cmh cancer program 2010 annual report
DESCRIPTION
Cancer Committee Chair‟s Report p.5Cancer Registry Report p.7Oncology Nursing Report p.9Lymphedema Program Report p.10Palliative Care Program Report p.11Multidisciplinary Cancer Conferences for 2010 p.15Primary Site Table for 2010 Cases p.17CMH Lung Cancer, 2006—2010 p.18CMH Cancer Resource Center Services p.302010 Cancer Committee Members p.32Glossary 33TRANSCRIPT
2010 Annual Report
CM
H C
an
ce
r P
rog
ram

Mission
To Heal, Comfort and Promote Health for the Communities We Serve.
Vision
To be the regional health system of choice for patients,
physicians and employees by providing the latest treatments. To be a valued community treasure.
Value Integrity, Excellence,
Caring and Transparency.


Contents
20
10
CM
H C
an
ce
r P
rog
ram
An
nu
al
Re
po
rt
Cancer Committee Chair‟s Report 5
Cancer Registry Report 7
Oncology Nursing Report 9
Lymphedema Program Report 10
Palliative Care Program Report 11
Multidisciplinary Cancer Conferences for 2010 15
Primary Site Table for 2010 Cases 17
CMH Lung Cancer, 2006—2010 18
CMH Cancer Resource Center Services 30
2010 Cancer Committee Members 32
Glossary 33
4
Cancer Committee Chair’s Report
20
10
CM
H C
an
ce
r P
rog
ram
An
nu
al
Re
po
rt
For patients suddenly facing the many uncertainties of cancer, knowing that they are receiving state of the art cancer care is very reassuring. At CMH, we are dedicated to providing excellent, high-quality care to our patients with both solid tumors and hematologic malignancies. This annual report highlights a few of the Cancer Program‟s activities of the past year. A major focus of the cancer program is to provide high quality multidisciplinary cancer treatment in our community. In November, the Coastal Communities Cancer Center opened its doors for both Radiation Oncology and Medical Oncology. The Cancer Resource Center, Radiology and Gynecology/Oncology are scheduled to open in early 2011. Once completed, this multidisciplinary center will combine many facets of oncology care in one location. Our weekly tumor board, which meets every Wednesday at noon, brings together the expertise of surgeons, medical oncologists, radiation oncologists, radiologists and pathologists to discuss individual cases. Many primary care physicians attend as well, when their own patients are discussed or simply for the continuing education. Another important ambition of the cancer program is to provide the supportive care to cancer patients. The inpatient Palliative Care Program has continued to grow this year providing a valuable service to both our patients and our physicians. Dr. Charles Pankratz was hired as the full-time director of the Palliative Care Program and a full-time dedicated chaplain was added. Outpatient support and survivorship goals are provided through the Cancer Resource Center in conjunction with the American Cancer Society and The Wellness Community. In 2010, the Cancer Resource Center added a lymphedema support group, a lymphedema therapist, a social worker and the Creativity Central art class. A grant is being pursued to fund additional services in 2011. Community outreach is an ongoing commitment. The Cancer Resource Center provides cancer education, support groups and, in general, is an invaluable resource for our community. CMH continues to provide cancer outreach programs for cervical cancer screening and mammography through the Healthy Women‟s Program. In October, the 5th annual community directed cancer education seminar was held; this year the multidisciplinary panel discussed “How the Environment Impacts Cancer.” A comprehensive website for the Cancer Program was launched which focuses on The Breast Center, The Prostate Institute, The Cancer Resource Center, and the Healthy Women‟s Program.
5

Cancer Committee Chair’s Report
20
10
CM
H C
an
ce
r P
rog
ram
An
nu
al
Re
po
rt
6
CMH maintains its own extensive tumor registry. Our data is transmitted to both the National Cancer Data Base and the California Cancer Registry. This data is the source for much of the information presented in this Annual Report. We are beginning to use this data for measuring cancer outcomes at CMH, which are compared to published guidelines and other community hospitals across the nation. According to this data, lung cancer is the third most commonly diagnosed cancer at CMH. So, we have dedicated this Annual Report to an overview of lung cancer and how it affects our community. I hope you find this information valuable. Lynn Kong, MD Chairman, Cancer Committee, CMH
CMH Cancer Committee Meeting

Cancer Registry Report
20
10
CM
H C
an
ce
r P
rog
ram
An
nu
al
Re
po
rt
In 2010, a total of 1007 cancer cases were accessioned into the cancer registry‟s computerized database. Of those, 814 were newly diagnosed and/or treated cancer cases. The remaining 193 cases were previously diagnosed and/or treated elsewhere but came to CMH for subsequent care. The five leading sites of new cancer at CMH in 2010 were breast (20%), prostate (17%), lung (10%) melanoma (8%), and colorectal (7%). With a reference date of January 1, 2006 the Community Memorial Hospital (CMH) Cancer Registry data base now has five years of complete data. This data includes information about the diagnostic work-up, primary site of origin, stage of disease at diagnosis, first course treatment and survival of all CMH cancer cases. The Cancer Registry data is available to CMH physicians to evaluate the effectiveness of early diagnosis, treatment and survival. Hospital administrators use the cancer registry data to assess the community‟s needs for services and public education. Staff physicians are encouraged to access the data available in the Cancer Registry. Requests for data can be made by calling (805) 652-5459. In 2010 the CMH Cancer Registry data was transmitted to the National Cancer Data Base (NCDB). All of the records transmitted met the NCDB quality acceptance criteria with zero data quality problems. Using the comparative data available from the NCDB Cancer Program Practice Profile Reports (CP3R) our cancer committee was able to evaluate adjuvant treatment for both breast and colon cancer cases. This has been a valuable tool for the CMH Cancer Committee to monitor quality of patient care. In addition to providing data to our medical staff, hospital administrators and the NCDB, the data is also used exhaustively by the California Cancer Registry through a state-mandated cancer reporting law. During 2010, the CMH Cancer Registry consistently exceeded the accuracy and timeliness standards set by the California Cancer Registry. Chris Wilborn, CTR Cancer Registrar
7

