colon cancer screening- rationale behind the guidelines
TRANSCRIPT

Colon Cancer Colon Cancer Screening- Screening-
Rationale Behind Rationale Behind the Guidelinesthe Guidelines

Problem #1Problem #1
42 y.o. asymptomatic caucasian 42 y.o. asymptomatic caucasian woman presents requesting CRC woman presents requesting CRC screening. Her mom, 69 y.o. was screening. Her mom, 69 y.o. was recently was diagnosed with Stage II recently was diagnosed with Stage II colon cancer. No other significant colon cancer. No other significant medical or family history. medical or family history. Do you screen her?Do you screen her? How?How?

Problem #2Problem #2 No longer employed by the US government and No longer employed by the US government and
in private practice in Mississippi, you are asked in private practice in Mississippi, you are asked by your hospital system to make by your hospital system to make recommendations to improve CRC screening recommendations to improve CRC screening within your system. Screening rates in your area within your system. Screening rates in your area are in the 40-50% range. are in the 40-50% range. Would you:Would you: A. Insist that more patients be referred for optical A. Insist that more patients be referred for optical
colonoscopy (OC)?colonoscopy (OC)? Recommend the hospital invest in Virtual Colonoscpy?Recommend the hospital invest in Virtual Colonoscpy? Direct and give guidance for a stool based detection Direct and give guidance for a stool based detection
program, and if you do this what test would you program, and if you do this what test would you recommend?recommend?

OverviewOverview
The “scope” of the problemThe “scope” of the problem Disease burden. Who do we screen? How do we Disease burden. Who do we screen? How do we
screen?screen?
The guidelinesThe guidelines ACG-2009ACG-2009
ASGE-2006- Screening pts with + family ASGE-2006- Screening pts with + family historyhistory
USPSTF-2008- Stop screening at 75? 85?USPSTF-2008- Stop screening at 75? 85?
RationaleRationale ““Preferred modality” vs. “Menu of Options”Preferred modality” vs. “Menu of Options” EvidenceEvidence

Screening TestsScreening Tests
Ideal test dependsIdeal test depends The diseaseThe disease
Common, high morbidity and mortalityCommon, high morbidity and mortality The testThe test
Early detection/treatment can prevent mortalityEarly detection/treatment can prevent mortality Screening test must be effectiveScreening test must be effective
The populationThe population Resources in community to provide screeningResources in community to provide screening Screening methods accepted by patients and Screening methods accepted by patients and
practitionerspractitioners

The DiseaseThe Disease
Colorectal cancer (CRC) is the #2 Colorectal cancer (CRC) is the #2 cause of cancer deathcause of cancer death
5-6% of Americans develop CRC 5-6% of Americans develop CRC
2009:2009: 145,000 new cases of CRC145,000 new cases of CRC 50,000 deaths50,000 deaths

Colon CancerColon Cancer Well defined disease progressionWell defined disease progression Treatable precancerous lesionTreatable precancerous lesion

How to screen?How to screen?

How Do We Screen?How Do We Screen?
Colon cancer prevention (ACG 2009)Colon cancer prevention (ACG 2009) ColonoscopyColonoscopy Flexible sigmoidoscopyFlexible sigmoidoscopy CT colonography (CTC)CT colonography (CTC) DCBEDCBE
Colon cancer detection (ACG 2009)Colon cancer detection (ACG 2009) FOBTFOBT FITFIT sDNAsDNA

The Guidelines-ACGThe Guidelines-ACG
Prevention is better than detection. Prevention is better than detection. Optical colonoscopy (OC) is best.Optical colonoscopy (OC) is best.

