columbia dental review
TRANSCRIPT

Columbia Dental Review
Volume 14 | 2009-2010

©2010ColumbiaDentalReview
Aim and Scope
TheColumbiaDentalReview(CDR)isanannualpublicationofColumbiaUniversityCollegeofDentalMedicine(CDM).Thisjournal isintendedtobeaclinicalpublication,featur-ingcasepresentationssupportedbysubstantialreviewsoftherelevant literature. It isapeer-reviewed journal,editedbythestudentsoftheschool.Theeditorsareselectedonthebasisofdemonstratedclinicalscholarship.AuthorsareprimarilyCDMstudentsfrompre-doctoralandpostdoctoralprograms,CDMfacultyandresidents,andattendingsfromaffiliated hospitals. Peer reviewers are selected primarilyfrom theCDM faculty. Instructions forauthorswishing tosubmitarticlesforfutureeditionsoftheCDRcanbefoundonthelastpageofthisjournal.OpinionsexpressedbytheauthorsdonotnecessarilyrepresentthepoliciesoftheCo-lumbiaUniversityCollegeofDentalMedicine.
Editors’ Note
DearReaders,
TheColumbiaDentalReviewwascreatedtogiveColum-biadentalstudentsavoiceincurrentdentalresearch.Tothis end,our authors, in collaborationwith faculty, haveresearchedawidearrayoftopicscoveringmanydifferentfacetsofclinicaldentistry.
It is with continual research that our profession is able toprogress. Thispublicationcontinues to stay committed tocontributingtoourfieldbyaddressingandhighlightingsomeofthemostinterestingcurrenttopicsinclinicaldentistry.
Onbehalfofall theeditorsandassistanteditors, IwouldliketothankDr.LettyMoss-Salentijnwhoseguidancehasensuredthispublicationcontinuestoserveourdentalcom-munityyearafteryear.Iwouldalsoliketothanktheauthors,facultyreviewers,editors,andgraphicdesignerforalltheirefforts.Withouttheircontributions,thisfourteenthvolumeoftheCDRwouldnothavebeenpossible.
Sincerely,
NicoleMadisonLambert‘10
Editorial Board
Editor-in-ChiefNicoleMadisonLambert‘10
EditorsRayCheng‘10Nhu-UyenCung‘10WhitneyFlorin‘10ZiWang‘10
Assistant Editors JacquelineHaker‘11RenataKhelemsky‘11GloriaLee‘11LaurenMidthun‘11StevenNadler‘11ReneeReynolds‘11RupaliShah‘11ViolettaVayner‘11AndyWan‘11
Design and LayoutRichardV.Miller
Faculty ReviewersMartinJ.Davis,DDSSidneyB.Eisig,DDSJamesB.Fine,DMDLouisMandel,DDSJosephM.McManusJr,DMD,MBAElizabethPhilipone,DMDCleberP.Silva,DDSLettyMoss-Salentijn,DDS,PhDGeorgeS.White,DDSDanaL.Wolf,DMD,MSCandiceB.Zemnick,DMD,MPH,MS
Columbia Dental Review 2009-2010

©2010ColumbiaDentalReview
Table of Contents
DentalDefectsConnected 8withChemoradiotherapy:ACaseReportAimee Leibowitz, Sue Hwang, DMD, Richard Yoon, DDS, Steven Chussid, DDS
MisdiagnosisofGingivalSquamous 12CellCarcinomaPresentingasaPeriodontalLesionoftheAnteriorPalateMona Daneshi, Simon Beylin DDS, Candice Zemnick DMD, MPH, MS, Karin Emde DDS
MaxillarySinusitisDuetoApicalRarefyingOsteitis 16Rupali Shah, Violetta Vayner, Steven R. Singer, DDS
IdiopathicExternalRootResorption: 20ACaseStudyChristopher Hsia, Andrew Han DMD
RamsayHuntSyndromepresenting 24asTMD:ACaseReportNicholas Andros, Edward Rudolph, Jennifer Bassiur DDS
VACTERLAssociation:ADentalCaseStudy 27Jennifer L. Wilbur, Sue Hwang, DMD, Richard Yoon, DDS, Steven Chussid, DDS
ChinBlockBoneGraftinPatientCongenitally 30MissingMaxillaryLateralIncisorsPriortoImplantPlacement:ACaseReportStephanie Dumanian, Julie Lamure DDS
UseofBlockAllograftsinPre-ImplantAlveolar 34RidgeAugmentation:ThreeCaseReportsGowhar Iravani, Renée Reynolds, Karin Emde DMD, Jeremy K Ueno DMD
Columbia Dental Review 2009-2010

©2010ColumbiaDentalReviewVolume14:2009-2010 8
Dental Defects Connected with Chemoradiotherapy: A Case ReportAimeeLeibowitz1,SueHwang,DMD2,RichardYoon,DDS3,StevenChussid,DDS4
1Classof2011,CollegeofDentalMedicine,ColumbiaUniversity,NewYork,NY22ndYearResident,PediatricDentistryResidency,CollegeofDentalMedicine,ColumbiaUniversity,NewYork,NY3AssistantProfessor,ProgramDirector,PediatricDentistryResidency,CollegeofDentalMedicine,ColumbiaUniversity,NewYork,NY4AssociateProfessorandDirector,DivisionofPediatricDentistry,CollegeofDentalMedicine,ColumbiaUniversity,NewYork,NY
AbstractDevelopmentalorofacialdentoalveolarcomplicationsasso-ciatedwithchemoradiotherapy ina7-year-oldchildwithahistoryofrhabdomyosarcomaarereported.Thisreportde-scribes,clinicallyandradiographically,theseeffectsinachilddiagnosedat3yearsofagewithalesionprimarytotheleftbuccinator.Earlyevaluationiscrucialtodeterminepotentialdentoalveolarcomplicationsandlong-termconsequences.
Keywords:chemotherapy, radiotherapy, dental defects, case
Introduction Developmentalorofacialdentoalveolarcomplicationsareas-sociatedwithbothchemotherapyandradiationtherapysub-sequenttotreatmentofrhabdomyosarcomas(RMS).RMSarethemostcommonsoft-tissuetumorsinchildren.Thesetumorsarederivedfromskeletalmuscle.Cellmarkerssuchasdesmin,sarcomericactin,sarcomericmyosinheavychainandMyoDsuggestmyogeniccelloriginforthistumor.1Thistypeofsarcomaaccountsfor4-8%ofallmalignanciesinchil-drenunder15yearsold.1ThetumorismorecommoninCau-casians,andmoststudiesshowslightgenderpredominanceinmale.WhileRMSmayoccurinallagegroups,itismostlyseeninthefirstandseconddecadesoflifewithapeakinci-dencebetweenagestwoandsix.2Themostcommonsitesofthistumorinchildrenareheadandneck(35%),genitouri-narytract(23%),andextremities(7%).3TherearethreemaintypesofRMSclassifedhistologicallyasembryonal,alveolar,andundifferentiated.Thealveolartypeaccountsfor20%andishistologicallycharacterizedbyclustersofsmallroundcellswithhyperchromaticnucleiandeosinophilliccytoplasmthatareseparatedbyfibrovascularseptae.2,4-6
Approximately65%ofchildrendiagnosedwithrhabdomyo-sarcoma survive after receiving multimodality treatment.7Animportantreasonfortheimprovedsurvivalratesiswell-timedinitiationofradiotherapycombinedwithchemothera-py.7Chemoradiotherapycanbeusedforlocalcontroloftheprimarylesion,toinduceregressionoftumorsize,andtotreattumorsnoteasilyaccessedforresectionintheheadandneckarea.2Chemotherapyconsistsofcombinationsofvincristine, actinomycin-D, cylcophosphamide, anddoxo-rubicin.Thedose for radiation therapyof rhabdomyosar-comarangesfromapproximately40to50Gy.7,8
Dentalandorofacialabnormalitiesaremostpredominantinchildren who have received chemoradiotherapy treatmentbefore threeyearsofage,as theydonothavea fullyde-veloped primary dentition and the permanent dentition isalso not yet completely formed. The developing teeth areexposedtoradiationduringthecourseoftreatmentforheadandnecksarcomas.Morethan85%ofsurvivorsofheadandneckRMSwhoreceiveradiationdosesgreaterthan40Gymayhavesignificantdentalabnormalities.9Theabnormalitiesincludemandibularormaxillaryhypoplasia, increasedcar-ies,hypodontia,microdontia,rootstunting,andxerostomia.9Chemoradiotherapyhasaconsiderableeffectonsoftandhardtissuegrowthintheaffectedregionsoftheheadandface.Thisleadstofacialanddentalirregularitiesthatexac-erbateduringgrowth.Theextensiveeffectof radiotherapyandchemotherapyoncraniofacialskeletalgrowthmustbemonitoredforallpatientsundergoingtreatmentfortumors.Consequentialdentalandmaxillofacialabnormalitiescanbeexpectedinallcases.Managementofthepatientcallsupontheinvolvementofdifferentmembersofahealthcareteamincludingmaxillofacialsurgeons,dentists,psychologists,di-eticians,andspeechtherapists,alongwiththepatientandtheprimarycaregiver.10Thefollowingcasereportdescribestheorofacialdentoalveolarfindingsforapediatricpatientdi-agnosedwithrhabdomyosarcoma.
Case ReportA7-year-oldmalepatientwithahistoryofalveolarRMS,hypothyroidism, and sickle cell anemia presented to theColumbiaUniversityMedicalCenterpediatricdental resi-dencyclinic forroutinedentalcare.Thechildpatienthadundergoneradiationtherapyontheleftsideoftheheadandneckregionattheageofthree;thecancerisinremissionatthepresenttime.Beforehewasdiagnosedwithcancer,thepatientdevelopedaproptosisofthelefteyeandaleftsubmandibularmass.ThemasswasfirstnotedduringaroutinevisittotheHematologyClinicofNewYork-Presby-terian.Computedaxialtomography(CT)imagingrevealeda2x2.4x2.5cmmassattheangleofthemandibleontheleftside.Additionally,magneticresonanceimagingre-vealedanenhancinglesionintheregionoftheleftethmoidaircells,extending into the leftanteriorcranial fossaandepidurallyalongthe left frontal lobe.Biopsyconfirmedanalveolarrhabdomyosarcoma(chromosome2:13transloca-tion).FurtherevaluationofthelungCTandbonerevealednometastasis.

©2010ColumbiaDentalReview Volume14:2009-20109
Dental Defects Connected with Chemoradiotherapy: A Case Report
Following thediagnosis,he received50.4Gy radiation totheheadandneckregionincludingtheethmoidandsphe-noidsinusesandcompletedthechemotherapyinDecem-ber2003.WhenaCTevaluationinJune2004revealedanewlyticbonyabnormalityinthemidlineofthefrontalboneextendingtotheethmoidbone,hewasre-examinedforacancerrelapse.Additionalexaminations,includingabonescanandchestCT,demonstratednootherevidenceofarelapse, and hence a biopsy was deferred. The imagingstudyinJune2005reportedthelesionasstableanditispresentlybelieved tobecausedbyan infarctdue to thepatient’ssicklecelldisease.
Complications during the patient’s cancer treatments in-cludedfever,neutropenia,andinfectionsthatrangedfromG-tube cellulitis to facial cellulitis. He also developed anepisodeoflegpainthatuponextensiveevaluation,wasat-tributed toa sicklepaincrisis.Hepreviouslyhadseveralepisodesoflife-threateningepistaxis,buthasnothadanyoccurrencesformorethantwoyears.Thepatient’sgrowthhadfallenbelowaverageforhisage,possiblyduetoendo-crineabnormalitiessubsequent tocranial irradiation.Cur-rently,hisgrowthisimprovingsincestartingsupplementalgrowthhormonesandiscarefullymonitoredbyanendocri-nologist.Hisprognosisisnowexcellent;hehasbeenfreeofthecancerandoffofchemoradiotherapy.Hecontinuestobefollowedwithsemi-annualscans.
Thepatientiscurrentlytakingfolicacid,growthhormone,synthroid,andpenicillin.Wheninitiallyexaminedatagefive,hepresentedwithpoororal hygieneandvisually evidentrampant dental caries and dental abscesses. Compre-hensive dental treatment was accomplished under gen-eralanesthesiaattheChildren’sHospitalofNewYork.Nocomplicationsfollowedtheprocedure,andwoundshealeduneventfully.Thepatientwasplacedonroutineoralhygienemaintenancevisits.
Theparentandpatientfailedtofollowupregularlyandre-turnedtotheclinicthreeyearslaterwithachiefcomplaintofuneruptedteeth.Therewerenosignsoffacialswellingorlymphadenopathy.Intra-oralexamination(Figure 1A)re-vealednormalsofttissuewithanabsenceofanysofttissuepathologyorgingivalinflammation.Spacinginthedentitionwasconsistentwith thechild’sage,and theocclusal re-lationshipwaswithinnormal limits.Althoughthepatient’soveralloralhygienewasgoodwithnoclinicalevidenceofcaries,hisincisorshadminorenamelhypocalcificationde-fects.Whiletheremainingdentitionwasfreefromanysignsofmobility,thecentral incisorsexhibitedGradeIImobility.Radiographicevaluationofthepatient(Figure 1B and Figure 2),presentlyeightyearsold,demonstratedmultipledevel-opmental dental defects. These includedcomplete toothagenesis of the permanent maxillary second premolars
andpartialodontogenicdeficits,suchasgeneralizedmod-eraterootstunting,agenesisofpermanentfirstmolarrootsinbotharches, taperingof lower rightpermanentcanineroots,andmicrodontiaofpermanentpremolarsandmaxil-larysecondmolars.Underdevelopedjawswerealsonotedradiographically.Futuretreatmentoptionswerediscussedandthepatientcontinuestobemonitoredthroughhisrou-tinedentalexaminations.
DiscussionRMSarea rapidlygrowing,aggressiveneoplasm inchil-dren.2Ofthethreetypes,theembryonalformissaidtohavethemostfavorableprognosis,whilethealveolarandundif-ferentiatedformsareunfavorable.11Theaforementionedpa-tientisunusualbecausehehasanexcellentprognosisforthealveolarRSandhasbeenfreeofthecancersinceJune2005.Thiscouldbedueinparttotheearlystagingofthecancerandtheabsenceofmetastases.
Thetreatment thepatient receivedwasbasedonthetu-morstageandclinicalpresentation(usingthepretreatmenttumor-node-metastasis (TNM) system).12 It included bothradiationtherapyandchemotherapy.Althoughcurative,thechemoradiotherapyforthepatient’srhabodomyosarcomaproducedlong-termsideeffects.Theseeffectstypicallyin-cludeneuroendocrine,dental,thyroid,andcognitiveissues.Neuroendocrine dysfunction and clinical hypothyroidism
Figure 1(A) Intraoral photo demonstrating splaying of incisor teeth, and (B) a periapical radiograph revealing root agenesis on incisor teeth resulting in delayed eruption.
Figure 2Panoramic radiograph. Note advanced root stunting of incisor teeth, microdontic premolars and second molars, root stunting of the six year molars, and root tapering of lower right permanent canine.

©2010ColumbiaDentalReviewVolume14:2009-2010 10
Dental Defects Connected with Chemoradiotherapy: A Case Report
typicallyoccurduringthefirst10yearsafterradiotherapy.7Thismatchesthepatient’spresentationinthecase,asheis currently taking growth hormone and synthroid for hisdelayedgrowthandhypothyroidism,respectively.Compli-cationsofchemotherapyincludealopecia,myelosuppres-sion(thrombocytopeniaandneutropenia),mucositis,nau-sea,vomiting,andneurotoxicity.Complicationsofradiationtherapytotheheadandneckregion include interferencewithgrowthofthecraniofacialskeletion,limitationofmouthopening, microdontia, hypoplastic enamel, underdevel-opedroots,delayedorprematureexfoliationofteeth,anddentalcaries.2Therampantdentalcariesthatthepatientpresentedwithatagefivewasdueinparttothexerosto-miaassociatedwithradiationtreatment.Radiationgreaterthan40Gythattargetsmorethan50percentofthesalivarygland(Table 1)cancausedecreasedsalivaryflow,xerosto-mia, andsubsequently increaseapatient’s riskofdentalcaries.Radiationaround10Gydestroysdevelopingrootsofthedentition.9
Dentaldefects,secondarytochemoradiotherapy,manifestascertainsignsandsymptoms.Chemotherapeuticagentscan cause microdontia, hypoplastic or hypomineralizedenamel,underdevelopedroots,anddelayederuption.Ra-
diationcan lead toprematureexfoliationofprimary teethandhypoplasiaofthemaxillaryandmandibularjaws,alongwithrootobliteration.Thepatient’sradiographsareprecise-lycharacteristicoftheaforementioneddentaldefects.Thedevelopingpermanenttoothbudswereclearlyaffectedbythecancertreatment, leadingtohypoplasticenamel,rootagenesis, microdontia of the premolars and underdevel-opedjaws(Figure 1B and Figure 2).Inastudyof17childrenwithheadandneckrhabdomyosarcoma,all17hadatleastone dental abnormality.7 The abnormalities ranged frommicrodontia, trismus,mandibular hypoplasia, hypodontia,rootstunting,maxillaryhypoplasia,xerostomia,andradia-tioncaries.7Thechildrenwithdentalabnormalitiesreceivedradiotherapyanywhere fromage3.4 to11.5yearswithadosetotheorofacialregionofapproximately40to60Gy.7Thesefindingssatisfyboththeagebracketandradiationdoserangeforthepatientmentionedabove.
Itmustbenotedthatthepatientpresentswithsicklecellanemiainhismedicalhistory.Sicklecelldiseaseisablooddisordercharacterizedbymorphologicallychangederyth-rocytes and a defective form of hemoglobin due to anaminoacidsubstitutionmutation.Systemicmanifestationsin patients with sickle cell anemia include dentoalveolar
Table1Dental and Oral Complications Secondary to Chemoradiotherapy*
Complication Signs/Symptoms Treatment
AbnormalDentalDevelopment Microdontia Dentalexaminationevery6months withattentiontoearlycaries,Chemotherapy:Vincristine, Hypoplasticor periodontaldisease,andgingivitis,actinomycinD,cyclophosphamide, hypomineralizedenamel andbaselinepanoramicandbitewing6-mercaptopurine(6-MP), radiographs(age5-6years)procarbazine,nitrogenmustard(HN2) Underdevelopedroots
Radiation: Generally10Gycan Delayederuption Carefulevaluationbeforetoothobliteratedevelopingroots extraction,endodonticsandorthodontics, Prematureexfoliationof topicalfluoride,antibioticsasneeded primaryteeth forpatientsatriskforinfection
HypoplasiaofjawsXerostomia,Stomatitis Decreasedsalivaryflow Dentalexamination,salivary flowstudies,attentiontoearlycaries,Radiation:>40Gyand>50%of Xerostomia periodontaldiseaseglandirradiated Alteredtasteperception Encouragemeticulousoralhygiene, Caries salivasubstitution,prophylactictopical fluorides,dietarycounselingregarding Candida avoidanceoffermentablecarbohydrates, nystatinfororalcandidiasis,pilocarpine
*Adapted from Schwartz et al. 9

