co-medications, pre-medication and common diseases in the elderly
DESCRIPTION
Co-medications, pre-medication and common diseases in the elderly. R3 Guo, Shu-lin 92.07.04. Pre-operation Visit Evaluation. Cardio-pulmonary function - PowerPoint PPT PresentationTRANSCRIPT

Co-medications, pre-Co-medications, pre-medication and common medication and common diseases in the elderlydiseases in the elderly
R3 Guo, Shu-linR3 Guo, Shu-lin
92.07.0492.07.04
Pre-operation Visit EvaluationPre-operation Visit Evaluation
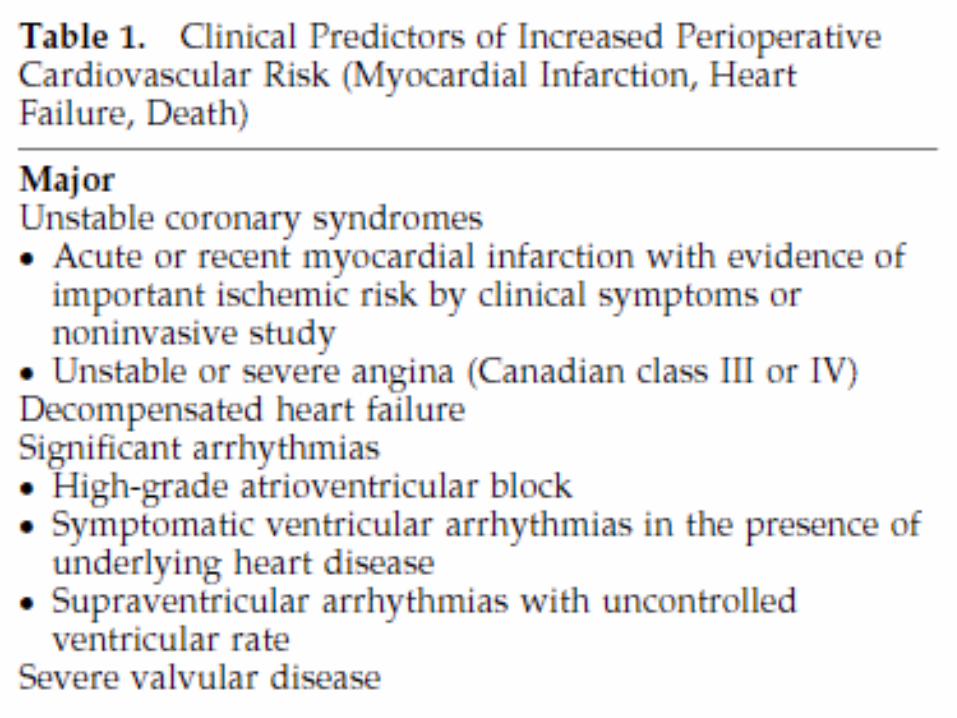
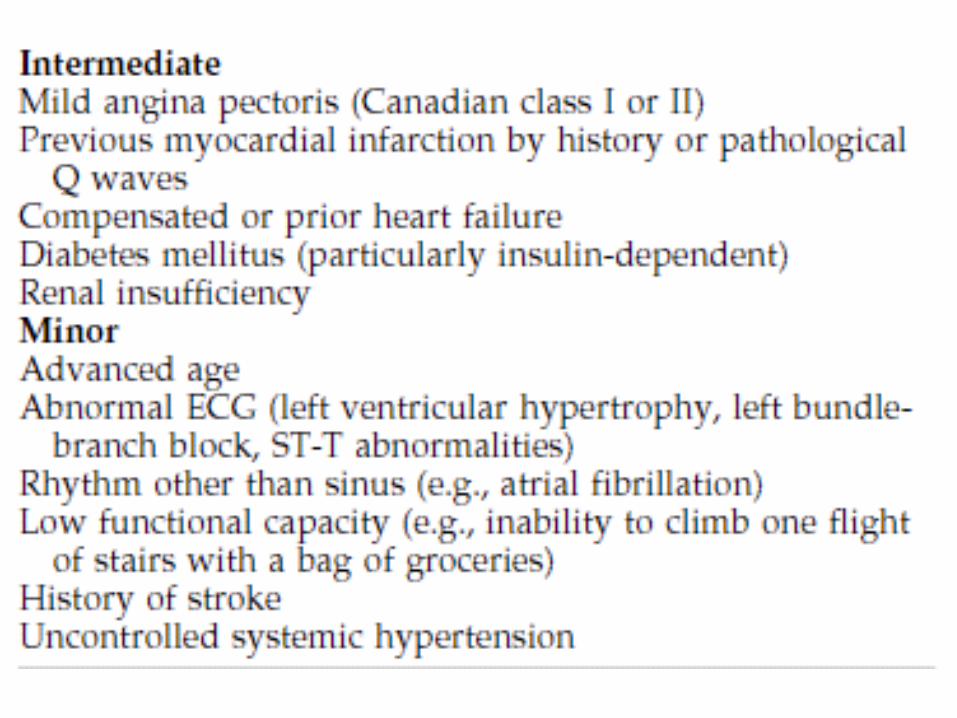
Cardio-pulmonary functionCardio-pulmonary functionThe American Heart Association and the The American Heart Association and the American College of Cardiology guideline American College of Cardiology guideline for cardiovascular evaluation for non-for cardiovascular evaluation for non-cardiac surgery— cardiac surgery— A&A 2002;94:1052-64A&A 2002;94:1052-64

