colonic diverticular disease. western population ½ of individuals >60y/o 20% of patients develop...
TRANSCRIPT

COLONIC DIVERTICULAR DISEASE



* US Census Bureau, International Data Base, 2004 ( the extrapolations for Diverticular Disease are only estimates and may have limited relevance to the actual incidence of Diverticular Disease in any region)


TYPES
FALSE DIVERTICULA- involves only protrusion of the mucosa through the muscularis propria of the colon- most common
TRUE DIVERTICULA- a saclike herniation of the entire bowel wall


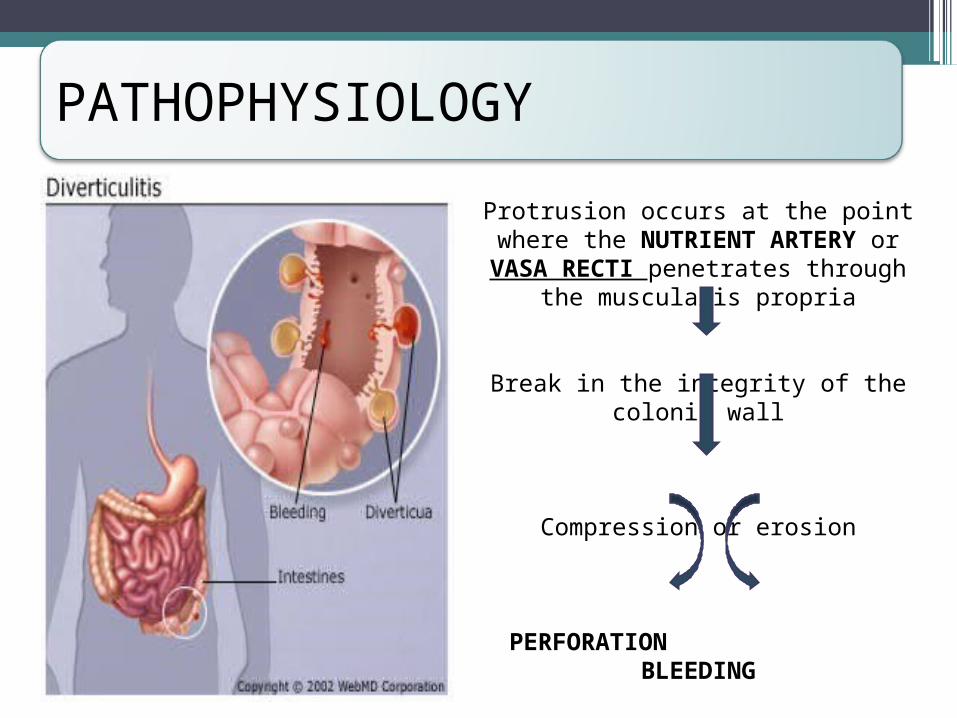
Protrusion occurs at the point where the NUTRIENT ARTERY or VASA RECTI penetrates
through the muscularis propria
Break in the integrity of the colonic wall
Compression or erosion
PERFORATION BLEEDING
PATHOPHYSIOLOGY

PATHOPHYSIOLOGY
commonly affect the SIGMOID COLON due to:
Relative high pressure zone within the muscular sigmoid colin.
Higher amplitude contractions combined with constipated, high fat content stool within the sigmoid lumen results in the creation of these diverticula
Related to retention of particulate material within the diverticular sac and formation of fecalith

Presentation, Evaluation, and Management

Diverticular Bleeding• Hemorrhage from a colonic diverticulum is the most common
cause of hematochezia in patients >60 years.• Only 20% of patients with diverticulosis will have GI bleeding.• Most bleeds are self-limited and stop spontaneously with
bowel rest.• Lifetime risk of rebleeding: 25%

Diverticular Bleeding• Colonoscopy
To localize the bleeding May be both diagnostic and therapeutic in the management of mild to
moderate diverticular bleeding
• Angiography Management of massive bleeding in a stable patient Mesenteric angiography can localize the bleeding site and occlude the
bleeding vessel successfully with a coil in 80% of the cases Follow up: Repetitive colonoscopy to look for evidence of colonic
ischemia
• Segmental resection of the colon To eliminate risk of further bleeding In patients on chronic blood thinners
Diverticular Bleeding•Highly selective coil embolization
Rate of colonic ischemia: <10% Risk of acute rebleeding: <25%
•Selective infusion of vasopressin To stop hemorrhage Complications: MI, intestinal ischemia Recurrence of bleeding in 50% of patients once infusion is
stopped

Diverticular Bleeding•Surgery
Indications: if patient is unstable or has had a 6-unit bleed within 24 h
Total abdominal colectomy Patients with presumed bleeding from diverticular
disease requiring emergent surgery without localization Rationale: Colonic diverticulosis is more often seen from
the R colon Surgical resection with primary anastomosis
In patients without severe comorbidities

Presentation, Evaluation, and Management

DIVERTICULITISUncomplicated – 75%Abdominal PainFeverLeukocytosisAnorexia/obstipation
Complicated – 25%Abscess 16%Perforation 10%Stricture 5%Fistula 2%

Diverticulitis•Diverticular perforation
Generalized peritonitis in <25% of cases (+) Abdominal distention
•Giant diverticulum of the sigmoid (+) Air fluid level in the LLQ on plain abdominal film Mx: resection to avoid impending perforation

Diverticulitis•Diagnosis is best made on CT.

