coding medicare update 2018 - palm beach county medical society medicare update... ·...
TRANSCRIPT
Presented by:
Jean Acevedo, LHRM, CPC, CHC, CENTC,AAPC Fellow
Acevedo Consulting Incorporated
Coding and Medicare Part B Update: 2018
Palm Beach County Medical SocietyJanuary 10, 2018
© Acevedo Consulting Incorporated 2016
About the Presenter Jean Acevedo, LHRM, CPC, CHC, CENTC has over 30 years of health care experience. She has a particular expertise in chart audits, compliance & education relative to physician documentation and coding. Jean has also been an expert witness in civil litigation and an investigative consultant for the DOJ and FBI in Federal fraud cases.Jean has demonstrated particular expertise in otolaryngology, rheumatology, therapy and rehabilitation documentation and coding and is well known for her knowledge of hospice and palliative care physician services billing. Recognizing physician reimbursement is moving from a pure “fee for service” model to one reimbursing for quality and value, she is helping ACOs and their physicians understand the rules and nuances of diagnosis coding and the impact on Medicare Risk Adjustment (MRA) coding.Jean is an instructor at Florida Atlantic University where she teaches the regulatory compliance modules of FAU’s Certificate in Medical Business Management program, and a member of several Coding Institute Editorial Advisory Boards. Jean has been a Participant in CMS’ Medicare Provider Feedback Group, CMS Division of Provider Information Planning and Development since 2007 and is a member of the Jurisdiction 9 MAC’s Provider Outreach and Education Advisory Group. She is a frequently sought after speaker as she possesses the unique perspective of avoiding risk and liability while optimizing reimbursement in the highly regulated health care industry.
Today’s Speaker:
Jean AcevedoLHRM, CPC, CHC, CENTC,
AAPC FellowPresident & Senior Consultant
© Acevedo Consulting Incorporated 2016
DisclaimerThe information enclosed was current at the time it was presented. Medicare and other payer policies change frequently. This presentation was prepared as a tool to assist providers and is not intended to grant rights or impose obligations.
Although every reasonable effort has been made to assure the accuracy of the information within these pages, the ultimate responsibility for your organization’s financial health, the correct submission of claims and response to any remittance advice lies with the provider of services. Acevedo Consulting Inc. employees, agents, and staff make no representation, warranty, or guarantee that this compilation of information is error‐free and will bear no responsibility or liability for the results or consequences of the use of this information.
This presentation is a general summary that explains certain aspects of the Medicare Program and other reimbursement and compliance information, but is not a legal document. The official Medicare Program provisions are contained in the relevant laws, regulations, and rulings.
SPECIAL NOTE: This content is based on the 2018 MPFS Rule; attendees should rely on information from the Rule and other forthcoming guidance from CMS as well as current CPT®, HCPCS and ICD‐10‐CM code books before implementing any of the material discussed here.

© Acevedo Consulting Incorporated 2016
Agenda
• Coding Highlights for 2018• ICD‐10‐CM Reminders• CPT & HCPCS Changes – Some Highlights
• Global Surgery Post Op Reporting• Transition to digital x‐rays• New Medicare Numbers• Billing dually eligible Medicare/Medicaid beneficiaries• Appropriate Use Criteria for Advanced Imaging• Medicare Audits and Risk Areas• And more….

5
Coding Highlights for 2018
© Acevedo Consulting Incorporated 2016
ICD‐10‐CM
• Check guidelines• Clarifications and changes• Check your 2018 ICD‐10 book
• Does it contain 2017 guidelines?
https://www.cdc.gov/nchs/data/icd/10cmguidelines_fy2018_final.pdf
6
© Acevedo Consulting Incorporated 2016
ICD‐10‐CM
Guidelines Worth Repeating….• Signs and Symptoms
• Codes that describe symptoms and signs, as opposed to diagnoses, are acceptable for reporting purposes when a related definitive diagnosis has not been established (confirmed) by the provider.
• Signs and symptoms that are associated routinely with a disease process should not be assigned as additional codes, unless otherwise instructed by the classification
• Additional signs and symptoms that may not be associated routinely with a disease process should be coded when present.
7
© Acevedo Consulting Incorporated 2016
ICD‐10‐CMGuidelines Worth Repeating….• Reporting Additional Diagnoses
• For reporting purposes the definition for “other diagnoses” is interpreted as additional conditions that affect patient care in terms of requiring: • clinical evaluation; or • therapeutic treatment; or • diagnostic procedures; or • extended length of hospital stay; or• increased nursing care and/or monitoring
8
Do not report an incidental finding on a diagnostic test, patient reported (but unverified) symptom, or other condition that does not impact the doctor’s treatment nor meet any of the above criteria.

9
CPT® and HCPCS 2018
© Acevedo Consulting Incorporated 2016
CPT: Hospital Observation Services
10
• Codes 99217, 99218, 99219, and 99220 have been revised by adding the term “outpatient hospital” in front of “observation status” in the code descriptor. This revision affects only the description of the site of service.
• Reminder: only the physician/NPP who initiates the observation care reports these codes• Other physicians/NPPs providing observation
encounters should report office/other outpatient visit codes (99201‐99215).

© Acevedo Consulting Incorporated 2016
CPT: Prolonged Services
11
Revisions to 99354‐99357 (Face‐to‐face prolonged services):• Inclusion of 90487 [Family psychotherapy
(conjoint psychotherapy) (with patient present), 50 minutes)]
• Added to the list of “do not report” codes:• 99483 (new code for cognitive assessment and
care plan services)
© Acevedo Consulting Incorporated 2016
CPT: Cognitive Assessment and Care Plan Services
12
99483 “Assessment of and care planning for a patient with cognitive impairment requiring an independent historian, in the office or other outpatient, home or domiciliary or rest home, with all of the following required elements:” “Do not report…if any of the required elements are not performed or are deemed unnecessary for the patient’s condition.”

