cme management of frontal sinus fractures - lipteh.com from prs/0505-frontal sinu… · management...
TRANSCRIPT

CME
Management of Frontal Sinus FracturesReha Yavuzer, M.D., Alper Sari, M.D., Christopher P. Kelly, M.D., Serhan Tuncer, M.D.,Osman Latifoglu, M.D., M. Cemalettin Celebi, M.D., and Ian T. Jackson, M.D., D.Sc.(Hon.)Ankara, Turkey; and Southfield, Mich.
Learning Objectives: After studying this article, the participant should be able to: 1. Understand the radiographicand clinical diagnosis of frontal sinus fractures. 2. Identify various management approaches to the frontal sinusfracture and the indications for each. 3. Understand the rationale behind the decision of sinus obliteration whenneeded. 4. Recognize the most common complications arising from frontal sinus fracture treatment and the methodsof avoiding or managing these complications.
Summary: Frontal sinus fracture manage-ment is still controversial and involves preservingfunction when feasible or obliterating the sinusand duct, depending on the fracture pattern.There is no single algorithm for the choice ofmanagement, but appropriate treatment de-pends on an accurate diagnosis using physicalexamination, computed tomography data, andthe findings of intraoperative exploration. Theamount and location of fixation and the need forfrontonasal duct and sinus obliteration or elim-ination of the entire sinus depend on the anat-omy of the fracture in general and the extent ofinvolvement of the anterior wall of the sinus, thefrontonasal duct, and the posterior wall in par-ticular. This article discusses an algorithm forfrontal sinus fractures that was obtained from theliterature and modified according to the au-thors’ experience. The decision-making processpresented by the authors has withstood the testof time over a period of more than 20 years intheir practice and has been proven to be safe andefficacious in treating frontal sinus fractures ofall types. (Plast. Reconstr. Surg. 115: 79e, 2005.)
Frontal sinus fractures constitute 5 to 15 per-cent of maxillofacial fractures, with motor ve-hicle accidents being the most common andsports injuries the second most common cause
of these injuries.1– 4 Usually, the trauma iscaused by high-velocity impact; therefore, ap-proximately 75 percent of the cases have asso-ciated orbital, nasal, and/or other midfacialfractures. In our experience, approximately 20percent of patients are unconscious at the timeof their initial evaluation, and 20 percent havecerebrospinal fluid leaks.
All patients require a thorough physical ex-amination and radiologic workup, with partic-ular attention given to the frontonasal ductand associated fractures. The treatment strat-egy should be individualized according to theextent of the injury. Inappropriate initial treat-ment of frontal sinus fractures may lead toboth early and late serious complications, suchas mucopyocele, meningitis, and brain abscess.Those patients with associated intracranial in-juries have a further increased incidence oflong-term complications, as most of the timecomplications are caused by inadequate resto-ration of the barrier between the upper airwayand the intracranial contents.5,6 To reconstructthis barrier, a variety of alloplastic materialsand autogenous tissues have been used as freenonvascularized grafts to obliterate the sinus,with autogenous fat and cancellous bone graftsbeing the most common.6–8
Over the years, a treatment algorithm hasbeen developed based on the experiences of
From the Department of Plastic, Reconstructive, and Aesthetic Surgery, Gazi University Medical Faculty; and the Institute for Craniofa-cial and Reconstructive Surgery. Received for publication January 27, 2004.
Presented in part at the 20th Annual Meeting of the European Society of Ophthalmic Plastic and Reconstructive Surgery, in Muenster, Germany, Sep-tember 19 to 21, 2002, and at the 71st Annual Meeting of the American Society of Plastic Surgeons, Plastic Surgery Educational Foundation, and Ameri-can Society of Maxillofacial Surgeons, in San Antonio, Texas, November 2 to 6, 2002.
DOI: 10.1097/01.PRS.0000161988.06847.6A
79e

others reported in the literature1–26 and modi-fied according to the senior author’s experi-ence. This decision-making process, which isguided mainly by the extent of the injury, hasbeen safe and efficacious both in treating fron-tal sinus fractures and in avoiding latecomplications.
