common mental health disorders: identification and pathways to care implementing nice guidance...
TRANSCRIPT
Common mental health disorders: identification
and pathways to care
Implementing NICE guidance within primary care
2011
NICE clinical guideline 123

What this presentation covers
Scope
Background
Key recommendations for implementation
Primary care costs avoided and benefits
Discussion
Find out more

Scope
The guideline aims to improve access to care and the identification and recognition of common mental health disorders, and provide advice on principles for local care pathways.
Advice from existing NICE guidelines has been combined with new recommendations on access, assessment and local care pathways.
Common mental health disorders include depression, panic disorder, generalised anxiety disorder, obsessive-compulsive disorder, post-traumatic stress disorder and social anxiety disorder.

Epidemiology
• 15% of the population are affected by common mental health disorders
• Women are 1.5 to 2.5 times more likely to experience depression than men
• 34% of South Asian women have a common mental health disorder compared with 10% of South Asian men

Background
• Depression is a leading cause of disability – and it is projected to become the second most common cause of loss of disability-adjusted life years in the world
• Only a small minority of people who experience anxiety disorders receive treatment
• Recognition of anxiety disorders in primary care is particularly poor

Abbreviations used
CBT - cognitive behavioural therapy
ERP - exposure and response prevention
EMDR - eye movement desensitisation and reprocessing
GAD - generalised anxiety disorder
OCD - obsessive compulsive disorder
IPT - interpersonal psychotherapy
PTSD - post-traumatic stress disorderA full glossary of terms used in the guidance can be foundalongside this slide set on the NICE website
Key priorities for implementation
Areas identified as key priorities for implementation:
•Identification
•Improving access to services
•Developing local care pathways

Be alert for possible depression, particularly in those with a past history or possible somatic symptoms of depression, or a chronic physical health problem
Consider asking:
Identification: depression
• During the last month, have you often been bothered by feeling down, depressed or hopeless?
• During the last month, have you often been bothered by having little interest or pleasure in doing things?

Be alert to possible anxiety disorders, particularly in those with a past history or possible somatic symptoms of an anxiety disorder, or who have experienced a recent traumatic event.
Consider asking about feelings of anxiety and the ability to stop or control worry, using the GAD-2 scale.
Identification: anxiety 1

Identification: anxiety 2
The GAD-7 tool was developed by Drs. Robert L. Spitzer, Janet B.W. Williams, Kurt Kroenke and colleagues, with an educational grant from Pfizer Inc.
GAD-2 is the first two questions of the GAD-7 scale
Over the last two weeks, how often have you been bothered by the following problems?
• Feeling nervous, anxious or on edge
• Not being able to stop or control worrying
Consider asking:

Score of 3 or more consider an anxiety disorder and follow the recommendations for assessment
Score of less than 3 but you still have concerns that the person may have an anxiety disorder ask:
Identification: anxiety 3
Do you find yourself avoiding places or activities and does this cause you problems?
N.B. The scoring of more or less than 3 applies to the use of the two GAD-2 questions

For significant communication difficulties, consider using the Distress Thermometer and/or asking a family member or carer about the person’s symptoms
Identification
If identification questions indicate a common mental health disorder, a competent practitioner should perform a mental health assessment
If this professional is not the person’s GP, informthe GP of the referral

Consider using:
• A diagnostic or problem identification tool, for example the Improving Access to Psychological Therapies (IAPT) screening prompts tool
• A validated measure relevant to the disorder to informassessment and support evaluation of interventions: - 9-item Patient Health Questionnaire (PHQ-9) - Hospital Anxiety and Depression Scale (HADS) - 7-item Generalized Anxiety Disorder scale (GAD-7)
Assessment
Ask directly about suicidal ideation and intent

Staff conducting assessments should be able to:
- determine the nature, duration and severity of the presenting disorder- take into account symptom severity and associated functional impairment- identify appropriate treatment and referral options in line with relevant NICE guidance
Consider factors that may affect the development,course and severity of a person’s presenting problem:
- history of mental health disorder or chronic physical health - past experience and response to treatments - quality of interpersonal relationships - living conditions and social isolation
Assessment: core components

Mild relatively few core symptoms, a limited duration and little impact on day-to-day functioning
Moderate all core symptoms of the disorder plus other related symptoms, duration beyond that required by minimum diagnostic criteria, and a clear impact on functioning
Severe most or all symptoms of the disorder, often of long duration and with very marked impact on functioning
Persistent subthreshold symptoms and associated functional impairment that do not meet full diagnostic criteria but have a substantial impact on a person’s life, and which are presentfor a significant period of time
Severity of common mental health disorders: definitions