© Acevedo Consulting Incorporated 2016
CPT: Cognitive Assessment and Care Plan Services
13
The required elements of 99483: Cognition‐focused evaluation including a pertinent H&P Medical decision making of moderate or high complexity Functional assessment, including decision‐making capacity Use of standardized instruments for staging of dementia (eg, FAST, clinical dementia rating Medication reconciliation and review for high‐risk medications Evaluation for neuropsychiatric and behavioral symptoms, including depression, including use of standardized screening instrument Evaluation of safety (eg, home), including motor vehicle operation ID of caregiver(s), caregiver knowledge, caregiver needs, social supports, and the willingness of caregiver to take on caregiving tasks Development, updating or revision, or review of an Advance Care Plan, Creation of a written care plan, including initial plans to address any neuropsychiatric symptoms, neurocognitive symptoms, functional limitations and referral to community resources as needed shared w/the patient and/or caregiver with initial education and support

© Acevedo Consulting Incorporated 2016
CPT: Cognitive Assessment and Care Plan Services
14
Not to be billed with another E&M code Replaces G0505 2017 temporary HCPCS code
99483 Reimbursement Typically, 50 minutes are spent F2F with the patient and/or family or caregiver. Allowable –$246.88 (FL Locale 3)
Compare this to 99215 Typically, 40 minutes are spent F2F w/the patient $151.41 (FL Locale 3)
© Acevedo Consulting Incorporated 2016
CPT: Cognitive Assessment and Care Plan Services
15
99484 “Care management services for behavioral health conditions, at least 20 minutes of clinical staff time, directed by a physician or other qualified health care professional, per calendar month, w/the following required elements Initial assessment or follow‐up monitoring, including use of applicable validated rating scales; Behavioral health care planning in relation to behavioral/psychiatric health problems, including revision for patients who are not progressing or whose status changes;
Facilitating and coordinating treatment such as psychotherapy, pharmacotherapy, counseling and/or psychiatric consultation; and
Continuity of care with a designated member of the care team. Allowable – Locale 3, Florida – $49.68 Chronic care management for the cognitively impaired
The practice’s Alzheimer’s, dementia and similar patients. Any other E&M services, including other care management services, may be reported during the same period as long as activities used to meet criteria for another reported service do not count toward meeting criteria for 99484.
© Acevedo Consulting Incorporated 2016
CPT: Cognitive Assessment and Care Plan Services
16
99484 Clinical Example: A 50‐year old female established patient presents with complaints of fatigue and sleep disturbance following the recent loss of her spouse. The primary care physician diagnoses the patient with a behavioral health disorder and recommends that the patient receive behavioral health care management as part of the treatment. Description: Direction and general supervision of care management services are provided for behavioral health conditions, which are generally provided by clinical staff. Management and/or coordination of services are provided and overseen, as needed, for all medical conditions, psychosocial needs, and activities of daily living.
© Acevedo Consulting Incorporated 2016
CPT: Anesthesia
17
5 codes deleted due to low utilization:0074000810011800119001682
© Acevedo Consulting Incorporated 2016
CPT: Anesthesia
18
5 codes added: 00731 – anesthesia for upper GI endoscopic procedure, endoscope introduced proximal to duodenum• 00732 ‐ …ERCP• 00811 – Anesthesia for lower intestinal endoscopic procedures, endoscope introduced distal to duodenum
• 00812 ‐ …screening colonoscopy• Deductible and coinsurance waived for Medicare patients• Note: Per CPT report 00812 for any screening colonoscopy regardless of ultimate findings• Note Per CMS: When a screening colonoscopy becomes a diagnostic colonoscopy…report 00811..with the PT modifier…Medicare will…waive only the deductible when submitted with the PT modifier. (MLN Matters MM10181)
• ‐PT ‐ Colorectal cancer screening test; converted to diagnostic test or other procedure

© Acevedo Consulting Incorporated 2016
CPT: Anesthesia
19
5 codes added, cont’d:• 00813 – Anesthesia for combined upper and lower GI endoscopic procedures, endoscope introduced both proximal and distal to the duodenum.Previously, the additional work for patients undergoing both upper & lower endoscopic procedures was not captured (repositioning, responding to physiologic changes, other nonduplicative work involved in the additional procedure).
© Acevedo Consulting Incorporated 2016
CPT: Surgery Code Changes
20
• Integumentary• Musculoskeletal• Respiratory – sinus endoscopy• Cardiovascular
• Heart/Lung Transplantation• Endovascular Repair• Vascular Injections
• Esophagus• Male and Female Genitalia
© Acevedo Consulting Incorporated 2016
CPT: Respiratory – Sinus Endoscopy Highlights
21
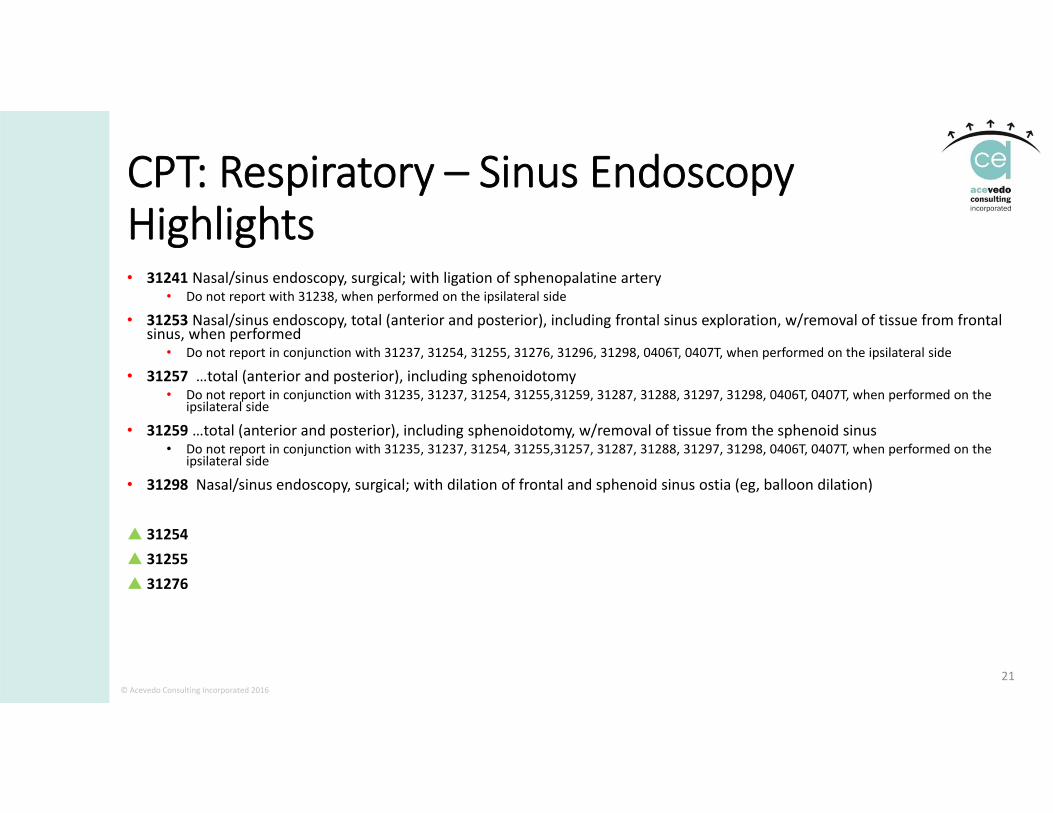
• 31241 Nasal/sinus endoscopy, surgical; with ligation of sphenopalatine artery• Do not report with 31238, when performed on the ipsilateral side
• 31253 Nasal/sinus endoscopy, total (anterior and posterior), including frontal sinus exploration, w/removal of tissue from frontal sinus, when performed
• Do not report in conjunction with 31237, 31254, 31255, 31276, 31296, 31298, 0406T, 0407T, when performed on the ipsilateral side
• 31257 …total (anterior and posterior), including sphenoidotomy• Do not report in conjunction with 31235, 31237, 31254, 31255,31259, 31287, 31288, 31297, 31298, 0406T, 0407T, when performed on the
ipsilateral side
• 31259 …total (anterior and posterior), including sphenoidotomy, w/removal of tissue from the sphenoid sinus• Do not report in conjunction with 31235, 31237, 31254, 31255,31257, 31287, 31288, 31297, 31298, 0406T, 0407T, when performed on the
ipsilateral side
• 31298 Nasal/sinus endoscopy, surgical; with dilation of frontal and sphenoid sinus ostia (eg, balloon dilation)
31254 31255 31276
© Acevedo Consulting Incorporated 2016
CPT: Respiratory – Sinus Endoscopy Code Changes – Why, per the AMA
22
AMA RUC survey identified the current code family as being potentially misvalued. “It was determined that adding and revising these codes would provide a solution to the family of surgical endoscopic services.”
Result: 31241 may be reported for a nasal/sinus endoscopy w/ligation of sphenopalatine artery. 31254 is revised to a parent code with four codes in its family. This new family of codes
(31254, 31255, 31253, 31257, 31259) should be used to report surgical nasal endoscopies with ethmoidectomy (partial, anterior and posterior, including frontal sinus exploration; with sphenoidotomy; and sphenoidotomy, with removal of tissue from the sphenoid sinus).
Guidelines referencing codes 31231‐31235 have been revised to provide instruction on the use of modifier 52 or modifier 53 depending on the circumstances of the examination “To report these services when all of the elements are not fully examined (eg, judged not
clinically pertinent), or because the clinical situation precludes such exam (eg, technically unable, altered anatomy), append modifier 52 if repeat examination is not planned, or modifier 53 if repeat examination is planned.”
© Acevedo Consulting Incorporated 2016
CPT: Cardiovascular Heart/Lung Transplantation• Category III codes 0051T, 0052T, 0053T, which were used for reporting artificial heart system procedures, have been deleted and replaced by Category I codes to reflect standard practice
• 33927 – Implantation of a total replacement heart system (artificial heart) with recipient cardiectomy
• 33928 – Removal and replacement of total replacement heart system• 33929 – Removal of a total replacement heart system for heart transplantation (list separately in addition to code for primary procedure)
23

