cognitive remediation work in anorexia nervosa - forside · cognitive remediation: a promising tool...
TRANSCRIPT
Cognitive Remediation Work in Anorexia Nervosa
Dr. Kate Tchanturia
Consultant Clinical Psychologist
Maudsley NHS/King’s College London

Map of the talk and workshop
• Research background and rational for CRT
• Why CRT for ED
• What is current evidence for CRT
In the workshop I will demonstrate HOW
Practical elements for assessments / exercises
Plans for the future research/clinical bridge

WHY CRT for ED
• Poor treatment engagement – drop out in AN clinical studies
• Findings in Cognitive characteristics for ED
• Successful use of CRT in other areas of MH

Level "A" Level "B” Level "C"
AN 0 1 49
BN 1 7 10
BED 2 5 2
EDNOS 0 0 1
National Institute of Clinical Excellence (2004) in UK
www. NICE. org
has concluded no grade A (reflecting strong empirical data)
recommendation for treatment for AN and
49 C (expert opinion in absence of strong data).
Further research in effective treatments was encouraged.
9 RCT-s for AN; drop out rates very
high (between 30-65%)

Many patients say in different words:
I think it is going to be difficult to think my way out of my problem because I think the problem is the way that I think
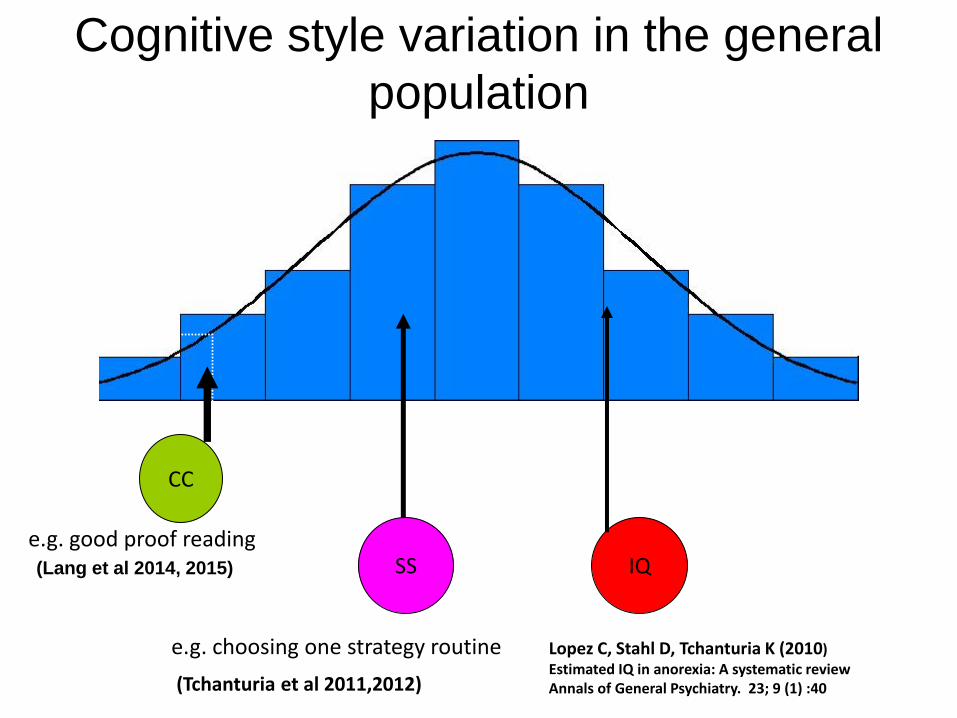
Cognitive style variation in the general
population
e.g. good proof reading
e.g. choosing one strategy routine
(Tchanturia et al 2011,2012)
IQ SS
CC
Lopez C, Stahl D, Tchanturia K (2010) Estimated IQ in anorexia: A systematic review Annals of General Psychiatry. 23; 9 (1) :40
(Lang et al 2014, 2015)

Research in cognitive characteristics
• Cognitive inflexibility in Anorexia Nervosa robustly replicated
(review Westwood et al 2016, Tchanturia et al 2012)
• Poor gestalt processing
(review Lang et al 2016, 2014)
• Perfectionism is strongly present in AN
(review Lloyd et al 2014)
• IQ is higher than average (Lopez et al 2010)

