coagulation monitoring during surgery: when and why? prof khaled yassen md ffarcsi department of...
TRANSCRIPT

Coagulation Monitoring During Surgery: When and Why?
Prof Khaled Yassen MD FFARCSIDepartment of Anaesthesia
Liver Institute, Menoufiya University, [email protected]

Old and New Liver Institute, Menoufiya University, Egypt
Introduction
• Coagulation changes frequently associate end stage liver disease.
• During liver transplantation these changes can present with complex haemostatic disorders. HYPER or HYPO
• Needs monitoring and management adequately for both Live Donors and Recipients

DONORS HYPERCOAGULATION

Live Liver Donors can be at risk
• Screening for coagulation disorders• Pulmonary embolism reported in a donor due to
an increased von Willebrand factor activity)• A policy which led to reject candidates for
donation in this center. Durand F, Liver Transpl. 2002 Feb;8(2):118-20.

Donors excluded due to Hypercoagulation
• Due to homozygous Factor V Leiden Mutation in a study from Menoufiya Liver Institute, Egypt.
• Coagulation changes for liver donors using the Rotational Thromboelastometry. Lotfy M et al. Poster presentation ILTS and LICAGE meeting Spain 2015
• Published in Clinical transplantation journal 2013; 03-16

Factor V Leiden Mutation Transmission to recipients
• Donor factor V Leiden mutation lead to vascular thrombosis following liver transplantation.
Hirshfield G Liver Transpl Surg. 1998 Jan;4(1):58-61
Recurrent deep-vein thrombosis acquired after liver transplantation due to a homozygous factor V Leiden mutation
Willems M Liver Transpl. 2003 Aug;9(8):870-3
• .

Donors Can Transmit Coagulation Disorders
• Factor V Leiden and hepatic artery thrombosis after liver transplantation. Dunn TB, Clin Transplant. 2006 Jan-Feb;20(1):132-5
• Activated protein C resistance acquired through liver transplantation and associated with recurrent venous thrombosis.
• Leroy-Matheron C J Hepatol. 2003 Jun;38(6):866-9.

Liver Donors Thrombotic Complications
• Hypercoagulability after partial liver resection.
Thromb Haemost. 2007 Dec;98(6):1252 Bezeaud A et al
• thromboprophylaxis is needed. • Thrombin-antithrombin complexes and sP-
selectin could serve as early biological predictors of thrombotic complications

Recipients’ Hypercoagulation

• These haemostatic changes, as well as technical and surgical factors, may have a role in the early development of hepatic artery thrombosis (HAT)
• Lisman T, Porte RJ. Hepatic artery thrombosis after liver transplantation: more than just a surgical complication? Transpl Int2009;22: 162–4.
Hypercoagulation studies

Thromboembolic Events with LTx
• Hamostaseologie. 2006 Aug;26(3 Suppl 1):S64-76. Coagulation management during liver transplantation] Görlinger K.
Recommendation
• Abolished the routine prophylaxis with antifibrinolytic drugs.

Is relatively well preserved with whole blood global viscoelastic tests (TEG/ROTEM) compared to INR aPTT and other classical lab tests
Mallett S, Chowdary P, Burroughs A. Clinical utility of viscoelastic tests of coagulation in patients with liver disease Liver Int. 2013;33:961-74
Coagulation in liver patients

• An imbalance between pro and anticoagulant systems and post operative fibrinolytic shutdown
• Stahl RL, Duncan A, Hooks MA,et al. A hypercoagulable state follows orthotopic liver transplantation.Hepatology 1990;1: 553–8.
Viscoelastic tests and hypercoagulation post liver transplant research

• McCrath DJ, et al Thromboelastography
maximum amplitude predicts postoperative thrombotic complication including myocardial infarction. Anesth Analg2005;100:1576–83.
• Dai Y, et al. Does thromboelastography predict postoperative thromboembolic events?. Anesth Analg 2009;108: 734–42.
Can Viscoelastoc tests predict vascular problems

Designing a study to look into the hypercoagulation in Recipients

Rotational thromboelastometry for
hypercoagulable recipients during and after live liver transplantation
Abdel Salam Y, Yassen K et al
To be presented during LICAGE 2015 Montpellier France

Research is funded by the Anaesthesia Department funds and Liver Transplant Unit facilities. Menoufiya University, Liver Institute, Egypt
No Conflict of Interest