Co-medicationCo-medication
Klugger (1991)— Klugger (1991)— Anaesthsia 1991;46:456-9Anaesthsia 1991;46:456-9
Incidence of concomitant medication was high Incidence of concomitant medication was high and rose steadily with the increase in ageand rose steadily with the increase in age
44% of all patients were given at least one dru44% of all patients were given at least one drugg
On average, patients took 2.1 drugs, especiallOn average, patients took 2.1 drugs, especially in CV fieldy in CV field
About 50% of patients scheduled for surgery, About 50% of patients scheduled for surgery, the regular medication was not given on the dthe regular medication was not given on the day of surgeryay of surgery

Co-medicationCo-medication
Kennedy(2000)— Kennedy(2000)— Br J of Clin Pharma 2000; 49:353-62Br J of Clin Pharma 2000; 49:353-62
The withdrawal of a regular cardiovascular druThe withdrawal of a regular cardiovascular drug for greater than 24 hrs was associated with g for greater than 24 hrs was associated with 14% incidence of cardiac complication14% incidence of cardiac complication
The complication rate showed a correlation wiThe complication rate showed a correlation with time without medicationth time without medication
If the time was over 48hrs, the rate of complicIf the time was over 48hrs, the rate of complication increased to 27%ation increased to 27%


Co-medicationCo-medication
It is generally accepted that at least three It is generally accepted that at least three half-times and ideally five Thalf-times and ideally five T1/21/2
Increasing age is associated with changes Increasing age is associated with changes in Vd, bio-availability, and limitations in renin Vd, bio-availability, and limitations in renal clearance and hepatic functional clearance and hepatic function
Medications associated with acute withdraMedications associated with acute withdrawal effects should be continued throughouwal effects should be continued throughout the perioperative periodt the perioperative period

Cardiovascular drugsCardiovascular drugs
Calcium-channel blockersCalcium-channel blockersBeta-adrenoreceptor blockersBeta-adrenoreceptor blockersAngiotensin-converting enzyme (ACE) inhiAngiotensin-converting enzyme (ACE) inhibitorsbitorsAngiotensin receptor II antagonistsAngiotensin receptor II antagonistsDigoxinDigoxinAnti-arrhythmic therapyAnti-arrhythmic therapyDiureticsDiuretics

Calcium-channel blockersCalcium-channel blockers
Short-acting calcium-channel blockersShort-acting calcium-channel blockers Cause sympathetic activation and increase thCause sympathetic activation and increase th
e risks of MI or heart failuree risks of MI or heart failure Avoid in perioperative period (ex: Verapamil)Avoid in perioperative period (ex: Verapamil)
Long-acting calcium-channel blockersLong-acting calcium-channel blockers No reports on severe complications in the periNo reports on severe complications in the peri
operative periodoperative period Continued on the morning of surgery and throContinued on the morning of surgery and thro
ughout the perioperative period (ex: Novasc)ughout the perioperative period (ex: Novasc)