FRONTAL SINUS
Embryology
During the fourth fetal month, the middlemeatus expands superiorly and anteriorly,forming the frontal recess. The nasal mucosathen migrates cranially, forming the lining ofthe frontal sinus. The frontal sinus may alsoarise from anterior ethmoidal cells. The frontalsinus is not pneumatized until the age of 2. Atthe age of 4, the frontal sinus reaches the sizeof a pea, and at the age of 8, it begins to beradiographically identifiable. As the pneumaticexpansion of the sinus is not completed untilthe late adolescent period, sinus fractures arerarely seen in children and are seldom seen inadolescents. Young adults are the most com-monly affected group.27 The sinus reaches itsadult size around the age of 15, but it usuallyattains its maximum dimension at age 19.1Early craniofacial surgery before developmentof the frontal sinus seems to have less of aneffect on sinus pneumatization, as demonstratedby Locher et al.,28 who showed radiographicallythat 72.7 percent of their patients who had un-dergone bilateral fronto-orbital osteotomies at anearly age had frontal sinus pneumatization be-tween the ages of 4 and 11. Developmentalanomalies of the frontal sinus, such as unilateralor bilateral agenesis, are not uncommon andeach is seen in approximately 4 percent of cases.When fully developed, the size and shape of thefrontal sinuses cover a wide spectrum, and theright and left frontal sinuses develop indepen-dently.29,30 The entire frontal bone may be pneu-matized during development, creating a mark-edly enlarged sinus (Fig. 1). This is especiallyimportant when planning for sinus obliterationor cranialization. In the former, the amount ofmaterial required to obliterate the large sinusshould be taken into consideration, especiallywhen autogenous material is to be used. In thelatter, the dead space that develops followingcranialization may not be filled by brain expan-sion because of its significant size.
The great range of frontal sinus variationbetween individuals is similar to that of finger-
prints, and the chance of two persons havingthe same size and shape of frontal sinus isextremely rare. This has found application indetermining personal identification in forensicscience.31
Anatomy
The frontal sinus is a strategic structure thatis located between the anterior cranial fossaand the naso-orbitoethmoid regions. Thesepaired pneumatized cavities are located in thefrontal bone. Each sinus is bordered by itsanterior and posterior walls, the orbital roofinferiorly, and a bony intersinus septum medi-ally. Because of their proximity to the anteriorcranial fossa, the dura mater, cribriform plate,and frontal lobes can be damaged by traumainvolving the posterior wall of the sinus. Theheight of the frontal sinus varies from 5 to 66mm, with an average height of 24.3 mm, and itslength ranges from 17 to 49 mm, with an aver-age length of 29 mm. The volume of an aver-age adult frontal sinus is 5 cm3. Its anterior wallis much stronger than the other facial bonesand resists up to 400 to 1000 kg before break-ing. The thick anterior wall with cancellousbone between its inner and outer corticalplates and the air cavity that lies between theanterior and posterior walls of the sinus arethe major determinants of this strongconstruction.
The frontonasal duct is the most anteriorand superior portion of the anterior ethmoidcomplex and drains the frontal sinus into themiddle meatus. The term frontal recess is alsoused instead of frontonasal duct, because ananatomical duct from the frontal sinus is not
FIG. 1. A computed tomographic scan demonstrating a verylarge frontal sinus occupying most of the frontal bone.
80e PLASTIC AND RECONSTRUCTIVE SURGERY, May 2005

present. In this article, the term frontonasalduct will be used, as it is a key element in thedecision-making process in addition to beinginvolved in one of the crucial steps of theoperative treatment in some instances. Likethe frontal sinus itself, the frontonasal ductdisplays significant anatomical variations. How-ever, in most individuals, the superior portionof the uncinate process forms the anterior bor-der of the duct. The ethmoid bulla forms theposterior border, the anterior portion of themiddle turbinate lies medially, and the laminapapyracea or suprainfundibular plate lies later-ally.32 Both the frontal sinus and its duct arelined with ciliated pseudostratified columnarepithelium. This lining is actively involved indrainage of the sinus, and after traumatic dis-ruption, stasis of frontal sinus secretions oc-curs, which eventually might lead to infectiouscomplications. At the posterior sinus wall,there are areas such as the foramina of Bre-schet, where mucosa is tethered deeply withinthe bone. These particular areas should also beremoved either by careful sharp dissection orwith the help of a high-speed contouring burrwhenever sinus obliteration is contemplated.
The arterial supply of the sinus comes fromthe supraorbital, supratrochlear, and anteriorethmoidal arteries. The superficial venous sys-tem drains to the angular vein, and the deepdrainage is to the subdural venous systemthrough the foramina of Breschet. Lymphaticdrainage follows the meningeal and nasal cav-ity lymphatics. This complex drainage systemexplains why there is a risk of serious compli-cation such as meningitis or brain abscess aftera frontal sinus fracture, even without disrup-tion of the posterior wall.