Cancer Registry Report
20
10
CM
H C
an
ce
r P
rog
ram
An
nu
al
Re
po
rt
8
Comparison of 2010 Major Site Distribution
Primary Site Community
Memorial California United States
Breast 20% 13% 14%
Prostate 17% 14% 14%
Lung 10% 12% 15%
Melanoma 8% 5% 5%
Colon & Rectum 7% 9% 9%
Cancer Survivors Day 2010
Oncology Nursing Report
20
10
CM
H C
an
ce
r P
rog
ram
An
nu
al
Re
po
rt
CMH has a 36 bed Medical/Surgical Oncology Department. We currently have 19 trained chemotherapy nurses that provide care to patients on the unit, including 2 that are OCN certified. There are also 3 Oncology trained nurses who work in the ICU/CCU areas that are licensed to administer chemotherapy. Many of the nurses have delivered care to our patient population for greater than 10 years and are proficient in all aspects of care encompassing the patient‟s diagnosis, treatment, symptom management, and death. For safety purposes we make every attempt to deliver care to our Oncology patients on the Oncology unit; however, when necessary, due to the patient‟s condition, our nurses can provide safe care throughout the facility. Each year we offer an Oncology Skills Lab to ensure staff remain proficient in the safe delivery of care to the patient , update the staff‟s skill level, and increase knowledge awareness in the field of Oncology. This skills lab is mandatory for all chemotherapy nurses and attendance encouraged to all members of the Department. Every other year, we plan to provide a half to full day Oncology Seminar as a continuing learning experience for the staff. Florence Roach, R.N. Director, 6th Floor Oncology Nursing
9
CMH Cancer Survivors Quilt
Lymphedema Program Report
20
10
CM
H C
an
ce
r P
rog
ram
An
nu
al
Re
po
rt
10
The Cancer Program in conjunction with Rehabilitation Services added the Lymphedema Program in August 2010. The Lymphedema Program serves patients with lymphedema as a result of cancer surgery involving lymph node dissection and/or radiation therapy. Lymphedema is the abnormal accumulation of lymph fluid in a body part due to obstruction of or insult to the transport capability of lymph fluid through the lymphatic system. Associated swelling of most commonly the arm(s) or leg(s) can result in discomfort, motion restriction, infection, and fitting problems with clothing and shoes. The current standard of care is Complete Decongestive Therapy (CDT), an intervention comprised of manual lymph drainage, compression therapy, exercises, and skin care. Education in self care and life time management of the condition is emphasized and assistance with compression garments and related specialty products is provided. Treatment is typically provided in 2 phases and lasts between 4-8 weeks. CDT is provided by a LANA- certified lymphedema therapist with twenty plus years of experience in the rehabilitation field. The Lymphology Association of North America established strict standards that have been set forth to establish minimum criteria to certify adequate competency in the treatment of lymphedema. The prevalence of lymphedema is getting more and more recognition and the Lymphedema Program is reaching out to the medical community as well as the public at large to provide information about risk reduction, early intervention, and treatment. At CMH, our focus is on the patient and his/her individual needs. No lymphedema patient
is exactly the same and we take particular care in addressing each person‟s unique
circumstance.
Claudia Steele-Major, PT, CLT Rehabilitation Services

Palliative Care Program Report
20
10
CM
H C
an
ce
r P
rog
ram
An
nu
al
Re
po
rt
The creation of the Palliative Care services is really a wonderful story. It reflects the best attributes of our community hospital, including commitment to patient care, innovation and teamwork. It is also a profoundly personal story, which has enhanced so many of us who were fortunate to be a part of its founding. But I am getting ahead of myself. Back in 2007, the CMH Cancer Committee was striving to have our hospital become an accredited comprehensive cancer program. As part of this effort, the committee began to explore the possibility of creating a formal Palliative Care service. They began by asking “What exactly is Palliative Care?” Over the next several months, they agreed on a forward thinking and holistic definition of Palliative Care. They decided that a Palliative Care service should improve the quality of life of patients and their families facing the challenges associated with life limiting illnesses. Palliative Care, they agreed, should also assess and expertly treat a patient‟s pain and other physical, psychosocial and spiritual issues. In addition, modern Palliative Care uses a novel interdisciplinary team approach which includes doctors, nurses, social workers and chaplains. It is truly whole person care delivered by professionals dedicated to improving the lives of patients facing serious illness. They then asked: “When can we start?” Since Palliative Care is really a team approach to patient care, so too the creation of our Palliative Care service was also a team effort. Five of us, including the hospital‟s CFO, Mr. Dave Glyer, and our hospital chaplain, Reverend Curtis Hotchkiss, travelled to the UC San Francisco Medical School to become immersed in the details of creating a new service. On our return, we selected the exceptionally qualified director of social service and case management, Ms. Bonnie Subira, to become the administrative director of our service. Over the next year, we subsequently hired the talented Janine Coronado, and a superb clinical nurse coordinator, Diana Jaquez. Reverend Curtis brought on Reverend Megan Delahanty, a uniquely kind and compassionate professional. But what about the doctor‟s role? Our program was an organic effort developed from our local talent, and we reached an early decision to have a team of committed physicians rotate weekly onto the Palliative Care service. Our doctors included two exceptional internal medicine hospitalists, Dr. Tara Snow and Dr. Deborah Carlson, two practicing hospice specialists, Dr. Lanyard Dial (Livingston Memorial Hospice) and Dr. Charles Pankratz (Assisted Home Hospice), and myself. Our group met regularly and taught one another skills and techniques to deliver high-quality inpatient Palliative Care.
11

