Sanitation The following are effective methods to obtain safe drinking water: Boiling To make water safe for drinking and hygiene purposes, bring water to a vigorous, rolling boil and keep it boiling for 1 minute. This will kill, or inactivate, most of the organisms that cause diarrhoea. Household filtration Household filtration should considerably reduce the pathogens in the water. It should be followed by disinfection through chlorination or boiling. Disinfection through chlorination The following guidelines should be translated into messages that take into account locally available products and measuring devices. To make water safe by chlorination, the first step is to make a stock solution of chlorine. This can be prepared by adding the following products to one litre of water:
Product (% concentration by weight of available chlorine) Amount for 1 litre Calcium hypochlorite (70 %); or 15g Bleaching powder or chlorinated lime (30%); or 33g Sodium hypochlorite (5%); or 250 ml Sodium hypochlorite (10 %); or 110 ml
The stock solution must be stored in a closed container, in a cool dark place and used within one month. It should be used to prepare safe water as follows:
Stock solution Added volume of Water 0.6 ml or 3 drops 1litre 6 ml 10 litres 60 ml 100 litres
Mix by stirring and allow the chlorinated water to stand for at least 30 minutes before using it. The free residual chlorine level after 30 minutes should be between 0.1 to 0.5 mg/litre. If the free residual chlorine is not within this range the number of drops of the stock solution should be adjusted so the final product falls within this range. If the water is cloudy or turbid it must either be filtered before chlorination or boiled vigorously rather than chlorinated. Chlorination of turbid water might not make it safe. See guidelines for cholera control, WHO 1993 and Fact Sheets on Environmental Sanitation for Cholera Control, WHO 1996
Sanitation Good sanitation can markedly reduce the risk of transmission of intestinal pathogens, especially where its absence may lead to contamination of clean water sources. High priority should be given to observing the basic principles of sanitary human waste disposal, as well as to ensuring the availability of safe water supplies. Appropriate facilities for human waste disposal are a basic need of all communities; in the absence of such facilities there is a high risk of water-related diseases. Sanitary systems that are appropriate for the local conditions should be constructed with the co-operation of the community.