Stepped-care model
CMHDs presentation and severity Recommended interventions
Step 1All disorders – known and suspected presentations
All disorders: Identification, assessment, psychoeducation, active monitoring; referral for further assessment and interventions
Step 2Persistent subthreshold depressive symptoms or mild to moderate depression; GAD; mild to moderate panic disorder; mild to moderate OCD; PTSD (including mild to moderate)
DepressionGAD and panic disorderOCD PTSDAll disorders – Support groups, educational and employment support services; referral for further assessment and interventions
Step 3Persistent subthreshold depressive symptoms; mild to moderate depression not responded to a low-intensity intervention; moderate or severe depression; GAD with functional impairment or has not responded to low-intensity intervention; moderate to severe panic disorder; OCD with moderate or severe functional impairment; PTSD
DepressionGADPanic disorderOCD PTSD All disorders – Support groups, educational and employment support services; referral for further assessment and interventions

Collaborate to develop local care pathways that:
• support integrated delivery across primary and secondary care
• have clear and explicit entry criteria
• focus on entry and not exclusion criteria
• have multiple means and points of access,including self-referral
• have a designated lead to oversee care
• promote access for people from sociallyexcluded groups
Improving access to services

Design local care pathways that promote a stepped-care model of integrated delivery to:
•provide least intrusive, most effective interventions first•have explicit criteria for different levels of intervention •not base movement between levels on a single criteria •monitor progress and outcomes •minimise the need for transition between services•establish clear access and entry points•have designated staff responsible for coordinationof care
Developing local care pathways:1

Develop protocols for communicating information:
•for service users about their care •with other professionals (including GPs) •between services within the pathway•to services outside the pathway
Robust systems should be in place to ensure routine reporting of outcomes
Developing local care pathways: 2

Primary care costs avoided and benefits
Due to variation in current practice, it is not possible to quantify the national cost impact of the NICE recommendations.The following areas may incur savings through drug costs avoidedby meeting additional demand with treatments such as talking therapies.
People with mild panic disorder.People with mild depression or anxiety or both.
Estimated reduction in need - GP services and medications
60%
Saving in GP visits and drug costs
£ 471 per person
People who have mild - moderate OCD.
Estimated reduction in need of medications
53%
Saving in drug costs
£202 per person

Interventions for anxiety: potential costs
Intervention Cost of intervention
Identification and assessment Minimal
Low-intensity psychological interventions (LIPI)
£540 for 6 sessions or £45 per person based on a group of 12
Drug treatment From £189 to £449
High-intensity psychological interventions (HIPI)
£1125 per person for 15 sessions
Highly specialist treatment As shown for drug treatment & HIPI but combined.Inpatient episode £6496
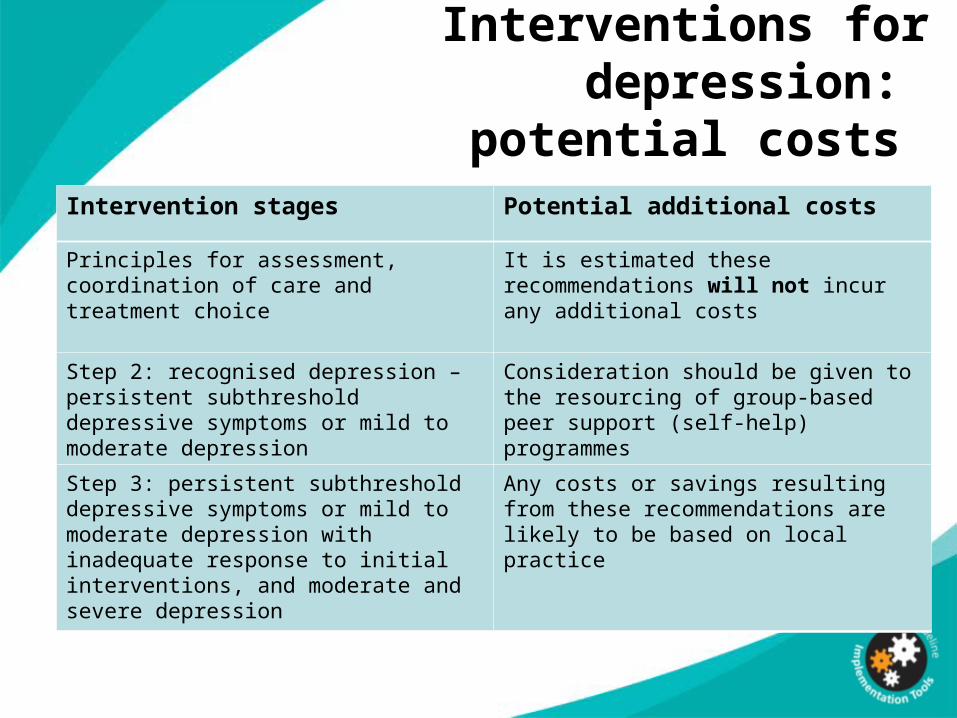
Interventions for depression: potential costs
Intervention stages Potential additional costs
Principles for assessment, coordination of care and treatment choice
It is estimated these recommendations will not incur any additional costs
Step 2: recognised depression – persistent subthreshold depressive symptoms or mild to moderate depression
Consideration should be given to the resourcing of group-based peer support (self-help) programmes
Step 3: persistent subthreshold depressive symptoms or mild to moderate depression with inadequate response to initial interventions, and moderate and severe depression
Any costs or savings resulting from these recommendations are likely to be based on local practice

