cognitive therapy of anxiety disorders -...
TRANSCRIPT

journal of Consulting and Clinical Psychology1993. Vol. 61, No. 2. 248-260
Copyright 1993 by the American Psychological Association. Inc0022-006X/93/J3.00
Cognitive Therapy of Anxiety Disorders
Dianne L. Chambless and Martha M. Gill is
A review of studies of cognitive-behavioral therapy (CBT) for generalized anxiety disorder, panicdisorder with and without agoraphobia, and social phobia indicates that CBT is consistently moreeffective than waiting-list and placebo control groups. In general, CBT has proved more beneficialthan supportive therapy as well. Comparisons with active behavioral treatments provide morevariable results. Converging evidence suggests that cognitive change may be a strong predictor oftreatment outcome, but that such change may be produced by a number of therapeutic approaches.Pretest-posttest change with CBT is depicted in meta-analytic summary form for each disorder.
In a seminal article, Beck, Laude, and Bohnert (1974) demon-strated that anxious clients report characteristic patterns ofthinking, such that increments in anxiety are accompanied bythoughts and images of social or physical harm, or both. Theresults of this early report have proved consistent with anemerging body of self-report and laboratory experimental find-ings concerning the cognitive psychopathology of anxiety dis-orders (see review by Chambless, 1988). Analysis of the contentof anxiety clients' thoughts provides some support for Beck andEmery's (1985) hypothesis of disorder specificity in anxiouscognitions. Thus, clients with panic disorder, with or withoutagoraphobia, are primarily concerned with harm to their physi-cal well-being caused by panic symptoms (part of the processdubbed "fear of fear" by Goldstein & Chambless, 1978),whereas clients with social phobia are more concerned withsocial failure (e.g., see Chambless & Gracely, 1989; Hope, Rapee,Heimberg, & Dombeck, 1990). The concerns of clients withgeneralized anxiety disorder are more diffuse, involvingthoughts of loss of control (e.g., Chambless & Gracely, 1989) andheightened vigilance for threats of both a social and physicalnature (e.g., MacLeod, Mathews, & Tata, 1986). The centralityof this diffuse pattern of worry for clients with generalizedanxiety disorder has been sufficiently documented (see reviewby Borkovec, Shadick, & Hopkins, 1991) that the criteria of thethird edition of the Diagnostic and Statistical Manual of MentalDisorders (DSM-HI) were changed to require excessive worryfor assignment of the generalized anxiety disorder diagnosis(see DSM-HI vs. DSM-III-R criteria; American PsychiatricAssociation, 1980,1987).
A variety of approaches have been used to modify cognitionsof anxious clients, most commonly rational-emotive therapy
Dianne L. Chambless and Martha M. Gillis, Department of Psychol-ogy, American University.
Preparation of this article was supported by National Institute ofMental Health Grant R01-MH44190-03.
We thank David A. F. Haaga for his valuable comments on a draft ofthis article and the following individuals for providing data: Aaron T.Beck, Thomas Borkovec, Gillian Butler, David Clark, Jurgen Margraf,Larry Michelson, and Lars-Goran 6st.
Correspondence concerning this article should be addressed toDianne L. Chambless, Department of Psychology, American Univer-sity, Washington, DC 20016-8062.
(RET; Ellis, 1962), self-instructional training (SIT; Meichen-baum, 1975), and Beck and Emery's (1985) model of cognitivetherapy. Therapy components include teaching clients to iden-tify and label irrational thoughts and to replace them with posi-tive self-statements or modify them by challenging their verac-ity. The cognitive modification approaches are often combinedwith behavioral treatments such as exposure or relaxation train-ing. The behavioral components are viewed either as importantin their own right or as a vehicle for practicing cognitive tech-niques. Hence, we will use the term cognitive-behavioral ther-apy (CBT) in this review.
For this brief review, we surveyed the results of cognitivetherapies for three anxiety disorders for which a substantialbody of treatment research on clinical samples is available: gen-eralized anxiety disorder, panic disorder with and withoutagoraphobia, and social phobia. For a descriptive summary, wehave converted treatment findings into effect sizes when au-thors provided means and standard deviations for the measuresacross treatment. We calculated two types of effect sizes usingM. L. Smith and Glass's delta (1977). To include the many stud-ies in which the effects of one treatment were compared, notwith a waiting-list control or placebo group, but only with an-other treatment, we first computed crude pretest-posttest andpretest-follow-up effects using the following formula: (Afprelest -Mposmsl)/SDpKKiV Second, for those studies with waiting-list orplacebo controls, we calculated controlled effect sizes compar-ing the posttest or follow-up scores of treatment groups withcontrol groups using the formula (A/control - M,realmem)/SZ)control.When multiple measures of a construct were used, we averagedeffect sizes for that construct within each study.
Generalized Anxiety Disorder
We located nine clinical trials for generalized anxiety dis-order in which clients were selected according to DSM-HI orDSM-III-R criteria (American Psychiatric Association, 1980,1987) or Research Diagnostic Criteria, thus enhancing the prob-ability of reasonably homogeneous samples.1 In seven of these
1 In two studies (Barlow et al., 1984; Borkovec & Mathews, 1988),clients with panic disorder were included in the sample. These investi-gations have been retained for this article because in both cases there
248

SPECIAL SECTION: COGNITIVE THERAPY OF ANXIETY DISORDERS 249
studies, data necessary for inclusion in a meta-analytic sum-mary were published or provided by the authors (see Table 1).Measures included in this analysis were interview (typically theHamilton Anxiety Scale [Hamilton, 1959]) and self-reportquestionnaires (e.g., the Zung Self-Rating of Anxiety [Zung,1971] and the Beck Anxiety Inventory [Beck & Steer, 1990]).
In almost all trials, Beck and Emery's (1985) version of CBTwas combined with one or more additional behavioral tech-niques, most commonly progressive relaxation training andmore rarely self-control desensitization or electromyogram bio-feedback. The exception is the study by Butler, Fennell, Rob-son, and Gelder (1991), who seem to have used Beck-EmeryCBT alone. The one study not based on the Beck and Emerymanual was that by Butler, Cullington, Hibbert, Klimes, andGelder (1987), who examined the effects of an anxiety manage-ment training package including positive self-talk, relaxation,exposure, and pleasant events scheduling, as well as challengingirrational thoughts.
Is CBT for Generalized Anxiety Disorder Effective?
The uncontrolled pretest-posttest effect sizes in Table 1 indi-cate that CBT consistently has a substantial impact on anxietymeasures. The effect sizes for the studies by Power and col-leagues (Power, Jerrom, Simpson, Mitchell, & Swanson, 1989;Power et al., 1990) are unusually large; however, the placeboresponse effect sizes are also very high for these studies, yield-ing controlled effect sizes comparable to those for other investi-gations. Although the reasons for these investigators' discrep-ant findings are not clear, the brief duration of their clients'disorder (3 or 4 months on average) may be related to an espe-cially powerful response to any intervention.2 When comparedwith the effects of control groups, the average effect size forCBT (including the Power et al. data) continues to be quite large(M= 1.54).
Figure 1 depicts the results of five studies in which CBT wascompared with one of several control conditions: pill placebo(Power et al., 1989, 1990), nondirective therapy (Borkovec &Costello, 1992), or waiting list (Butler, Cullington, et al., 1987;Butler et al., 1991). Not shown (requisite data were not avail-able), but also including nondirective therapy, waiting-list con-trol groups, or both, are studies by Barlow et al. (1984) andBlowers, Cobb, and Mathews (1987). In all seven investigations,CBT was more effective than waiting list or pill placebo atposttest.
The results of the two studies using nondirective therapy tocontrol for nonspecific treatment effects are conflicting, de-spite some collaboration between the two research groups.Whereas Borkovec and Costello (1992) found CBT superior tonondirective therapy, Blowers et al. (1987) did not. However, inthe latter study CBT was superior to a waiting-list control whennondirective therapy, yielding an intermediate response rate,was not. A number of methodological differences between thetwo studies might account for the discrepant findings. In the
were no significant differences in treatment response for the general-ized anxiety disorder versus panic disorder groups.
more recent study, Borkovec and Costello included a number ofimportant methodological refinements that should reduce vari-ance and provide a cleaner picture of the results. In addition,Borkovec and Costello provided subjects with 50% more treat-ment sessions (12 vs. 8), including slower and more thoroughtraining in relaxation, and added self-control desensitization totheir treatment package.
Do CBT Effects Persist Once Treatment Has Ended?
Examination of the uncontrolled pretest-follow-up effectsizes in Table 1 demonstrates that treatment effects were main-tained or augmented over 6-12 months of follow-up. The largeeffect size for the Borkovec and Costello (1992) study is particu-larly impressive in that the data reported are for subjects whoreceived no further treatment during the follow-up period.Comparison of CBT and control groups at follow-up is problem-atical in that, for ethical reasons, control subjects generally re-ceive treatment after posttest. Thus, the only controlled follow-up contrasts are from the two trials comparing CBT with non-directive therapy. In the Blowers et al. (1987) study, CBT andnondirective therapy continued to be equivalent 6 months aftertreatment. Borkovec and Costello (1992) also found no differ-ences between treatments at follow-up, but these long-term out-come data were confounded in that, because of their poor ini-tial treatment response, significantly more nondirective ther-apy clients received additional treatment during the follow-upperiod (61% of nondirective clients vs. 16% of CBT clients).
