combined hamartoma of the retina and retinal pigment epithelium with hypo-autofluorescence and...
TRANSCRIPT

CLINICAL PICTURE
Combined hamartoma of the retina and retinal pigment epithelium withhypo-autofluorescence and cystic degeneration at the macula
Clin Exp Optom 2014; 97: 475–476 DOI:10.1111/cxo.12164
Tarjani V Dave* DNBVivek Dave† MD FRCS DNBRajeev R Pappuru§ MS*Ocular Oncology, Orbit and Facial AestheticSurgery, Netra Mandir Eye Institute, Mumbai, India† Netra Mandir Eye Institute, Mumbai, India§ Smt. Kanuri Santhamma Center for Vitreo RetinalDiseases, LV Prasad Eye Institute, Hyderabad, IndiaE-mail: [email protected]
Submitted: 7 February 2014Revised: 28 February 2014Accepted for publication: 17 March 2014
Combined hamartoma of the retina andretinal pigment epithelium is a congenitalnon-hereditary benign retinal tumour ofunknown aetiology possibly due to translo-cation between the short arms of chromo-somes 11 and 18.1 It usually presents as agreyish ill-defined mass over the posteriorpole. Characteristic location is near orover the optic disc. Secondary intraretinalchanges with a combined hamartoma arevery unusual. In this case report, we describeintraretinal degenerative changes in a com-bined hamartoma and its features onautofluorescence imaging.
CASE HISTORY
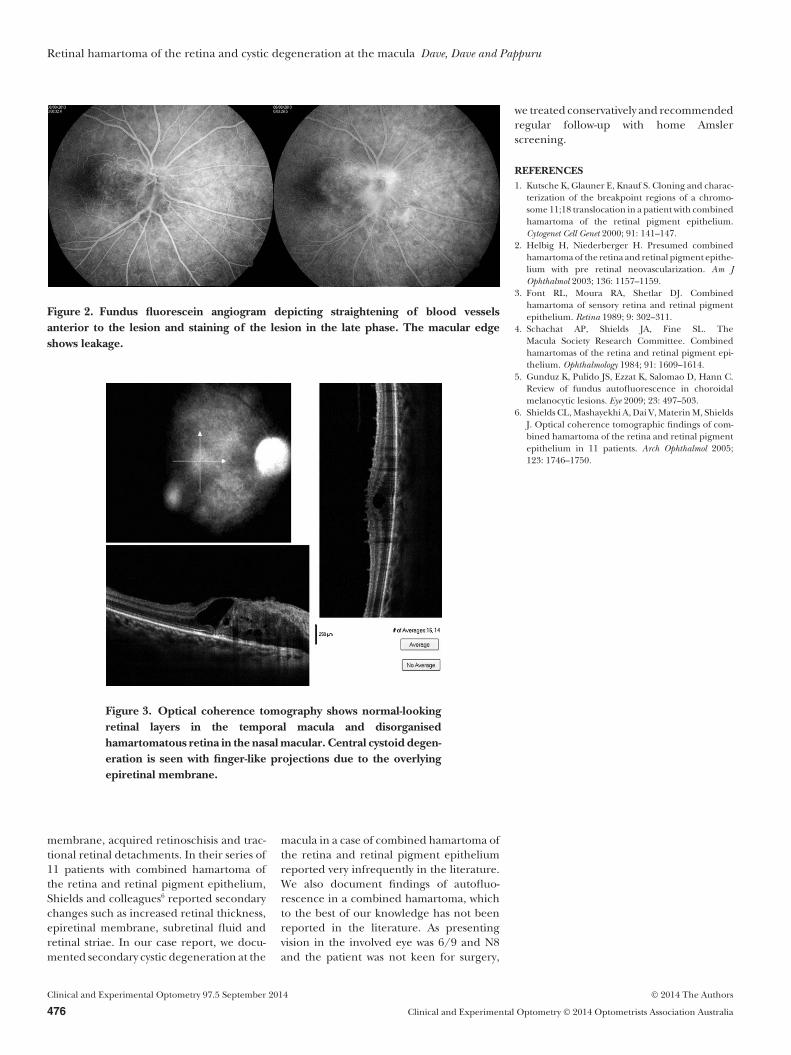
A 40-year-old woman presented with asudden loss of vision in the right eye noted.Visual loss was incidentally noted and wasnot associated with any other complaints.Vision was R 6/9 and L 6/6. Near vision wasR N8 and L N6. Left eye appeared withinnormal limits. Right eye showed a peri-papillary greyish translucent membranewith underlying straightening of bloodvessels (Figure 1). Fundus camera auto-fluorescence examination showed hypo-autofluorescence over the entire lesion(Figure 1). Fundus fluorescein angiographyshowed mild hyper-fluorescence over thelesion with late leakage and staining andtortuosity of the peri-papillary blood vessels
with straightening anteriorly (Figure 2).Optical coherence tomography (OCT)showed partial posterior vitreous detach-ment with attachment at the disc. Tempo-rally, OCT in the right eye showed normalretinal architecture. Nasal to the fovea,retinal thickening was noted with disorgani-sation of the retinal layers. Multiple cysticspaces with cystoid degeneration were seennasally. An epiretinal membrane was notedon the surface of the retina (Figure 3).
