committed to complete stroke care
TRANSCRIPT
_ 01.May. 2014
Copyright © 2014 Stryker Stroke: Our Only Focus. Our Ongoing Promise.
Committed to Complete Stroke Carewith Innovative Endovascular Solutions for Severe Stroke Patientswww.trevoinformation.com
SNV-689 Times 2014 Patient Ad_264x50_C4a.indd 1 4/24/14 1:54 PM
PAGE 03
SPECIALISTUNITS ARETHE FUTURE
PAGE 08
SAVING LIVESALSO SAVESNHS MONEY
PAGE 12
MOVIE TECHIS AIDINGRECOVERY
UNDERSTANDING STROKE
raconteur.net twitter: @raconteur
CONTACT US AT 0800 411 8100 | [email protected] results vary. Consult with a qualified physician to determine if these product are right for you. Contraindications, Adverse Reactions and Precautions are available on-line at www.bioness.com (also available in the L300/L300 Plus User’s Guide).NESS®, NESS L300®, NESS L300® Plus, Intelli-Gait®, Intelli-Sense Gait Sensor®, Bioness®, the Bioness Logo and LiveOn® are trademarks of Bioness Inc. are trademarks of Bioness Inc. in the United States or other countries | www.bioness.com | Rx Only© 2014 Bioness Inc.
Walk more naturally with the award-winning L300® FootDrop System and the L300® Plus System and improve handfunction with the H200® Wireless Hand Rehabilitation System.
These advanced-technology systems stimulate the nerves controlling your muscles, helping to lift your foot or open your hand to give you more freedom and a greater sense of confidence to enjoy your daily activities.
START YOUR JOURNEY TODAY
&MobilityRegainyour
Independence.
0 4 7 3
03
Ȗ The human misery and financial burden of strokes have a devastat-ing impact on the 152,000 peo-ple across the UK who suffer the potentially debilitating condition every year. More than 900,000 are living with a legacy of physical and neurological impairment, and half of them depend on others for help in their everyday lives.
Landmark studies by Professor Alistair McGuire at the London School of Economics (LSE) and colleagues from King’s College London estimate that dealing with stroke costs the UK economy £8.9 billion a year, made up of £4 billion in treatment costs, around £2.5 million for informal care and the rest in lost productivity.
Despite great strides forward since the introduction of the National Stroke Strategy (NSS) by the Department of Health in 2007, effective treatment in the crucial therapeutic window, which experts have recently extended from three to four-and-a-half hours after the stroke, can be inconsistent.
“We have seen very good pro-gress in many aspects of stroke
care, but there is a lot of unfinished business and an overarching con-cern is that people think the job is done – when that is not the case,” says Joe Korner, director of exter-nal affairs at the Stroke Associa-tion, the UK’s stroke charity.
The NSS has seen a dramatic reduction in 30-day mortality rates – from 30 per cent to below 20 per cent over the last seven years – because patients are get-ting to dedicated stroke units quickly with rapid access to clot-busting drugs and brain scans.
“Some services are very good, but others have too many delays,” says Mr Korner. “Unfortunately there are places around the country where, if you are unlucky enough to have your stroke on a Friday evening, you may not get the level of support you need.”
The need and financial impera-tive of getting stroke services right has been established with the LSE research indicating that invest-ment in stroke units saves money in the long run by minimising the damage caused by the stroke, and reducing the long-term rehabilita-
tion and care bill that follows for most patients.
Repeated healthy lifestyle mes-sages from successive govern-ments are not achieving the sea change in public habits that could drastically reduce stroke, along with cardiovascular dis-ease, and a misconception that the condition only affects the elderly has also acted as a barrier to improvement.
One in three people who suffer a stroke are under 65 years old. Many of them will have had a TIA – a transient ischaemic attack – also known as a mini stroke that causes a temporary blockage in the blood supply to the brain with the symptoms usually receding after 24 hours with no perma-nent damage.
The 54-year-old broadcaster Andrew Marr, who is still recov-ering from his stroke in January last year, revealed that he had two mini strokes without seeking extra medical help leading up to the full stoke. He considers himself lucky to be alive.
Mr Korner commented: “The impression that stroke is some-thing for an elderly age group is a major break on progress. With TIAs, the general assumption among the public and to an extent GPs is that you have had a funny turn so you need to go home, have a cup of tea and an aspirin, and you will be all right.
“You should be treated as an emergency because there are pro-
tocols that can reduce the danger which is vital as the risk of a stroke after a TIA is very high within the next two days.”
Tim England, clinical associ-ate professor in stroke medicine at Nottingham University and a consultant at the Royal Derby Hospital, points out that the move towards bespoke stroke centres offering gold-standard care had boosted patient outcomes.
Patients are now taken to regional hospitals that are centres of excellence for immediate assess-ment and treatment from a multi-disciplinary team to get the best chance of survival and recovery.
Reconfigured services in Lon-don, Manchester, Nottingham and the East Midlands, and soon Birmingham, are changing the dynamics of stroke treatment and raising it to the response level of cardiac services.
But research into finding drugs to minimise damage after strokes, including stem cell therapy, is still in its infancy. “If I had a magic wand, I would wish for drugs that would help prevent damage after a stroke,” says Dr England. “People are working on that, but it is some way off.”
Mr Korner concludes: “This is a preventable and treatable condi-tion, but unless concerted action is taken in this country and across the world we are going to see huge numbers of needless deaths and needless suffering of many thou-sands, if not millions, of people.”
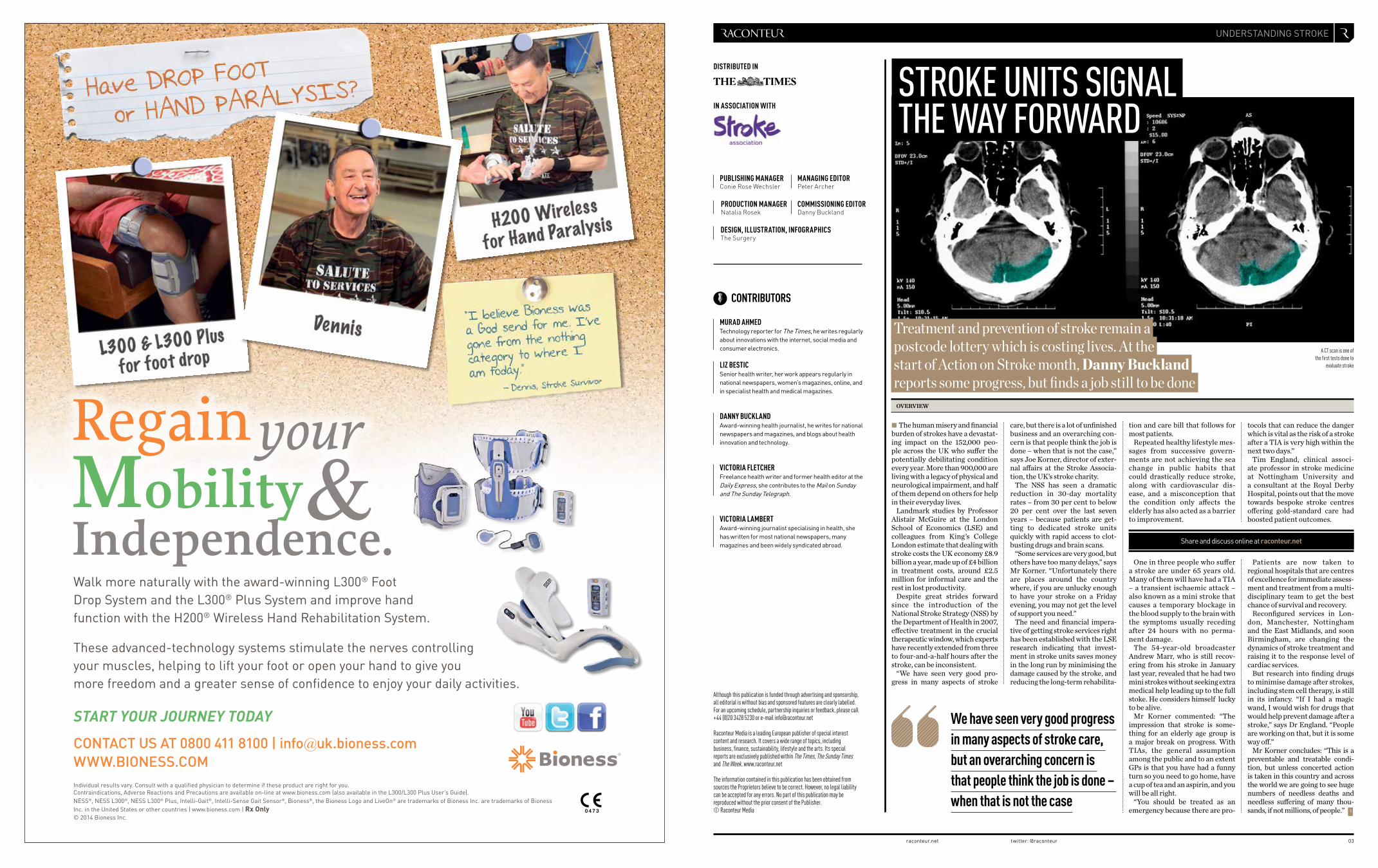
Treatment and prevention of stroke remain a postcode lottery which is costing lives. At the start of Action on Stroke month, Danny Buckland reports some progress, but finds a job still to be done OVERVIEW
STROKE UNITS SIGNAL THE WAY FORWARD
We have seen very good progress in many aspects of stroke care, but an overarching concern is that people think the job is done – when that is not the case
DISTRIBUTED IN
IN ASSOCIATION WITH
MURAD AHMEDTechnology reporter for The Times, he writes regularly about innovations with the internet, social media and consumer electronics.