Communicable Disease Profile for Afghanistan and Neighbouring Countries
WHO Communicable Disease WG on Emergencies/October 2001 47
People will need to taught how to use latrines, about the dangers of defecating on the ground, or in or near waters, and about the importance of thorough hand-washing with soap or ash after any contact with excreta. The disposal of children's excreta in latrines needs to be emphasized. See Fact Sheets on Environmental Sanitation for Cholera Control, WHO 1996 and A Guide to the Development of On-site Sanitation, WHO 1992
Communicable Disease Profile for Afghanistan and Neighbouring Countries
WHO Communicable Disease WG on Emergencies/October 2001 48
ANNEX 4 : Injection Safety Preliminary analysis of data collected as part of the Comparative Risk Assessment component of the Global Burden of Disease study suggests that the Region which includes Afghanistan, Iran and Pakistan faces a major challenge in terms of unsafe injection practices and transmission of blood-borne pathogens through injections. In this region, the estimated proportion of re-use of injection equipment in the absence of sterilization is 69%. Prevalence in the region of Hepatitis B is 4.3%, of Hepatitis C is 5.5%, and of HIV is 0.03%. The proportion of new infections with Hepatitis B, Hepatitis C, and HIV that are attributable to unsafe injections practices are 59%, 81% and 4% respectively. Thus, in any relief efforts to assist the population and the refugees in this region of the world, safe and appropriate use of injections should be ensured through:
�� Education of the population and of the healthcare workers regarding the need to observe the “one syringe / needle set - one injection” rule;
�� Provision of sufficient quantities of new disposable injection equipment and sharps waste collection boxes IN QUANTITIES THAT MATCH ANY PLANNED DELIVERIES OF INJECTABLES DRUGS OR VACCINES; and