© Acevedo Consulting Incorporated 2016
CPT: Endovascular Repair of Abdominal Aorta and/or Iliac Arteries• Major revisions to interpretive guidelines and codes due to AMA RUC findings that many of the 34800‐34806, 34825 and 34826 codes were being billed together frequently. The entire family of codes has been revised to reflect current practice and to bundle services that are frequently performed together
• 34800‐34806, 34825 and 34826 codes are deleted• Sixteen new codes (34701‐34716)• Four related codes (34812, 34820, 34833, 34834) have been revised
24
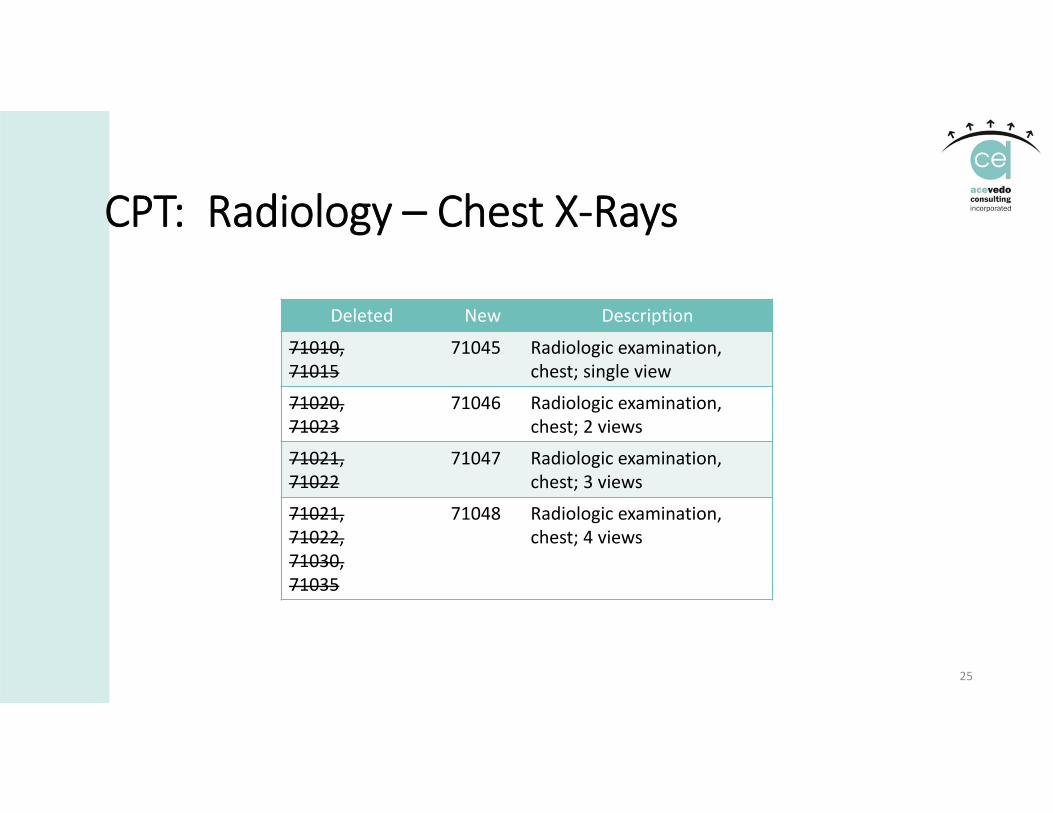
CPT: Radiology – Chest X‐Rays
25
Deleted New Description
71010,71015
71045 Radiologic examination, chest; single view
71020, 71023
71046 Radiologic examination,chest; 2 views
71021, 71022
71047 Radiologic examination, chest; 3 views
71021, 71022, 71030, 71035
71048 Radiologic examination, chest; 4 views
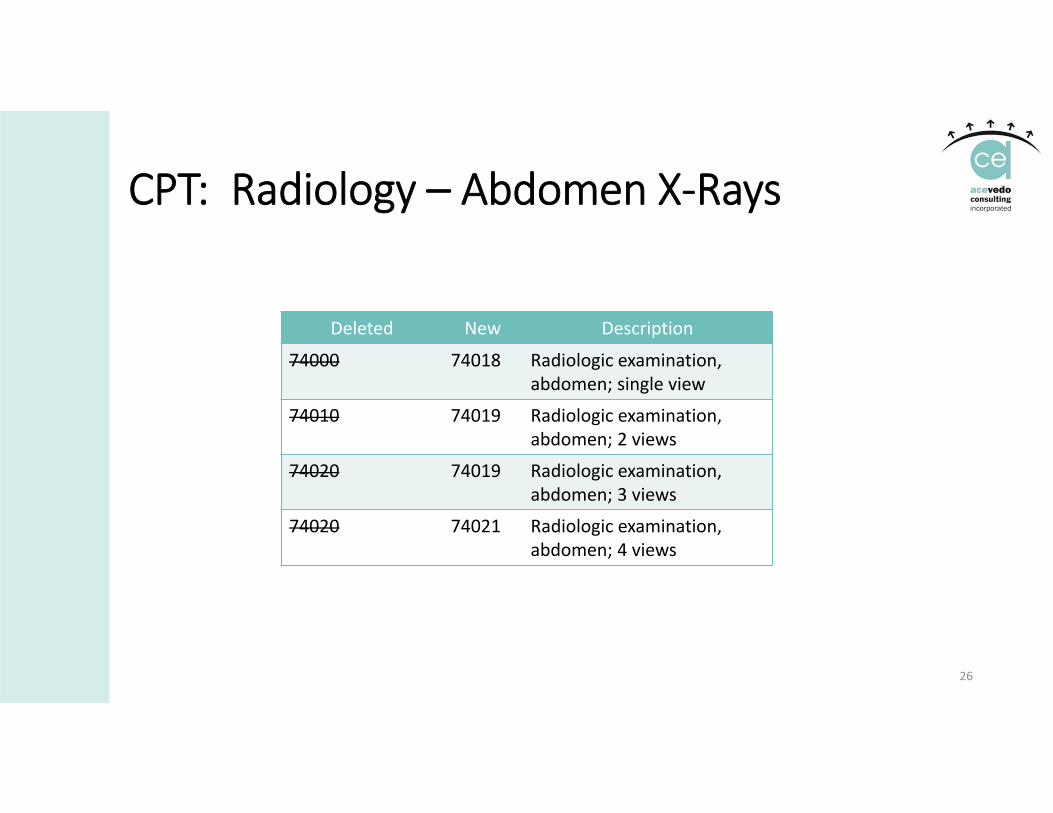
CPT: Radiology – Abdomen X‐Rays
26
Deleted New Description
74000 74018 Radiologic examination, abdomen; single view
74010 74019 Radiologic examination,abdomen; 2 views
74020 74019 Radiologic examination, abdomen; 3 views
74020 74021 Radiologic examination, abdomen; 4 views
© Acevedo Consulting Incorporated 2016
CPT: Radiology – Extremity Ultrasound (76881, 76882)
• Diagnostic ultrasound requires permanently recorded images and a written report containing a description of each of the elements evaluated.
• Guidelines revision: “When fewer than all of the required elements for a “complete” exam (76881) are performed, report the “limited” code (76882).”
• Why: In response to a RUC analysis, it was determined that codes 76881 and 76882 and the diagnostic ultrasound extremities introductory guidelines should be revised and updated to clarify the distinction between complete and limited studies. Key terms have been added to the guidelines to distinguish between complete and limited studies.
27