Beta-adrenoreceptor blockersBeta-adrenoreceptor blockers
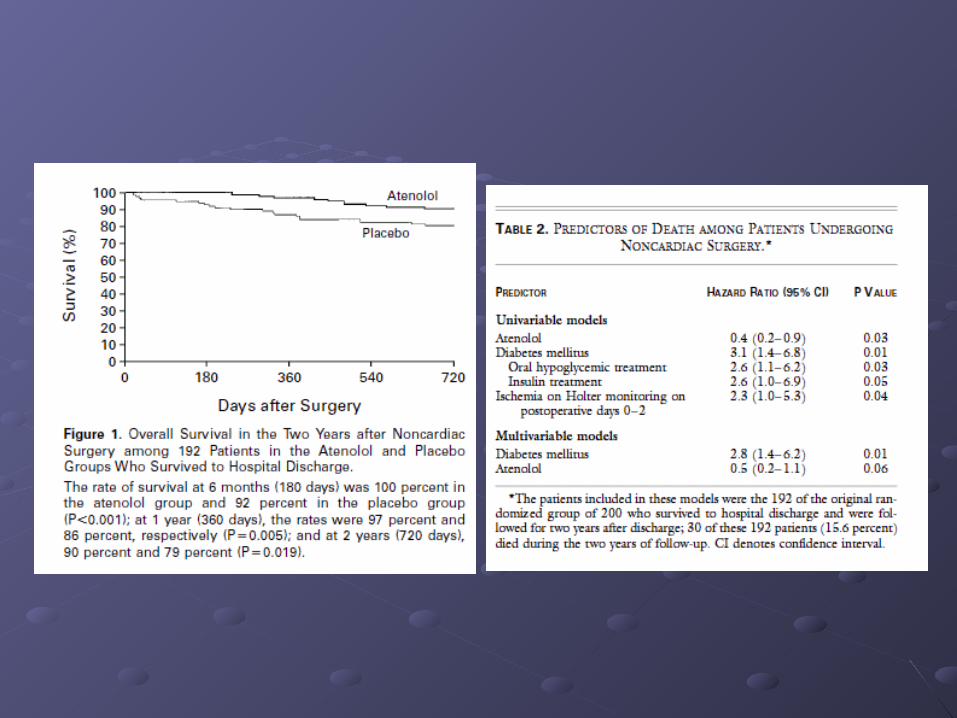
Mangano (1996)— Mangano (1996)— NEJM 1996;335:1713-20NEJM 1996;335:1713-20
Patients with CAD or high risks showed lower mortalitPatients with CAD or high risks showed lower mortality with y with during the perioperative periodduring the perioperative period
Even 2 years after discharge, the mortality in Even 2 years after discharge, the mortality in ββ-blocke-blocker vs. placebo groups is 10% vs. 21%r vs. placebo groups is 10% vs. 21%
Wallace (1998)— Wallace (1998)— Anesthesiology 1998;88:7-17Anesthesiology 1998;88:7-17
Atenolol given prior to or during the induction of anestAtenolol given prior to or during the induction of anesthesia and continued for several days after surgery cahesia and continued for several days after surgery cause a significant in the incidence of perioperative MI use a significant in the incidence of perioperative MI (5-10mg iv, 50 or 100mg po q12hr)(5-10mg iv, 50 or 100mg po q12hr)

Angiotensin-converting enzyme Angiotensin-converting enzyme inhibitorsinhibitors
ACEI can cause a significant reduction in ACEI can cause a significant reduction in the body’s ability to compensate for the body’s ability to compensate for hypotensive episodeshypotensive episodes
The hypotension can be reversed by the The hypotension can be reversed by the volume support or moderate doses of volume support or moderate doses of vasoconstrictorsvasoconstrictors
Withholding ACEI on the morning of Withholding ACEI on the morning of surgerysurgery

Angiotensin receptor II antagonistAngiotensin receptor II antagonist
Brabant(1999)– Brabant(1999)– A&A 1999;89: 1388-92A&A 1999;89: 1388-92
Compared to the incidence and severity of hypotensioCompared to the incidence and severity of hypotension during induction of anesthesian during induction of anesthesia
Angiotensin receptor blocker is the most frequent to cAngiotensin receptor blocker is the most frequent to cause hypotensionause hypotension
Adequate treatment of these often quite severe hypotAdequate treatment of these often quite severe hypotensive episodes could not be achieved by ephedrine ensive episodes could not be achieved by ephedrine but required 1mg boluses of terlipressinbut required 1mg boluses of terlipressin
Angiotensin receptor antagonist should not be given oAngiotensin receptor antagonist should not be given on the day of surgeryn the day of surgery

DigoxinDigoxin
DigoxinDigoxin A narrow therapeutic ratio, is further reduced A narrow therapeutic ratio, is further reduced
by hypokalemiaby hypokalemia Withhold digoxin on the morning of surgery, Withhold digoxin on the morning of surgery,
and reduce the chance for toxicityand reduce the chance for toxicity Continuation of digoxin therapy through the Continuation of digoxin therapy through the
day of surgery and justify their approach by day of surgery and justify their approach by indicating that it provides cardiac stabilityindicating that it provides cardiac stability
Other cardiovascular drugsOther cardiovascular drugs
Anti-arrhythmic therapyAnti-arrhythmic therapy Not withhold these drugs if they are given for Not withhold these drugs if they are given for
a serious conditiona serious condition
DiureticsDiuretics Diuretics therapy should be stopped on the Diuretics therapy should be stopped on the
day of surgeryday of surgery To avoid further volume loss in an already To avoid further volume loss in an already
volume-depleted elderly patientsvolume-depleted elderly patients