�� Sharps waste management through open-air incineration of full sharps boxes
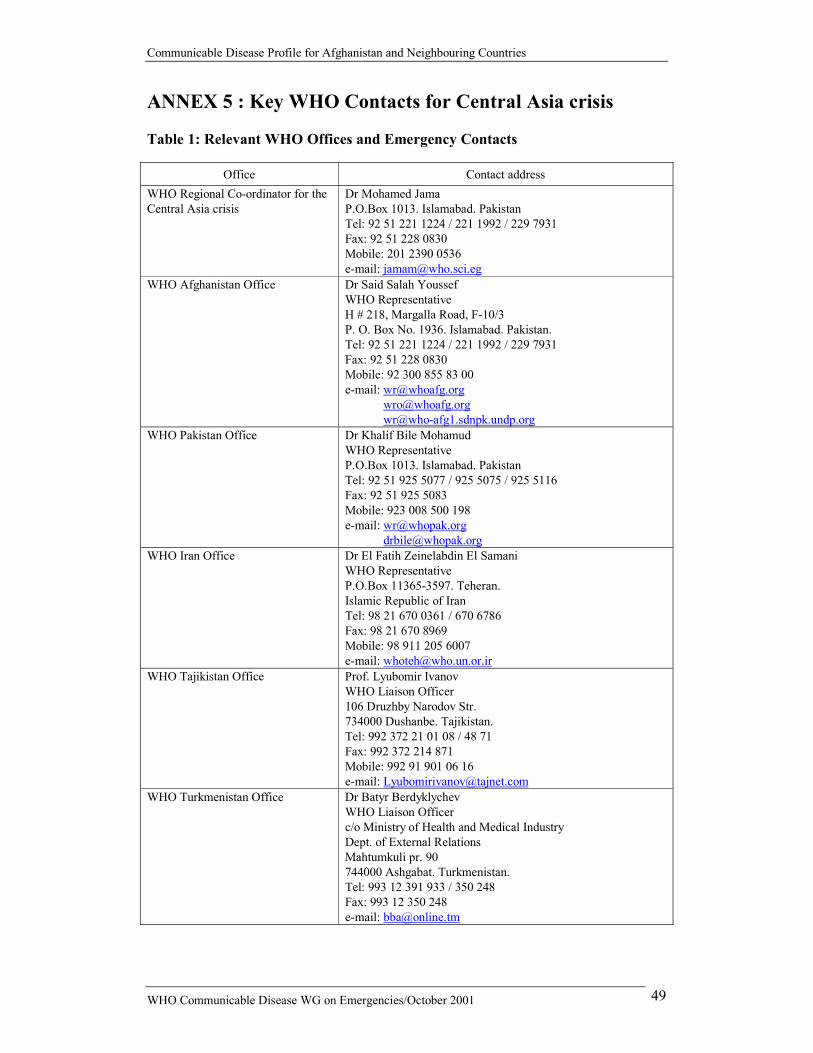
Communicable Disease Profile for Afghanistan and Neighbouring Countries
WHO Communicable Disease WG on Emergencies/October 2001 49
ANNEX 5 : Key WHO Contacts for Central Asia crisis
Table 1: Relevant WHO Offices and Emergency Contacts
Office Contact address WHO Regional Co-ordinator for the Central Asia crisis
Dr Mohamed Jama P.O.Box 1013. Islamabad. Pakistan Tel: 92 51 221 1224 / 221 1992 / 229 7931 Fax: 92 51 228 0830 Mobile: 201 2390 0536 e-mail: [email protected]
WHO Afghanistan Office Dr Said Salah Youssef WHO Representative H # 218, Margalla Road, F-10/3 P. O. Box No. 1936. Islamabad. Pakistan. Tel: 92 51 221 1224 / 221 1992 / 229 7931 Fax: 92 51 228 0830 Mobile: 92 300 855 83 00 e-mail: [email protected]
[email protected] [email protected]
WHO Pakistan Office Dr Khalif Bile Mohamud WHO Representative P.O.Box 1013. Islamabad. Pakistan Tel: 92 51 925 5077 / 925 5075 / 925 5116 Fax: 92 51 925 5083 Mobile: 923 008 500 198 e-mail: [email protected]
[email protected] WHO Iran Office Dr El Fatih Zeinelabdin El Samani
WHO Representative P.O.Box 11365-3597. Teheran. Islamic Republic of Iran Tel: 98 21 670 0361 / 670 6786 Fax: 98 21 670 8969 Mobile: 98 911 205 6007 e-mail: [email protected]
WHO Tajikistan Office Prof. Lyubomir Ivanov WHO Liaison Officer 106 Druzhby Narodov Str. 734000 Dushanbe. Tajikistan. Tel: 992 372 21 01 08 / 48 71 Fax: 992 372 214 871 Mobile: 992 91 901 06 16 e-mail: [email protected]
WHO Turkmenistan Office Dr Batyr Berdyklychev WHO Liaison Officer c/o Ministry of Health and Medical Industry Dept. of External Relations Mahtumkuli pr. 90 744000 Ashgabat. Turkmenistan. Tel: 993 12 391 933 / 350 248 Fax: 993 12 350 248 e-mail: [email protected]

Communicable Disease Profile for Afghanistan and Neighbouring Countries
WHO Communicable Disease WG on Emergencies/October 2001 50
WHO Uzbekistan Office Dr Jukka Pukkila WHO Liaison Officer c/o Ministry of Health Navoi Str. 12 700011 Tashkent. Uzbekistan. Tel: 998 71 241 5343 / 144 7534 Mobile: 998 71 131 92 40 / 131 75 35 / 130 37 93 Fax: 998 711 441 040 e-mail: [email protected]
[email protected] WHO Eastern Mediterranean Regional Office