©2010ColumbiaDentalReview Volume14:2009-201011
Dental Defects Connected with Chemoradiotherapy: A Case Report
2.ChigurupatiR,AlfatooniA,MyallRW,HawkinsD,OdaD (2002) Orofacial rhabdomyosarcoma in neonates andyoungchildren:areviewof literatureandmanagementoffourcases.Oral Oncol38:508-15.
3.Gordon-NunezMA,PivaMR,DosAnjosED,FreitasRA(2008)OrofacialRhabdomyosarcoma:Reportofcaseandreviewofliterature.Med Oral Patol Oral Cir Bucal.13:E765-9.
4.TobarA,AvigadS,ZoldanM,MorC,GoshenY,ZaizovR(2000)Clinicalrelevanceofmoleculardiagnosisinchild-hoodrhabdomyosarcoma.Diagn Mol Pathol9:9-13.
5.GrundyR,AndersonJ,GazeM,GerrardM,GlaserA,GordonA,MaloneM,Pritchard-JonesK,Michalski,A(2001)CongenitalAlveolarRMSclinicalandmoleculardistinctionfromalveolarRMSinolderchildren.Cancer91:601-12.
6.ParhamDM(2001)Pathologicclassificationofrhabdo-myosarcomas and correlations with molecular studies.Mod Pathol14:506-14.
7.PaulinoAC,SimonJH,ZhenW,WenBC(2000)Long-termeffectsinchildrentreatedwithradiotherapyforheadandneckrhabdomyosarcoma.Int J Radiat Oncol Biol Phys 48:1489-95.
8.ChenSY,ThakurA,MillerAS,HarwickRD(1995)Rhab-domyosarcomaoftheoralcavity.Reportoffourcases.Oral Surg Oral Med Oral Pathol Oral Radiol Endod80:192-201.
9.SchwartzCL,HobbieWL,ConstineLS(1994)SurvivorsofChildhoodCancer:AssessmentandManagement.St.Louis,Mosby.
10.MakdissiJ,SleemanD(2004)Dentalandmaxillofacialabnormalities followingtreatmentofmalignant tumours inchildren.Ir Med J97:86-8.
11.PavithranK,DovalD,MukherjeeG,KannanV,Kumaras-wamySV,BapsyPP(1997)Rhabdomyosarcaomaoftheoralcavity:reportofeightcases.Acta Oncologica36:819-21.
12.PappoAS,MezaJL,DonaldsonSS,WharamMD,Wie-nerES,QualmanSJ,MaurerHM,CristWM(2003)Treatmentof localized nonorbital, nonparameningeal head and neckrhabdomyosarcoma:lessonslearnedfromintergrouprhab-domyosarcomastudiesIIIandIV.J Clin Oncol21:638-45.
13. Alves PVM, Alves DKM, de Souza MMG, Torres SR(2006) Orthodontic treatment of patients with sickle cellanemia.Angle Orthod76:269-73.
14.AmericanAcademyofPediatricDentistry(2009)Guide-lineonDentalManagementofPediatricPatientsReceivingChemotherapy,HematopoieticCellTransplantation,and/orRadiation.AAPD Reference Manual31(6):09-10.
15.NationalCancer Institute.OralComplicationsofChe-motherapy and Head/Neck Radiation. Physician DataQuery.2009.Availableat:www.cancer.gov /cancertopics/pdq/supportivecare/oralcomplications/HealthProfessional.AccessedFebruary23,2010.
complications,impairedgrowth,anddelayedskeletalmat-uration.Thedentoalveolarsequelaeincludeenamelhypo-plasia,delayedtootheruption,andimpaireddentinminer-alization.13Thesetraitsresemblethedentalproblemsseeninthepatient.Duetothebroadoverlapofdentalmanifesta-tionsbetweensicklecelldiseaseandchemoradiotherapy,itisimportanttonotethatchemoradiotherapymaynotbethesolecauseofthepatient’sdentalcomplications.
According to general guidelines on dental managementofpediatricpatientsreceivingchemotherapyand/orradia-tion,14earlyanddefinitivedental interventioncanminimizethe risks fororalcomplications.Educationaboutoralhy-gieneandoptimalcarecanpreparetheparentstodealwiththeacuteandlong-termeffectsoftherapytotheorofacialregion.Aftercancertherapyiscompleted,periodicevalu-ationsof thepatientare recommendedat leasteverysixmonths.14Thepatientinthiscasereportfailedtoreturnforroutinefollow-upsuntiluneruptedteethwerenoticed.Po-tentialdentaltreatmentplansforachildwhohasreceivedchemoradiotherapymust includea thoroughassessmentandadiscussionwithcaregiversaboutthepotentialdentaldisturbancescausedbythecancertherapy.
Inorder to curtail dental defects it is ideal to reduce theradiationtohealthyoraltissues.Thiscanbeaccomplishedthrough the use of lead-lined stents, prostheses andshields.14Althoughhigh-intensitycoursesof treatment forheadandnecksarcomasareoftennecessary,studiessug-gestitispossibletodecreaseradiotherapyforcertainpa-tientswithoutcompromisingsurvival,inhopesofdecreas-inglong-termsideeffects.15
ConclusionChemoradiotherapy can lead to various abnormalities inboththeprimaryandpermanentdentition.Headandneckrhabdomyosarcomatreatmentoftendirectly involveshighdoses of radiation to the orofacial region. Consequently,one should expect dental and maxillofacial abnormalitiesin long-term cancer survivors of childhood malignancies.Early evaluation is necessary to determine the potentialdentalabnormalitiesandlong-termconsequencesforchil-drenreceivingchemoradiotherapy.Thiscasedemonstratesseveral signs indicativeofdevelopmentalorofacialdento-alveolarcomplicationsassociatedwithchemoradiotherapyasreviewedintheliterature.Itisanticipatedthatcontinuedroutinedentalexaminations,managementbyamultidisci-plinarymedicalteam,andsemi-annualscanswillhelpen-surethepatientremainsfreeofcancer.
References1. Asakura A, Rudnicki MA (2003) Rhabdomyosarcoma-genesis-Novelpathwayfound.Cancer Cell4:421-2.

©2010ColumbiaDentalReviewVolume14:2009-2010 12
AbstractDuetoitscloseproximitytoperiodontiumandteeth,gingi-valsquamouscellcarcinomacaneasilyresembleabenignlesionwhichcanleadtoamisdiagnosis.Thisisacasere-portofan87-year-oldfemalewithnohistoryofalcoholorto-baccouseinwhichproperdiagnosisofgingivalsquamouscellcarcinomatooknearly6monthsdespiterepeatedvisitstohergeneraldentist.
Introduction OralCanceraccountsforlessthan3%ofallcancersintheUnitedStates,thoughit istheeighthmostcommoncan-cer inmalesandthefifteenthmostcommon in females1.Approximately94%ofalloralmalignanciesaresquamouscellcarcinoma(SCC).WhiletheexactetiologyoforalSCCremains unknown, some of the most common risk fac-tors include theuseof tobacco,consumptionofalcohol,thechewingofareca (betel)quid, syphilis (tertiarystage),candida albicans infection,oncogenicviruses,andimmu-nosuppression1,2.
Oral SCC may have a varied clinical appearance. How-ever, studieshaveshownerythroplakia tobe theearliestmanifestationoforalSCCintheUnitedStatesandEurope,especially in smokersandconsumersofalcohol3. Itmayappearasanexophyticmasswithagranular,papillary,orverrucoussurface.Itmayalsoappearulcerated4.Thestageofdiagnosis isthemost importantpredictoroflong-termprognosis5.Forthisreason,delayeddetectionoforalcancerresultsinalowfiveyearsurvivalratewhencom-paredtoothertypesofcancers6.ThemostcommonsitesfororalSCCincludethelateraltongue,floorofthemouth,andsoftpalate.Other less frequentsites includegingiva,buccalmucosa,labialmucosa,andhardpalate1.Whenaf-fectingthegingiva,themandibularmolarregion isgener-ally themostcommonsite,withmostcasesoccurring inedentulousareas7.
GingivalSCCisoneofthemostdevastatingmalignanciesdue to itscommon invasion intounderlyingbone8.Sincethelesionisusuallyveryclosetoteethandperiodontium,mostpatientswithgingivalSCCvisitageneraldentistfirst.
Misdiagnosis of Gingival Squamous Cell Carcinoma Presenting as a Periodontal Lesion of the Anterior PalateMonaDaneshi1,SimonBeylinDDS2,CandiceZemnickDMD,MPH,MS3,KarinEmdeDDS4
1Classof2011,CollegeofDentalMedicine,ColumbiaUniversity,NewYork,NY2Classof2010,CollegeofDentalMedicine,ColumbiaUniversity,NewYork,NY3AssistantProfessor,DirectorofPredoctoralProsthodontics,MaxillofacialProsthodontist,DivisionofProsthodontics,CollegeofDentalMedicine,ColumbiaUniversity,NewYork,NY4ColumbiaUniversity,CollegeofDentalMedicine,DivisionofPeriodontics,NY,NY
Thus,dentistsplayacrucialroleinearlydetectionandman-agementofgingivalSCC9.
Thefollowingisacaseofan87-year-oldfemalewhopre-sentedwithagingival lesionwhichwas incorrectlyattrib-utedtoherperiodontalconditionratherthangingivalSCC.
Case ReportAn 87-year-old female presented to a general dentist on9/9/2007 requesting tobeseen forcomprehensivecare.Shereportedthelossofarestorationontooth#8aswellasgingivalsorenessintheregionof#8.Thepatient’spastmedicalhistoryincludedhypertension,arthritis,andPaget’sdisease.Medicationsincludedverapamil,atorvastatincal-cium,meclizine,andacetaminophen.Duetoatypicalclini-calpresentationandalackofriskfactorsfororalSCC,thepatient’slesionwasattributedtolocaletiology,andshewasdiagnosedwithgeneralizedmoderatechronicperiodontitis.Shewas treatmentplanned for fourquadrantsofscalingandrootplaningalongwithrestorativetreatment.Betweenthedatesof10/2/07and11/1/07thepatientwasseenthreetimesbyhergeneraldentistforscalingandrootplaningoftheupperrightquadrantbecausetherewasnoimprovementinthegingivallesionaroundtooth#8.
On2/15/08thepatientpresentedtoColumbiaUniversityCol-legeofDentalMedicinewiththechiefcomplaintofswollenandsorepalataltissueintheregionofteeth#8and#9(Figures 1, 2).
Figure 1Fractured tooth #8 on clinical exam when patient presented on 2/15/2008 to the periodontics department at Columbia University Col-lege of Dental Medicine.

©2010ColumbiaDentalReview Volume14:2009-201013
Misdiagnosis of Gingival Squamous Cell Carcinoma Presenting as a Periodontal Lesion of the Anterior Palate
Figure 2Palatal gingival lesion between teeth #8 and #9.
Thepatientreportedanincreaseinpainaroundthegingivalregionoftooth#8forthepastseveralmonths.Thepatienttookantibioticsprescribedbyhergeneraldentist in1/08andreportedthattheantibioticsdidnothelpandherpainpersisted.Aperiapicalradiographoftheregionwastakenandnoperiapicalradiolucencywasnoted(Figure 3).
Figure 3Radiograph showing no periapical radiolucency or endodontic lesion around tooth #8 or #9
Thepatientwasreferredtothepostdoctoralperiodonticsclinic for furtherevaluation. Intraoralexamination revealedagranulomatousanderythematouslesionextendingfromthegingivalmargin toapproximately1cmonto thehardpalatefromthedistaloftooth#8tothedistalof#9.Palatalprobingdepthswere5mmonbothtooth#8and#9,andthe marginal gingiva was erythematous and edematouswithbleedingonprobingpresent.Amoderateamountofplaqueandcalculuswaspresent. Thepatientwasdiag-nosedwithchronicpyogenicgranuloma.Scalingandrootplaningofteeth#7-#10wasperformedwithagingivalflap,whichallowedabiopsyofthelesiontobetakeninordertoconfirmthediagnosis(Figures 4, 5).
Figure 4Gingival flap, buccal view.
Figure 5Gingival flap, palatal view.
Submarginalandsulcularincisionswerecarriedoutonthepalatal regionof teeth#7-#10,whichallowedtheremovalof the abnormal granulomatous tissue for biopsy. Similarincisionsandflapdesignwerecreatedonthebuccalsideofteeth#7-#10,followedbythoroughdebridementofthearea.Sutureswereplacedandhealingoccurredbysec-ondaryintention.
Histologicexaminationrevealedcurvedpiecesofsofttissuecoveredbyatypicalandhyperplasticstratifiedsquamousepi-theliumwithoverlyingparakeratoticmaterial.Epitheliumwasdyskeratoticanddemonstratedbulgingofretepegs(Figure 6).
Figure 6Photomicrograph (H&E, 40x) revealed hyperplastic and hyperkeratotic epithelium with bulging rete pegs. Strands of invasive squamous cells were also present.

©2010ColumbiaDentalReviewVolume14:2009-2010 14
Misdiagnosis of Gingival Squamous Cell Carcinoma Presenting as a Periodontal Lesion of the Anterior Palate
Islandsandstrandsof invasivesquamouscellsexhibitingpleomorphiccellular featureswere identified.These inva-siveislandsdeeplyinfiltratedtheunderlyingfibrousconnec-tivetissue (Figures 7, 8).Alsonotedwerefungalhyphaeandspores,consistentwithcandidaalbicans.
Figure 7Photomicrograph (H&E, 100x) showed invasive islands deeply infiltrating the underlying fibrous connective tissue.
Figure 8Photomicrograph (H&E, 200x) with squamous cells exhibiting pleomorphic cellular features including enlarged and hyperchromatic nuclei with prominent nucleoli, increased mitotic activity, and chronic inflammatory cell infiltrate.
Adiagnosisofmoderatelydifferentiatedsquamouscellcar-cinomaoftheanteriorpalatalgingivawasmade.Thepa-tientwasreferredtoanotolaryngologistforresectionoftheanteriormaxillafromteeth#6-#11.Resectiontookplaceon3/28/08,atwhichtimeIodoformpackingandaskingraftfromthepatient’sthighwasplacedovertheresectedarea(Figure 9).Asurgicalobturatorwasdelivered,andthreeliga-turewireswereplacedtoretaintheobturator.
On4/4/08the ligaturewiresweresectionedandthesur-gicalobturatorwas removed.The interimprosthesiswasdelivered(Figure 10).
Figure 9Skin graft placed after resection of anterior maxilla.
Figure 10Interim prosthesis.
DiscussionOverthepast40yearsdespiteadvancesmadeindiagno-sis, theoverallfiveyearsurvival rate fororalSCChasre-mainedrelativelyconstantataround50%5.Severalreasonsmayaccountforthis:1)highriskpatientsdonotseekmedi-calattention,2)oralcancerexaminationsarenotfrequentlyperformed,and3)existinglesionsareoftenoverlookedbythegeneraldentist.Delaysfromtheonsetofsigns/symp-tomstoclinicaldiagnosisarealsocommon10.
Gingivalcarcinomas inparticularareusuallypainlessandaremostfrequentlyfoundinthekeratinizedmucosaoftheposteriormandible.Ifthetumorpresentsonthemaxillaryridgeitcanextendontothehardpalate.Tumorsindentateareasareeasilymistaken forperiodontaldiseaseorpyo-genicgranuloma.Gingivalcarcinomashaveatendencytodestroyunderlyingbone,thuscausingtoothmobility.Ofallintraoralcarcinomas,gingivalSCCisleastassociatedwithtobaccosmokersandhasahigherfrequencyinfemales1.

©2010ColumbiaDentalReview Volume14:2009-201015
Misdiagnosis of Gingival Squamous Cell Carcinoma Presenting as a Periodontal Lesion of the Anterior Palate
AsisthecaseformanypatientswithoralSCC,asurgicalresectionwasnecessary to remove the tumor.Thismaybeverydevastatingbothfromapsychologicalandphysicalstandpoint.The rationale forcreatingasurgicalobturatorhasthreepurposes.Thefirstpurposeistomaintainfunc-tion.Theobturatoractsasamatrixforthesurgicaldress-ingandallowsthepatienttoswallowandspeaknormally.Thesecondpurposeistomaintainhygiene.Theobturatorseparatesthesurgicalsitefromtheoralcavity.Finally,theobturatorhelpsthepatientmaintaintheirselfimagesotheycancontinuetofunctionsocially11.
Conclusion ThegingivalSCCinourpatientpresentedasgeneralizedmoderatechronicperiodontitis.Afteraflapwascreatedfordebridement,thelesionwasbiopsiedduetoabnormalap-pearanceofgranulomatoustissue.Abiopsyofthislesioncouldhaveeasilybeenoverlookedbecauseclinicallythele-sioncouldhavebeenattributedtolocaletiologyorchronicperiodontitis.Also,commonetiology,riskfactors,andtypi-cal location fororalSCCwerenotpresent inourpatient.Overall,thiscasereportisareminderoftheimportanceoforalcancerscreeningandappropriatereferralifthediagno-sisisquestionable.
References1.NevilleBW,DammDD,AllenCM,etal, (2009)Epithe-lialpathology.In:Oral and Maxillofacial Pathology,3rded.Philadelphia,W.B.Saunders,409-421.
2.LaVecchiaC,TavaniA,FranceshiS,etal,(1997)Epidemiol-ogyandpreventionoforalcancer.Oral Oncology33:302-12.
3.MashbergA,MorrisseyJB,GarfinkelL(1973)Astudyoftheappearanceofearlyasymptomaticoralsquamouscellcarcinoma.Cancer32:1436-1445.
4.ShiuMN,ChenTHH(2003)Impactofbetelquid,tobaccoandalcoholonthree-stagediseasenaturalhistoryoforalleukoplakia and cancer: implication for preventionof oralcancer.Eur J Cancer Prev13:39-45.
5.GreenleeRT,MurrayT,BoldenS,WingoPA(2000)Can-cerstatistics,2000.J Clin Cancer50:7-33.
6.PisaniP,ParkinDM,BrayF,FerlayJ(1999)Estimatesoftheworldwidemortalityfrom25cancersin1990.Int J Can-cer83:18-29.
7.MakridisSD,MelladoJR,FreedmanAL,SalkinLM,SteinMD,MillerAS(1998)Squamouscellcarcinomaofgingivalandedentulousalveolarridge:aclinicopathologicstudy.Int J Periodont Redt Dent18:293-8.
8.WhitehouseGH(1976)Radiologicalbonechangespro-ducedbyintraoralsquamouscarcinomainvolvingtheloweralveolus.Clin Otolaryngol1:45-52.
9.LeeJang-Jaer,etal,(2007)GingivalSquamousCellCar-cinoma Mimicking a Dentoalveolar Abcess: Report of aCase.JOE33:177-180.
10.PitiphatW,DiehlSR,LaskarisG,CartsosV,DouglasCW,ZavrasA(2002)Factorsassociatedwithdelaysinthediagnosisoforalcancer.J Dent Res81:192-197.
11.HurynJM,PiroJD(1989)Themaxillaryimmediatesurgi-calobturatorprosthesis.J Prosthet Dent61:343-7.

