cognitive-behavioral psychotherapy for anxiety and
TRANSCRIPT

R E S E A R C H U P D A T E R E V I E W
Cognitive-Behavioral Psychotherapy for Anxiety andDepressive Disorders in Children and Adolescents:
An Evidence-Based Medicine ReviewSCOTT N. COMPTON, PH.D., JOHN S. MARCH, M.D., M.P.H., DAVID BRENT, M.D.,
ANNE MARIE ALBANO, PH.D., V. ROBIN WEERSING, PH.D., AND JOHN CURRY, PH.D.
ABSTRACT
Objective: To review the literature on the cognitive-behavioral treatment of children and adolescents with anxiety and
depressive disorders within the conceptual framework of evidence-based medicine. Method: The psychiatric and
psychological literature was systematically searched for controlled trials applying cognitive-behavioral treatment to
pediatric anxiety and depressive disorders. Results: For both anxiety and depression, substantial evidence supports the
efficacy of problem-specific cognitive-behavioral interventions. Comparisons with wait-list, inactive control, and active
control conditions suggest medium to large effects for symptom reduction in primary outcome domains. Conclusions:
From an evidence-based perspective, cognitive-behavioral therapy is currently the treatment of choice for anxiety and
depressive disorders in children and adolescents. Future research in this area will need to focus on comparing cognitive-
behavioral psychotherapy with other treatments, component analyses, and the application of exportable protocol-driven
treatments to divergent settings and patient populations. J. Am. Acad. Child Adolesc. Psychiatry, 2004;43(8):930–959.
Key Words: outcome studies, children and adolescents with major depression and dysthymic disorder, children and
adolescents with anxiety disorder, literature review.
Due in part to a productive interplay between researchand clinical practice (Rutter, 1999), many clinical re-searchers now believe that cognitive-behavioral therapy(CBT) administered within an evidence-based, multi-modal, multidisciplinary practice model is the psycho-therapeutic treatment of choice for youth withinternalizing disorders (Geddes et al., 1997; March andWells, 2003). In this context, the past 10 years wit-nessed the emergence of diverse, sophisticated, and em-pirically supported CBTs covering the range ofchildhood-onset anxiety and depressive disorders
(Bernstein and Shaw, 1997; Birmaher et al., 1996a,b).Using the tools of evidence-based medicine (EBM)(Sackett et al., 1997), this article provides a criticalreview of CBT for these conditions. We do not addressobsessive-compulsive disorder and posttraumatic stressdisorder, for which recent critical reviews are available(Cohen et al., 2000; Franklin et al., 2002; March,1995), or bipolar disorder, for which cognitive-behavioral interventions are just now emerging (Mc-Clellan and Werry, 1997). The reader interested in a“how-to-do-it” perspective may wish to pursue recentoverviews of CBT (Hibbs and Jensen, 1996; Reineckeet al., 2003) interventions for childhood-onset anxiety(Kendall et al., 1999, 2000, 2003; March and Mulle,1998; Rapee et al., 2000; Silverman and Kurtines,1996) and depressive disorders (Brent et al., 1997;Clarke et al., 1990).
GUIDING THEORY
Although a comprehensive review of the theoreticalrationale of CBT is clearly beyond the scope of thisarticle (for a still cogent précis, see Kendall, 1993; Ken-
Accepted November 17, 2003.Drs. Compton, March, and Curry are with the Department of Psychiatry and
Behavioral Psychology, Duke University Medical Center, Durham, NC; Dr.Brent is with Western Psychiatric Institute and Clinic, Pittsburgh, PA; Dr.Albano is with New York University School of Medicine, NY; and Dr. Weersingis with the Yale Child Study Center, New Haven, CT.
Correspondence to Dr. Compton, Duke University Medical Center, Box3527, Durham, NC 27710; e-mail: [email protected].
0890-8567/04/4308–0930©2004 by the American Academy of Childand Adolescent Psychiatry.
DOI: 10.1097/01.chi.0000127589.57468.bf
J . AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 43:8, AUGUST 2004930

dall and Panichelli-Mindel, 1995), a short overview isheuristically valuable. Historically, behavior therapy(the BT in CBT) evolved within the theoretical frame-work of classical and operant conditioning, with cog-nitive interventions (the C in CBT) assuming a moreprominent role with the increasing recognition thatperson–environment interactions are mediated by cog-nitive processes (Van Hasselt and Hersen, 1993).Looked at in the context of situational and/or cognitiveprocesses, BT is sometimes referred to as nonmedia-tional (emphasizing the direct influence of situationson behavior) and CT as mediational (emphasizing thatthoughts and feelings underlie behavior). Hence, be-havioral psychotherapists work with patients to changebehaviors and thereby to reduce distressing thoughtsand feelings. Cognitive therapists work to first changethoughts and feelings, with improvements in func-tional behavior following in turn.
Although CBT is often referred to as a unitary treat-ment, it is actually a diverse collection of complex andsubtle interventions that must each be mastered andunderstood from the social learning perspective. Sub-sequently, a cognitive-behavioral case formulationguides the therapist in administering treatment tech-niques in a flexible manner for the patient presentingwith any one disorder or comorbid presentation ofmental disorders (for an overview of a modular ap-proach to CBT interventions, see Curry and Reinecke[2003]). Nonetheless, despite their seeming differences,cognitive-behavioral interventions typically share fivequalities: (1) adherence to the scientist–clinicianmodel, whereby treatments are chosen based on dem-onstrated evidence or are applied within a case evalu-ation format to determine efficacy; (2) a thoroughidiographic assessment (e.g., functional analysis) of tar-get behaviors and the situational, cognitive, and behav-ioral factors that have established or are maintainingthe symptoms of interest (for a detailed overview ofhow to conduct a functional analysis, see Haynes andO’Brien [1990]); (3) an emphasis on psychoeducation;(4) problem-specific treatment interventions designedto ameliorate the symptoms of concern; and (5) relapseprevention and generalization training at the end oftreatment. For example, using cognitive restructuringand exposure-based interventions, CBT for anxiety dis-orders encourages cognitions and behaviors designed topromote habituation or extinction of inappropriatefears. Likewise, CBT for depression directly confronts
maladaptive depressogenic cognitions, including help-lessness, hopelessness, and hostility, and aims behavior-ally to reconstitute pleasant relationships, be theyintrapsychic, interpersonal, school, or spiritual. As evi-dence-based therapies, each is supported by a more orless robust research literature, and manuals are usuallyavailable to guide practitioners in using CBT for spe-cific problems. Thus, CBT fits nicely into the currentmedical practice environment that appropriately valuesempirically supported, brief, problem-focused treat-ments.
From this vantage point, CBT represents a develop-mentally sound approach to pediatric mental illness.Children normally acquire social-emotional (self andinterpersonal) competencies across time. The failure todo so, relative to age, gender, and culture-matchedpeers, may reflect capacity limitations, individualdifferences in the rate of skill acquisition for specificcompetencies, environmental factors, and/or the devel-opment of a mental illness. In CBT, the task of themental health practitioner is to understand the present-ing symptoms in the context of child-specific con-straints to normal development and to devise a tailoredtreatment program that eliminates those constraints sothat the youngster can resume a normal developmentaltrajectory insofar as is possible.
To the extent that symptom relief occurs, it can beassumed that improvement reflects concurrent changes(e.g., learning) in the CNS (Andreason, 1997; Hyman,2000). Thus, the cognitive-behavioral treatment of pe-diatric mental illness can be thought of as partiallyanalogous to the treatment of, for example, juvenile-onset diabetes, with the caveat that the target organ, thebrain in the case of major mental illness, requires in-terventions of much greater complexity. Althoughmedications are of importance—in diabetes, insulin,and in the anxiety or affective disorders, a serotoninreuptake inhibitor—the critical point is that each alsoinvolves crucial psychosocial interventions that work inpart by biasing the somatic substrate of the disordertoward more normal functioning (Hyman, 2000). Indiabetes, the behavioral intervention of choice is dietand exercise, and in the anxiety or affective disorders, itis cognitive-behavioral psychotherapy.
METHOD
EBM has emerged as a promising paradigm for medical practice(for a comprehensive review, see Sackett et al. [2000]) and is clini-
RESEARCH UPDATE REVIEW: CBT
J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 43:8, AUGUST 2004 931

cally akin to the scientist–practitioner model in academic psychol-ogy (Barlow, 1993). EBM deemphasizes the more typical relianceon unsystematic clinical experience as a sufficient ground for clini-cal decision making. Instead, EBM stresses the examination of evi-dence from systematic diagnostic assessment technologies andclinical research as a tool to inform clinical practice, and it providesa heuristically valuable organizing focus for the individual clinicianseeking to transition efficacy and effectiveness studies into clinicalpractice at the level of the individual patient (Geddes et al., 1997).
Using established EBM criteria for assessing the validity of treat-ment studies as guides to clinical practice (Guyatt et al., 1993,1994, 1999), a search for relevant literature was conducted viaMedline and PsycINFO, using the following text terms: anxiety,depression, cognitive therapy, and behavior therapy. Only random-ized, controlled trials (RCTs) for individuals with a specific disorderwere included. Additionally, to be included, articles must have metthe following criteria: published in an English-language, peer-reviewed journal between 1990 and 2002; included children be-tween the ages of 8 and 18; included an outcome measure of knownclinical significance; and used an analytic strategy consistent withthe study design. A follow-up assessment was preferred but notrequired. Excluded from consideration were articles concerning thetreatment of obsessive-compulsive disorder, posttraumatic stressdisorder, or bipolar disorder; included were articles concerning thetreatment of specific phobias, social phobia, selective mutism, over-anxious disorder, separation anxiety disorder, panic disorder, gen-eralized anxiety disorder, major depression, and dysthymia.
The text of this article is supported by a series of tables thatsummarize the main findings of each study identified during theliterature search. The tables are organized by type of disorder (anxi-ety versus depression); within each disorder, separate tables sum-marize findings at post-treatment and at long-term follow-up.
The information presented in each table includes study citation(studies are listed in alphabetical order by first author), researchdesign (type, control condition, analysis sample), sample informa-tion (total number, age range, percentage of males, and ethnicity),the diagnoses targeted by the intervention, brief details about theintervention, primary dependent measures (both categorical andscalar), sample size in each treatment condition, proportion ofsample responding, magnitude of the treatment effect (portrayed interms of number needed to treat [NNT] and standardized effectsize estimates), and general comments by the authors.
The NNT is a measure of the average response, presented as theprobability of response in single patient units. Arithmetically, theNNT is the inverse of the absolute risk reduction (1/ARR), definedas the percentage of response in the experimental group minus thepercentage of response in the control condition. In practice, NNTrepresents the number of patients who need to be treated with theactive treatment to produce one additional positive outcome be-yond that obtainable with the control or comparison condition. Forexample, an NNT of 10 describes the number of patients whom aclinician would need to treat with the active treatment rather thanthe control treatment to see one additional positive outcome. A verysmall NNT (that is, an NNT that approaches 1) suggests that afavorable outcome occurs in nearly every patient who receives thetreatment and in relatively few patients in the comparison group.An NNT of 2 or 3 indicates that a treatment is quite effective.
Standardized effect size estimates were calculated with the assis-tance of ES (Shadish et al., 1999), a computer software programdesigned to calculate effect size estimates from published studies. EScalculates the standardized mean difference statistic, commonly re-ferred to as Cohen’s d and computed as d = (Mt − Mc)/SD, where
Mt is the mean of the treatment group, Mc is the mean of thecomparison group, and SD is the pooled within-group standarddeviation. All effect size estimates are reported such that positivescores indicate that the treatment group improved more than thecomparison group.
TREATMENT OF ANXIETY DISORDERS
To their advantage, cognitive-behavioral therapistshave a robust literature validating the effectiveness ofspecific psychological techniques for anxiety disordersand a steadily growing literature supporting the use ofprescriptive treatment protocols for these disorders.
Types of Investigations
Twenty-one RCTs evaluating a variety of cognitive-behavioral interventions for the treatment of child andadolescent anxiety disorders were identified (Table 1).As a group, these studies are noteworthy for their meth-odological rigor and the systematic way in which theyhave advanced the understanding of childhood anxietydisorders and how best to treat this important popula-tion. With respect to methodological rigor, all studiesused contrasting group designs in which active treat-ments were compared with either a wait-list or no-treatment control condition (Cornwall et al., 1996;Hayward et al., 2000; Kendall, 1994; Kendall et al.,1997; King et al., 1998; Shortt et al., 2001; Silvermanet al., 1999a) or an attention placebo-controlled con-dition (Beidel et al., 2000; Last et al., 1998; Muris etal., 2002). Moreover, several studies compared morethan one active treatment condition (Barrett, 1998;Barrett et al., 1996; Beidel et al., 2000; Cobham et al.,1998; Flannery-Schroeder and Kendall, 2000; Mend-lowitz et al., 1999; Menzies and Clarke, 1993; Muris etal., 2001; Nauta et al., 2003; Silverman et al., 1999b;Spence et al., 2000).
Investigators in this area have also systematicallyevaluated a variety of clinically relevant questions: forinstance, whether group CBT is more effective thanindividual CBT (Flannery-Schroeder and Kendall,2000; Manassis et al., 2002; Muris et al., 2001), wheth-er adding parental participation enhances treatmentoutcomes (Barrett, 1998; Barrett et al., 1996; Cobhamet al., 1998; Mendlowitz et al., 1999; Nauta et al.,2003; Shortt et al., 2001; Spence et al., 2000), whetherconcurrent treatment of parental anxiety enhancestreatment outcomes (Cobham et al., 1998), andwhether two active treatment components, which are
COMPTON ET AL.
J . AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 43:8, AUGUST 2004932

TA
BL
E1
Ran
dom
ized
Clin
ical
Tri
als
ofC
BT
for
Chi
ldan
dA
dole
scen
tA
nxie
tyD
isor
ders
:E
ffec
tsat
Post
-tre
atm
ent
Aut
hor(
s)D
esig
nSa
mpl
eIn
form
atio
nT
arge
tD
iagn
osis
Tre
atm
ent
Info
rmat
ion
Prim
ary
Dep
ende
ntM
easu
res
Sam
ple
Size
(Ini
tial
/C
ompl
eted
)Pr
opor
tion
Res
pond
ing
Post
trea
tmen
tE
BM
NN
TE
ffec
tSi
zeC
omm
ents
Bar
rett
,19
98R
CT
,al
tern
ativ
etr
eatm
ent
and
WL
cont
rol,
blin
das
sess
men
t,co
mpl
eter
anal
ysis
N=
607–
14ye
ars,
53%
mal
eE
thni
city
unsp
ecifi
ed
OA
D(n
=30
)SA
D(n
=26
)SO
P(n
=4)
12se
ssio
ns,
grou
pC
BT
-C12
sess
ions
,gr
oup
fam
ilyC
BT
-CP
WL
(12
wee
ks,
then
offe
red
trea
tmen
t)
FSSC
-RC
BC
LN
oan
xiet
ydx
23/1
917
/15
20/1
6
11/1
911
/15
4/16
4 2 FSSC
-RG
CB
T=
1.58
GC
BT
+=
2.53
CB
CL-
I(m
othe
r)G
CB
T=
3.37
GC
BT
+=
3.98
Bot
htr
eatm
ents
asso
ciat
edw
ith
sign
ifica
ntim
prov
emen
ts;
GC
BT
+as
soci
ated
wit
hm
argi
nally
bett
erou
tcom
es
Bar
rett
,D
adds
,&
Rap
ee,
1996
RC
T,
WL
cont
rol,
blin
das
sess
men
t,co
mpl
eter
anal
ysis
N=
7 99.
3ye
ars
57%
mal
eE
thni
city
unsp
ecifi
ed
OA
D(n
=30
)SA
P(n
=30
)SO
P(n
=19
)
12se
ssio
ns,
indi
vidu
alC
BT
12se
ssio
ns,
indi
vidu
alC
BT
-CP
WL
(12
wee
ks,
then
offe
red
trea
tmen
t)
RC
MA
SFS
SC-R
CB
CL
No
anxi
ety
dx
28/2
825
/25
26/2
3
16/2
821
/25
6/23
3 2 RC
MA
SC
BT
=0.
40C
BT
+=
0.94
FSSC
-RC
BT
=0.
49C
BT
+=
0.73
CB
CL-
I(m
othe
r)C
BT
=0.
96C
BT
+=
1.19
Bot
hac
tive
trea
tmen
tssh
owed
posi
tive
bene
fit,
CB
T+
was
supe
rior
onse
vera
lou
tcom
es
Bei
del,
Tur
ner,
&M
orri
s,20
00
RC
T;
nons
peci
fictr
eatm
ent
cont
rol,
blin
das
sess
men
t,co
mpl
eter
anal
ysis
N=
6 710
.5ye
ars;
40%
mal
e,70
%w
hite
SOP
(n=
67)
12in
divi
dual
and
12gr
oup
sess
ions
,C
BT
12in
divi
dual
and
12gr
oup
sess
ions
,N
onsp
ecifi
ctr
eatm
ent
cont
rol
SPA
I-C
,C
-GA
S,A
DIS
-CC
SR,
No
anxi
ety
dx
36/3
031
/20
20/3
01/
202 SP
AI-
C=
0.91
C-G
AS
=1.
46A
DIS
-CC
SR=
2.04
Act
ive
trea
tmen
tw
asas
soci
ated
wit
hsi
gnifi
cant
impr
ovem
ents
acro
ssm
ulti
ple
dom
ains
—co
ntin
ued
RESEARCH UPDATE REVIEW: CBT
J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 43:8, AUGUST 2004 933