Palliative Care Program Report
20
10
CM
H C
an
ce
r P
rog
ram
An
nu
al
Re
po
rt
12
Our service formally began operation in September 2008. With strong support from our hospital‟s private physicians, we began seeing a wide variety of patients from birth to advanced old age. As an evolving program, we have seen impressive growth and commitment to quality. In 2010, the Palliative Care Service (PCS) saw a continued increase in consults with 368 patients. It became clear that our service had expanded so that we needed a full time Palliative Care physician to meet our patients‟ needs. In December 2010, after an extensive national search, our own Dr. Chuck Pankratz became our hospital‟s first full-time Board-certified Palliative Care physician. Along with Bonnie, Diana, Janine, and Megan, our service now truly reflects the team spirit and the clinical excellence which was our goal to create. We are also fortunate to have three other team physicians achieve board certification this year. This is evidence of our commitment to maintain and exceed the national standards for Palliative Care. As we refine our service to meet the needs of the community, we utilize surveys submitted to patients, families and physicians. Our 2010 patient/family satisfaction surveys continue to show improvement in areas that align us with national quality outcomes. Compared to 2009, areas of dramatic improvement include comprehensive symptom management, spiritual/emotional support, and advanced care planning.
2009/2010 Palliative Care Service
Physician Satisfaction
Survey Results
82%
84%
86%
88%
90%
92%
94%
96%
98%
100%
2009 2010
Good Care
Respond Timely
Symptoms Well Controlled
Clarify Wishes
Pt/Family Communication
Psychsoc/ Spiritual
Comm. With you
Palliative Care Program Report
20
10
CM
H C
an
ce
r P
rog
ram
An
nu
al
Re
po
rt
Palliative Care continues to participate in performance improvement projects. Over the last year the PCS has developed and implemented a Comfort Measures physician order set in collaboration with Pharmacy services and Oncology physicians. These order sets are hospital-wide and available to all physicians, which provide consistent comfort and dignity for all terminally ill patients. We are also actively participating in the develop-ment of protocols for ICU and pediatric palliative patients. Education is a primary role of the Palliative Care Service. Our team is committed to serve as a resource for our patients and the health care community beyond inpatient medical consultations. Palliative Care RN‟s strive to be available on the medical-surgical floors and in the ICU to assist with evaluation of potential Palliative Care patients. Their support includes one-on-one educational and patient care support for their nursing colleagues. The Palliative Care physician assists in symptom management as a clinical consultant. He frequently meets with the Pharmacy Services to expand the formulary and routes of administration of medications for effective symptom management by all treating physicians. Care planning for the acutely or chronically debilitated is a challenging and unanticipated need. Our Palliative Care Social Worker provides information and support to patients and families as they assess personal and financial resources to optimize care and support for the patient. In 2010, we now provide comprehensive Palliative Care services with the addition of a chaplain devoted exclusively to our consultation team.
13
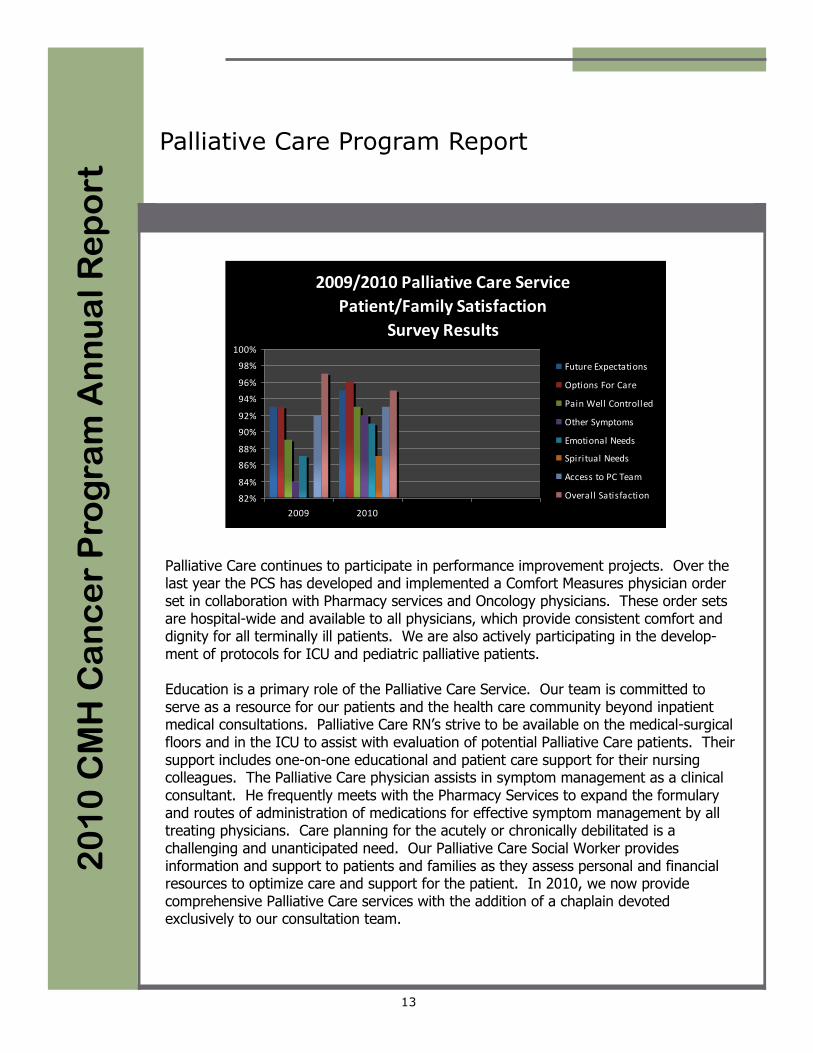
2009/2010 Palliative Care Service
Patient/Family Satisfaction
Survey Results
82%
84%
86%
88%
90%
92%
94%
96%
98%
100%
2009 2010
Future Expectations
Options For Care
Pain Well Controlled
Other Symptoms
Emotional Needs
Spiritual Needs
Access to PC Team
Overall Satisfaction