The Guideline USPSTFThe Guideline USPSTF
Any screening is better than noneAny screening is better than none
““The USPSTF recommends screening The USPSTF recommends screening for colorectal cancer using fecal for colorectal cancer using fecal occult blood testing, sigmoidoscopy, occult blood testing, sigmoidoscopy, or colonoscopy in adults, beginning at or colonoscopy in adults, beginning at age 50 years and continuing until age age 50 years and continuing until age 75 years. The risks and benefits of 75 years. The risks and benefits of these screening methods vary. “these screening methods vary. “

GuidelinesGuidelines
Points of significant departurePoints of significant departure Preferred modality vs. menu of optionsPreferred modality vs. menu of options Early screening and interval Early screening and interval
colonoscopy for family history of polypscolonoscopy for family history of polyps Age to stop screeningAge to stop screening Virtual colonoscopy Virtual colonoscopy FIT vs. FOBT vs. sDNAFIT vs. FOBT vs. sDNA

ColonoscopyColonoscopy
ProsPros Examines entire Examines entire
coloncolon Detects Detects
precancerous precancerous lesionslesions
Can apply therapyCan apply therapy 10 year interval in 10 year interval in
average risk average risk patientspatients
ConsCons SedationSedation PrepPrep InvasiveInvasive

Preferred modality-OCPreferred modality-OC
Substantial but indirect evidence Substantial but indirect evidence that OC with polypectomy reduces that OC with polypectomy reduces mortality from CRCmortality from CRC
Thiis-Everson et al Scand J Gastrol;1999;34:414-20.

Preferred modality-OCPreferred modality-OC
Winawer et al. National Polyp Study: Winawer et al. National Polyp Study: NEJM 1993NEJM 1993
Mueller et al. VA Cohort study: Annals Mueller et al. VA Cohort study: Annals 19951995

Preferred modality-OCPreferred modality-OC
Complete exam offers durable risk Complete exam offers durable risk reductionreduction
Brenner H et al. Gut 2006;55:1145-60

Preferred Modality OCPreferred Modality OC
Detect lesions not seen on Detect lesions not seen on sigmoidoscopysigmoidoscopy Rex et al GIE 1999 Rex et al GIE 1999 Lieberman et al, NEJM 2000. VA Lieberman et al, NEJM 2000. VA
prospective cohortprospective cohort Jass et al. Clin Gastro-Hep 2004. Jass et al. Clin Gastro-Hep 2004.
Hyperplastic polyps, serrated Hyperplastic polyps, serrated adenomas, DNA methylation, mismatch adenomas, DNA methylation, mismatch repair genesrepair genes
Lieberman et al. NEJM 2000;343:162-8
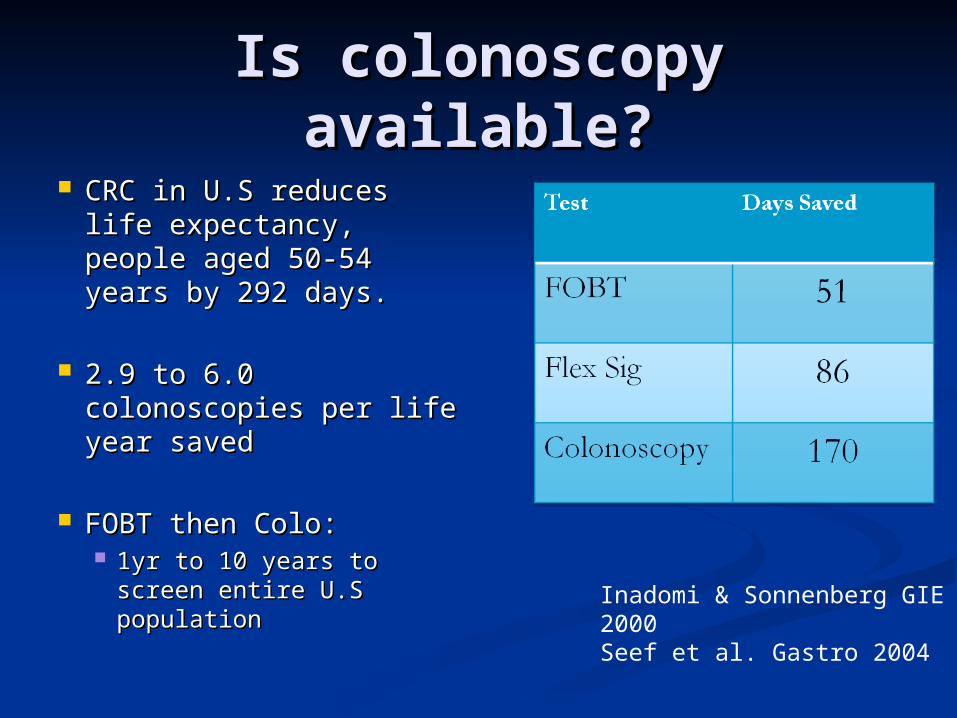
Is colonoscopy available?Is colonoscopy available? CRC in U.S reduces life CRC in U.S reduces life
expectancy, people aged expectancy, people aged 50-54 years by 292 50-54 years by 292 days.days.
2.9 to 6.0 colonoscopies 2.9 to 6.0 colonoscopies per life year savedper life year saved
FOBT then Colo: FOBT then Colo: 1yr to 10 years to screen 1yr to 10 years to screen
entire U.S populationentire U.S populationInadomi & Sonnenberg GIE 2000Seef et al. Gastro 2004