Diverticulitis•Suspected diverticulitis that does not meet CT
criteria or is not associated with a leukocytosis or fever is not diverticular disease
•Conditions that mimic diverticular disease: IBS Ovarian cyst Endometriosis Acute appendicitis PID

Diverticulitis•Barium enema or colonoscopy
Should be performed ~6 weeks after an attack of diverticular disease A sigmoid malignancy can masquerade as diverticular
disease. Should not be performed in the acute setting
Higher risk of colonic perforation associated with insufflation or insertion of barium-based contrast material under pressure.

Diverticulitis•Complicated diverticular disease
Diverticular disease associated with an abscess or perforation, and less commonly with a fistula.
With fistula formation Common locations include cutaneous, vaginal or vesicle
fistulae Present with either passage of stool through skin or
vagina, or pneumaturia Colovaginal fistulae: more common in women who have
undergone hysterectomy

Hinchey Classification of Perforated Diverticular Disease
Medical Management of Diverticular Disease•Asymptomatic
Diet alterations – fiber-enriched diet, including 30g of fiber/day
Supplementary fiber products: Metamucil, Fibercon, Citrucel
Avoid nuts and popcorn – may obstruct the lumen of the diverticulum

Medical Management of Diverticular Disease• Symptomatic
Radiographic and hematologic confirmation of inflammation and infection within the colon
Treated initially with antibiotics and bowel rest TMP-SMX or ciprofloxacin and metronidazole (+) Ampicillin – for nonresponders Alternative: IV piperacillin or oral penicillin/clavulinic acid Usual course: 7-10 days Rifixamin + fiber – less frequent recurrent symptoms from
uncomplicated diverticular disease
Limited diet until pain resolves Medical therapy can be continued beyond 2 attacks without an
increased risk of perforation requiring a colostomy, especially in those >50 years.

Surgical Management ofDiverticular Disease• In patients who are low risk (ASA I and II) who have
had at least 2 documented attacks requiring hospitalization or those who do not rapidly improve on medical therapy
•Younger patients – more aggressive form of disease▫Waiting beyond two attacks is not recommended.
• In all low surgical risk patients with complicated diverticular disease

Surgical Management ofDiverticular Disease•Goals of Surgical Management
Control sepsis Eliminate complications such as fistula or obstruction Remove diseased colonic segment Restore intestinal continuity
Surgical Management ofDiverticular Disease