Discussion
• How are diagnostic or problem identification tools used in primary care?What audit activity reviews their use?
• How do our care pathways compare with the NICE guidance?
• What methods are used to review service user treatment outcomes?
• How can we address cases where there is persistent subthreshold CMHD symptoms?
Find out more
Visit www.nice.org.uk/guidance/CG123 for:
•the guideline •the quick reference guide•‘Understanding NICE guidance’•costing report and template•baseline assessment •Resource for primary care•online educational tools

Presenter notes
The previous slide marks the end of the presentation;slides from this point on are for use by the presenter.
For information, the stepped-care table on slide 16 contains action buttons that link to more detailed content (which is stored within slides 25-28). Action buttons only operate when the presentationis in slide show view. The presenter will need to click on a hyperlink to access the further detail.

Feedback
Did the implementation tool you accessed today meet your requirements, and will it help you to put the NICE guidance into practice?
We value your opinion and are looking for ways to improve our tools.Please complete this short evaluation form
The feedback survey can be accessed by right clicking your mouse overthe hyperlink, and then selecting open hyperlink from the menu options
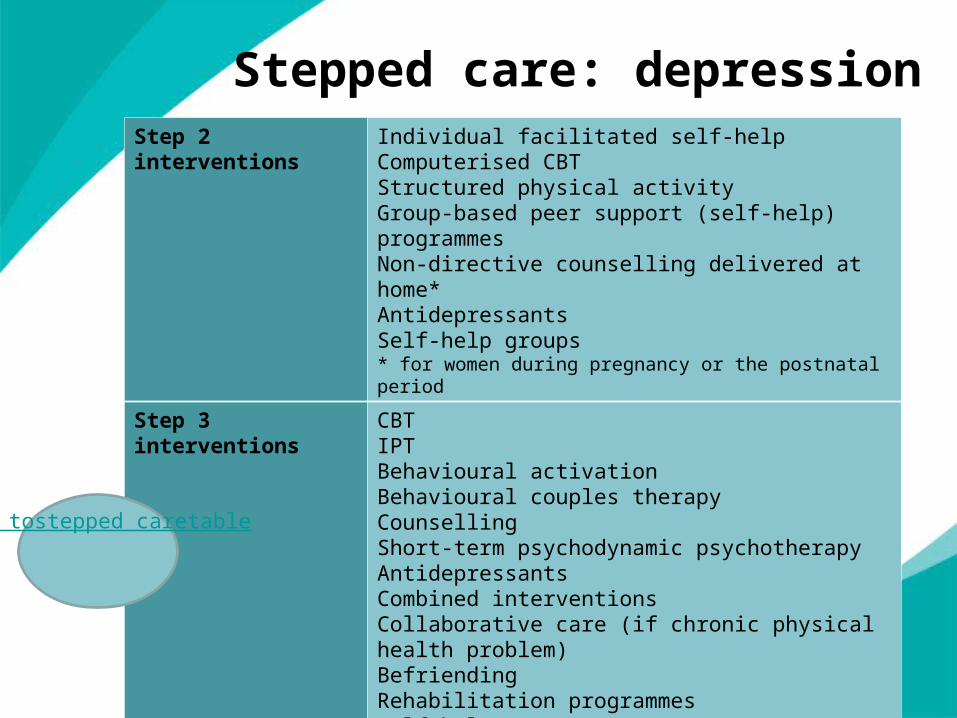
Stepped care: depressionStep 2 interventions Individual facilitated self-help
Computerised CBTStructured physical activityGroup-based peer support (self-help) programmesNon-directive counselling delivered at home*AntidepressantsSelf-help groups* for women during pregnancy or the postnatal period
Step 3 interventions CBTIPTBehavioural activationBehavioural couples therapyCounsellingShort-term psychodynamic psychotherapyAntidepressantsCombined interventionsCollaborative care (if chronic physical health problem)BefriendingRehabilitation programmesSelf-help groups
Back tostepped caretable

Stepped care: GAD and panic disorder
Step 2 interventions
GAD and Panic disorder
Individual non-facilitated self-help Facilitated self-helpPsychoeducational groupsSelf-help groups
Step 3 interventions
GAD
CBTApplied relaxationDrug treatmentCombined interventionsSelf-help groups
Step 3 interventions
Panic disorder
CBTAntidepressantsSelf-help groups
Back tostepped caretable

Stepped care: obsessive-compulsive disorder
Step 2 interventions Individual CBTGroup CBT (including ERP)Self-help groups
Step 3 interventions CBT (including ERP)AntidepressantsCombined interventions and case managementSelf-help groups
Back tostepped care
table

Stepped care: post-traumatic stress disorder
Step 2 interventions Trauma-focused CBTEMDR
Step 3 interventions Trauma-focused CBTEMDRDrug treatment
Back tostepped care
table