Colonoscopy and Colonoscopy and PolypectomyPolypectomy

Colonoscopy. Who? Colonoscopy. Who? When?When?
Average Risk: 10 year intervals.Average Risk: 10 year intervals. Black men and women, beginning at 45Black men and women, beginning at 45 White men and women, beginning at 50White men and women, beginning at 50
Single first degree relative with CRC Single first degree relative with CRC or advanced adenomaor advanced adenoma > 60 years at diagnosis:> 60 years at diagnosis:
10 year interval beginning at age 50.10 year interval beginning at age 50. < 60 at diagnosis:< 60 at diagnosis:
Colonoscopy every 5 years beginning at age 40 or Colonoscopy every 5 years beginning at age 40 or 10 years younger than youngest affected individual10 years younger than youngest affected individual

The Guidelines-ACGThe Guidelines-ACG
If no HNPCC but + family history If no HNPCC but + family history (cancer or advanced adenoma); early (cancer or advanced adenoma); early screening for 1screening for 1stst degree and age < degree and age < 60.60.

The Guideline ASGEThe Guideline ASGE

Family History of Family History of Advanced Adenoma or Advanced Adenoma or
CRCCRCCondition Screening
Recommendations
Single 1st degree relative with CRC or advanced adenoma > age 60
Same as average risk*
Single 1st degree relative with CRC or advanced adenoma < age 60
Begin at 40 or 10 years prior to diagnosis and then every 5 years
Two or more 2nd degree relatives with CRC or advanced adenoma
Begin at 40 or 10 years prior to diagnosis and then every 5 years

Who do we screen?Who do we screen?
General populationGeneral population 6%6% One 1One 1stst degree relative with: degree relative with:
Advanced AdenomaAdvanced Adenoma 12%12% CRCCRC 12-18%12-18% CRC diagnose before age 50CRC diagnose before age 50 18-24%18-24%
Two FDR with CRCTwo FDR with CRC 18-24%18-24%
One 2One 2ndnd or 3 or 3rdrd degree, CRC degree, CRC 9%9% Two 2Two 2ndnd degree, CRC degree, CRC 12-18%12-18%

Probability of Invasive Probability of Invasive CR cancer by Age and CR cancer by Age and
GenderGenderAge (years) Men (%) Women (%)
< 40 0.08 (1/1,296) 0.07 (1/1343)
40-59 0.92 (1/109) 0.72 (1/138)
60-69 1.55 (1/65) 1.10 (1/138)
70+ 4.63 (1/22) 4.16 (1/24)
Lifetime 5.51 (1/18) 5.10 (1/20)
Risk of death from CRC
Lifetime
2.45 (1/41) 2.45 (1/41)
Cancer Statistics, 2009. CA Cancer J Clin. 2009;59:225-249

History of polypsHistory of polyps
Patients with Patients with personal hx personal hx of small of small TA is at no increased risk for CRC TA is at no increased risk for CRC over the general populationover the general population
Increased CRC risk correlates with Increased CRC risk correlates with size, villous histology, and number of size, villous histology, and number of adenomasadenomas
Atkin WS et al. NEJM 1992Atkin WS et al. NEJM 1992 22,464 patients w/ flex sig and 14 year 22,464 patients w/ flex sig and 14 year
follow upfollow upPolyps Seen # Incident CRC (IR)<1cm, not villous and < 3
4/7776 (0.5)
>1cm, villous, or >3 31/842 (3.6-6.6)