CPT: Radiology – Extremity Ultrasound (revised definitions)
28
76881 Complete evaluation of a specific joint in an extremity including all of the ff’ing:• Joint space • Peri‐articular soft‐tissue structures (muscles, tendons, other soft tissue structures surrounding the joint), and
• Any identifiable abnormality.• Permanent recorded image(s) and a written report containing a description of each of the required elements or reason an element could not be visualized (eg, absent due to surgery or trauma)
76882 limited evaluation of a joint or evaluation of a structure in an extremity other than a joint (soft‐tissue mass, fluid collection, or nerve); use when fewer than all required elements of a “complete” exam (76881) are performed.• Specific anatomic structure (eg, joint space only or tendon, muscle, and/or other soft tissue structures that surround the joint that does not assess all of the required elements included in 76881.
© Acevedo Consulting Incorporated 2016
CPT: Radiology
• Mammography HCPCS Codes Replaced• Effective for dates of service on/after 01/01/2018, the following codes are replaced• G0102: Use 77067 (Screening mammo, bilateral, with CAD when performed)
• G0204: Use 77066 (Diagnostic mammogram, including CAD when performed, bilateral)
• G0206: Use 77065 (Diagnostic mammogram, including CAD when performed, unilateral)
29
30
Presumptive Drug Class Screening revisions:ΔMolecular PathologyΔGenomic Sequencing ProceduresΔMultianalyte Assays with Algorithmic Analyses
CPT: Pathology and Laboratory
31
Presumptive Drug ScreeningΔ80305 Drug test(s), presumptive, any number of drug classes, any number of devices or procedures capable of being read by direct optical observation only (eg, utilizing immunoassay [eg, dipsticks, cups, cards, or cartridges]), includes sample validation when performed, per date of service.
Δ80306 ..read by instrument assisted direct optical observation (eg, utilizing immunoassay [eg, dipsticks, cups, cards, or cartridges]), includes sample validation when performed, per date of service
Δ80307 ..by instrument chemistry analyzers and mass spectrometry either with or without chromatography, includes sample validation when performed, per date of service
CPT: Pathology and Laboratory

© Acevedo Consulting Incorporated 2016
Medicine: Vaccines
• Codes 90651, 90620, and 90621 have been revised to include dosage amounts and/or the Advisory Committee on Immunization Practices (ACIP) abbreviations. In addition, four new codes have been added:• 90587 for reporting a quadrivalent dengue vaccine; • 90750 for Zoster vaccine; • 90756 quadrivalent influenza virus vaccines; cclr4 and • 90682 for quadrivalent influenza virus vaccines
32

© Acevedo Consulting Incorporated 2016
Medicine: Pulmonary Services
• Numerous changes have been made, including • the addition of new and revised parenthetical notes, • deletion of code 94620, and • revision to code 94621 to include measurements of minute ventilation and electrocardiographic recordings.
• Two new codes have been added: • 94617 to identify exercise testing for bronchospasm and • 94618 to identify pulmonary stress testing.
33
© Acevedo Consulting Incorporated 2016
Medicine: Endocrinology
• Two codes have been revised: • 95250 includes ambulatory continuous glucose monitoring with office‐provided equipment and
• 95251 includes the word “analysis.” • New code 95249 has been added to include patient‐provided equipment
34