TA
BL
E1
cont
inue
d
Aut
hor(
s)D
esig
nSa
mpl
eIn
form
atio
nT
arge
tD
iagn
osis
Tre
atm
ent
Info
rmat
ion
Prim
ary
Dep
ende
ntM
easu
res
Sam
ple
Size
(Ini
tial
/C
ompl
eted
)Pr
opor
tion
Res
pond
ing
Post
trea
tmen
tE
BM
NN
TE
ffec
tSi
zeC
omm
ents
Cob
ham
,D
adds
,&
Spen
ce,
1998
RC
T,
alte
rnat
ive
trea
tmen
tco
ntro
l,bl
ind
asse
ssm
ent,
ITT
anal
ysis
N=
679.
6ye
ars
51%
mal
eE
thni
city
unsp
ecifi
ed
SAD
(n=
8)O
AD
(n=
3)G
AD
(n=
40)
SIP
(n=
12)
SOP
(n=
3)A
GP
(n=
1)
10se
ssio
ns,
child
-foc
used
grou
pC
BT
(par
ents
part
icip
ated
)10
sess
ions
plus
4pa
rent
anxi
ety
man
agem
ent
sess
ions
,gr
oup
CB
T+P
AM
(par
ents
part
icip
ated
);ou
tcom
esw
ere
also
cros
sed
onpa
rent
alan
xiet
y(n
onan
xiou
spa
rent
vs.
anxi
ous
pare
nt)
RC
MA
SST
AIC
No
anxi
ety
dx(u
sing
AD
IS-P
CSR
)
35/3
532
/32
(not
e:3
fam
ilies
inea
chco
ndit
ion
com
plet
edle
ssth
an50
%of
the
sess
ions
)
CB
TN
AP
=14
/17
CB
TA
P=
7/18
CB
T+P
AM
NA
P=
12/1
5C
BT
+PA
MA
P=
13/1
7
(Cal
cula
tion
sm
ade
usin
gC
BT
AP
asco
ntro
lco
ndit
ion)
CB
TN
AP
=2
CB
T+P
AM
NA
P=
2C
BT
+PA
MA
P=
3
ESs
wer
eno
tca
lcul
ated
onse
lf-re
port
mea
sure
sdu
eto
low
com
plet
ion
rate
ofth
eas
sess
men
tin
stru
men
ts(n
=29
)
Chi
ldre
nw
ith
anxi
ous
pare
nt(s
)re
spon
ded
less
favo
rabl
yto
child
-foc
used
CB
Tat
post
-tre
atm
ent;
the
addi
tion
ofPA
Mim
prov
edou
tcom
esfo
rch
ildre
nw
ith
anxi
ous
pare
nt(s
)bu
tno
tfo
rch
ildre
nw
ith
nona
nxio
uspa
rent
s
Cor
nwal
l,Sp
ence
,&
Scho
tte,
1996
RC
T,
WL
cont
rol,
blin
dnes
sun
clea
r,co
mpl
eter
anal
ysis
N=
2 48.
25ye
ars
Gen
der
unsp
ecifi
edE
thni
city
unsp
ecifi
ed
SIP
(dar
knes
sph
obia
,n
=24
)
6se
ssio
ns,
emot
ive
imag
ery
WL
(3m
onth
sin
dura
tion
)
FSSC
-RR
CM
AS
FT DFB
Q
12/1
212
/?D
ata
unav
aila
ble
Dat
aun
avai
labl
eto
calc
ulat
eN
NT
FSSC
-R=
0.53
RC
MA
S=
0.52
DFB
Q=
1.59
Act
ive
trea
tmen
tas
soci
ated
wit
hsi
gnifi
cant
impr
ovem
ent
inal
lou
tcom
es
Flan
nery
-Sc
hroe
der
& Ken
dall,
2000
RC
T,
WL
cont
rol,
blin
das
sess
men
t,IT
Tan
dco
mpl
eter
anal
ysis
N=
4 58–
14ye
ars
46%
mal
es89
%w
hite
GA
D(n
=21
)SA
D(n
=11
)SO
P(n
=5 )
18se
ssio
ns,
indi
vidu
alC
BT
18se
ssio
ns,
grou
pC
BT
WL
(9w
eeks
,th
enof
fere
dtr
eatm
ent)
RC
MA
SC
BC
L-I
No
anxi
ety
dx(u
sing
AD
IS-P
)
18/1
313
/12
14/1
2
No
anxi
ety
dx(I
TT
)8/
186/
130/
14
2 2 RC
MA
SIC
BT
=0.
79G
CB
T=
1.11
CB
CL-
IIC
BT
=1.
52G
CB
T=
0.84
Bot
hin
divi
dual
and
grou
pC
BT
wer
eas
soci
ated
wit
hlo
wer
rate
sof
anxi
ety
diso
rder
san
den
hanc
edco
ping
abili
ties
;ou
tcom
esfo
rIC
BT
and
GC
BT
wer
eco
mpa
rabl
e
—co
ntin
ued
COMPTON ET AL.
J . AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 43:8, AUGUST 2004934

TA
BL
E1
cont
inue
d
Aut
hor(
s)D
esig
nSa
mpl
eIn
form
atio
nT
arge
tD
iagn
osis
Tre
atm
ent
Info
rmat
ion
Prim
ary
Dep
ende
ntM
easu
res
Sam
ple
Size
(Ini
tial
/C
ompl
eted
)Pr
opor
tion
Res
pond
ing
Post
trea
tmen
tE
BM
NN
TE
ffec
tSi
zeC
omm
ents
Hay
war
det
al.,
2000
RC
T,
no-t
reat
men
tco
ntro
l,bl
ind
asse
ssm
ent,
com
plet
eran
alys
is
N=
3515
.8ye
ars
100%
fem
ales
Eth
nici
tyun
spec
ified
SOP
(n=
35)
16se
ssio
ns,
grou
pC
BT
No-
trea
tmen
tco
ntro
l
AD
ISC
SR,
SPA
I-C
No
anxi
ety
dx
12/1
123
/22
6/11
1/22
2 AD
IS-C
=1.
23A
DIS
-P=
0.67
SPA
I-C
=0.
29
Act
ive
trea
tmen
tw
asas
soci
ated
wit
hsi
gnifi
cant
impr
ovem
ent;
55%
ofsu
bjec
tsco
ntin
ued
tom
eet
diag
nost
iccr
iter
iafo
rdx
Ken
dall,
1994
RC
T,
WL
cont
rol,
blin
dnes
sun
clea
r,co
mpl
eter
anal
ysis
N=
479–
13ye
ars
60%
mal
es76
%w
hite
OA
D(n
=30
)SA
D(n
=8 )
AV
D(n
=9 )
16se
ssio
ns,
indi
vidu
alC
BT
WL
(8w
eeks
,th
enof
fere
dtr
eatm
ent)
RC
MA
SFS
SC-R
CB
CL-
I
No
prim
ary
anxi
ety
dx(u
sing
AD
IS-P
)
27/N
R20
/NR
(Not
e:13
subj
ects
drop
ped,
not
repo
rted
bygr
oup)
17/2
71/
202 R
CM
AS
=0.
87FS
SC-R
=0.
38C
BC
L-I
=1.
22
Indi
vidu
alC
BT
was
asso
ciat
edw
ith
low
erra
tes
ofan
xiet
ydi
sord
ers
and
enha
nced
copi
ngab
iliti
esK
enda
ll,Fl
anne
y-Sc
hroe
der,
Pani
chel
li-M
inde
l,So
utha
m-
Ger
owet
al.,
1997
RC
T,
WL
conr
ol,
blin
dnes
sun
clea
r,co
mpl
eter
anal
ysis
N=
9 49–
13ye
ars
62%
mal
e85
%w
hite
OA
D(n
=55
)SA
D(n
=22
)A
VD
(n=
17)
16se
ssio
ns,
indi
vidu
alC
BT
WL
(8w
eeks
,th
enof
fere
dtr
eatm
ent)
RC
MA
SST
AIC
No
anxi
ety
dxby
AD
IS-P
75/6
043
/34
32/6
02/
342 R
CM
AS
-0.
59ST
AIC
-TA
=0.
72ST
AIC
-SA
=0.
40
Ove
rall,
resu
ltsw
ere
very
sim
ilar
toea
rlie
rst
udy
ofin
divi
dual
CB
T
Kin
get
al.,
1998
RC
T,
WL
cont
rol,
blin
dnes
sun
clea
r,co
mpl
eter
anal
ysis
N=
3 411
.03
year
s53
%m
ale
Eth
nici
tyun
spec
ified
SR(n
=34
)6
sess
ions
(ove
r4
wee
ks;
plus
5pa
rent
sess
ions
and
1te
ache
rm
eeti
ng),
indi
vidu
alC
BT
WL
(4w
eeks
,th
enof
fere
dtr
eatm
ent)
Scho
olat
tend
ance
(%da
yspr
esen
t)FT G
AF
CB
CL-
I
17/1
717
/17
No.
who
achi
eved
90%
scho
olat
tend
ance
15/1
75/
17
2 FT=
1.38
GA
F=
1.50
CB
CL-
I=
0.59
Act
ive
trea
tmen
tw
asas
soci
ated
wit
hsi
gnifi
cant
impr
ovem
ents
onal
lou
tcom
esex
cept
teac
her
repo
rts
—co
ntin
ued
RESEARCH UPDATE REVIEW: CBT
J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 43:8, AUGUST 2004 935

TA
BL
E1
cont
inue
d
Aut
hor(
s)D
esig
nSa
mpl
eIn
form
atio
nT
arge
tD
iagn
osis
Tre
atm
ent
Info
rmat
ion
Prim
ary
Dep
ende
ntM
easu
res
Sam
ple
Size
(Ini
tial
/C
ompl
eted
)Pr
opor
tion
Res
pond
ing
Post
trea
tmen
tE
BM
NN
TE
ffec
tSi
zeC
omm
ents
Last
,H
anse
n,&
Fran
co,
1998
RC
T,
alte
rnat
ive
trea
tmen
tco
ntro
l,bl
indn
ess
uncl
ear,
com
plet
eran
alys
is
N=
5612
.04
year
s,40
%m
ale
89%
whi
te
ASR
(n=
56)
12se
ssio
ns,
indi
vidu
alC
BT
12se
ssio
ns,
indi
vidu
alE
S
Scho
olat
tend
ance
GIS
FSSC
-RST
AIC
-MN
oan
xiet
ydx
32/2
024
/21
No.
who
atta
ined
95%
atte
ndan
ce13
/20
10/2
1
6 95%
atte
ndan
ce=
0.39
Clin
icia
nG
IS=
0.20
FSSC
-R=
0.49
STA
IC-M
=0.
31N
odx
=0.
39
Bot
htr
eatm
ents
wer
eeq
ually
effe
ctiv
ein
retu
rnin
gch
ildre
nto
scho
ol
Man
assi
set
al.,
2002
RC
T,
alte
rnat
ive
trea
tmen
tco
ntro
l,bl
indn
ess
uncl
ear,
com
plet
eran
alys
is
N=
789.
98ye
ars
54%
mal
e85
%w
hite
GA
D(n
=47
)SA
D(n
=20
)SI
P(n
=5)
SOP
(n=
5)PA
D(n
=1)
12se
ssio
ns,
indi
vidu
alC
BT
12se
ssio
ns,
grou
pC
BT
(Not
e:pa
rent
spa
rtic
ipat
edin
both
trea
tmen
ts)
MA
SCC
GA
S41
/NR
37/N
RC
ateg
oric
alou
tcom
esw
ere
not
prov
ided
NA
Rel
ativ
eto
indi
vidu
alC
BT
MA
SC=
−0.3
1C
GA
S=
−0.6
4
Bot
htr
eatm
ents
wer
eas
soci
ated
wit
him
prov
emen
tson
child
and
pare
ntra
ting
s;cl
inic
ian
CG
AS
rati
ngs
favo
red
indi
vidu
alC
BT
;in
divi
dual
CB
Tw
asm
ore
effe
ctiv
efo
rch
ildre
nre
port
ing
high
rate
sof
soci
alan
xiet
yM
endl
owit
zet
al.,
1999
RC
T,
alte
rnat
ive
trea
tmen
tco
ntro
l,bl
indn
ess
uncl
ear,
com
plet
eran
alys
is
N=
6 89.
8ye
ars
43%
mal
eE
thni
city
unsp
ecifi
ed
Chi
ldre
nw
ith
DSM
-IV
anxi
ety
dx(u
sing
DIC
A-R
-P)
12se
ssio
ns,
grou
pC
BT
(chi
ldon
ly)
12se
ssio
ns,
grou
pC
BT
-P12
sess
ions
,gr
oup
CB
T-C
PW
L(2
to6
mon
ths,
then
offe
red
trea
tmen
t)
RC
MA
SC
CSC
GIS
23/2
321
/21
18/1
8
Cat
egor
ical
outc
omes
wer
eno
tpr
ovid
ed
NA
RC
MA
SC
BT
-C=
0.18
CB
T-P
=0.
18C
BT
-CP
=0.
35C
CSC
(Act
ive
Cop
ing)
CB
T-C
=0.
26C
BT
-P=
−0.6
5C
BT
-CP
=0.
57C
CSC
(Avo
idan
tC
opin
g)C
BT
-C=
0.33
CB
T-P
=−0
.39
CB
T-C
P=
0.39
All
thre
etr
eatm
ents
wer
eas
soci
ated
wit
hsi
gnifi
cant
impr
ovem
ents
insy
mpt
oms
ofan
xiet
yan
dde
pres
sion
;ch
ildre
nin
CB
T(c
hild
+pa
rent
)co
ndit
ion
repo
rted
usin
gm
ore
adap
tive
copi
ngsk
ills
than
the
othe
rtw
otr
eatm
ent
cond
itio
ns
—co
ntin
ued
COMPTON ET AL.
J . AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 43:8, AUGUST 2004936

TA
BL
E1
cont
inue
d
Aut
hor(
s)D
esig
nSa
mpl
eIn
form
atio
nT
arge
tD
iagn
osis
Tre
atm
ent
Info
rmat
ion
Prim
ary
Dep
ende
ntM
easu
res
Sam
ple
Size
(Ini
tial
/C
ompl
eted
)Pr
opor
tion
Res
pond
ing
Post
trea
tmen
tE
BM
NN
TE
ffec
tSi
zeC
omm
ents
Men
zies
&C
lark
e,19
93
RC
T,
alte
rnat
ive
trea
tmen
tco
ntro
l,bl
ind
asse
ssm
ent,
com
plet
eran
alys
is
N=
485.
5ye
ars
65%
mal
eE
thni
city
unsp
ecifi
ed
SIP
(wat
erph
obia
,n
=48
)
3se
ssio
ns,
IVV
E3
sess
ions
,V
E3
sess
ions
,IV
EN
o-tr
eatm
ent
cont
rol
BR
SPC
WP
CW
PO
R
13/1
213
/12
12/1
2
Cat
egor
ical
outc
omes
wer
eno
tpr
ovid
ed
NA
Una
ble
toca
lcul
ate
due
toin
suff
icie
ntda
ta
Bot
hIV
VE
and
IVE
wer
eeq
ually
effe
ctiv
ean
dm
ore
effe
ctiv
eth
anW
Lin
redu
cing
wat
erph
obia
;IV
Ere
sulte
din
grea
ter
gene
raliz
atio
nto
nove
lsi
tuat
ions
;V
Esh
owed
nobe
nefit
over
no-t
reat
men
tco
ntro
lM
uris
,M
ayer
,B
arte
lds,
Tie
rney
,&
Bog
ie,
2001
RC
T,
alte
rnat
ive
trea
tmen
tco
ntro
l,bl
indn
ess
uncl
ear,
com
-pl
eter
anal
ysis
N=
3 69.
9ye
ars
25%
mal
e97
%w
hite
GA
D(n
=14
)SA
D(n
=14
)SO
P(n
=7 )
OC
D(n
=1 )
12se
ssio
ns,
indi
vidu
alC
BT
12se
ssio
ns,
grou
pC
BT
SCA
RE
D-R
STA
IC17
/not
repo
rted
19/n
otre
port
ed
Cat
egor
ical
outc
omes
wer
eno
tpr
ovid
ed
NA
Rel
ativ
eto
indi
vidu
alC
BT
SCA
RE
D-R
(tot
al)
=−0
.32
STA
IC(t
rait
anxi
ety)
=0.
14
Bot
htr
eatm
ents
wer
eas
soci
ated
wit
heq
ual
impr
ovem
ents
insy
mpt
oms
ofan
xiet
y
Mur
is,
Mee
ster
s,&
van
Mel
ick
2002
RC
T,
psyc
holo
gica
lPB
Oan
dno
-tre
atm
ent
cont
rol,
blin
dnes
sun
clea
r,co
mpl
eter
anal
ysis
N=
3 010
.2ye
ars
33%
mal
e90
%w
hite
SAD
(n=
10)
GA
D(n
=7 )
SOP
(n=
3 )D
iagn
osti
cst
atus
ofno
-tre
at-
men
tco
ntro
lsno
tas
sess
ed
12se
ssio
ns,
grou
pC
BT
12se
ssio
ns,
grou
pE
DN
o-tr
eatm
ent
cont
rol
RC
AD
SST
AIC
10/1
010
/10
10/1
0
Cat
egor
ical
outc
omes
wer
eno
tpr
ovid
ed
NA
Com
bine
dac
tive
trea
tmen
tre
lati
veto
no-t
reat
men
tco
ntro
lR
CA
DS
(tot
alan
xiet
y)C
BT
=1.
48E
D=
−0.1
7ST
AIC
(tra
itan
xiet
y)C
BT
=0.
83E
D=
−0.4
6
CB
Tre
lati
veto
ED
RC
AD
S(t
otal
anxi
ety)
=0.
98ST
AID
(tra
itan
xiet
y)=
1.05
CB
Tw
assu
peri
orto
ED
and
no-t
reat
men
tco
ntro
l;E
Dsh
owed
nobe
nefit
over
no-t
reat
men
tco
ntro
l
—co
ntin
ued
RESEARCH UPDATE REVIEW: CBT
J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 43:8, AUGUST 2004 937