Personal History of Personal History of PolypsPolyps
Condition Surveillance recommendations
Sporadic hyperplastic polyps
Average risk screening recs
1-2 small adenomas 5-10 years
3-10 adenomas or 1 adenoma > 10 mm or any villous or high-grade dysplasia
3 years and then every 5 years
>10 adenomas <3 years
Incomplete resection 2-6 months

CRC African AmericansCRC African Americans Black Americans are 43% more likely to die of Black Americans are 43% more likely to die of
colon cancercolon cancer Rates of CRC in whites down 20-25% since 1985. Rates of CRC in whites down 20-25% since 1985.
Rates for blacks are increasingRates for blacks are increasing

CRC ObesityCRC Obesity
CRC risk increased obesity by 1.5-CRC risk increased obesity by 1.5-2.8 fold2.8 fold
NIH-AAPR cohort study¹NIH-AAPR cohort study¹ BMI increases CRC risk at young age BMI increases CRC risk at young age
(50-66)(50-66) Risk higher in men than women who Risk higher in men than women who
are obeseare obese Meta-analysis: Obesity 33% higher Meta-analysis: Obesity 33% higher
risk CRC ²risk CRC ² 1. Gunter MJ. J Nutr Biochem 2006 2. Bergstrom et al. Int J Can 2001

CRC SmokingCRC Smoking
Possibly 30% increased risk in Possibly 30% increased risk in smokerssmokers
> 20 pack years has 2-3x risk> 20 pack years has 2-3x risk
Increase in advances adenomas and Increase in advances adenomas and early cancers in smokers detected early cancers in smokers detected by colonoscopyby colonoscopy
Gianvannucci E. Cancer Epidemiol Biomarkers Prev 2001;10:725-31

What Am I Missing?What Am I Missing?
Tandem colonoscopy- Meta analysis Tandem colonoscopy- Meta analysis Any size 22%, Any size 22%, ≥≥ 10mm 2.1%, 5-9 mm 13%, 10mm 2.1%, 5-9 mm 13%,
1-4 mm 26%1-4 mm 26%
CTC and OC tandem studyCTC and OC tandem study OC prior to un-blinded CTCOC prior to un-blinded CTC
Missed 55 of 511 polyps (10.8%)Missed 55 of 511 polyps (10.8%) Missed 21 of 210 adenomas >6mmMissed 21 of 210 adenomas >6mm Missed 5 of 51 adenomas > 1cmMissed 5 of 51 adenomas > 1cm 71+% missed colon adenomas on proximal fold71+% missed colon adenomas on proximal fold
Van Rijn JC. Am J Gastro 2006;101:343-350Pickhardt, Annals 2004; 349:
219

Right Sided CRC and Right Sided CRC and ColonoscopyColonoscopy
Baxter et al, Ann Intern Med. 2009 Jan 6;150(1):1-8.
Attempted colonoscopyAttempted colonoscopy All cancer – All cancer – OR of 0.69OR of 0.69 (0.63-0.74) (0.63-0.74) Right sided – Right sided – OR of 1.07OR of 1.07 (0.94-1.21) (0.94-1.21) Left sided – Left sided – OR of 0.39 OR of 0.39 (0.34-0.45)(0.34-0.45)

Colonoscopic Withdrawal Colonoscopic Withdrawal TimesTimes
2053 screening colonoscopies2053 screening colonoscopies
*P<0.05 for all comparisons(>6 vs. <6 min)
%
*
*
*
Barclay RL, et al. N Eng J Med. 2006;355:2533


Screening High Risk Screening High Risk PopulationsPopulations
Condition Surveillance
FAP or suspected FAP Begin age 10-12 with annual flex sig or colo as appropriateConsider colectomy
Genetic or clinical diagnosis of HNPCC
Begin age 20-25 (or 10 years prior youngest family member with cancer) and then colonoscopy every 1-2 years
Inflammatory Bowel Disease
Begin 8 years (pancolitis) or 12-15 years (left-sided colitis) with colonoscopy every 1-2 years

