collaboration toward universal perioperative documentation: phase 2 clinical testing susan v.m....
TRANSCRIPT

Collaboration Toward Universal Perioperative
Documentation: Phase 2 Clinical Testing
Susan V.M. Kleinbeck, RN, PhD, CNOR

Collaborators
Kathie Shea RN, BSN, CNOR, Alameda County Research Chair and members of the research committee
Doris Gaw, RN, CNOR & Judy Carlson, RN, CNOR, Greater Kansas City Research Co-chairs and members of the research committee
Susan V.M. Kleinbeck, RN, PhD, CNOR, University of Kansas, nurse scientist for the project.

Background
The Perioperative Nursing Data Set (PNDS) is a nationally recognized nursing language that offers the potential of standardized perioperative patient records. Phase 1 of this study used the Delphi consensus-building method to identify the minimum PNDS nursing interventions and expected outcomes believed by experienced nurses essential to patient documentation.

Purpose
Operationalize the minimum PNDS data elements identified by consensus for a universal written pre/intraoperative record
Clinically test the new written record in a variety of perioperative settings

Research Questions
Does the written pre/intraoperative record have clarity and ease of use in clinical practice?
What recommendations do experienced perioperative nurses suggest for improvement of the new written pre/intraoperative record?

Conceptual Framework
©AORN. Inc.
To maintain construct validity, interventions and outcomes were taken from original Perioperative Nursing Data Set documents published by AORN, Inc.

Phase 1: Minimum Data Identified
Phase 1 funded by AORN Foundation
PNDS
Agency Data
Universal Minimum Record
All Perioperative DataConsensus achieved as to the ideal minimum PNDS interventions and outcomes needed on a universal patient record

Phase 2: The Written Record
Check-box format Chronological order Content Validity 100%
agreement (n=21) Applicability to clinical
setting 98% agreement
Preoperative / Intraoperative
record

Sections of Record
Pre-admission Preop assessment Preparation
immediately before OR Intraoperative Postop and Discharge
from the OR
Preoperative / Intraoperative
record

Testing Procedure
No names of patients, surgeons, or facilities were recorded
Assigned case was documented in usual manner, then test chart was documented
Charting Rules:
check in box indicates yes
no mark in box indicates no or none

Testing Sample
38 RN volunteers, 29 with CNOR 57 Records tested
Urban/suburban -45 Rural-1222 KS, 13 MO, 12 CA10 unknown state
4-22 OR Rooms All surgical services in testing

Pre-Admit ExampleDate of Interview/Teaching ______________ Phone In facility Preoperative Teaching: Proposed Surgery __________________________________ Surgeon __________Teaching Protocol:_____________________________________________________
NPO Guidelines Time and*Date to Arrive:__________*_____Postop expectations Discharge See Nurses’ Notes
Advanced directive: On file Declines info Power of atty DNR verified Present for teaching: Patient Family Friend Translator____________Materials provided: Verbal Written Video Teaching by:__________Allergies:NKA (=yes has no known allergies)
Meds: _________________ Reactions_______________________Food: _________________ Reactions_______________________Prep Sol: ______________ Reactions_______________________Latex: if yes OR Notified Reactions_______________________
Infor given
*Indicates changes suggested: added terms