Is CBT More Effective Than Behavioral Treatments forGeneralized Anxiety Disorder?
Borkovec and colleagues compared CBT plus relaxation andnondirective therapy plus relaxation in studies with college stu-dents with generalized anxiety disorder (Borkovec et al., 1987)and with a more severely anxious community sample (Borkovec& Mathews, 1988). Despite the similarity in the protocols andhigh level of methodological refinement in both studies, theresults are conflicting. Only with the student sample was CBTsuperior to nondirective therapy plus relaxation; for the clinicalsample, effects of the two treatments were similar at posttestand 12-month follow-up. However, these differences may bemore apparent than real. The superiority of CBT for the stu-dent sample was found only for self-report questionnaires. Theeffect sizes for comparison of CBT and nondirective therapyplus relaxation on the assessor-rated Hamilton Anxiety Scaleare comparable and modestly, if not statistically significantly, infavor of CBT in both investigations (student effect size = 0.32,clinical effect size = 0.43). Hence, these discrepancies may re-flect the sampling variance associated with tests of modesteffects at low power. Nevertheless, on the basis of this research,one cannot safely conclude that the CBT effects depicted inTable 1 and Figure 1 reflect more than simple nonspecific treat-ment effects in combination with relaxation training.
2 For a diagnosis of generalized anxiety disorder according to theDSM-IH-R, symptoms must have persisted for 6 months; however, aduration of only 1 month was required under the DSM-HI scheme.
250 DIANNE L. CHAMBLESS AND MARTHA M. GILLIS
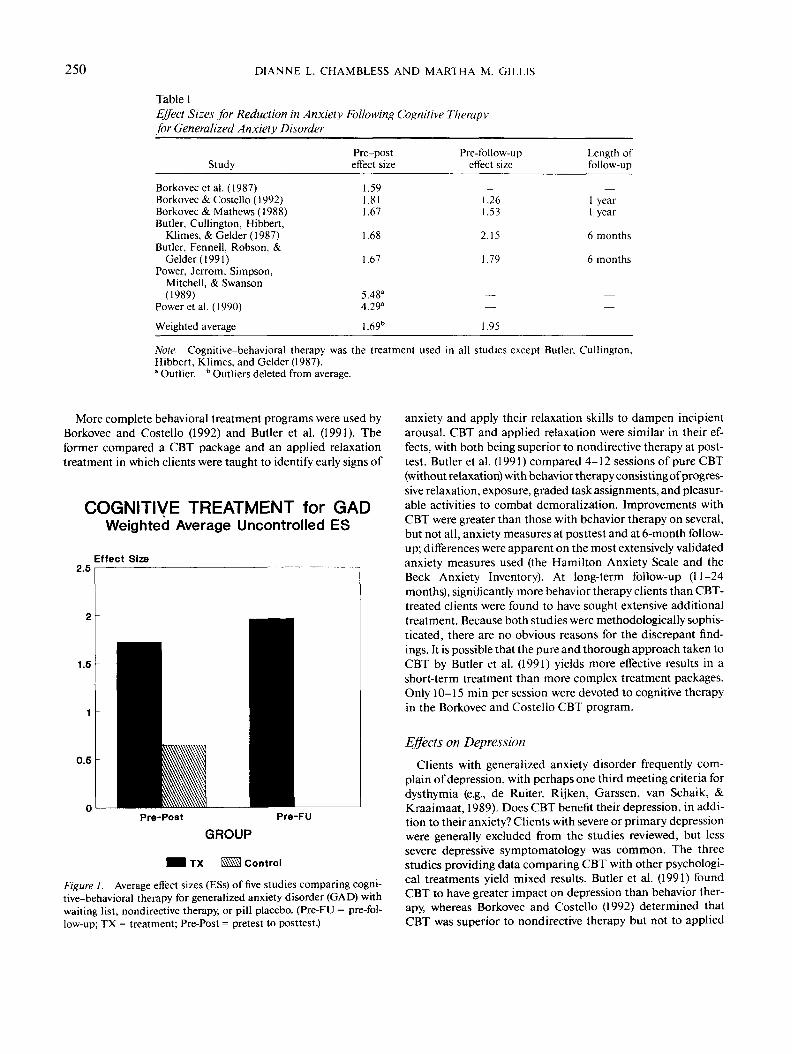
Table 1Effect Sizes for Reduction in Anxiety Following Cognitive Therapyfor Generalized Anxiety Disorder
Study
Borkovec et al. (1987)Borkovec & Costello (1992)Borkovec & Mathews (1988)Butler, Cullington, Hibbert,
KJimes, &Gelder(1987)Butler, Fennell, Robson, &
Gelder(1991)Power, Jerrom, Simpson,
Mitchell, & Swanson(1989)
Power et al. (1990)
Weighted average
Pre-posteffect size
1.591.811.67
1.68
1.67
5.48"4.29"
1.69b
Pre-follow-upeffect size
1.261.53
2.15
1.79
——
1.95
Length offollow-up
_1 year1 year
6 months
6 months
——
Note. Cognitive-behavioral therapy was the treatment used in all studies except Butler, Cullington,Hibbert, Klimes, and Gelder (1987)." Outlier. b Outliers deleted from average.
More complete behavioral treatment programs were used byBorkovec and Costello (1992) and Butler et al. (1991). Theformer compared a CBT package and an applied relaxationtreatment in which clients were taught to identify early signs of
COGNITIVE TREATMENT for GADWeighted Average Uncontrolled ES
Effect Size
Pre-Post Pre-FU
GROUP
I TX Control
Figure 1. Average effect sizes (ESs) of five studies comparing cogni-tive-behavioral therapy for generalized anxiety disorder (GAD) withwaiting list, nondirective therapy, or pill placebo. (Pre-FU = pre-fol-low-up; TX = treatment; Pre-Post = pretest to posttest.)
anxiety and apply their relaxation skills to dampen incipientarousal. CBT and applied relaxation were similar in their ef-fects, with both being superior to nondirective therapy at post-test. Butler et al. (1991) compared 4-12 sessions of pure CBT(without relaxation) with behavior therapy consisting of progres-sive relaxation, exposure, graded task assignments, and pleasur-able activities to combat demoralization. Improvements withCBT were greater than those with behavior therapy on several,but not all, anxiety measures at posttest and at 6-month follow-up; differences were apparent on the most extensively validatedanxiety measures used (the Hamilton Anxiety Scale and theBeck Anxiety Inventory). At long-term follow-up (11-24months), significantly more behavior therapy clients than CBT-treated clients were found to have sought extensive additionaltreatment. Because both studies were methodologically sophis-ticated, there are no obvious reasons for the discrepant find-ings. It is possible that the pure and thorough approach taken toCBT by Butler et al. (1991) yields more effective results in ashort-term treatment than more complex treatment packages.Only 10-15 min per session were devoted to cognitive therapyin the Borkovec and Costello CBT program.
Effects on Depression
Clients with generalized anxiety disorder frequently com-plain of depression, with perhaps one third meeting criteria fordysthymia (e.g., de Ruiter, Rijken, Garssen, van Schaik, &Kraaimaat, 1989). Does CBT benefit their depression, in addi-tion to their anxiety? Clients with severe or primary depressionwere generally excluded from the studies reviewed, but lesssevere depressive symptomatology was common. The threestudies providing data comparing CBT with other psychologi-cal treatments yield mixed results. Butler et al. (1991) foundCBT to have greater impact on depression than behavior ther-apy, whereas Borkovec and Costello (1992) determined thatCBT was superior to nondirective therapy but not to applied

SPECIAL SECTION: COGNITIVE THERAPY OF ANXIETY DISORDERS 251
relaxation. In contrast, Borkovec et al. (1987) found no signifi-cantly superior CBT effects for depression among treatmentcompleters. However, the low levels of pretreatment depressionin this student sample may have made the detection of differen-tial treatment effects unlikely. In all three studies, the authorsreported having to drop clients from the nondirective, appliedrelaxation, or behavior therapy conditions because of increaseddepression; no such losses occurred in the CBT groups. Thus,CBT may have an added benefit in addressing mixed anxietyand depression among clients with generalized anxiety dis-order. Given the considerable comorbidity of anxiety and de-pression, this question warrants further study.
Effects on Cognitive Measures
Only three of the studies reviewed here included an examina-tion of cognitive changes. In the earliest effort, Blowers et al.(1987) assessed self-report of the perceived controllability andintensity of cognitive symptoms of anxiety. Both nondirectiveand CBT groups reported greater reduction in intensity thanthe waiting-list group, but only the CBT group reported signifi-cantly enhanced control over cognitive symptoms comparedwith the waiting-list group. Butler et al. (1991) used five mea-sures of anxious cognition. Pure CBT yielded better resultsthan behavior therapy on two measures at posttest and on allfive measures at 6-month follow-up. Using the Penn StateWorry Questionnaire (Meyer, Miller, Metzger, & Borkovec,1990), Borkovec and Costello (1992) found that CBT led togreater reductions in worry than did nondirective therapy; ap-plied relaxation and CBT were equivalent in their effects. Labo-ratory measures of thoughts and imagery also showed thattreatment responders in this study became more like normalsubjects in their mentation, regardless of therapy type (Borko-vec & Inz, 1990). Thus, a variety of treatment procedures maylead to change on cognitive measures; CBT may result ingreater cognitive change than other therapies only when it is themore effective treatment for the clients' overall symptoms.