LIZ BESTICSenior health writer, her work appears regularly in national newspapers, women’s magazines, online, and in specialist health and medical magazines.
DANNY BUCKLANDAward-winning health journalist, he writes for national newspapers and magazines, and blogs about health innovation and technology.
VICTORIA FLETCHERFreelance health writer and former health editor at the Daily Express, she contributes to the Mail on Sunday and The Sunday Telegraph.
VICTORIA LAMBERTAward-winning journalist specialising in health, she has written for most national newspapers, many magazines and been widely syndicated abroad.
DESIGN, ILLUSTRATION, INFOGRAPHICSThe Surgery
PUBLISHING MANAGERConie Rose Wechsler
MANAGING EDITORPeter Archer
PRODUCTION MANAGERNatalia Rosek
COMMISSIONING EDITORDanny Buckland
Although this publication is funded through advertising and sponsorship, all editorial is without bias and sponsored features are clearly labelled. For an upcoming schedule, partnership inquiries or feedback, please call +44 (0)20 3428 5230 or e-mail [email protected]
Raconteur Media is a leading European publisher of special interest content and research. It covers a wide range of topics, including business, finance, sustainability, lifestyle and the arts. Its special reports are exclusively published within The Times, The Sunday Times and The Week. www.raconteur.net
The information contained in this publication has been obtained from sources the Proprietors believe to be correct. However, no legal liability can be accepted for any errors. No part of this publication may be reproduced without the prior consent of the Publisher. © Raconteur Media
Share and discuss online at raconteur.net
CONTRIBUTORS
A CT scan is one of the first tests done to
evaluate stroke
raconteur.net twitter: @raconteur raconteur.net twitter: @raconteur 0504
UNDERSTANDING STROKEUNDERSTANDING STROKE
The most important risk factor of stroke is whether you have high blood pressure as it can damage or narrow the arteries. So says Professor Tony Rudd, national clinical director for stroke, based at Guy’s and St Thomas’ NHS Foundation Trust. “If everyone had well-controlled blood pressure – below 130mmol/80mmol – it would prevent 60 per cent of strokes,” he says. High blood pressure is a com-mon problem, affecting about ten mil-lion people in the UK. It often has no
symptoms; having it measured is the only way to tell if your blood pressure is high, and putting a strain on your arteries and heart. This makes it more likely that you will suf-fer a stroke or other health problems, such as a heart attack or kidney disease. Blood pressure varies throughout the day, going down if you are asleep or sitting quietly and going up if you are rushing about or stressed. The NHS recommends that all adults should have their blood pressure checked at least every five years. If you haven’t had yours measured or don’t know what your reading is, ask your GP to check it.
ONE
Insomnia may significantly increase your risk of stroke and subsequent stroke hospitalisations, according to the American Heart Association journal Stroke. The risk was highest – up to eight times – among insom-niacs aged 18 to 34 years old in a study by Professor Ya-Wen Hsu of the Department of Medical Research at Chi-Mei Medical Center in Taiwan. The risk also seems far greater when insomnia occurs as a young adult compared to those who are older. Research by Dr Chien-Yi Hsu, a cardiologist at Taipei Veterans General Hospital, also in Taiwan, shows that people with insom-nia are twice as likely to have heart attacks or strokes as those without the sleep disorder. “Doctors should pay more attention to their patient’s insomnia symp-toms, and consider using different methods to improve sleep, including medical, psychological or behavioural therapy, which might improve subject quality of life and reduce the risk of cardiovascular disease,” he says. The link between insomnia and stroke is not yet fully understood, but 90 per cent of people with insomnia have another health condition so further research is required.
FOUR
Moderate exercise such as brisk walking may cut stroke risk in women by 20 per cent, says Professor Sophia Wang of the Department of Population Sciences at the City of Hope Beckman Research Institute in Duarte, California, who presented research to the American Stroke Association meet-ing in February. She found that moderate exercise also helps offset some of the increased stroke risk in women taking postmenopausal hormone therapy. “I was surprised that moderate physical activity
was most strongly associated with a reduced risk of stroke,” she says. “More strenuous activity, such as running, didn’t further reduce women’s stroke risk. Moderate activity, such as brisk walking, appeared to be ideal in this scenario.” The Stroke Associa-tion concurs. “Regular exercise, such as walking, can dramatically reduce a range of health risks including stroke,” says Dr Quadir. “We recommend 30 minutes’ moderate exercise five times a week to keep your risk of stroke down.” You can choose any form of exercise as long as the activity increases your heart rate, makes you feel warm and a little out of breath. You could join a class or simply make small changes to your lifestyle.
SEVEN
Eating foods that contain vitamin C may reduce the risk of the most common type of haemorrhagic stroke, according to a new study by Dr Stéphane Vannier, of Pon-tchaillou University Hospital in Rennes, France. Vitamin C is found in fruits and vegetables such as oranges, papaya, peppers, broccoli and strawberries. “It’s important to eat healthily as high amounts of fruit and veg reduce your risk of stroke by 30 per cent,” adds Dr Quadir. “Eating your five a day and having plenty of fibre can reduce stroke risk. But high-fat foods
can raise cholesterol and a lot of salt in food can cause high blood pressure, the biggest risk factor for stroke.” The Stroke Association suggests limiting salt to a teaspoon (6g) a day. This includes hidden salt found in some ready-made and processed foods. Most pre-packed foods have a nutrition label on the packaging, which lists amounts of fat, saturated fat, salt or sugar. Watch out for foods which are high in total fat (more than 17.5g of fat per 100g), have more than 5g of saturated fat per 100g, more than 22.5g of total sugars per 100g and more than 1.5g of salt per 100g (or 0.6g sodium).
THREE
Smoking doubles the risk of stroke as it narrows the arteries, while high alcohol intake is potentially dangerous because it exacerbates obesity and high blood pres-sure. Family history matters too. “We’re not sure to what extent stroke is genetic,” says Dr Quadir. “Some stroke risk is hereditary while many strokes are caused by lifestyle factors, such as smoking – factors or habits that can run in the family too. But it is cer-tainly true that if a close relative has a stroke your risk is likely to be higher.” And heritage is a factor. Although it is not understood why, people of South Asian, black African and Caribbean origin in the UK are more at risk of stroke than the rest of the population. According to new consensus recommendations in the British Medical Journal on how best to stave off a worldwide epidemic of cardiovascular disease, understanding the true age of your heart is key to curbing the lifetime risk of developing – and dying from – stroke and heart disease. You can do this using a new method of risk assessment, the JBS3 risk calculator (http://www.jbs3risk.com/pages/risk_calculator.htm) which builds a whole-risk picture taking into account age, lifestyle, weight and blood pressure.
SIX
An erratic pulse could be a symptom of atrial fibrillation (AF) a type of irregular heart beat which affects about 750,000 people in the UK. An estimated 15 per cent of all strokes occur in someone with untreated AF. “Having AF means that your heart may not be pumping as well as it should. As a result, blood clots are more likely to form in your heart, increasing your risk of having a stroke,” says neuroscientist Shamim Quadir, research communications manager at the Stroke Association. Symptoms of AF include palpitations, breathlessness, chest pain, fatigue or you may have no symptoms except an irregular pulse over one minute. If concerned, check with your GP. Treatments for AF include medication such as beta blockers which can restore a normal heart rhythm or control the rate at which the heart beats. Other interventions include cardioversion, a controlled electric shock to restore a normal rhythm, or catheter ablation where thin, soft wires are guided through a vein into your heart to record and restore correct electrical activity. Some patients with AF may be prescribed anticoagulants as these can prevent blood clots.
TWO
Healthy postmenopausal women who drink two or more diet drinks a day may be more likely to have a stroke, heart attack or other cardiovascular problems, according to research presented earlier this year at the American College of Cardiology’s 63rd Annual Scientific Session. In fact, compared to women who never or only rarely consume diet drinks, those who consumed two or more a day were 30 per cent more likely to suffer a car-diovascular event and 50 per cent more likely to die from related disease. While scientists don’t yet understand why this is, the Stroke Association’s Dr Quadir highlights that obesity is a significant symptom for stroke as exces-sive weight strains the cardiovascular system, forcing the heart to work too hard. “Even making small changes to your eating habits can make a difference to your over-all health, particularly if you have been told that you are
at risk of having a stroke or mini stroke,” he says. The Stroke Association recommends you use smaller plates and bowls to stay in control of your portion sizes. Switch white pasta and white bread for brown versions, and grill food rather than fry. When ordering a takeaway, swap creamy sauces for less fatty tomato-based sauces.