Dr Altaf Musani WHO/EMRO P.O.Box 7608, Cairo 11371. Egypt Tel: 202 276 5027 / 276 5025 Mobile: 201 2390 0536 / 0537 Fax: 202 276 5428 e-mail: [email protected]
[email protected] WHO European Regional Office Dr Jan Theunissen / Dr Vladimir Verbitski
WHO/EURO 8, Scherfigsvej, DK-2100 Copenhagen 0. Denmark Tel: 4539 17 15 51 / 17 17 17 Mobile: 4521 20 47 20 / 4526 46 58 46 Fax: 4539 17 18 18 e-mail: [email protected]
[email protected] WHO Headquarters Dr Khalid Shibib
Duty Officer Avenue Appia 20 1211 Geneva 27. Switzerland Tel: 4122 791 2756 Mobile: 4179 475 5548 Fax: 4122 791 4844 e-mail: [email protected]
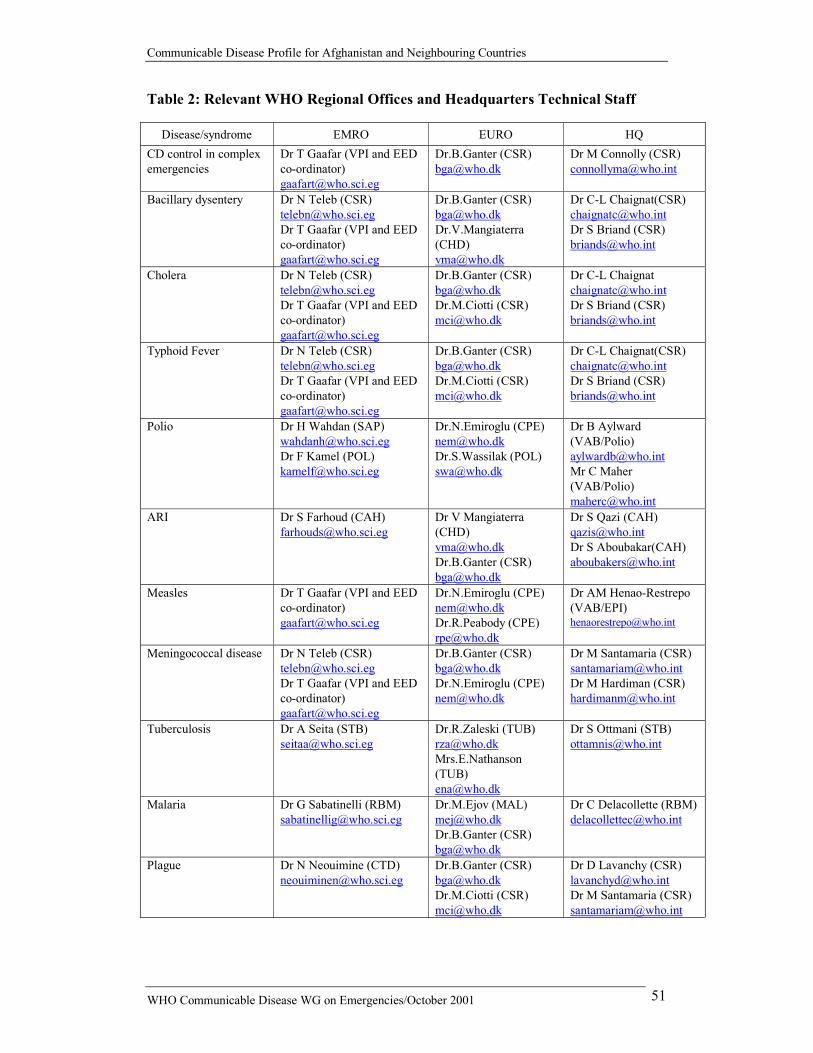
Communicable Disease Profile for Afghanistan and Neighbouring Countries
WHO Communicable Disease WG on Emergencies/October 2001 51
Table 2: Relevant WHO Regional Offices and Headquarters Technical Staff
Disease/syndrome EMRO EURO HQ CD control in complex emergencies
Dr T Gaafar (VPI and EED co-ordinator) [email protected]
Dr.B.Ganter (CSR) [email protected]
Dr M Connolly (CSR) [email protected]
Bacillary dysentery Dr N Teleb (CSR) [email protected] Dr T Gaafar (VPI and EED co-ordinator) [email protected]
Dr.B.Ganter (CSR) [email protected] Dr.V.Mangiaterra (CHD) [email protected]
Dr C-L Chaignat(CSR) [email protected] Dr S Briand (CSR) [email protected]
Cholera Dr N Teleb (CSR) [email protected] Dr T Gaafar (VPI and EED co-ordinator) [email protected]
Dr.B.Ganter (CSR) [email protected] Dr.M.Ciotti (CSR) [email protected]
Dr C-L Chaignat [email protected] Dr S Briand (CSR) [email protected]
Typhoid Fever Dr N Teleb (CSR) [email protected] Dr T Gaafar (VPI and EED co-ordinator) [email protected]
Dr.B.Ganter (CSR) [email protected] Dr.M.Ciotti (CSR) [email protected]
Dr C-L Chaignat(CSR) [email protected] Dr S Briand (CSR) [email protected]
Polio Dr H Wahdan (SAP) [email protected] Dr F Kamel (POL) [email protected]
Dr.N.Emiroglu (CPE) [email protected] Dr.S.Wassilak (POL) [email protected]
Dr B Aylward (VAB/Polio) [email protected] Mr C Maher (VAB/Polio) [email protected]
ARI Dr S Farhoud (CAH) [email protected]
Dr V Mangiaterra (CHD) [email protected] Dr.B.Ganter (CSR) [email protected]
Dr S Qazi (CAH) [email protected] Dr S Aboubakar(CAH) [email protected]
Measles Dr T Gaafar (VPI and EED co-ordinator) [email protected]