Panic Disorder and Agoraphobia
Although dichotomizing clients with panic disorder intothose with and without agoraphobia belies a continuum ofavoidance, we will follow this convention because (a) samplesare described in this fashion and (b) severity of phobic avoid-ance may have some effect on outcome (Clum, 1989). Studiesincluded in our meta-analysis all followed DSM-III or DSM-III-R criteria for selection. Samples in some earlier studies onagoraphobia described here were selected on the basis of clini-cal interviews, whereas later studies relied on structured, reli-able diagnostic interviews.
Because the effects of exposure on phobic features of panicdisorder are well documented and have already been summa-rized in meta-analytic form (see reviews by Jansson & 6st,1982; Trull, Nietzel, & Main, 1988), and because studies withcognitive therapy omitting exposure are rare, we did not focuson avoidance behavior in our meta-analytic summary. Rather,we prepared effect size summaries of data on generalized anxi-ety, diary-rated panic frequency, and fear of fear. Measures of
fear of fear included the Agoraphobic Cognitions Question-naire (Chambless, Caputo, Bright, & Gallagher, 1984), thePanic Belief Questionnaire (Greenberg, 1989), and the BodySensation Interpretation Questionnaire (Clark et al., 1991), allof which measure catastrophic misinterpretation of panicsymptoms or fear of interoceptive cues associated with panic.Also, we note the percentage of subjects reporting themselves tobe panic free after treatment.
Cognitive Therapy of Agoraphobia
Is cognitive therapy effective for agoraphobia? There are notrials of CBT as a sole treatment for agoraphobia comparedwith control groups. Rather, the research question has beenwhether CBT can equal or surpass the established treatment ofchoice, in vivo exposure. In two studies, Emmelkamp and col-leagues (Emmelkamp, Brilman, Kuiper, & Mersch, 1986; Em-melkamp, Kuipers, & Eggeraat, 1978) compared the efficacy ofSIT or RET alone with exposure. In each case, brief cognitiveinterventions (5 or 6 sessions over a 1 - or 3-week period) failed toequal the success of equivalent amounts of the benchmark ex-posure treatment.
Does cognitive therapy add to the effects of exposure foragoraphobia? Investigators comparing cognitive modificationplus exposure with exposure alone have used a variety of ap-proaches: paradoxical intention, SIT, RET, and Beck-EmeryCBT (Emmelkamp & Mersch, 1982; Michelson, Mavissaka-lian, & Marchione, 1988; Michelson, Marchione, & Green-wald, 1989; Ost, Westling, & Hellstrom, 1991; Williams&Rap-poport, 1983). Pretest-posttest effect sizes are depicted in Ta-ble 2; the subset from studies comparing combined treatmentswith a control group are included in Figure 2. Combined treat-ments were consistently more effective than waiting-list controlgroups, but in only one investigation did combined treatmentexceed the effects of exposure alone. In that study, Michelson etal. (1989) found that adding Beck-Emery CBT to exposure foragoraphobia led to significantly better results on some mea-sures of phobia and panic and on a composite measure of highend-state functioning at follow-up. Michelson et al.'s data maybe unique because they are the only investigators to have com-bined Beck-Emery CBT with exposure for agoraphobics (allcognitive therapies may not be created equal). Another impor-tant factor may be the longer treatment (16 sessions) Michelsonet al. provided.
Cognitive Therapy of Panic Disorder
CBT of panic disorder, following Clark and Salkovskis's (inpress) model (an adaptation of Beck-Emery CBT specificallydevised for this disorder), has now been tested in six trials con-ducted in four nations (see Table 3). In all studies, CBT yieldedvery large effect sizes for fear of fear, generalized anxiety, andpanic frequency; these effect sizes were maintained or en-hanced at follow-up of 1-12 months duration (effect sizes atfollow-up averaged 1.00-1.73). An average of 85% of the clientswere panic free at posttest and 88% at follow-up.
Comparisons with control groups. For three of the six studiesdescribed, control group data are available for either a waiting-
252 DIANNE L. CHAMBLESS AND MARTHA M. GILLIS
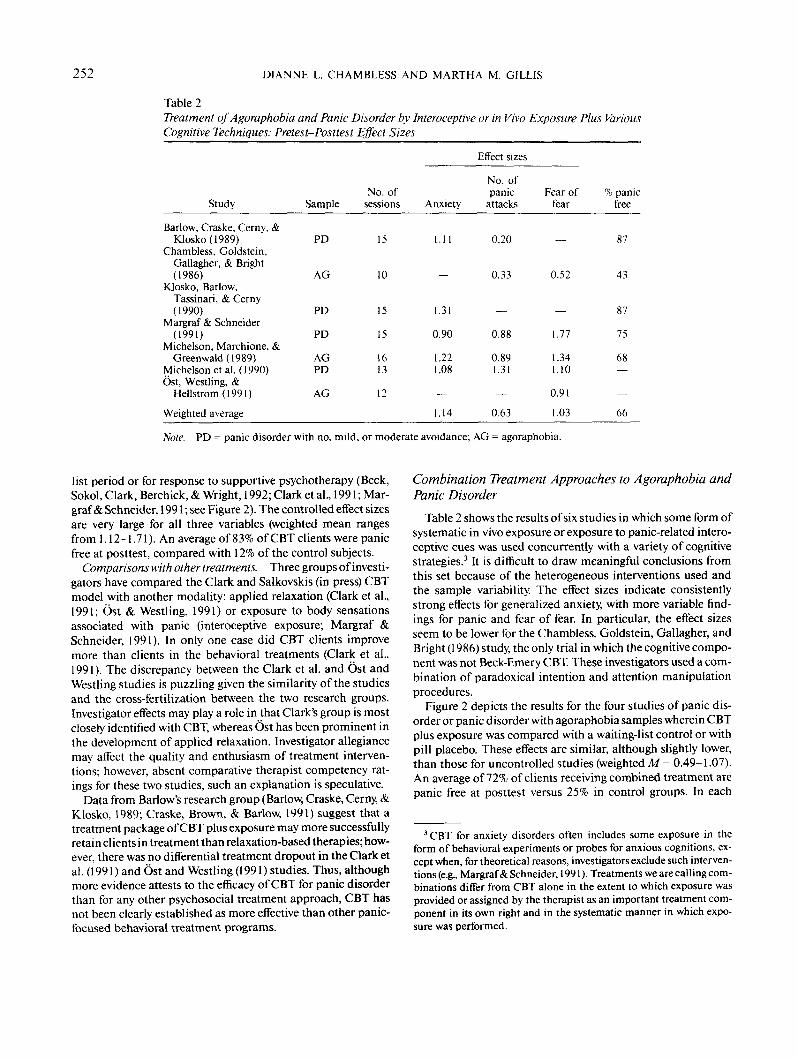
Table 2Treatment of Agoraphobia and Panic Disorder by Intemceptive or in Vivo Exposure Plus VariousCognitive Techniques: Pretest-Posttest Effect Sizes
Effect sizes
Study
Barlow, Craske, Cerny, &Klosko(1989)
Chambless, Goldstein,Gallagher, & Bright(1986)
Klosko, Barlow.Tassinari, & Cerny(1990)
Margraf & Schneider(1991)
Michelson, Marchione, &Greenwald(1989)
Michelson etal. (1990)Ost, Westling, &
Hellstrom(1991)
Weighted average
Sample
PD
AG
PD
PD
AGPD
AG
No. ofsessions
15
10
15
15
1613
12
Anxiety
1. 11
—
1.31
0.90
1.221.08
—
1.14
No. ofpanic
attacks
0.20
0.33
—
0.88
0.891.31
—
0.63
Fear offear
—
0.52
—
1.77
1.341.10
0.91
1.03
% panicfree
87
43
87
75
68—
—
66
Note. PD = panic disorder with no, mild, or moderate avoidance; AG = agoraphobia.
list period or for response to supportive psychotherapy (Beck,Sokol, Clark, Berchick, & Wright, 1992; Clark et al., 1991; Mar-graf & Schneider, 1991; see Figure 2). The controlled effect sizesare very large for all three variables (weighted mean rangesfrom 1.12-1.71). An average of 83% of CBT clients were panicfree at posttest, compared with 12% of the control subjects.
Comparisons with other treatments. Three groups of investi-gators have compared the Clark and Salkovskis (in press) CBTmodel with another modality: applied relaxation (Clark et al.,1991; Ost & Westling, 1991) or exposure to body sensationsassociated with panic (interoceptive exposure; Margraf &Schneider, 1991). In only one case did CBT clients improvemore than clients in the behavioral treatments (Clark et al.,1991). The discrepancy between the Clark et al. and Ost andWestling studies is puzzling given the similarity of the studiesand the cross-fertilization between the two research groups.Investigator effects may play a role in that Clark's group is mostclosely identified with CBT, whereas Ost has been prominent inthe development of applied relaxation. Investigator allegiancemay affect the quality and enthusiasm of treatment interven-tions; however, absent comparative therapist competency rat-ings for these two studies, such an explanation is speculative.
Data from Barlow's research group (Barlow, Craske, Cerny, &Klosko, 1989; Craske, Brown, & Barlow, 1991) suggest that atreatment package of CBT plus exposure may more successfullyretain clients in treatment than relaxation-based therapies; how-ever, there was no differential treatment dropout in the Clark etal. (1991) and Ost and Westling (1991) studies. Thus, althoughmore evidence attests to the efficacy of CBT for panic disorderthan for any other psychosocial treatment approach, CBT hasnot been clearly established as more effective than other panic-focused behavioral treatment programs.