TA
BL
E1
cont
inue
d
Aut
hor(
s)D
esig
nSa
mpl
eIn
form
atio
nT
arge
tD
iagn
osis
Tre
atm
ent
Info
rmat
ion
Prim
ary
Dep
ende
ntM
easu
res
Sam
ple
Size
(Ini
tial
/C
ompl
eted
)Pr
opor
tion
Res
pond
ing
Post
trea
tmen
tE
BM
NN
TE
ffec
tSi
zeC
omm
ents
Nau
ta,
Scho
ling,
Em
mel
kam
p,& M
inde
raa,
2003
RC
T,
WL
cont
rol,
blin
das
sess
men
t,IT
Tan
alys
is
N=
7911
.0ye
ars
49%
mal
eE
thni
city
unsp
ecifi
ed
SAD
(n=
26)
SOP
(n=
31)
GA
D(n
=15
)PA
D(n
=7)
12se
ssio
ns,
indi
vidu
alC
BT
12se
ssio
ns,
indi
vidu
alC
BT
plus
7se
ssio
nsC
PTW
L(d
urat
ion
not
spec
ified
,th
enof
fere
dtr
eatm
ent)
SCA
S-c/
pFS
SC-R
CB
CL
No
anxi
ety
dx(A
DIS
-Can
dP)
29/2
630
/30
20/1
7
Com
bine
dvs
.W
L32
/59
2/18
CB
Tvs
.C
BT
+20
/37
23/3
9
Act
ive
trea
tmen
tre
lati
veto
WL
2 Una
ble
toca
lcul
ate
due
toin
suff
icie
ntda
ta
CB
Tre
lati
veto
CB
T+
20
SCA
S-c
=−0
.20
SCA
S-p
=−0
.33
FSSC
-R=
−0.1
2
Rel
ativ
eto
WL,
acti
vetr
eatm
ent
show
edlo
wer
scor
eson
pare
ntre
port
san
dm
ore
child
ren
diag
nost
icfr
ee;
nodi
ffer
ence
betw
een
WL
and
acti
vetr
eatm
ent
onch
ildre
port
s;th
ead
diti
onof
CPT
show
edno
addi
tion
albe
nefit
acro
ssal
lou
tcom
esSh
ortt
,B
arre
tt,
&Fo
x,20
01
RC
T,
WL
cont
rol,
blin
das
sess
men
t,co
mpl
eter
anal
ysis
N=
7 17.
85ye
ars
41%
mal
e92
%A
ustr
alia
n
GA
D(n
=42
)SA
D(n
=19
)SO
P(n
=10
)
10se
ssio
ns(p
lus
2bo
oste
rse
ssio
ns),
grou
pC
BT
WL
(10
wee
ks,
then
offe
red
trea
tmen
t)
RC
MA
SC
BC
LN
oan
xiet
ydx
54/4
817
/16
33/4
81/
162 R
CM
AS
=0.
99M
othe
rC
BC
L-I
=5.
08Fa
ther
CB
CL-
I=
1.91
Act
ive
trea
tmen
tw
asas
soci
ated
wit
hsi
gnifi
cant
impr
ovem
ents
acro
ssal
lou
tcom
es
Silv
erm
anet
al.,
1999
aR
CT
,W
Lco
ntro
l,bl
ind
asse
ssm
ent,
com
plet
eran
alys
is
N=
569.
66ye
ars
61%
mal
es45
%w
hite
GA
D(n
=12
)SO
P(n
=15
)O
AD
(n=
29)
12se
ssio
ns,
grou
pC
BT
(con
curr
ent
child
and
pare
ntgr
oups
wit
h15
min
.co
njoi
ntm
eeti
ng)
WL
(8to
10w
eeks
,th
enof
fere
dtr
eatm
ent)
RC
MA
SFS
SC-R
CB
CL-
IPG
RS
No
anxi
ety
dx(A
DIS
-C/P
)
37/2
519
/16
16/2
52/
162 R
CM
AS
=0.
58FS
SC-R
=0.
65C
BC
L-I
=1.
25PG
RS
=1.
78
Gro
upC
BT
was
asso
ciat
edw
ith
sign
ifica
ntim
prov
emen
tsac
ross
all
prim
ary
outc
ome
dom
ains
s
—co
ntin
ued
COMPTON ET AL.
J . AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 43:8, AUGUST 2004938

TA
BL
E1
cont
inue
d
Aut
hor(
s)D
esig
nSa
mpl
eIn
form
atio
nT
arge
tD
iagn
osis
Tre
atm
ent
Info
rmat
ion
Prim
ary
Dep
ende
ntM
easu
res
Sam
ple
Size
(Ini
tial
/C
ompl
eted
)Pr
opor
tion
Res
pond
ing
Post
trea
tmen
tE
BM
NN
TE
ffec
tSi
zeC
omm
ents
Silv
erm
anet
al.,
1999
bR
CT
,al
tern
ativ
etr
eatm
ent
cont
rol,
blin
das
sess
men
t,co
mpl
eter
anal
ysis
N=
104
9.83
year
s52
%m
ales
62%
whi
te
SIP
(n=
87)
SOP
(n=
10)
AG
P(n
=7)
10se
ssio
ns,
indi
vidu
alch
ildan
dpa
rent
SC10
sess
ions
,in
divi
dual
child
and
pare
ntC
M10
sess
ions
,in
divi
dual
child
and
pare
ntE
S
RC
MA
SFS
SC-R
PGR
SN
oan
xiet
ydx
40/3
341
/32
23/1
6
29/3
318
/32
9/16
3 NA
RC
MA
SSC
=0.
72C
M=
0.13
FSSC
-RSC
=1.
07C
M=
0.18
PGR
SSC
=0.
47C
M=
0.40
All
thre
etr
eatm
ent
cond
itio
nssh
owed
com
para
ble
impr
ovem
ent
Spen
ceet
al.,
2000
RC
T,
WL,
blin
das
sess
men
t,co
mpl
eter
anal
ysis
N=
5 010
.7ye
ars
62%
mal
eE
thni
city
unsp
ecifi
ed
SOP
(n=
50)
12se
ssio
ns,
child
and
pare
ntgr
oup
CB
T12
sess
ions
,ch
ildon
lygr
oup
CB
TN
o-tr
eatm
ent
WL
AD
IS-P
CSR
RC
MA
SN
oan
xiet
ydx
(AD
IS-P
)
17/1
619
/15
14/9
14/1
69/
151/
9
1 2 AD
IS-P
CSR
CB
T-C
P=
1.88
CB
T=
1.01
RC
MA
SC
BT
-CP
=0.
45C
BT
=0.
46
Bot
htr
eatm
ents
wer
eas
soci
ated
wit
hsi
gnifi
cant
impr
ovem
ents
;no
sign
ifica
ntdi
ffer
ence
betw
een
acti
vetr
eatm
ents
note
d
Not
e:A
DIS
CSR
=A
nxie
tyD
isor
ders
Inte
rvie
wSc
hedu
lefo
rC
hild
ren,
clin
icia
nse
veri
tyra
ting
(sum
mar
ysc
ore)
;A
DIS
-C=
Anx
iety
Dis
orde
rsIn
terv
iew
Sche
dule
for
Chi
ldre
n;A
DIS
-CC
SR=
Anx
iety
Dis
orde
rsIn
terv
iew
Sche
dule
for
Chi
ldre
n,cl
inic
ian
seve
rity
rati
ngch
ildba
sed;
AD
IS-P
=A
nxie
tyD
isor
ders
Inte
rvie
wSc
hedu
lefo
rC
hild
ren,
Pare
ntV
ersi
on;
AD
IS-P
CSR
=A
nxie
tyD
isor
ders
Inte
rvie
wSc
hedu
lefo
rChi
ldre
n,cl
inic
ian
seve
rity
rati
ngpa
rent
base
d;A
GP
=ag
orap
hobi
a;A
SR=
anxi
ety-
base
dsc
hool
refu
sal;
AT
cont
rol=
alte
rnat
ive
trea
tmen
tco
ntro
l;A
VD
=av
oida
ntdi
sord
er;
BR
S=
Beh
avio
urR
atin
gSc
ale;
CB
CL
=C
hild
Beh
avio
rC
heck
list;
CB
CL-
I=
Chi
ldB
ehav
ior
Che
cklis
t-In
tern
aliz
ing
Subs
cale
;C
BT
=co
gnit
ive-
beha
vior
alth
erap
y;C
BT
AP
=C
BT
wit
han
xiou
spa
rent
; CB
TN
AP
=C
BT
wit
hno
nanx
ious
pare
nt;C
BT
+PA
M=
CB
Tpl
uspa
rent
alan
xiet
ym
anag
emen
t;C
BT
+PA
MA
P=
CB
Tpl
uspa
rent
alan
xiet
ym
anag
emen
twit
han
xiou
spa
rent
;CB
T+P
AM
NA
P=
CB
Tpl
uspa
rent
alan
xiet
ym
anag
emen
twit
hno
nanx
ious
pare
nt;C
BT
-C=
CB
Tch
ildon
ly;C
BT
-CP
=C
BT
child
and
pare
nt;
CB
T-P
=C
BT
pare
nton
ly;
CC
SC=
Chi
ldre
n’s
Cop
ing
Stra
tegi
esC
heck
list;
CG
AS
=C
hild
ren’
sG
loba
lA
sses
smen
tSc
ale;
CM
=co
ntin
genc
y-m
anag
emen
tth
erap
y;C
WP
=W
ater
Phob
iaSu
rvey
Sche
dule
,ch
ildve
rsio
n;D
FBQ
=D
arkn
ess
Fear
Beh
avio
urQ
uest
ionn
aire
;D
ICA
-R-P
=D
iagn
osti
cIn
vent
ory
for
Chi
ldre
nan
dA
dole
scen
ts-
Rev
ised
,Pa
rent
Ver
sion
;dx
=di
agno
sis;
ED
=em
otio
nald
iscl
osur
e;E
Ss=
effe
ctsi
zees
tim
ates
;FS
SC-R
=Fe
arSu
rvey
Sche
dule
for
Chi
ldre
n-R
evis
ed;
FT=
fear
ther
mom
eter
;G
AD
=ge
nera
lized
anxi
ety
diso
rder
;G
AF
=G
loba
lA
sses
smen
tof
Func
tion
ing;
GC
BT
=gr
oup
cogn
itiv
e-be
havi
oral
ther
apy;
GIS
=G
loba
lIm
prov
emen
tSc
ale;
ICB
T=
indi
vidu
alco
gnit
ive
beha
vior
ther
apy;
ITT
=in
tent
totr
eat;
IVE
=in
vivo
expo
sure
;IV
VE
=in
vivo
expo
sure
plus
vica
riou
sex
posu
re;
MA
SC=
Mul
tidi
men
sion
alA
nxie
tySc
ale
for
Chi
ldre
n;N
A=
not
avai
labl
e;N
R=
not
repo
rted
;N
Tco
ntro
l=no
-tre
atm
ent
cont
rol;
OA
D=
over
anxi
ous
diso
rder
;O
R=
over
all
reac
tion
toph
obic
situ
atio
n;PA
D=
pani
cdi
sord
erw
ith
orw
itho
utag
orap
hobi
a;PA
M=
pare
ntal
anxi
ety
man
agem
ent;
PBO
=pl
aceb
o;PC
WP
=W
ater
Phob
iaSu
rvey
Sche
dule
,Par
entV
ersi
on;P
GR
S=
pare
ntgl
obal
rati
ngof
seve
rity
;RC
AD
S=
Rev
ised
Chi
ldre
n’s
Anx
iety
and
Dep
ress
ion
Scal
e;R
CM
AS
=R
evis
edC
hild
ren’
sM
anife
stA
nxie
tySc
ales
;RC
T=
rand
omiz
edcl
inic
altr
ial;
SAD
=se
para
tion
anxi
ety
diso
rder
;SC
=se
lf-co
ntro
lth
erap
y;SC
AR
ED
-R=
Scre
enfo
rC
hild
Anx
iety
Rel
ated
Em
otio
nal D
isor
ders
-Rev
ised
;SC
AS-
c/p
=Sp
ence
Chi
ldA
nxie
tySc
ale,
Chi
ldan
dPa
rent
Ver
sion
;SIP
=si
mpl
eph
obia
;SO
P=
soci
alph
obia
;SPA
I-C
=So
cial
Phob
iaan
dA
nxie
tyIn
vent
ory
for
Chi
ldre
n;SR
=sc
hool
-ref
usin
gch
ildre
n;ST
AIC
=St
ate-
Tra
itA
nxie
tyIn
vent
ory
for
Chi
ldre
n;ST
AIC
-M=
Mod
ified
Stat
e-T
rait
Anx
iety
Inve
ntor
yfo
rC
hild
ren;
STA
IC-S
A=
Stat
e-T
rait
Anx
iety
Inve
ntor
yfo
rC
hild
ren
stat
ean
xiet
y;ST
AIC
-TA
=St
ate-
Tra
itA
nxie
tyIn
vent
ory
for
Chi
ldre
ntr
ait
anxi
ety;
VE
=vi
cari
ous
expo
sure
;W
L=
wai
t-lis
tco
ntro
l.
RESEARCH UPDATE REVIEW: CBT
J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 43:8, AUGUST 2004 939

often combined in traditional cognitive-behavioral pro-tocols (e.g., behavioral contingency management versuscognitive self-control), are differentially effective (Sil-verman et al., 1999b). Moreover, several of the studiescited were replications and extensions of existing pro-tocols by independent researchers (Barrett, 1998; Bar-rett et al., 1996; Manassis et al., 2002; Mendlowitz etal., 1999; Muris et al., 2001, 2002).
Assessment Issues
Diagnosis and Symptom Profile. Valid and reliableassessment is essential to the skillful application andevaluation of cognitive-behavioral treatments (Thyer,1991) and is a strength of the cited studies taken as awhole. All but 2 of the 21 studies cited in Table 1(Cornwall et al., 1996; Menzies and Clarke, 1993) usedsemistructured clinical interviews to identify subjects ashaving an anxiety disorder as well as documenting di-agnostic comorbidities and assessing treatment out-comes. By a significant margin (13 of 21), the mostwidely used semistructured clinical interview was theAnxiety Disorders Interview Schedule, Child and Par-ents Versions (ADIS-C/P) (Silverman, 1987; Silver-man and Albano, 1996a,b; Silverman and Nelles,1988). This interview is most commonly administeredseparately to children and parents, and then data arecombined from both sources to derive a final “com-posite” diagnosis; however, several studies deviatedfrom this standard practice and relied solely on infor-mation obtained from parents to determine diagnosticstatus (Shortt et al., 2001; Spence et al., 2000) andtreatment outcome (Cobham et al., 1998; Flannery-Schroeder and Kendall, 2000; Kendall, 1994; Kendallet al., 1997; Shortt et al., 2001; Spence et al., 2000). Inaddition to providing a diagnosis, the ADIS requiresthe clinician to provide a clinician severity rating(CSR). The CSR is the clinician’s estimate of the de-gree of functional impairment and distress engenderedby the disorder (Albano and Silverman, 1996). Unfor-tunately, only two studies characterized the sample interms of the CSR (Hayward et al., 2000; Silverman etal., 1999a). Because the CSR may predict the natureand outcome of treatment, the failure of researchers toadequately characterize the baseline characteristics oftheir sample along this dimension is a notable defi-ciency.
Demographics and Severity. Both genders are largelyrepresented in the treated population, with only one
study containing a sample that was limited to females(Hayward et al., 2000). Although the majority of stud-ies attempted to recruit children and adolescents, theaverage age of subjects across all studies was approxi-mately 9.85 years. This leaves open the question ofgeneralizability of the research findings, as well as pro-tocol-driven interventions, to older adolescent popula-tions. Other demographic variables, such as ethnicityor socioeconomic status, were generally well docu-mented. However, with the exception of two trials (Sil-verman et al., 1999a,b), most studies had extremelylow rates of ethnic minority participation (see Pina etal. [2003] who examined the differential treatment re-sponse of Hispanic/Latino youth and European-American youth). A noted strength of the citedinvestigations was the clinical severity of the researchsample. All studies focused on subjects who soughtclinical services and whose impairment was severeenough to warrant a psychiatric diagnosis. No studyincluded children who were simply endorsing symp-toms of anxiety on a self-report measure.
Outcome Measures. To their credit, the majority ofcited investigations relied on a multimethod (e.g., clini-cal interview, self-report measures), multiinformant(e.g., child, parent, clinician) approach to documenttreatment outcomes. Both scalar and dichotomousmeasures that sampled specific symptom domains wereregularly reported. Another strength of many of thecited investigations was that outcomes were not re-stricted to the simple reporting of statistically signifi-cant symptom improvement or symptom change.More clinically informative outcomes were commonlyreported, such as clinically significant improvement(defined as changes that return deviant subjects towithin nondeviant limits [Kendall and Grove, 1988])and posttreatment diagnostic status (defined as the per-centage of children who no longer meet criteria for acurrent anxiety disorder). For instance, 14 of the 21investigations reported the posttreatment diagnosticstatus of subjects. However, the methods used to quan-tify diagnostic status varied moderately from study tostudy, which made it difficult to compare outcomesacross trials. For instance, some studies combined in-formation obtained from separate child and parentclinical interviews to determine posttreatment diagnos-tic status (Barrett, 1998; Barrett et al., 1996; Beidel etal., 2000; Last et al., 1998; Nauta et al., 2003; Silver-man et al., 1999a,b), whereas others relied solely on
COMPTON ET AL.
J . AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 43:8, AUGUST 2004940

information obtained from the parent (Cobham et al.,1998; Flannery-Schroeder and Kendall, 2000; Kendall,1994; Kendall et al., 1997; Shortt et al., 2001; Spenceet al., 2000). Moreover, some studies defined a subjectas diagnosis free if criteria for his or her primary anxietydiagnosis were no longer met (Last et al., 1998),whereas others used a more restrictive definition anddefined a subject as diagnosis free if criteria for both hisor her primary and secondary (if present) anxiety di-agnoses were no longer met (e.g., Barrett, 1998).
Moderators of Outcome. Ten of the 21 cited investi-gations reported results of secondary analyses that at-tempted to determine whether basic demographic andclinical variables moderated treatment outcome (e.g.,age, sex, ethnicity, clinical severity, pretreatment diag-nosis, comorbidities). The most frequent finding is thatnone of the variables analyzed moderate treatment out-come (for a notable exception, see Barrett et al.[1996]). However, the strength of this conclusion mustbe tempered because few studies were sufficiently pow-ered to adequately address this important question.
Long-Term Follow-up. Although the follow-up pe-riod varied widely across the cited investigations (from3 months to 6 years, with a modal length of 12months), the general conclusion that can be reached isthat CBT for anxiety disorders in children and adoles-cents is a durable intervention (Table 2). With fewexceptions (Cobham et al., 1998), posttreatment gainswere largely maintained at follow-up and showed littledeterioration. Interestingly, several studies that foundsignificant differences between two active treatmentspost-treatment reported that, at follow-up, the twotreatments were equally effective. However, because allcited studies lacked an adequate control group duringthe follow-up period, competing explanations for thepositive results reported cannot be dismissed.
Treatments
The behavioral treatment of fear and anxiety in chil-dren builds on early studies indicating that anxiety isreadily conceptualized as a set of classically conditionedresponses that can be unlearned or counterconditionedthrough associative pairing with anxiety-incompatiblestimuli and responses. For example, in systematic de-sensitization (SD), anxiety-arousing stimuli are system-atically and gradually paired (imaginally or in vivo)with competing stimuli such as food, praise, imagery,or cues generated from muscular relaxation. SD with
children consists of three basic steps: (1) training inprogressive muscle relaxation, (2) rank ordering of fear-ful situations from lowest to highest, and (3) hierarchi-cal presentation of fear stimuli via imagery while thechild is in a relaxed state (Eisen and Kearney, 1995).SD appears to work well with older children and ado-lescents. Younger children, however, often have diffi-culty with both obtaining vivid imagery and acquiringthe incompatible muscular relaxation. Strategies suchas using developmentally appropriate imagery and ad-junctive use of workbooks may boost the effectivenessof these procedures with younger children.
Without encouragement, anxious children and ado-lescents often find it difficult to remain in the presenceof anxiety-arousing stimuli for a sufficient length oftime to allow habituation to occur in the natural en-vironment. In fact, in some cases, the process of nega-tive reinforcement maintains the anxiety response.That is, when an individual initially confronts an anxi-ety-provoking situation (e.g., the assignment of an oralreport for the socially anxious youth), there is an in-crease in discomforting sensations and anxiousthoughts (e.g., rapid heart rate, sweating, thoughts suchas “I’ll look stupid to others”). By escaping or avoidingthe situation, such as through complaints of feeling illand needing to leave class or the behavior of schoolavoidance/refusal, the individual feels immediate relieffrom the anxiety. This is the process of negative rein-forcement. The escape behavior is reinforced by therelief and sets the stage for cycles of anxiety arousalfollowed by escape or avoidance and relief.
After the adult treatment literature, the identifica-tion of the negative reinforcement paradigm led to thedevelopment of exposure-based interventions for awide range of pediatric anxiety disorders. Because es-cape and avoidance behaviors are negatively reinforcedby the cessation of anxiety, exposure-based proceduresrequire extended presentation of fear stimuli with con-current prevention of escape and avoidance behaviorsin order for the extinction of the conditioned responsesto occur. Unlike systematic desensitization, stimuluspresentation is not accompanied by progressive musclerelaxation. Rather, graduated imaginal and/or in vivoexposure to hierarchically presented fear stimuli is usedto attenuate anxiety to phobic stimuli. Gradual expo-sure, with the consent of the child, is generally consid-ered to produce less stress for the client (and therapist)and thus is often preferred over the use of more pre-
RESEARCH UPDATE REVIEW: CBT
J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 43:8, AUGUST 2004 941