Excessive attention to detail
• Normal tendency to examine context of information, link together items of information to understand the “broad picture” (U. Frith 1991)
• Individuals with autistic spectrum disorders have weak central coherence and are not able to see “wood for trees” (F. Happe 1996)

Attention to detail:
Embedded Figures Test

Embedded Figures Test
0
2
4
6
8
10
12
14
16
A N HC
Tim
e t
ak
en
med
ian
(m
ean
)
0
0 .2
0 .4
0 .6
0 .8
1
1 .2
1 .4
A N HC
N t
imeo
ut
err
ors
(m
ean
)
p < 0.01 p < 0.001
N = 42 (AN) and 42 (HC) –pilot
Lopez, C., et al (2008); IJED, 41(2), 143-152, Lang et al 2016 Plos one.

CC studies in adults ROCFT (N=252)
Lang K, Tchanturia K (2014) A Systematic Review of Central Coherence in Young People with Anorexia Nervosa
NOTE: Weights are from random effects analysis
.
.
.
Overall (I-squared = 0.0%, p = 0.871)
ID
Lopez et.al (2008)
Danner et al. (2012)
Subtotal (I-squared = 0.0%, p = 0.850)
Harrison et al. (2011)
Tenconi et al. (2010)
Lopez et al. (2009)
Roberts et al. (2012)
Harrison et al. (2011)
Roberts et al. (2012)
Subtotal (I-squared = 0.0%, p = 0.514)
Harrison et al. (2011)
Lopez et.al (2008)
AN
ED Rec
Tenconi et al. (2010)
Favaro et al. (2012)
BN
Subtotal (I-squared = 0.0%, p = 0.725)
Roberts et al. (2012)
Danner et al. (2012)
Study
-0.57 (-0.70, -0.43)
ES (95% CI)
-0.79 (-1.42, -0.17)
-0.80 (-1.72, 0.12)
-0.56 (-0.76, -0.35)
-0.69 (-1.19, -0.19)
-0.53 (-0.89, -0.17)
-0.53 (-1.14, 0.08)
-0.52 (-0.96, -0.08)
-0.54 (-1.00, -0.07)
-0.09 (-0.60, 0.41)
-0.49 (-0.71, -0.26)
-0.84 (-1.32, -0.37)
-0.53 (-1.14, 0.08)
-0.40 (-0.76, -0.03)
-0.74 (-1.28, -0.19)
-0.74 (-1.04, -0.43)
-0.75 (-1.28, -0.23)
-0.71 (-1.60, 0.17)
100.00
Weight
4.73
2.17
44.66
7.28
14.07
4.89
9.45
8.49
7.17
35.75
8.13
4.89
13.72
6.10
19.59
6.57
2.35
%
-0.57 (-0.70, -0.43)
ES (95% CI)
-0.79 (-1.42, -0.17)
-0.80 (-1.72, 0.12)
-0.56 (-0.76, -0.35)
-0.69 (-1.19, -0.19)
-0.53 (-0.89, -0.17)
-0.53 (-1.14, 0.08)
-0.52 (-0.96, -0.08)
-0.54 (-1.00, -0.07)
-0.09 (-0.60, 0.41)
-0.49 (-0.71, -0.26)
-0.84 (-1.32, -0.37)
-0.53 (-1.14, 0.08)
-0.40 (-0.76, -0.03)
-0.74 (-1.28, -0.19)
-0.74 (-1.04, -0.43)
-0.75 (-1.28, -0.23)
-0.71 (-1.60, 0.17)
100.00
Weight
4.73
2.17
44.66
7.28
14.07
4.89
9.45
8.49
7.17
35.75
8.13
4.89
13.72
6.10
19.59
6.57
2.35
%
0-2 -1.5 -1 -.5 0 .5 1
Forest plot of Rey Osterrieth Complex Figures Test (ROCFT)
Studies not included in meta-analysis: • Lindner et al., 2012 – did not report CCI • Goddard et al., 2013 – Only included males, but found that ED males had
weaker central coherence than HC males (d=-0.5, p=0.009). • Kanakam et al., 2012- Included mixed AN & ANREC: reported no differences
between ED twins and HC (d=0.1, p=0.05).