Combination Treatment Approaches to Agoraphobia andPanic Disorder
Table 2 shows the results of six studies in which some form ofsystematic in vivo exposure or exposure to panic-related intero-ceptive cues was used concurrently with a variety of cognitivestrategies.3 It is difficult to draw meaningful conclusions fromthis set because of the heterogeneous interventions used andthe sample variability. The effect sizes indicate consistentlystrong effects for generalized anxiety, with more variable find-ings for panic and fear of fear. In particular, the effect sizesseem to be lower for the Chambless, Goldstein, Gallagher, andBright (1986) study, the only trial in which the cognitive compo-nent was not Beck-Emery CBT. These investigators used a com-bination of paradoxical intention and attention manipulationprocedures.
Figure 2 depicts the results for the four studies of panic dis-order or panic disorder with agoraphobia samples wherein CBTplus exposure was compared with a waiting-list control or withpill placebo. These effects are similar, although slightly lower,than those for uncontrolled studies (weighted M= 0.49-1.07).An average of 72% of clients receiving combined treatment arepanic free at posttest versus 25% in control groups. In each
3 CBT for anxiety disorders often includes some exposure in theform of behavioral experiments or probes for anxious cognitions, ex-cept when, for theoretical reasons, investigators exclude such interven-tions (e.g., Margraf & Schneider, 1991). Treatments we are calling com-binations differ from CBT alone in the extent to which exposure wasprovided or assigned by the therapist as an important treatment com-ponent in its own right and in the systematic manner in which expo-sure was performed.

SPECIAL SECTION: COGNITIVE THERAPY OF ANXIETY DISORDERS 253
Cognitive Therapy EffectsAlone and Combined with Exposure
Eliect Size*
Anxiety # of Panics Fear oi Fear
Outcome Measure
Cog Tz lor PD
Comb Ti/PD & AGOR
PD Control
Comb Control
Figure 2. Average effect sizes of three studies comparing Beck-Emery/Clark-Salkovskis cognitive therapy for panic disorder withwaiting list or supportive therapy and four studies comparing cogni-tive-behavioral therapy for panic disorder (PD) with and without ago-raphobia (AGOR) with waiting list or pill placebo. ('Weighted averageby outcome measure. Cog = cognitive; TX = treatment; Comb = com-bined.)
study, CBT was associated with more change than a waitingperiod. Although Klosko, Barlow, Tassinari, and Cerny (1990)did not find CBT to yield better results than pill placebo, withthe exception of the CBT clients' greater achievement of panic-free status, posttest comparisons of completer samples in thisstudy are compromised by the significantly higher placebogroup drop-out rate.
In the one study that compared the effects of combined cog-nitive therapy plus exposure (interoceptive) with Clark-Salkov-skis cognitive therapy alone (carefully eschewing behavioral in-terventions), Margraf and Schneider (1991) observed no addi-tional benefit for the combined treatment package with theirpanic disorder clients. Similarly, Barlow and colleagues (Barlowet al., 1989; Craske et al., 1991) found that adding relaxation totheir Beck-Emery CBT plus interoceptive exposure package forpanic disorder provided no better results than Beck-EmeryCBT plus interoceptive exposure alone. At posttest and 6-month follow-up, the groups receiving CBT and interoceptiveexposure, alone or in combination, fared better than the relax-ation group on a number of measures. Moreover, the relaxationgroup was more likely to drop out during treatment and to havesought additional treatment by the 2-year follow-up.
Thus, although CBT in combination with behavioral tech-
niques has been established as an effective treatment for panicdisorder, it is doubtful that combination treatments are moreeffective than CBT alone, at least for panic disorder withoutagoraphobia. For severely phobic cases, the findings might bedifferent; additional research on this question is required.
CBT Effects on Associated Psychopathology
Effects on depression. Depression is a common feature ofpanic disorder. For example, Renneberg, Chambless, andGracely (1992) found 15% of panic disorder clients to sufferfrom current major depression and 27% from dysthymia. Com-parisons with waiting-list control groups demonstrate that de-pressed mood is ameliorated by CBT (Chambless et al, 1986;Clark et al, 1991). However, the available studies do not indi-cate that CBT's effects are greater than those of other behav-ioral or supportive treatments (Beck et al, 1992; Clark et al,1991; Emmelkamp et al, 1978; Margraf & Schneider, 1991; Mi-chelson et al, 1988). Depression among these clients often re-sults from demoralization, and any treatment instilling hope ofchange or leading to relief from panic may be sufficient. Note,however, that some investigators excluded clients in a majordepressive episode (exclusion when depression was the primaryproblem was typical), and none have tested the possible moder-ating effects of major depression on treatment outcome. Givenits success in treatment of depression (see Dobson, 1989), CBTmight have superior effects for panic disorder clients with ma-jor depression. In light of the frequent comorbidity of thesedisorders, this hypothesis is worth testing.
Cognitive change. Comparisons of CBT and waiting-listcontrol groups show that the cognitively based treatments areeffective in reducing negative cognitions about the disastrouseffects of panic as assessed by questionnaires or audiotapedreports of thoughts collected during behavioral avoidance tests(Chambless et al, 1986; Clark et al, 1991; Margraf & Schneider,1991; Williams & Rappoport, 1983). Tests of treatment effectson laboratory measures of cognitive schemata have yet to bereported.
The positive effects on cognitive measures cannot be said tobe exclusive to CBT. In a set of five studies comparing CBT andother treatments such as exposure alone and applied relaxation(Emmelkamp et al, 1986; Margraf & Schneider, 1991; Michel-son et al, 1989; Williams & Rappoport, 1983), only Clark et al.(1991) found CBT to have superior effects on cognitive mea-sures, despite some overlap in the cognitive measures usedacross investigations. Recall that CBT in the Clark et al. studywas the most efficacious treatment on a number of outcomemeasures.
Normalization of the cognitive responses of panic disorderclients after CBT has been investigated by three researchgroups, with conflicting results. Although both Chambless etal. (1986) and Williams and Rappoport (1983) found decre-ments in agoraphobic clients' negative cognitions after treat-ment, clients still reported higher levels of negative thinkingabout anxiety than did normal control subjects. On the otherhand, Michelson, Schwartz, and Marchione (1992), examiningthe States of Mind ratio (number of positive thoughts divided bythe number of positive and negative thoughts), found that agora-

254 DIANNE L. CHAMBLESS AND MARTHA M. GILLIS
Table 3Cognitive Therapy for Panic Disorder: Pretest-Posttest Effects of Studies Usingthe Beck and Emery/Clark and Salkovskis Model
Effect sizes
Study
Beck, Sokol, Clark, Berchick,& Wright (1992)
Clark etal. (1991)Margraf & Schneider ( 1 99 1 )Newman, Beck, Beck, & Tran
(1990)6st&Westling(1991)Sokol, Beck, Greenberg,
Wright, & Berchick (1989)
Weighted average
No. ofsessions
121215
12-1612
15"
Anxiety
1.502.041.18
1.622.13
1.69
1.68
No. ofpanic
attacks
1.052.201.00
0.511.21
0.80
0.98
Fear offear
—1.261.00
2.291.55
—
1.75
% Panicfree
949090
8375
100
85
' Average number of sessions.
phobic clients had a lower States of Mind ratio than normalsbefore treatment but an equivalent ratio after treatment. Al-though differences could be due to variety in the methodolo-gies used, the lengthier and more thorough Beck-Emery CBTprovided in the Michelson et al. study might account for theirsuperior results.
A different, but equally important, issue is the relationship ofcognitive factors to treatment outcome on panic and avoidance.An emerging body of evidence indicates that cognitive mea-sures of catastrophic thinking about panic predict treatmentoutcome on measures of panic and avoidance regardless oftreatment modality (Chambless & Gracely, 1988; Clark et al.,1991; Margraf & Schneider, 1991; Michelson et al, 1989), withgreater improvement on cognitive measures being strongly as-sociated with larger decrements in panic and avoidance orhigher levels of negative thinking at pretest predicting poorertreatment response. Indeed, cognitive measures are often thebest predictor of treatment outcome. Maintenance of treatmentgains may also be related to cognitive variables. Clark et al.found that, controlling for symptom severity at posttest, clients'clinical status at follow-up was predicted by their cognitive dis-tortions at posttest whether they had been treated with CBT,applied relaxation, or even pharmacotherapy. Thus, whateverthe method of treatment, clients who continued to report think-ing that physical symptoms of panic were signs of physical ill-ness or mishap fared poorly at final evaluation. Although theydo not prove causality, such data are consistent with the hypoth-esis that treatment efficacy is mediated by cognitive processes,whether or not the treatment is explicitly cognitive in nature.
Social Phobia
Because symptoms of social phobia overlap with those ofother anxiety disorders and avoidant personality disorder andcomorbidity is common, only clinical studies using explicit,standardized diagnostic criteria are included in our statisticalanalyses. Even so, there are considerable differences among the
10 selected trials in the number of subjects with specific versusgeneralized social phobias or with additional diagnoses, in-cluding avoidant personality disorder. For example, all the sub-jects included in the Stravynski, Marks, and Yule study (1982)met DSM-IH criteria for avoidant personality disorder,whereas Mattick and Peters (1988) and Heimberg et al. (1990)excluded subjects meeting these criteria. Such subtype differ-ences may affect treatment outcome (Chambless, 1989).