TA
BL
E2
Ran
dom
ized
Clin
ical
Tri
als
ofC
BT
for
Chi
ldan
dA
dole
scen
tA
nxie
tyD
isor
ders
:E
ffec
tsat
Follo
w-u
p
Aut
hor(
s)Fo
llow
-up
Cit
atio
nFo
llow
-up
Des
ign
Sam
ple
Size
Prim
ary
Dep
ende
ntM
easu
res
Tre
atm
ent
Con
diti
ons
Sam
ple
Size
(Ini
tial
/FU
)Pr
opor
tion
Res
pond
ing
FUE
BM
NN
TE
ffec
tSi
zeC
omm
ents
Bar
rett
etal
.,19
96In
orig
inal
arti
cle
12-m
oFU
(act
ive
trea
tmen
tson
ly)
EN
=79
FUN
=53
RC
MA
S,FS
SC-R
,C
BC
L,in
depe
nden
tcl
inic
ian
rati
ngs;
noan
xiet
ydx
12se
ssio
ns,
indi
vidu
alC
BT
12se
ssio
ns,
indi
vidu
alch
ildan
dpa
rent
CB
T
28/2
725
/23
19/2
722
/23
NA
NA
CB
T+
had
sign
ifica
ntly
mor
ech
ildre
ndi
agno
sis
free
,lo
wer
FSSC
-Rsc
ores
,an
dhi
gher
clin
icia
nra
ting
sof
impr
ovem
ent;
nosi
gnifi
cant
diff
eren
ceon
CB
CL;
youn
ger
child
ren
and
fem
ales
resp
onde
dbe
tter
toC
BT
+B
arre
ttet
al.,
1996
Bar
rett
etal
.,20
016-
yrFU
EN
=79
FUN
=52
RC
MA
S,FS
SC-R
,no
anxi
ety
dx12
sess
ions
,in
divi
dual
CB
T12
sess
ions
,in
divi
dual
child
and
pare
ntC
BT
28/3
1,18
/21
(inc
lude
son
lysu
bjec
tsw
hom
etdx
stat
usat
pret
reat
men
tby
child
inte
rvie
w)
24/2
818
/21
NA
NA
12-m
otr
eatm
ent
gain
sw
ere
larg
ely
mai
ntai
ned
at6-
yrFU
;co
ntra
ryto
auth
ors’
pred
icti
ons,
CB
T+
was
not
mor
eef
fect
ive
than
CB
T
Bar
rett
,19
98In
orig
inal
arti
cle
12-m
oFU
(act
ive
trea
tmen
tson
ly)
EN
=60
FUN
=di
ffic
ult
tode
term
ine
FSSC
-R,
CB
CL,
inde
pend
ent
clin
icia
nra
ting
s,no
anxi
ety
dx
12se
ssio
ns,
grou
pC
BT
(chi
ldon
ly)
12se
ssio
ns,
grou
pfa
mily
CB
T(c
hild
and
pare
nt)
Diff
icul
tto
dete
rmin
eG
CB
T=
64.5
%,
GC
BT
+=
84.8
%
NA
NA
Bot
hac
tive
trea
tmen
tgr
oups
cont
inue
dto
show
impr
ovem
ent;
nosi
gnifi
cant
diff
eren
cebe
twee
n2
acti
vetr
eatm
ents
ondi
agno
stic
stat
us;
GC
BT
+gr
oup
repo
rted
sign
ifica
ntly
low
erFS
SC-R
scor
esan
dC
BC
Lsc
ores
;G
CB
T+
rece
ived
sign
ifica
ntly
high
ercl
inic
ian
rati
ngs
ofim
prov
emen
t —co
ntin
ued
COMPTON ET AL.
J . AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 43:8, AUGUST 2004942

TA
BL
E2
cont
inue
d
Aut
hor(
s)Fo
llow
-up
Cit
atio
nFo
llow
-up
Des
ign
Sam
ple
Size
Prim
ary
Dep
ende
ntM
easu
res
Tre
atm
ent
Con
diti
ons
Sam
ple
Size
(Ini
tial
/FU
)Pr
opor
tion
Res
pond
ing
FUE
BM
NN
TE
ffec
tSi
zeC
omm
ents
Bar
rett
etal
.,19
96In
orig
inal
arti
cle
6-m
oFU
(act
ive
trea
tmen
tson
ly)
EN
=79
FUN
=53
RC
MA
S,FS
SC-R
,C
BC
L,in
depe
nden
tcl
inic
ian
rati
ngs,
noan
xiet
ydx
12se
ssio
ns,
indi
vidu
alC
BT
12se
ssio
ns,
indi
vidu
alch
ildan
dpa
rent
CB
T
28/2
825
/25
20/2
821
/25
NA
NA
Bot
hac
tive
trea
tmen
tgr
oups
cont
inue
dto
show
impr
ovem
ent;
nosi
gnifi
cant
diff
eren
cebe
twee
n2
acti
vetr
eatm
ents
ondi
agno
stic
stat
us,
RC
MA
S,FS
SC-R
,or
CB
CL
scor
es;
CB
T+
rece
ived
sign
ifica
ntly
high
ercl
inic
ian
rati
ngs
ofim
prov
emen
tB
eide
let
al.,
2000
Inor
igin
alar
ticl
e6-
mo
FUE
N=
67FU
N=
22(c
hild
ren
inth
eno
nspe
cific
trea
tmen
tco
ndit
ion
wer
eN
Afo
rFU
anal
ysis
SPA
I-C
,C
GA
S,A
DIS
-CC
SR,
noan
xiet
ydx
12in
divi
dual
and
12gr
oup
sess
ions
,C
BT
12in
divi
dual
and
12gr
oup
sess
ions
,no
nspe
cific
trea
tmen
tco
ntro
l
36/2
219
/22
NA
NA
Tre
atm
ent
gain
sw
ere
mai
ntai
ned
at6-
mo
FU
Cob
ham
etal
.,19
98In
orig
inal
arti
cle
12-m
oFU
EN
=67
FUN
=65
No
anxi
ety
dx10
sess
ions
,ch
ild-f
ocus
edgr
oup
CB
T(p
aren
tspa
rtic
ipat
ed)
10se
ssio
ns+
4pa
rent
anxi
ety
man
agem
ent
sess
ions
,gr
oup
CB
T=P
AM
(par
ents
part
icip
ated
);gr
oups
wer
eal
socr
osse
don
pare
ntal
anxi
ety
NA
Pvs
.A
P
33/3
532
/32
CB
TN
AP
=12
/16
CB
TA
P=
10/1
7C
BT
+PA
MN
AP
=12
/15
CB
T+P
AM
AP
=12
/17
NA
NA
Ove
rall,
trea
tmen
tef
fect
sw
eake
ned
by12
-mo
FU;
nosi
gnifi
cant
mai
nef
fect
for
anxi
ety
cond
itio
n(a
nxio
uspa
rent
vs.
nona
nxio
uspa
rent
);no
sign
ifica
ntm
ain
effe
ctfo
rtr
eatm
ent
cond
itio
n(C
BT
vs.
CB
T+P
AM
);no
sign
ifica
ntin
tera
ctio
nsbe
twee
npa
rent
anxi
ous
stat
usan
dtr
eatm
ent
cond
itio
n
—co
ntin
ued
RESEARCH UPDATE REVIEW: CBT
J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 43:8, AUGUST 2004 943

TA
BL
E2
cont
inue
d
Cob
ham
etal
.,19
98In
orig
inal
arti
cle
6-m
oFU
EN
=67
FUN
=66
No
anxi
ety
dx10
sess
ions
,ch
ild-f
ocus
edgr
oup
CB
T(p
aren
tspa
rtic
ipat
ed)
10se
ssio
ns+
4pa
rent
anxi
ety
man
agem
ent
sess
ions
,gr
oup
CB
T+P
AM
(par
ents
part
icip
ated
);gr
oups
wer
eal
socr
osse
don
pare
ntal
anxi
ety
NA
Pvs
.A
P
34/3
532
/32
CB
T NA
P=
14/1
6C
BT
AP
=8/
18C
BT
+PA
MN
AP
=12
/15
CB
T+P
AM
AP
=12
/17
NA
NA
Chi
ldre
nw
ith
anxi
ous
pare
nt(s
)co
ntin
ued
tore
spon
dle
ssfa
vora
bly
toch
ild-f
ocus
edC
BT
;ov
eral
l,ch
ildre
nw
ith
nona
nxio
uspa
rent
sre
spon
ded
mor
efa
vora
bly
totr
eatm
ent
rega
rdle
ssof
trea
tmen
tco
ndit
ion
Cor
nwal
let
al.,
1996
Inor
igin
alar
ticl
e3-
mo
FUE
N=
24FU
N=
24FS
SC-R
,R
CM
AS,
FT,
DFB
Q6
sess
ions
,em
otiv
eim
ager
yW
L(3
mo
indu
rati
on)
12/1
212
/12
NR
NA
FSSC
-R=
0.90
RC
MA
S=
0.79
DFB
Q=
1.82
Tre
atm
ent
gain
sin
the
acti
vetr
eatm
ent
cond
itio
nw
ere
mai
ntai
ned
at3-
mo
FU
Flan
nery
-Sc
hroe
der
& Ken
dall,
2000
Inor
igin
alar
ticl
e3-
mo
FUE
N=
45F U
N=
2 9(i
nclu
des
subj
ects
trea
ted
afte
rW
L)
RC
MA
S,C
BC
L-I,
noan
xiet
ydx
18se
ssio
ns,
indi
vidu
alC
BT
18se
ssio
ns,
grou
pC
BT
WL
(9w
k,th
enof
fere
dtr
eatm
ent)
18/1
418
/15
Prim
ary
dx:
11/1
48/
15
Any
Anx
dx:
7/14
8/15
NA
NA
Tre
atm
ent
gain
sw
ere
mai
ntai
ned
at3-
mo
FU;
nosi
gnifi
cant
diff
eren
ces
betw
een
the
two
acti
vetr
eatm
ents
onse
lf-re
port
and
pare
ntre
port
mea
sure
sH
ayw
ard
etal
.,20
00
Inor
igin
alar
ticl
e12
-mo
FUE
N=
35F U
N=
2 8A
DIS
CSR
,SP
AI
No
anxi
ety
dx16
sess
ions
,gr
oup
CB
TN
otr
eatm
ent
cont
rol
12/1
023
/18
4/10
10/1
8−6 SP
AI
=0.
07
No
sign
ifica
ntbe
twee
n-gr
oup
diff
eren
cein
rate
sof
soci
alph
obia
orSP
AI
mea
nsc
ores
at12
-mo
FU;
addi
tion
alan
alys
esco
mbi
ning
soci
alph
obia
and
depr
essi
ondi
agno
ses
prod
uced
mor
ero
bust
betw
een
grou
ptr
eatm
ent
chan
ges
Ken
dall,
1994
Inor
igin
alar
ticl
e12
-mo
FUE
N=
47F U
N=
3 8(i
nclu
des
Sstr
eate
daf
ter
WL
peri
od)
RC
MA
SFS
SC-R
CB
CL-
I
No
prim
ary
anxi
ety
dx(A
DIS
-P)
16se
ssio
ns,
indi
vidu
alC
BT
WL
(8w
k,th
enof
fere
dtr
eatm
ent)
47/3
8Pe
rcen
tdx
-fre
eno
tre
port
edN
A
NA
Tre
atm
ent
gain
sw
ere
mai
ntai
ned
at12
-mo
FUon
self-
repo
rtan
dpa
rent
repo
rtm
easu
res
—co
ntin
ued
COMPTON ET AL.
J . AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 43:8, AUGUST 2004944

TA
BL
E2
cont
inue
d
Aut
hor(
s)Fo
llow
-up
Cit
atio
nFo
llow
-up
Des
ign
Sam
ple
Size
Prim
ary
Dep
ende
ntM
easu
res
Tre
atm
ent
Con
diti
ons
Sam
ple
Size
(Ini
tial
/FU
)Pr
opor
tion
Res
pond
ing
FUE
BM
NN
TE
ffec
tSi
zeC
omm
ents
Ken
dall,
1994
Ken
dall
&So
utha
m-
Ger
ow,
1996
2–5
yrFU
EN
=47
FUN
=36
(inc
lude
sSs
trea
ted
afte
rW
Lpe
riod
)
RC
MA
SFS
SC-R
CB
CL-
I
No
prim
ary
anxi
ety
dx(A
DIS
-C)
Indi
vidu
alC
BT
47/3
6Pe
rcen
tdx
-fre
eno
tre
port
edN
A
NA
Tre
atm
ent
gain
sw
ere
larg
ely
mai
ntai
ned
atlo
ng-t
erm
FUon
self-
repo
rtan
dpa
rent
repo
rtm
easu
res
Ken
dall
etal
.,19
97In
orig
inal
arti
cle
12-m
oFU
EN
=94
FUN
=85
(inc
lude
sSs
trea
ted
afte
rW
Lpe
riod
)
RC
MA
SST
AIC
No
anxi
ety
dxby
AD
IS-P
16se
ssio
ns,
indi
vidu
alC
BT
WL
(8w
k,th
enof
fere
dtr
eatm
ent)
85/9
4Pe
rcen
tdx
free
not
repo
rted
NA
NA
Post
trea
tmen
tre
duct
ions
wer
em
aint
aine
dat
12-m
oFU
wit
hth
eex
cept
ion
that
CB
CL-
I(m
othe
r)ra
ting
sw
ere
sign
ifica
ntly
low
erK
ing
etal
.,19
98In
orig
inal
arti
cle
3-m
oFU
EN
=34
FUN
=17
(WL
not
asse
ssed
)
Scho
olat
tend
ance
(1%
days
pres
ent)
FT GA
FC
BC
L-I
6se
ssio
ns(o
ver
4w
k;pl
us5
pare
ntse
ssio
nsan
d1
teac
her
mee
ting
),in
divi
dual
CB
TW
L(4
wk,
then
offe
red
trea
tmen
t)
17/1
7N
o.w
hoac
hiev
ed90
%sc
hool
atte
ndan
ce14
/17
NA
NA
Tre
atm
ent
gain
sac
ross
all
prim
ary
outc
omes
wer
em
aint
aine
dat
3-m
oFU
Last
etal
.,19
98In
orig
inal
arti
cle
2w
kin
toth
esu
bseq
uent
scho
olye
ar
EN
=56
F UN
=4 1
%re
port
ing:
(1)
nodi
ffic
ulty
retu
rnin
gto
scho
olin
new
year
(2)
mild
diff
icul
ty(3
)m
oder
ate
diff
icul
ty(4
)ex
trem
edi
ffic
ulty
12se
ssio
ns,
indi
vidu
alC
BT
12se
ssio
ns,
indi
vidu
aled
ucat
iona
lsu
ppor
t
32/2
024
/21
CB
Tvs
.E
S(1
)40
%vs
.52
%(2
)30
%vs
.19
%(3
)10
%vs
.5%
(4)
20%
vs.
24%
NA
NA
Rou
ghly
30%
oftr
eatm
ent
com
plet
ers
inbo
thgr
oups
repo
rted
mod
erat
eto
seve
redi
ffic
ulty
retu
rnin
gto
scho
olth
efo
llow
ing
scho
olye
ar
Last
etal
.,19
98In
orig
inal
arti
cle
4-w
kFU
EN
=56
F UN
=2 9
%re
port
ing:
(1)
mai
ntai
ned
impr
ovem
ent
(2)
show
edfu
rthe
rim
prov
emen
t(3
)re
laps
ed(4
)ne
ver
impr
oved
12se
ssio
ns,
indi
vidu
alC
BT
12se
ssio
ns,
indi
vidu
aled
ucat
iona
lsu
ppor
t
32/1
424
/15
CB
Tvs
.E
S(1
)65
%vs
.40
%(2
)14
%vs
.13
%(3
)7%
vs.
7%(4
)14
%vs
.40
%
4 NA
The
maj
orit
yof
Ssco
ntin
ued
tosh
owim
prov
emen
t,w
ith
nosi
gnifi
cant
betw
een
grou
pdi
ffer
ence
sat
4-w
kFU
Men
zies
&C
lark
e,19
93
Inor
igin
alar
ticl
e12
-wk
FUE
N=
51F U
N=
3 6(W
Lno
tas
sess
ed)
BR
SPC
WP
CW
PO
R
3se
ssio
ns,
IVV
E3
sess
ions
,V
E3
sess
ions
,IV
EN
otr
eatm
ent
cont
rol
13/1
213
/12
13/1
2
NA
NA
NA
Non
sign
ifica
ntde
teri
orat
ion
intr
eatm
ent
gain
sno
ted,
IVV
Egr
oup
perf
orm
edbe
tter
than
IVE
grou
pat
FU
—co
ntin
ued
RESEARCH UPDATE REVIEW: CBT
J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 43:8, AUGUST 2004 945