Dr.N.Emiroglu (CPE) [email protected] Dr.R.Peabody (CPE) [email protected]
Dr AM Henao-Restrepo (VAB/EPI) [email protected]
Meningococcal disease Dr N Teleb (CSR) [email protected] Dr T Gaafar (VPI and EED co-ordinator) [email protected]
Dr.B.Ganter (CSR) [email protected] Dr.N.Emiroglu (CPE) [email protected]
Dr M Santamaria (CSR) [email protected] Dr M Hardiman (CSR) [email protected]
Tuberculosis Dr A Seita (STB) [email protected]
Dr.R.Zaleski (TUB) [email protected] Mrs.E.Nathanson (TUB) [email protected]
Dr S Ottmani (STB) [email protected]
Malaria Dr G Sabatinelli (RBM) [email protected]
Dr.M.Ejov (MAL) [email protected] Dr.B.Ganter (CSR) [email protected]
Dr C Delacollette (RBM) [email protected]
Plague Dr N Neouimine (CTD) [email protected]
Dr.B.Ganter (CSR) [email protected] Dr.M.Ciotti (CSR) [email protected]
Dr D Lavanchy (CSR) [email protected] Dr M Santamaria (CSR) [email protected]
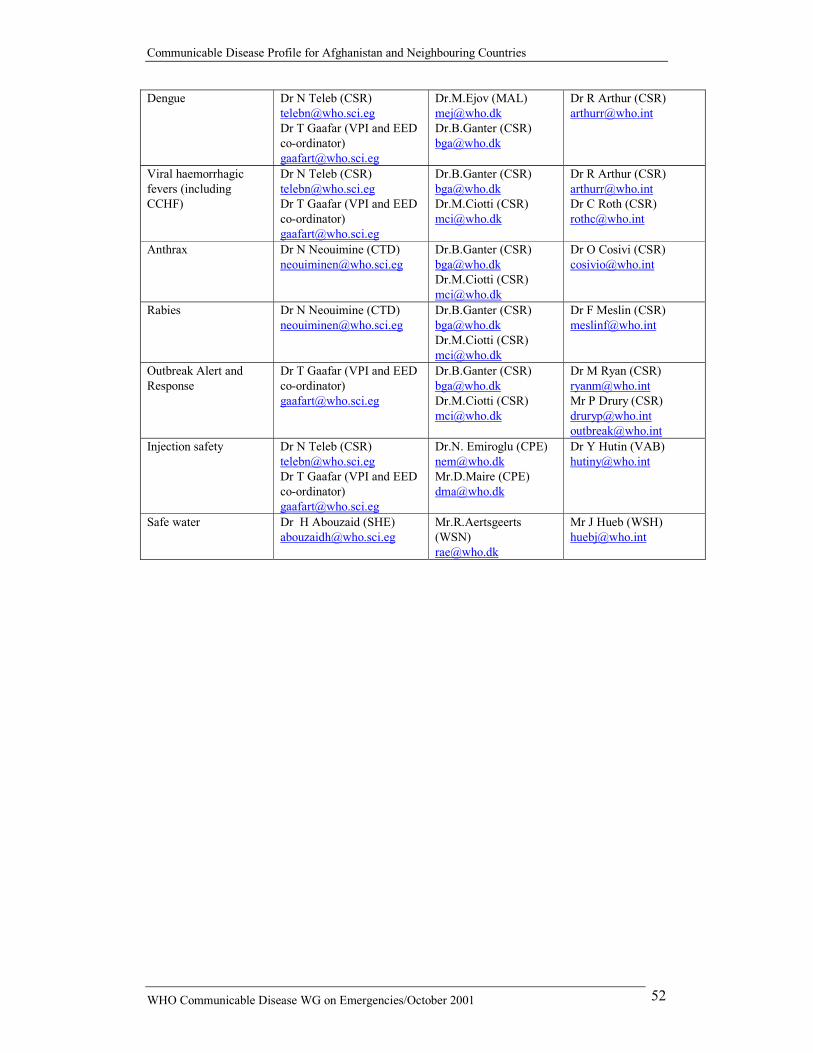
Communicable Disease Profile for Afghanistan and Neighbouring Countries
WHO Communicable Disease WG on Emergencies/October 2001 52
Dengue Dr N Teleb (CSR) [email protected] Dr T Gaafar (VPI and EED co-ordinator) [email protected]
Dr.M.Ejov (MAL) [email protected] Dr.B.Ganter (CSR) [email protected]
Dr R Arthur (CSR) [email protected]
Viral haemorrhagic fevers (including CCHF)
Dr N Teleb (CSR) [email protected] Dr T Gaafar (VPI and EED co-ordinator) [email protected]
Dr.B.Ganter (CSR) [email protected] Dr.M.Ciotti (CSR) [email protected]
Dr R Arthur (CSR) [email protected] Dr C Roth (CSR) [email protected]
Anthrax Dr N Neouimine (CTD) [email protected]
Dr.B.Ganter (CSR) [email protected] Dr.M.Ciotti (CSR) [email protected]
Dr O Cosivi (CSR) [email protected]
Rabies Dr N Neouimine (CTD) [email protected]
Dr.B.Ganter (CSR) [email protected] Dr.M.Ciotti (CSR) [email protected]
Dr F Meslin (CSR) [email protected]
Outbreak Alert and Response
Dr T Gaafar (VPI and EED co-ordinator) [email protected]
Dr.B.Ganter (CSR) [email protected] Dr.M.Ciotti (CSR) [email protected]
Dr M Ryan (CSR) [email protected] Mr P Drury (CSR) [email protected] [email protected]
Injection safety Dr N Teleb (CSR) [email protected] Dr T Gaafar (VPI and EED co-ordinator) [email protected]