A variety of interventions have been shown to be effective forsocial phobia (for reviews, see Agras, 1990; Heimberg, 1989). Inthe studies reviewed here, cognitive interventions include anxi-ety management training (relaxation, distraction, and rationalself-talk) combined with in vivo exposure (Butler, Cullington,Munby, Amies, & Gelder, 1984), Heimberg's group CBT (Ge-lernter et al, 1991; Heimberg, Becker, Goldfinger, & Vermilyea,1985; Heimberg et al, 1990), SIT (Emmelkamp, Mersch, Vissia,& van der Helm, 1985; Jerremalm, Jansson, & 6st, 1986), andRET, alone (Emmelkamp et al, 1985; Mattick, Peters, &Clarke, 1989; Mersch, Emmelkamp, Bogels, & van der Sleen,1989), combined with exposure (Mattick & Peters, 1988; Mat-tick et al, 1989), or combined with social skills training (Stra-vynski etal, 1982).
Outcome measures included in our summary in Table 4 in-clude fear of negative evaluation (Fear of Negative EvaluationScale [FNES; Watson & Friend, 1969]), cognitive measures (e.g.,the Irrational Beliefs Test [IBT; Jones, 1969] and the SocialInteraction Self-Statement Test [SISST; Glass, Merluzzi, Biever,& Larsen, 1982]), and social phobia or anxiety measures (e.g.,the Social Phobia subscale of the Fear Questionnaire [Marks &Mathews, 1979] and the Social Avoidance and Distress Scale[Watson & Friend, 1969]).
Is CBT for Social Phobia Effective?
The consistently large pre-post effect sizes reflect substan-tial and significant within-group change. Comparisons withwaiting-list and supportive therapy control groups (Butler et al.

SPECIAL SECTION: COGNITIVE THERAPY OF ANXIETY DISORDERS 255
Table 4Cognitive-Behavioral Treatment for Social Phobia: Pre- to Posttreatment Effect Sizes
Study
Butler, Cullington,Munby, Amies, &Gelder(1984)
Gelernter et al. (1991)Heimberg, Becker,
Goldfinger, &Vermilyea(1985)
Heimberg et al. (1990)Jerremalm, Jansson, &
6st(1986)Mattick& Peters (1988)Mattick, Peters, &
Clarke (1989)
Stravynski, Marks, &Yule (1982)
Weighted average
Group
EXP/GAMTCBGT
CBGTCBGT
SITEXP + CBGT
CBGTCBGT + EXP
SST + RET
Socialphobia
0.621.15
1.210.73
0.940.71
0.911.79
1.53
1.00
Fear ofnegative
evaluation
0.56—
0.780.76
—0.74
0.571.59
1.00
0.85
Cognitivemeasure
——
0.69—
—0.47
1.041.21
0.55
0.67
Note. EXP = exposure; GAMT = group anxiety management training; CBGT = cognitive-behavioralgroup treatment; SIT = self-instructional training; RET = rational-emotive therapy; SST = self-statementtraining.
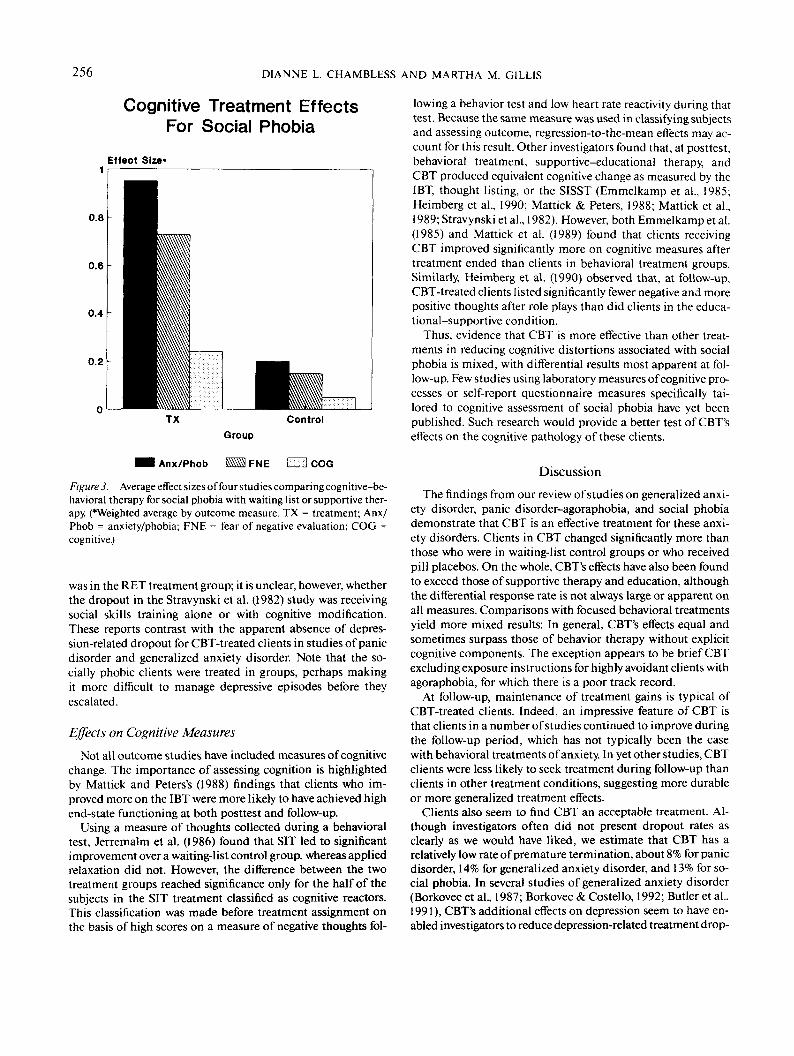
1984; Heimberg et al., 1985,1990; Jerremalm et al., 1986; Mat-tick et al., 1989) indicate that CBT-treated clients improvedsignificantly more than did control groups on some, if not all,measures (see Figure 3). Weighted average controlled effectsizes are 0.68 and 0.70 for social phobia and fear of negativeevaluation, respectively. Because fear of scrutiny and negativeevaluation by others distinguishes social phobia from relateddiagnoses and change on the FNES has been the best predictorof treatment outcome across a variety of treatments (Mattick &Peters, 1988; Mattick et al., 1989), results on fear of negativeevaluation bear special attention. CBT has led to consistentlylarge improvements on this variable (Table 4).
Do Treatment Effects Persist?
Overall, CBT treatment gains are maintained or have in-creased at 1-6 month follow-up. Indeed, Heimberg, Salzman,Holt, and Blendall (1991) found that CBT subjects were stillsignificantly improved 5 years after treatment. Mattick et al.(1989), in comparing CBT, alone or in combination with expo-sure, with exposure alone, found that both groups of subjectswho received CBT required significantly less subsequent treat-ment than the exposure-only group. Not only do CBT-treatedclients maintain their gains after treatment, in some studiesthey have continued to improve during the follow-up period(Gelernter et al., 1991; Mattick & Peters, 1988).
Is CBT for Social Phobia More Effective ThanBehavioral Treatment?
Although clearly effective with the socially phobic clinicalpopulation, CBT is not consistently superior to behavioral
treatments. Investigators comparing applied relaxation, expo-sure, or social skills training with CBT have typically found thetreatments to be equivalent (Emmelkamp et al., 1985; Gelernteret al., 1991; Jerremalm et al., 1986; Mattick et al., 1989; Merschet al., 1989; Stravynski et al., 1982). In only two of the eightcomparative trials did the effects of combined cognitive-beha-vioral treatment exceed those of exposure alone (Butler et al.,1984; Mattick & Peters, 1988), although one treatment or an-other may show superior effects on a given measure. Thus, thedetermination of which treatment is more effective may be af-fected by how outcome is assessed, as well as when, but wefound no clear association between assessment method anddifferential treatment effectiveness.
Effects on Depression
Although exclusionary criteria for subjects were not alwaysstated, it appears that about half the studies excluded subjectssuffering from current major depression. Comorbidity statis-tics for clients included in treatment samples were providedonly by Gelernter et al. (1991). In that study, 14% of the subjectshad a current comorbid diagnosis of dysthymia. Unpublisheddata from our own laboratory suggest that comorbidity may beas high as 30% for social phobia and depressive disorders. It istherefore an important finding that, in the studies reviewed,CBT for social phobia also had a positive impact on depression,with a large controlled effect size of 0.91. These effects wereconsistently, but not significantly, greater than the comparisongroup effects.
Conversely, it is troubling that Mersch et al. (1989) and Stra-vynski et al. (1982) each reported one treatment dropout result-ing from increased suicidality. The Mersch et al. (1989) dropout
256 DIANNE L. CHAMBLESS AND MARTHA M. GILLIS
Cognitive Treatment EffectsFor Social Phobia
Effect Size*
ControlGroup
I Anx/Phob FNE El COG
Figure 3. Average effect sizes of four studies comparing cognitive-be-havioral therapy for social phobia with waiting list or supportive ther-apy. fWeighted average by outcome measure. TX = treatment; Anx/Phob = anxiety/phobia; FNE = fear of negative evaluation; COG =cognitive.)
was in the RET treatment group; it is unclear, however, whetherthe dropout in the Stravynski et al. (1982) study was receivingsocial skills training alone or with cognitive modification.These reports contrast with the apparent absence of depres-sion-related dropout for CBT-treated clients in studies of panicdisorder and generalized anxiety disorder. Note that the so-cially phobic clients were treated in groups, perhaps makingit more difficult to manage depressive episodes before theyescalated.