FIVE
FACTFILE
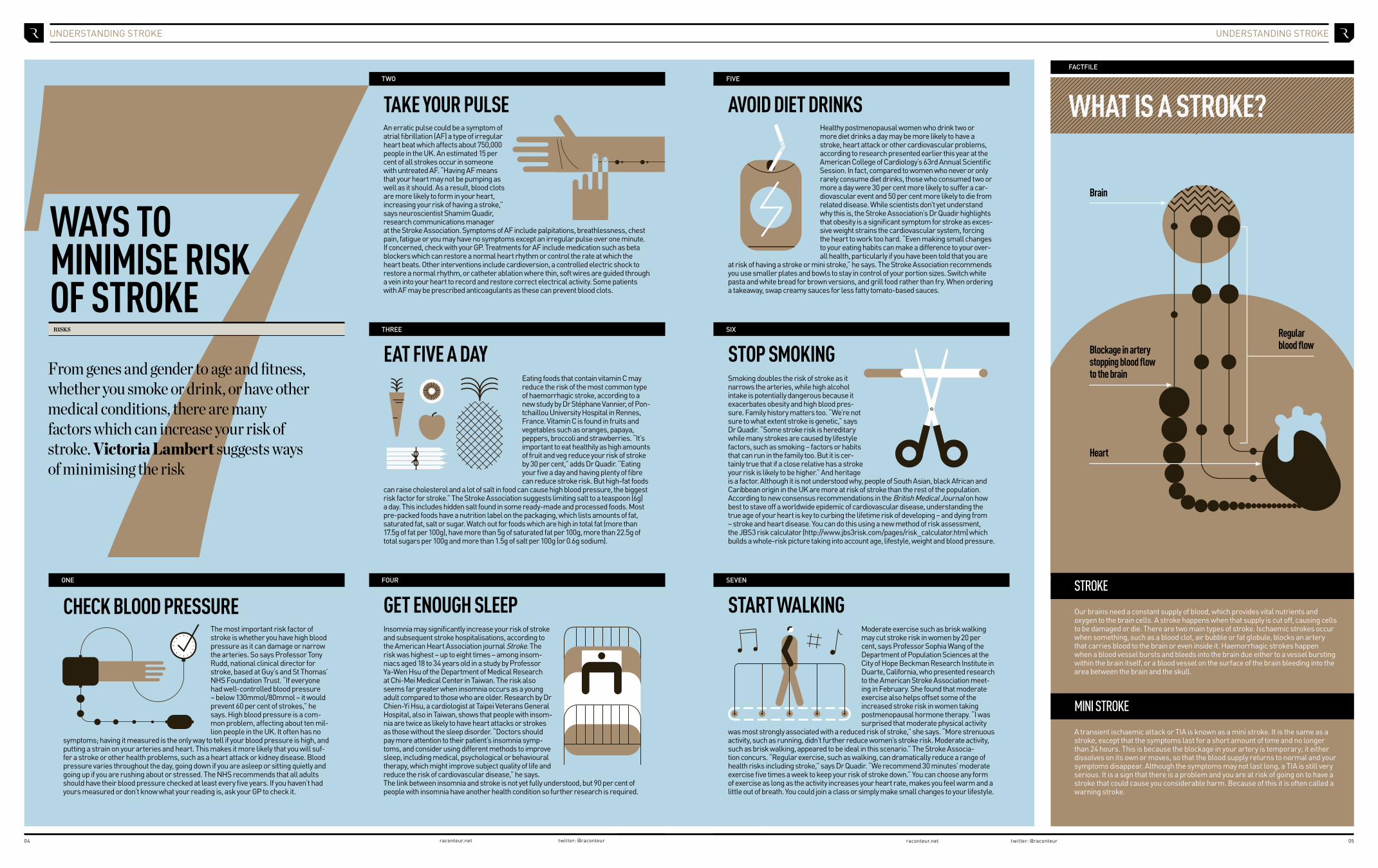
WHAT IS A STROKE?
A transient ischaemic attack or TIA is known as a mini stroke. It is the same as a stroke, except that the symptoms last for a short amount of time and no longer than 24 hours. This is because the blockage in your artery is temporary; it either dissolves on its own or moves, so that the blood supply returns to normal and your symptoms disappear. Although the symptoms may not last long, a TIA is still very serious. It is a sign that there is a problem and you are at risk of going on to have a stroke that could cause you considerable harm. Because of this it is often called a warning stroke.
CHECK BLOOD PRESSURE
TAKE YOUR PULSE AVOID DIET DRINKS
EAT FIVE A DAY STOP SMOKING
GET ENOUGH SLEEP START WALKING
WAYS TO MINIMISE RISK OF STROKE
MINI STROKE
STROKE
Our brains need a constant supply of blood, which provides vital nutrients and oxygen to the brain cells. A stroke happens when that supply is cut off, causing cells to be damaged or die. There are two main types of stroke. Ischaemic strokes occur when something, such as a blood clot, air bubble or fat globule, blocks an artery that carries blood to the brain or even inside it. Haemorrhagic strokes happen when a blood vessel bursts and bleeds into the brain due either to a vessel bursting within the brain itself, or a blood vessel on the surface of the brain bleeding into the area between the brain and the skull.
Blockage in artery stopping blood flow to the brain
Brain
Heart
Regular blood flow
RISKS
From genes and gender to age and fitness, whether you smoke or drink, or have other medical conditions, there are many factors which can increase your risk of stroke. Victoria Lambert suggests ways of minimising the risk
UNDERSTANDING STROKE UNDERSTANDING STROKE
raconteur.net twitter: @raconteur raconteur.net twitter: @raconteur 0706
TREATMENT
Ȗ Stroke nurse specialist Alison Loosemore is passionate about her job on the Acute Stroke Unit at St George’s Hospital, South London. “It’s the total embodiment of what nursing should be about – compas-sion, care, understanding, focus and hard work,” she says.
“A stroke is everyone’s fear and is dramatic and potentially com-pletely life-changing. You have to work closely with the patient, offer-ing strategies that support their personal dignity and expectations.”
Underpinning that humanity is advanced diagnostic equipment, stroke consultants with banks of knowledge and a flow system that would be the envy of any con-sumer business.
Stroke treatment is about com-bining empathy, expertise and efficiency in a seamless delivery.
St George’s in Tooting is one of eight London hospitals that, under London’s stroke service reor-ganisation in 2010, now operate a Hyper Acute Stroke Unit (HASU). Patients get rapid access to CT scans, thrombolytics (clot-busting drugs) and continuous specialist care during the first 72 hours fol-lowing a stroke.
A recent study by UCLPartners has shown that centralising acute stroke services in London has saved more than 400 lives since 2010.
“Before then, stroke services were provided in 30 acute hospitals across the region and stroke care in London was pretty patchy,” says Geoff Cloud, consultant stroke physician at St George’s. “We know that ‘time is brain’ which means the sooner someone who has a stroke is treated with clot-busting drugs, the better their chances of survival and being able to lead a normal life.
“A typical patient loses 1.9 mil-
lion neurons for each minute their stroke is left untreated. Our aspira-tion at St George’s is for so-called ‘door to needle’ time to be within 30 minutes. Nationally, the typical time it takes to get to hospital is an hour. We currently average around 45 minutes.”
The stroke service provides a 24-hour, seven-day-a-week service for thrombolysis to unblock arter-ies, which have caused the stroke. Care is provided in a 20-bed HASU and a 16-bed stroke unit for less acute cases.
Patients are stabilised within three days and then start their rehabilitation at the NHS trust’s specialist stroke unit.
St George’s is unique in provid-ing comprehensive rehabilitation at the Wolfson Neurorehabilita-tion Unit, a tertiary neuroscience centre with latest equipment and a wealth of neurological expertise.
“We have specialist diagnostic services, state-of-the-art brain imaging and specialist neuroint-erventional surgery all under one roof. It is about as good as it gets,” says Dr Cloud.
The hospital has consistently been rated the best in the Royal College of Physicians’ stroke audit, and a study recently praised staff for the way they communicate with patients and carers.
“You see patients who have lost control over their faculties in a very short space of time and you need to be able to console them in a way which sets them off on their journey. Their stroke can completely change their long-term expectations,” says Ms Loosemore.
“And then there are the Lazarus moments when you see someone who thought their whole life was over, and is given thrombolysis
and starts to get the feeling back in their arm and leg. It’s tremen-dously rewarding.”
The gold-standard treatment for stroke doesn’t stop at stabilisa-tion. A team of experts swings into action to integrate patients back into the community.
“The way we measure stroke ser-vices is as much about how people adjust at home to life after stroke as hyperacute care in the first phase of their stroke,” Dr Cloud adds.
“People spend far more time living with the effects of stroke in their own homes than in hospi-tal. There has historically been a mismatch between how much has been invested in hospital care com-pared to rehabilitation at home, but that is rapidly changing.”
At St George’s, the early sup-ported discharge team (ESDT) ensures that acute treatment dove-tails with rehab. For many years there has been an assumption
that if a stroke survivor has not improved in four to six weeks there will be no further improvement.
“This is patently untrue particu-larly for aphasia [speech difficulties] where intensive speech and lan-guage therapy can really improve the condition,” says Dr Cloud.
The ESDT consists of speech and language therapists, occupational therapists and psychologists who can all help make the transition to living back at home smoother.
“Research shows that people do better back in familiar surround-ings. It’s not just about being able to discharge people back home, but about giving them a role in the fam-ily and the community,” says stroke nurse specialist Helen Mann.
“Rehabilitation in the home also makes it much more functional. It’s all very well learning to go up and down steps in the hospital, but that may not translate to the stairs in your own home.”
The ESDT can also help patients return to work by negotiating with employers about adaptations in the
workplace, phased return or consid-ering a different employment role.
Fatigue is often a serious side-effect of a stroke. “Even those who have had a comparatively mild stroke may say they are better, but they forget they are not doing normal things in hospital. When they get home, they are shocked at how shattered they feel. I always advise people not to return to work for at least two weeks,” says Ms Mann.
St George’s is also a centre of excellence in stroke research and is currently looking at the science around the different stages of the stroke journey. “One major piece of research examines methods for the interventional treatment of acute ischemic stroke, such as removing clots through endovas-cular techniques,” says Dr Cloud.
Other clinical trials are looking at preventative treatment for stroke, including drugs to reduce atherosclerosis (furring up of the arteries), which is a major risk factor for stroke, and a trial on implanting pumps so that drugs can be infused into the spinal cord to improve walking.
As Ms Loosemore says: “Stroke medicine is an exciting field now – and seeing someone recover from a stroke and get back home gives a real sense of achievement to every-one involved.”