InsulinInsulin
During the course of anesthesia and surgery, it iDuring the course of anesthesia and surgery, it is the severe hyperglycemia state that is associats the severe hyperglycemia state that is associated with adverse outcomeed with adverse outcome
Type I (IDDM)Type I (IDDM) Receive insulin during perioperative period Receive insulin during perioperative period 5-10g of glucose per hour and insulin giving depends 5-10g of glucose per hour and insulin giving depends
on blood sugaron blood sugar Keep blood sugar within 110-180 to minimise the risk Keep blood sugar within 110-180 to minimise the risk
of accident hypoglycemiaof accident hypoglycemia


InsulinInsulin
Type II (NIDDM)Type II (NIDDM) OHA should not be given on the day of surgerOHA should not be given on the day of surger
yy A long half-life should be withhold for 48 hrsA long half-life should be withhold for 48 hrs Biguanides (metformin) acts by inhibiting hepaBiguanides (metformin) acts by inhibiting hepa
tic gluconeogenesis and causes a significant itic gluconeogenesis and causes a significant impairment of lactate metabolismmpairment of lactate metabolism
Withhold metformin for at least 24 hrs prior to Withhold metformin for at least 24 hrs prior to surgerysurgery

InsulinInsulin
Minor proceduresMinor procedures With good control (HbAIc<8), short duration cWith good control (HbAIc<8), short duration c
an be performed without glucose supportan be performed without glucose support [Glu]250~300 Insulin 4-6U[Glu]250~300 Insulin 4-6U [Glu]>300 Insulin 6-8U[Glu]>300 Insulin 6-8U
Major proceduresMajor procedures Should receive an insulin-based regime (5-10Should receive an insulin-based regime (5-10
g/hr glu, insulin from 1 U/hr)g/hr glu, insulin from 1 U/hr) Check blood sugar every 1-2 hrs Check blood sugar every 1-2 hrs
Psychotropic medicationsPsychotropic medications
Tricyclic antidepressantsTricyclic antidepressants
Monoamine oxidase inhibitorsMonoamine oxidase inhibitors
LithiumLithium

Tricyclic antidepressantsTricyclic antidepressants
Inhibit the re-uptake of biogenic amines Inhibit the re-uptake of biogenic amines (NE and 5-HT)(NE and 5-HT)Chronic use will cause a reduction in the Chronic use will cause a reduction in the endogenous NE poolendogenous NE poolAnti-cholinergic effects: sedation, urinary Anti-cholinergic effects: sedation, urinary retention, hyperthermia, cardiac retention, hyperthermia, cardiac arrhythmia, and deliriumarrhythmia, and deliriumContinuation of these agents through the Continuation of these agents through the perioperative periodperioperative period

Monoamine oxidase inhibitorsMonoamine oxidase inhibitors
Not to block the re-uptake, but inhibit their Not to block the re-uptake, but inhibit their metabolismmetabolism
Chronic use will result in reduced Chronic use will result in reduced neurotransmitters and an accumulation of neurotransmitters and an accumulation of the false neurotransmittersthe false neurotransmitters
Side-effect is orthostatic hypotensionSide-effect is orthostatic hypotension
Adverse interaction of MAOI is with opioid, Adverse interaction of MAOI is with opioid, especially meperidineespecially meperidine
Monoamine oxidase inhibitorsMonoamine oxidase inhibitors
The use of meperidine in the patients with The use of meperidine in the patients with chronic use of MOAI causes excitatory chronic use of MOAI causes excitatory reaction due to inhibition of 5-HT re-uptakereaction due to inhibition of 5-HT re-uptake
Recent expert opinion recommends Recent expert opinion recommends continuation of the treatment with MAOI, continuation of the treatment with MAOI, but with consideration of certain drug but with consideration of certain drug interactionsinteractions
LithiumLithium
Li produces an antagonism to ADHLi produces an antagonism to ADHThis causes polyuria and hypovolemiaThis causes polyuria and hypovolemiaIn the presence of Li, non-depolarising NM In the presence of Li, non-depolarising NM blocker might be prolongedblocker might be prolongedHigh Li cause sedation, muscle weakness, High Li cause sedation, muscle weakness, hypotension, wide QRS complex, seizure hypotension, wide QRS complex, seizure and comaand comaCessation of Li 24 hrs before minor surgerCessation of Li 24 hrs before minor surgery and 2-3 days in major proceduresy and 2-3 days in major procedures

Anti-parkinson medicationAnti-parkinson medication
The withdrawal of levodopa therapy may cThe withdrawal of levodopa therapy may cause an exacerbation of symptoms of Parkause an exacerbation of symptoms of Parkinson’s disease and possibly a neuroleptic inson’s disease and possibly a neuroleptic syndromesyndromeLevodopa is with a short elimination half-tiLevodopa is with a short elimination half-time and a short acting timeme and a short acting timeLevodopa should be given in the morning Levodopa should be given in the morning of surgery and continued throughout the pof surgery and continued throughout the perioperative period.erioperative period.
Question ?Question ?