Surgical Management ofDiverticular Disease
• Open or laparoscopic sigmoid resection – current option of uncomplicated diverticular disease
• Benefits of laparoscopic over open resection:▫Early discharge (by at least 1 day)▫ Less narcotic use▫Earlier return to work
• Benefits of open over laparoscopic resection:▫Shorter operative procedure▫ Less costly
• Complication rates are similar.
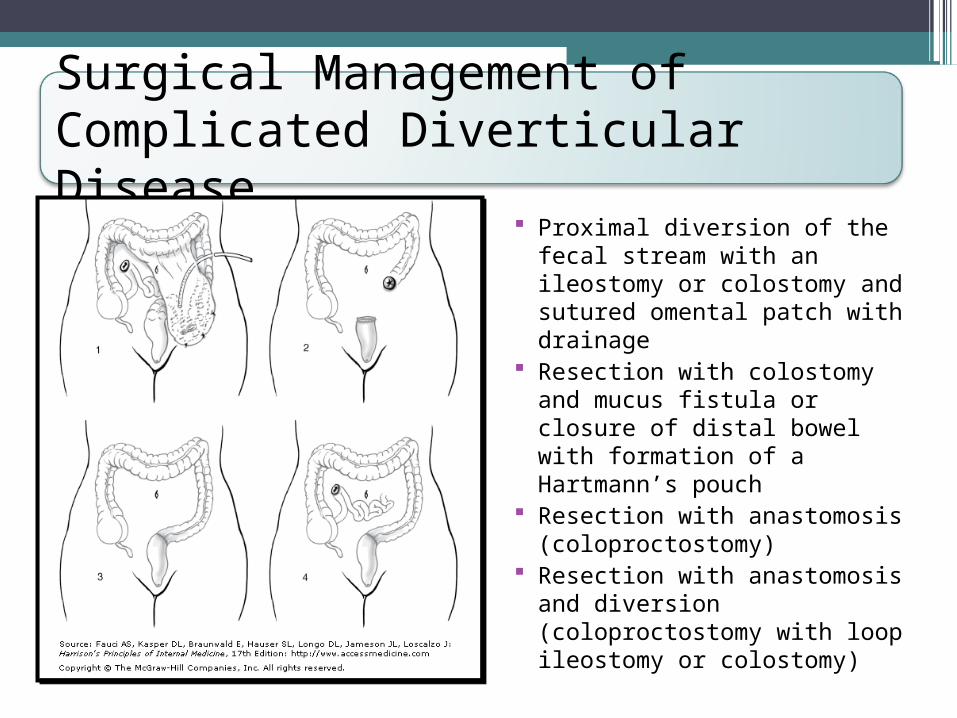
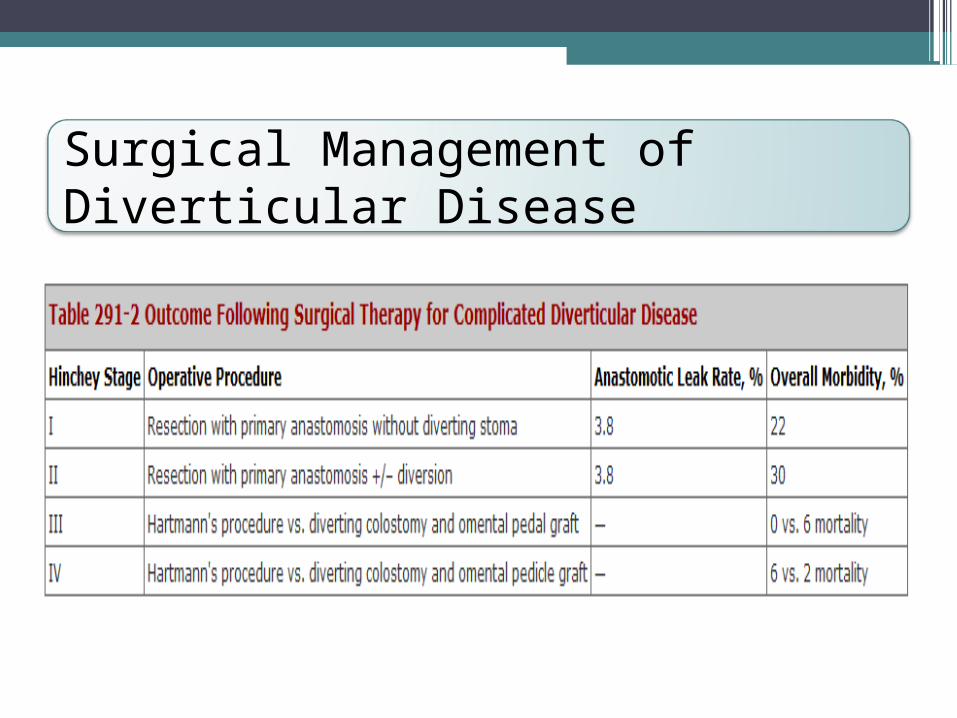
Surgical Management ofComplicated Diverticular Disease
Proximal diversion of the fecal stream with an ileostomy or colostomy and sutured omental patch with drainage
Resection with colostomy and mucus fistula or closure of distal bowel with formation of a Hartmann’s pouch
Resection with anastomosis (coloproctostomy)
Resection with anastomosis and diversion (coloproctostomy with loop ileostomy or colostomy)
Surgical Management ofDiverticular Diseases•Hinchey Stages I and II
▫Percutaneous drainage followed by resection with anastomosis about 6 weeks later
▫Percutaneous drainage For abscesses ≥ 5 cm with a well-defined wall that is
accessible If <5cm, may resolve with antibiotics alone Contraindications to percutaneous drainage:
No percutaneous access route Pneumoperitoneum Fecal peritonitis

Surgical Management ofDiverticular Diseases•Hinchey Stages I and II
▫If patients develop generalized peritonitis Hartmann’s procedure
▫Nonoperative therapy – 20% recurrence rate at 2 years in patients with Hinchey Stage I disease
▫80% of patients with Hinchey Stage II required surgical resection for recurrent symptoms.

Surgical Management ofDiverticular Diseases• Hinchey Stage III
▫Hartman’s procedure or with primary anastomosis and proximal diversion
▫ If patient has significant comorbidities: intraoperative peritoneal lavage (irrigation), omental patch to the oversewn perforation, and proximal diversion of the fecal stream with either an ileostomy or transverse colostomy can be performed
• Hinchey Stage IV▫No anastomosis of any type should be attempted.

Recurrent Symptoms inDiverticular Disease•Occurs in 10% of patients.•Recurrence develops in patients following
inadequate surgical resection.•A retained segment of diseased rectosigmoid colon is
associated with twice the incidence of recurrence.• IBS – may also cause recurrence of initial symptoms•Patients undergoing surgical resection for presumed
diverticulitis and symptoms consistent with IBS have functionally poorer outcomes.