Effects on Cognitive Measures
Not all outcome studies have included measures of cognitivechange. The importance of assessing cognition is highlightedby Mattick and Peters's (1988) findings that clients who im-proved more on the IBT were more likely to have achieved highend-state functioning at both posttest and follow-up.
Using a measure of thoughts collected during a behavioraltest, Jerremalm et al. (1986) found that SIT led to significantimprovement over a waiting-list control group, whereas appliedrelaxation did not. However, the difference between the twotreatment groups reached significance only for the half of thesubjects in the SIT treatment classified as cognitive reactors.This classification was made before treatment assignment onthe basis of high scores on a measure of negative thoughts fol-
lowing a behavior test and low heart rate reactivity during thattest. Because the same measure was used in classifying subjectsand assessing outcome, regression-to-the-mean effects may ac-count for this result. Other investigators found that, at posttest,behavioral treatment, supportive-educational therapy, andCBT produced equivalent cognitive change as measured by theIBT, thought listing, or the SISST (Emmelkamp et al., 1985;Heimberg et al., 1990; Mattick & Peters, 1988; Mattick et al.,1989; Stravynski etal., 1982). However, both Emmelkamp etal.(1985) and Mattick et al. (1989) found that clients receivingCBT improved significantly more on cognitive measures aftertreatment ended than clients in behavioral treatment groups.Similarly, Heimberg et al. (1990) observed that, at follow-up,CBT-treated clients listed significantly fewer negative and morepositive thoughts after role plays than did clients in the educa-tional-supportive condition.
Thus, evidence that CBT is more effective than other treat-ments in reducing cognitive distortions associated with socialphobia is mixed, with differential results most apparent at fol-low-up. Few studies using laboratory measures of cognitive pro-cesses or self-report questionnaire measures specifically tai-lored to cognitive assessment of social phobia have yet beenpublished. Such research would provide a better test of CBT'seffects on the cognitive pathology of these clients.
Discussion
The findings from our review of studies on generalized anxi-ety disorder, panic disorder-agoraphobia, and social phobiademonstrate that CBT is an effective treatment for these anxi-ety disorders. Clients in CBT changed significantly more thanthose who were in waiting-list control groups or who receivedpill placebos. On the whole, CBT's effects have also been foundto exceed those of supportive therapy and education, althoughthe differential response rate is not always large or apparent onall measures. Comparisons with focused behavioral treatmentsyield more mixed results: In general, CBT's effects equal andsometimes surpass those of behavior therapy without explicitcognitive components. The exception appears to be brief CBTexcluding exposure instructions for highly avoidant clients withagoraphobia, for which there is a poor track record.
At follow-up, maintenance of treatment gains is typical ofCBT-treated clients. Indeed, an impressive feature of CBT isthat clients in a number of studies continued to improve duringthe follow-up period, which has not typically been the casewith behavioral treatments of anxiety. In yet other studies, CBTclients were less likely to seek treatment during follow-up thanclients in other treatment conditions, suggesting more durableor more generalized treatment effects.
Clients also seem to find CBT an acceptable treatment. Al-though investigators often did not present dropout rates asclearly as we would have liked, we estimate that CBT has arelatively low rate of premature termination, about 8% for panicdisorder, 14% for generalized anxiety disorder, and 13% for so-cial phobia. In several studies of generalized anxiety disorder(Borkovec et al., 1987; Borkovec & Costello, 1992; Butler et al.,1991), CBT's additional effects on depression seem to have en-abled investigators to reduce depression-related treatment drop-

SPECIAL SECTION: COGNITIVE THERAPY OF ANXIETY DISORDERS 257
out. Reporting on treatment of panic disorder, Barlow et al.(1989) noted a lower dropout rate for CBT than for behaviortherapy alone, although it is not known whether the increaseddropout rate with relaxation training was related to depression.On the other hand, in the literature on group CBT of socialphobia there have been one or two reports of dropout asso-ciated with increased suicidality. We urge researchers to reportcomorbidity and dropout data carefully to allow more defini-tive conclusions to be drawn.
Although investigators have shown that clients change inCBT, they have inadequately assessed or reported the clinicalsignificance of that change. When indices of clinically signifi-cant change are reported, comparisons across studies are madedifficult by variable and often arbitrary criteria. Estimates ofclinically significant change or high end-state functioningrange from 7%-75% for social phobia, 46%-86% for panic dis-order, and 32%-73% for generalized anxiety disorder. Thesedata suggest that even more powerful treatment interventionsare needed. Moreover, end-state functioning criteria basedsolely on compilations of focused measures for the disordermay obscure remaining psychopathology. For example, on in-terviewer-rated global assessment of severity, Michelson et al.(1989) found that only 24% of the CBT clients were rated ascompletely recovered after treatment (although this figure hadrisen to 47% at 3-month follow-up), whereas 86% were rated ashaving achieved high end-state functioning on the major out-come measures. Thus, CBT may be effective, but, as practicedin research trials, it is no panacea.
In the search for more effective treatments, investigators haveturned to combinations of treatment components. Given themultiple ways in which anxiety is manifest (physiologicalarousal, maladaptive cognition, behavioral disturbance oravoidance, and subjective distress), the idea that using differenttreatments to attack each aspect of the problem would be maxi-mally effective has great intuitive appeal. Unfortunately, ourreview of the results of studies on combination treatments indi-cates that this is not uniformly true. The incremental efficacyof combination treatments seems to differ according to diagno-sis and the particular outcome measures used.
There seem to be at least two possible limitations to the util-ity of combination treatments. First, given a fixed number ofsessions, as is typical in research or managed care settings,introducing a variety of treatment approaches may preclude theclient from becoming the master of any of them. Second, ajumble of treatments may prevent the client from having a clearsense of the rationale and direction of the treatment, which isproblematical because the rationale itself is an important thera-peutic component (Butler, Gelder, Hibbert, Cullington, &Klimes, 1987). Whether combinations could be used more ef-fectively in lengthier treatments is yet to be explored. If so, itmay be necessary to develop strategies for determining the bestsequence or integration of treatment elements. Extrapolatingfrom the present set of studies, we suggest that vigorous, system-atic exposure instructions in addition to cognitive modificationtechniques will be required for clients who consistently avoidphobic situations.
We know that CBT works, but does it work in the way itshould? Theoretically, CBT should lead to improvement and
maintenance of treatment gains via alteration of maladaptivecognitions. Relatively few studies have addressed this issue, andthe measures have almost exclusively been limited to self-reportof thoughts and attribution. The results indicate that CBT doeslead to cognitive change and that cognitive change is related toreduction of anxious symptoms and to the durability of treat-ment gains at follow-up. In fact, cognitive measures have provedto be the best predictor of outcome in several investigations.Nevertheless, CBT is not the only road to cognitive modifica-tion. The pattern of results across studies suggests that success-ful treatment will be accompanied by change on cognitive mea-sures and that cognitive measures predict outcome with a vari-ety of treatment approaches, including pharmacotherapy.
There are a number of possible explanations for such find-ings; these have been described by Hollon, DeRubeis, andEvans (1987) in the context of the CBT depression literature. Atleast three explanations seem pertinent here: (a) cognitivechange represents a common mechanism for change withvarious treatments (Bandura, Adams, & Beyer, 1977) and isnecessary for durable benefits; (b) cognition, anxiety, and avoid-ance are linked so that changing any one aspect of the systemleads to changes in other components; or (c) cognitive changecovaries with change in anxiety and has no special explanatoryproperties. The latter explanation becomes less likely in theface of studies such as that by Clark et al. (1991), who controlledfor posttreatment severity in anxiety symptoms when demon-strating that cognitive measures predicted outcome on anxietysymptoms at follow-up.
More research using statistical approaches allowing approxi-mation of causal explanations is required (see Baron & Kenny,1986). Greater attention to cognitive assessment procedures isalso necessary (for a review, see Arnkoff & Glass, 1989). Mea-sures often used to assess cognitions in anxiety disorders re-search, such as the IBT (see T. W Smith & Zurawski, 1983) andthe FNES, may not discriminate adequately between anxietyand cognitions. In addition, studies assessing change with labo-ratory rather than self-report measures are highly desirable. Ontransparent questionnaires, CBT-treated clients might feelgreater pressure to report increased rational thinking aftertreatment than clients in noncognitive therapies. Moreover, notall important aspects of cognitive psychopathology (e.g., sche-mata) may be accessible to self-report.
Heterogeneous approaches to cognitive modification weretaken in the studies we reviewed, yet few studies have providedcomparisons among the types of cognitive treatments.Currently, the most common cognitive treatment used is someform of Beck-Emery (1985) CBT. Michelson and Marchione(1991) have suggested that Beck-Emery CBT may prove to be amore powerful approach for anxiety than other cognitive ap-proaches (e.g., SIT) because it is designed to change not only thecontent of clients' thoughts but also the process and structure ofcognition. Indeed, CBT seems to add to the effectiveness ofexposure for agoraphobia when RET and SIT have not. How-ever, a variety of cognitive approaches have proved effective forsocial phobia, including SIT and RET. Hence, whether one cog-nitive treatment is better than another remains an open ques-tion, although the documentation of the efficacy of Beck-Emery CBT is more extensive at present. The development of

258 DIANNE L. CHAMBLESS AND MARTHA M. GILLIS
more sophisticated laboratory measurement of cognitive sche-mata for research on psychopathology of anxiety disordersmakes possible a test of whether more explicitly metacognitivetherapies (see Hollon & Kriss, 1984) have stronger effects ondeeper structures than therapies that rely on distraction or self-statement training. We encourage anxiety researchers to in-clude such tests in their trials on treatment outcome.