Stroke treatment is about combining empathy, expertise and efficiency in a seamless delivery
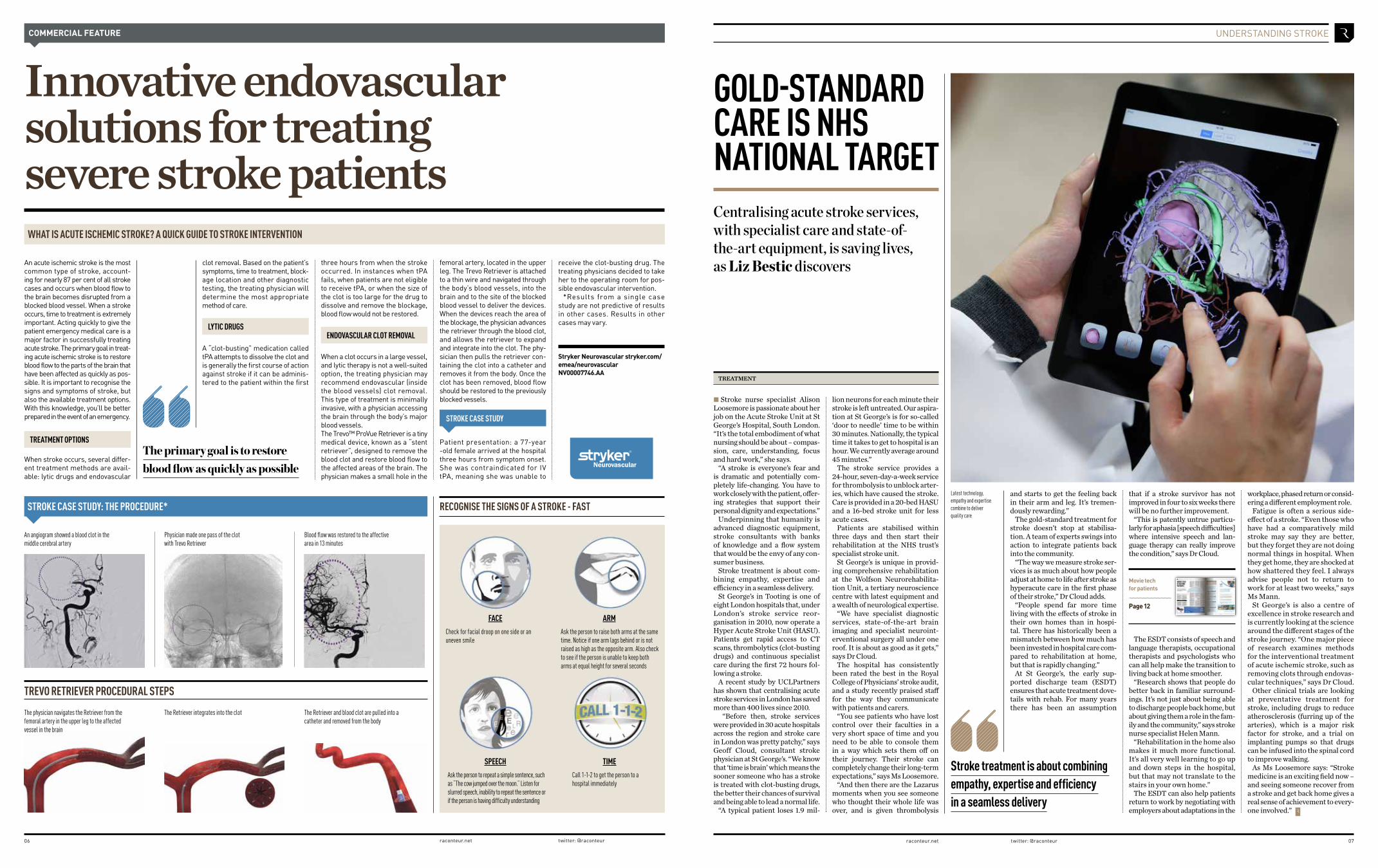
Latest technology, empathy and expertise combine to deliver quality care
GOLD-STANDARD CARE IS NHSNATIONAL TARGETCentralising acute stroke services, with specialist care and state-of- the-art equipment, is saving lives, as Liz Bestic discovers
Movie techfor patients
Page 12
clot removal. Based on the patient’s symptoms, time to treatment, block-age location and other diagnostic testing, the treating physician will determine the most appropriate method of care.
A “clot-busting” medication called tPA attempts to dissolve the clot and is generally the fi rst course of action against stroke if it can be adminis-tered to the patient within the first
An acute ischemic stroke is the most common type of stroke, account-ing for nearly 87 per cent of all stroke cases and occurs when blood flow to the brain becomes disrupted from a blocked blood vessel. When a stroke occurs, time to treatment is extremely important. Acting quickly to give the patient emergency medical care is a major factor in successfully treating acute stroke. The primary goal in treat-ing acute ischemic stroke is to restore blood flow to the parts of the brain that have been affected as quickly as pos-sible. It is important to recognise the signs and symptoms of stroke, but also the available treatment options. With this knowledge, you’ll be better prepared in the event of an emergency.
When stroke occurs, several differ-ent treatment methods are avail-able: lytic drugs and endovascular
three hours from when the stroke occurred. In instances when tPA fails, when patients are not eligible to receive tPA, or when the size of the clot is too large for the drug to dissolve and remove the blockage, blood fl ow would not be restored.
When a clot occurs in a large vessel, and lytic therapy is not a well-suited option, the treating physician may recommend endovascular (inside the blood vessels) clot removal. This type of treatment is minimally invasive, with a physician accessing the brain through the body’s major blood vessels. The Trevo™ ProVue Retriever is a tiny medical device, known as a “stent retriever”, designed to remove the blood clot and restore blood flow to the affected areas of the brain. The physician makes a small hole in the
femoral artery, located in the upper leg. The Trevo Retriever is attached to a thin wire and navigated through the body’s blood vessels, into the brain and to the site of the blocked blood vessel to deliver the devices. When the devices reach the area of the blockage, the physician advances the retriever through the blood clot, and allows the retriever to expand and integrate into the clot. The phy-sician then pulls the retriever con-taining the clot into a catheter and removes it from the body. Once the clot has been removed, blood flow should be restored to the previously blocked vessels.
Patient presentation: a 77-year -old female arrived at the hospital three hours from symptom onset. She was contraindicated for IV tPA, meaning she was unable to
receive the clot-busting drug. The treating physicians decided to take her to the operating room for pos-sible endovascular intervention.
*Results from a single case study are not predictive of results in other cases. Results in other cases may vary.
Stryker Neurovascular stryker.com/emea/neurovascularNV00007746.AA
The primary goal is to restore blood � ow as quickly as possible
Innovative endovascular solutions for treating severe stroke patients
LYTIC DRUGS
TREATMENT OPTIONS
ENDOVASCULAR CLOT REMOVAL
RECOGNISE THE SIGNS OF A STROKE - FAST
Check for facial droop on one side or an uneven smile
FACE
SPEECH
Ask the person to repeat a simple sentence, such as “The cow jumped over the moon.” Listen for slurred speech, inability to repeat the sentence or if the person is having diffi culty understanding
ARM
Ask the person to raise both arms at the same time. Notice if one arm lags behind or is not raised as high as the opposite arm. Also check to see if the person is unable to keep both arms at equal height for several seconds
TIME
Call 1-1-2 to get the person to a hospital immediately
An angiogram showed a blood clot in the middle cerebral artery
Physician made one pass of the clot with Trevo Retriever
Blood fl ow was restored to the affective area in 13 minutes
The physician navigates the Retriever from the femoral artery in the upper leg to the affected vessel in the brainvessel in the brain
The Retriever integrates into the clot The Retriever and blood clot are pulled into a catheter and removed from the body
WHAT IS ACUTE ISCHEMIC STROKE? A QUICK GUIDE TO STROKE INTERVENTION
TREVO RETRIEVER PROCEDURAL STEPS

raconteur.net twitter: @raconteur raconteur.net twitter: @raconteur 0908
UNDERSTANDING STROKEUNDERSTANDING STROKE
Ȗ Having a stroke is among the conditions people in the UK fear most, with one in twenty admit-ting it scares them more than can-cer, dementia and motor neurone disease. However, 70 per cent of strokes could be avoided through changes in lifestyle and better pre-ventive medicine.
High blood pressure, raised cholesterol, diabetes and a heart condition called atrial fibrillation (AF) all dramatically increase the risk of stroke and yet each one can be managed with the correct drugs.
Over the last ten years there has been a major drive to improve the emergency care provided to stroke patients resulting in an impressive 37 per cent fall in stroke deaths.
Now experts are turning their focus to prevention and asking if enough is being done to stop strokes from happening in the first place, through eating well, stopping smoking and also ensur-ing those at high risk are being treated effectively.
They also want to see high stand-ards of treatment to be available across the UK with no postcode lottery of services.
The tide against strokes has turned although there are vagar-ies in the prescribing of antico-agulants and the availability of healthcare. The dominant mes-sage is that levels of stroke can be reduced, but there is plenty of room for improvement from GPs, members of the public and health policy-makers.
In Bradford, for example, there has been an astonishing 11 per cent drop in strokes among patients with atrial fibrillation in only one year, thanks to a local initiative to ensure GPs gave these patients anticoagulation drugs rather than
aspirin or no treatment at all.But in other areas this does
not always happen, resulting in avoidable stroke deaths and dis-ability. The cost of implementing the Bradford programme was just £50,000. Yet each stroke victim would have cost the NHS £15,000 in care over five years.
High blood pressure is the biggest cause of stroke and is responsible for at least 50 per cent of cases.
According to guidelines from the National Institute of Health and Care Excellence (NICE), every incremental 2mmHg rise in sys-tolic blood pressure can increase stroke risk by 10 per cent. Once a patient has a reading above 140/90 mmHg, they may need treatment.