©2010ColumbiaDentalReviewVolume14:2009-2010 16
AbstractOdontogenicinfectionsarecommonoccurrences,buttheincidenceofsinusitisseenwiththese infectionsaccountsfor approximately 10%-12% of cases of maxillary sinus-itis.1,2IfaperiapicalinfectionofamaxillarytoothviolatestheSchneiderianmembrane,infectionwilllikelyspreadintothesinus, leadingtosinusitis.Athirty-oneyearoldwomaningoodgeneralhealthpresentedforaConeBeamComput-edTomography (CBCT)scan toevaluatepotentialdentaletiologyofher left-sidedBell’spalsy.TheCBCTscanre-vealedthepresenceofanapicalradiolucencyassociatedwithanendodonticallytreatedtooth#15.Theleftmaxillarysinuswasfilledwithasignificantamountof inflammatorytissueinabubble-likepattern.However,noperforationofthecorticalfloorofthesinuswasnotedbetweentheapi-calinflammatorylesionandthemaxillarysinus.Therefore,althoughcausalitycouldnotbeestablishedbetween thetwolesions,clinicalandradiographicinformationindicatedarelationship.Managementofthisconditionrequiredcon-comitanttherapyoftheodontogenicinfectionandsinusitis.
IntroductionPeriapicalinflammatorylesionscomeaboutastheresultofchronicinfectionortraumatothepulpaltissuesandthere-sultantnecrosisofthedentalpulp.Toxinsproducedbypulp-alnecrosiscanthencausechronicoracuteapicalinflamma-torylesions,suchasaperiapicalgranuloma,radicularcyst,orapicalabscess.3Diagnosisofperiapicalgranuloma,alsoknownaschronicapicalperiodontitis,canbemadewhenthere isgranulation tissueat theapexofanonvital tooth.The lesion may be either chronic or subacutely inflamed.The lesion first develops as an acute apical periodontitis,where neutrophils release prostaglandins, which activateosteoclaststhatresorbthesurroundingbone.Asthebodycontinuestowallofftheinfection,chronicinflammatorycellsbegin to dominate the host response. The lymphocytesrelease mediators stimulating osteoclasts and fibroblasts,whichhistologicallywillappearasinflamedgranulationtis-suesurroundedbya fibrousconnective tissuewall.Asaresultoftheseactions,chroniclesionsareoftenasymptom-atic.Boneresorptioncanbedetectedradiographicallyasaperiapicalradiolucency,whichcanbediscoveredonroutineradiographicexamination.Theaffectedtoothwillgenerallyrevealalossofapical laminadura.4Thelesioncanbeill-defined,showingagradualtransitionfromthesurroundingnormaltrabecularboneintotheabnormalbonepatternofthelesion.Alternately,itmayhaveawell-definedperipherywithacorticatedborder,attributedtothestimulationofos-teoblasticactivityinthesurroundingbone.5Duetothevaria-
tioninsize,theradiographicappearanceisnotsufficienttoconfirmadiagnosisofaperiapicalgranuloma,sinceperiapi-calgranulomacantransformintoacystoranabscess(andviceversa)withoutaradiographicchange.4
TheSchneiderianmembraneisthethinepithelial liningofthemaxillarysinus. In the rareevent that theSchneideri-anmembraneisperforatedbyadentalpathosisthathascrossedthecorticalboundaryofthesinus,amaxillarysi-nusitis can manifest.1 Odontogenic sinusitis accounts foronlyaboutonetenthofallcasesofmaxillarysinusitis.1,2Inadditiontoperiapicalinfection,sinusitisrelatedtoodonto-geniccausesalsooccurwhentheSchneiderianmembraneisviolatedbyotherpathologiclesionsofthejawsandteeth,maxillary(dental)trauma,orbyiatrogeniccausessuchascomplicationsofimplantplacementormaxillofacialsurgery.1Thehealthymaxillarysinuscontainsanormalbacterialflorathatmayincludeacombinationofaerobicandanaerobicbacteria.Duetolocalorsystemicfactors,abilateralmaxil-larysinusinfectionmaydevelop,leadingtothethickeningofthesinusmembraneandimproperdrainagecausedbytheblockageoftheostium.4,6Intheeventoffocalareasofinflammationwithinasinglesinus,aunilateralsinusitismayoccur,whichcanbeattributedtoanodontogenicsource.4Maxillarysinusitisofodontogenicoriginisusuallychronic.6
Computed tomography (CT) is currently the modality ofchoiceforevaluatingthepresenceandextentofdiseaseaswellasanyanatomicpredisposingfactorsinpatientswithsymptomsofchronicmaxillarysinusitis.7CBCTisarecenttechnologythatwasfirstdevelopedforangiographyin1982andlaterappliedtomaxillofacialimaging.CBCTusesadi-vergentor“cone-shaped”sourceofionizingradiationandatwo-dimensionalareadetectorfixedonarotatinggantrytoacquiremultiplesequentialprojectionimagesinonecom-pleterevolutionaroundtheareaofinterest.5Althoughsofttissuescannotbedifferentiated,hyperplastictissueinthesinuscanusuallybeeasilyvisualizedonCBCTscans.
Case ReportA31-year-oldfemalepresentedtoaprivateperiodontist’sofficewithacomplaintof left-sided facialnumbnessandafeelingof“fullness”intheleftsideofherface.Thesymp-tomswereof recentonset.Previousmedicalhistorywasotherwise unremarkable. Clinical examination revealed amarked“droop”totheleftsideofherface.Shewasunabletosmileontheleftside.AtentativediagnosisoffacialnerveparalysiswasmadeafterelicitingtheBells’ssign.ACBCTscanwasprescribedtoevaluatepotentialdentalorotologi-
Maxillary Sinusitis Due to Apical Rarefying OsteitisRupaliShah1,ViolettaVayner1,StevenR.Singer,DDS2
1Classof2011,ColumbiaUniversity,CollegeofDentalMedicine,NewYork,NY2AssociateProfessor,DivisionofOralandMaxillofacialRadiology,ColumbiaUniversityCollegeofDentalMedicine,NewYork,NY

©2010ColumbiaDentalReview Volume14:2009-201017
Maxillary Sinusitis Due To Apical Rarefying Osteitis
caletiologyofherleftBell’spalsyandtoseekacausativefactor for the feeling of “fullness”. Previous dental historywas significant for endodontic treatmentof anupper leftsecondmolar andmultiple restorations.TheCBCTscanwassenttoColumbiaUniversityCollegeofDentalMedicineforconsultationandradiologyreport.
The CBCT scan viewed in panoramic reconstruction, aswellasmultiplanarreconstructions,revealedthepresenceof an apical radiolucency associated with endodonticallytreatedtooth#15 (Figure 1). Itwasapproximately1cminitsgreatestdimensionandwassurroundedbyacorticatedborder. The lesion appeared to have caused remodelingofthefloorofthesinussuperiorly intheregion (Figure 2).Themaxillarysinuswasfilledwithasignificantamountofinflammatorytissueinabubble-likepattern(Figure 3).Non-contributory findings includedseveral restored teeth.The
Figure 1CBCT Panoramic reconstruction. Apical inflammatory lesion associated with tooth # 15 and maxillary sinusitis can be seen on the patient’s left side.
Figure 3CBCT Axial reconstruction demonstrating hyperplastic soft tissue in the left maxillary sinus.
Figure 2CBCT Coronal reconstruction. Remodeling of the floor of the left maxil-lary sinus is noted.
contralateral maxillary sinus, ethmoidal air cells, and thesphenoidsinuswerenormallyaerated.Nocommunicationwasnotedbetweentheapicalinflammatorylesionandthemaxillary sinus.Thediagnosesofapical rarefyingosteitisandacutesinusitisweremadebasedon theclinicalandradiographicinformation.
Thepatientwasplacedonantibioticsforthesinusitisandtheoffendingtooth#15wasextracteduneventfully.Thepa-tientwasreferredtoaneurologist,whowasabletoconfirmthediagnosisofunilateralBell’sPalsy.Thepatientwaskeptonfollow-up.DiscussionOdontogenic infections are common in occurrence, buttheincidenceofsinusitisseenwiththeseinfectionsisex-tremelylow.1,2Mostinfectionswillspreadalongthepathofleastresistance,whichisgenerallythroughthethinnerboneofthelateralwallofthemaxillaryalveolusandpresentasfacialorintraoralswellingsandabscesses.1Thethickcorti-calboneof thefloorof themaxillarysinususuallyservesasaneffectivebarrier,preventingthedirectpenetrationofodontogenic infections into themaxillarysinus.As in thiscase,whenodontogenic infectionsspread intothesinus,thesecondmolar isoften involveddue to its roothavingtheclosestdistance to the sinus floor (meandistanceof1.97mm).Also,itiscommonformaxillaryposteriorteethtobeassociatedwithsinusitis,becauseas themaxillarysi-nusexpandsduringdevelopmentthemaxillaryteethrootsmayprotrudeintotheformingsinuscavity,resultingintheroot apices being surrounded by sinus mucoperiosteum(Schneidarianmembrane).2Rootcanal therapyofamax-illary tooth is alsoapotential causeofmaxillary sinusitis,

©2010ColumbiaDentalReviewVolume14:2009-2010 18
Maxillary Sinusitis Due To Apical Rarefying Osteitis
duetoinstrumentationthatmayintroducebacteriaclosetothesinuscavity,orextrusionofmaterialusedinrootcanaltherapyintothesinus.1,6Whetherthesinusitisisduetothespreadofodontogenicinfectionorcausediatrogenicallyviarootcanaltherapy,adirectcommunicationexistswiththesinus.Thiscaseisuniqueinthat,althoughamucositis isapparentintheleftmaxillarysinus,aperforationofthesinusmembraneorextrusionofmaterialfromthepreviousend-odontictreatmentofthetoothisnotapparent.
Radiologyisanimportanttoolinestablishingthediagnosis.TheadventofCBCTgreatlyfacilitatesaccesstotheinternalmorphologyofsofttissueandskeletalstructure,andcausesnomagnificationerrorsbecauseofgeometricdistortions.8Althoughapanoramicradiographicviewishelpfulforevalu-ationofthemaxillaryteethtothesinus,CBCTisbettersuitedto visualizeboneand soft tissueoutlineswithmultiplanarreconstructions.InthisstudytheinitialpurposeoforderingtheCBCTwas toevaluateapotentialdentalorotologicaletiologyofthepatient’sleft-sidedBell’sPalsy.Sincethesig-nificantfindingsoftheCBCTexaminationwereconfinedtothemaxilla (thealveolusand thesinus), it canbe inferredthattheapicalrarefyingosteitiswasincidentaltotheBell’sPalsy andnodirect connectionbetween the twocanbemade.Therefore,whiletheCBCTfindingsdidnotconfirmthediagnosisofBell’sPalsy,thethree-dimensionalimagesgavetheradiologisttheabilitytoviewcommunicationsbe-tweenthemaxillarysinusandthemaxillaryteeth,aswellasmucosalchangesofthesinus.7,9Incasesofapicalrarefyingosteitis, the radiographic termusedtodescribeperiapicalinflammatorylesions,a“haloshadow”maybenotedwithinthemaxillarysinus.This“haloshadow”istheresultofanin-flammatoryperiostealreaction,whichresultsinathinlayerofnewboneproducedbytheinflamedperiosteumwithinthemaxillaryantrum.5Inthepresentedcasea“haloshadow”ispresent,butanoro-antralcommunicationisnotnoted.
Inthiscase,whiletheradiographicfindingsdonotrevealoro-antral communication, the maxillary sinusitis is mostlikelyduetotheodontogenicinflammatorylesion.Manage-mentofthisconditionrequiresconcomitantmanagementofthedentaloriginandtheassociatedsinusitistoensurecompleteresolutionof the infection.2 Inorder toeliminatethesourceoftheinfection,extractionorrootcanaltherapyof the infected tooth is recommended.10 However, if rootcanaltherapyisunsuccessful,itisadvisablethatthetoothbeextracted.Forthispatient,thiswastheoptionselected,sincetooth#15hadpreviouslybeenendodonticallytreated.Itisrecommendedthatantibiotictherapyeffectiveagainstoralfloraandsinuspathogensbetakenfor21to28days.2The oral flora implicated in maxillary sinusitis of odonto-genicorigin is similar to thatof usualoral and jaw infec-tionsofodontogenicorigin,whichistypicallyacombinationofaerobicandanaerobicbacteria includingstreptococci,
Bacteroides, Veillonella, Corynebacterium, Fusobacterium, Peptostreptococcus,andEikenellaspecies.1Achronicsi-nusitis has a greater percentage of anaerobic bacteria,mainlybecausetheobstructedostiumandresultantinflam-mationofthesinusproducechangesintheSchneiderianmembraneand reduce theoxygen tensionwithin the si-nus.Theantibioticofchoiceisstillamoxicillin,butwithin-creasedresistanceduetoß-lactamase-producingbacteriaalternative antibiotic therapy is nowused (eg. amoxicillin-clavulanic acid, cephalexin, cefoxitin, ceftriaxone, azithro-mycin,clindamycin).1Alongwithantibiotictherapy,theuseof systemic and local intranasal decongestants also aidsinreducingmucusproduction,alteringtheenvironmentofthesinuscavity,andimprovingciliaryfunction.Salinenasalspraysalsoaidtomechanicallyloosenbacteriaandallevi-atesideeffectsofnasalmucosaldryness.1,2
ConclusionConcomitantapicalrarefyingosteitisandunilateralmaxillarysinusitisareuncommonevents.Withoutdirectevidenceofperforationofthecorticalboundaryofthesinusandcom-municationbetweenthesinusandtheapicalinflammatorylesion, it is difficult to assign causality. Nonetheless, theproximityof the two lesions in thepresentedcase,alongwiththeabsenceofdetectablelesionsintheotherparana-salsinusesinthispatientdosuggestarelationship.CBCTimagingprovidesthree-dimensionalviewingoftheaffectedregions, along with accurate measurements and correctanatomicrelationshipsbetweenadjacentstructures.References1.MehraP,JeongD(2009).MaxillarySinusitisofOdontogenicOrigin.Current Allergy and Asthma Reports9(3):238-43.
2.BrookI(2006).SinusitisofOdontogenicOrigin.Otolaryn-gology–Head and Neck Surgery 135(3):349-55.
3.CarrilloC,PenarrochaM,OrtegaB,MartiE,BaganJ,Vera F (2008). Correlation of Radiographic Size and thePresenceofRadiopaqueLaminaWithHistologicalFindingsin70PeriapicalLesions.Journal of Oral Maxillofacial Sur-geons66(8):1600-605.
4.NevilleB(2009).OralandMaxillofacialPathology.3rded.St.Louis,Mo,Saunders/Elsevier.
5.WhiteS,PharoahM (2009).OralRadiology:PrinciplesandInterpretation.St.Louis,Mo,Mosby/Elsevier.
6 Arias-Irimia O, Barona-Dorado C, Santos-Marino J,Martinez-RodriguezN,Martinez-GonzalezJ(2010).Meta-analisisoftheEtiologyofOdontogenicMaxillarySinusitis.Medicina Oral, Patología Oral Y Cirugía Bucal15(1):70-73.

©2010ColumbiaDentalReview Volume14:2009-201019
Maxillary Sinusitis Due To Apical Rarefying Osteitis
7. Connor S., Chavda V, Pahor A (2000). Computed To-mographyEvidenceofDentalRestorationasAetiologicalFactorforMaxillarySinusitis.Journal of Laryngology & Otol-ogy114(7):510-13.
8. Huang C, Brunsvold M (2006). Maxillary Sinusitis andPeriapicalAbscessfollowingPeriodontalTherapy:ACaseReport Using Three-dimensional Evaluation. Journal of Periodontology77(1):129-34.
9.AggarwalV, LoganiA,ShahN (2008). TheEvaluationofComputedTomographyScansandUltrasounds in theDifferentialDiagnosisofPeriapicalLesions.Journal of End-odontics34(11):1312-315.
10.IikuboM,SasanoT,ShojiN,SakamotoM(2002).Non-surgicalTreatmentforOdontogenicMaxillarySinusitisUsingIrrigationthroughtheRootCanal:PreliminaryCaseReport.Tohuku Journal of Experimental Medicine197(1):47-53.