In a final point, we note the dearth of studies comparingCBT with psychodynamic therapies. Both psychotherapies relyon introspection and client-therapist verbal interaction fortheir effects, although the type of insight sought differs. Withthe current emphasis in CBT on modification of self-schemata,CBT has moved closer to psychodynamic therapy in its goals.These similarities appear to make CBT more acceptable to psy-chodynamically oriented practitioners than behavior therapy.Given the continued popularity of psychodynamic approacheswith American clinical psychologists (Norcross & Prochaska,1982), controlled comparisons of process and outcome of theseapproaches would be fruitful.
References
Agras, W S. (1990). Treatment of social phobias. Journal of ClinicalPsychiatry, 51, 52-58.
American Psychiatric Association. (1980). Diagnostic and statisticalmanual of menial disorders (3rd ed.). Washington, DC: Author.
American Psychiatric Association. (1987). Diagnostic and statisticalmanual of mental disorders (Rev. 3rded.). Washington, DC: Author.
Arnkoff, D. B., & Glass, C. R. (1989). Cognitive assessment in socialanxiety and social phobia. Clinical Psychology Review, 9, 61 -74.
Bandura, A., Adams, N. E., & Beyer, J. (1977). Cognitive processesmediating behavioral change. Journal of Personality and Social Psy-chology, 35, 125-139.
Barlow, D. H, Cohen, A. S., Waddell, M. T., Vermilyea, B. B., Klosko,J. S., Blanchard, E. B., & DiNardo, P. A. (1984). Panic and general-ized anxiety disorders: Nature and treatment. Behavior Therapy, 15,431-449.
Barlow, D. H., Craske, M. G., Cerny, J. A., & Klosko, J. (1989). Behav-ioral treatment of panic disorder. Behavior Therapy, 20, 261-282.
Baron, R. M., & Kenny, D. A. (1986). The moderator-mediator variabledistinction in social psychological research: Conceptual, strategic,and statistical considerations. Journal of Personality and Social Psy-chology, 51, 1173-1182.
Beck, A. T, & Emery, G. (1985). Anxiety disorders and phobias: Acognitive perspective. New \brk: Basic Books.
Beck, A. T, Laude, R., & Bohnert, M. (1974). Ideational components ofanxiety neurosis. Archives of General Psychiatry, 31, 319-325.
Beck, A. T, Sokol, L., Clark, D. A., Berchick, B., & Wright, F. (1992). Acrossover study of focused cognitive therapy for panic disorder.American Journal of Psychiatry, 149, 778-783.
Beck, A. T, & Steer, R. A. (1990). Manual for the Beck Anxiety Inven-tory. New York: Psychological Corporation.
Blowers, C., Cobb, J., & Mathews, A. (1987). Generalized anxiety: Acontrolled treatment study. Behaviour Research and Therapy, 25,493-502.
Borkovec, T. D., & Costello, E. (1992). Efficacy of applied relaxation andcognitive behavioral therapy in the treatment of generalized anxietydisorder. Manuscript submitted for publication.
Borkovec, T. D, & Inz, J. (1990). The nature of worry in generalizedanxiety disorder: A predominance of thought activity. Behaviour Re-search and Therapy, 28, 153-158.
Borkovec, T. D, & Mathews, A. M. (1988). Treatment of nonphobicanxiety disorders: A comparison of nondirective, cognitive, and cop-ing desensitization therapy. Journal of Consulting and Clinical Psy-chology, 56, 877-884.
Borkovec, T. D, Mathews, A. M., Chambers, A., Ebrahimi, S., Lytle, R.,& Nelson, R. (1987). The effects of relaxation training with cognitiveor nondirective therapy and the role of relaxation-induced anxiety inthe treatment of generalized anxiety. Journal of Consulting and Clini-cal Psychology, 55, 883-888.
Borkovec, T. D, Shadick, R., & Hopkins, M. (1991). The nature ofnormal and pathological worry. In R. Rapee & D. H. Barlow (Eds.).Chronic anxiety and generalized anxiety disorders (pp. 29-51). NewYork: Guilford Press.
Butler, G., Cullington, C, Hibbert, G., Klimes, I., & Gelder, M. (1987).Anxiety management for persistent generalised anxiety. BritishJournal of Psychiatry, 151. 535-542.
Butler, G., Cullington, A., Munby, M., Amies, P., & Gelder, M. (1984).Exposure and anxiety management in the treatment of social pho-bia. Journal oj'Consulting and Clinical Psychology, 52, 642-650.
Butler, G, Fennell, M., Robson, P., & Gelder, M. (1991). Comparisonof behavior therapy and cognitive behavior therapy in the treatmentof generalized anxiety disorder. Journal of Consulting and ClinicalPsychology, 59, 167-175.
Butler, G., Gelder, M., Hibbert, G., Cullington, A., & Klimes, I. (1987).Anxiety management: Developing effective strategies. BehaviourResearch and Therapy, 25. 517-522.
Chambless, D. L. (1988). Cognitive mechanisms in panic disorder. In S.Rachman & J. D. Maser (Eds.), Panic: Psychological perspectives (pp.205-218). Hillsdale, NJ: Erlbaum.
Chambless, D. L. (1989, November). Familial and social factors in sim-ple and social phobias and their treatment. Paper presented at theNational Institute of Mental Health Workshop on Specific Phobias,Bethesda, MD.
Chambless, D. L., Caputo, G. C., Bright, P., & Gallagher, R. (1984).Assessment of fear of fear in agoraphobics: The Body SensationsQuestionnaire and the Agoraphobic Cognitions Questionnaire.Journal of Consulting and Clinical Psychology, 52, 1090-1097.
Chambless, D. L., Goldstein, A. J., Gallagher, R., & Bright, P. (1986).Integrating behavior therapy and psychotherapy in the treatment ofagoraphobia. Psychotherapy, 23, 150-159.
Chambless, D. L., & Gracely, E. J. (1988). Prediction ofoutcomefollow-ing in vivo exposure treatment of agoraphobia. In I. Hand & H.-UWittchen (Eds.), Panic and phobias 2 (pp. 209-220). Berlin:Springer-Verlag.
Chambless, D. L., & Gracely, E. J. (1989). Fear of fear and the anxietydisorders. Cognitive Therapy and Research, 13, 9-20.
Clark, D. M., & Salkovskis, P. M. (in press). Cognitive therapy with panicand hypochondriasis. Elmsford, NY: Pergamon Press.
Clark, D. M., Salkovskis, P. M., Hackman, A., Middleton, H., Anasta-siades, P., & Gelder, M. (1991, November). A comparison of cognitivetherapy, applied relaxation, and imipramine in the treatment of panicdisorder. Paper presented at the meeting of the Association for Ad-vancement of Behavior Therapy, New York.
Clum, G. A. (1989). Psychological interventions vs. drugs in the treat-ment of panic. Behavior Therapy, 20, 429-457.
Craske, M. G., Brown, T. A., & Barlow, D. H. (1991). Behavioral treat-ment of panic disorder: A two-year follow-up. Behavior Therapy, 22,289-304.
de Ruiter, C., Rijken, H., Garssen, B., van Schaik, A., & Kraaimaat, F.(1989). Comorbidity among the anxiety disorders. Journal of AnxietyDisorders, 3, 57-68.
Dobson, K. S. (1989). A meta-analysis of the efficacy of cognitive ther-apy for depression. Journal of Consulting and Clinical Psychology, 57,414-419.
SPECIAL SECTION: COGNITIVE THERAPY OF ANXIETY DISORDERS 259
Ellis, A. (1962). Reason and emotion in psychotherapy. New York: LyleStuart.
Emmelkamp, P. M. G., Brilman, E., Kuiper, H., & Mersch, P. P. (1986).The treatment of agoraphobia: A comparison of self-instructionaltraining, rational emotive therapy, and exposure in vivo. BehaviorModification, 10, 37-53.
Emmelkamp, P. M. G., Kuipers, A., & Eggeraat, J. (1978). Cognitivemodification versus prolonged exposure in vivo: A comparison withagoraphobics. Behaviour Research and Therapy, 16, 33-41.
Emmelkamp, P. M. G., & Mersch, P. P. (1982). Cognition and exposurein vivo in the treatment of agoraphobia: Short-term and delayedeffects. Cognitive Therapy and Research, 6, 77-90.
Emmelkamp, P. M. G., Mersch, P. P., Vissia, E., & van der Helm, M.(1985). Social phobia: A comparative evaluation of cognitive andbehavioral interventions. Behaviour Research and Therapy, 23, 365-369.
Gelernter, C. S., Uhde, T. W, Cimbolic, P., Arnkoff, D. B., Vittone, B. J.,Tancer, M. E., & Bartko, J. J. (1991). Cognitive-behavioral and phar-macological treatments for social phobia: A preliminary study. Ar-chives of General Psychiatry, 48, 938-945.
Glass, C. R., Merluzzi, T. V, Biever, J. L., & Larsen, K. H. (1982).Cognitive assessment of social anxiety: Development and validationof a self-statement questionnaire. CognitiveTherapy and Research, 6,37-55.