Graham MacGregor, professor of cardiovascular medicine at the Wolfson Institute of Preventive Medicine, says: “Preventing high blood pressure is the single most cost-effective strategy for prevent-ing death and disability. Despite this, only around half of the eight million patients being treated for hypertension, a stroke risk factor, have the condition under control.”
Guidelines are in place to ensure patients with hypertension are treated with a range of drugs, but there is concern that high blood pressure is not being taken seri-ously enough.
Professor Tony Rudd, national clinical director for stroke and chairman of the intercollegiate stroke working party for the Royal College of Physicians, adds: “Sometimes doctors are reluctant to treat someone with high blood pressure aggressively in case the reading is caused by the ‘white coat’ effect of seeing the doctor. But we now know that hypertension is something that
PREVENTION
Treatment to reduce the number of people suffering a stroke can help the NHS balance the books, writes Victoria Fletcher
SAVING LIVESSAVES MONEYAND HEARTACHE
Preventing high blood pressure is the single most cost-effective strategy for preventing death and disability
needs to be brought down rapidly with medication.”
Later this year, new targets within the Quality Outcomes Framework (QOF), through which GPs are paid, will tell family doc-tors to be more ambitious in how far they reduce hypertension in patients who have already suffered a stroke.
However, some patients may have themselves to blame. A study, published last month in the journal Heart, of just over 200 patients, used urine tests to reveal that one in four hypertension patients did not take their medi-cation properly, one in ten didn’t take any of their medication and one in seven took it occasionally, often due to side effects.
Professor MacGregor believes a good doctor should be able to prevent side effects by switching patients on to different dosages of pills or a combination of dif-ferent pills.
Figures from the Stroke Asso-ciation show that statins can reduce stroke risk by 25 per cent. A 1mmol/L drop in cholesterol reduces the risk by 21 per cent.
The benefits of taking statins are particularly key for anyone who has already had a stroke. New figures from the Sentinel Stroke National Audit Programme show that 80 per cent of patients are now put on a statin within six months of suffering a stroke to prevent further stroke and a similar focus is now needed on all patients with high cholesterol to prevent stroke.
But perhaps one of the most eas-ily preventable causes of stroke is AF, which causes an uneven or fast heartbeat that puts patients at higher risk of blood clots.
Figures from the QOF reveal there are more than a million patients in England and Wales with AF. This figure has risen by 20 per cent in only six years, due in part to better detection, but also because AF is more common in an ageing population. By 2050, the figure is expected to double.
AF patients are five to six times more likely to have a stroke because blood pools in the heart, leading to clots.
Estimates suggest that 12,500 strokes a year are caused by AF, and 7,100 strokes and 2,100 deaths could be prevented if these patients were on the correct medication.
Anticoagulation drugs, such as warfarin, stop the blood from clotting and can reduce the risk
of AF stroke by 70 per cent. Yet according to an analysis, published last year in Heart, more than one in three AF patients, who should have been on anticoagulants such as warfarin, were not.
Dr Matthew Fay, a GP in Brad-ford, says: “Many GPs and hospital doctors are afraid of using warfarin because they worry they won’t get the dose right and patients will suffer a dangerous bleed. Instead, they prescribe aspirin, especially to elderly patients, because they think it’s safer, but we now know this is wrong.”
Recent studies have shown aspi-rin can still cause bleeding while being far less effective than warfa-rin at preventing stroke.
The current guidelines set out by NICE are that aspirin can be used for AF patients when warfa-rin is ‘not appropriate’. GPs also still get paid if they give these patients aspirin.
Later this year, however, new NICE guidelines will alter this emphasis and instead call for patients to be given warfarin or a new range of medicines called novel oral anticoagulants (NOAC).
Patients on NOACs do not need regular blood tests and the medi-cation provides an alternative for those who do not fare well on warfarin.
Bradford’s success at reducing AF-related strokes by 11 per cent was achieved by encouraging GPs with a league table showing their results. “GPs are competitive and reviewed their AF patients, and many who were not on anticoagu-lants were switched. The results were astonishing,” says Greg Fell, a former consultant in public health at Bradford and Airedale Teaching Primary Care Trust, who worked on the programme.
But data from Oberoi Consulting show that, while the best ten per-forming clinical commissioning groups in England anticoagulate between 70 and 97 per cent of AF patients, this falls to between 55 and 58 per cent for the ten worst. The figures suggest the cost of stroke in AF patients, who could have been anticoagulated, is almost £200 million a year.
“Many doctors worry about the patient who bleeds to death on warfarin and no one thinks of the patient who never suffers a stroke because they are effectively treated. We have to change this view among doctors as it will save many, many lives,” says Mr Fell.
Share and discuss online at raconteur.net
STROKE IN THE UK
Strokes per year
People living with stroke
YORKSHIRE & HUMBER
10,600
112,330
NORTHWEST14,600
157,370
N. IRELAND4,000
32,000
EAST MIDLANDS
9,700
93,385
SOUTH WEST 12,500
120,408
SOUTHEAST
18,000
168,650
NORTH EAST 5,500
58,883
SCOTLAND12,500
120,000
WALES11,000
65,100
Source: Atrial Fibrillation Association/Anticoagulation Europe
THE REALITY OF STROKECOMPARING STROKE RATES IN EUROPE
Source: Stroke Association
Source: Stroke Association
Source: Stroke Association
Latvi
aPo
rtuga
lGr
eece
Czec
h Rep
ublic
Eston
iaHu
ngary
Slove
niaLit
huan
iaLu
xemb
ourg
Italy
Malta
Cypru
sPo
land
Finlan
dNo
rway
Germ
any
Irelan
dAu
stria UK
Swed
enDe
nmark
Icelan
dNe
therla
nds
Belgi
umSlo
vakia
Spain
Franc
eSw
itzerl
and
25,000
20,000
15,000
10,000
5,000
0
FINANCIAL IMPACT ON STROKE SURVIVORS AND THEIR FAMILIES
of 25-59 year olds are unable to return to work
report a decrease in household income
are living in fuel poverty
cut back on food
report an increase in household expenses
69% 65% 63% 40%58%
ESTIMATED COST OF STROKE
Productivity losses due to care, disability and death
Informal care costs
Total economic costs in the UK from a societal perspective
£9bn £4.38bn £2.42bn £1.33bn
EAST OF
ENGLAND11,300
118,526
WEST MIDLANDS
11,600
125,452
Direct NHS costs
LONDON13,500
128,175

1110
UNDERSTANDING STROKEBUSINESS RISK STRATEGIES
raconteur.net twitter: @raconteurraconteur.net twitter: @raconteurL.GB.03.2014.5714b Date of preparation: March 2014 020
Increased use of blood-thinning drugscan reduce strokes and save livesThousands of patients with the heart rhythm disorder atrial fi brillation could avoid strokes with access to the right treatments
Patients with atrial fi brillationshould always ask their doctor about the best treatment to reduce their risk of stroke. Dr Khalid Khan, consultant cardiologist at Wrexham Maelor Hospital, answers some common questions
the 1950s. It is cheap, effective and well understood by doctors. But warfarin and other, more recently introduced, anticoagulant medi-cines are not always used.
In August 2013, data from the Sentinel Stroke National Audit Pro-gramme showed only one in three of the patients with AF who had a stroke were on anticoagulants such as warfarin.
This may be because getting the dose of warfarin right is not a sim-ple process, and is complicated by the fact that it interacts with certain
One in five of the patients admit-ted to hospital with a stroke have a heart rhythm disorder known as atrial fi brillation or AF.
The condition means that blood can pool in the heart, causing clots to form. People with AF are at five to six times greater risk of having a stroke which can often be fatal.
Although it can affect anyone, AF is more common the older we get, affecting almost one in ten of the over-80s.
Overall, there are now more than one million people diagnosed with AF and many more who are thought to have it, but are unaware that they do.
By 2050, experts say these fi gures could double.
Trudie Lobban, founder and chief executive of the AF Association, says: “We know there are many people with AF who do not know they have it. In the first instance, detection can be as simple as a pulse check.
"If you have AF and are at risk of an AF-related stroke, it is imperative you are assessed and considered for anticoagulation medicine.
"We know that at least 7,100 AF-related strokes could be prevented every year if people with AF were appropriately treated.
"It is critical that greater aware-ness of AF and appropriate pre-scribing of effective therapies are NHS priorities – saving lives while also reducing cost to the NHS.”
The danger from AF occurs when the atria – the upper chambers in the heart – beat irregularly and the blood stagnates causing clots. When a clot forms, it can be pushed around the circulatory system and may get lodged in blood vessels in the brain, resulting in a stroke.
Fortunately, anticoagulants, often referred to as blood-thinning pills, can significantly reduce the risk of a stroke.
Warfarin, for example, is an anti-coagulant that has been used since
foods and alcohol.Careful monitoring is needed and
patients must go regularly to a spe-cial INR clinic to have a blood sam-ple taken that ensures their dosage is correct.
Worse still, many AF patients are not prescribed anticoagulation therapy at all and are instead given aspirin. This may increase their risk of a bleed while doing little to reduce stroke risk.
Eve Knight, chief executive and co-founder of the charity AntiCo-agulation Europe, says: “There are a large number of people diagnosed with AF, who are known to be at risk of stroke, but they are not receiving the anticoagulation they need, either because it isn’t offered to them or because it isn’t being used optimally.
“Results from our recent sur-vey showed that more than half of respondents would have liked to have been more involved in deci-sions about which anticoagulation therapy they use. We believe eve-ryone requiring anticoagulation should receive the medicine that is right for them and should be sup-ported to use it effectively.”
The good news is that major changes should soon alter how AF patients are treated.