Dr.N. Emiroglu (CPE) [email protected] Mr.D.Maire (CPE) [email protected]
Dr Y Hutin (VAB) [email protected]
Safe water Dr H Abouzaid (SHE) [email protected]
Mr.R.Aertsgeerts (WSN) [email protected]
Mr J Hueb (WSH) [email protected]
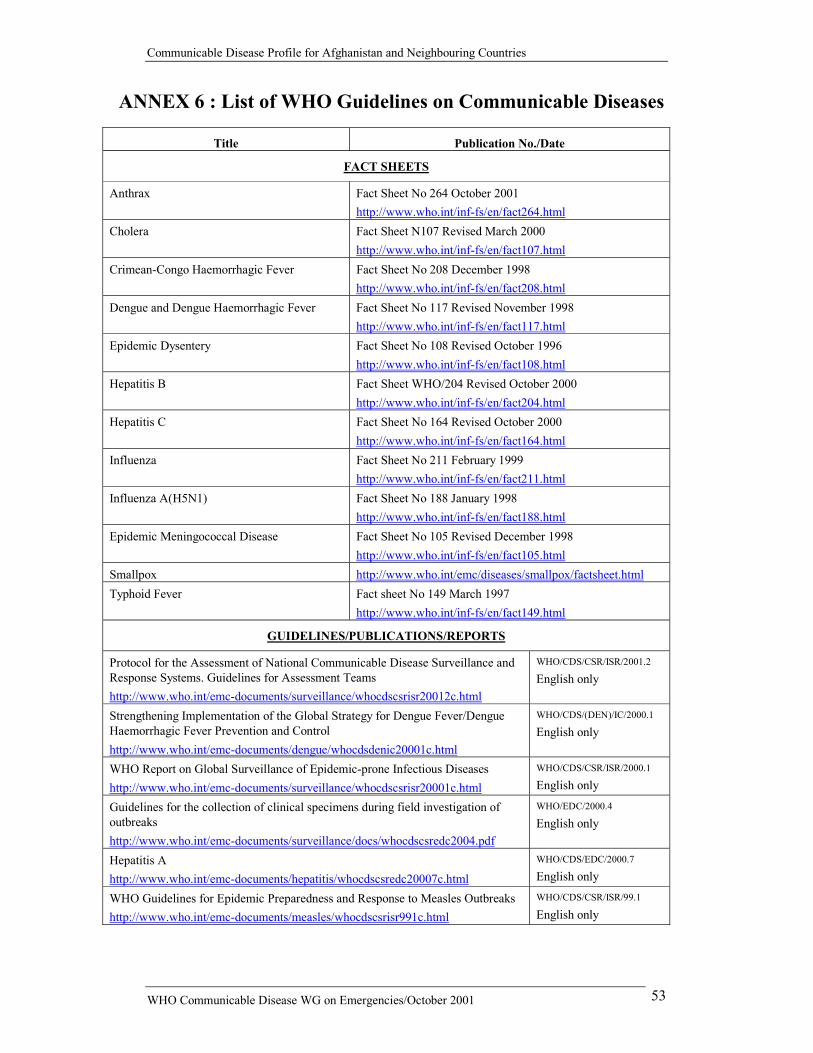
Communicable Disease Profile for Afghanistan and Neighbouring Countries
WHO Communicable Disease WG on Emergencies/October 2001 53
ANNEX 6 : List of WHO Guidelines on Communicable Diseases
Title Publication No./Date
FACT SHEETS
Anthrax Fact Sheet No 264 October 2001 http://www.who.int/inf-fs/en/fact264.html
Cholera Fact Sheet N107 Revised March 2000 http://www.who.int/inf-fs/en/fact107.html
Crimean-Congo Haemorrhagic Fever Fact Sheet No 208 December 1998 http://www.who.int/inf-fs/en/fact208.html
Dengue and Dengue Haemorrhagic Fever Fact Sheet No 117 Revised November 1998 http://www.who.int/inf-fs/en/fact117.html
Epidemic Dysentery Fact Sheet No 108 Revised October 1996 http://www.who.int/inf-fs/en/fact108.html
Hepatitis B Fact Sheet WHO/204 Revised October 2000 http://www.who.int/inf-fs/en/fact204.html
Hepatitis C Fact Sheet No 164 Revised October 2000 http://www.who.int/inf-fs/en/fact164.html
Influenza Fact Sheet No 211 February 1999 http://www.who.int/inf-fs/en/fact211.html
Influenza A(H5N1) Fact Sheet No 188 January 1998 http://www.who.int/inf-fs/en/fact188.html
Epidemic Meningococcal Disease Fact Sheet No 105 Revised December 1998 http://www.who.int/inf-fs/en/fact105.html
Smallpox http://www.who.int/emc/diseases/smallpox/factsheet.html Typhoid Fever Fact sheet No 149 March 1997
http://www.who.int/inf-fs/en/fact149.html
GUIDELINES/PUBLICATIONS/REPORTS
Protocol for the Assessment of National Communicable Disease Surveillance and Response Systems. Guidelines for Assessment Teams http://www.who.int/emc-documents/surveillance/whocdscsrisr20012c.html
WHO/CDS/CSR/ISR/2001.2
English only
Strengthening Implementation of the Global Strategy for Dengue Fever/Dengue Haemorrhagic Fever Prevention and Control http://www.who.int/emc-documents/dengue/whocdsdenic20001c.html
WHO/CDS/(DEN)/IC/2000.1
English only
WHO Report on Global Surveillance of Epidemic-prone Infectious Diseases http://www.who.int/emc-documents/surveillance/whocdscsrisr20001c.html
WHO/CDS/CSR/ISR/2000.1