© Acevedo Consulting Incorporated 2016
Medicine: Dermatology
• Two new codes have been established in the Photodynamic subsection of the Medicine section. • Code 96573 describes photodynamic therapy to destroy premalignant lesions provided by a physician or other qualified health care professional. • Note that the code specifies who can perform this treatment
• Code 96574 describes debridement of premalignant hyperkeratotic lesion(s) followed by photodynamic therapy.
• Exclusionary parenthetical notes have been added to preclude the use of code 96573 with 96574, and vice versa for the same anatomic area.
35
© Acevedo Consulting Incorporated 2016
HCPCS: Prolonged Preventive Services
• G0513: Prolonged preventive service(s) (beyond the typical service time of the primary procedure), in the office or other outpatient setting requiring direct patient contact beyond the usual service; first 30 minutes (list separately in addition to code for preventive service)
• G0514: Prolonged preventive service(s) (beyond the typical service time of the primary procedure), in the office or other outpatient setting requiring direct patient contact beyond the usual service; each additional 30 minutes (list separately in addition to code G0513 for additional 30 minutes of preventive service)
36

© Acevedo Consulting Incorporated 2016
HCPCS: Prolonged Preventive Services
• “Effective for claims with dates of service on or after January 1, 2018, prolonged preventive services will be payable by Medicare when billed as an add‐on to an applicable preventive service that is payable from the Medicare Physician Fee Schedule, and both deductible and coinsurance do not apply to G0513 and G0514 for prolonged preventive services will be added as part of January 1, 2018, HCPCS update and the coinsurance and deductible will be waived.”• MLN Matters MM10181 and CR10181
37

PPS Can Be Billed With and When….
38
HCPCS Code/Min. Short Descriptor76706 / 32 Us abdl aorta screen aaa76977 / 7 Us bone density measure77067 / 22 screening mammography77063 / 12 Breast tomosynthesis bi77078 / 29 Ct bone density axial77080 / 33 Dxa bone density axial77081 / 22 Dxa bone density/peripheralG0101 / 10 Ca screen;pelvic/breast examG0104 / 17 Ca screen;flexi sigmoidscopeG0105 / 30 Colorectal scrn; hi risk ind
HCPCS Code/ Min. Short DescriptorG0121 / 30 Colon ca scrn not hi rsk indG0130 / 26 Single energy x‐ray studyG0296 / 15 Visit to determ ldct eligG0297 / 32 Ldct for lung ca screenG0402 / 30 Initial preventive examG0438 /30 Ppps, initial visitG0439 / 25 Ppps, subseq visitQ0091 / 16 Obtaining screen pap smear
© Acevedo Consulting Incorporated 2016
Telehealth
• Effective 1/1/18, modifier GT (via interactive audio and video telecommunications systems) is no longer required on professional claims for telehealth services.
• Place of service code 02 certifies that the telehealth service meets Medicare’s requirements for reimbursement.
• “One every 3 days” frequency edit for 99231‐99233 telehealth services when billed with POS 02
• “One every 30 days” frequency edit for 99307‐99310 telehealth services when billed with POS 02
• POS 02 also applies to:• ED and Initial inpatient telehealth consultations (G0425‐G0427)• F/Up InPt telehealth consultations (G0406‐G0408)• Diabetes self‐management training (G0108‐G0109)
39MLN Matters MM10152

Medicare Changes & Policies

Collecting Data for 10‐ and 90‐Day Global Periods Continues
© Acevedo Consulting Incorporated 2016
Collecting Data on Resources Used in Furnishing Global Services• Under the PFS, certain services, such as surgery, are valued and paid for as part of global packages that include the procedure and the services typically furnished in the periods immediately before and after the procedure.
• For each of these global packages, there is a single PFS payment that includes payment for particular services that are assumed to be typically furnished during the established global period.
• But:• What resources/how many and what level of visits are actually provided today? W/o this information, CMS cannot attribute accurate value.
• When a patient leaves the area within the global period and receives post‐op care elsewhere, that 2nd doctor bills E&M codes that were included in the RVUs for the surgical procedure. Medicare and others are paying twice.

© Acevedo Consulting Incorporated 2016
Collecting Data on Resources Used in Furnishing Global Services• Goal: transform all 10‐ and 90‐day global codes to 0‐day global codes in CY 2017 and CY 2018.
• Section 1848(c)(8)(B)(i) of the MACRA requires CMS to develop, through rulemaking, a process to gather information needed to value surgical services from a representative sample of physicians, and requires that the data collection begin no later than January 1, 2017.
• The collected information must include the number and level of medical visits furnished during the global period and other items and services related to the surgery and furnished during the global period, as appropriate.
• “There is a critical need to obtain complete information if we are to value global packages accurately and in a way that preserves relativity across the fee schedule.”
© Acevedo Consulting Incorporated 2016
Claims‐based Data Collection• CPT code 99024 will be used for reporting post‐operative services.• Reporting is not required for pre‐operative visits included in the global package or for services not related to patient visit.
• Reporting is required only for services related to codes reported annually by more than 100 practitioners and that are reported more than 10,000 times or have allowed charges in excess of $10 million annually.• CPT codes 15732, 34802, and 34825 are deleted in 2018. Reporting is not required after December 31, 2017.
• New codes added for 2018: 15730, 15731, 34705, 34706, 34710, 58575• Mandatory requirement to report will be effective for services related to global procedures furnished on or after July 1, 2017 through at least 12/31/18.
© Acevedo Consulting Incorporated 2016
Claims‐based Data Collection• Only practitioners who practice in groups with 10 or more practitioners in the following 9 states will be required to report:• Florida• Kentucky• Louisiana• Nevada• New Jersey• North Dakota• Ohio• Oregon, and • Rhode Island
• Practitioners who only practice in smaller practices or in other geographic areas are encouraged to report data, if feasible.
© Acevedo Consulting Incorporated 2016
Claims‐based Data Collection
• “Since CPT code 99024 will only provide data on the number of visits and no data on the level or resources used in furnishing the visit, we believe this is only the first step in gathering the data required.”
• Need information on the level of visits and other resources needed to value surgical services accurately.
• Collecting data on services that are furnished by more than 100 practitioners and are either furnished more than 10,000 times or have allowed charges of more than $10 million annually, CMS estimates it will collect data on• 87 percent of all furnished 10‐ and 90‐day global services.
• For 2018 about 290 codes that describe approximately
www.cms.gov/Medicare/Medicare‐Fee‐for‐Service‐Payment/PhysicianFeeSched/Global‐Surgery‐Data‐Collection‐.html
© Acevedo Consulting Incorporated 2016
Claims‐based Data Collection
• Teaching physicians will be subject to the reporting requirements in the same way that other physicians are:• Such physicians should report CPT code 99024 only when the services furnished would meet the general requirements for reporting services and should use the GC or GE modifier as appropriate.
• By excluding practitioners who only practice in practices with fewer than 10 practitioners, we estimate that about 45 percent of practitioners will not be required to report. In defining small practices, we reviewed other programs:• We chose 10 practitioners as the threshold for reporting as practices of this size are large enough to support coding and billing staff, which will make this reporting less burdensome;
• Also, this is the same threshold used by the value‐based modifier program for its phase‐in of a new requirement because of concerns about the burden of small practices.
© Acevedo Consulting Incorporated 2016
Claims‐based Data Collection
• In summary, CMS’ claims‐based data collection policy requires that, for procedures furnished on or after July 1, 2017, practitioners who practice in practices that includes of 10 or more practitioners in Florida, Kentucky, Louisiana, Nevada, New Jersey, North Dakota, Ohio, Oregon, and Rhode Island will be required to report on claims data on post‐operative visits furnished during the global period of a specified procedure using CPT code 99024.
• The specified procedures are those that are furnished by more than 100 practitioners and either are nationally furnished more than 10,000 times annually or have more than $10 million in annual allowed charges.
© Acevedo Consulting Incorporated 2016
Survey Data Collection
• Remember, 99024 will only provide a raw number of post‐operative visits:• No intensity;• No information on how patients’ comorbid conditions impact care and treatment.
• Since the end result of CMS’s data collection will undoubtedly impact payment more information is indeed needed.
© Acevedo Consulting Incorporated 2016
Survey Data Collection
• Survey will complement claims‐based reporting and will provide CMS with important information on non‐face‐to‐face activities and other activities that are not reported with CPT code 99024.
• The resulting visit‐level survey data would allow CMS to explore in detail the variation in activities, time, intensity, and resources associated with global services within and between physicians and procedures, and would help to validate the information gathered through claims.
© Acevedo Consulting Incorporated 2016
Survey Data Collection
• Practitioners will be asked to describe 20 post‐operative visits furnished to Medicare beneficiaries or other patients during the reporting period. Example:• Procedure codes(s) and date of service for procedure upon which the global period is based;
• Procedure place of service;• Whether or not there were complications during or after the procedure; • The number in sequence of the follow‐up visit (for example, the first visit after the procedure).
• The information collected will be developed based upon direct observation and discussions in a small number of pilot sites.