Existing guidelines from the Euro-pean Society of Cardiology (ESC)
will be bolstered in the forthcoming updated guidelines from the UK’s National Institute for Health and Care Excellence (NICE) which makes clear that anticoagulation is key.
The NICE guidelines will also include another important change for patients.
Three medicines that mark a signif-icant innovation in anticoagulation for AF patients in more than half a cen-tury are now being recommended in the draft NICE guidelines, which will be finalised and published in June.
Known as novel oral anticoagu-lants or NOACs, these medicines provide a fixed dose without the need for anticoagulation monitoring and eliminate the need to visit an INR clinic. Three NOACs are available on the NHS and all of them are at least as good as warfarin in reducing the risk of a stroke in AF patients.
While the ESC guidelines make
clear that there is insufficient evi-dence to recommend one of these NOACs over another, they do point out that some patient characteris-tics, drug compliance, tolerability and cost may be important consid-erations in the choice of an agent.
In some parts of the UK, these more recently introduced medicines are already being embraced.
Craig Barr, a consultant cardiolo-gist at the Dudley Group NHS Foun-dation Trust, says: “When we looked at the options available and all of the data, we felt that novel anticoagu-lants, which don’t require constant blood tests, were the best option for the majority of our patients. We now have options in anticoagulation management, whereas three years ago we didn’t. This means patients and doctors alike now have choice so that factors, such as age, lifestyle and preferences, can be taken into
account when considering the treat-ment plan.”
Charities such as the Stroke Asso-ciation say they hope that the new guidelines for doctors, combined with a wider range of treatments, will lead to a reduction in strokes.
Joe Korner, director of external affairs at the Stroke Association, says: “We know that people with AF A large number of people
diagnosed with AF are known to be at risk of stroke, but they are not receiving the anticoagulation they
to them or because it isn’t being used optimally
Q&A
More recent evidence and international guidelines recognise that aspirin is much
The purpose of anticoagulation in AF is to reduce your chance of having a stroke. It achieves this by reducing the risk of clot for-mation in your heart that might then cause a stroke. We now have very good tools that can be used to estimate what your personal risk of having a stroke is. The calculation is based on known risk factors for stroke, including your age, sex and medical his-tory, notably diabetes, high blood pressure, heart disease or a his-tory of previous stroke. Based on these results, your doctor can advise you on whether you need anticoagulation and, if so, which approach is most suitable for you.
Warfarin has been used for many years and is certainly effective when used correctly. Its down-side is that it can be hard to get the dose right for some patients as warfarin’s action varies between individuals, and it can interact with certain foods and other medi-cations. For this reason, you may need to go for regular blood tests at a clinic. There are three alter-native anticoagulants to warfa-rin, called rivaroxaban, apixaban and dabigatran. These novel oral anticoagulants or NOACs are not affected by food or other drugs, so you do not need monitoring by regular blood tests. In terms of their ability to reduce your stroke risk, they are at least as good as warfarin, but some of the NOACs work differently to others. Your doctor can advise.
We have clear guidelines and measures that we can undertake to manage bleeding when it does occur, whatever a patient might be taking, including for the more recently introduced oral antico-agulants. The action of warfa-rin lasts for several days and an injection of vitamin K can reverse its effects, but this takes eight to twelve hours and is therefore not a true antidote (which reverses the effects immediately). Com-
pared with warfarin, the blood thinning effect of NOACs wears off much faster. It is reassuring that in all the studies with the more recently introduced oral antico-agulants, they had at least a com-parable safety profi le to warfarin in terms of overall bleeding rates.
Older guidelines from 2006 sug-gested that aspirin could be used in patients at low or medium risk of stroke. More recent evidence and international guidelines rec-ognise that aspirin is much less effective in preventing stroke in AF, and is no safer than an antico-agulant in terms of bleeding risk. Guidelines due to be published by NICE in June are expected to rec-ommend anticoagulation for all patients who are thought to be at risk of stroke from AF.
As you get older, both your chance of having AF and your chance of having a stroke increase signifi-cantly. Older patients also have a somewhat higher bleeding risk with anticoagulation. However, overall, older patients are more likely to benefit from receiving anticoagulation when compared to younger patients. The risks and benefits of treatment should be considered for every individual to ensure the anticoagulation they receive is appropriate for them. Your own doctor, with knowledge of your medical history, is in the best position to advise you of the most appropriate treatment.
are five times more likely to have a stroke and that it’s linked to around 22,500 strokes in the UK each year. That’s why it’s vital that people with AF get the right treatment as soon as possible. If the underlying conditions of stroke, such as AF, are picked up at an early stage and people get the right treatment, they can reduce their risk of stroke which will save lives.”
This commercial feature was developed and supported by Bayer HealthCare
www.anticoagulationeurope.org020 8289 6875 The Heart Rhythm Charity
www.heartrhythmcharity.org.uk
Date of preparation: March 2014L.GB.03.2014.5714b

13raconteur.net twitter: @raconteur12 raconteur.net twitter: @raconteur
UNDERSTANDING STROKEUNDERSTANDING STROKE
REHABILITATION
Ȗ Hollywood blockbusters pro-vide the world with popcorn-fuelled escapism. One of the great-est leaps forward for the movie industry in recent times has been computer animation.
Now researchers have begun to use the same techniques used to create the “human” move-ments of Gollum in The Lord of the Rings trilogy and Na’vi from Avatar to form better treatments for stroke patients.
The effort is among the most inno-vative uses of cutting-edge technol-ogy to treat stroke victims, which have emerged from a new and bet-ter understanding of how the brain can develop following a stroke.
The project to use modern film-making techniques in stroke treat-ment comes from the University of Gothenburg in Sweden, where researchers are using motion capture technology, similar to
that used to convert actors’ move-ments into computer animation, to analyse the movements of stroke patients.
Margit Alt Murphy and her team at the university’s Sahlgrenska Academy have devised techniques to translate the movements of stroke patients into 3D animations to give them extra layers of detail about their mobility that doctors and physiotherapists are unable to notice with the naked eye.
“Computer technology provides better and more objective docu-mentation of the problem, in terms of the everyday life of the patient, than human observation can pro-vide,” says Ms Alt Murphy.
“With 3D technology, we can measure a patient’s movements in numbers, which means that small changes in the motion pattern can be detected and fed back to the patient in a clear manner.”
In a study, subjects were equipped with small, round balls on their arm, trunk and head and told to drink water from a glass. That action was filmed using high-speed cameras and infrared light reflected by the balls sent to a computer. The data was then used to build a 3D-animated image in the form of a stick figure.
“With 3D animation, we can measure the joint angle, speed and smoothness of the arm motion, as well as which compensat-ing motion pat-terns the
stroke patient is using. This gives us a measurement for the motion that we can compare with an optimal arm motion in a healthy person,” says Ms Alt Murphy.
But why is it important to detect, in such minute detail, what issues have been caused to a person’s movement during a stroke? The answer lies in the modern under-standing of what happens to the brain following a stroke and how it is possible that it can “rewire” itself over time.
Experts say you can view the brain as a set of circuits that con-trol thinking, movement, emotion and behaviour. During a stroke, blood and the oxygen it carries suddenly fails to reach areas of the brain, leading to the destruction of millions of cells. The damage can include paralysis, speech and visual problems as well as cognitive issues.
According to Thomas Carmi-chael, a neurologist at the Uni-versity of California, Los Angeles, who has written papers on how the brain can rewire, the circuits nearest the area damaged by the stroke naturally form new con-nections with other areas of the brain. This means it is possible to train other brain centres to take over the functions that used to be controlled by parts that have died
or been damaged during a stroke. “What is happening is the brain
is remapping and reorganising itself, and that is where recovery is occurring,” says Dr Carmichael.
Madina Kara, a neuroscientist at the Stroke Association, says the underlying reasons for this recov-ery remain uncertain. But what is clear is that people can relearn actions, training a different part of the brain to do something they were capable of before a stroke.
“People are recognising that the brain
is ‘plas-
tic’ or that it has a plasticity that means it has the ability to rewire itself,” says Dr Kara. “In order to do this it needs to receive that mes-sage. Like any learning, repetition of the message is key.”
This understanding has trans-formed treatment. In the past, victims were taught coping strat-egies, such as how to tie a shoe with one hand or operate a long-handled “reacher”.
But new technologies, such as virtual reality, are now opening up pathways to better treatment and recovery in place of labour-inten-sive therapies that are becoming harder to fund.
Researchers at the University of Illinois have taken patients into an Alice in Wonderland world thanks to a headset and electronic glove. Patients, who struggle to move an arm and grip objects, can get a therapeutic work out by “attend-ing” the Mad Hatter’s Tea Party and pouring him a cup of tea,
responding to the cartoon action on screen. Researchers believe it beats other therapies, such as moving objects from one box to another, because patients are less likely to get bored.
Teleconferencing, a fundamental element of e-health, is offering patients and doctors an easier way to conduct therapy sessions.
Last month, researchers at the National University of Singapore (NUS) showed off a “tele-reha-bilitation system” which is made up three elements. First, a screen allows you to chat to a therapist over a video link on the internet, much like Skype. Second, doctors
can check on a person’s move-ment remotely thanks
to a series of sensors placed on the body
which feedback to the surgery so
therapy pro-gress can be assessed.
Finally, instruc-tions can be
relayed via an app that works on a tablet, such as an iPad.
It means that therapists can help patients without the sometimes difficult logistics and cost of travel-ling to and from clinics.
“Our approach makes use of affordable, wireless, lightweight motion sensors to guide the patient whenever they are doing their exercises,” says Yen Shih Cheng, assistant professor at the NUS Department of Electri-cal and Computer Engineering. “Video recordings of the patient performing the exercises are also saved for visual review later by therapists.