©2010ColumbiaDentalReviewVolume14:2009-2010 20
AbstractExternal root resorption is an uncommon occurrence indentistryand therearevery fewcasesandsparse litera-tureintheareaofgeneralizedidiopathicresorption.Itisthepurposeofthisarticletohighlightaclinicalcasepresentedtothepost-doctoralPeriodonticsclinicatColumbiaUniver-sity,CollegeofDentalMedicine.Throughthis,theetiology,characteristicsandpossibletreatmentwillbehighlightedtodescribetheprocessofidiopathicexternalrootresorption.
IntroductionExternal root resorption has been described as early as1930.1Sincethattime,theetiologyhasbeendeterminedtobeprimarilyduetotraumaticinjury.Thisincludesinjurytotherootsurfacecausedbytrauma,orthodontictreatment,periapicalinflammation,andneoplasticdiseaseofthejaw.1However,therehasbeenlittledocumentationandliteratureassociatedwith idiopathic external root resorption. Thereareevenfewerreportsofgeneralizedexternalrootresorp-tioninwhichresorptionaffectstheentiredentition.Ingener-al,idiopathicrootresorptioncanbedescribedasresorptionintheabsenceofanyofthetraditionaletiologiesdescribedabove. There may be numerous nontraditional reasonsforrootresorption, includingageneticpredispositionandperhapsmaybeundetectedminortrauma.However,thesenontraditionaletiologieshavenotbeenconclusivelystudiedordocumented.2Thus,itisclearthatexternalrootresorp-tionwithoutanyexternalinducingfactorsremainsuncleartothisdate.3
Although thecausesof idiopathic root resorptionarenotclear,thepathophysiologyhasbeenextensivelystudiedanddescribed.Externalrootresorption,whetherfromtraumaoridiopathicreasons,isduetoaninflammatoryresponse.Theinflammatoryresponseincludesthepresenceofcytokines,proteinases,collagenasesandmulti-nucleatedosteoclaststhatresorbthecementumanddentinoftheroot,causingthe root tobebluntedand lose itsnaturalanatomy.4Ad-ditionally,thehardtissuesareusuallyprotectedbylayersofosteoblasts,cementoblastsandtheperiodontal ligament.Thelossoftheperiodontalligament,fromsourcessuchasinflammation,causestheexposedcementumtobecomechemotatictoclasticcells.4,5,6
Ingeneral,externalrootresorptioncanbesubdividedintothreetypes.Thisincludessurface resorption, replacement resorption associated with ankylosis and inflammatory re-sorption.2Thefirst,surface resorption,iswhenadenudedroot surface has osteoclast-activating factors that attractosteoclastsandcementoclasts,causingresorptionof the
Idiopathic External Root Resorption: A Case StudyChristopherHsia1,AndrewHanDMD2
1Classof2011,CollegeofDentalMedicine,ColumbiaUniversity,NewYork,NY22ndYearResident,DivisionofPeriodontics,CollegeofDentalMedicine,ColumbiaUniversity,NewYork,NY
externalsurfaceof the root.However,besides resorptionatthesites,thereisacyclicbalanceofresorptionandde-position fromnearbycementoblasts thatwill try to repairthedamage.2,4Externalrootresorptionoccursasaresultofanimbalance,inwhichresorptionactivityexceedsthatofdeposition.
The second, replacement resorption with ankylosis, oc-curswhensurfaceresorptionstopsandbonecellsinvadethesiteandestablishthemselvesintheareaandthusformboneontheexternalsurfaceoftheroot.Thispreventsthenormalreparativecellsoftheperiodontalligamentfromde-positingatthesiteofresorptionandcausesthefusionofthetoothtothebone(anklyosis).2Becauseofthisankylosis,thebonyareaofthetoothaswellasthesurroundingalveo-larprocessaresubjecttobodilyturnoverprocesses,whichcontinuallylaynewbonearoundtherootsurface.
The last process, inflammatory resorption, can furtherbedividedintotwotypes;peripheral inflammatory root resorp-tion(PIRR)andexternal inflammatory root resorption(EIRR).Peripheralinflammatoryrootresorptionisduetodestructionbycementoblasts throughcementoclast-activating factorsderivedfromtheperipheryoftheroot.Externalinflammatoryrootresorptioniscausedbyanecroticpulpthatstimulatestheexternalclasticcells.InbothPIRRandEIRR,theosteo-clastsactasspecializedmacrophagestoremovetheinfect-edcalcifiedtissuefromthebody.6Thus,itisclearfromtheabovedescriptionsthatexternalrootresorptionisastalwartreactiontotherootsurfaceofthedentitionandthatitrarelyoccursintheabsenceofaspecificetiologicfactor.
Case PresentationA45yearoldfemalepresentedtoColumbiapost-doctoralPeriodonticclinicwithareferralfromSt.Luke’sHospital.Thepatient’s chief complaintwas that “her teethwere loose.”Herdentalhistory included13differentrestorationsandahistoryoflooseteeth.Shedeniedhavinganyprevioushis-toryoforthodontictreatmentoranyfactorsthatarenormallyassociatedwithexternalrootresorption.Thepatientreport-ed scaling done bi-annually and had acceptable hygiene(brushestwiceaday,butdoesnotflossregularly).Thepastmedicalhistoryincludedhypercholesterolemiaandasthmaasachild,but thepatientdeniedanysignificantsystemichealth issues.She iscurrentlymedicatedwithTricor,Cal-cium,andVitaminDsupplements.Shehasnoknowndrugallergiesanddoesnotsmokeorconsumealcohol.
Upon examination, both extraoral and intraoral examina-tionsshowedallhardandsofttissuestobewithinnormal

©2010ColumbiaDentalReview Volume14:2009-201021
Idiopathic External Root Resorption: A Case Study
Figure 1-1A full-mouth-series of the patient showing generalized bone loss, with furcation involvements on most molars. Additionally, the root apices are blunted and have lost their original anatomy and form.
limits.Heroralhygienewasevaluatedanddiagnosedaspoorbecauseofgeneralizedmoderateplaquebuildup.Theamountofplaquehadledtothedevelopmentofgeneral-ized,pink-redgingivalthatwasnotswollen.Periodonticex-aminationrevealed20percentofsiteswithpocketdepthsof5mmorgreaterintheposteriorregions,furcationinvolve-mentsonroughly60percentofmolars,bleeding-on-prob-ingatapproximately50percentofallsitesandmobilityofamajorityofherteeth.
Afull-mouth-seriesofradiographswastakenandshowninFigure1-1.Itisevidentfromthefull-mouthseriesthateverytoothhasundergoneextensivelossofrootstructure.
Figure 1-2Periapical radiograph of the anterior mandibular segment of patient presenting with idiopathic external root resorption. It is observed that the patient has decreased amounts of bone with blunting of the apices of the teeth as indicated.
Figure 1-3Periapical radiographs and bitewings of the posterior left segment of patient presenting with idiopathic external root resorption. It is observed that the patient has decreased amounts of bone with blunting of root tips, loss of root length and loss of anatomy.
Specifically,itcanclearlybeshownthatgeneralizedblunt-ingofroots,adecreaseinrootlengthandalossofanato-my.Theseissuesaregeneralized,havingeffectsonallteethin thedentition.To illustrate this, Figure1-2 shows thesefeatures in theanteriormandibular regionandFigure1-3showsthisintheleftposteriorregion.
Basedontheclinicalandradiographicevaluations,thepa-tient’sprognosiswasdeterminedthatshewouldeventuallyloseallherteethandbecomeedentulous.Currently,therewasnotanyspecifictreatmentmodalitytostophercon-

©2010ColumbiaDentalReviewVolume14:2009-2010 22
Idiopathic External Root Resorption: A Case Study
ditionbut rather, aggressiveperiodontal scaling and rootplanningwasplannedtopossiblyhelparresttheinflamma-toryresponsethatwascausingtherootresorption.
DiscussionGeneralizedidiopathicrootresorptionisarareanduncom-mon occurrence in dentistry. Despite the fact that mostpractitionerswillneverobservethisphenomenonfirsthand,itisstillimportanttodocumentthesecasesandnoteanypossibletreatments.Oneoftheearliestcasesofidiopathicexternal root resorptionwasdescribed in 1930,where a36-year-old female had generalized progressive cervicalrootresorption.Strangely,itwasthenbelievedthatthispa-tient’srootresorptionwascausedbya“functionalhepaticdisturbance.”7Thetreatmenttohalttherootresorptionwasdietary modification until the liver returned to normal. Al-thoughthedeterminedetiologyin1930wasunsound,thenotionofalinkbetweensystemicillnessesandrootresorp-tionisaccurate.1,4,8,9Toclarify,previousliteraturehasshownthatsystemic illnessesassociatedwithexternal idiopathicroot resorption include hypophosphatasia, hyperparathy-roidism, renal disease, hepatic disease, bone dysplasia,Papillon Lefevre syndrome, endocrine disorders and soforth.1,4,8,9However, thepatientwhopresentedtotheCo-lumbiadentalclinicdidnothaveanysystemicfeaturesthathavebeendocumentedwithexternalrootresorption.Ad-ditionally,thepatientdidnothaveanyofthemorecommonetiological factors that are associated with external rootresorptionsuchasexcessivepressure,orthodontic treat-ment,occlusaltrauma,impactedteeth,periradicularinfec-tionoreventoothbleaching.
Figure 2-1A photograph of the patient’s upper right posterior dentition, which did not show any signs of adverse loading or observable etiological factors.
Thus,accordingtohermedicalanddentalhistory,therearenoknownsystemicorcommonetiologicfactorsassociatedwiththispatient’scondition.Whatispresent,however,doesnotseemtobeassociativewithherdisease.Primarily,the
patient’s poor periodontic health and generalized plaquebuild-upcouldplaya role in theexternal root resorption.However,similar levelsofplaque inotherpatientsdonotcause such generalized destruction. Moreover, this pa-tient’sdentitiondidnotshowanysignsofadverseocclusalloadingorwear,asillustratedinFigure 2-1.OnenotionthathasbeendiscussedinSaravia’sstudyin1989,isthattherecouldbe ageneticpredisposition towards external boneresorption.9 It isconclusive that thecauseofher root re-sorptioncannotbe isolated to identifiablecauses.This isalsoinaccordancetoKerrandhisconclusionthatdespitelabexaminationsandhistologicstudies,therehasbeenlittleevidenceofadirectcausativepathology.1
Despitethefactthatthesourceofthepatient’srootresorp-tionisunresolved,theconditionofidiopathicrootresorptioncanbecharacterizedandthereforeaidintheidentificationanddiagnosisinotherpatients.Frompreviousliterature,id-iopathicrootresorptioncanbecharacterizedbyseveralfac-tors.AccordingtoKerr,predisposingfactorsincludefemalegender,beingintheagerangeof30-40,andperhapshighlevels (highspectrumofnormal)ofalkalinephosphatase.1However,otherresearchershavedescribedcasesranginginagefrom14-39andexternalrootresorptiondominanceinmalesbyaratioof11:1.4Clearly,largerstudiesmustbeconductedtoresolvethisdiscrepancy.Furthermore,theremaybeageneticrelationship.Multiplestudieshaveshowna“tentativegeneticassociation”whetherbyanautosomaldominant inheritance pattern or recessive pattern.4,9 Butthese studies were small and not deemed of statisticalsignificance.Nevertheless,thesemayaid indiagnosingapatientbyaskingthemif“suchaneventhasoccurred intheirfamilies.”Clinically,thesepatientsusuallypresentwithnormal-appearingdentitionandperiodontia,toothmobility,andalackofperiodontalinflammation.4Furthermore,Cho-liaandhispeershavestatedthatidiopathicrootresorptionisusuallyassociatedwiththepremolarandmolarareas.Yetthiscaseisanexceptionandshowsrootresorptiontobeaffectingherentiredentition.Radiographically,theremaybealossofanatomyoftherootstructurewithbluntingoftheapiceswithabsenceofperiapicalradiolucenies.Histologi-cally,clasticcellsarepresentinabundance.Thesecharac-teristicsmayaidpractitionersinrecognizingidiopathicex-ternalrootresorptionandprovidetheirpatientswithsometreatmentoptions.
Treatments described in the past literature include modifi-cationofanyexistingadverseocclusalloading,endodontictreatmentoftheaffectedteethandpossibleinhibitionoftheclasticcells responsible for the resorptionprocess.Tobe-gin,themostnon-invasivesolutionistoremoveanyadverseloadingortraumainducingfactors.However,mostidiopathicrootresorptionsarerarelysosimpleanditisoftenthatthereasonsforthisresorptionarecomplexandundisclosed.

©2010ColumbiaDentalReview Volume14:2009-201023
Idiopathic External Root Resorption: A Case Study
Amoreinvasiveprocedurehasbeendescribedinpastlit-erature where root-canal therapy could halt external rootresorption.5Thiswasalsoshowntohaltrootresorptionduetotraumaorevenfromavulsedteeth.5EndodonticliteraturehasshownthatthehighpHofthecalciumhydroxideusedinendodontictreatment,canpermeatethroughthedentinaltubulestotherootsurfaceandcanchangetherootsurfaceenvironmenttopreventinflammation.5Itisthoughtthatcal-ciumhydroxideisbeneficialforrootresorptionbecauseofitshighcalciumionconcentrationwhichpromoteshealing,calcificationandremineralization.5,10Additionally,thealkalinepHofcalciumhydroxidestimulatesmatrixformationbyfor-mativecells,aswellasneutralizestheacidicproductsoftheresorptive cells.5,10 Previous studies have shown that rootcanal therapyhashalted theexternal root resorptionpro-cessandpatientspresentaspost-operativelyasymptom-atic.However,inthiscase,thepracticalityofperformingrootcanalsonallherteethdoesnotseemlikeaviableoption.
Anothermodalityproposedforexternalrootresorptionisin-hibitionoftheclasticcellsintheresorptionprocess.Clasticcells,suchasosteoclastsandfibroclastscanbeinhibitedviacalcitonin.Thisissimilartotheactionofcalcitoninproducts,suchasCibacalcin,whichreduceboneturnoverinthebodyinconditionssuchasosteoporosis.4Anotheroptionwouldbestimulationofosteoprotegerin(OPG)productionwhichisknowntoinhibitosteoclastactivity.Suchtreatmentoptionshaveyettoberesearchedextensivelyandtherearenostud-iestoconfirmthattheywouldworkeffectivelyonapatient.
Conclusively, with all these proposed treatment modali-ties, therehasyet tobeanestablishedtreatmentoption.Perhapswithmorecasesofgeneralizedidiopathicrootre-sorption,moreresearchonappropriatetreatmentcanbefurtherstudied.Asaresultofthecurrentlevelofresearch,theprognosisforthepatientwasdescribedaspoorasitwasexpectedthatshewouldloseherremainingteeth.Heridiopathicrootresorptionpresentsasaninterestingcasetoreviewthepathophysiology,possibleetiologies,predispos-ingfactorsandpossibletreatment.
ConclusionToconclude,thereismuchthatisunknownaboutgener-alizedidiopathicexternalrootresorption.Paststudiesandliteraturehaveprovidedverylittleinformationaboutthisrarephenomenon.Thepresentationofthis40-yearoldfemaletoPGperiodonticsatColumbiaUniversityprovidedavalu-able insight into this occurrence and re-established thestancethatfurtherstudyisrequiredinordertounderstandandproperlytreatthisseeminglyuntreatablecondition.
References1.KerrDA,CourtneyRM,BurkesEJ.Multiple idiopathicrootresorption.Oral Surg Oral MED Oral Pathol. 1970:29,552-565.
2.GorrelC.“ToothResorption-WSAVA2004Congress.”VeterinaryInformationNetwork(VIN)-ForVeterinarians,ByVeterinarians. 2004. Web. 26 Feb. 2010. http://www.vin.com/proceedings/Proceedings.plx?CID=WSAVA2004&PID=8645&O=Generic.
3.YokoI,MasatsuguH,ToshinoriY,HideakiE,HoroshiH,KohiK,ShizukoS,ReiichiO.ACaseofMultipleIdiopathicExternalRootResorption.Japanese Journal of Conserva-tive Dent.1999:42,878-885
4.Choliaetal2005SS,WilsonPHR,MakdissiJ.Multipleidiopathicexternalapicalrootresorption:reportoffourcas-es.Dentomaxillofacial Rad.2005:34,240-246.
5.HedgeMN,PardalD.Healingofexternalinflammatoryrootresorption–acasereport.Indian Endo Soc.2007:1,34-38.
6.AndreasenJO.ExternalRootresorption:itsimplicationsindental traumatology,pedodontics,periodontics, ortho-donticsandendodonticfs.Int Endo J.1985:18,109-118.
7.PostlethwaiteKR,HamiltonM.MultipleIdiopathicRootRe-sorption.Oral Surg, Oral MED Oral Pathol.1989:68,640-643.
8.NarendarSN,WilliamLVE. IdiopathicRootResorption.Oral Sur, University of Iowa Dent.1970.
9.SaraviaME,MeyerML.Multipleidiopathicrootresorptioninmonozygotictwins:casereport.Ped Dent1989:11,76-79.
10.SafaviKE,DowdenWE,IntrocasoJH,LangelandK.Acomparison of antimicrobial effects of calcium hydroxideandiodine-potassiumiodide.J Endo1985:11,454-456.