Palliative Care Program Report
20
10
CM
H C
an
ce
r P
rog
ram
An
nu
al
Re
po
rt
14
Outside the hospital, we continue our community commitment while working with Independent Living, Assisted Living and Skilled Nursing facilities to identify areas for Palliative Care screening and coordination of care. Education about and implementation of the POLST (Physician Orders for Life-Sustaining Treatment) document reflects our ongoing goal to improve advanced care planning to reflect the patient‟s goals and expec-tations for treatment. Our team members are also involved in multiple projects to con-tinue the development and improvement of Palliative Care at both the regional and na-tional levels. As we look forward, the Palliative Care service strives to expand our inpatient services with a goal of a 50% increase in team consultations. When the terms for national accreditation are finalized we will pursue our need and eligibility to standardize our level of services. We will continue to align our efforts with the Cancer Center to enhance the Palliative Care services outreach to physicians, the public, healthcare facilities and other organizations in our community. To address the needs of our increasing role in patient and family care we plan expansion of our Palliative Care services to patients outside the hospital. Although Palliative Care is our nation‟s newest medical specialty, it is fundamentally a specialty uniquely focused on helping people. Those of us who were fortunate to see this program grow know we could not have done so without the ongoing support of many wonderful people: Dr. Marty Pops and the entire CMH Board of Trustees, Mr. Gary Wilde and the helpful administrative staff, Dr. Lynn Kong and the Cancer Committee and, of course, our patients and their families. Ultimately, we of the CMH Palliative Care team find our strength and motivation in being of service to our friends and our neighbors whenever they need us, want us, or call us. Jim Hornstein, MD Founding Medical Director CMH Palliative Care Service
CMH Palliative Care Team
Cancer Conferences
20
10
CM
H C
an
ce
r P
rog
ram
An
nu
al
Re
po
rt
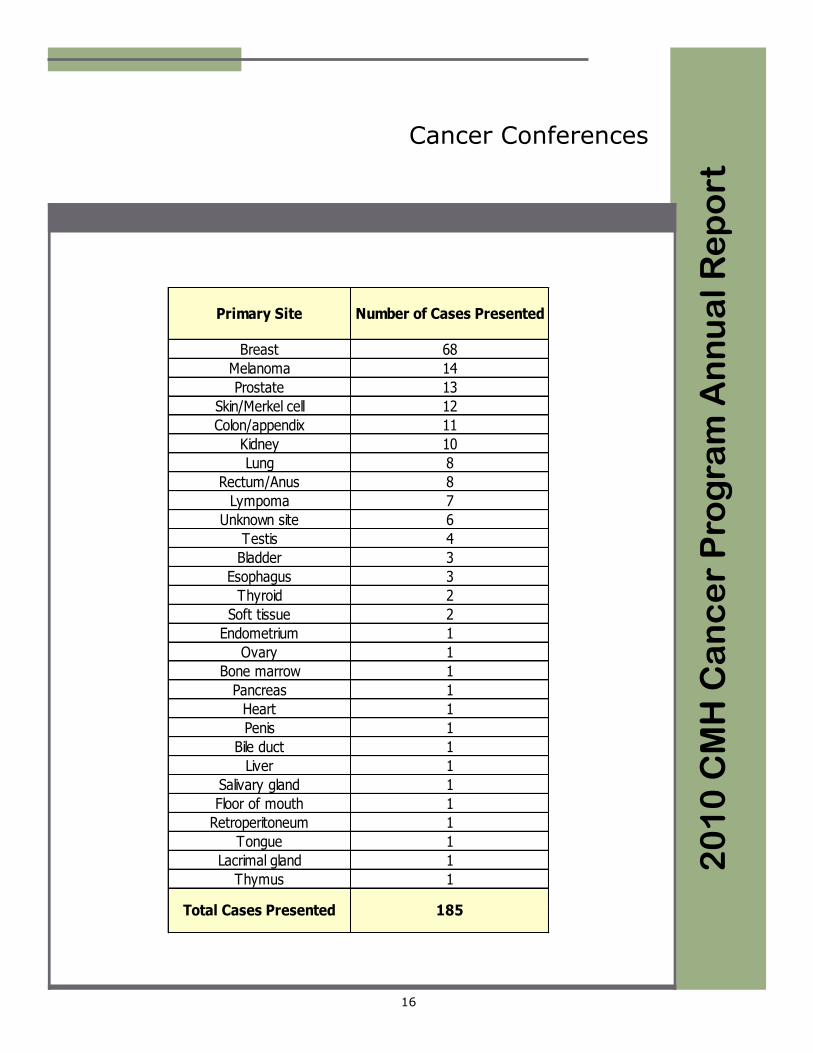
Cancer Conferences (Tumor Boards) at Community Memorial Hospital are held weekly. Cancer conferences are both multidisciplinary and patient-oriented. Presentations serve both educational and consultative purposes with the focus on diag-nosis, staging, treatment strategy, including use of National Comprehensive Cancer Network (NCCN) treatment guidelines, and follow up. In 2010, Community Memorial held 49 Cancer Conferences. Of these, 48 were general cancer conferences and one was an educational cancer conference. One hun-dred eighty-five (185) cases were presented and of those, one hundred sixty-four (164) cases were prospective presentations. In 2010, one continuing medical education presentation was held on a cancer related topic. That presentation was: 03/31/2010 „Votrient (Pazopanib) for Advanced Renal Cell Carcinoma‟ Sopida Cheundarndee, PharmD. GlaxoSmithKline The table on the following page shows the number of cases per site that were presented to Cancer Conference at CMH in 2010. Kevin Chang, M.D. Medical Oncology Cancer Conference Moderator
15
CMH Cancer Conference Meeting
Cancer Conferences
20
10
CM
H C
an
ce
r P
rog
ram
An
nu
al
Re
po
rt
16
Primary Site Number of Cases Presented
Breast 68
Melanoma 14
Prostate 13
Skin/Merkel cell 12
Colon/appendix 11
Kidney 10
Lung 8
Rectum/Anus 8
Lympoma 7
Unknown site 6
Testis 4
Bladder 3
Esophagus 3
Thyroid 2
Soft tissue 2
Endometrium 1
Ovary 1
Bone marrow 1
Pancreas 1
Heart 1
Penis 1
Bile duct 1
Liver 1
Salivary gland 1
Floor of mouth 1
Retroperitoneum 1
Tongue 1
Lacrimal gland 1
Thymus 1
Total Cases Presented 185