TA
BL
E2
cont
inue
d
Aut
hor(
s)Fo
llow
-up
Cit
atio
nFo
llow
-up
Des
ign
Sam
ple
Size
Prim
ary
Dep
ende
ntM
easu
res
Tre
atm
ent
Con
diti
ons
Sam
ple
Size
(Ini
tial
/FU
)Pr
opor
tion
Res
pond
ing
FUE
BM
NN
TE
ffec
tSi
zeC
omm
ents
Nau
taet
al.,
2003
Inor
igin
alar
ticl
e3-
mo
FUE
N=
79FU
N=
73SC
AS-
c/p
FSSC
-RC
BC
LN
oan
xiet
ydx
12se
ssio
ns,
indi
vidu
alC
BT
12se
ssio
ns,
indi
vidu
alC
BT
plus
7se
ssio
nsC
PTW
L(d
urat
ion
not
spec
ified
,th
enof
fere
dtr
eatm
ent)
37/3
439
/39
23/3
427
/39
0 Rel
ativ
eto
CB
TSC
AS-
c=
−0.3
1SC
AS-
p=
−0.2
4FS
SC-R
=−0
.24
Bot
hac
tive
trea
tmen
tgr
oups
cont
inue
dto
show
impr
ovem
ent
acro
ssal
lpr
imar
you
tcom
esdu
ring
FUpe
riod
;th
ead
diti
onof
CPT
conf
erre
dno
addi
tion
albe
nefit
acro
ssal
lou
tcom
esSh
ortt
etal
.,20
01In
orig
inal
arti
cle
12-m
oFU
EN
=71
FUN
=63
(inc
lude
sSs
trea
ted
afte
rW
Lpe
riod
)
RC
MA
SC
BC
LN
oan
xiet
ydx
10se
ssio
ns(p
lus
2bo
oste
rse
ssio
ns),
grou
pC
BT
WL
(10
wk,
then
offe
red
trea
tmen
t)
47/6
332
/47
NA
NA
Clin
icia
nra
ting
sw
ere
mai
ntai
ned
atFU
,R
CM
AS
scor
esw
ere
sign
ifica
ntly
low
erth
anat
post
-tre
atm
ent
Silv
erm
anet
al.,
1999
a
Inor
igin
alar
ticl
e3-
,6-
,12
-mo
FU(r
esul
tsfr
omea
chFU
asse
ssm
ent
peri
odpr
esen
ted
and
anal
yzed
toge
ther
)
EN
=5 6
F UN
=3 1
(inc
lude
spo
oled
GC
BT
and
WL
data
)
RC
MA
SFS
SC-R
CB
CL-
IPG
RS
No
anxi
ety
dx
12se
ssio
ns,
grou
pC
BT
(con
curr
ent
child
and
pare
ntgr
oups
wit
h15
min
.co
njoi
ntm
eeti
ng)
WL
(8to
10w
k,th
enof
fere
dtr
eatm
ent)
3-m
oFU
=41
/31
6-m
oFU
=41
/33
12-m
oFU
=41
/25
3-m
oFU
=24
/31
6-m
oFU
=26
/33
12-m
oFU
=19
/25
NA
NA
Ove
rall
patt
ern
ofre
sults
show
eda
larg
epr
e-to
post
trea
tmen
tch
ange
follo
wed
bygr
adua
lbu
tco
ntin
ued
impr
ovem
ent
acro
ssal
lpr
imar
you
tcom
esdu
ring
FUpe
riod
Silv
erm
anet
al.,
1999
b
Inor
igin
alar
ticl
e3-
,6-
,12
-mo
FU(r
esul
tsfr
omea
chFU
asse
ssm
ent
peri
odpr
esen
ted
and
anal
yzed
toge
ther
)
EN
=10
4FU
N=
15%
unav
aila
ble
for
FUas
sess
men
ts
RC
MA
SFS
SC-R
PGR
SN
oan
xiet
ydx
10se
ssio
ns,
indi
vidu
alch
ildan
dpa
rent
SC10
sess
ions
,in
divi
dual
child
and
pare
ntC
M10
sess
ions
,in
divi
dual
child
and
pare
ntE
S
NR
bytr
eatm
ent
grou
p
NR
NA
NA
Ove
rall
patt
ern
ofre
sults
show
eda
larg
epr
e-to
post
trea
tmen
tch
ange
follo
wed
bygr
adua
lbu
tco
ntin
ued
impr
ovem
ent
acro
ssal
lpr
imar
you
tcom
esdu
ring
FUpe
riod
Spen
ce,
Don
ovan
,& B
rech
man
-Tou
ssai
nt,
2000
Inor
igin
alar
ticl
e12
-mo
FUE
N=
50F U
N=
3 6(n
umbe
rof
drop
outs
,if
any,
wer
eno
tsp
ecifi
ed)
AD
IS-P
CSR
RC
MA
SN
oan
xiet
ydx
(AD
IS-P
)
12se
ssio
ns,
child
and
pare
ntgr
oup
CB
T12
sess
ions
,ch
ildon
lygr
oup
CB
TN
otr
eatm
ent
WL
16/1
717
/19
13/1
69/
17N
A
NA
Tre
atm
ent
gain
sw
ere
larg
ely
mai
ntai
ned
at12
-mo
FUac
ross
all
prim
ary
outc
omes
;in
vest
igat
ors
mod
ified
AD
ISto
fitD
SM-I
Vcr
iter
ia;
only
pare
nts
wer
ein
terv
iew
ed;
only
phon
ein
terv
iew
sco
nduc
ted
for
post
and
follo
w-u
pas
sess
men
ts.
Res
ults
for
self-
repo
rtan
dbe
havi
oral
mea
sure
sal
sore
port
ed
—co
ntin
ued
COMPTON ET AL.
J . AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 43:8, AUGUST 2004946

scriptive techniques, especially massed exposure orflooding.
Cognitive interventions, usually combined with ex-posure, also play a prominent role in CBT for anxiouschildren and adolescents. For example, Kendall andcolleagues developed a comprehensive cognitive-behavioral protocol for anxious youth that focuses ontransmitting coping skills to children in need (Kendall,1994; Kendall et al., 1997). Based on the premise thatanxious children view the world through a “template”of threat, automatic questioning (e.g., “What if . . .”),and behavioral avoidance, treatment is focused on pro-viding educational experiences to build a new “copingtemplate” for the child. Therapists assist the children toreconceptualize anxiety-provoking situations as prob-lems to be solved and situations with which to cope. Avariety of cognitive-behavioral components assist thetherapist and child in building the coping template:relaxation training, imagery, correcting maladaptiveself-talk, problem-solving skills, and managing rein-forcers. Therapists use coping modeling, role-play re-hearsals, in vivo exposure, and a collaborativetherapeutic relationship with the child to facilitate thetreatment progress. As a rule, parents are actively in-volved in all facets of treatment as collaborators in thechange process.
For example, when significant others are trapped inthe child’s anxiety symptoms, it is crucial that they stopparticipating in or reinforcing the child’s avoidancestrategies or rituals. To test the hypothesis that addinga family anxiety management component would boosttreatment effectiveness, Barrett et al. (1996) developeda parallel family program to Kendall’s “Coping Cat”based on behavioral family intervention strategiesfound effective for the treatment of externalizing dis-orders in youth. After the completion of each childsession with the therapist, the child and parents wouldparticipate in a family anxiety management sessionwith the therapist. The crux of the program is to em-power parents and children by forming an “expertteam” to overcome and master anxiety. Parents aretrained in reinforcement strategies, with an emphasison differential reinforcement and systematic ignoringof excessive complaining and anxious behavior. How-ever, unilateral extinction strategies, such as when aparent returns the school-phobic child to school byforce, have significant disadvantages relative to consen-sual child involvement: (1) lack of a workable strategy
TA
BL
E2
cont
inue
d
Not
e:A
DIS
=A
nxie
tyD
isor
ders
Inte
rvie
wSc
hedu
le;
AD
ISC
SR=
Anx
iety
Dis
orde
rsIn
terv
iew
Sche
dule
for
Chi
ldre
n,cl
inic
ian
seve
rity
rati
ng(s
umm
ary
scor
e);
AD
IS-C
=A
nxie
tyD
isor
ders
Inte
rvie
wSc
hedu
lefo
rC
hild
ren;
AD
IS-C
CSR
=A
nxie
tyD
isor
ders
Inte
rvie
wSc
hedu
lefo
rC
hild
ren,
clin
icia
nse
veri
tyra
ting
child
base
d;A
DIS
-P=
Anx
iety
Dis
orde
rsIn
terv
iew
Sche
dule
for
Chi
ldre
n,Pa
rent
Ver
sion
;AD
IS-P
CSR
=A
nxie
tyD
isor
ders
Inte
rvie
wSc
hedu
lefo
rC
hild
ren,
clin
icia
nse
veri
tyra
ting
pare
ntba
sed;
BR
S=
Beh
avio
urR
atin
gSc
ale;
CB
CL
=C
hild
Beh
avio
rC
heck
list;
CB
CL-
I=
Chi
ldB
ehav
ior
Che
cklis
t-In
tern
aliz
ing
Subs
cale
;CB
T=
cogn
itiv
e-be
havi
oral
ther
apy;
CB
TA
P=
CB
Tw
ith
anxi
ous
pare
nt;C
BT
NA
P=
CB
Tw
ith
nona
nxio
uspa
rent
;CB
T+P
AM
=C
BT
plus
pare
ntal
anxi
ety
man
agem
ent;
CB
T+P
AM
AP
=C
BT
plus
pare
ntal
anxi
ety
man
agem
entw
ith
anxi
ous
pare
nt;C
BT
+PA
MN
AP
=C
BT
plus
pare
ntal
anxi
ety
man
agem
ent
wit
hno
nanx
ious
pare
nt;
CM
=co
ntin
genc
y-m
anag
emen
tth
erap
y;C
WP
=W
ater
Phob
iaSu
rvey
Sche
dule
,C
hild
Ver
sion
;D
FBQ
=D
arkn
ess
Fear
Beh
avio
urQ
uest
ionn
aire
;E
N=
entr
ynu
mbe
r;E
S=
educ
atio
nsu
ppor
t;FS
SC-R
=Fe
arSu
rvey
Sche
dule
for
Chi
ldre
n-R
evis
ed;
FT=
fear
ther
mom
eter
;FU
=fo
llow
-up;
FUN
=fo
llow
-up
num
ber;
GA
F=
Glo
bal
Ass
essm
ent
ofFu
ncti
onin
g;G
CB
T=
grou
pco
gnit
ive-
beha
vior
alth
erap
y;IV
E=
invi
voex
posu
re;
IVV
E=
invi
voex
posu
repl
usvi
cari
ous
expo
sure
;C
GA
S=
Chi
ldre
n’s
Glo
balA
sses
smen
tSca
le;N
A=
nota
vaila
ble;
NR
=no
trep
orte
d;O
R=
over
allr
eact
ion
toph
obic
situ
atio
n;PC
WP
=W
ater
Phob
iaSu
rvey
Sche
dule
,Par
entV
ersi
on;
PGR
S=
pare
ntgl
obal
rati
ngof
seve
rity
;RC
MA
S=
Rev
ised
Chi
ldre
n’s
Man
ifest
Anx
iety
Scal
es;S
C=
self-
cont
rolt
hera
py;S
PAI
=So
cial
Phob
iaan
dA
nxie
tyIn
vent
ory;
SPA
I-C
=So
cial
Phob
iaan
dA
nxie
tyIn
vent
ory
for
Chi
ldre
n;V
E=
vica
riou
sex
posu
re;
WL
=w
ait-
list
cont
rol.
RESEARCH UPDATE REVIEW: CBT
J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 43:8, AUGUST 2004 947

for managing the child’s distress, (2) disruption of thetreatment relationship, (3) inability to target symptomsthat are out-of-sight for parents and teachers, and (4),most important, failure to help the child internalize amore skillful strategy for coping with current and po-tential future anxiety symptomatology.
MAJOR DEPRESSION
At any one time, approximately 1 in 20 children andadolescents suffers from major depressive disorder, withrates of depression rising dramatically in adolescents,especially in girls. Although the economic burden ofdepression in youth is uncertain, the human burden isconsiderable, especially with teenage suicide. Hence, itis of critical importance to note that the empirical lit-erature is more supportive for problem-specific psycho-therapies, especially CBT, than for medicationmanagement of pediatric depressive disorders (Birma-her et al., 1996a; Hoberman et al., 1996). In particular,several controlled trials have demonstrated that indi-vidual or group administered cognitive-behavioral psy-chotherapy is an effective treatment for depressedyouth (Brent et al., 1997; Lewinsohn et al., 1994), andsome investigators now consider CBT to be the treat-ment of choice for this disorder (Reinecke et al., 1998).
Types of Investigations
Twelve articles describing a variety of cognitive-behavioral intervention packages for the treatment ofchild and adolescent depression were identified (Table3). Although these depression trials are equally meth-odologically rigorous when compared with child andadolescent anxiety trials (e.g., contrasting group designscomparing one or more active treatments with eitherno treatment, wait-list, or attention placebo controls),the number of studies is significantly fewer, and theresearch agenda to date has been less coherent andsystematic. Moreover, several of the studies with nullfindings likely had insufficient power to detect a be-tween-group treatment effect due to the small samplesize of each treatment condition. This is a notable de-ficiency and contributes to the widely held notionamong practitioners that all treatments for depressionare equally effective. It also makes it difficult, if notimpossible, to reach strong conclusions regarding thedifferential efficacy of the treatments evaluated.
Two studies addressed the question of whether add-ing a separate treatment module for parents incremen-
tally improves outcomes (Clarke et al., 1999;Lewinsohn et al., 1990). One study compared indi-vidual CBT to systemic behavioral family therapy(Brent et al., 1997). Another study evaluated the rel-evant question of whether adding CBT to usual care ina health maintenance organization is better than usualcare alone (Clarke et al., 2002). Five studies evaluatedthe efficacy of one or more CBT interventions in de-signs that included either an attention placebo condi-tion (Kahn et al., 1990; Liddle and Spence, 1990;Vostanis et al., 1996; Wood et al., 1996) or a no-treatment control (Weisz et al., 1997). One studycompared individual CBT with interpersonal psycho-therapy (Rossello and Bernal, 1999). One investigationevaluated the effects of maintenance CBT for depressedadolescents (Clarke et al., 1999). One study evaluatedthe acceptability and efficacy of a combined cognitive-behavioral family education treatment (Asarnow et al.,2002). Finally, one study evaluated the efficacy of cog-nitive bibliotherapy for adolescents with mild to mod-erate depressive symptoms (Ackerson et al., 1998). Nopublished investigations compared components oftreatments, and there were no systematic replicationstudies by independent investigators.
Assessment Issues
Diagnosis and Symptom Profile. Six of the 12 studiesused semistructured clinical interviews to identify sub-jects as having DSM major depressive disorder or dys-thymia (Brent et al., 1997; Clarke et al., 1999, 2002;Lewinsohn et al., 1990; Vostanis et al., 1996; Wood etal., 1996). The most commonly used interview was theSchedule for Affective Disorders and Schizophrenia forSchool-Age Children (Chambers et al., 1985; Orvas-chel and Puig-Antich, 1986; Puig-Antich and Cham-bers, 1978). The remaining six studies either failed tomention the specific assessment procedures used to de-termine inclusion criteria (Rossello and Bernal, 1999)or enrolled subjects solely on the basis of mild to mod-erate levels of self-reported depressive symptomatology(Ackerson et al., 1998; Asarnow et al., 2002; Kahn etal., 1990; Liddle and Spence, 1990; Weisz et al., 1997).The same six investigations that used semistructuredclinical interviews also assessed comorbidity but failedto analyze whether comorbidity status was related totreatment outcome. Thus, failure to systematically as-sess the impact of comorbidity on outcome is a criticaldeficiency in both the anxiety and depression literature.
COMPTON ET AL.
J . AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 43:8, AUGUST 2004948
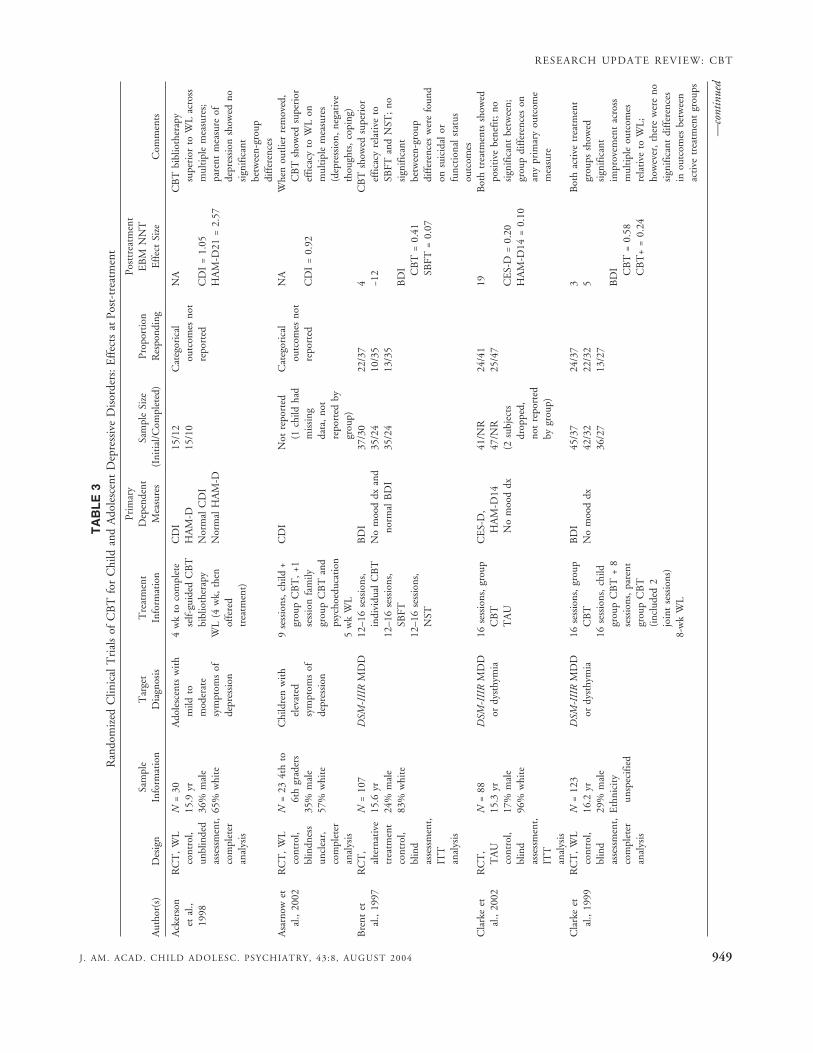
TA
BL
E3
Ran
dom
ized
Clin
ical
Tri
als
ofC
BT
for
Chi
ldan
dA
dole
scen
tD
epre
ssiv
eD
isor
ders
:E
ffec
tsat
Post
-tre
atm
ent
Aut
hor(
s)D
esig
nSa
mpl
eIn
form
atio
nT
arge
tD
iagn
osis
Tre
atm
ent
Info
rmat
ion
Prim
ary
Dep
ende
ntM
easu
res
Sam
ple
Size
(Ini
tial
/Com
plet
ed)
Prop
orti
onR
espo
ndin
g
Post
trea
tmen
tE
BM
NN
TE
ffec
tSi
zeC
omm
ents
Ack
erso
net
al.,
1998
RC
T,
WL
cont
rol,
unbl
inde
das
sess
men
t,co
mpl
eter
anal
ysis
N=
3015
.9yr
36%
mal
e65
%w
hite
Ado
lesc
ents
wit
hm
ildto
mod
erat
esy
mpt
oms
ofde
pres
sion
4w
kto
com
plet
ese
lf-gu
ided
CB
Tbi
blio
ther
apy
WL
(4w
k,th
enof
fere
dtr
eatm
ent)
CD
IH
AM
-DN
orm
alC
DI
Nor
mal
HA
M-D
15/1
215
/10
Cat
egor
ical
outc
omes
not
repo
rted
NA
CD
I=
1.05
HA
M-D
21=
2.57
CB
Tbi
blio
ther
apy
supe
rior
toW
Lac
ross
mul
tipl
em
easu
res;
pare
ntm
easu
reof
depr
essi
onsh
owed
nosi
gnifi
cant
betw
een-
grou
pdi
ffer
ence
sA
sarn
owet
al.,
2002
RC
T,
WL
cont
rol,
blin
dnes
sun
clea
r,co
mpl
eter
anal
ysis
N=
234t
hto
6th
grad
ers
35%
mal
e57
%w
hite
Chi
ldre
nw
ith
elev
ated
sym
ptom
sof
depr
essi
on
9se
ssio
ns,
child
+gr
oup
CB
T,
+1se
ssio
nfa
mily
grou
pC
BT
and
psyc
hoed
ucat
ion
5w
kW
L
CD
IN
otre
port
ed(1
child
had
mis
sing
data
,no
tre
port
edby
grou
p)
Cat
egor
ical
outc
omes
not
repo
rted
NA
CD
I=
0.92
Whe
nou
tlier
rem
oved
,C
BT
show
edsu
peri
oref
ficac
yto
WL
onm
ulti
ple
mea
sure
s(d
epre
ssio
n,ne
gati
veth
ough
ts,
copi
ng)
Bre
ntet
al.,
1997
RC
T,
alte
rnat
ive
trea
tmen
tco
ntro
l,bl
ind
asse
ssm
ent,
ITT
anal
ysis
N=
107
15.6
yr24
%m
ale
83%
whi
te
DSM
-III
RM
DD
12–1
6se
ssio
ns,
indi
vidu
alC
BT
12–1
6se
ssio
ns,
SBFT
12–1
6se
ssio
ns,
NST
BD
IN
om
ood
dxan
dno
rmal
BD
I
37/3
035
/24
35/2
4
22/3
710
/35
13/3
5
4 −12
BD
I CB
T=
0.41
SBFT
=0.
07
CB
Tsh
owed
supe
rior
effic
acy
rela
tive
toSB
FTan
dN
ST;
nosi
gnifi
cant
betw
een-
grou
pdi
ffer
ence
sw
ere
foun
don
suic
idal
orfu
ncti
onal
stat
usou
tcom
esC
lark
eet
al.,
2002
RC
T,
TA
Uco
ntro
l,bl
ind
asse
ssm
ent,
ITT
anal
ysis
N=
8 815
.3yr
17%
mal
e96
%w
hite
DSM
-III
RM
DD
ordy
sthy
mia
16se
ssio
ns,
grou
pC
BT
TA
U
CE
S-D
,H
AM
-D14
No
moo
ddx
41/N
R47
/NR
(2su
bjec
tsdr
oppe
d,no
tre
port
edby
grou
p)
24/4
125
/47
19 CE
S-D
=0.
20H
AM
-D14
=0.
10
Bot
htr
eatm
ents
show
edpo
siti
vebe
nefit
;no
sign
ifica
ntbe
twee
n;gr
oup
diff
eren
ces
onan
ypr
imar
you
tcom
em
easu
re
Cla
rke
etal
.,19
99R
CT
,W
Lco
ntro
l,bl
ind
asse
ssm
ent,
com
plet
eran
alys
is
N=
123
16.2
yr29
%m
ale
Eth
nici
tyun
spec
ified
DSM
-III
RM
DD
ordy
sthy
mia
16se
ssio
ns,
grou
pC
BT
16se
ssio
ns,
child
grou
pC
BT
+8
sess
ions
,pa
rent
grou
pC
BT
(inc
lude
d2
join
tse
ssio
ns)
8-w
kW
L
BD
IN
om
ood
dx45
/37
42/3
236
/27
24/3
722
/32
13/2
7
3 5 BD
I CB
T=
0.58
CB
T+
=0.
24
Bot
hac
tive
trea
tmen
tgr
oups
show
edsi
gnifi
cant
impr
ovem
ent
acro
ssm
ulti
ple
outc
omes
rela
tive
toW
L;ho
wev
er,
ther
ew
ere
nosi
gnifi
cant
diff
eren
ces
inou
tcom
esbe
twee
nac
tive
trea
tmen
tgr
oups
—co
ntin
ued
RESEARCH UPDATE REVIEW: CBT
J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 43:8, AUGUST 2004 949