©2010ColumbiaDentalReviewVolume14:2009-2010 24
AbstractRamsay Hunt syndrome (RHS) results from the reactiva-tionofthevaricellazostervirus inthepre-auricularregionthat is associated with facial paralysis. Additional symp-tomsmayincludetinnitus,hearingloss,nausea,vomiting,vertigo, synkinesis, and nystagmus. TemporomandibularJointDisorder(TMD)isatermthatcoversarangeofclinicalproblemsthat involvesthemasticatorymuscles,thetem-poromandibularjoint(TMJ),andthesurroundinganatomy.ThisarticlepresentsacasereportthatdescribesapatientwithRHSwhopresentedwithpre-auricularpainandwasdiagnosedwithTMD.
IntroductionJamesRamsayHunt,aprofessoratColumbiaUniversity,firstdescribedRamsayHuntsyndrome (RHS)asvaricellazostervirus(VZV)oticusinconjunctionwithperipheralfacialnerveparalysis.1CloselyassociatedwithRamsayHuntsyn-dromearesymptomsoftinnitus,hearingloss,nausea,vom-iting,vertigo,synkinesis,andnystagmus.2Thesesymptomstypicallypresentunilaterally.3RHSissecondtoBell’spalsyasthemostcommoncauseofatraumaticperipheralfacialnerveparalysis.4PrimaryVZVinfectioncanleadtodormantcranialnerveinfection.RamseyHuntsyndromeresultsfromareactivationoftheVZVinthegeniculateganglion;5there-fore,apositivehistoryofVZVinfectionorchickenpoxises-sentialfordiagnosis.ReactivationofVZVmayleadtodeepfacialpainthatradiatestotheear,followedbytheappear-anceofavesicularrashonthegeniculateregionoftheear.6
StandardtreatmentofRHSincludesadministrationofAcy-clovir(250mgthreetimesdailyIVor800mgfivetimesdailyPO)andPrednisone (1mg/kg/dayPOfor5days followedbya10day tapering).7Earlydiagnosisand treatmentarethemostimportantpredictorsforsuccessfulrecovery.Re-centstudieshaveshownthatcompeterecoveryfromRHSsymptomsoccurred75%of the timewhenpatientswithRHSweretreatedwithin3daysofreactivationcomparedto30%completerecoverywhenpatientsreceivedtreatment7dayspostreactivation.7Moreover,50%ofpatientswhodidnotreceivetreatmentinthefirst3daysprogressedtocompletelossoffacialnerveresponse.7
TMD isamajor formofnon-odontogenicorofacialpain.8ThereareanumberofdifferenttypesofTMD,allofwhichinvolvethemasticatorymuscles,theTMJ,and/orthesur-
Ramsay Hunt Syndrome presenting as TMD: A Case ReportNicholasAndros¹,EdwardRudolph²,JenniferBassiurDDS³¹Classof2011,CollegeofDentalMedicine,ColumbiaUniversity,NewYork,NY²Classof2011,CollegeofDentalMedicine,ColumbiaUniversity,NewYork,NY³DirectorAssistantProfessor,DivisionofOralandMaxillofacialSurgeryNewYorkPresbyterianHospital
roundingstructures.ThemostprevalentsymptomofTMDispain.Thepainisusuallylimitedtothemusclesofmasti-cationandthepre-auricularareaandhasbeendescribedasjawpain,earache,headache,andfacialpain.Thepainmay be exacerbated by chewing and other jaw move-ments.ManypatientswithTMDhaveclickingorpoppingsoundswhentheyopenandclosetheirjaw.9Upto75%oftheworld’spopulationhasatleastonesignofjointdysfunc-tionanduptoonethirdhaveatleastonesymptom.10,11ThemostcommonformofTMDisarticulardiscdisplacement,whichoccurswhenthediscisabnormallypositionedinre-lation to thecondylarhead.9Anteriordisplacement is themostcommonposition.12This typeofTMDisnotusuallyassociatedwithpainorlimitedjawmovementandthereforedoesnottypicallyrequiretreatment.13
AccordingtotheliteraturetherehavebeennocitedcasesofRHSmanifestingwithTMJpain.14WereportapatientinwhompainduetoRHSinconjunctionwithsignsgenerallyassociatedwithTMD,ledtoadelayincorrectdiagnosis.
Case ReportA43-year-oldwomanpresentedtotheColumbiaUniversityCenter forOral,Facial,andHeadPain,witha4-dayhis-toryofgraduallyincreasingright-sidedTMJpain,whichwasmostsevereinthepre-auricularregion.Shehadnofever,vomitingorneurologicsymptoms.Chewingandpressureresultedinexacerbationofpain.Twodayspriortopresen-tation she had been diagnosed with TMD and was pre-scribedIbuprofen(600mgTID)andValium(5mgs)forpainmanagement.Herpastmedicalhistorywassignificantforchildhoodvaricellainfection.Onexamination,thepatientreportedpainintherightpre-auricular area upon active mouth opening and left lat-erotrusivemovement.Activemouthopeningwasrestrictedto43mmwithslightdeviationtotherightside.Maximumopeningcouldbestretchedto46mmandwasassociatedwithanincreaseinpain.PalpationoftherightTMJcapsulewasalsoassociatedwithanincreaseinpain.Thepainwasdescribedasburning,stinging,andstabbing.TherewasanaudiblereciprocalclickingoftherightTMJthatwaselimi-natedby1mmofopening.Additionally,therewaspainonpalpationoftherightmasseterandtemporalismuscles,aswell aspain to light touch in the rightpre-auricular area.CranialnervesII-XIIwereotherwiseintact;pupilswereequal

©2010ColumbiaDentalReview Volume14:2009-201025
Ramsay Hunt Syndrome presenting as TMD: A Case Report
andreactivetolight,andstrengthandsensationwerenor-mal.Erythemaandslightrashwerepresentoverthecon-chaandantihelixoftherightear.(Figure1)Thediagnosisofherpeszosterwasmadeandthepatientwasprescribedoralacyclovir.FurtherdiagnosesofTMJdiscdisplacementandcapsulitis, aswell asmyofacialpainwasmade,andtreatmentwasdeferreduntilaftertheherpeszosterinfec-tioncouldbemanaged.
Fourdayslater,thepatientreturnedtotheclinicwithwors-eningsymptoms.Shehadnot taken theprescribedacy-clovirandreportedincreasedpainintherightpre-auricularregion,inabilitytocloseherrighteye,vertigo,andtinnitus.Therewerevesiclespresentovertheconchaandanti-helixoftherightearandtherewasright-sidedfacialweakness.ThediagnosisofRamsayHuntsyndromewasconfirmedandthepatientwasadmittedtothehospitalforintravenousacyclovirandsteroids.MRIwithcontrastrevealedmildlin-earenhancementoftherightinternalauditorycanalconsis-tentwithenhancementalongthe7thand8thcranialnervesandthroughouttheremainderofthe7thcranialnerve.At1-monthfollow-up,thepatient’ssymptoms,includingthevesicles,facialweakness,TMJpain,andmyofacialpain,hadresolved.Allthatremainedofher initialcomplaintwastheright-sidedTMJclicking,whichdidnotrequiretreatment.
Discussion and ConclusionRamsayHuntsyndromeisdiagnosedclinicallyasperiph-eralfacialnervepalsyinassociationwithzosterotitis.3ThisdiagnosisisbasedonpatienthistoryofpreviousVZVinfec-tionandneurologicalexamination.3 Ithas longbeenheldthatthissyndromeisduetoreactivationoftheVZVinthegeniculateganglionresultinginvariousneuropathicsymp-tomsfromthenervesleavingthisganglion.5Variousstud-ieshavereportedRHSinassociationwithconcurrentVZV
Figure 1Erythema and slight rash were present over the concha and antihelix of the right ear
infectionsinCNVIII,IX,X,XI,XIIanduppercervicalnervesthatstemfromwidespreadcontaminationofVZVvianerveanastomoses2orconnectingbloodvessels.15ThedifficultywithdiagnosingRHSisusuallyduetoitssimi-larity toBell’spalsy,especiallywhen thevesicular rash isabsent.ThisformisknownasRHSzostersinehepeteandinrecentstudieshasbeenshowntoaccountforupto19%ofBell’sPalsydiagnoses.16Fortunately,therearefewnega-tiveconsequencesofmisdiagnosingRHSforBell’spalsyasstudiesshowthatbotharetreatedeffectivelywithpred-nisoneandacyclovir.
However,missingadiagnosisofRHSduetoTMD,whichisarareoccurrence,canhavenegativeconsequences.Aswasstatedearlier, earlydetectionand treatment ispara-mountindecreasingtheprobabilityofpermanentneuropa-thiesassociatedwithRHS.RHSandvariousformsofTMDmayincludesymptomsofpaininandaroundtheear.Al-thoughthiscasemanifestedthehallmarksignsofRHS,itisuniqueinthatthepatientpresentedwithTMJpainaswell.Itislikelythatthepatient’sTMJdiscdisplacementexistedpriortoherRHSpresentationandaccordinglyitcontinuedafterhersymptomshad resolved. It ispossible thatpainfromthelocalizedinflammationassociatedwithRHSwasworsenedby jawmovement, leading tomuscleguardingandsubsequentlymorepain.ThepainwaslocatedinthemasticatorymusclesandaroundtheTMJ,bothofwhicharecommonfeaturesofTMD.ThesesymptomsmaymaskthediagnosisofRHS;however,TMDisnotassociatedwithallodynia, rash,vesicles,or facialnerveweakness.Theseclinical signs and symptoms are not usually associatedwithTMDandshouldpromptthecliniciantoconsideral-ternatesourcesforapatient’spaincomplaint.Whilecon-servativemanagement,includingNSAIDs,isoftenthefirststepinmanagingTMDsymptoms,inacasesuchasthis,anincompletediagnosiscoulddelaypropertreatmentandtherebynegativelyaffectthepatient’sprognosisforfullre-covery.AfterthecorrectdiagnosisofRHSwasdeterminedandtreated,allsymptoms,includingthemyofacialpainandTMDassociatedpainhad resolved.Theclinician treatingpatientswithTMDmustbeawareofconditionsthatshouldbe included in the differential diagnosis, especially whentherearesignsorsymptomsthatarenotexplainedbyprob-lemsinvolvingthetemporomandibularjointorsurroundingmusculature.Thesecharacteristicsmustbefullyexaminedandanalyzedtoobtainaproperdiagnosisandhavetheap-propriatetreatmentapplied.

©2010ColumbiaDentalReviewVolume14:2009-2010 26
Ramsay Hunt Syndrome presenting as TMD: A Case Report
References1.SweeneyCJ,GildenDH(2001)RamseyHuntsyndrome.J Neurol Neurosurg Psychiatry71:149-154.
2.HuntJR(1910).Thesymptomcomplexoftheacutepos-teriorpoliomyelitisofthegeniculate,auditory,glossopharyn-gealandpneumogastricganglia.Arch Intern Med5:631-75.
3.SweeneyCJ,GildenDH(2001)RamseyHuntsyndrome.J Neurol Neurosurg Psychiatry71:149-154.
4.DevriesePP,MoeskerWH(1988)Thenaturalhistoryoffa-cialparalysisinherpeszoster.Clin Otolaryngol13:289-298.
5.HuntJR(1907)OnHerpeticinflammationsofthegenu-culateganglion:anewsyndromeanditscomplications.J Nerv Ment Dis 34:73-76.
6.HuntJR(1937)Geniculateneuralgia:afurthercontribu-tiontothesensorysystemofthefacialnerveanditsneural-gicconditions.Arch Neurol Psychiatry37:253-85.
7. Murakami S, Hato N, Horiucho J (1997) Treatment ofRamsey Hunt with acyclovir-prednisone; significance ofearlydiagnosisandtreatment.Ann Neurol41:353-357.
8.OkesonJP(2005).Bell’sOrofacialPained5.Chicago,Quintessence.
9.DeLeeuw(2008).OrofacialPain:GuidelinesforAssess-ment,DiagnosisandManagement4thed.Illinois,Quintes-sencePublishingCo,Inc.
10.RughJD,SolbergWK(1985)OralhealthstatusintheUnitedStates:Temporomandibulardisorders.J Dent Educ 398-404.
11.SchiffmanE,FrictonJR(1988)EpidemiologyoftheTMJandcraniofacialpain.In:TMJandCraniofacialPain:Diag-nosisandManagement(JRFrition,RJKroening,KMHa-thaway,Eds).StLouis,IEA,pp1-10.
12. Isberg-HolmAM,WestessonPL (1982)Movementofthediscandcondyleintemporomandibularjointswithclick-ing:Anarthrographicandcineradiographicstudyonautop-syspecimens.Acta Odontol Scand40:151-164.
13. Lamster, Ira B; Northridge, Mary E (2008) ImprovingOralHealthfortheElderly:AnInterdisciplinaryApproach.NewYork,NY,USA:SpringerNewYork.
14.AkyolA,KiyliogluN,CopcuE(2006)Anunusualcauseoftrismus:ramsayhuntsyndrome.J Plast Recontr Aesther Surg59(2):206-207.
15.LapreselJ,LasjauniasP(1986)Cranialnerveischaemicarterialsyndromes.Brain109:207-215.
16.MurakamiS,HondaN,MizobuchM(1998)Rapiddiag-nosisofvaricellazolstervirusinfectioninacutefacialpalsy.Neurology51:1202-1205.

©2010ColumbiaDentalReview Volume14:2009-201027
AbstractVACTERLassociationisanassociationofcongenitalanom-alies,whichoccurtogetherwithenoughfrequencythattheirsimultaneouspresentationcannotbeattributedtorandomchance.Thiscasedescribesthedentalfindingsofa3-year-oldmalewithVACTERLassociationthatpresentswithbili-rubin-discolored teeth,gingivalovergrowth,andabundantcalculus.Inthisreportweconsidertheuniquedentalchal-lenges that facepatientswith this association, aswell asvariousmethodsinapproachingtheiroralhealthcare.
Introduction ‘Associations’areusedtodescribetheexistenceofaspe-cificsetofmalformationsthattendtooccurtogethermorefrequentlythancanbeattributedtochance.Onesuch‘as-sociation’ isVATERassociation, inwhichpatientspresentwithanon-randomgroupofcongenitalanomaliesthatin-clude:defectsofthevertebrae(v),analatresias(a),tracheo-esophagealfistulasandatresiasoftheesophagus(te),andrenalandradiallimbabnormalities(r).Recently,ithasbeensuggestedthatVATERassociationbeexpandedtoincludecongenital heart lesions (c) and limb defects (l), and canthusbereferredtoasVACTERLassociation.1Diagnosisre-quiresthepresenceofatleastthreeofthepreviouslylistedelements.2CleftlipandpalatealsopresentmoreoftenthanwouldbeexpectedinpatientswithVACTERLassociation.3ThedegreeofinvolvementofanyoneelementofVACTERLassociation is case-dependent, and consequently, eachpatientistrulydistinct.2,4Theunderlyingcausesofthisas-sociationremaintobeelucidated.1
Earlydocumentationofthisgroupofassociatedbirthde-fects appeared more than 30 years ago,5-9 and the inci-denceofeachassociatedcomponenthasnotbeenwellquantifiedincontemporaryliterature.ThevastspectrumofanomaliesthatexistinVACTERLassociationmakeitverydifficulttocreateaprecisedefinitionfortheassociationandthustodevelopstudieswiththeappropriatepatientpopula-tions.10Inaddition,therearemanyVACTERL-likecasesthatpresentfeaturesoftheassociation,whichmayhaveactu-allyresultedfromothersyndromesorsinglegenedisorderssuch as Feingold, Charge, Townes-Brocks, Pallister-Halland 22q11 deletion syndromes, as well as Fanconi ane-mia.11Thesefactorsmakeitverydifficulttoobtainaccurateinformationandstatisticsforthisassociation.10
VACTERLassociationaffectsabout1 in5,000 livebirthsandhasbeenhypothesized tooriginate from themidline
developmentalfielddue toerrors inblastogenesis.1,12Theetiology remainsunclearbut isbelieved tobemultifacto-rial.Certainchromosomaldefectsanddeletionshavebeenfound inpatientswithVACTERLassociationbut, todate,nosinglechromosomalabnormalityhasbeen implicated.Additionally,ithasbeenproposedthatexposuretocertainenvironmentalfactorsduringpregnancy,suchassexhor-mones,canalsoinfluencethisassociation.3
Patientscanoftenbeidentifiedashavingeitherthe‘cranial’or‘caudal’phenotypeoftheassociation.Thecranialphe-notypeoftenpresentswithesophagealatresia,defectsofthepreaxiallimbs,andmalformationsofthethoracicverte-brae.Incontrast,thecaudalphenotypefrequentlyincludesdefects of the lower vertebrae, renal malformations, analatresias,andpossiblegeneticanomalies.2
Children born with this association often require urgentsurgicalinterventionimmediatelyafterbirthbecauseoftheforegut and hindgut anomalies.12 Approximately 70 per-centofpatientswithVACTERLassociationareaffectedbyesophageal atresia with tracheo-esophageal fistula (EA/TEF).13SeveralcomplicationsarepossibleaftercorrectionofEA/TEF,suchasrespiratoryproblems–respiratoryar-rest, apnea,bradycardia, andaspiration– leading tonu-merousboutsofpneumonia.10Upto75percentofpatientswith VACTERL association have been reported to havecongenitalheartdisease.Themostcommonheartdefectsseen with the association are ventricular septal defects(VSD), atrial septal defects, andTetralogyof Fallot (TOF).Lesscommondefectsaretruncusarteriosusandtranspo-sitionofthegreatarteries.Patientsmayhaveamurmuratbirth,however,absenceofamurmurdoesnotruleoutcon-genitalheartdisease.13 Ifapatient issuspectedofhavingtheassociation,aconsultationwithapediatriccardiologistis recommendedtodeterminewhetherantibioticprophy-laxisaccordingtotheAmericanHeartAssociationguide-lines is required.13PatientswithVACTERLassociationdonottypicallypresentwithlearningdisabilitiesorgrowthab-normalities,nordotheyshowdysmorphicfacialfeatures.11ThefollowingcasepresentsinterestingdentalfindingsinapediatricpatientwithVACTERLassociation.
Case ReportA3-year-oldmalepatientwithamedicalhistorysignificantforVACTERLassociation,TetralogyofFallot(TOF),gastro-esophagealreflux,andasthmapresentedtothepediatricdentalresidencyclinicatColumbiaUniversityMedicalCen-
VACTERL Association: A Dental Case StudyJenniferL.Wilbur1,SueHwang,DMD2,RichardYoon,DDS3,StevenChussid,DDS4
1Classof2011,CollegeofDentalMedicine,ColumbiaUniversity,NewYork,NY22ndYearResident,DivisionofPediatricDentistry,CollegeofDentalMedicine,ColumbiaUniversity,NewYork,NY3AssistantProfessor,ProgramDirector,PediatricDentistryResidency,CollegeofDentalMedicine,ColumbiaUniversity,NewYork,NY4AssociateProfessorandDirector,DivisionofPediatricDentistry,CollegeofDentalMedicine,ColumbiaUniversity,NewYork,NY