2010 Site Table 2
01
0 C
MH
Ca
nc
er
Pro
gra
m A
nn
ua
l R
ep
ort
17
Total
Cases Analytic NonAn Male Female Stage 0 Stage I Stage IIStage IIIStage IV N/A Unk
ALL SITES 1008 814 194 544 464 70 221 199 104 112 68 40
Tongue 5 4 1 4 1 0 2 0 0 1 0 1
Salivary Glands, major 1 1 0 1 0 0 0 1 0 0 0 0
Floor of Mouth 1 1 0 1 0 0 0 0 1 0 0 0
Tonsil 2 1 1 1 1 0 0 0 0 0 0 1
Hypopharynx 1 1 0 0 1 0 0 0 0 1 0 0
Esophagus 5 3 2 4 1 0 0 0 0 2 0 1
Stomach 9 8 1 8 1 0 2 2 0 3 0 1
Small Intestine 2 2 0 2 0 0 0 0 1 1 0 0
Colon 51 47 4 22 29 1 10 12 13 9 0 2
Rectum & Rectosigmoid 13 10 3 8 5 0 5 1 2 0 0 2
Anus, Anal Canal & Anorectum 3 3 0 0 3 1 0 1 1 0 0 0
Liver 8 6 2 6 2 0 0 1 2 2 0 1
Bile Ducts 1 1 0 1 0 0 0 0 0 1 0 0
Pancreas 11 11 0 5 6 0 4 1 1 4 0 1
Peritoneum, Omentum, Mesent 3 3 0 0 3 0 0 0 0 1 1 1
Other Digestive 1 1 0 0 1 0 0 0 0 0 1 0
Larynx 2 2 0 1 1 0 1 0 0 1 0 0
Lung/Bronchus-sm cell 14 14 0 4 10 0 0 3 1 10 0 0
Lung/Bronchus-non sm cell 72 66 6 32 40 1 17 5 9 34 0 0
Pleura 2 2 0 1 1 0 1 1 0 0 0 0
Other Resp & Thoracic 1 1 0 0 1 0 0 0 1 0 0 0
Leukemia 21 17 4 13 8 0 0 0 0 0 17 0
Myeloma 6 4 2 3 3 0 0 0 0 0 4 0
Other Hematopoietic 14 10 4 6 8 0 0 0 0 0 10 0
Soft Tissue 2 2 0 2 0 0 0 0 1 0 1 0
Melanoma of Skin 69 67 2 46 23 17 31 10 5 1 0 3
Other Skin CA 2 2 0 1 1 0 1 0 0 1 0 0
Breast 171 163 8 3 168 32 57 38 22 6 0 8
Cervix Uteri 6 5 1 0 6 0 2 0 3 0 0 0
Corpus Uteri 28 28 0 0 28 0 20 2 4 1 1 0
Uterus NOS 1 1 0 0 1 0 0 0 0 1 0 0
Ovary 20 14 6 0 20 0 2 2 7 2 0 1
Vagina 6 3 3 0 6 0 2 0 1 0 0 0
Vulva 8 5 3 0 8 1 4 0 0 0 0 0
Other Female Genital 3 2 1 0 3 0 0 0 2 0 0 0
Prostate 269 139 130 269 0 0 12 100 19 6 0 2
Testis 10 7 3 10 0 0 5 0 1 0 0 1
Bladder 34 33 1 29 5 15 9 1 2 0 0 6
Kidney and Renal Pelvis 23 23 0 14 9 0 12 2 1 5 1 2
Ureter 2 2 0 2 0 2 0 0 0 0 0 0
Eye 1 1 0 1 0 0 0 0 0 0 1 0
Brain 6 6 0 2 4 0 0 0 0 0 6 0
Other Nervous System 9 8 1 4 5 0 0 0 0 0 8 0
Thyroid 37 34 3 8 29 0 18 5 4 3 0 4
Other Endocrine 1 1 0 0 1 0 0 0 0 0 1 0
Hodgkin's Disease 3 3 0 2 1 0 0 2 0 0 0 1
Non-Hodgkin Lymphoma 31 30 1 17 14 0 4 9 0 16 0 1
Unknown or Ill-Defined 17 16 1 11 6 0 0 0 0 0 16 0
Class SexSite
Stage

CMH Lung Cancer, 2006-2010
20
10
CM
H C
an
ce
r P
rog
ram
An
nu
al
Re
po
rt
18
We decided to dedicate this CMH Annual Report to a discussion of Lung Cancer. According to the American Cancer Society, an estimated 221,130 new cases of lung cancer are expected in 2011. Lung cancer is the second most commonly diagnosed malignancy for both men and women, and the leading cause of cancer deaths for both sexes. At CMH, 80 new cases of lung cancer were diagnosed in 2010, which is slightly fewer than in previous years (Figure 1). The mean and median age at diagnosis was 72 years and 74 years, respectively (Figure 2). The majority of cases were diagnosed in Caucasians (Figure 3). Men were diagnosed more frequently than women (52% vs. 48%), which correlates well with national statistics.
CMH 2006-2010 Analytic Lung Cancer Cases Shown by Year of Diagnosis
80
87
83
83
92
0 20 40 60 80 100Number of Cases
Figure 1
2006
2007
2008
2009
2010
CMH 2006-2010 Analytic Lung Cancer Cases Shown by Age of Diagnosis
11
36
106
154
109
8
0
20
40
60
80
100
120
140
160
180
200
Nu
mb
er o
f C
ases
40-49
50-59
60-69
70-79
80-89
90-99
Figure 2

CMH Lung Cancer, 2006-2010
20
10
CM
H C
an
ce
r P
rog
ram
An
nu
al
Re
po
rt
19
The majority of diagnoses were confirmed by histology or cytology, but 5.7% of diagnoses were given presumptively based on radiographic or clinical findings. The most common methods to obtain tissue for diagnosis include thoracentesis, bronchoscopy, CT guided biopsy, mediastinoscopy or surgical biopsy. All methods are available at CMH. Adenocarcinoma was the most common histology diagnosed, followed by squamous cell carcinoma. Approximately 10.8% of the non-small cell carcinomas could not be further classified (Figure 4). Only 13.4% of the lung cancers were small cell carcinoma, which is consistent with national trends.
CMH 2006-2010 Analytic Lung Cancer CasesShown by Race/Ethnicity
Figure 3
86.4%
0.2%
1.9%0.2%
0.5%
1.4%
0.2%8.7%
0.5%
Caucasian
Chinese
Filipino
Black
Uknown
Asian NOS
Pacific Islander
Hispanic
Japanese
CMH 2006-2010 Analytic Lung Cancer CasesShown by Histologic Type
Pleomorphic (0.2%)
Papillary (0.2%)
Mucinous Bronchiolo-Alveolar (0.5%)
Mixed adenocarcinoma (0.5%)
Carcinoid (1%)
Adenosquamous (1%)
Bronchiolo-Alveolar (1.7%)
Mucinous (1.9%)
Neuroendocrine (1.9%)
Carcinoma NOS (10.8%)
Small Cell (13.4%)
Non-small cell (19.2%)
Squamous cell (21.8%)
Adenocarcinoma (25.9%)
Figure 4

CMH Lung Cancer, 2006-2010
20
10
CM
H C
an
ce
r P
rog
ram
An
nu
al
Re
po
rt
20
Treatment of lung cancer depends on the histology and the stage at diagnosis. For non-small cell lung carcinoma, the mainstay of treatment remains surgical resection if the lung cancer is diagnosed at an early stage. Since 2006, only 25.4% of cases were diagnosed at stage I or II (Figure 5). Occasionally patients with stage III disease are candidates for surgery; 26.8% presented with stage III disease according to our database. Figure 6 shows a comparison of stage at diagnosis for CMH, California and all states.
CMH 2006-2010 Analytic Lung Cancer CasesShown by AJCC Stage at Diagnosis
Figure 5
0.5%
44.2%26.8%
5.4%
20.0%
0.5%
2.6%
Stage 0
Stage I
Stage II
Stage III
Stage IV
Stage Not Appl
Stage Unknown
Non-Small Cell Lung Cancer Cases Stage at Diagnosis CMH Compared to Comprehensive Hospitals in All
States and California, Class of Case 1 and 2, 2006-2008
0
5
10
15
20
25
30
35
40
Pe
rce
nt
Figure 6
CMH 0.0 23.0 5.1 30.1 37.8 0.0 4.1
California 0.2 22.5 5.2 21.1 4.1 0.0 16.7
All States 0.1 24.1 6.4 22.3 34.0 1.1 12.7
Stage 0 Stage I Stage II Stage III Stage IV OC Unknown