Effect size is similar in CC in children Lang et al 2015, 2016 Plos one
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
Lopez etal., 2008
Tenconiet al.,2010
Harrisonet al.,2011
Robertset al.,2012
Danner etal., 2012
Favaro etal., et al.,
2012
Lang etal., 2015
Adult Child
N= (AN -42; HC =42) in children

Wisconsin Card Sort
Task (WCST)
Brixton Task
Trail Making Task (TMT)
Set-shifting
measures

TMT - Alphanumeric
A
2
3
C B
1
The task (Part B) requires rapid and sustained alternation between two
sets. This alternation is thought to require executive control,
specifically flexibility.

Set Shifting WCST
• Measures abstract reasoning and ability to shift strategies efficiently.
Tchanturia et al (2012, 2011) Plos one

WCST in AN and ASD
No significant difference in perseverative errors between AN
and ASD participant groups, suggesting similar set-shifting profiles
Westwood et al. (2016) Psychological Medicine

Weight gain alone does not change the flexibility of thinking
Me an ZCBSUMT
Me an ZCBP
Me an ZBRIXTON
Me an ZILLUSIO
Me an ZDYAD1
Me an ZDYAD2
Me an ZFAS
Me an ZPICTURE
.50.0-.5-1.0-1.5-2.0-2.5
group
anorexia
anorexics after we ig
ANWR
BMI=18.4
ANUW
BMI=13.3
Tchanturia et al., (2004) Journal of Psychiatric Research, Vol 38, 545-552.

Research and clinic - NEUROPSYCHOLOGY
RESEARCH
Sensitive experimental paradigms
What happens
Before and after
psychological
treatment?
- Information for the treatment
- What do we treat?
INFORM THE TREATMENT
MEASURE THE OUTCOMES

Cognitive Remediation Therapy CRT
Is a psychological intervention that:
• Consists of mental exercises aimed at improving cognitive strategies.
• Encourages thinking about thinking (Reflection).
• Helps to explore new thinking strategies in everyday life.
Target for CBT reduction in symptoms, CRT thinking skills themselves.

Is there evidence that
executive impairments can be
effectively treated?
What patients think How patients think

Cognitive remediation: a promising tool for the treatment of schizophrenia
(Demily, C & Frank, N. 2008)
• Integrated Psychological Treatment (IPT) - Brenner & Volker (1992, 2005)
• Cognitive Remediation Therapy (CRT) – Delahunty & Morice 1993; Wykes, Reeder (2000, 2007)
• Neuropsychological Educational Approach to Rehabilitation (NEAR) – Medalia et al (2002)
• Cognitive Enhancement Therapy (CET) – Hogarty & Flesher (1999)
• Neurocognitive Enhancement Therapy (NET) – Bell et al (2007)
• Cognitive Adaptation Training (CAT) – Velligan et al 2008)

Meta-Analyses of RCTs of Cognitive Training/Remediation
2003: 17 studies
Cognition=.32
Symptoms=.26
Functioning=.51
2007: 26 studies
Cognition=.41
Symptoms=.28
Functioning=.36
2011: 40 studies
Cognition=.45
Symptoms=.18
Functioning=.42

What therapists think they are changing with CRT
• Brain connectivity - fMRI
• Cognition – Flexibility, memory, planning, information processing (e.g. Wykes et al 2007)
• Metacognition – thinking about the thinking
• Quality of Life (e.g McGurk et al 2007)
• General functioning
• Symptoms

Targeting cognitive styles and strategies in ED
CRT for AN
Cognitive Flexibility Central Coherence Perfectionism
Cognitive Remediation Therapy for Anorexia
Manual for Clinicians
Tchanturia, Davies, Reeder, Wykes
2007, 2010
London 2 version
available from the SLAM ED website
http://www.national.slam.nhs.uk/wp-
content/uploads/2014/03/Cognitive-remediation-therapy-for-
Anorexia-Nervosa-Kate-Tchantura.pdf