DISCUSSION
The mass causes abnormal tortuosity of theretinal blood vessels with a characteristicstraightening anterior to the lesion towardthe peripheral fundus. Most cases presentin childhood with strabismus and/or poorvision. An adult presentation as in thepresent case may be due to either a delayedaffection of the fovea by the epiretinal mem-brane enlargement or contracture or due toan incidental observation by the patient.Many may have amblyopia due to macularinvolvement causing macular drag. Theremay be associated peripheral retinal ischae-mia with retinal neovascularisation.2 Patho-
logically, the combined hamartoma is anadmixture of pigment epithelial cells, prolif-erating blood vessels and glial tissue.3
Epiretinal membrane formation is a promi-nent feature of a combined hamartoma.4
Although unlikely, diagnoses of a mela-nocytic tumour such as a melanomais possible due to stippled leakage onangiogram and hypo-autofluorescence.Unlike choroidal melanocytic lesions, whichhave either a patchy or a diffuse hypo-autofluorescence with indistinct borders,5
the present case demonstrates a uniformlydiffuse hypo-autofluorescence with distinctborders delineating the extent of the surfaceepiretinal membrane. Surgically peeling ofthe epiretinal membrane is controversialas improvement in vision is likely to belimited due to the disorganised underlyingretina. Other treatment options such asradiation therapy and tumour excision haveno role as the tumour is neither radiosensi-tive nor amenable to excision, as it diffuselyinvolves the retinal tissue. In cases withacceptable vision, patients can be managedconservatively with a close follow-up toobserve secondary changes such as intra-retinal haemorrhage, choroidal neovascular
Figure 1. Colour fundus photograph showing peripapillary epiretinal membrane withretinal traction and hypo-autofluorescence over the lesion.
C L I N I C A L A N D E X P E R I M E N T A L
OPTOMETRY
© 2014 The Authors Clinical and Experimental Optometry 97.5 September 2014
Clinical and Experimental Optometry © 2014 Optometrists Association Australia 475
membrane, acquired retinoschisis and trac-tional retinal detachments. In their series of11 patients with combined hamartoma ofthe retina and retinal pigment epithelium,Shields and colleagues6 reported secondarychanges such as increased retinal thickness,epiretinal membrane, subretinal fluid andretinal striae. In our case report, we docu-mented secondary cystic degeneration at the
macula in a case of combined hamartoma ofthe retina and retinal pigment epitheliumreported very infrequently in the literature.We also document findings of autofluo-rescence in a combined hamartoma, whichto the best of our knowledge has not beenreported in the literature. As presentingvision in the involved eye was 6/9 and N8and the patient was not keen for surgery,
we treated conservatively and recommendedregular follow-up with home Amslerscreening.
REFERENCES1. Kutsche K, Glauner E, Knauf S. Cloning and charac-
terization of the breakpoint regions of a chromo-some 11;18 translocation in a patient with combinedhamartoma of the retinal pigment epithelium.Cytogenet Cell Genet 2000; 91: 141–147.
2. Helbig H, Niederberger H. Presumed combinedhamartoma of the retina and retinal pigment epithe-lium with pre retinal neovascularization. Am JOphthalmol 2003; 136: 1157–1159.
3. Font RL, Moura RA, Shetlar DJ. Combinedhamartoma of sensory retina and retinal pigmentepithelium. Retina 1989; 9: 302–311.
4. Schachat AP, Shields JA, Fine SL. TheMacula Society Research Committee. Combinedhamartomas of the retina and retinal pigment epi-thelium. Ophthalmology 1984; 91: 1609–1614.
5. Gunduz K, Pulido JS, Ezzat K, Salomao D, Hann C.Review of fundus autofluorescence in choroidalmelanocytic lesions. Eye 2009; 23: 497–503.
6. Shields CL, Mashayekhi A, Dai V, Materin M, ShieldsJ. Optical coherence tomographic findings of com-bined hamartoma of the retina and retinal pigmentepithelium in 11 patients. Arch Ophthalmol 2005;123: 1746–1750.
Figure 2. Fundus fluorescein angiogram depicting straightening of blood vesselsanterior to the lesion and staining of the lesion in the late phase. The macular edgeshows leakage.
Figure 3. Optical coherence tomography shows normal-lookingretinal layers in the temporal macula and disorganisedhamartomatous retina in the nasal macular. Central cystoid degen-eration is seen with finger-like projections due to the overlyingepiretinal membrane.
Retinal hamartoma of the retina and cystic degeneration at the macula Dave, Dave and Pappuru
Clinical and Experimental Optometry 97.5 September 2014 © 2014 The Authors
476 Clinical and Experimental Optometry © 2014 Optometrists Association Australia