©2010ColumbiaDentalReviewVolume14:2009-2010 28
VACTERL Association: A Dental Case Study
terforcomprehensivedentalcare.Thepatient’spastsurgi-cal history includeda liver transplant andcorrectiveTOFrepairin2006.Thepatienthadatracheotomyandgastros-tomytube.Hewastakingcyclosporineandantibioticpro-phylaxis,whichisrecommendedpriortoalldentalproce-duresthatinvolveperforationoforalmucosa,manipulationofgingiva,ortreatmentofapicalregionsoftheteeth.
Oralexamination(Figure 1A-C)revealedanormalcomple-mentofprimary teethwithevidenceofgeneralized toothdiscoloration, early childhood dental caries, generalizedcalculusaccumulation,andgingivalovergrowth.Extra-oralexaminationexhibitedfindingsthatwerewithinnormallim-its.Thepatientwasunabletohaveanydentaltreatmentinanambulatorysettingduetohisacutestressreactionandmedicalcondition.Consequently,dentaltreatmentsweretobeperformedintheoperatingroomundergeneralanes-thesiatoeliminateinfectionandpreventunnecessarypainorprolongedsuffering.
Followingmedicalclearance,thepatientreceivedcompre-hensive dental care under general anesthesia (Children’sHospital,NewYork).Thetreatmentincluded:extra-oralandintra-oralexaminations,dentalradiographs,dentalprophy-
Figure 1(A) Frontal view reveals green intrinsic staining of all primary teeth caused by hyperbilirubinemia during dentin development. Gingival soft tissue reveals generalized inflammation in response to calculus build-up. (B) Upper left quadrant of a patient with VACTERL association revealing calculus on the occlusal surfaces of molar teeth. Gingivitis in response to calculus accumulation and generalized staining of the teeth and can also be seen. (C) Gingival overgrowth caused as a negative side effect of cyclosporine use along with superimposed gingival inflammation is visible here.
A
B C
laxis,scaling,multipledentalrestorations,andgingivecto-mies at four sites. Radiographs revealed and confirmednormaldevelopingteeth.Nopost-treatmentcomplicationswerenoted.After theprocedureswereperformed in theoperatingroom,thepatientpresentedforfollow-upatthepediatricdental residencyclinic.Recent extra- and intra-oral examinations revealed intact dental restorations anduneventfulhealingofwoundsites.
DiscussionWhentreatingpatientswithVACTERLassociation,itises-sential to identify associated defects and treat them ac-cordingly. This patient had congenital cardiac anomaliesandtracheo-esophagealfistula,andcanthusbeidentifiedashavingthecranialphenotypeofthisassociation.Asare-sultofbeingbornwithaTEF,healsopresentedwithagas-trostomytube.Ithasbeenpostulatedthatwhenagastros-tomytubeisplacedinapatientwithEAorTEF,thepressureof the loweresophagealsphinctercanbecompromised,leadingtogastroesophagealreflux(GERD).14Thepatient’smedicalhistorywassignificantforGERD,whichincreasedhisriskfordentalcaries.GERDmaycauseenamelerosionand is associated with higher S. mutans counts, of 106CFU’s/mlorabove,causingpatientstohavenotablyhigherdmftscoresthanpatientswithoutreflux.15
Greenintrinsicstainingofalloftheprimaryteethwasnotedinthepatient’sintra-oralexamination.Greenpigmentationlikely resulted from hyperbilirubinemia which occurred inconjunctionwith thepatient’s hepatic problemsand livertransplant.Bilirubin, oneof thebreakdownproducts thatresultsfromdegradationofredbloodcells,causesjaundiceathighbloodconcentrations.16Thebilirubinispermanentlytrappedindentinduringthetoothmaturation/mineralizationprocess,producinggreenstainedbandsthatappearontheteeth.17
Furthermore,dueto livertransplantation,thispatientmusttakecyclosporine,animmunosuppressantusedtopreventorganrejection.Cyclosporineusecancausegingivalover-growthand isassociatedwithmanyoral lesions,suchashairyleukoplakia,andincreasedoccurrenceofviralandfun-galinfections.Ofalloralproblems,gingivalovergrowthisthemostcommon.18Thispatient’sgingivalovergrowthwasex-acerbatedbyincreasedplaqueandcalculusaccumulation.
Treatmentoptionsforbothhyperbilirubinemiaandgingivalovergrowthdoexist.Toconceal thegreenstainingasso-ciatedwithhyperbilirubinemiaandimproveesthetics,resincrownsandresinveneersoftenserveasthebestoptions.Whiteningdoesnotdecreasethegreenpigmentationbe-causeitisconfinedtothedentin.17Gingivalovergrowthcanalsobereducedbyimprovedoralhygiene,gingivectomies,andtheuseofantimicrobialrinses.18

©2010ColumbiaDentalReview Volume14:2009-201029
VACTERL Association: A Dental Case Study
PatientswithVACTERLassociationshouldbeseenatfre-quentintervalsforscalingandprophylaxisinordertomain-tainoralhealth.Parent-assistedtoothbrushingandflossingshouldbeemphasizedtodecreaseplaqueaccumulation.Sincefungalinfectionsarecommoninthosetakingcyclo-sporine,topicalapplicationofantimicrobialrinsesmayhelptopreventtheseinfections.Withregularandfrequentoralexaminations, oral health can be better maintained andproblemscanbeaddressedpromptly.
ConclusionDuetothewiderangeofmanifestationsofVACTERLasso-ciation,theexactincidencewithinthepopulationisstillun-known.1Exceptincaseswithseveredefects,patientswithVACTERL association can lead normal productive lives.11Hence,thedentistmustbeawareoftheoralmanifestationsofapatient’sunderlyingmedicalconditionandtheneces-sarymodificationsintreatmentofsuchpatientswithexten-sivemedicalhistories,suchasVACTERLassociation.
References1. Kallen K, Mastroiacovo P, Castilla E, Kallen B (2001).VATER Non-random association of congenital malforma-tions:studybasedondatafromfourmalformationregisters.Am J Med Genet.101(1):26-32.
2.BottoLD,KhouryMJ,MastroiacovoP,CastillaEE,MooreCA,SkjaervenR,MutchinickOM,BormanB,CocchiG,CzeizelAE,GoujardJ,IrgensLM,LancasterPA,Martinez-FriasML,MerlobP,RuusinenA,StollC,SumiyoshiY(1997).ThespectrumofcongenitalanomaliesoftheVATERasso-ciation:aninternationalstudy.Am J Med Genet.71(1):8-15.
3.deJongEM,FelixJF,DeurlooJA,vanDoorenMF,Ar-onsonDC,TorfsCP,HeijHA,TibboelD(2008).Non-VAC-TERL-typeanomaliesarefrequentinpatientswithesopha-geal atresia/tracheo-esophageal fistula and full or partialVACTERL association. Birth Defects Research. Part A,Clinical and Molecular Teratology.82(2):92-7.
4.LawhonSM,MacEwenGD,BunnellWP(1986).Ortho-paedicaspectsoftheVATERassociation.J Bone Jt Surg, Am.68(3):424-429.
5.QuanL,SmithD(1973).TheVATERassociation.Verte-braldefects,analatresia,T-Efistulawithesophagealatre-sia, radial and renaldysplasia: a spectrumof associateddefects.J Pediatr.2:104-107.
6.SmithD(1974).TheVaterassociation.Am J Dis Child 128:767.
7.TemtamyS,MillerJ (1974).ExtendingthescopeoftheVATERassociation:definitionoftheVATERsyndrome.J Pe-diatr.85:345-349.
8.BarnesJ,SmithW(1978).TheVATERassociation.Radi-ology126:445-449.
9.BarryJ,AuldistA(1974).TheVaterassociation;oneendofaspectrumofanomalies.Am J Dis Child.128:769-771.
10.HatemiAC,GursoyM,CevikerK,TongutA,CetinG,CelebiS,KansizE(2008).VentricularseptaldefectclosureinapatientwithVACTERLsyndrome:anticipatingsequel-aeinararegeneticdisorder.Texas Heart Institute Journal. 35(2):203-5.
11.Shaw-SmithC (2006).Oesophageal atresia, traqueo-oesophageal fistula and VACTERL association: review ofgeneticsandepidemiology.J Med Genet43:545-554.
12.RittlerM,PazJE,CastillaEE(1996).VACTERLAssocia-tion,EpidemiologicDefinitionandDelineation.Am J Med Genet.63:529-536.
13. “VACTERL or VATER Association: Causes, Defects,Heart Problems and Prognosis.” Cincinnati Children’sHospitalMedicalCent.http://www.cincinnatichildrens.org/health/heart-encyclopedia/disease/syndrome/vacterl.htm. AccessedJanuary2nd,2009.
14.LittleDC,RescorlaFJ,GrosfeldJL,WestKW,SchererLR,EngumSA(2003).Long-termanalysisofchildrenwithesophagealatresiaandtreacheo-esophagealfistula.Jour-nal of Pediatric Surgery.38(6):852-6.
15.AlfaroEV,ApsJK,MartensLC(2008).Oralimplicationsin childrenwithgastroesophageal refluxdisease.Current Opinion in Pediatrics20(5):576-83.
16.AltoLA,PomaricoL,SouzaIP,JaniniME(2004).Greenpigmentation of deciduous teeth: report of two cases. J Dent Child.71(2):179-182.
17.AmaralTH,GuerraCdeS,Bombonato-PradoKF,Gar-ciadePaulaESilvaFW,deQueirozAM(2008).Toothpig-mentationcausedbybilirubin:acasereportandhistologi-calevaluation.Spec Care Dentist.28(6):254-7.
18WrightG,WelburyRR,HoseyMT(2005).Cyclosporin-inducedgingivaloergrowthinchildren.IntJPaediatrDent.15(6):403-11.

©2010ColumbiaDentalReviewVolume14:2009-2010 30
Chin Block Bone Graft in Patient Congenitally Missing Maxillary Lateral Incisors Prior to Implant Placement: A Case ReportStephanieDumanian1,JulieLamureDDS2
1Classof2011,CollegeofDentalMedicine,ColumbiaUniversity,NewYork,NY23rdYearResident,DivisionofPeriodontics,CollegeofDentalMedicine,ColumbiaUniversity,NewYork,NY
AbstractInsufficient alveolar bone can hinder successful implantplacement,compromisingimplantpositioningandstability.Variousregenerativeproceduresareavailabletorepairhardtissue defects. Ridge augmentation techniques includeguidedboneregeneration,andridgeexpansion.Thetypesof bone grafts include synthetic bone substitutes, xeno-grafts,allografts,andautogenousbonegrafts.Becauseoftheirbiocomptabilityandosteogenic,osteoconductive,andosteoinductive potential, autogenous bone grafts are thegoldstandardofbonegraftmaterials.Inthiscasereport,anautogenouschinblockgraftwasusedtoresolvemaxillaryhorizontal ridgedeficiencyatsitesofcongenitallymissing#7and#10prior to implantplacement.A two-stageap-proachwasemployedwithimplantplacementsixmonthsafterridgeaugmentationsurgery.Onaverage6mmofal-veolarbonewidthwasgained.Implantswereplacedinanidealpositionandwerestableafterplacement.
IntroductionSafetyandaestheticsofimplantplacementmaybecom-promisedifsufficientboneheight,width,ordensityisnotavailable.Trauma,toothloss,orinfectioncancontributetoinsufficientbonevolume,preventingthesuccessfulplace-mentofimplants.Accordingtoclinicalevidence,aminimumof5to6mmalveolarwidthisrequiredforplacementofim-plants.1Inparticulartheanteriormaxilladisplayslessdenseboneandsmallervolumeofbonethanthemandible,oftennecessitating a bone graft prior to implant placement.2,3Theseboneaugmentationproceduresmayincludesocketpreservation,horizontalorverticalridgeaugmentation,andsinusaugmentation.
The type of bone augmentation procedure and materialusedoftendependonthetypeofalveolarridgedeformity.Seibert has classified the types of alveolar ridge defectsinto3categories:aClass Idefect isdescribedasa lossofbucco-lingualwidth,ClassIIdescribesalossofapico-coronalridgeheight,andClassIIIdescribesalossofbothapico-coronalheightandbucco-lingualwidth.4
Therehavebeenvariousproceduresdescribedtoincreaseverticalandhorizontaldimensionsofalveolarboneaswellasdensity.Ridgeaugmentationtechniquesincludeparticu-lategrafting,membraneuse,blockgrafting,anddistractionosteogenesis,eitheraloneor incombination.2,5Thetech-
niquechosenoftendependson theextentof thedefectandthespecificprocedurestobeperformed.5Bonegraftscanbecategorizedasautograft,allograft,xenograft,andalloplast.Syntheticgraftmaterialsaredefinedasalloplasts.Anallograft isagraftfromanon-identicalmemberofthesamespecies,oftencadavericbone,whileaxenograft isagraftfromadifferentspecies,oftenbovine.Autogenousbone,ontheotherhand,isfromthesameindividualandrequiresbonetobeharvestedatthetimeofsurgeryfromasecondsurgicalsite.Thesurgerycanbesomewhatin-vasiveandasaresult,somepatientsprefertheuseofal-lograftsorxenograftsasanalternative.
Manycliniciansviewanautogenousbonegraftasthegoldstandardsinceitisosteogenic(hastheabilitytoformbone),osteoconductive(hastheabilitytoserveasascaffoldforbone regeneration) and most importantly, osteoinductive(iscapableofinducingboneformation).6Autogenousbonehasbeenharvestedfromawiderangeofsitesincludingtheanteriorandposteriorcrestsoftheileum,calvarium,tibia,fibula,scapula,ribs,maxillarytuberosity,mandibularretro-molararea,ramus,andmandibularsymphysis.Whileintra-oralsiteshavetheadvantageofbeinglessinvasive,extra-oralsites,suchasiliaccrest,craniumortibia,arenecessaryifbonedefectsexceed2cm.5Ifbonedefectsarelessthan2cm,intraoralsitessuchasmandibularsymphysisandra-musarepreferred.Oneclinicanevenreportedusingmaxil-larytuberosityforbonegraftsexplainingthatinsituationsoftuberosityovergrowth,itservedasalargevolumeofboneeasilyharvestedwithfewcomplications.7Inadditiontotheease of intraoral harvest, grafts derived from intramem-branousbone (suchaspart of the ramusand theman-dibularsymphysis)havelessresorptionthanendrochondralbone.3,5Sincehealingofbonegraftsisdependentonan-giogenesisandrevascularization,corticocancellousblocksarepreferredtocorticalblockssincerevascularizationoc-cursfasterintheformer.5Themostcommonintraoralsitesdescribedarethemandibularsymphysisandramusfromwhichcorticocancellousboneisharvested.1
Mostsuccessfulridgeaugmentationmethodsincludetheplacementofamembraneontopofagraft,preferablyanautogenousbonegraft, tohelpguidebonegrowth.Thistechniqueiscalledguidedboneregenerationandisbeingusedsuccessfullybymanyclinicianstoachievefavorableridgeaugmentationresults.1