CMH Lung Cancer, 2006-2010
20
10
CM
H C
an
ce
r P
rog
ram
An
nu
al
Re
po
rt
21
In total, 28.2% of patients with newly diagnosed lung cancer underwent surgery, either alone or in conjunction with chemotherapy and radiation (Figure 7). Lobectomy, with or without mediastinal lymph node dissection, was the most frequent surgery performed (Figure 8). Chemotherapy can be administered in a neo-adjuvant approach, to down-size a tumor and allow surgical resection, or in an adjuvant setting, following surgery, in patients who are at high risk of relapse.
CMH 2006-2010 Analytic Lung Cancer Cases Shown by First Course of Treatment
62
79
64
51 4
88
1
116
0
20
40
60
80
100
120
Number of Cases
Figure 7
Surgery
Chemo
Radiation
Surg/Chemo
Surg/Rad
Surg/Rad/Chemo
Rad/Chemo
Chemo/Horm
No Treatment
CMH 2006-2010 Analytic Lung Cancer CasesShown by Type of Surgery
Figure 8
83.0%
0.2%0.2%
2.1%0.5%8.0%5.7%
0.2%
Cryoablation Wedge Resection Segmental Resection NOS
Lobectomy Lobectomy & Med LN diss Pneumonectomy & Med LN diss
Lung Resection NOS No Surgery

CMH Lung Cancer, 2006-2010
20
10
CM
H C
an
ce
r P
rog
ram
An
nu
al
Re
po
rt
22
However, the majority of patients present with advanced disease. According to the SEER data, 56% of patients nationally present with distant metastasis. At CMH, 44% of newly diagnosed patients presented with distant metastasis (Figure 5). Chemotherapy or radiation therapy can be administered to control symptoms or improve survival, but treatment remains palliative and cannot cure this disease. As depicted in Figure 7, 36.4% of patients were treated with chemotherapy alone or in conjunction with radiation. Approximately 25% of patients elected supportive care only for their lung cancer. The focus of lung cancer treatment is shifting from a generalized one-size-fits-all approach to a more personalized approach based on histology and tumor specific molecular targets. For example, chemotherapy regimens have been identified that perform better in specific histology subtypes. Alimta (Pemetrexed), a standard chemotherapy drug, has better efficacy in non-squamous cell histology. Avastin (Bevacizumab), a monoclonal antibody targeting angiogenesis, improves survival in non-small cell lung cancer when added to standard chemotherapy (squamous cell carcinomas are excluded due to an increased risk of hemoptysis). Tarceva (Erlotinib), an epidermal growth factor (EGFR) inhibitor, is as effective as standard chemotherapy in tumors that express EGFR.
CMH 2006-2010 Analytic Lung Cancer Cases Shown by Small Cell versus Non-Small Cell
Histology and Vital Status
56
262
8
98
Nu
mb
er
of
Cas
es
Small Cell Non-Small CellFigure 9
Alive
Deceased