• To study the perioperative coagulation profile and outcome for live liver transplant recipients with tendency to hypercoagulability.
AIM
South African Cochrane Registration Single-blinded diagnostic study.
Patients and Methods:
•A prospective diagnostic study •53 consecutive recipients
•Only 43 positive for three or more of the following tests demonstrating tendency to hypercoagulate . (abnormal Factor V leidin mutation, low Protein C, low ProteinS, low Antithrombin III, increased Lupus anticoagulant, increased Homocystein IgG-IgM).
•HCV 36/43 (83.7%) •HCV+HCC 16/43 (37.2%)
• Rotational thromboelastometry (ROTEM) (EXTEM, INTEM and FIBTEM)
• CCT (Prothrombin time (PT), activated partial thromboplastin time (a PTT), fibrinogen level, platelets count, and International normalization ratio (INR)
• Preoperatively, anhepatic phase, post-reperfusion, postoperative Day 1, 3 and 7.
Coagulation studies


Spring
Rotating axis (+/ - 4.75°)
Light source
Detector
Plastic sensor Cuvette with blood Fibrin strands and platelet aggregates between surfaces Heated cuvette holder
Ball bearing

Main parameters of ROTEM
CT = Clotting Time (sec)
CFT = Clot Formation Time (Sec)
α- angle (°)
MCF = Maximum Clot Firmness (mm)
Clot Quality
Maximum Lysis (%)

F (Repeated Measures ANOVA) = 1105.801, p=0.000*
p=0.000*
p=0.000*

F (Repeated Measures ANOVA) = 443.808, p=0.000*
CT normal range 38-79

F (Repeated Measures ANOVA) = 1174.001, p=0.000*
p=0.001*Normal CT 100-240
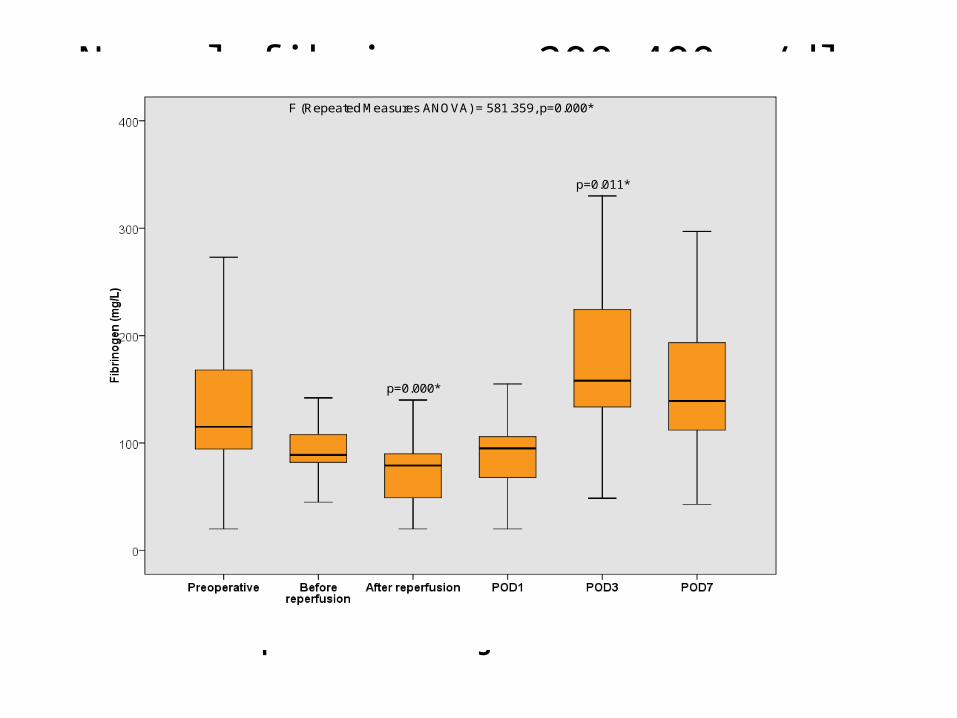
F (Repeated Measures ANOVA) = 581.359, p=0.000*
p=0.000*
p=0.011*
Box and Whisker plot of fibrinogen blood levels
Normal fibrinogen 200-400mg/dl

F (Repeated Measures ANOVA) = 1732.300, p=0.000*
p=0.000*
p=0.000*
p=0.000*
Box and Whisker plot of MCF level of FIBTEM
MCF FIBTEM 9-25