©2010ColumbiaDentalReview Volume14:2009-201031
Chin Block Bone Graft in Patient Congenitally Missing Maxillary Lateral Incisors Prior to Implant Placement: A Case Report
Ridge augmentation and implant placement techniquescanoccurviaaone-stagesimultaneousapproachoratwo-stageapproach.Duringthesimultaneousapproachtheim-plantisplacedinthesamevisitasthebonegraft,whileinthetwostageapproach,thebonegraftisallowedtohealandtheimplantisplacedsixmonthslater.Bothtreatmentoptionsarebeingusedandwhiletimeandmoneymaybesavedwithsinglestagetherapy,thetwostagetechniquehasreportedbetterpositioning,stability,andintegrationoftheimplant.8
Case ReportA 29-year-old male was referred to Columbia College ofDentalMedicineforanimplantconsultation(Figure 1).Hismedicalhistorywasnoncontributory.Thepatientpresentedwithcongenitallymissingmaxillary lateral incisors#7and#10andwasinterestedinhavingimplantsplaced.HehadcompletedInvisaligntreatmentleavingsufficientmesio-dis-talspaceforimplantsandworeaflipper.
Thepatientwasreferredforconebeamcomputedtomog-raphy scan (CBCT) constructed using Xoran and Visionsoftware.AfteranalysisoftheCBCTscanthepatientwasdiagnosedwithbilateralhorizontalridgedefectsatsites#7and#10(Figure 2).Thepatienthadsufficientverticalheightforplacementofimplants.ThedefectswerediagnosedasClassI(according to the Seibert classification).4
Figure 1Initial record. Arrows show large labial ridge defects at site of congeni-tally missing lateral incisors (#7 and #10).
Thepatientwasthentreatmentplannedforatwostageap-proach to lateral ridge augmentation with autogenous bonegraftsfromthemandibularsymphysis.Fullthicknessflapswerereflectedfrombelowteeth#22to#27andtwo10x7mmcorti-cocancellousboneblockswereharvested5mmapicaltoman-dibularroots(Figure 3).HarvestsiteswerefilledinwithBio-Oss.
Figure 2 Initial CBCT pre-op prior to grafting of #7 (left scan) and #10 (right scan). Arrows show large labial defect. Width of defect at site #7 measures 2.3 mm and at site #10 measures 2 mm.
Figure 3Left image shows donor site after full thickness flap. Right image shows donor site with two 10 x7 mm blocks designed.
Maxillary recipient sites were prepared for placement ofgraftswitha full thicknessflapfromteeth#5to#12.Therecipient sites were decorticated and bone blocks wereshapedandfixedwith1.5x7mmfixationscrews(Figure 4). Autogenous particulate bone and Bio-oss® were placedaroundbothblockstofillanyvoids.Anabsorbableextracel-lularcollagenmatrixmembrane,Dynamatrix®,wasplacedoverbothblockgraftsandtheflapswerereplaced.
Figure 4Left image shows decortications of recipient site. Right image shows placement of chin block graft in sites # 7 and #10 with fixation screws
Thepatientwasfollowedupatregularvisitsandgraftsap-pearedstablebothclinicallyandradiographically.(Figure 5)
Figure 5Two months post-op. Labial ridge defects have been greatly reduced. On average 4-5mm bone has been gained.
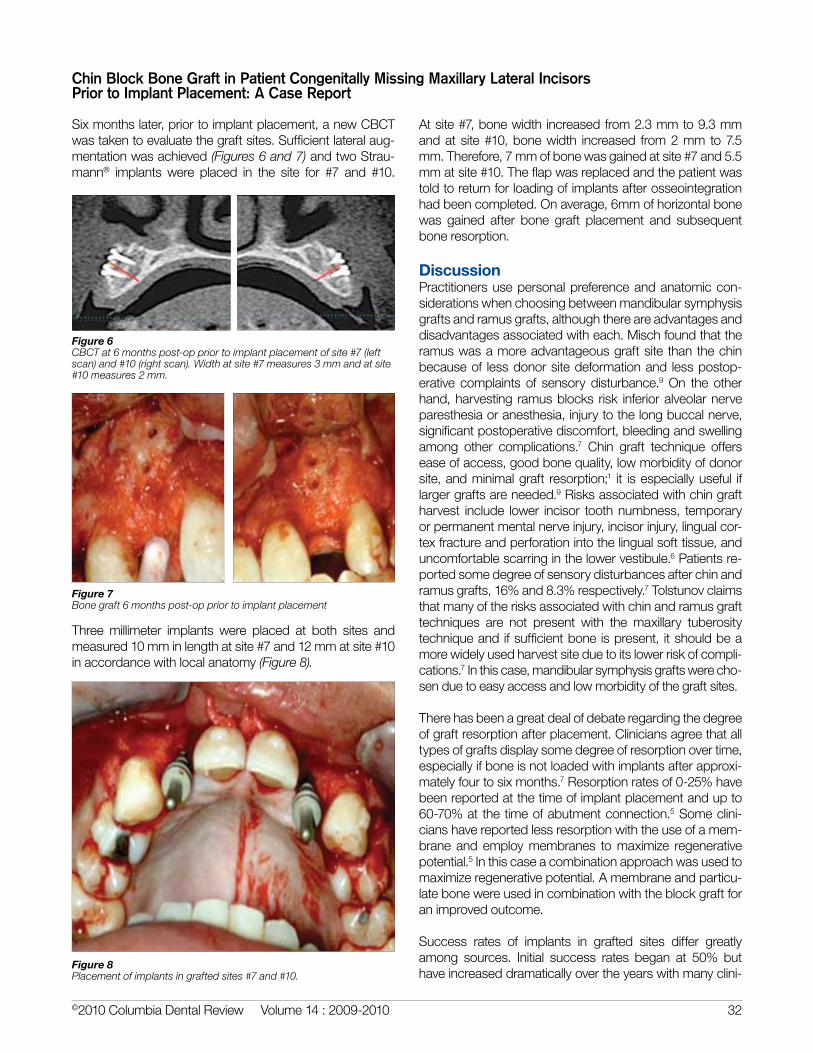
©2010ColumbiaDentalReviewVolume14:2009-2010 32
Chin Block Bone Graft in Patient Congenitally Missing Maxillary Lateral Incisors Prior to Implant Placement: A Case Report
Sixmonthslater,priortoimplantplacement,anewCBCTwastakentoevaluatethegraftsites.Sufficientlateralaug-mentationwasachieved(Figures 6 and 7)andtwoStrau-mann® implants were placed in the site for #7 and #10.
Figure 6 CBCT at 6 months post-op prior to implant placement of site #7 (left scan) and #10 (right scan). Width at site #7 measures 3 mm and at site #10 measures 2 mm.
Figure 7Bone graft 6 months post-op prior to implant placement
Three millimeter implants were placed at both sites andmeasured10mminlengthatsite#7and12mmatsite#10inaccordancewithlocalanatomy(Figure 8).
Atsite#7,bonewidthincreasedfrom2.3mmto9.3mmandatsite#10,bonewidth increased from2mmto7.5mm.Therefore,7mmofbonewasgainedatsite#7and5.5mmatsite#10.Theflapwasreplacedandthepatientwastoldtoreturnforloadingofimplantsafterosseointegrationhadbeencompleted.Onaverage,6mmofhorizontalbonewas gained after bone graft placement and subsequentboneresorption.
DiscussionPractitionersusepersonalpreferenceandanatomiccon-siderationswhenchoosingbetweenmandibularsymphysisgraftsandramusgrafts,althoughthereareadvantagesanddisadvantagesassociatedwitheach.Mischfoundthattheramuswasamoreadvantageousgraftsitethanthechinbecauseof lessdonorsitedeformationand lesspostop-erative complaints of sensorydisturbance.9On theotherhand,harvesting ramusblocks risk inferioralveolarnerveparesthesiaoranesthesia,injurytothelongbuccalnerve,significantpostoperativediscomfort,bleedingandswellingamong other complications.7 Chin graft technique offerseaseofaccess,goodbonequality,lowmorbidityofdonorsite,andminimalgraft resorption;1 it isespeciallyuseful iflargergraftsareneeded.9Risksassociatedwithchingraftharvest include lower incisor toothnumbness, temporaryorpermanentmentalnerveinjury,incisorinjury,lingualcor-texfractureandperforationintothelingualsofttissue,anduncomfortablescarringinthelowervestibule.6Patientsre-portedsomedegreeofsensorydisturbancesafterchinandramusgrafts,16%and8.3%respectively.7Tolstunovclaimsthatmanyoftherisksassociatedwithchinandramusgrafttechniques are not present with the maxillary tuberositytechniqueandifsufficientboneispresent, itshouldbeamorewidelyusedharvestsiteduetoitslowerriskofcompli-cations.7Inthiscase,mandibularsymphysisgraftswerecho-senduetoeasyaccessandlowmorbidityofthegraftsites.
Therehasbeenagreatdealofdebateregardingthedegreeofgraftresorptionafterplacement.Cliniciansagreethatalltypesofgraftsdisplaysomedegreeofresorptionovertime,especiallyifboneisnotloadedwithimplantsafterapproxi-matelyfourtosixmonths.7Resorptionratesof0-25%havebeenreportedatthetimeofimplantplacementandupto60-70%atthetimeofabutmentconnection.5Someclini-cianshavereportedlessresorptionwiththeuseofamem-braneandemploymembranes tomaximize regenerativepotential.5Inthiscaseacombinationapproachwasusedtomaximizeregenerativepotential.Amembraneandparticu-latebonewereusedincombinationwiththeblockgraftforanimprovedoutcome.
Success rates of implants in grafted sites differ greatlyamong sources. Initial success rates began at 50% buthaveincreaseddramaticallyovertheyearswithmanyclini-
Figure 8Placement of implants in grafted sites #7 and #10.

©2010ColumbiaDentalReview Volume14:2009-201033
cians reportingsurvival ratesbetween81.2%and100%.1,6Somehavereportedhighersuccessrateswithdelayedimplantplacementafterbonegraftandalsodelayed im-plant loading.Factorssuchassmokinganduncontrolleddiabetescanalsogreatlydiminishsuccess rates.7There-fore,patientselectionisveryimportantinimplantsuccess.
Coordinating treatmentwithpatients’ expectations is justasimportantaspatientselectionwhentreatmentplanningapatientforaboneaugmentationprocedure.Althoughau-togenousboneisthegoldstandard,itisnotthestandardofcarebecauseapatient’smedicalconditionsorrefusaltoundergoamore invasivesurgerymay limit treatmentop-tions.Inourcase,thepatientwasveryhealthyandhadnopreconceivednotionsregardinggraftmaterials.Thepatientwas informed thatconsideringhisgoodhealthand largehorizontaldefect,anautogenousblockbonegraftwouldbethebest.Insituationsofsuchalargedefect,aparticulategraftwouldnothavesufficientunderlyingbonevolumetofillintheentiredefectandwouldprobablyrequireasecondgrafttofillinanyremainingconcavity.Anautogenousblockbonegraftcancausesomemorbidityatthehostsite,butsinceourpatientwashealthyandhada largevolumeofboneatthedonorsite,wechosetouseautogenousbone.In combination with some particulate bone and a mem-brane, the block graft provided a rather predictable andstableoutcome.
ConclusionIntheabsenceofsufficientbone,itmaynotbepossibletoachievesuccessfulimplantplacement.Inthesesituations,abonegraftmaybenecessarytoachievefavorableplace-mentandstabilityofimplants.Thiscasereporthasshownautogenousblockbonegraftscanbeharvestedfromthemandibular symphysis and can be successfully graftedonto the maxillary buccal alveolar ridge at sites #7 and#10.Theblockgraftsshowedsubstantial improvementinthehorizontalwidthofboneallowingforidealpositioningofdentalimplants.Thiscasehasshownthatridgeaugmen-tationcanbesuccessfullyaccomplishedwithsubsequentimplantstabilitywhileusingarelativelyatraumaticintraoralsurgicalsiteandlowmorbiditytothedonorsite.
References1.BalajiSM(2002)Managementofdeficientanteriormaxil-laryalveoluswithmandibularparasymphysealbonegraftforimplants.Implant Dentistry11(4):363-369.
2.CoxJF,etal. (1987)The longitudinalclinicalefficacyofossesointegraded dental implants: A 3-year report. Int J Oral Maxillofac Implants2:91-100.
3.CordaroL (2002)Clinical resultsofalveolar ridgeaug-mentation with mandibular block bone graft in partiallyedentulouspatientsprior to implantplacement.Clin. Oral Impl. Res.13:103-111.
4.SeibertJS(1983)Reconstructionofdeformed,partiallyedentulous ridges, using full thickness onlay grafts. PartI. Techniqueandwoundhealing.Compend Contin Educ Dent4(5):437-453.
5.McAllisterBS,HaghighatK (2007)Boneaugmentationtechniques.J Periodontol78(3):377-396.
6.FiorelliniJP,NevinsML(2003)Localizedridgeaugmenta-tion/preservation.Asystematicreview.AnnPeriodontol8(1):321-327.
7.TolstunovL(2009)Maxillarytuberosityblockbonegraft:innovative technique and case report. J Oral Maxillofac Surg67:1723-1729.
8.RasmussonL,etal.(1999)Theinfluenceofsimultaneousversusdelayedplacementonthestabilityoftitaniumimplantsinonlaygrafting.Int J Oral Maxillofac Surg.28:224-231.
9.MischCM(1997)Comparisonofintraoraldonorsitesforonlaygraftingpriortoimplantplacement.Int J Oral Maxil-lofac Implants12:767-776.
Chin Block Bone Graft in Patient Congenitally Missing Maxillary Lateral Incisors Prior to Implant Placement: A Case Report

©2010ColumbiaDentalReviewVolume14:2009-2010 34
Use of Block Allografts in Pre-Implant Alveolar Ridge Augmentation: Three Case ReportsGowharIravani1,RenéeReynolds1,KarinEmdeDMD2,JeremyKUenoDMD21Classof2011,CollegeofDentalMedicine,ColumbiaUniversity,NewYork,NY2PeriodonticsResident,CollegeofDentalMedicine,ColumbiaUniversity,NewYork,NY
AbstractAsdentalimplantsbecometheincreasinglydesiredalterna-tiveforreplacementofmissingteeth,theneedtomaximizethesuccessofbonegraftmethodshas increased inkind.Theallogenicblockgraftisarelativelynewoptionforbonegrafting that eliminates the autograft’s need for a secondsurgicalsitebutprovidesthesamebenefitsofphysicalbulk,stability,andstructurewhilebeinginvirtuallyunlimitedsupply.Italsoaimstoaddverticalheightaswellashorizontalwidth.Thiscasereportseriesdetailstheuseofallograftsonvariousalveolarridgelocations.Inallinstancesofallograftplacementdiscussedhere,theendresultwasanaugmentationofbonecomparabletothattypicallyachievedwiththeuseofothertechniques and materials. However, two of the allograftsdiscussedinthisreportpresentedthecomplicationofgraftexposure,whichisnotusuallyexperiencedwithautografts.Variouswaysofmitigatingthisriskhavebeenproposed,oneofwhichyieldedsuccessfulresultsinthelastcasedescribedbelow, indicating that further investigation into the optimalmethodsforusingcadavericblockgraftsisworthwhile.
IntroductionManyof thepatientswhodesiredental implants lackthenecessaryalveolarbonewidthand/orheight to retainanimplantsecurelyoverthelong-termandensureosseointe-gration.Severalsourcesofbonegraftmaterialareavailabletoaddresstheproblem,howeverallhavesomedrawbacks.Autografts—harvestedfromintraoralsitessuchastheman-dibular symphysis or ramus, and extraoral sites such asclavicle,ribs,oriliaccrest—havetodatebeenconsideredthegoldstandard,becausetheyarereadilyadoptedbytherecipientsite1andprovideosteoconductive,osteoinductive,andosteogenicpropertiesthatencouragebonegrowth.2,3
However,forthepatient,theprospectofexposingtwosur-gicalsites,withtheaccompanyingdiscomfort,cost,time,and increased riskof infection,paresthesia,or fracture isnotalwaysanattractiveoption.1Commonalternativemeth-ods forboneaugmentation includebutarenot limited toguided bone regeneration, short and narrow implants toavoid ridge augmentation, sinus lift for posterior maxilla,andridgesplitforhorizontaldeficiency.However,theseal-ternativesalsobringpotentialcomplicationsthatmightnotmakethemsuitableforallpatients.
Useofthecadaverblockgraftisarelativelynewmethodofbonegraftingthatprovidesoneadditionaloptiontopatientsandclinicians.Theseallographicblocksarecorticocancel-lousorcancelloussegmentsofbonethathavebeendehy-
dratedviavariousmethods,sterilized,andtreatedtoremoveantigenicpotentialandcanbefixatedtodeficientalveolarridgeswithfixationscrewstoincreasebonethickness.
Thecasesthatfollowdiscusstheadvantagesanddisad-vantagesfoundwhenusingallograftblockstoaugmentthemandibleormaxillapriortoimplantplacement.
Case Report 1 A26yearoldnon-smokingfemalepresentedtotheColum-biaUniversityPost-GraduatePeriodonticsClinic for ridgeaugmentationofthemaxillaryanteriorregioninanticipationofimplantplacementafterextractionoftooth#9.Thistoothwasseverelycompromisedwithananteriorfistulaandsen-sitivitytopercussion.Hermedicalhistorywasnon-contrib-utorytohercondition.Afteracompletediagnosticworkup,includingphotographs,radiographs,andaCTscan,itwasdecidedtouseablockallografttoincreasethethicknessoftheridge.Uponextractionof#9,socketpreservationwasperformedinordertoincreaseosseoustissueandsupportamoreestheticoutcome.Thesocketwasfilledwithpar-ticulateallograftmaterial(Puros)andcoveredwitharesorb-ablecollagenmembrane(BiomendExtend).Aconnectivetissuepediclewasharvested fromthepalateandplacedoverthesocket(Figure 1).
Figure 1Case 1: The socket was filled with Puross and covered with a layer of Biomend Extend membrane
Figure 2Case 1: CT pedicle necrosis

©2010ColumbiaDentalReview Volume14:2009-201035
Use of Block Allografts in Pre-Implant Alveolar Ridge Augmentation: Three Case Reports
Oneweekpostoperation,therewasevidenceofconnectivetissuepediclenecrosis(Figure 2)andlossofsomeparticulateallograftinthesocket.Bothahorizontalandverticaldefectwas present (residual Class III Seibert defect), significantlycompromisinganyfutureimplantrestorationesthetics.Thus,itwasdecidedtoaugmenttheridgewithablockallograft.
Sixweeksbeforetheplacementoftheblock,afrenectomywasperformedtodecreasetheflaptensionanticipatedafterplacementofthebonegraft.Sulcularandmid-crestal inci-sionsweremadeovertheedentulousridgefrom#6-12.Afullthicknessflapwasraisedandthedefectiveareawasvisual-izedandmeasuredtobeapproximately11mm(Figure 3).
The block was shaped to the size of the defected areaand to fit passively over the ridge (Figure 4). The buccalbonewasdecorticated toencouragevascularizationandbone-blockintegration.Bonescrewsof10.5mmand7.5mmwereinsertedintothecrestalandbuccalaspectsre-spectively.Particulateallograft(Allo-Oss)wasplacedtofillthevoidsaroundtheblock(Figure 5)andaresorbablecol-lagenmembrane(OssixPlus)wasplacedovertheblock.Periostealreleasingincisionsweremadeandtheflapwascoronallypositioned.Theconnectivetissuegraft(CTG)wassecuredundertheflapandthetissuewassuturedtoobtainprimaryclosure.TheCTGcoveredthe2mmdehiscencebetweenthebuccalandpalatalflaps(Figure 6).
Figure 3 (left)Case 1: Incision and full thickness flap
Figure 4 (right)Case 1: block allograft shaped to fit the recipient site
Figure 5 Case 1: block graft inserted
Figure 6Case 1: Primary closure of hard and soft tissue grafts
Thepatientwasgivenaninterimprosthesisandcarewastakentorelieveanypressuretheprosthesishadonthesofttissue,whichcouldpotentiateresorption.Twoweeksafterthesurgery, theblockgraftandscrewbecameexposedcoronally,butthepatientwasnot indiscomfort.Afteran-otherfourweeks,theblockwascompletelyexposed(Fig-ure 7),thusitwasdecidedtoattempttocovertheexposedareawithaconnectivetissuepediclegraftrotatedfromtheleftpalate.
Figure 7Case 1: Six weeks post-op, block exposed.
Thisattemptwasunsuccessfulandledtocompletenecro-sisofpedicleflap.Atthispointitwasdecidedtoleavetheblockexposedandre-evaluatefromweektoweek,reduc-ing exposedboneat each visit until healthy vascularizedbonewasreached.Softtissueclosurewasfinallyachievedaftersixmonths(Figure 8).ThefinalCTscanshowedthatbonethicknessintheareahadincreasedto6.5mmafterintegrationoftheblockgraft(Figure 9).Theimplantwastheplacedsuccessfully(Figures 10, 11).
Figure 8 (left)Case 1: Soft tissue closure achieved.
Figure 9 (right)Case 1: Final CT scan shows adequate horizontal and vertical bone (6.5x14.5mm)