CMH Lung Cancer, 2006-2010
20
10
CM
H C
an
ce
r P
rog
ram
An
nu
al
Re
po
rt
23
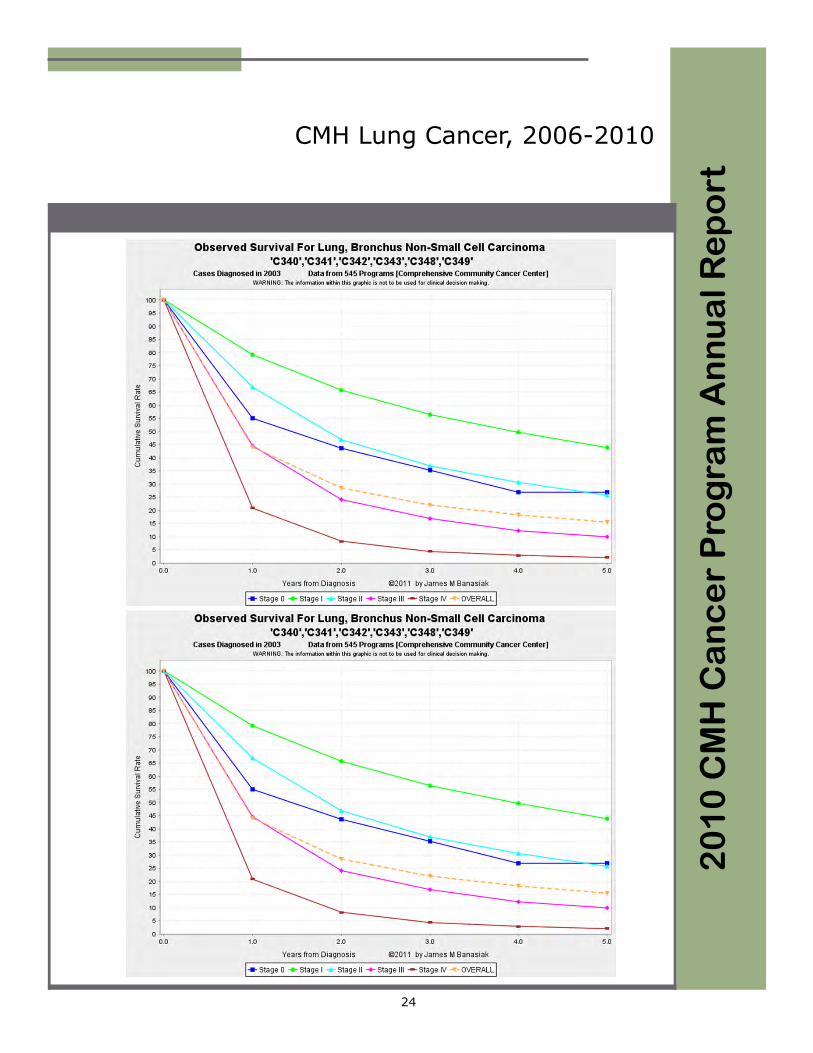
Clinical trials are continually seeking new treatments which may offer better response rates, longer survival or fewer side effects. Several clinical trials are available locally through Ventura County Hematology Oncology Specialists for first, second or third line non-small cell lung cancer. A complete list of clinical trials available nationally is available through the National Cancer Institute (NCI) website. The overall 5 year survival for lung cancer, according to national SEER data, is 16%. Our 5 year survival data (2006-2010) for all lung cancers diagnosed at CMH is 25% (Figure 9). Figure 10 depicts the survival curves of all lung cancer patients here at CMH by stage at diagnosis from 2006 to 2010. Although longer follow-up is needed, our statistics are in keeping with the national averages (Figure 11 & 12). Our ability to treat, and possibly cure, lung cancer depends upon diagnosing it at an early stage or preventing its development. The value of screening high risk populations continues to be investigated. There are 2 clinical trials currently open through the NCI looking at screening high risk people with low dose CT scans and biomarkers. Six prevention studies are available for present or prior smokers. Primary prevention, namely smoking cessation, is vital. Lynn Kong, MD Medical Oncology
Observed Survival forCMH 2006-2010 Analytic Lung Cancer Cases
Figure 10
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 1 2 3 4 5
Years from Diagnosis
Cu
mu
lati
ve S
urv
ival
Rat
e All Stages
Stage 0
Stage I
Stage II
Stage III
Stage IV
Not appl
Unknown
CMH Lung Cancer, 2006-2010
20
10
CM
H C
an
ce
r P
rog
ram
An
nu
al
Re
po
rt
24
CMH Lung Cancer, 2006-2010
20
10
CM
H C
an
ce
r P
rog
ram
An
nu
al
Re
po
rt
25
DIAGNOSING LUNG CANCER The diagnosis, staging, and management of lung cancer is a collaborative effort on behalf of the patient by physicians representing multiple specialties. Pulmonologists are often involved in the initial evaluation and diagnosis of lung cancer. Clinical presentations of lung cancer may include such symptoms as dyspnea/shortness of breath at rest or with exertion, hemoptysis (coughing up blood), chest pain, hoarseness, weight loss, and bone pain. Chest radiographic findings may include new pulmonary nodules (“shadows”), pleural effusion, and non-resolving, persistent pneumonia. Pulmonologists guide the evaluation of these symptoms or abnormal chest x-rays through the use of flexible fiberoptic bronchoscopy, thoracentesis, CT guided transthoracic needle biopsy and thoracic surgical biopsies to help establish a definitive histologic diagnosis. Since no single procedure can 100% reliably establish the diagnosis of the various types of lung cancer, these invasive biopsy techniques are directed with a prudent understanding of their otential risks and benefits customized to the individual patient. The staging and management of newly diagnosed lung cancer is also a collaborative, multidisciplinary effort. Pulmonologists assist in the clinical staging and initial treatment planning of lung cancer. This involves an understanding of the pathophysiology of lung cancer with respect to its typical pattern of spread. Lung cancer is known to spread or metastasize to the lymph nodes, liver, brain, bones, adrenal glands and the opposite lung. Clinical staging involves a series of tests to search for the possible spread of tumor. Pulmonologists help direct the use of CT, MRI and PET scans to evaluate for metastatic tumor. If the lung cancer has not spread, and surgery is being considered, pulmonologists assess whether a patient can tolerate removing a lung or even a portion of it. Patients are then referred to a thoracic surgeon, medical oncologist or radiation oncologist as deemed appropriate based on the results of these tests. All of these procedures, imaging tests, and specialists are available in Ventura and at CMH. The Ventura Pulmonary and Critical Care Medical Group is a single specialty group of 4 Board certified pulmonologists who specialize in the diagnosis and management of various diseases of the respiratory tract, including lung cancer. Ashghar Arfaei, M.D. Pulmonary Medicine

CMH Lung Cancer, 2006-2010
20
10
CM
H C
an
ce
r P
rog
ram
An
nu
al
Re
po
rt
26
7th Edition AJCC Staging Form for Lung Cancer
CMH Lung Cancer, 2006-2010
20
10
CM
H C
an
ce
r P
rog
ram
An
nu
al
Re
po
rt
27
Local physicians who diagnose and treat lung cancer: Pulmonary Medicine Thomas Brugman, M.D. Robert Bernstein, M.D. John Handley, M.D. Asghar Arfaei, M.D. Thoracic/Cardiovascular Surgery Lamar Bushnell, M.D. Richard Declusin, M.D. Siobain Horan, M.D. Dominic Tedesco, M.D. Bruce Toporoff, M.D. Radiation Oncology Thomas Fogel, M.D. Jeffrey Rodnick, M.D. Medical Oncology Kevin Chang, M.D. Chirag Dalsania, M.D. Soo Im, M.D. Ann Kelley, M.D. Lynn Kong, M.D. Austin Ma, M.D. David Massiello, M.D. Rosemary McIntyre, M.D. Kooros Parsa, M.D. Deepika Wali, M.D. Todd Yates, D.O.

CMH Lung Cancer, 2006-2010
20
10
CM
H C
an
ce
r P
rog
ram
An
nu
al
Re
po
rt
28
Resources for Patients with Lung Cancer
American Cancer Society American Lung Association
Toll Free: 800-227-2345 Phone: 212-315-8700
http://www.cancer.org Toll Free: 800-586-4872
http://www.lungusa.org
Lung Cancer Alliance Lung Cancer Circle of Hope Phone: 202-463-2080 Phone: 732-363-4426 Toll Free: 800-298-2436 http://www.lungcancercircleofhope.org http://www.lungcanceralliance.org
Lung Cancer Foundation of America Lung Cancer Online Phone: 507-354-1361 http://www.lungcanceronline.org http://www.lcfamerica.org
LungCancer.org Lungevity Foundation Toll Free: 800-813-4673 Phone: 312-464-0716 http://www.lungcancer.org http://www.lungevity.org
National Lung Cancer Partnership Rare Cancer Alliance Phone: 608-233-7905 Toll Free: 800-345-6324 http://www.nationallungcancerpartnership.org http://www.rare-cancer.org
Uniting Against Lung Cancer Phone: 212-627-5500 http://www.unitingagainstlungcancer.org