© Acevedo Consulting Incorporated 2016
Survey Data Collection
• Information about the visit will include:• Which level of visit using existing billing codes;• Specific face‐to‐face and non‐face‐to‐face activities furnished on the day of the visit;
• The total time spent on face‐to‐face and non‐face‐to‐face activities on the day of the visit;
• Direct practice expense items used during the visit, for example supplies like surgical dressings and clinical staff time.
Would you be able to provide this information?
What will have to change in patient post‐op visit information?
© Acevedo Consulting Incorporated 2016
Survey Data Collection
• The survey instrument will also collect information on the visit in question including, for example:• Which level of visit using existing billing codes;• Specific face‐to‐face and non‐face‐to‐face activities furnished on the day of the visit;• The total time spent on face‐to‐face and non‐face‐to‐face activities on the day of the visit;
• Direct practice expense items used during the visit, for example supplies like surgical dressings and clinical staff time.
• The instrument will ask respondents to report other prior or anticipated care furnished to the patient by the practice outside of the context of a post‐operative visit, for example non‐face‐to‐face services.
© Acevedo Consulting Incorporated 2016
Survey Data Collection
• Statistically valid target population: 4,872 practitioners:• 311 reporting practitioners from each specialty which is the only specialty contributing at least 5 percent of billings for any one procedure group code;
• For other specialties, the target will be defined by the maximum value of 311 divided by the number of specialties contributing at least 5 percent for any procedure group code for which that specialty contributes.
• CMS expects a response rate in excess of 50%. • Given this response rate (and some uncertainty in this response rate estimate), they’ll need to approach at least 9,722 practitioners to attain the target of 4,872 practitioners.
• Should the response rate be lower than expected, CMS will continue to sample in waves until reaching the target of approximately 4,872 practitioners.

© Acevedo Consulting Incorporated 2016
Direct Observation Component
The direct observation component will consist of external observers capturing the activities conducted in a sample of post‐operative visits at a small number of practices. It is designed to provide additional context to inform future data collection efforts and to gauge where the practitioner survey does or does not capture the full range of activities. It is not a data collection activity per se.
© Acevedo Consulting Incorporated 2016
Required to Report
• If we find that compliance with required claims‐based reporting is not acceptable, CMS will consider in future rulemaking imposing up to a 5 percent payment withhold as authorized by the statute.
• A survey of practitioners participating in approximately 4 to 6 ACOs using the survey instrument along with an additional ACO‐specific module will be used to collect data from on pre‐ and post‐operative visits.• Do physicians and practices affiliated with ACOs expend greater time and effort in providing post‐operative global services in keeping with their goal of improving care coordination for their assigned beneficiaries?
• Questions? Contact [email protected]
© Acevedo Consulting Incorporated 2016
Conversion Factor, Therapy Cap
• Contains a statutory update factor of 0.5% (MACRA)• $35.9996 for 2018
• $35.8887 for 2017• $35.8043 in 2016.
Check your managed care contracts to help ensure your fee schedule goes up in 2017 if applicable and monitor payments on 2018 services. CY 2018 Therapy cap$2,010 for physical and speech therapy combined$2,010 for occupational therapy
© Acevedo Consulting Incorporated 2016
Important Reminders and Payment Policies