Cognitive Remediation Therapy: ‘The how rather what of thinking’
(Tchanturia et al 2008, Whitney et al 2007, Davies et al 2005)
• Manual based 10-session intervention, twice a week, for adult AN admitted to a specialist ED Unit
• Include exercises to: (1) increase cognitive flexibility (2) see the ‘bigger picture’ (3) relate to real life

Research evidence for CRT in ED
MRC Framework for the Development of Complex Interventions
Routledge 2015 London
www.katetchanturia.com

Framework for Development /
Evaluation of RCTs for
Complex Health
Interventions
Definitive
RCT
Long-term
Implementation
Exploratory
Trial Modelling
Theory
Pre-clinical Phase I Phase II Phase III Phase IV
* Empirical
evidence from ED
* Intervention tailored
from psychosis
• Case Series
23 patients
• Qualitative feedback
Patients / professionals
• Replication
• 7 papers
CRT
Testing
in group
settings
RCT-s published from
USA
Germany
Netherlands
France in progress

First RCT – Stanford USA:
Lock J, Agras S, Fitzpatrick K, Bryson S, Booil J, Tchanturia K (2013) A Randomised assessment of Novel Treatment for anorexia nervosa addressing inefficient cognitive process. International Journal of Eating
Disorders doi: 10.1002/eat.22134
Stanford trial (N=46)
Baseline
1
Post
6 month
Follow
Up
0 14 26
CRT + CBT
CBT
28 sessions Does CRT help to keep patients in the treatment?

RCT from Heidelberg Germany
Heidelberg trial (N=40)
Baseline 1
Post
0 14 26
TAU = CRT
TAU= Non- Specific CT
30 sessions Does CRT improve flexibility of thinking better than NSCT?
Brockmeyer, T., Ingenerf, K., Walther, S., Wild, B., Hartmann, M., Herzog, W., Bents, H., & Friederich, H.-C. (2013) IJED. Training cognitive flexibility in patients with anorexia nervosa: A pilot randomized controlled trial of cognitive remediation therapy.

Dutch trial (N=82)
Baseline
1
Post
6 month
Follow
Up
0 6 30
CRT + TAU
TAU
10 CRT sessions
Does CRT help to improve quality of life and eating pathology?
RCT from The Netherlands
Dingemans, A.E., Danner, U.N., Donker, J.M., Aardoom, J.J., van Meer, F., Tobias, K., van Elburg, A.A., & van Furth, E.F. (2013). The effectiveness of Cognitive Remediation Therapy in patients with a severe or enduring eating disorder: A randomized controlled trial.
Manuscript submitted for publication

RCT – on going France : TRECOGAM
Paris trial (N=120 : 60 AN-R + 60 AN-BP)
Baseline 1
Post
6 month Follow
Up
0 6 30
CRT
PER (Personality-
Emotions- Relationships)
10 sessions
Does CRT improve neuropsychological functioning ?
1 year Follow
Up
54
Does CRT improve clinical outcome ?

CRT improves cognitive task performance
(Tchanturia et al 2014 for review EERD)
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9
Tchanturia et al. (2008)
Abbate-Daga et al. (2013)
Lock et al. (2013)
Dingemans et al. (2013)
Brockmeyer et al. (2013)
Lock et al. (2013)
Dingemans et al. (2013)
Tchanturia et al. (2008)
Set
Shif
tin
gC
en
tral
Co
her
en
ce
Effect sizes of the CRT treatment studies including cognitive assessments

Drop out from the treatment (psychological and psychopharmacological 35-65% reported in the past studies before 2004)
From available evidence drop out from CRT is low! (0-15%)
0
10
20
30
40
50
60
70
Case series

Quality of life more than symptoms improve in Schizophrenia what about AN?
Evidence for QoL improvement from one case series and one RCT trial!
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1

What patients think about CRT
• Qualitative studies in adults (Whitney et al 2008) • Recently larger qualitative study in young people
(12-18): Giombini et al in press: ‘Looking at the big picture is also relevant to real life, especially in stressful situations where it is important to prioritise, such GCSE’. ‘I discovered that I do not like changes, but over the course of my CRT meetings I attempted to change small things. Most of them felt weird, but some changes were good …”

Suggested improvements by patients
• ‘I think that CRT could be improved by having more and longer sessions because they are so much fun. I also think it would be interesting to do some group CRT as well as individual’.
• the use of homework books so it could be discussed and perhaps be more useful…

First case study CRT for AN 2005

What we think works for AN patients well from CRT active
ingredients:
- Shifting from symptoms to thinking styles,
-later to the idea of bigger picture of recovery,
-motivation style,
-playful nature, opportunity to reflect

Future directions Clinical and research developments

Fonville, L., et al. (2014) Cognitive remediation, brain function and central coherence: an anorexia nervosa pilot study. Annals of General Psychiatry, 13:25.