“The sensors produce metrics that can provide the therapist with a quick assessment of how many repetitions the patient has performed and which exercises the patient is performing correctly. The system also flags exercises that the patient may be perform-ing incorrectly, which the thera-pists will be able to verify through video review.”
Understanding the granular detail of how a stroke affects a patient allows a powerful fusion of therapy and technology to create better, personalised treatments that can be vital in achieving more effective rehabilitation.
MOVIE TECHIS HELPINGPATIENTSScientists have discovered that the brain can “rewire” itself after stroke damage and are devising fun forms of rehabilitation, as Murad Ahmed reports
OUR TOP FOURINNOVATIONS
Tabletsand pills
Page 14
Share and discuss online at raconteur.net
The brain’s ability to reprogramme itself, known as neural plasticity, is being applied to help stroke patients recover lost movement in limbs using the latest technological advances. Murad Ahmed showcases four of the most promising developments which offer the prospect of a brighter future for those in stroke rehabilitation
RESEARCH
NEURAL IMAGING
Israeli company Neurokeeper has developed a portable stroke-detecting device that is worn on the patient’s head to read brain waves and identify discrepancies picked up by its electrodes. It can be deployed as an early-warning system in at-risk patients, giving doctors real-time information to spot and treat patients before a stroke takes hold.The startup company believes the device can be used at home, allowing sufferers to notice the signs in an approaching stroke and seek emergency medical assistance.
BRAINWAVE-READING HEADSET
The University of Wisconsin School of Medicine and Public Health has created a machine that can “read” a person’s thoughts to “shock” and stimulate paralysed limbs into action. Researchers demonstrated that a special skullcap with electrodes could translate brainwaves into electrical impulses that help activate the nerves in a stroke victim’s limbs. Its aim is to help the brain recover the neural connections that drive movement. Similar products are available, including the SaeboFlex Functional Arm Training System, the Myomo and InMotion robotic systems.
ELECTRICAL STIMULATION
It looks like a Star Trek prop, but a new arm shell fitted with metallic sensors is stimulating improved function for everyday movements. The Bioness H200 wireless hand system effectively provides a bionic arm. A wireless system delivers low-level impulses that activate the nerves which control the muscles in the hand and forearm to restore functions, such as grasping, pinching and holding. Its lightweight shell gives support so the arm can carry out repetitive actions that make it easier to recover functions.
ROBOTIC ARM
Recent advances, such as transcranial magnetic stimulation, which use magnetic fields to stimulate brain cells to assist brain-mapping, can help with better diagnosis of stroke sufferers. The Oculus Rift virtual reality headset, an immersive computer games system bought by Facebook, could help clinicians detect brain patterns following research unveiled at this year’s SXSW (South by Southwest) Festival in Austin, Texas. A team of bio-engineering and neurology graduate students have already devised six games to aid stroke rehabilitation.
“Eagle Wood Neurological Care Centre exemplifies quality in the care sector.” Sir Tony Robinson
Eagle Wood is an award winning, purpose built residential care centre in Peterborough. It has five neurological care units.
Each unit provides a distinct care model catering for different aspects of neurological nursing needs; including long term neurological conditions, neuro-rehabilitation for people with acquired brain injuries (including strokes), frontal temporal dementias, learning disabilities and complex care.
Its exceptional and well thought out facilities include large ensuite bedrooms, a hydrotherapy pool, a skills kitchen, therapy room, gym and a complimentary coffee bar for residents and their families.
Please contact us on: 0330 20 20 305 or email: [email protected]
Compassion. Commitment. Care.PJ Care Limited | 0330 20 20 305 | www.pjcare.co.uk

UNDERSTANDING STROKE UNDERSTANDING STROKE
15raconteur.net twitter: @raconteur14 raconteur.net twitter: @raconteur
Acute care of stroke victims is much improved, but less progress has been made in rehabilitation, says national clinical director for stroke Professor Tony Rudd
Smartphones, tablets and games consoles are being used to harness technology for stroke recovery at home, writes Murad Ahmed
DIAGNOSIS OF DOINGMORE WITH LESS?
TABLETS, NOT JUSTPILLS, AID RECOVERY
Ȗ Stroke care has improved dramatically since I was first appointed as a consultant 26 years ago. A patient admitted then would have been looked after on a general medical or geriatric ward. Very lit-tle would have happened as no one really believed there was anything you could usefully do that would make much difference.
If the person was lucky, they would have received some reha-bilitation from the geriatric team while in hospital, but the chances of getting any rehabilitation after get-ting home would have been slight. Better than in earlier days though when treatments advocated for stroke or apoplexy, as it was called then, included stimulating enemas or vomits and blood-letting.
The most important develop-ment in stroke care was the dem-onstration about 20 years ago that managing patients on a specialist stroke unit saved lives and resulted in people having less long-term disability compared to manage-ment on a non-specialist ward.
This led to the government setting a target that by 2004 all hospitals treating stroke patients should have a stroke unit. This was achieved and at the same time it became possible for doctors, nurses and therapists to train as stroke specialists.
The Royal College of Physicians has been auditing the quality of stroke care since 1998 and has shown steady improvements.
Data on all people admitted to hospital because of stroke has been collected documenting how quickly they arrive in hospital, whether they receive clot-busting treatment (thrombolysis) and, if so, how quickly it is delivered, as delays result in the treatment being less effective.
In addition, the data shows how soon patients get to the stroke unit and are seen, start treatment from therapists and how much therapy they receive each day. The quality and quantity of care once they are discharged into the community are also collected together with measures of the effectiveness of the care.
Having to report the anonymised data, which is then made public, enabling professionals and lay people to scrutinise how their local health services are performing, is a powerful tool to encourage improvements in services.
There is, however, still a great deal to do to ensure that all patients with stroke, regardless of where they live or what day or time they become ill, can be certain they receive the highest quality of care possible.
In London the organisation of stroke care was radically changed about four years ago. Until then, 32 hospitals in the capital were offering acute stroke care, and we knew from the national stroke audit that the quality provided varied dramatically from some of
Ȗ It is accepted that targeted, intensive and personalised therapy can make an enormous difference in a stroke victim’s recovery. But how do we connect patients with effective treatments in a landscape of dwindling resources?
The answer is increasingly being supplied by smartphones, tablets and games consoles. The technology is allowing many patients to take charge of their own recovery and access a therapy stream at home.
Technology will be a major focus at the European Stroke Confer-ence in Nice, from May 6 to 9, when the latest developments in stroke therapy will be on the agenda. Limbs Alive, a boundary-chal-lenging tech company spun out of the University of Newcastle, has created a suite of games, designed to help return motor functions to a patient’s arms, that can be played on tablets and PCs.
One title, Circus Challenge, encourages players to move their arms up and down, and from left to right, to control the actions of entertainers such as jugglers or clowns who need to keep balls in the air or plates spinning. These movements, while the mind is concentrating on the images on screen, improve limb function.
With 70 per cent of stroke sur-vivors experiencing impaired arm movement, the games are an engaging way to get the repeti-tive movements that are so vital to recovery.
“One of the benefits of rehabili-tation through technology is that you can make things more fun, more interactive,” says Dr Madina Kara, a neuroscientist at the Stroke Association. “Patients may not see that as rehab, but actually a game. You may only have access to physiotherapists once a week. Technology allows you to get that extra therapy.”
Home-gaming devices can pro-vide more bespoke therapy. Devel-opment of motion-sensitive games consoles, such as Nintendo’s Wii and Microsoft’s Kinect system for the Xbox, which operate by track-ing a person’s body movements, has helped create new opportu-
nities for stroke sufferers.
The Able-X sys-tem, which has a special handset that can be plugged into a games machine, is designed for patients with more severe paralysis. It allows them to use their stronger arm to co-ordinate movements from the affected side of the body.
Roke, a British company working in conjunction with the Univer-sity of Southampton, has created another potentially potent gam-ing system that uses the Kinect device to track the movements of individual fingers.
Patients follow an exercise rou-tine as directed through a televi-sion screen and the Kinect sensor measures the hand joint, angles and the dexterity of fingers. This allows therapists to monitor the progress of patients and fine tune the hand and finger movements that may have been affected by a stroke. The project is now creating a series of computer games to bring an aspect of fun into stroke rehabilitation.
The Stroke Association has also harnessed game technology to develop CogWatch for patients with apraxia, the motor planning condition that makes it difficult to carry out everyday tasks in the correct sequence.
With ingenious adaptation of the Kinect motion tracking system, it recognises objects, such as a mug or kettle, and determines if the
stroke patient has made an error – forgetting to boil the water, for example, while making a cup of tea – before prompting them to take the correct course of action.
Games can also aid stroke pre-vention by educating family mem-bers about relatives who may be at risk of stroke. In the United States, researchers from Columbia University have produced a video game called Stroke Hero, aimed at teaching young children to recognise the physical symptoms of a stroke.
In a study, published in the jour-nal Stroke in February, a group of nine to ten year olds, who played the game for just 15 minutes, were 30 per cent more likely to recognise when a person was having a stroke.
There are also apps to help suf-ferers with other issues stemming from strokes. Many are available for aphasia sufferers, where victims suffer problems with their speech.
Apps such as SmallTalk, Easy Speak and Talk Assist, which are available for Apple’s iPhone and iPad, are text-to-talk systems. Users can tap a number of words or simple photographs and the device “speaks” for them. Small icons can be touched on screen, representing a range of useful phrases.
Development of motion-sensitive games consoles, which operate by tracking a person’s body movements, has helped create new opportunities for stroke sufferers
If we took the measures necessary to cut salt intake, reduce obesity, cut smoking rates and alcohol consumption, we would need far fewer stroke physicians
the best care available anywhere in the world to care that was at best ineffective and at worst actually causing harm.