©2010ColumbiaDentalReviewVolume14:2009-2010 36
Use of Block Allografts in Pre-Implant Alveolar Ridge Augmentation: Three Case Reports
Figures 10 (left) and 11 (right)Case 1: Successful implant placement at 6 months post-graft
Case Report 2A56yearoldfemalepresentedtotheColumbiaUniversityPost-GraduatePeriodonticsClinicforanimplantconsulta-tionasshewasedentulousinmultipleareas,includingtheregionof#28-30(Figure 12).Thepatienthadnosignificantmedical history and was a non-smoker. The diagnosticwork-upwhichincludedaCTscanindicatedthattherewasinsufficientbonewidth in the lower rightmandible toac-commodateimplantsandabonegraftwouldbenecessary.
Priortoplacingthebonegraft,aconnectivetissueallograftwouldalsobeneeded tobetteraccommodate theboneblockmaterial,deepenthevestibule,andensurekeratinizedgingivaforprimaryclosure.Thepatientwasgivenmultipleoptions including theuseof anautograft harvested fromhermandibleortheallogenicblockgraftandsheelectedtoproceedwiththeallograftblock.
Figure 13Case 2: Complete healing of alloderm graft in mandible; increased at-tached gingiva seen compared to baseline
Figure 12Case 2: Baseline mandibular alveolar ridge, buccal view
Inordertocreatetheneededincreaseinattachedgingivaandvestibulardepthitwasdecidedtoperformavestibu-loplastywiththeuseofacellulardermalmatrix(alloderm)afewweeksbeforetheblockgraft.Thelowerrightmandiblehealedafterfiveweekswithoutincident(Figure 13).
Threeandahalfmonthsaftertheallodermgraftofthelowerrightmandiblewasplaced,thepatientpresentedforplace-mentoftheblockgraft.Alingualcrestalincisionwasmadebetweenteeth#27-31.Asulcular incisionwasthenmadewithoneverticalreleaseandafullthicknessflapwasraised.Afterdissectionaroundthementalnerve,thebuccalplatewasdecorticatedforbettergraftintegration(Figure 14).
Figure 14Case 2: Decorticated recipient site
Theblockwasshapedtomatchthecurvatureandsizeoftherecipientsiteandtwopilotholesweredrilled into theblock.Initialstabilitywasnotachievedwithoneofthepilotholes,soanewonewasmademesiallytosecuretheblockwithbi-corticalstabilization.Screwsof10.5mmlengthwerescrewedinthepilotholes(Figure 15).
Figure 15Case 2: Allograft secured by screws at recipient site
Voidswerefilledwithparticulatecortico-cancellousallograft(Allo-Oss) and a resorbable collagen membrane (Ossix-Plus)wasplacedovertheblockgraft.Primaryclosurewasachieved.Attheoneweekfollow-upvisits,thetissueatthecrestofthealveolarridgewasthinningandthepatientex-periencedparesthesia inthetissueanterior tothementalforamen.Attwo,four,andtenweekfollow-ups,therewasexposure of the block, but the tissue appeared clinicallyhealthy(Figure 16).
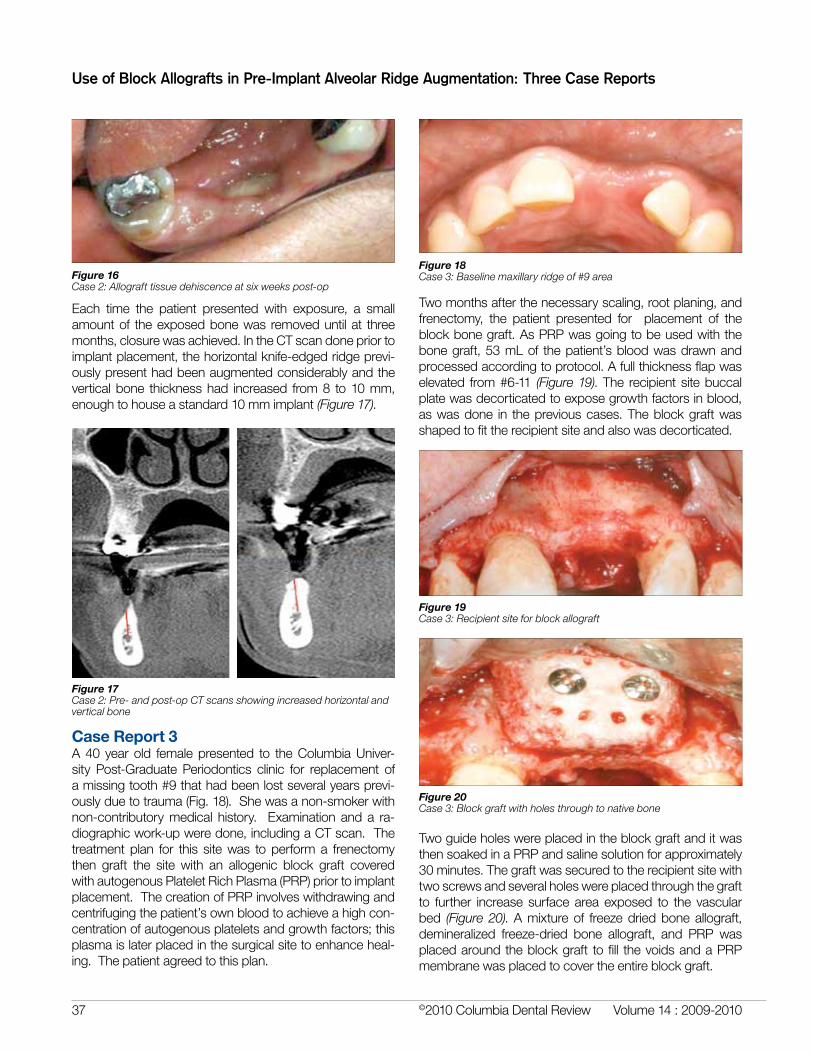
©2010ColumbiaDentalReview Volume14:2009-201037
Use of Block Allografts in Pre-Implant Alveolar Ridge Augmentation: Three Case Reports
Figure 16Case 2: Allograft tissue dehiscence at six weeks post-op
Each time the patient presented with exposure, a smallamountof theexposedbonewas removeduntilat threemonths,closurewasachieved.IntheCTscandonepriortoimplantplacement,thehorizontalknife-edgedridgeprevi-ouslypresenthadbeenaugmentedconsiderablyandtheverticalbone thicknesshad increased from8 to10mm,enoughtohouseastandard10mmimplant(Figure 17).
Figure 17Case 2: Pre- and post-op CT scans showing increased horizontal and vertical bone
Case Report 3A40 yearold femalepresented to theColumbiaUniver-sity Post-Graduate Periodontics clinic for replacement ofamissingtooth#9thathadbeenlostseveralyearsprevi-ouslyduetotrauma(Fig.18).Shewasanon-smokerwithnon-contributorymedical history. Examinationanda ra-diographicwork-upweredone,includingaCTscan.Thetreatmentplan for this sitewas toperforma frenectomythen graft the site with an allogenic block graft coveredwithautogenousPlateletRichPlasma(PRP)priortoimplantplacement.ThecreationofPRPinvolveswithdrawingandcentrifugingthepatient’sownbloodtoachieveahighcon-centrationofautogenousplateletsandgrowthfactors;thisplasmaislaterplacedinthesurgicalsitetoenhanceheal-ing.Thepatientagreedtothisplan.
Twomonthsafterthenecessaryscaling,rootplaning,andfrenectomy, the patient presented for placement of theblockbonegraft.AsPRPwasgoingtobeusedwiththebonegraft,53mLof thepatient’sbloodwasdrawnandprocessedaccordingtoprotocol.Afullthicknessflapwaselevated from#6-11 (Figure 19).The recipientsitebuccalplatewasdecorticatedtoexposegrowthfactorsinblood,aswasdone in thepreviouscases.Theblockgraftwasshapedtofittherecipientsiteandalsowasdecorticated.
Figure 18Case 3: Baseline maxillary ridge of #9 area
Figure 19Case 3: Recipient site for block allograft
Figure 20Case 3: Block graft with holes through to native bone
TwoguideholeswereplacedintheblockgraftanditwasthensoakedinaPRPandsalinesolutionforapproximately30minutes.Thegraftwassecuredtotherecipientsitewithtwoscrewsandseveralholeswereplacedthroughthegraftto further increase surface area exposed to the vascularbed (Figure 20).Amixtureof freezedriedboneallograft,demineralized freeze-dried bone allograft, and PRP wasplacedaroundtheblockgraft tofill thevoidsandaPRPmembranewasplacedtocovertheentireblockgraft.

©2010ColumbiaDentalReviewVolume14:2009-2010 38
Use of Block Allografts in Pre-Implant Alveolar Ridge Augmentation: Three Case Reports
Attheoneandtwomonthfollow-upvisits,healingproceed-eduneventfullyandnograftexposurewasnoted(Figure 21).
Figure 21Case 3: Site of block graft two months post-op
Eightmonthsaftertheplacementoftheallograftthepatientpresentedforimplantplacement.Theimplantpre-surgeryCTscanindicatedthatthealveolarridgewidthatthesiteof thegrafthad increasedbyapproximately3.5mm,thussufficientbonewasnowpresenttoplaceanimplant(Figure 22).A4x11.5mmimplantwasplacedatthesiteofthebonegraft (Figures 23, 24).
Figures 23, 24Case 3: Implant placement at site of block graft, prior to osseointegration
Figure 22Case 3: Before and after CT scans
DiscussionTheallograftsusedasdescribedaboveshowedclearad-vantagesoveralternativemethodsofbothsofttissueandbonegrafting.Ineachcase,attachedgingivawasincreasedpriortoplacementoftheblockallograft.Theprimaryaimofthiswastoallowforatension-freeclosureoncethebonegraftwasinplaceandtoincreasekeratinizedgingivasur-rounding the future implant to minimize future recessionandmaximizeestheticresults.
Studies in the literaturedescribetheadvantagesofusingallodermratherthanafreegingivalgraftforvestibuloplas-ties,whichinadditiontothosesameadvantagesofboneallografts (nosecondsurgicalsite, lessmorbidity)also in-cludethepreventionoftransferringcellsthatcouldtransmitviruses.3Althoughtheadditionoftheallodermgraftaddedthreeandahalfmonthstothepatient’streatmentandde-spite the issueofsomeexpectedsloughingofsuperficialepitheliumduringhealinginthefirstfewweeksduetopoorvascularization,thiswaseasilymanaged.
Similarly hard tissue allografts were successfully used toaugment deficient alveolar bone both vertically and hori-zontally,allowingadequatewidthtohouseadentalimplant.Previouscasestudieshaveshowngraftdehiscencetobeaparticularproblemwhenverticalaugmentationisattempt-ed.4Unlikecasesthatuseautogenousbonetograftdefi-cientridges,thepatientsheredidnotneedtoendurethetime,risks,costs,anddiscomfortsassociatedwithcreatingasecondsurgicalsitetoharvesttheirownbone.5
Oncethetissuewashealthyandthevestibuledeepenedenough to proceed with the bone allograft, the allograftblockwasplacedandprimaryclosurewasachieved.How-ever,graftsitesincases1and2aboveexperiencedprob-lemswithblockexposure.
Other clinicians have had success with allograft blockswithoutexperiencingproblemswithgraftexposure.1,6Thereareseveralpossiblevariablesthatmaycontributetowheth-erornotblockallograftsbecomeexposed.First,thetypeofboneintheallograft,eitherallcancellousorcortico-can-cellousmayinfluenceexposure.Apurelycancellousblockgraftwithalowerdensitythancorticalbonemaybemoreamenabletoarapidvasularizationandintegration.1Inaddi-tion,cancellousbonegainsmechanicalstrengthduringtherepairprocess,whereascorticalboneisweakenedduringrepair.2InsimilarcasesdescribedbyWallaceandLyfordetal.,severalalveolarridgesitesweregraftedwithcancellousallograftblockscoveredwithcorticalboneparticlesonmul-tiplepatients,andthroughoutthehealingperiodinallsites,graftexposurewasneveraproblem.1,2Nevertheless,casesof cortico-cancellous allografts have also been reportedinhumanswithoutdehiscence,somost likelythetypeofboneintheallograftisonlyonefactorpotentiallycontribut-ingtoexposure,ifitdoesatall.5,6,7
Otherfactorspotentiallyinfluencingsofttissuedehiscenceare the locationof the initial flap incision (crestal vs. ves-tibular incisions) and the way in which the block graft isprocessed (freeze-dried, fresh-frozen,solvent-dehydrated,etc.). Processing techniques could affect the graft’s me-chanical strength and persistence of bone morphogenicproteins.4,8 Thekindofmembraneplacedon topof the

©2010ColumbiaDentalReview Volume14:2009-201039
Use of Block Allografts in Pre-Implant Alveolar Ridge Augmentation: Three Case Reports
graft(resorbablevs.non-resorbable,orboth,thegraftcon-touring prior to placement, and pressure placed on thetissuebyatemporaryprosthesis1,6mayimpactsofttissuedehiscenceaswell.
Althoughextensiveeffortsweremadetoensuretensionfreeprimaryclosuresviasoft tissuegraftsprior toblockgraftplacement,perhapsanevengreaterexcessofsofttissueisneededtoaccountforthetissuethatwillpossiblyexperi-enceresorption;propersofttissueclosuretechniquesarecrucialtodehiscenceprevention.Case3describedabovealsoincorporatedholesplacedentirelythroughthewidthoftheblockgrafttoencouragevascularization,andthismayhavecontributedtothefactthatnoexposurewasseeninthiscase.Somecasesdescribedintheliteraturepreparedtherecipientbedwithanindentationthatmatchedthesizeof theblockgraftso that itfitsnugly in thesiteandthusincreasedthesurfaceareaofthegraftexposedtonativebone.5Thisalsomayhaveimprovedvascularization,prevent-ingexposure.However,thiswasnotdoneinthecasesabovesoastomaximizepreservationofnativebone;itisuncertainwhethersacrificingthealreadydeficientnativeboneisworththeincreasedsurfaceareacontact.Clearly,useoftheblockallograftsisextremelytechnique-sensitive.6
Lastly, somesuccesshasbeen foundwith soaking theallograftorthecoveringmembraneinapreparationofthepatient’splatelet-richplasma(PRP).5,7Thiswasaproce-durethatwasnotdone inthefirsttwocasesdescribedbutwasincorporatedintothelastcaseaboveaswellasseveralcases in the literature,noneofwhichhadprob-lems with block graft exposure. Use of PRP has beensomewhatcontroversial,as therearesomestudies thatindicatethatthegrowthfactorspresumedtobehelpfulinosteogenesisareactuallyveryshort-livedinPRPanddonotlastlongenoughtohaveasignificantimpact.7,9How-ever, there isalsoevidencetothecontrary,asPRPhasbeenfoundtoenableamorepredictableflapadaptationandclosure,improvehemostasis,andpromoteepithelialdevelopmentandhemostasiswhenappropriatedeliverymethodsareusedtoadministerPRPinatime-controlledmanner.7,9 Some studies have shown that surgical sitesenhancedwithPRPhealataratetwotothreetimesfasterthansurgicalsiteswithoutPRP.10GiventhatuseofPRPincertaininstancesmayimproveoutcomesandthattheclinicalcasesthatusedPRPappearedtohavelesscom-plications,thisiscertainlyafactorthatshouldbeexploredin the future via randomized controlled trials of alveolarridgeallografts.
Patient selection is also very important in these cases.Someimportantselectioncriteriaforpatientsinclude:pa-tient compliance/ motivation (since strict adherence topost-opinstructionsandreturnforfollow-upvisitsiscrucial),
negativehistoryofsmoking,goodoralhygiene,andlackofsignificantsystemicdiseases.
ConclusionCasespresentedaboveand in the literature indicate thatthereisademandforreliablealternativestoautograftsforaugmentingwidespansofalveolar ridgeprior to implantplacement.Blockallograftsthatcanbeformedintovariousshapesshowpromiseinbecomingaviablesolutiontothisneed.However,todate,therearenoknownrandomizedcontrolledtrialsonhumansthatconsidervariablessuchastheamountofbonebeingreplaced,useofsofttissuegraftpriortoblockplacement,graftbonetype,graftpreparationmethod, incision type, suture type,orPRPuse toquan-tifydifferences intheoutcomesseen inautograftsvs.al-lografts. Such studies should be done and would provebeneficialinelicitingarepeatablemethodforsecuringgoodresultsinallograftuse.
References1.LyfordR,MichaelM,KnappC,ScheyerE,MellonigJ(2003).Clinicalevaluationoffreeze-driedblockallograftsforalveolarridgeaugmentation:acaseseries.Int J Periodon-tics Restorative Dent.23(5):416-425.
2.WallaceS,GellinR(2008).ClinicalEvaluationofacan-cellousblockallograftforridgeaugmentationandimplantplacement:acasereport.Implant Dentistry.17(2):151-158.
3.BholaM,NewelD,HancockE(2003).Acellulardermalal-lograftforvestibuloplasty-analternativetoautogenoussofttissuegraftsinperprostheticsurgicalprocedures:aclinicalreport.J Prosthodont.12(2):133-137.
4. Barone A, Varanini P, Orlando B, Tonelli P, Covani U(2009).DeepfrozenAllogeniconlaybonegraftsforrecon-structionofatrophicmaxillaryalveolarridges:apreliminarystudy.J Oral Maxillofac Surg67:1300-1306.
5.PetrungaroP,AmarS(2005).Localizedridgeaugmenta-tionwithAllogenicblockgraftspriortoimplantplacement:casereportsandhistologicalevaluations.Implant Dentistry.14(2):139-148.
6.KeithJD,LeonettiJA,PetrungaroP,LeonettiJ,ElwellC,ZarenKJ,CaputoC,NikitakisN,SchopfC,Warner,M(2006).Clinicalandhistologicalevaluationofamineralizedblockal-lograft:resultsfromthedevelopmentalperiod(2001-2004).Int J Periodontics Restorative Dent.26(4):320-327.
7. Keith JD (2004). Localized ridge augmentation with ablockallograftfollowedbysecondaryimplantplacement:acasereport.Int J Periodontics Restorative Dent.24(1):10-17.

©2010ColumbiaDentalReviewVolume14:2009-2010 40
Use of Block Allografts in Pre-Implant Alveolar Ridge Augmentation: Three Case Reports
8.ContarCMM,SarotJR,BordiniJr.J,GalvaoGH,NicolauGV,MachadoMANM(2009).Maxillaryridgeaugmentationwith fresh-frozen bone allografts. J Oral Maxillofac Surg 67:1280-1285.
9.IntiniG(2009).Theuseofplatelet-richplasmainbonereconstructiontherapy.Biomaterials.30(2009)4956-4966.
10.CarlsonNE,RoachJr.RB (2002). Platelet-richplas-ma: clinical applications in dentistry. J Am Dent Assoc. 133:1383-1386.