TA
BL
E3
cont
inue
d
Aut
hor(
s)D
esig
nSa
mpl
eIn
form
atio
nT
arge
tD
iagn
osis
Tre
atm
ent
Info
rmat
ion
Prim
ary
Dep
ende
ntM
easu
res
Sam
ple
Size
(Ini
tial
/Com
plet
ed)
Prop
orti
onR
espo
ndin
g
Post
trea
tmen
tE
BM
NN
TE
ffec
tSi
zeC
omm
ents
Kah
net
al.,
1990
RC
T,
WL
cont
rol,
blin
dnes
sun
clea
r,co
mpl
eter
anal
ysis
N=
6812
.1yr
49%
mal
eE
thni
city
unsp
ecifi
ed
Chi
ldre
nw
ith
mod
erat
eto
seve
resy
mpt
oms
ofde
pres
sion
12se
ssio
ns,
grou
pC
BT
12se
ssio
ns,
indi
vidu
alR
T12
sess
ions
,in
divi
dual
SM10
-wk
WL
CD
IN
orm
alC
DI
17/1
717
/17
17/1
717
/17
15/1
713
/17
10/1
72/
17
1 2 2 CD
I CB
T=
1.68
RT
=1.
06SM
=1.
11
All
trea
tmen
tsre
lati
veto
WL
show
edsi
gnifi
cant
decr
ease
insy
mpt
oms
ofde
pres
sion
;ve
rysm
all
sam
ple
size
s
Lew
inso
hnet
al.,
1990
RC
T,
WL
cont
rol,
blin
dnes
sun
clea
r,co
mpl
eter
anal
ysis
N=
6916
.2yr
39%
mal
eE
thni
city
unsp
ecifi
ed
DSM
-III
MD
D,
min
orde
pres
sion
,or
inte
rmit
tent
depr
essi
on
14se
ssio
ns,
grou
pC
BT
14se
ssio
ns,
child
grou
pC
BT
+8
sess
ions
,pa
rent
grou
pC
BT
(inc
lude
d2
join
tse
ssio
ns)
7to
8-w
kW
L
BD
IN
om
ood
dx24
/21
21/1
924
/19
9/21
9/19
1/19
3 1 BD
I CB
T=
0.94
CB
T+
=1.
48
Bot
hac
tive
trea
tmen
tgr
oups
show
edsi
gnifi
cant
impr
ovem
ent
acro
ssm
ulti
ple
outc
omes
rela
tive
toW
L;ho
wev
er,
ther
ew
ere
nosi
gnifi
cant
diff
eren
ces
inou
tcom
esbe
twee
nac
tive
trea
tmen
tgr
oups
Lidd
le&
Spen
ce,
1990
RC
T,
notr
eatm
ent
cont
rol
and
atte
ntio
npl
aceb
oco
ntro
l,co
mpl
eter
anal
ysis
N=
3 19.
2yr
68%
mal
eE
thni
city
unsp
ecifi
ed
Chi
ldre
nw
ith
mild
tom
oder
ate
sym
ptom
sof
depr
essi
on
8se
ssio
ns,
grou
pC
BT
8se
ssio
ns,
grou
pA
PCN
TC
CD
I11
/11
10/1
010
/10
Cat
egor
ical
outc
omes
not
repo
rted
NA
CD
I CB
Tvs
.A
PC=
0.71
CB
Tvs
.N
TC
=0.
36
All
trea
tmen
tsas
soci
ated
wit
ha
sign
ifica
ntde
clin
ein
sym
ptom
sof
depr
essi
on;
very
smal
lsa
mpl
esi
zes
Ros
sello
&B
erna
l,19
99
RC
T,
WL
cont
rol,
blin
dnes
sun
clea
r,co
mpl
eter
anal
ysis
N=
7 114
.7yr
46%
mal
e10
0%La
tino
DSM
-III
RM
DD
ordy
sthy
mia
12se
ssio
ns,
indi
vidu
alC
BT
12se
ssio
ns,
indi
vidu
alIP
T12
-wk
WL
(the
nof
fere
dtr
eatm
ent)
CD
I25
/21
23/1
912
/18
15/2
117
/19
12/1
8(b
ased
onC
DI
cuto
ffpo
ints
)
10 4 CD
I CB
T=
0.35
IPT
=0.
76
Bot
hac
tive
trea
tmen
tgr
oups
show
edpo
siti
vebe
nefit
rela
tive
toW
L;no
sign
ifica
ntdi
ffer
ence
sin
outc
omes
betw
een
acti
vetr
eatm
ent
grou
psV
osta
nis,
Feeh
an,
Gra
ttan
,& B
icke
rton
,19
96
RC
T,
alte
rnat
ive
trea
tmen
tco
ntro
l,bl
indn
ess
uncl
ear,
com
plet
eran
alys
is
N=
5 712
.7yr
44%
mal
e88
%w
hite
DSM
-III
RM
DD
9se
ssio
ns,
indi
vidu
alC
BT
9se
ssio
ns,
indi
vidu
alN
FI
MFQ
-CN
om
ood
dx29
/29
28/2
825
/29
21/2
89 M
FQ=
0.05
Bot
hgr
oups
show
edsi
gnifi
cant
impr
ovem
ent;
alth
ough
MFQ
show
eda
tren
dfa
vori
ngth
eC
BT
cond
itio
n,no
sign
ifica
ntbe
twee
n-gr
oup
diff
eren
ces
wer
efo
und
oncl
inic
alou
tcom
es
—co
ntin
ued
COMPTON ET AL.
J . AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 43:8, AUGUST 2004950

TA
BL
E3
cont
inue
d
Aut
hor(
s)D
esig
nSa
mpl
eIn
form
atio
nT
arge
tD
iagn
osis
Tre
atm
ent
Info
rmat
ion
Prim
ary
Dep
ende
ntM
easu
res
Sam
ple
Size
(Ini
tial
/Com
plet
ed)
Prop
orti
onR
espo
ndin
g
Post
trea
tmen
tE
BM
NN
TE
ffec
tSi
zeC
omm
ents
Wei
sz,
Thu
rber
,Sw
eene
y,Pr
offit
t,& Le
Gag
noux
,19
97
RC
T,
notr
eatm
ent
cont
rol,
blin
das
sess
men
t,co
mpl
eter
anal
ysis
N=
489.
6yr
old
51%
mal
e38
%w
hite
Chi
ldre
nw
ith
mild
tom
oder
ate
sym
ptom
sof
depr
essi
on
8se
ssio
ns,
grou
pC
BT
NT
C
CD
IC
DR
S-R
16/1
632
/32
8/16
5/32
3 CD
I=
0.48
CD
RS-
R=
0.16
Chi
ldre
nin
the
acti
vetr
eatm
ent
grou
pre
port
edsi
gnifi
cant
lyfe
wer
sym
ptom
sof
depr
essi
on
Woo
d,H
arri
ngto
n,& M
oore
,19
96
RC
T,
alte
rnat
ive
trea
tmen
tco
ntro
l,bl
ind
asse
ssm
ent,
ITT
anal
ysis
N=
5 314
.2yr
31%
mal
eE
thni
city
unsp
ecifi
ed
DSM
-III
RM
DD
5–8
sess
ions
indi
vidu
alC
BT
5–8
sess
ions
RT
MFQ
-CM
FQ-P
No
moo
ddx
26/2
427
/24
13/2
45/
243 M
FQ-P
=0.
41C
BT
was
asso
ciat
edw
ith
sign
ifica
ntly
mor
eim
prov
emen
tac
ross
mul
tipl
eou
tcom
es
Not
e:A
PC=
atte
ntio
npl
aceb
oco
ntro
l;B
DI
=B
eck
Dep
ress
ion
Inve
ntor
y;C
BT
=co
gnit
ive-
beha
vior
alth
erap
y;C
DI
=C
hild
ren’
sD
epre
ssio
nIn
vent
ory;
CD
RS-
R=
Chi
ldre
n’s
Dep
ress
ion
Rat
ing
Scal
e-R
evis
ed;
CE
S-D
=C
ente
rfo
rE
pide
mio
logi
cSt
udie
s-D
epre
ssio
nSc
ale;
HA
M-D
14=
14-I
tem
Ham
ilton
Dep
ress
ion
Rat
ing
Scal
e;H
AM
-D21
=21
-Ite
mH
amilt
onD
epre
ssio
nR
atin
gSc
ale;
IPT
=in
terp
erso
nalp
sych
othe
rapy
; IT
T=
inte
ntto
trea
t;M
DD
=m
ajor
depr
essi
vedi
sord
er;M
FQ=
Moo
dan
dFe
elin
gsQ
uest
ionn
aire
;MFQ
-C=
Moo
dan
dFe
elin
gsQ
uest
ionn
aire
,Chi
ldV
ersi
on;M
FQ-P
=M
ood
and
Feel
ings
Que
stio
nnai
re,P
aren
tVer
sion
;NA
=no
tava
ilabl
e;N
FI=
nonf
ocus
edin
terv
enti
on;N
R=
notr
epor
ted;
NST
=no
ndir
ecti
vesu
ppor
tive
ther
apy;
NT
C=
no-t
reat
men
tco
ntro
l;R
CT
=ra
ndom
ized
clin
ical
tria
l;R
T=
rela
xati
ontr
aini
ng;
SBFT
=sy
stem
icbe
havi
orfa
mily
ther
apy;
SM=
self-
mod
elin
g;T
AU
=tr
eatm
ent
asus
ual;
WL
=w
ait-
list
cont
rol.
RESEARCH UPDATE REVIEW: CBT
J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 43:8, AUGUST 2004 951

Demographics. Although both males and females arerepresented in the treated populations, other basic de-mographic variables, such as ethnicity, were generallynot well documented. Only 7 of the 12 cited investi-gations provided the ethnic breakdown of the sample.Moreover, the majority of children who have partici-pated in research studies to date have been overwhelm-ingly white, suggesting that future studies will beneeded to evaluate the exportability of protocol-drivenCBT treatment packages to divergent patient popula-tions.
Outcome Measures. All the cited investigations reliedon psychometrically sound measures to documenttreatment results and changes in specific symptom do-mains. One-half of the studies reported the percentageof subjects who no longer met criteria for a depressivedisorder after treatment (Brent et al., 1997; Clarke etal., 1999, 2002; Lewinsohn et al., 1990; Vostanis et al.,1996; Wood et al., 1996), and several studies reportedthe percentage of subjects who returned to the nonde-viant ranges on the primary outcome measures. Onlythree investigations provided quantitative measures ofchange in functional status (Brent et al., 1997; Clarkeet al., 1999, 2002). Because little is currently knownabout how treatments affect academic, social, and fam-ily domains, future studies would benefit from includ-ing a more diverse range of outcomes (Compton et al.,2002).
Long-Term Follow-up. The data addressing the du-rability of CBT for adolescent depression are mixed(Table 4). In general, studies characterized by a rela-tively short follow-up period (from 1 to 9 months)report that posttreatment gains are largely maintained,with several studies showing continued improvement.However, studies with longer follow-up periods (from9 months to 2 years) and low attrition rates at follow-up found that a sizable percentage of subjects contin-ued to report significant depressive symptoms or arecurrence of their depressive illness (Birmaher et al.,2000; Vostanis et al., 1996, 1998; Wood et al., 1996).Factors found to predict a lack of recovery or relapseinclude low self-esteem (Vostanis et al., 1996, 1998),comorbidity at post-treatment (Vostanis et al., 1998),severity of depression or high level of functional im-pairment at baseline (Birmaher et al., 2000), the pres-ence of subsyndromal depression (Brent et al., 2001),parental depression (Brent et al., 1998; Clarke et al.,2002), parent–child conflict (Birmaher et al., 2000),
and the source of treatment referral (Birmaher et al.,2000). These studies suggest that depression in adoles-cence is associated with a high risk of recurrence. Theyalso underscore the importance of developing interven-tions that specifically target adolescents at risk of re-lapse and investigate the impact of continuationtreatment on long-term outcomes.
Treatments
Like other cognitive-behavioral treatment packages,CBT for depression in youths is a present-oriented,skills-based treatment that, in this case, is based on theassumption that depression is either caused or main-tained by the way one perceives situations and events(e.g., cognitions about the world and self) and the pres-ence of skill deficits (both emotional and behavioral)that prevent the patient from interacting effectivelywith the world. Because personality is an interactivemultidirectional system of cognitions, behaviors, andemotions, depression is manifested in each of the threecomponents of the personality. However, CBT for de-pression assumes that symptom change is most likely tooccur through interventions that modify patterns ofbehavior through skills acquisition and patterns of cog-nition, with changes in depressed mood following inturn. Among the behavioral and cognitive skill deficitsthat may characterize a depressed youth are low levelsof involvement in pleasant activities, poor problem-solving and assertion skills, cognitive distortions thatnegatively bias perceptions, negative automaticthoughts, negative views of self and future, and failureto attribute positive outcomes to internal, stable, orglobal causes. The role of the therapist, therefore, is toestablish a collaborative working relationship with theadolescent and to help the adolescent learn new ways ofbehaving and thinking, which in turn reduces depres-sive severity and risk of relapse.
Current cognitive-behavioral treatment packagesfor depressed youths share two salient characteristics:(1) general and “required” skill building sessions andoptional “modular” sessions for specific problems and(2) the integration of parent and family sessions withindividual CBT (Treatment for Adolescents with De-pression Study, 2003). Treatment is generally designedto improve the teenager’s problem-solving abilitywhen faced with a stressful situation, for example,parent–child conflict, role transitions, grief reactions,or peer problems. Therefore, the required aspects of
COMPTON ET AL.
J . AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 43:8, AUGUST 2004952