CMH Lung Cancer, 2006-2010
20
10
CM
H C
an
ce
r P
rog
ram
An
nu
al
Re
po
rt
29
References
Cancer Statistics, 2011. CA: Cancer J Clin 2011; 61;212-236
National Cancer Database (NCDB), Commission on Cancer
AJCC Staging, 7th ed.
www.tarceva.com
www.alimta.com
www.avastin.com
National Comprehensive Cancer Network, Inc. www.nccn.org
National Cancer Institute. www.cancer.gov 1-800-4-CANCER
California Facts and Figures, 2010; California Cancer Registry and the American Cancer Society
CMH Cancer Resource Center Support Group Meeting Room

CMH Cancer Resource Center Services
20
10
CM
H C
an
ce
r P
rog
ram
An
nu
al
Re
po
rt
30
Man-to-Man - Prostate Cancer Support Group Second Thursday of the month at 6:30 pm Facilitator: Helmut Hoenigsberg, volunteer (American Cancer Society) Breast Cancer Support Group Every Thursday, 1:30 - 3:30 pm Facilitator: Gina Cole, MS, MFT (The Wellness Community) General Cancer Support Group Every Wednesday, 6:00 - 7:30 p.m. Facilitator: Gina Cole, MS, MFT (The Wellness Community) Every Thursday, 4:00 - 5:30 p.m. Facilitator: Maryana Palmer, MFT (The Wellness Community) Caregivers welcome Head and Neck Cancer Support Group Fourth Thursday of the month at 6:00 p.m. Facilitator: Ronald Brand, Ph.D. (SPOHNC/American Cancer Society) Lymph Luminaries - Lymphedema Support Group Third Tuesday of the month - 12:00 noon Facilitator: Claudia Steele-Major, PT, CLT-LANA Mindfulness-Based Stress Reduction Program 8 week course beginning in March and September Call (805) 652-5459 to register for this course Look Good Feel Better (Program for women undergoing treatment) Second Monday at 6:30 pm in March, June, September and December Facilitator: American Cancer Society Yoga Every Tuesday, 4:00 - 5:30 pm Facilitator: Tami Robinson (The Wellness Community) Restorative Yoga Please call for day and time Facilitator: Tami Robinson (The Wellness Community)

CMH Cancer Resource Center Services
20
10
CM
H C
an
ce
r P
rog
ram
An
nu
al
Re
po
rt
31
Guided Meditation First Monday of the month at 12:00 noon Facilitator: Roger Ford Third Friday of the month at 11 a.m. Facilitator: Frances Starr Creativity Central Fourth Monday of the month Facilitator: M. Nicole van Dam Please call 652-5459 for time and to RSVP Reiki Various practitioners Please call 652-5459 for an appointment Reflexology Jane Ivey Please call 652-5459 for an appointment Feldenkrais (Movement Therapy) Renee Garcia, GCFP Please call 652-5459 for an appointment Social Services Jody Giacopuzzi, LCSW Please call 652-5459 for an appointment Lymphedema Therapy Claudia Steele-Major, PT, CLT-LANA Please call 652-5459 for an appointment

CMH 2010 Cancer Committee Members
20
10
CM
H C
an
ce
r P
rog
ram
An
nu
al
Re
po
rt
32
Lynn Kong, M.D. Cindy DeMotte Chair, Cancer Committee VP, Quality Services Hematology/Oncology Jody Giacopuzzi, LCSW Thomas Fogel, M.D. Social Services Cancer Liaison Physician Radiation Oncology Kathleen Horton, RTT, CTR Cancer Program Kevin Chang, M.D., Ph.D. Hematology/Oncology Reverend Curtis Hotchkiss, M.A. Director, Spiritual Services Erwin Clahassey, M.D. Pathology Diana Jaquez, R.N., MSN, OCN Palliative Care Services James Hornstein, M.D. Family Practice and Bobbie McCaffrey, R.N. Palliative Care Services VP, Patient Services Geoffrey Loman, M.D. Carolyn Morales, R.N. Family Practice Quality Services Nelly Mac, M.D. Florence Roach, R.N. Pain Management Oncology Nursing Jeffrey Rodnick, M.D. Adam Thunell, COO Radiation Oncology VP, Operations Priscilla Wong, M.D. Chris Wilborn, CTR Radiology Cancer Registry Douglas Woodburn, M.D. Gary Wilde, Ph.D. General Surgery President and CEO

Glossary
20
10
CM
H C
an
ce
r P
rog
ram
An
nu
al
Re
po
rt
33
Stage at Diagnosis Describes the extent of disease based on all diagnostic and therapeutic evidence avail-able within four (4) months of diagnosis. There are currently two major staging classifi-cations, Collaborative Stage and AJCC (American Joint Committee on Cancer) Stage.
AJCC Stage This stage classification uses the TNM system which describes the anatomic extent of disease. This system is based on the assessment of three components: T: The extent of the primary tumor
N: The presence or absence and extent of regional lymph node metastasis
M: The presence or absence of distant metastasis Primary Tumor (T): TX: Primary tumor cannot be assessed T0: No evidence of primary tumor Tis: Carcinoma in situ
T1,T2,T3,T4: Increasing size and/or local extent of the primary tumor
Regional Lymph Nodes (N): NX: Regional lymph nodes cannot be assessed N0: No regional lymph node metastasis N1,N2,N3: Increasing involvement of regional lymph nodes Metastasis (M): MX: Presence of distant metastasis cannot be assessed M0: No distant metastasis present M1: Distant metastasis Treatment The first course of cancer directed therapy received by the patient, usually performed within four (4) months after date of first diagnosis. The major types of treatments avail-able are:
Chemotherapy: Chemicals which are administered to attack or treat malignant tissue. Hormonal: Use of hormones, antihormones, steroids and endocrine
surgery to attack cancer tissue by changing the patient‟s hormone balance.
Immunotherapy: Biological response modifiers, bone marrow transplants, stem cell transplants, and vaccine therapy.
Glossary
20
10
CM
H C
an
ce
r P
rog
ram
An
nu
al
Re
po
rt
34
Other: Any cancer related treatment which is not defined in the above categories such as experimental therapy and unproven methods.
None: Case which received no definitive therapy or supportive care only.
Class of Case
Analytic: Case first diagnosed and/or treated at Community Memorial Hospital Non-analytic: Case first diagnosed and/or treated at another facility,
but treated at a later time at Community Memorial Hospital.
CMH Wig and Hat Bank
The CMH 2010 Cancer Program Annual Report was designed and prepared by Kathleen Horton.