Thanks to the home and international
For manuals and more information visit:
www.katetchanturia.com
Research gate
If we have time for questions?
If not email me:

Thanks
BRC- NIHR Biomedical Research Centre for Mental Health and the National Institute of Health Research (NIHR)
Swiss Anorexia Nervosa Foundation

References Systematic reviews:
• Tchanturia K, Lounes N, Holttum S (2014) Cognitive remediation in anorexia nervosa and related conditions: A systematic review. European Eating Disorders Review 22(6):454-62;DOI: 10.1002/erv.2326
• Tchanturia K, Lloyd S, Lang K (2013) Cognitive Remediation in eating disorders International Journal of Eating Disorders Special Issue. 46(5)492-496
Group CRT:
• Genders R, Tchanturia K (2010) Cognitive Remediation Therapy (CRT) for Anorexia in Group Format: A Pilot study. Eating Weight Disorders. 15 (4):234-239
Patients feedback:
• Whitney J. Easter, A. Tchanturia K (2008) Service users' feedback on cognitive training in the treatment of anorexia nervosa: a qualitative study. International Journal of Eating Disorders; 41(6):542-50
Child adolescent adaptation:
• Pretorius N, Dimmer M, Power E, Eisler I, Simic M, Tchanturia K (2012) Evaluation of a Cognitive Remediation Therapy Group for Adolescents with Anorexia Nervosa: Pilot study. European Eating Disorder Review 20(4):321-5. doi: 10.1002/erv.2176
Careers and family:
• Lang K, Treasure J, Tchanturia K. (2015) Acceptability and feasibility of self-help cognitive remediation therapy for anorexia nervosa delivered in collaboration with carers: A qualitative preliminary evaluation. Psychiatry Research 225 (387-394)- doi: 10.1016/j.psychres

References (fMRI studies) • Fonville L, Giampietro V, Williams S, Simmons A, Tchanturia K. (2013) Alterations in Brain Structure in Adults
with Anorexia Nervosa and the Impact of Illness Duration; Psychological Medicine DOI: 10.1017/S0033291713002389
• Fonville L, Giampietro V, Williams S, Simmons A, Tchanturia K. (2014) Evidence for Neural Changes following Cognitive Remediation Therapy in Anorexia Nervosa; a Pilot fMRI Study; The Annals of General Psychiatry.13,25
• Fonville L, Lao-Kaim NP, Giampietro V, Van den Eynde F, Davies H, Lounes N, Andrew C, Dalton J, Baron-Cohen S, Simmons A, Williams SCR, Tchanturia K. (2013) Evaluation of Enhanced Attention to Local Detail in Anorexia Nervosa using the Embedded Figures Test. Plos One 2013;8.
• Lao-Kaim N, Fonville L, Giampietro V, Williams S, Simmons A, Tchanturia K (2015) Dysregulation of separable brain networks associated with learning and cognitive control underlies inefficient cognitive flexibility in Anorexia Nervosa. Plos one 10(5): e0124027 doi:10.1371/journal.
• pone.0124027
• Lao-Kaim NP, Giampietro V, Williams SCR, Simmons A, Tchanturia K. (2013) Functional MRI investigation of verbal working memory in adults with Anorexia Nervosa. European Psychiatry doi10.1016/j.eurpsy.2013.05.2003
• Fonville L, Giampietro V, Surguladze S, Williams S, Tchanturia K (2014) Increased BOLD signal in the fusiform gyrus during implicit emotion processing in anorexia nervosa; NeuroImage: Clinical; 266–273
• Chapter 11-Cognitive Remediation for Eating and Weight Disorders (2014) edited by Kate Tchanturia; Routledge ISBN 978-1-138-79403-0