© Acevedo Consulting Incorporated 2016
Transition from Traditional X‐Ray Imaging to Digital Radiography: “Payment incentive” • Beginning January 1, 2018 thru CY 2022, claims for imaging services that are X‐rays taken using computed radiography (cassette‐based imaging) must include the modifier “FY.”• Example: 71020 ‐FY
• The use of this modifier will result in a 7 percent reduction of the X‐ray technical component and the TC of the global code• Increases to a 10% reduction starting in CY 2023• Beneficiary is not liable for the payment reduction
• Payment incentive?• The “incentive” is to avoid the penalty by upgrading equipment and no longer using film or cassettes.
See MM10188 “Payment Reduction for X‐Rays Taken Using Computed Radiography”
© Acevedo Consulting Incorporated 2016
Transition from Traditional X‐Ray Imaging to Digital Radiography: “Payment incentive” • And remember:
• 20% reduction from the technical component for x‐rays taken with film continues.
• ‐FX modifier required
• “For claims billed with the FY modifier and another X‐ray reduction modifier on the same line, contractors shall apply both reductions if applicable. The FY modifier reduction will be applied after the other reduction (for example, claims billed with both FX and FY modifiers will have the FX modifier reduction applied first).”
See MM10188 “Payment Reduction for X‐Rays Taken Using Computed Radiography”
© Acevedo Consulting Incorporated 2016
Prohibition on Billing Qualified Medicare Beneficiary Individuals for Medicare Cost‐Sharing
• Federal law prohibits providers from collecting Medicare Part A and Medicare Part B deductibles, coinsurance, or copayments, from beneficiaries enrolled in the Qualified Medicare Beneficiaries (QMB) program.
• QMB is a Medicaid program which helps certain low‐income individuals with Medicare cost‐sharing liability.
• States can limit provider payment for Medicare cost‐sharing to the lesser of the Medicare cost‐sharing amount, or the difference between the Medicare payment and the Medicaid rate for the service.
© Acevedo Consulting Incorporated 2016
Prohibition on Billing Qualified Medicare Beneficiary Individuals for Medicare Cost‐Sharing• Medicare providers must accept the Medicare payment and Medicaid payment (if any) as payment in full sharing from the beneficiary) as payment in full for services rendered to a QMB individual.
• Medicare providers who violate these billing prohibitions are violating their Medicare Provider Agreement and may be subject to sanctions.
• QMB status and exemption from cost‐sharing on the Medicare RA since October 3, 2017
• “If you have erroneously billed an individual enrolled in the QMB program, recall the charges (including referrals to collection agencies) and refund the invalid charges he or she paid.”
MLN Matters Number: SE1128
© Acevedo Consulting Incorporated 2016
Social Security Number Removal Initiative (SSNRI)• MACRA requires CMS to remove SS #s from all Medicare cards
• by April 2019.• A new randomly generated Medicare Beneficiary Identifier (MBI) will replace the SSN‐based HICN on the new Medicare cards.• 11‐characters made up only of numbers and uppercase letters• No separate ID # for Railroad Retirement Board beneficiaries (look for the RRB logo on the card)
• CMS will be sending each beneficiary a new Medicare card with the MBI.• Plans are to start sending the cards by April 2018• To be mailed in geographical waves
• All systems (Medicare’s and Yours) will require updating:• Transition period 4/1/18 thru 12/31/2019• What system changes will need to take place
• Intake forms• Billing software, Clearinghouse, Billing Company• Other
www.cms.gov/Medicare/SSNRI/Index.htmlICN 909365 September 2017
© Acevedo Consulting Incorporated 2016
Protecting Access to Medicare Act (PAMA) of 2014 Requires AUC for Advanced Imaging • CMS proposes to define “appropriate use criteria” as a collection of individual appropriate use criteria that are presented to the ordering physician in a manner that links a specific clinical condition or symptom with an assessment of the appropriateness of advanced diagnostic imaging services.
• These criteria would be developed or endorsed by provider‐led entities and, to the extent feasible, should be evidence‐based.
• CMS defines provider‐led entities (PLE) as national professional medical specialty societies (such as the American College of Radiology/ACR) and organizations that are “comprised primarily of providers and [are] actively engaged in the practice and delivery of healthcare.”
64
© Acevedo Consulting Incorporated 2016
Appropriate Use Criteria for Advanced Diagnostic Imaging• Goal: That patients get the right test at the right time
• Mandated in PAMA, and MACRA• Requires an ordering professional to consult with a qualified Clinical Decision Support Mechanism (CDSM) for advanced imaging.• MR, CT, Nuclear Medicine, PET
• AUC consultation information must be included on the furnishing professional’s claim for that claim to be paid;
• January 1, 2020, the program will begin with an educational and operations testing period and during this time CMS will continue to pay claims whether or not they correctly include the AUC information.
65
© Acevedo Consulting Incorporated 2016
Appropriate Use Criteria for Advanced Diagnostic Imaging• What will be required to be reported:1. Which qualified CDSM was consulted by the ordering professional; 2. Whether the service ordered would adhere to specified applicable
AUC, would not adhere to specified applicable AUC, or whether the specified applicable AUC consulted was not applicable to the service ordered; and
3. NPI of the ordering professional (if different from the furnishing professional).
66

© Acevedo Consulting Incorporated 2016
Appropriate Use Criteria for Advanced Diagnostic Imaging• Applies to all three fee schedules:
• PFS, • Hospital outpatient prospective payment system and• Ambulatory surgical center payment system).
• CMS is working to develop a modifier that confirms the AUC criteria was/was not met
• CMS is working to align AUC reporting with MIPS’ Improvement Activities.
67
© Acevedo Consulting Incorporated 2016
Changes to E&M Codes in the Future
• “We agree with continued feedback from stakeholders that these guidelines are potentially outdated and need to be revised.”
• “CMS is seeking comment from stakeholders on specific changes we should undertake to update the guidelines, to reduce the associated burden, and to better align E/M coding and documentation with the current practice of medicine. We are especially seeking comment on how we might focus on initial changes to the guidelines for history and exam, because we believe documentation for these elements may be more significantly outdated.”
• All physicians should keep their eyes and ears open and be willing to provide in put via their specialty societies, CMS, etc.
68
Note:Information from CMS 1676‐F was relied upon in developing this presentation. Keep on the alert for Transmittals, Change Requests and CMS articles to
further refine coverage criteria.