TA
BL
E4
Ran
dom
ized
Clli
nica
lT
rial
sof
CB
Tfo
rC
hild
and
Ado
lesc
ent
Dep
ress
ive
Dis
orde
rs:
Eff
ects
atFo
llow
-up
Aut
hor(
s)Fo
llow
-up
Cit
atio
nFo
llow
-up
Des
ign
Tar
get
Dia
gnos
es
Prim
ary
Dep
ende
ntM
easu
res
Tre
atm
ent
Con
diti
ons
Sam
ple
Size
(Ini
tial
/FU
)Pr
opor
tion
Res
pond
ing
Follo
w-u
pE
BM
NN
TE
ffec
tSi
zeC
omm
ents
Ack
erso
net
al.,
1998
Inor
igin
alar
ticl
e1-
mo
FUA
dole
scen
tsw
ith
mild
tom
oder
ate
sym
ptom
sof
depr
essi
on
CD
IH
AM
-D21
Nor
mal
CD
IN
orm
alH
AM
-D21
4w
kto
com
plet
ese
lf-gu
ided
CB
Tbi
blio
ther
apy
4-w
kW
L
15/1
215
/10
NA
NA
The
imm
edia
te-t
reat
men
tgr
oup
cont
inue
dto
show
impr
ovem
ent
inde
pres
sive
sym
ptom
son
the
HA
M-D
;tr
eatm
ent
gain
son
CD
Iw
ere
mai
ntai
ned
Bre
ntet
al.,
1997
Bir
mah
eret
al.,
2000
24-m
oFU
(mul
tipl
ein
terv
iew
s)
DSM
-III
RM
DD
BD
IN
om
ood
dxan
dno
rmal
BD
I
12–1
6se
ssio
ns,
indi
vidu
alC
BT
12–1
6se
ssio
ns,
SBFT
12–1
6se
ssio
ns,
NST
37/N
R35
/NR
35/N
R
97%
ofsa
mpl
eco
mpl
eted
atle
ast
3FU in
terv
iew
s
Not
sepa
rate
dby
grou
pIn
suff
icie
ntda
tapr
ovid
edO
ver
FUpe
riod
,th
e3
trea
tmen
tgr
oups
did
not
sign
ifica
ntly
diff
erin
term
sof
rem
issi
on,
reco
very
,re
laps
e,or
recu
rren
ce,
alth
ough
desc
ript
ive
data
favo
red
CB
T;
acro
ssgr
oups
,39
%of
pati
ents
had
pers
iste
ntre
cove
ryfr
omde
pres
sion
,40
%ha
din
term
itte
ntde
pres
sion
sym
ptom
s,an
d21
%w
ere
pers
iste
ntly
depr
esse
dC
lark
eet
al.,
2002
Inor
igin
alar
ticl
e12
-mo
FUD
SM-I
IIR
MD
Dor
dyst
hym
ia
CE
S-D
HA
M-D
14N
om
ood
dx
16se
ssio
ns,
grou
pC
BT
TA
U
41/N
R47
/NR
(6su
bjec
tsdr
oppe
d,no
tre
port
edby
grou
p)
71%
82%
Insu
ffic
ient
data
prov
ided
Bot
htr
eatm
ent
grou
psco
ntin
ued
tosh
owm
aint
enan
ceof
trea
tmen
tga
ins,
wit
hno
sign
ifica
ntbe
twee
n-gr
oup
diff
eren
ces
onm
ain
outc
omes
Cla
rke
etal
.,20
02In
orig
inal
arti
cle
24-m
oFU
DSM
-III
RM
DD
ordy
sthy
mia
CE
S-D
,H
AM
-D14
No
moo
ddx
16se
ssio
ns,
grou
pC
BT
TA
U
41/N
R47
/NR
(13
subj
ects
drop
ped,
not
repo
rted
bygr
oup)
89%
92%
Insu
ffic
ient
data
prov
ided
Bot
htr
eatm
ent
grou
psco
ntin
ued
tosh
owm
aint
enan
ceof
trea
tmen
tga
ins,
wit
hno
sign
ifica
ntbe
twee
n-gr
oup
diff
eren
ces
onm
ain
outc
omes
—co
ntin
ued
RESEARCH UPDATE REVIEW: CBT
J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 43:8, AUGUST 2004 953

TA
BL
E4
cont
inue
d
Aut
hor(
s)Fo
llow
-up
Cit
atio
nFo
llow
-up
Des
ign
Tar
get
Dia
gnos
es
Prim
ary
Dep
ende
ntM
easu
res
Tre
atm
ent
Con
diti
ons
Sam
ple
Size
(ini
tial
/FU
)Pr
opor
tion
Res
pond
ing
Follo
w-u
pE
BM
NN
TE
ffec
tSi
zeC
omm
ents
Cla
rke,
Roh
de,
Lew
inso
hn,
Hop
s,&
Seel
ey,
1999
Inor
igin
alar
ticl
e12
-an
d24
-mo
FUto
addr
ess
ques
tion
ofre
cove
ryfr
oman
dre
curr
ence
ofde
pres
sion
epis
ode
DSM
-III
AR
MD
Dor
dyst
hym
ia
BD
IN
om
ood
dxSu
bjec
tsin
the
2ac
tive
trea
tmen
tco
ndit
ions
wer
era
ndom
lyas
sign
edto
:(1
)bo
oste
rse
ssio
nsev
ery
4m
o(2
)as
sess
men
ton
lyse
ssio
nsev
ery
4m
o(3
)as
sess
men
ton
lyse
ssio
nsev
ery
12m
o
24 16 24 (87
subj
ects
orig
inal
lyra
ndom
ized
toac
ute
trea
tmen
t,64
subj
ects
rand
omiz
eddu
ring
follo
w-u
pph
ase)
NA
NA
By
12-m
oFU
, 100
%of
subj
ects
who
wer
est
illde
pres
sed
atpo
st-t
reat
men
tan
das
signe
dto
the
boos
ter
cond
ition
had
reco
vere
dvs
.50%
ofth
ose
subj
ects
inth
e2
asse
ssm
ent-
only
cond
ition
s;ho
wev
er,a
t24
-mo
FU,r
ates
conv
erge
dw
ith10
0%of
subj
ects
inth
ebo
oste
rco
nditi
onre
cove
red
vs.
90%
inth
e2
asse
ssm
ent-
only
cond
ition
sB
y12
-mo
FU,r
ecur
renc
era
tes
wer
e14
%in
the
12-m
oas
sess
men
t-on
lyco
nditi
on,0
%in
the
4-m
oas
sess
men
t-on
lyco
nditi
on,a
nd27
%in
the
boos
ter
cond
ition
;at
24-m
oFU
,rec
urre
nce
rate
sw
ere
23%
inth
e12
-mo
asse
ssm
ent-
only
cond
ition
,0%
inth
e4-
mo
asse
ssm
ent-
only
cond
ition
,and
36%
inth
ebo
oste
rco
nditi
onLe
win
sohn
,C
lark
e,H
ops,
&A
ndre
ws,
1990
Inor
igin
alar
ticle
6-,1
2-,2
4-m
oFU
DSM
-III
MD
D,
min
orde
pres
sion,
orin
term
itten
tde
pres
sion
BD
I14
sess
ions
grou
pC
BT
14se
ssio
ns,c
hild
grou
pC
BT
plus
8se
ssio
ns,
pare
ntgr
oup
CB
T(in
clud
ed2
join
tse
ssio
ns)
(WL
subj
ects
wer
eof
fere
dtr
eatm
ent
imm
edia
tely
follo
win
gpo
st-t
reat
men
t)
At
24m
onth
s24
/10
21/1
3
NR
bytr
eatm
ent
cond
ition
NA
Bot
hac
tive
trea
tmen
tgr
oups
show
edco
ntin
ued
impr
ovem
ent
durin
gFU
resu
lting
ina
signi
fican
tdi
ffere
nce
betw
een
post
trea
tmen
tan
d6-
mo
FUsc
ores
;im
prov
emen
tsw
ere
mai
ntai
ned
atth
e12
-an
d24
-mo
asse
ssm
ents
—co
ntin
ued
COMPTON ET AL.
J . AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 43:8, AUGUST 2004954

TA
BL
E4
cont
inue
d
Aut
hor(
s)Fo
llow
-up
Cit
atio
nFo
llow
-up
Des
ign
Tar
get
Dia
gnos
es
Prim
ary
Dep
ende
ntM
easu
res
Tre
atm
ent
Con
diti
ons
Sam
ple
Size
(ini
tial
/FU
)Pr
opor
tion
Res
pond
ing
Follo
w-u
pE
BM
NN
TE
ffec
tSi
zeC
omm
ents
Lidd
le&
Spen
ce,
1990
Inor
igin
alar
ticl
e2-
mo
FUC
hild
ren
wit
hm
ildto
mod
erat
esy
mpt
oms
ofde
pres
sion
CD
I8
sess
ions
,gr
oup
CB
T8
sess
ions
,gr
oup
APC
NT
C
11/1
110
/10
10/1
0
Cat
egor
ical
outc
omes
not
repo
rted
NA
CD
I CB
Tvs
.A
PC=
0.41
CB
Tvs
.N
TC
=0.
20
All
trea
tmen
tgr
oups
show
edco
ntin
ued
impr
ovem
ent
at2-
mo
FU,
wit
hno
sign
ifica
ntbe
twee
n-gr
oup
diff
eren
ces
Ros
sello
&B
erna
l,19
99
Inor
igin
alar
ticl
e3-
mo
FUD
SM-I
IIR
MD
Dor
dyst
hym
ia
CD
I12
sess
ions
,in
divi
dual
CB
T12
sess
ions
,in
divi
dual
IPT
12-w
kW
L(t
hen
offe
red
trea
tmen
t)
25/1
423
/11
NR
NA
Tre
atm
ent
grai
nsw
ere
mai
ntai
ned
at3-
mo
FU;
nosi
gnifi
cant
betw
een-
grou
pdi
ffer
ence
sin
3-m
oou
tcom
esbe
twee
nth
e2
acti
vetr
eatm
ent
grou
psV
osta
nis,
Feeh
an,
Gra
ttan
,& B
icke
rton
,19
96b
Vos
tani
s,Fe
ehan
,G
ratt
an,
& Bic
kert
on,
1996
a
9-m
oFU
DSM
-III
RM
DD
MFQ
-CN
om
ood
dx9
sess
ions
,in
divi
dual
CB
T9
sess
ions
,in
divi
dual
NFI
29/2
828
/28
20/2
821
/28
−28
MFQ
-C=
−0.0
3
Tre
atm
ent
gain
sw
ere
mai
ntai
ned
inbo
thtr
eatm
ent
grou
psat
9-m
oFU
;ho
wev
er,
27%
ofth
esa
mpl
em
etcr
iter
iafo
rM
DD
and
45%
repo
rted
sign
ifica
ntde
pres
sive
sym
ptom
sdu
ring
the
prev
ious
9-m
ope
riod
;lo
wse
lf-es
teem
pred
icte
dlo
ng-t
erm
outc
ome
Vos
tani
set
al.,
1996
b
Vos
tani
s,Fe
ehan
,& G
ratt
an,
1998
2-yr
FUD
SM-I
IIR
MD
DM
FQ-C
No
moo
ddx
9se
ssio
ns,
indi
vidu
alC
BT
9se
ssio
ns,
indi
vidu
alN
FI
29/2
728
/27
20/2
723
/27
−9 MFQ
-C=
−0.3
6
Ove
rall,
trea
tmen
tga
ins
wer
em
aint
aine
din
both
trea
tmen
tgr
oups
at2-
yrFU
;ho
wev
er,
20%
ofsa
mpl
em
etcr
iter
iafo
rM
DD
and
39%
repo
rted
sign
ifica
ntde
pres
sive
sym
ptom
sdu
ring
the
prev
ious
year
;lo
wse
lf-es
teem
cont
inue
dto
pred
ict
long
-ter
mou
tcom
e
—co
ntin
ued
RESEARCH UPDATE REVIEW: CBT
J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 43:8, AUGUST 2004 955

TA
BL
E4
cont
inue
d
Aut
hor(
s)Fo
llow
-up
Cit
atio
nFo
llow
-up
Des
ign
Tar
get
Dia
gnos
es
Prim
ary
Dep
ende
ntM
easu
res
Tre
atm
ent
Con
diti
ons
Sam
ple
Size
(ini
tial
/FU
)Pr
opor
tion
Res
pond
ing
Follo
w-u
pE
BM
NN
TE
ffec
tSi
zeC
omm
ents
Wei
szet
al.,
1997
Inor
igin
alar
ticl
e9-
mo
FUC
hild
ren
wit
hm
ildto
mod
erat
esy
mpt
oms
ofde
pres
sion
CD
IC
DR
S-R
8se
ssio
ns,
grou
pC
BT
NT
C
60.4
%of
the
orig
inal
sam
ple
avai
labl
efo
rFU
(not
repo
rted
bygr
oup)
NA
NA
Inge
nera
l,tr
eatm
ent
gain
sw
ere
mai
ntai
ned
over
the
9-m
oFU
;m
ore
child
ren
inth
etr
eatm
ent
grou
pm
oved
into
the
norm
alra
nge
onth
eC
DI
and
CD
RS-
RW
ood
etal
.,19
96In
orig
inal
arti
cle
6-m
oFU
DSM
-III
RM
DD
MFQ
-C,
MFQ
-PN
om
ood
dx5–
8se
ssio
nsin
divi
dual
CB
T5–
8se
ssio
nsR
T
26/2
127
/22
14/2
116
/22
−16.
5
MFQ
-P=
0.14
Post
trea
tmen
tdi
ffer
ence
sbe
twee
nC
BT
and
RT
wer
ere
duce
dby
6-m
oFU
;du
ring
FUpe
riod
,R
Tgr
oup
cont
inue
dto
impr
ove
acro
ssm
ulti
ple
outc
omes
Not
e:A
PC=
atte
ntio
npl
aceb
oco
ntro
l;B
DI
=B
eck
Dep
ress
ion
Inve
ntor
y;C
BT
=co
gnit
ive-
beha
vior
alth
erap
y;C
DI
=C
hild
ren’
sD
epre
ssio
nIn
vent
ory;
CD
RS-
R=
Rev
ised
Chi
ldre
n’s
Dep
ress
ion
Rat
ing
Scal
e;C
ES-
D=
Cen
ter
for
Epi
dem
iolo
gic
Stud
ies-
Dep
ress
ion
Scal
e;FU
=fo
llow
-up;
HA
M-D
14=
14-I
tem
Ham
ilton
Dep
ress
ion
Rat
ing
Scal
e;H
AM
-D
21=
21-I
tem
Ham
ilton
Dep
ress
ion
Rat
ing
Scal
e;IP
T=
inte
rper
sona
lpsy
chot
hera
py;M
DD
=m
ajor
depr
essi
vedi
sord
er;M
FQ-C
=M
ood
and
Feel
ings
Que
stio
nnai
re,C
hild
Ver
sion
;M
FQ-P
=M
ood
and
Feel
ings
Que
stio
nnai
re,P
aren
tV
ersi
on;N
A=
not
avai
labl
e;N
FI=
nonf
ocus
edin
terv
enti
on;N
R=
not
repo
rted
;NST
=no
ndir
ecti
vesu
ppor
tive
ther
apy;
NT
C=
no-t
reat
men
tco
ntro
l;R
T=
rela
xati
ontr
aini
ng;
SBFT
=sy
stem
icbe
havi
orfa
mily
ther
apy;
TA
U=
trea
tmen
tas
usua
l;W
L=
wai
t-lis
tco
ntro
l.
COMPTON ET AL.
J . AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 43:8, AUGUST 2004956