The decision was made to cen-tralise all the care that patients needed in the first two or three days after the stroke in just eight units, and to ensure that there were always well-trained and ade-quate numbers of staff available in these centres with access to all the equipment needed to investigate patients rapidly.
An additional tariff was paid to the hospitals for each patient treated to cover the increased costs of care, but only if the regular inspections carried out by the Lon-don clinical director and the com-missioners deemed the required standards were being met.
If the patient still required in-patient care after the first 72 hours, they were transferred to their local stroke unit that also had to meet high standards of care requiring additional nurses and therapists to deliver them. More than 400 additional nurses and 100 thera-pists were recruited in London to deliver the new model.
It has been very successful with the outcomes of patients improv-ing significantly in terms of reduced mortality and disability as well as shorter lengths of stay and fewer people needing to go into long-term nursing-home care. Despite an increased initial cost of care to the health service, when longer-term savings are taken into account, it is resulting in millions of pounds of savings to taxpayers.
As the national clinical director, I am determined to make sure that where possible similar standards of care are provided in the rest of the country. Plans are already being developed in some other urban areas. Manchester recon-figured their care at the same time as London and is currently making some further changes. Parts of the East and West Midlands are closely examining their services and are likely to make changes within the next year or two.
The London model would not be appropriate for rural areas where the population density is low and travel times to the local hospital long. Here many hospitals are either already using or are plan-ning to implement telemedicine enabling the specialist stroke physician to see the patient being examined at the local hospital, talk to them and review their brain scans to provide advice about management.
Not everyone with a stroke is suitable for clot-busting treat-ment, probably only about 20 per cent, because there are many situ-ations where it can be more likely to cause harm than do good.
In England, Wales and Northern Ireland, we are currently managing to treat about 12 per cent of stroke admissions. This is better than most other high-income countries and the figure is rising each year.
So the picture for acute care is getting much better. The same rate of progress is not being seen in rehabilitation. There are still many parts of the country where there are no specialist early supported
discharge teams to continue care once people leave hospital. There are often long waits to continue rehabilitation after leaving hos-pital and patients are often dis-charged from therapy far too early in the misguided belief that there is little likelihood of further recovery after the first three to six months.
Access to psychological treat-ments is extremely poor despite up to 50 per cent of stroke patients suffering depression and about 30 per cent having significant cogni-tive problems.
We have to accept that major investment in new services is unlikely at the present time in the health service. We are going to struggle to maintain the invest-ment that we currently have. But there are things that we can do to use the money that we currently have more effectively.
People are staying in hospital too long at huge expense because of the lack of community ser-vices or because of delays in providing services.
Separation of the budgets of health, social care, housing and employment has led to the nonsen-sical situation where it is difficult to spend more on effective health care that will save large amounts of money on providing social care or enabling people to get back to employment, paying taxes and supporting their families.
And about 70 per cent of all strokes are preventable. If as a country we took the measures necessary to cut salt intake, reduce obesity, cut smoking rates and alcohol consumption, we would need far fewer stroke physicians.
Stroke is an awful disease. Many cases could be prevented and there is effective treatment. There is still much that we need to learn and we must support the work of organisa-tions such as the Stroke Associa-tion so there can be more research to answer the many unknowns and help provide the additional sup-port the health service currently cannot or will not provide.
MOBILE TECHNOLOGY OPINION
11 theraconteur.co.uk twitter.com/raconteurmedia
FUTURE OF PAYMENT
New technologyto improve stroke diagnosis
With this software, ASPECTS can realise its potential to revolutionise stroke care
e-ASPECTS will standardise the interpretation of stroke CT scans to increase signifi cantly the uptake of stroke treatments
The majority of the 16 million peo-ple worldwide who have a stroke every year suffer long-term disability or death unless they are diagnosed and treated in time. This number is expected to more than double world-wide by 2030. But up to half of patients who could be treated are not.
Most strokes are ischaemic – a result of a blocked artery preventing oxygen reaching brain cells. Treat-ment with either clot-busting drugs (thrombolysis) or mechanical clot-removal devices can re-establish blood flow to the brain and limit oth-erwise fatal or permanent damage. Treatment is only effective when administered within six hours after the stroke. A 2014 study in the jour-nal Stroke found every 15-minute delay in giving thrombolysis adds one month of disability to a patient’s life.
Critically, treatment can only be given following expert assessment of a patient’s brain CT scan and detect-ing ischaemic damage is challeng-ing. Fortunately, a solution is on the horizon. The medical imaging soft-ware e-ASPECTS, from Brainomix, is expected to improve this dramatically.
The Alberta Stroke Programme Early CT Score or ASPECTS score is a clinically validated way of assess-ing the extent of stroke damage using brain CT scans. It is a strong predictor of patient outcome and can be used to help identify patients who are likely to suffer a haem-orrhage as a result of treatment.
Currently, the use of ASPECTS in routine clinical practice is lim-ited because it requires extensive expertise and there is variability between experts.
Inventor of ASPECTS Professor Alastair Buchan is co-founder of Brainomix, a University of Oxford startup company that has been developing e-ASPECTS. This is the fi rst imaging software to automati-cally assess and quantify ischaemic brain damage on CT scans of acute stroke patients, by applying the ASPECTS method.
The e-ASPECTS software fully integrates with existing clinical infra-structure, and provides a reliable and standardised interpretation of a patient’s CT scan. By equipping clini-cians with this additional expertise, e-ASPECTS is expected to increase the uptake of existing stroke treat-ments, improving the likelihood that a patient has a good outcome.
Professor Buchan, professor of stroke medicine and dean of medicine at the University of Oxford, says: “With this software, ASPECTS can realise its potential to revolutionise stroke care.”
Further feedback from clinicians is important to Brainomix in the run-up to CE marking in early-2015. Clinicians are invited to see a demo of e-ASPECTS, fi nd out more and give feedback at www.brainomix.com
M1
M2
Lentiform
Insula
M4
M5ASPECTS SCORE
LEFT REGIONS DAMAGEDR RL L
11 theraconteur.co.uk twitter.com/raconteurmedia
FUTURE OF PAYMENT
New technologyto improve stroke diagnosis
With this software, ASPECTS can realise its potential to revolutionise stroke care
e-ASPECTS will standardise the interpretation of stroke CT scans to increase signifi cantly the uptake of stroke treatments
The majority of the 16 million peo-ple worldwide who have a stroke every year suffer long-term disability or death unless they are diagnosed and treated in time. This number is expected to more than double world-wide by 2030. But up to half of patients who could be treated are not.
Most strokes are ischaemic – a result of a blocked artery preventing oxygen reaching brain cells. Treat-ment with either clot-busting drugs (thrombolysis) or mechanical clot-removal devices can re-establish blood flow to the brain and limit oth-erwise fatal or permanent damage. Treatment is only effective when administered within six hours after the stroke. A 2014 study in the jour-nal Stroke found every 15-minute delay in giving thrombolysis adds one month of disability to a patient’s life.
Critically, treatment can only be given following expert assessment of a patient’s brain CT scan and detect-ing ischaemic damage is challeng-ing. Fortunately, a solution is on the horizon. The medical imaging soft-ware e-ASPECTS, from Brainomix, is expected to improve this dramatically.
The Alberta Stroke Programme Early CT Score or ASPECTS score is a clinically validated way of assess-ing the extent of stroke damage using brain CT scans. It is a strong predictor of patient outcome and can be used to help identify patients who are likely to suffer a haem-orrhage as a result of treatment.
Currently, the use of ASPECTS in routine clinical practice is lim-ited because it requires extensive expertise and there is variability between experts.
Inventor of ASPECTS Professor Alastair Buchan is co-founder of Brainomix, a University of Oxford startup company that has been developing e-ASPECTS. This is the fi rst imaging software to automati-cally assess and quantify ischaemic brain damage on CT scans of acute stroke patients, by applying the ASPECTS method.
The e-ASPECTS software fully integrates with existing clinical infra-structure, and provides a reliable and standardised interpretation of a patient’s CT scan. By equipping clini-cians with this additional expertise, e-ASPECTS is expected to increase the uptake of existing stroke treat-ments, improving the likelihood that a patient has a good outcome.
Professor Buchan, professor of stroke medicine and dean of medicine at the University of Oxford, says: “With this software, ASPECTS can realise its potential to revolutionise stroke care.”
Further feedback from clinicians is important to Brainomix in the run-up to CE marking in early-2015. Clinicians are invited to see a demo of e-ASPECTS, fi nd out more and give feedback at www.brainomix.com
M1
M2
Lentiform
Insula
M4
M5ASPECTS SCORE
LEFT REGIONS DAMAGEDR RL L

Specialist Neurological Occupational Therapy and Interactive Metronome from Krysalis ConsultancyStroke should not mean that you lose yourself. Interactive Metronome is a research-based training program that helps individuals overcome attention, memory, speech and physical limitations. Occupational Therapists are skilled professionals who aim to promote independence and wellbeing aft er illness or injury. Interactive Metronome integrated alongside specialist rehabilitation will maximise recovery. Visit our website www.krysalisconsultancy.co.uk to fi nd out more about stroke survivor Gill Carter and her experience of using Interactive Metronome 5 years aft er her stroke. ‘I can’t go back but I can go forward’ via Interactive Metronome link. Krysalis Consultancy is the number one independent specialist Neurological Occupational Therapy rehabilitation provider in the UK. Our service is evidence based and aff ordable for all. For more information on how Interactive Metronome and Occupational Therapy can benefi t you, or to speak to our locally based professional please call 01373 837263 or email off [email protected]
" I want to use my arm…have a better memory... join in the
conversation…be more independent
and walk confi dently "
What are your personal goals?