Goldstein, A. J., & Chambless, D. L. (1978). A reanalysis of agorapho-bia. Behavior Therapy, 9, 47-59.
Greenberg, R. L. (1989). Panic disorder and agoraphobia. In J. Scott,J. M. G. Williams, & A. T. Beck (Eds.), Cognitive therapy in clinicalpractice: An illustrative casebook (pp. 25-49). London: Routledge &Kegan Paul.
Hamilton, M. (1959). The assessment of anxiety states by rating. Brit-ish Journal of Medical Psychology, 32, 50-55.
Heimberg, R. G. (1989). Cognitive and behavioral treatments for socialphobia: A critical analysis. Clinical Psychology Review, 9, 107-128.
Heimberg, R. G, Becker, R. E., Goldfinger, K., & Vermilyea, J. A.(1985). Treatment of social phobia by exposure, cognitive restructur-ing, and homework assignments. Journal of Nervous and Mental Dis-ease, 173, 236-245.
Heimberg, R. G., Dodge, C. S., Hope, D. A., Kennedy, C. R., Zollo, L. J.,& Becker, R. E. (1990). Cognitive behavioral group treatment forsocial phobia: Comparison with a credible placebo control. Cogni-tive Therapy and Research, 14, 1-23.
Heimberg, R. G, Salzman, D. G., Holt, C. S., & Blendall, K. (1991).Cognitive behavioral group treatment for social phobia: Effectivenessat five-year follow-up. Manuscript submitted for publication.
Hollon, S. D, DeRubeis, R. J., & Evans, M. D. (1987). Causal mediationof change in treatment for depression: Discriminating between non-specificity and noncausality. Psychological Bulletin, 102,139-149.
Hollon, S. D, & Kriss, M. R. (1984). Cognitive factors in clinical re-search and practice. Clinical Psychology Review, 4, 35-76.
Hope, D. A., Rapee, R. M., Heimberg, R. G, & Dombeck, M. J. (1990).Representations of the self in social phobia: Vulnerability to socialthreat. Cognitive Therapy and Research, 14, 177-189.
Jansson, L., & 6st, L.-G. (1982). Behavioral treatments for agorapho-bia: An evaluative review. Clinical Psychology Review, 2, 311 -336.
Jerremalm, A., Jansson, L., & 6st, L.-G. (1986). Cognitive and physio-logical reactivity and the effects of different behavioral methods inthe treatment of social phobia. Behaviour Research and Therapy, 24,171-180.
Jones, R. G. (1969). A factored measure of Ellis' irrational belief sys-tem, with personality and adjustment correlates (Doctoral disserta-tion, Texas Technological College, 1968). Dissertation Abstracts In-ternational, 29, 4379B-4380B. (University Microfilms No. 69-6443)
Klosko, J. S., Barlow, D. H., Tassinari, R., & Cerny, J. A. (1990). Acomparison of alprazolam and behavior therapy in treatment ofpanic disorder. Journal of Consulting and Clinical Psychology, 58,77-84.
MacLeod, C., Mathews, A., & Tata, P. (1986). Attentional bias in emo-tional disorders. Journal of Abnormal Psychology, 95,15-20.
Margraf, J., & Schneider, S. (1991, November). Outcome and active in-gredients of cognitive-behavioral treatments for panic disorder. Paperpresented at the meeting of the Association for Advancement ofBehavior Therapy, New York.
Marks, I. M., & Mathews, A. M. (1979). Brief standard self-rating forphobic patients. Behaviour Research and Therapy, 17, 263-267.
Mattick, R. P., & Peters, L. (1988). Treatment of severe social phobia:Effects of guided exposure with and without cognitive restructuring.Journal of Consulting and Clinical Psychology, 56, 251-260.
Mattick, R. P., Peters, L., & Clarke, J. C. (1989). Exposure and cognitiverestructuring for social phobia: A controlled study. Behavior Ther-apy, 20, 3-23.
Meichenbaum, D. (1975). Self-instructional methods. In F. H. Kanfer& A. P. Goldstein (Eds.), Helping people change (pp. 357-391). Elms-ford, NY: Pergamon Press.
Mersch, P. P. A., Emmelkamp, P. M. G., Bogels, S. M., & van der Sleen,J. (1989). Social phobia: Individual response patterns and the effectsof behavioral and cognitive interventions. Behaviour Research andTherapy, 27,421-434.
Meyer, T. J., Miller, M. L., Metzger, R. L, & Borkovec, T. D. (1990).Development and validation of the Penn State Worry Question-naire. Behaviour Research and Therapy, 28, 487-495.
Michelson, L. K., & Marchione, K. (1991). Behavioral, cognitive, andpharmacological treatments of panic disorder with agoraphobia:Critique and synthesis. Journal of Consulting and Clinical Psychol-ogy, 39, 100-114.
Michelson, L., Marchione, K., & Greenwald, M. (1989, November).Cognitive-behavioral treatments of agoraphobia. Paper presented atthe meeting of the Association for Advancement of Behavior Ther-apy, Washington, DC.
Michelson, L., Marchione, K., Greenwald, M., Glanz, L., Testa, S., &Marchione, N. (1990). Panic disorder: Cognitive-behavioral treat-ment. Behaviour Research and Therapy, 28, 141-152.
Michelson, L., Mavissakalian, M., & Marchione, K. (1988). Cognitive,behavioral, and psychophysiological treatments of agoraphobia: Acomparative outcome investigation. Behavior Therapy, 19, 97-120.
Michelson, L., Schwartz, R. M., & Marchione, K. E. (1992). States-of-Mind model: Cognitive balance in the treatment of agoraphobia—II. Advances in Behaviour Research andTherapy, 13, 193-213.
Newman, C. F, Beck, J. S., Beck, A. T, & Tran, G. Q. (1990, November).Efficacy of cognitive therapy in reducing panic attacks and medica-tion. Paper presented at the meeting of the Association for Advance-ment of Behavior Therapy, San Francisco.
Norcross, J. C., & Prochaska, J. O. (1982). A national survey of clinicalpsychologists: Affiliations and orientations. The Clinical Psycholo-gist, J5(3), 1, 4-8.
6st, L.-G, & Westling, B. E. (1991). Treatment of panic disorder byapplied relaxation vs. cognitive therapy. Manuscript in preparation.
Ost, L.-G., Westling, B. E., & Hellstrom, K. (1991). Applied relaxation,exposure in vivo, and cognitive methods in the treatment of agorapho-bia. Manuscript submitted for publication.
Power, K. G, Jerrom, D. W A., Simpson, R. J., Mitchell, M! J., &Swanson, V (1989). A controlled comparison of cognitive-behaviourtherapy, diazepam and placebo in the management of generalizedanxiety. Behavioural Psychotherapy, 17, 1-14.
260 DIANNE L. CHAMBLESS AND MARTHA M. GILLIS
Power, K. G., Simpson, R. J., Swanson, V, Wallace, L. A., Feistner,A. T. C, & Sharp, D. (1990). A controlled comparison of cognitive-behaviour therapy, diazepam, and placebo, alone and in combina-tion, for the treatment of generalised anxiety disorder. Journal ofAnxiety Disorders, 4, 267-292.
Renneberg, B., Chambless, D. L., & Gracely, E. J. (1992). Prevalence ofSCID-diagnosed personality disorders in agoraphobic outpatients.Journal of Anxiety Disorders, 6, 111-118.
Smith, M. L., & Glass, G. V (1977). Meta-analysis of psychotherapyoutcome studies. American Psychologist, 32, 752-760.
Smith, T. W, & Zurawski, R. M. (1983). Assessment of irrational be-liefs: The question of discriminant validity. Journal of Clinical Psy-chology, 39, 976-979.
Sokol, L., Beck, A. T, Greenberg, R. L., Wright, F. D., & Berchick, R. J.(1989). Cognitive therapy of panic disorder: A nonpharmacologicalalternative. Journal of Nervous and Mental Disease, 177, 711-716.
Stravynski, A., Marks, I., & Yule, W (1982). Social skills problems inneurotic outpatients. Archives of General Psychiatry, 39, 1378-1384.
Trull, T. J., Nietzel, M. T, & Main, A. (1988). The use of meta-analysisto assess the clinical significance of behavior therapy for agorapho-bia. Behavior Therapy, 19, 527-538.
Watson, D.,& Friend, R. (1969). Measurementofsocial-evaluativeanxi-ety. Journal of Consulting and Clinical Psychology, 33, 448-457.
Williams, S. L., & Rappoport, A. (1983). Cognitive treatment in thenatural environment for agoraphobics. Behavior Therapy, 14, 299-313.
Zung, W W K. (1971). A rating instrument for anxiety disorders. Psy-chosomatics, 12, 371-379.
Received January 31,1992Revision received June 25,1992
Accepted July 27,1992 •
CALLFOR
BOOKPROPOSALS
ON
CLINICALTOPICS
The APA Book Program is seeking proposals for practice-oriented volumeson important clinical issues. Books in this series should be stronglyinformed by theory and research and structured according to the establishedmodel:
• Presentation of the problem, including definition and discussionof incidence and prevalence
• Systematic review of theoretical issues
• Summary of empirical research
• Integration of theoretical review, research synthesis, andpractice issues
• Implications for interventions and practice
Please send your proposal (including topic outline andtable of contents) and a current CV to APA Books,Acquisitions and Development, 750 First Street, NE,Washington, DC 20002-4242. FAX: 202-336-5630.