Preop Assessment Example
Skin: Warm Dry Cool Wet Without evidence of rash, swelling, inflammation
Musculoskeletal: Needs assistance Moves all extremities Steady balance/gait Limited mobility Pulses present in operative limb Pulses absent in operative limb
Neuro:Alert Memory intact Speech clear Hearing deficit Visual deficit Language deficitOriented Disoriented to: Person Place Time Situation Responds only with stimuli*Pain on a 0-10 scale (10 = high pain) _______ Location: ____________
*Needs to be bold to increase documentation of pain
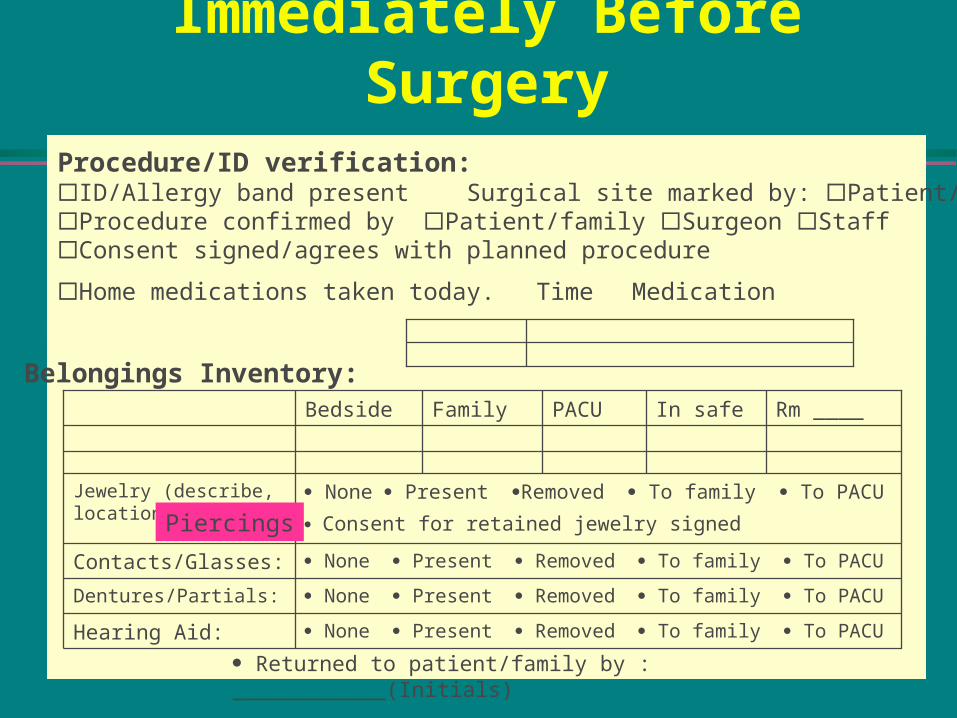
Procedure/ID verification:ID/Allergy band present Surgical site marked by: Patient/family Surgeon StaffProcedure confirmed by Patient/family Surgeon StaffConsent signed/agrees with planned procedure
Home medications taken today. Time Medication
None Present Removed To family To PACUHearing Aid:
None Present Removed To family To PACUDentures/Partials:
None Present Removed To family To PACUContacts/Glasses:
None Present Removed To family To PACU
Consent for retained jewelry signed
Jewelry (describe, location)
Rm ____In safePACUFamilyBedside
Belongings Inventory:
Returned to patient/family by : ____________(Initials)
Piercings
Immediately Before Surgery

Positioning/Safety Aids: Safety Belt________ Warm blanket Head rest: Type __________ Pressure protection pad Site:_____________ Chest roll Shoulder roll Axillary roll Pillow/wedge Sandbag Beanbag Stirrup/*Leg Holder Boot Sling Cysto/Gyn padded with blanket Arm rest padded/secured: L R Arms tucked/padded: L R Other ______________________________________________________________ Body alignment checked Positioned by: _____________________________Skin Prep: Hair: Clipped Shaved __________ Hair removal by______________Iodophor scrub Iodophor solution Duraprep Hibiclens Alcohol Other_______Prep by _____________Wound class:
Site 1________________ I II III IV 4 No IncisionElectrocautery: Location __________________________
Unit #______ Coag/Cut ________ Pad _________ Location ______________Bipolar # ________ Setting _______________
Tourniquet: Location ___________ TestedUnit# ______ Setting ______ Up ____ Down _____ Applied by __________
Intraoperative Example
*Term unclear:

Discharge from ORPatient Outcomes at Discharge for OR
Postop Assessment at Discharge for OR
Physiological status within acceptable limits for discharge from OR
Skin warm and dry
Cool WetSkin color consistent with adequate profusionPulses present in operated extremity
Pulses absent operated extremityDressing dry and intactRespirations spontaneous
Assisted IntubatedConsciousness: able to follow directions
Non-responsiveResponds when stimulated
See discharge note

Content Analysis Summary
Positive Commentscheck marks minimal writingpostop assessmentcompletenessliked flow preop to
intraop
Negative Commentsseparate pre/intrachange sponge
count tableseparate sheet for
laser and local monitoring
want human graphic to label

Perioperative Implications
A tested clinical record is prerequisite to the development of computerized standards for a universal perioperative patient record.
Phase 3 of the project will develop data field names with attached PNDS construct validity codes.