Other Changes and “Heads up”
© Acevedo Consulting Incorporated 2016
Audits, Recoupments, Risk Areas
• “OIG Claims $729 Million in meaningful use over payments.”• 100 providers reviewed• 14 EPs with payments totally $291,222 that did not meet the MU requirements
• Extrapolated over the $6.1B in MU payments = $729M• Specific Findings
• 13:14 EPs cold not produce “support that they had generated at least one report listing patients with a specific condition” or to show they’d performed a SRA
• Insufficient documentation/support accounted for 87% of the overpayments.
• Remember to keep all your MU documentation for at least 6 years
71
© Acevedo Consulting Incorporated 2016
Audits, Recoupments, Risk Areas
• OIG Reports and CBRs – Physical therapy – National stats• KX Modifier – average use 21%• Average minutes per visit – 45.67• Average total allowed charges per beneficiary ‐ $724.03
• Are any of your billing patterns significantly higher?
72
© Acevedo Consulting Incorporated 2016
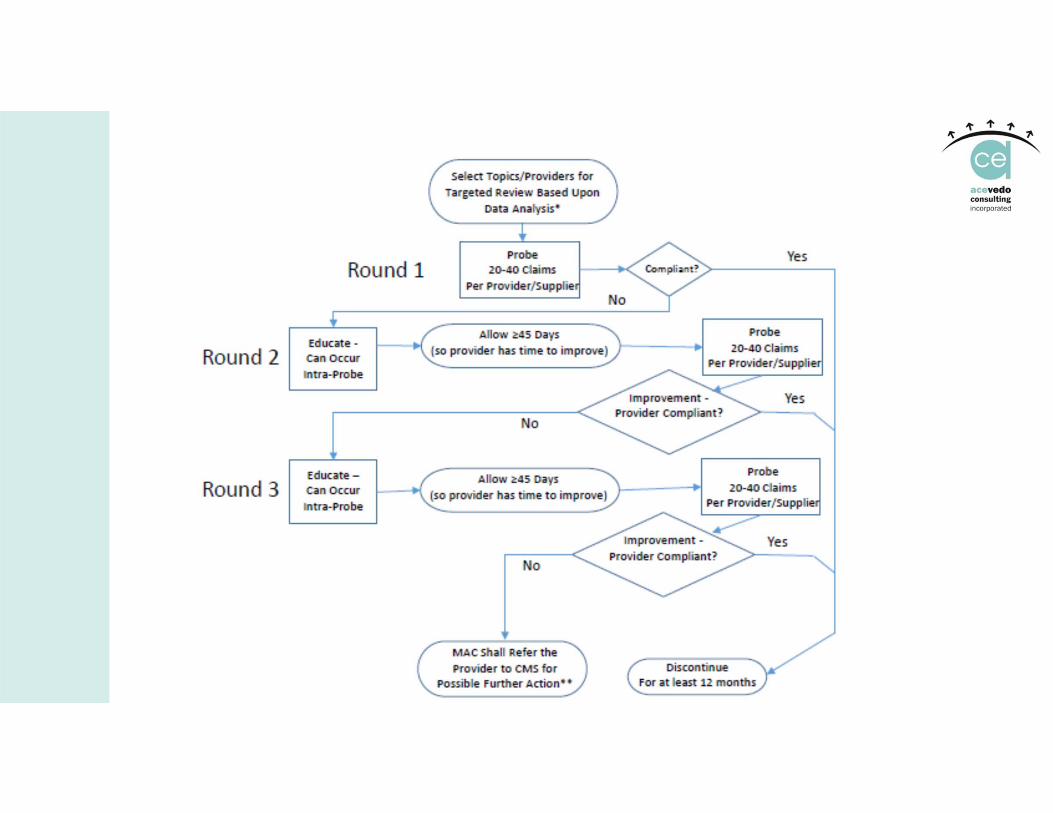
Medicare’s Targeted Probe & Educate
• Effective 10/1/17, based on data analysis of claims payment, your MAC will identify areas with the greatest risk of inappropriate program payment:• Analysis of billing data indicating aberrancies that may suggest questionable billing practices, or
• Targeted review based on error rates, or• Service specific review error rate results
• MACs will focus only on providers/suppliers who have the highest claim error rates or billing practices that vary significantly from their peers. • No more widespread probe reviews
73
© Acevedo Consulting Incorporated 2016
Medicare’s Targeted Probe & Educate
• An Additional Documentation Request (ADR) will be generated for each claim selected• For prepayment reviews, MAC has 30 days from the date the documentation is received to review the documentation and make a payment decision
• For post‐pay reviews, MAC has 60 days from the date the documentation is received to review the documentation and make a payment decision.
• Non‐response denials count as an error when calculating the provider's error rate.• Do not ignore those ADRs!
• After each round, providers are offered individualized education based on the results of their reviews.
• Prior to each round’s conclusion, MAC will call all providers with moderate to high error rate to discuss the summary of errors found.
74

© Acevedo Consulting Incorporated 2016
Medicare’s Targeted Probe & Educate
• At the conclusion of each round, a letter with the review results will be mailed.
• This letter to include the number of claims reviewed, number of claims allowed in full, and number of claims denied in full or in part.
• When high denial rates continue after three rounds of TPE, MAC will send a referral to CMS for additional action.
• Further Action May Include 100% Prepayment Review, Extrapolation, Referral To ZPIC/UPIC, etc.
CMS Change Request 10249
75
© Acevedo Consulting Incorporated 2016
Modifier ‐25: Outlier Policy or a Trend?
• Pennsylvania’s Independence Blue Cross Blue Shield• 50% payment reduction of E&M codes billed with ‐25 and a minor procedure.• And, when using ‐25, “documentation for the additional E/M must be entered in a separate section of the medical record in order to validate the separate and distinct nature of the E/M service.”• ? No longer allows the E&M and a procedure in the same note ?
• Make sure your doctors and NPPs know when to use ‐25 (and when not to), and, that their documentation for the two services billed is separate and distinct.
77
© Acevedo Consulting Incorporated 2016
Incident to Billing and NPPs
• Investigations, Civil and Criminal Cases in process• Remember, this is a Medicare benefit; never assume another payer honors Medicare’s policy on incident to billing.• FL Blue expects NPPs to bill under their own NPI or FL Blue number• UHC requires the –SA modifier
• For Medicare there is only one circumstance when your ARNP or PA can see a patient and the bill go out under the doctor’s NPI• The NPP is seeing an established patient in follow up of a problem for which the doctor initiated the treatment plan. The NPP makes NO CHANGES (not even a new/revised Rx) and orders no tests. The claim can always be billed to Medicare under the NPP’s NPI, but if all incident to criteria are met, you may submit the claim under the NPI of the physician who was in the office suite when the patient was seen (whether or not that is the patient’s doctor).
78
© Acevedo Consulting Incorporated 2016
HIPAA: How Well do You Follow Your Policies?• Memorial Health System paid $5.5M in February 2017 to settle potential HIPAA violations.
• The login credentials of a former employee of an affiliated doctor’s office had been used to access ePHI in the hospital’s system daily for a year. This information (names, dates of birth, SSNs) was accessed by and disclosed to the office’s staff impermissibly. 80,000 individuals impacted.
• Although MHS had policies and procedures in place, it failed to implement procedures with respect to reviewing, modifying and/or terminating users’ right of access. This risk had been identified on prior SRAs.
79
© Acevedo Consulting Incorporated 2016
Some Changes for MIPS in 2018
• Quality measures will be reported for a full year (no longer just 90 days)• Measures will be worth 3 to 10 points • If you don’t report a quality measure for at least 50% of the applicable Medicare patients, you will not get more than 1 point for it• Unless you’re in a small practice (≤15 eligible clinicians)
• Quality will account for 50% of the score• Cost is back
• 10% of the 2018 score• Comes from claims data: yours, other doctors, hospitals, HHA, Part B drugs, etc.
• Diagnosis coding is critical!
80
© Acevedo Consulting Incorporated 2016
Some Changes for MIPS in 2018
• Advancing Care Information • Report for a 90‐day period
• Practice Improvement Activities• Report for a 90‐day period
• Virtual Groups
81

© Acevedo Consulting Incorporated 2016
QUESTIONS?
© Acevedo Consulting Incorporated 2016
Acevedo Consulting Incorporated prides itself on not providing cookie‐cutter programs, but a quality work product formulated and designed to meet your desired goals. We treat each client as unique, and we tailor our reviews, recommendations, training and action plans accordingly.
One size does not fit all!
You can rely on us to guide you and your staff through the labyrinth of coding, reimbursement and regulatory compliance issues of the ever‐changing and complex health care industry.
We are a client‐focused, service‐oriented firm specializing in:
• Chart Reviews for Proper Coding• Compliance & HIPAA Programs• Medicare/Medicaid Credentialing• Appeal Assistance• Education for Staff, Physicians, Nonphysician Practitioners
About Acevedo Consulting Incorporated
© Acevedo Consulting Incorporated 2016
Acevedo Consulting Incorporated2605 West Atlantic Avenue, Suite D‐102
Delray Beach, FL 33445561.278.9328