The Guidelines-ACGThe Guidelines-ACG
FAP and HNPCCFAP and HNPCC Genetic testingGenetic testing

Post-CRC SurveillancePost-CRC Surveillance
““High quality” High quality” peri-operative clearing peri-operative clearing colonoscopycolonoscopy
Repeat intervalsRepeat intervals 1 year after resection1 year after resection 3 years later3 years later 5 years later5 years later

Alternative Prevention Alternative Prevention TestsTests
Flexible SigmoidoscopeFlexible Sigmoidoscope Every 5-10 yearsEvery 5-10 years
Computed Tomographic Computed Tomographic Colonoscopy (CTC)Colonoscopy (CTC) Every 5 yearsEvery 5 years

Computed Tomographic Computed Tomographic Colonoscopy (CTC)Colonoscopy (CTC)

CT ColonographyCT Colonography
ConsCons PrepPrep ReproducibilityReproducibility RadiationRadiation 5 year interval5 year interval Reimbursement/Reimbursement/
CostCost
ProPro No sedationNo sedation Detects Detects
precancerous precancerous lesionslesions
Extra colonic Extra colonic findingsfindings

3D Multicenter Trial 3D Multicenter Trial CT ColonographyCT Colonography
Multicenter – military hospitalsMulticenter – military hospitals
1233 asymptomatic patients1233 asymptomatic patients
10mm10mm 8mm8mm 6mm6mm
CT Sens AD by pt 94%CT Sens AD by pt 94% 94%94% 89%89%
OC Sens AD by pt 88%OC Sens AD by pt 88% 92%92% 92%92%
CT Specificity 96%CT Specificity 96%92%92% 80% 80%
Pickhardt, NEJM 2003; 349: 2191

Copyright ©Radiological Society of North America, 2005
Zalis, M. E. et al. Radiology 2005;236:3-9
C-RADS

Copyright ©Radiological Society of North America, 2005
Zalis, M. E. et al. Radiology 2005;236:3-9
E-RADS

Screening CTC Screening CTC Cost EffectivenessCost Effectiveness
CTC is cost effective compared to no CTC is cost effective compared to no screeningscreening
CTC is effective but expensive CTC is effective but expensive compared to OCcompared to OC

CTC and PolypectomyCTC and Polypectomy
No CRC reductions without polypectomyNo CRC reductions without polypectomy C-RADS 2 (intermediate polyps) choice C-RADS 2 (intermediate polyps) choice
for colonoscopy vs. surveillancefor colonoscopy vs. surveillance Repeat CTC in 3 years for intermediate Repeat CTC in 3 years for intermediate
polypspolyps Models suggest this will lead to 65 deaths Models suggest this will lead to 65 deaths
and 735 cancers/100,000 compared to and 735 cancers/100,000 compared to immediate referral for colonoscopyimmediate referral for colonoscopy
Hur Cet al. Clin Gastroenterol Hep 2007;5:237-44

CTC Cost Effectiveness of CTC Cost Effectiveness of PolypectomyPolypectomy
Pickardt et al. Am J Rad 2008. Pickardt et al. Am J Rad 2008. Polypectomy for small polyps not cost Polypectomy for small polyps not cost
effectiveeffective

Flexible SigmoidoscopyFlexible Sigmoidoscopy
ProsPros Easier prepEasier prep Technically easier Technically easier
procedureprocedure Less expensiveLess expensive No sedationNo sedation
ConsCons Prep often limits Prep often limits
examexam Higher miss ratesHigher miss rates No sedationNo sedation Limited extent of Limited extent of
examexam

Double Contrast Barium Double Contrast Barium Enema (DCBE)Enema (DCBE)
Essentially no data for screeningEssentially no data for screening Not recommended by ACG Not recommended by ACG
guidelinesguidelines DCBE replaced by CTCDCBE replaced by CTC Negative predictive value is lowNegative predictive value is low May be useful if CTC not May be useful if CTC not
available available

Cancer Detection TestsCancer Detection Tests
Offer only if cancer prevention test Offer only if cancer prevention test unavailableunavailable
Fecal immunochemistry, FIT testing Fecal immunochemistry, FIT testing is preferredis preferred
FOBTFOBT sDNAsDNA