treatment include psychoeducation about depressionand its causes, goal setting with the adolescent, andgeneral problem-solving skills. Modules, chosen jointlyby the therapist and adolescent, then address thespecific skill deficits of the teenager. Because parent–child conflict is both a risk factor for depression andpredictive of poor treatment outcome and relapse, in-cluding a parent component in CBT is justified on anad hoc basis. Moreover, evidence is beginning toemerge that combined child and parent treatment maybe more effective than treatment directed at the teen-ager alone (Lewinsohn et al., 1990). In addition toteaching contingency management procedures, parentsare provided with alternative, effective methods for par-enting and creating a more positive family environ-ment. Furthermore, family interactions are targeteddirectly to shape and reinforce effective communica-tion and to increase pleasant activities and positive af-fect.
DISCUSSION
A substantial evidence base supports the efficacy ofproblem-specific cognitive-behavioral interventions fora variety of childhood and adolescent anxiety and de-pressive disorders. Unlike other psychotherapeutictechniques that have been applied to these disorders,CBT is consistent with an EBM perspective that valuesempirically supported problem-focused treatments.CBT presents a logical theoretical framework to guidepractitioners through an idiographic assessment of spe-cific problem domains, the delivery of problem-specifictreatment interventions, and well-specified outcomesto monitor treatment progress. However, CBT is notsimplistic. Helping children, adolescents, and parentsmake rapid and difficult behavior change over shorttime intervals requires considerable expertise and train-ing.
Future research in the areas of childhood and ado-lescent anxiety and depressive disorders will need tofocus on the following areas. First, controlled trialscomparing medications, CBT, and their combinationare needed to determine whether combined treatmentprovides an additive benefit in terms symptom reduc-tion. Second, treatment-dismantling studies are neededto identify the relative contributions of specific CBTcomponents to symptom reduction and treatment ac-ceptability. Third, mediational analyses (how a treat-
ment works) are needed to refine treatmentinterventions and better understand the mechanism(s)through which treatments achieve their therapeutic ef-fect. Fourth, follow-up studies with adequate controlgroups will be necessary to evaluate the long-term ben-efit of CBT, including examining whether boosterCBT sessions reduce relapse rates and whether inter-vening in childhood prevents the onset of adult psy-chiatric disorders. Finally, studies with diverse patientpopulations are needed to evaluate the exportabilityand generalizability of currently available protocol-driven treatments.
Disclosure: Dr. March receives consulting fees from Solvay, Pfizer,GSKI, Wyeth-Ayerst, and BMS and serves as Scientific Advisor forShire and Pfizer and DSMB Chair for the Organon Study. He hasfinancial relationships with MultiHealth Systems for the Multidimen-sional Anxiety Scale for Children.
REFERENCES
Ackerson J, Scogin F, McKendree-Smith N, Lyman RD (1998), Cognitivebibliotherapy for mild and moderate adolescent depressive symptom-atology. J Consult Clin Psychol 66:685–690
Albano AM, Silverman WK (1996), Clinician’s Guide to the Anxiety Disor-ders Interview Schedule for DSM-IV, Child Version. Boulder, CO: Gray-wind Publications
Andreason N (1997), Linking mind and brain in the study of mentalillnesses: a project for a scientific psychopathology. Science 275:1586–1598
Asarnow JR, Scott CV, Mintz J (2002), A combined cognitive-behavioralfamily education intervention for depression in children: a treatmentdevelopment study. Cognit Ther Res 26:221–229
Barlow DH (1993), On the relation of clinical research to clinical practice:current issues, new directions. In: Issues in Clinical Psychology: The Re-lationship Between the Scientist and the Practitioner, Mindell J, ed. Du-buque, IA: Wm. C. Brown, pp 11–35
Barrett PM (1998), Evaluation of cognitive-behavioral group treatments forchildhood anxiety disorders. J Clin Child Psychol 27:459–468
Barrett PM, Dadds MR, Rapee RM (1996), Family treatment of childhoodanxiety: a controlled trial. J Consult Clin Psychol 64:333–342
Barrett PM, Duffy AL, Dadds MR, Rapee RM (2001), Cognitive-behavioral treatment of anxiety disorders in children: long-term (6-year)follow-up. J Consult Clin Psychol 69:135–141
Beidel DC, Turner SM, Morris TL (2000), Behavioral treatment of child-hood social phobia. J Consult Clin Psychol 68:1072–1080
Bernstein GA, Shaw K (1997), Practice parameters for the assessment andtreatment of children and adolescents with anxiety disorders. J Am AcadChild Adolesc Psychiatry 36:69S–84S
Birmaher B, Brent DA, Kolko D et al. (2000), Clinical outcome aftershort-term psychotherapy for adolescents with major depressive disor-der. Arch Gen Psychiatry 57:29–36
Birmaher B, Ryan ND, Williamson DE, Brent DA, Kaufman J (1996a),Childhood and adolescent depression: a review of the past 10 years. PartII. J Am Acad Child Adolesc Psychiatry 35:1575–1583
Birmaher B, Ryan ND, Williamson DE et al. (1996b), Childhood andadolescent depression: a review of the past 10 years. Part I. J Am AcadChild Adolesc Psychiatry 35:1427–1439
Brent DA, Birmaher B, Kolko D, Baugher M, Bridge J (2001), Subsyn-
RESEARCH UPDATE REVIEW: CBT
J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 43:8, AUGUST 2004 957

dromal depression in adolescents after a brief psychotherapy trial: courseand outcome. J Affect Disord 63:51–58
Brent DA, Holder D, Kolko D et al. (1997), A clinical psychotherapy trialfor adolescent depression comparing cognitive, family, and supportivetherapy. Arch Gen Psychiatry 54:877–885
Brent DA, Kolko DJ, Birmaher B et al. (1998), Predictors of treatmentefficacy in a clinical trial of three psychosocial treatments for adolescentdepression. J Am Acad Child Adolesc Psychiatry 37:906–914
Chambers WJ, Puig-Antich J, Hirsch M et al. (1985), The assessment ofaffective disorders in children and adolescents by semistructured inter-view. Test-retest reliability of the schedule for affective disorders andschizophrenia for school-age children, present episode version. Arch GenPsychiatry 42:696–702
Clarke G, Lewinsohn P, Hops H (1990), Instructor’s Manual for the Ado-lescent Coping With Depression Course, 4th ed. Eugene, OR: Castalia Press
Clarke GN, Hornbrook M, Lynch F et al. (2002), Group cognitive-behavioral treatment for depressed adolescent offspring of depressedparents in a health maintenance organization. J Am Acad Child AdolescPsychiatry 41:305–313
Clarke GN, Rohde P, Lewinsohn PM, Hops H, Seeley JR (1999), Cogni-tive-behavioral treatment of adolescent depression: efficacy of acutegroup treatment and booster sessions. J Am Acad Child Adolesc Psychiatry38:272–279
Cobham VE, Dadds MR, Spence SH (1998), The role of parental anxietyin the treatment of childhood anxiety. J Consult Clin Psychol 66:893–905
Cohen J, March J, Berliner L (2000), Treatment of PTSD in Children andAdolescents. In: Effective Treatments for PTSD, Foa E, Davidson J,Keane T, eds. New York: Guilford, pp 106–138
Compton SN, Burns BJ, Egger HL, Robertson E (2002), Review of theevidence base for treatment of childhood psychopathology: internalizingdisorders. J Consult Clin Psychol 70:1240–1266
Cornwall E, Spence SH, Schotte D (1996), The effectiveness of emotiveimagery in the treatment of darkness phobia in children. Behav Change13:223–229
Curry JF, Reinecke MA (2003), Modular therapy for adolescents withmajor depression. In: Cognitive Therapy With Children and Adolescents:A Casebook for Clinical Practice, 2nd ed., Reinecke MA, Dattilio FM etal., eds. New York: Guilford, pp 95–128
Eisen A, Kearney C (1995), Treating Fear and Anxiety in Children andAdolescents. Northvale, NJ: Jason Aronson
Flannery-Schroeder EC, Kendall PC (2000), Group and individual cogni-tive-behavioral treatments for youth with anxiety disorders: a random-ized clinical trial. Cognit Ther Res 24:251–278
Franklin ME, Rynn M, March JS, Foa EB (2002), Obsessive-compulsivedisorder. In: Clinical Behavior Therapy: Adults and Children, Hersen M,ed. New York: Wiley, pp 276–303
Geddes J, Reynolds S, Streiner D, Szatmari P (1997), Evidence basedpractice in mental health [editorial]. BMJ 315:1483–1484
Guyatt GH, Sackett DL, Cook DJ (1993), Users’ guides to the medicalliterature. II. How to use an article about therapy or prevention. A. Arethe results of the study valid? Evidence-Based Medicine WorkingGroup. JAMA 270:2598–2601
Guyatt GH, Sackett DL, Cook DJ (1994), Users’ guides to the medicalliterature. II. How to use an article about therapy or prevention. B.What were the results and will they help me in caring for my patients?Evidence-Based Medicine Working Group. JAMA 271:59–63
Guyatt GH, Sinclair J, Cook DJ, Glasziou P (1999), Users’ guides to themedical literature: XVI. How to use a treatment recommendation. Evi-dence-Based Medicine Working Group and the Cochrane ApplicabilityMethods Working Group. JAMA 281:1836–1843
Haynes SN, O’Brien WH (1990), Functional analysis in behavior therapy.Clin Psychol Rev 10:649–668
Hayward C, Varady S, Albano AM, Thienemann M, Henderson L,Schatzberg AF (2000), Cognitive-behavioral group therapy for socialphobia in female adolescents: results of a pilot study. J Am Acad ChildAdolesc Psychiatry 39:721–726
Hibbs E, Jensen P (1996), Psychosocial Treatments for Child and AdolescentDisorders Washington, DC: American Psychological Press
Hoberman HM, Clarke GN, Saunders SM (1996), Psychosocial interven-tions for adolescent depression: issues, evidence, and future directions.Prog Behav Modif 30:25–73
Hyman SE (2000), The millennium of mind, brain, and behavior. Arch GenPsychiatry 57:88–89
Kahn JS, Kehle TJ, Jenson WR, Clark E (1990), Comparison of cognitive-behavioral, relaxation, and self-modeling interventions for depressionamong middle-school students. School Psychol Rev 19:196–211
Kendall P (1993), Guiding theory for therapy with children and adoles-cents. In: Child and Adolescent Therapy, Kendall P, ed. New York:Guilford, pp 3–22
Kendall PC (1994), Treating anxiety disorders in children: results of arandomized clinical trial. J Consult Clin Psychol 62:100–110
Kendall PC, Aschenbrand SG, Hudson JL (2003), Child-focused treatmentof anxiety. In: Evidence-Based Psychotherapies for Children and Adoles-cents, Kazdin AE, ed. New York: Guilford, pp 81–100
Kendall PC, Chu BC, Pimentel SS, Choudhury M (2000), Treating anxietydisorders in youth. In: Child and Adolescent Therapy: Cognitive-Behavioral Procedures, 2nd ed. Kendall PC, ed. New York: Guilford, pp235–287
Kendall PC, Flannery-Schroeder E, Panichelli-Mindel SM, Southam-Gerow M (1997), Therapy for youths with anxiety disorders: a secondrandomized clinical trial. J Consult Clin Psychol 65:366–380
Kendall PC, Grove WM (1988), Normative comparisons in therapy out-come. Behav Assess 10:147–158
Kendall PC, Krain A, Treadwell KR (1999), Generalized anxiety disorder.In: Handbook of Prescriptive Treatments for Children and Adolescents, 2nded. Ammerman RT, Hersen M, Last CG, eds. Boston: Allyn and Bacon,pp 155–171
Kendall PC, Panichelli-Mindel SM (1995), Cognitive-behavioral treat-ments. J Abnorm Child Psychol 23:107–124
Kendall PC, Southam-Gerow MA (1996), Long-term follow-up of a cog-nitive-behavioral therapy for anxiety-disordered youth. J Consult ClinPsychol 64:724–730
King NJ, Tonge BJ, Heyne D et al. (1998), Cognitive-behavioral treatmentof school-refusing children: a controlled evaluation. J Am Acad ChildAdolesc Psychiatry 37:395–403
Last CG, Hansen C, Franco N (1998), Cognitive-behavioral treatment ofschool phobia. J Am Acad Child Adolesc Psychiatry 37:404–411
Lewinsohn P, Clarke GN, Rohde P (1994), Psychological Approaches to theTreatment of Depression in Adolescents. New York: Plenum
Lewinsohn PM, Clarke GN, Hops H, Andrews JA (1990), Cognitive-behavioral treatment for depressed adolescents. Behav Ther 21:385–401
Liddle B, Spence SH (1990), Cognitive-behaviour therapy with depressedprimary school children: a cautionary note. Behav Psychother 18:85–102
Manassis K, Mendlowitz SL, Scapillato D et al. (2002), Group and indi-vidual cognitive-behavioral therapy for childhood anxiety disorders. Arandomized trial. J Am Acad Child Adolesc Psychiatry 41:1423–1430
March J, Mulle K (1998), OCD in Children and Adolescents: A Cognitive-Behavioral Treatment Manual. New York: Guilford
March J, Wells K (2003), Combining medication and psychotherapy. In:Pediatric Psychopharmacology: Principles and Practice, Martin A, ScahillL, Charney DS, Leckman JF, eds. London: Oxford University Press, pp426–446
March JS (1995), Cognitive-behavioral psychotherapy for children and ado-lescents with OCD: a review and recommendations for treatment. J AmAcad Child Adolesc Psychiatry 34:7–18
McClellan J, Werry J (1997), Practice parameters for the assessment andtreatment of children and adolescents with bipolar disorder. J Am AcadChild Adolesc Psychiatry 36:157S–176S
Mendlowitz SL, Manassis K, Bradley S, Scapillato D, Miezitis S, Shaw BF(1999), Cognitive-behavioral group treatments in childhood anxietydisorders: the role of parental involvement. J Am Acad Child AdolescPsychiatry 38:1223–1229
Menzies RG, Clarke J (1993), A comparison of in vivo and vicarious exposurein the treatment of childhood water phobia. Behav Res Ther 31:9–15
Muris P, Mayer B, Bartelds E, Tierney S, Bogie N (2001), The revised
COMPTON ET AL.
J . AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 43:8, AUGUST 2004958

version of the Screen for Child Anxiety Related Emotional Disorders(SCARED-R): treatment sensitivity in an early intervention trial forchildhood anxiety disorders. Br J Clin Psychol 40:323–336
Muris P, Meesters C, van Melick M (2002), Treatment of childhood anxi-ety disorders; A preliminary comparison between cognitive-behavioralgroup therapy and a psychological placebo intervention. J Behav TherExp Psychiatry 33:143–158
Nauta MH, Scholing A, Emmelkamp PM, Minderaa RB (2003), Cogni-tive-behavioral therapy for children with anxiety disorders in a clinicalsetting: no additional effect of a cognitive parent training. J Am AcadChild Adolesc Psychiatry 42:1270–1278
Orvaschel H, Puig-Antich J (1986), Schedule for Affective Disorders andSchizophrenia for School-Age Children, Epidemiologic Version. Pittsburgh:Western Psychiatric Institute and Clinic
Pina AA, Silverman WK, Fuentes RM, Kurtines WM, Weems CF (2003),Exposure-based cognitive-behavioral treatment for phobic and anxietydisorders: treatment effects and maintenance for Hispanic/Latino rela-tive to European-American youths. J Am Acad Child Adolesc Psychiatry42:1179–1187
Puig-Antich J, Chambers W (1978), The Schedule for Affective Disorders andSchizophrenia for School-Aged Children. New York: New York StatePsychiatric Institute
Rapee R, Spense S, Cobham V, Wignal A (2000), Helping Your AnxiousChild: A Step-By-Step Guide for Parents. San Francisco: New Harbinger
Reinecke MA, Dattilio FM, Freeman A (2003), What makes for an effectivetreatment? In: Cognitive Therapy With Children and Adolescents: A Case-book for Clinical Practice, 2nd ed. Reinecke MA, Dattilio FM, FreemanA, eds. New York: Guilford, pp 1–18
Reinecke MA, Ryan NE, DuBois DL (1998), Cognitive-behavioral therapyof depression and depressive symptoms during adolescence: a review andmeta-analysis. J Am Acad Child Adolesc Psychiatry 37:26–34
Rossello J, Bernal G (1999), The efficacy of cognitive-behavioral and in-terpersonal treatments for depression in Puerto Rican adolescents.J Consult Clin Psychol 67:734–745
Rutter M (1999), The Emanuel Miller Memorial Lecture 1998. Autism:two-way interplay between research and clinical work. J Child PsycholPsychiatry 40:169–188
Sackett D, Richardson W, Rosenberg W, Haynes B (1997), Evidence-BasedMedicine. London: Churchill Livingstone
Sackett D, Richardson W, Rosenberg W, Haynes B (2000), Evidence-BasedMedicine, 2nd ed. London: Churchill Livingstone
Shadish WR, Robinson L, Congxiao L (1999), ES: A Computer Program forEffect Size Calculation, 1.0 ed. St. Paul, MN: Assessment Systems
Shortt AL, Barrett PM, Fox TL (2001), Evaluating the FRIENDS Program:a cognitive-behavioral group treatment for anxious children and theirparents. J Clin Child Psychol 30:525–535
Silverman W, Kurtines W (1996), Anxiety and Phobic Disorders: A Prag-matic Approach. New York: Plenum
Silverman WK (1987), Anxiety Disorders Interview Schedule for Children.Boulder, CO: Graywind Publications
Silverman WK, Albano AM (1996a), The Anxiety Disorders InterviewSchedule for DSM-IV: Child Interview Schedule. Boulder, CO: Graywind
Silverman WK, Albano AM (1996b), The Anxiety Disorders InterviewSchedule for DSM-IV: Parent Interview Schedule. Boulder, CO: Gray-wind
Silverman WK, Kurtines WM, Ginsburg GS, Weems CF, Lumpkin PW,Carmichael DH (1999a), Treating anxiety disorders in children withgroup cognitive-behavioral therapy: a randomized clinical trial. J ConsultClin Psychol 67:995–1003
Silverman WK, Kurtines WM, Ginsburg GS, Weems CF, Rabian B, Se-rafini LT (1999b), Contingency management, self-control, and educa-tion support in the treatment of childhood phobic disorders: a random-ized clinical trial. J Consult Clin Psychol 67:675–687
Silverman WK, Nelles WB (1988), The Anxiety Disorders Interview Sched-ule for Children. J Am Acad Child Adolesc Psychiatry 27:772–778
Spence SH, Donovan C, Brechman-Toussaint M (2000), The treatment ofchildhood social phobia: the effectiveness of a social skills training-based, cognitive-behavioural intervention, with and without parentalinvolvement. J Child Psychol Psychiatry 41:713–726
Thyer BA (1991), Diagnosis and treatment of child and adolescent anxietydisorders. Behav Modif 15:310–325
Treatment for Adolescents with Depression Study (2003), Treatment forAdolescents with Depression Study (TADS): rationale, design, andmethods. J Am Acad Child Adolesc Psychiatry 42:531–542
Van Hasselt V, Hersen M (1993), Handbook of Behavior Therapy and Phar-macotherapy for Children. Boston: Longwood
Vostanis P, Feehan C, Grattan E (1998), Two-year outcome of childrentreated for depression. Eur Child Adolesc Psychiatry 7:12–18
Vostanis P, Feehan C, Grattan E, Bickerton W-L (1996b), Treatment forchildren and adolescents with depression: lessons from a controlled trial.Clin Child Psychol Psychiatry 1:199–212
Vostanis P, Feehan C, Grattan E, Bickerton W-L (1996a), A randomisedcontrolled out-patient trial of cognitive-behavioural treatment for chil-dren and adolescents with depression: 9-month follow-up. J Affect Dis-ord 40:105–116
Weisz JR, Thurber CA, Sweeney L, Proffitt VD, LeGagnoux GL (1997),Brief treatment of mild-to-moderate child depression using primary andsecondary control enhancement training. J Consult Clin Psychol 65:703–707
Wood A, Harrington R, Moore A (1996), Controlled trial of a brief cog-nitive-behavioural intervention in adolescent patients with depressivedisorders. J Child Psychol Psychiatry 37:737–746
RESEARCH UPDATE REVIEW: CBT
J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 43:8, AUGUST 2004 959