English only
Guidelines for the collection of clinical specimens during field investigation of outbreaks http://www.who.int/emc-documents/surveillance/docs/whocdscsredc2004.pdf
WHO/EDC/2000.4
English only
Hepatitis A http://www.who.int/emc-documents/hepatitis/whocdscsredc20007c.html
WHO/CDS/EDC/2000.7
English only
WHO Guidelines for Epidemic Preparedness and Response to Measles Outbreaks http://www.who.int/emc-documents/measles/whocdscsrisr991c.html
WHO/CDS/CSR/ISR/99.1
English only
Communicable Disease Profile for Afghanistan and Neighbouring Countries
WHO Communicable Disease WG on Emergencies/October 2001 54
Influenza Pandemic Preparedness Plan. The Role of WHO and Guidelines for National and Regional Planning http://www.who.int/emc-documents/influenza/whocdscsredc991c.html
WHO/CDS/CSR/EDC/99.1
English only
Plague Manual: Epidemiology, Distribution, Surveillance and Control http://www.who.int/emc-documents/plague/whocdscsredc992c.html
WHO/CDS/CSR/EDC/99.2
English and French
Laboratory methods for the diagnosis of meningitis caused by Neisseria meningitidis, Streptococcus pneumoniae, and Haemophilus influenzae http://www.who.int/emc-documents/meningitis/whocdscsredc997c.html
WHO/CDS/CSR/EDC/99.7
English and French
Infection Control for Viral Haemorrhagic Fevers in the African Health Care Setting http://www.who.int/emc-documents/haem_fevers/whoemcesr982c.html
WHO/EMC/ESR/98.2
English and French
Control of epidemic meningococcal disease. WHO practical guidelines 2nd edition http://www.who.int/emc-documents/meningitis/whoemcbac983c.html
WHO/EMC/BAC/98.3
English and French
Guidelines for the Surveillance and Control of Anthrax in Human and Animals. 3rd edition
WHO/EMC/ZDI/98.6
Guidelines for the safe transport of infectious substances and diagnostic specimens http://www.who.int/emc-documents/biosafety/whoemc973c.html
WHO/EMC/97.3
English, French and Spanish
Dengue haemorrhagic fever: Diagnosis, treatment, prevention and control. 2nd edition http://www.who.int/emc/diseases/ebola/Denguepublication/index.html
1997
English only
Guidelines for the control of epidemics due to Shigella dysenteriae type 1 http://www.who.int/emc-documents/cholera/whocdr954c.html
WHO/CDR/95.4
English only
Guidelines for Cholera Control 1993