• Observational study of 298 liver transplant patients, high fibrinogen levels and low protein C levels were significantly associated with post-transplant thrombotic events
• Ayala R, et al. Recipient and donor thrombophilia and risk of portal venous thrombosis and hepatic artery thrombosis in liver recipients.BMC Gastroenterol2011;11: 130.
Hypercoagulation and Fibrinogen
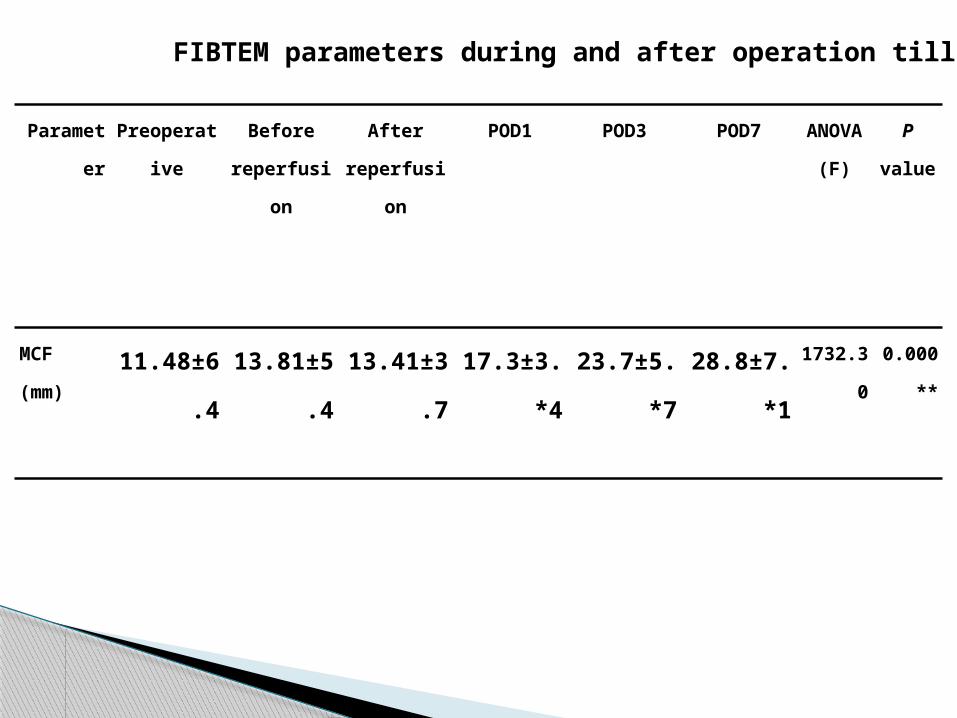
FIBTEM parameters during and after operation till POD7 .
Parameter Preoperative Before
reperfusion
After
reperfusion
POD1 POD3 POD7 ANOVA
)F(
P value
MCF
(mm)11.48±6.4 13.81±5.
4
13.41±3.
7
17.3±3.4* 23.7±5.7* 28.8±7.1* 1732.30 0.000*
*

Limited number of recipients involved The study did not extend beyond Day 7
postoperative Other factors involved in the coagulation as
factor VIII and Ptn C were not followed up Fibrinoltyic system need to be investigated
in depth
Limitations of the study

An increase in fibrinogen activity
demonstrated by FIBTEM postoperatively
The ability of FIBTEM to be used as a
predictor for thromboembolic events need to be investigated when CCTs fails to diagnose the condition.
FIBTEM after 7 Days need to be followed
Conclusion

No correlation between CCT and ROTEM
A New Anticoagulation regimes monitored and guided by ROTEM parameters should be the focus of future research studies to replace the conventional lab tests
Conclusion

Use of thromboelastography Platelet Mapping (TM) to monitor antithrombotic therapy in a patient with Budd-Chiari syndrome.Liver Transpl2010;16:38–41.
A case report of a patient with BCS and TIPS occluded with thrombus, describes the use of
TEG to guide management of anticoagulant therapy and recanalisation of the stent
James K, Bertoja E, O’Beirne J, Mallett S.

Anticoagulation after liver transplantation: a retrospective audit and case control study. Blood Coagul Fibrinolysis2009;20: 615–18.
Optimal anticoagulant regime in these
patients is still an open question, using heparin with monitoring CCT still leads to significant bleeding complications in certain patients
Widen A, Rolando N, Manousou P,et al.

Larger randomised control studies are need to investigate coagulopathy in liver disease in depth using
viscoelastic tests as ROTEM particularly FIBTEM
and present cut off values to predict thrombosis or bleeding
In depth study of Platelets function not represented by routine lab tests.
Recommendation

New Liver Institute 2015
THANK YOU