Fecal Occult Blood Test Fecal Occult Blood Test (FOBT)(FOBT)
ProsPros Proven effective in Proven effective in
randomized trialsrandomized trials Non-invasiveNon-invasive Cost-effectiveCost-effective
ConsCons Relatively low Relatively low
mortality mortality reductions (15-reductions (15-33%)33%)
High false positiveHigh false positive Evaluation of pos Evaluation of pos
results often results often inadequateinadequate
OverusedOverusedMandel et al, N Engl J Med 1993;328:1365 Jorgensen et al, Gut 2002;50:29 Scholefield et al, Gut 2002;50:840 Lurie, Welch, J Natl Cancer Inst 1999;91:1641

False Positives and FOBTFalse Positives and FOBT
FoodsFoods Red meat, turnips, broccoli, horseradishRed meat, turnips, broccoli, horseradish
DrugsDrugs Colchicine, NSAIDs, anti-coagulants, Colchicine, NSAIDs, anti-coagulants,
iron supplements, reserpine, oxidizing iron supplements, reserpine, oxidizing agentsagents
Recent dental proceduresRecent dental procedures Sample obtained by DRESample obtained by DRE

Flex Sig plus FOBTFlex Sig plus FOBT
Little dataLittle data VA Cooperative study (CONcERN)VA Cooperative study (CONcERN)
Advanced lesionsAdvanced lesions Flex sig sens – 40-70%Flex sig sens – 40-70% FOBT sens – 24%FOBT sens – 24% Flex sig + FOBT – 45-76%Flex sig + FOBT – 45-76%
Lieberman DA, et al, NEJM 2000
Schoenfeld et al, NEJM 2005

Preferred Detection TestPreferred Detection TestFITFIT
FIT has comparable sensitivity and FIT has comparable sensitivity and higher specificity than FOBT = < false higher specificity than FOBT = < false positivespositives
Easier to perform, no dietary Easier to perform, no dietary restrictionsrestrictions
Improved compliance = better use of Improved compliance = better use of positivespositives

Preferred Detection TestPreferred Detection TestFITFIT
Nakajima M et al. Br J Cancer 2003;89:23-8

FIT vs. FOBTFIT vs. FOBT ~10,300 in each arm~10,300 in each arm 12.7% more FIT tests 12.7% more FIT tests
returnedreturned CancersCancers
FOBT- 11FOBT- 11 FIT- 24FIT- 24
Number to scope detection Number to scope detection to detect cancer were similarto detect cancer were similar
Overall detection rates for Overall detection rates for adenomas and cancers, FIT adenomas and cancers, FIT is superioris superior

Stool DNA TestingStool DNA Testing
Detects DNA shed from cancers and Detects DNA shed from cancers and adenomasadenomas
5 targets – 5 targets – K-RAS, P53, APC, BAT-26, long K-RAS, P53, APC, BAT-26, long DNADNA
SensitivitySensitivity Cancer – 52%Cancer – 52% Advanced adenoma – 15%Advanced adenoma – 15%
Specificity – 94%Specificity – 94% Feasibility and cost are major issuesFeasibility and cost are major issues

Screening Intervals – Screening Intervals – Average RiskAverage Risk
Colonoscopy – 10 yearsColonoscopy – 10 years CTC – 5 yearsCTC – 5 years DCBE – 5 yearsDCBE – 5 years Flex Sig – 5 yearsFlex Sig – 5 years FIT, sDNA, FOBT – 1 yearFIT, sDNA, FOBT – 1 year

Stopping Screening-Stopping Screening-USPSTFUSPSTF
Cancer Intervention and Cancer Intervention and Surveillance Modeling Network Surveillance Modeling Network
(CISNET)(CISNET) Life years saved outweighs costs and Life years saved outweighs costs and
harms in patients 50-75 years harms in patients 50-75 years undergoing FOBT, flex sig, colonoscopy undergoing FOBT, flex sig, colonoscopy in US persons aged 50-75.in US persons aged 50-75.
No clear benefit in these models after No clear benefit in these models after age 75.age 75.

Questions?Questions?