Little is known about the function of thefrontal sinus. Although this has not beenproved, it is thought to play a minor role inrespiration, olfaction, vocalization, thermalregulation, and baroregulation. None of ourpatients who had frontal sinus obliteration orablation caused by trauma or tumor has beendocumented to have any functional impair-ment of any kind.
FRONTAL SINUS FRACTURES
Diagnosis
The most common clinical finding is a lac-eration of the forehead. Any hematoma or ec-chymosis over the glabellar region should raisesuspicion of sinus injury. The entire forehead,
including the superior orbital rims, should beevaluated for bony irregularities or crepitus inaddition to sensory loss. The nose should beexamined for cerebrospinal fluid leak. If thereis any doubt, the halo test or laboratory confir-mation of beta-2 transferrin can be used toidentify the cerebrospinal fluid.
Because of the nature of the injury, there isa high likelihood of accompanying facial frac-tures; thus, the entire maxillofacial regionshould be examined thoroughly. Clinical ex-amination alone is not enough to determinethe extent of injury.3 A combined clinical andradiographic workup goes hand in hand with aprecise intraoperative exploration to fully ap-preciate the severity of the bony trauma. Thin-section axial and coronal computed tomo-graphic scans are an essential part of theradiographic workup and allow an accuratepreoperative surgical plan to be formulated.1,2
Computed tomographic scanning provides es-sential information regarding the anatomy ofthe sinus and involvement of the anteriorand/or posterior wall, and it also reveals anydamage to adjacent structures or associatedintracranial abnormality. Coronal sectionsshould focus on the frontonasal duct to eluci-date whether it has been traumatized.
The treatment of a patient with a nasofronto-orbital injury is a multidisciplinary procedurethat involves the plastic surgery, neurosurgery,ophthalmology, and maxillofacial surgery dis-ciplines. This combined approach ensures thatthe correct diagnosis is made, thus avoidingfuture problems.
Preoperative Preparation
The surgical plan is formulated after a com-plete clinical and radiographic workup has beenperformed. All patients receive intravenous anti-biotic treatment with ceftriaxone and metronida-zole for 7 days; in those with cerebrospinal fluidleakage, it is continued for 14 days.
Surgical Treatment
The surgical plan must be formulated fromobjective criteria based on the extent of theinjury. Although many different classificationshave been presented, involvement of the ante-rior sinus wall, posterior sinus wall, dural lin-ing, and frontonasal duct is the major determi-nant of the type and extent of the procedurethat is selected.1–7,11,12 Early surgical explora-tion and treatment, as soon as the systemicconditions are stabilized, are the preferred
Vol. 115, No. 6 / FRONTAL SINUS FRACTURES 81e

protocol in acute injuries. As stated by Lee etal.,11 early treatment of frontal sinus fracturesreduces the incidence of long-term complica-tions; thus, we operate within the first week ofacute injury whenever the patient’s generalcondition is satisfactory.
Adequate exposure of the affected region isvital for intraoperative assessment of the fracture;this also allows a symmetrical contour to beachieved. Therefore, any existing laceration isnot recommended for access unless there is avery minor anterior wall fracture. In all of ourcases, the frontal regions were explored using abicoronal incision to obtain full exposure of bothfrontal bones and to repair any intracranial trau-ma.32 The coronal flap is elevated down to thenasoglabellar junction medially and the frontozy-gomatic junctions laterally, to expose the ante-rior frontal sinus wall bilaterally.
Anterior Wall Fractures
Undisplaced fractures of the anterior wall ofthe frontal sinus do not require surgical inter-vention, provided that the frontonasal duct isundamaged. However, we recommend thatthese patients be treated with antibiotics for 7days. Nevertheless, there is always the possibil-ity of a late infection; thus, we recommend thatthey should undergo a long-term follow-up ex-amination and 12-month control computed to-mographic scanning.
Isolated anterior wall fractures with dis-placed fragments require surgical correctionmost of the time to restore normal foreheadcontour. Once exposure is achieved by thecoronal flap, any displaced fractured fragmentsare removed. This is then followed by an ex-ploration of the posterior wall and frontonasalduct. If there are no other injuries, the dam-aged sinus mucosa is removed. The anteriorwall is returned to its anatomical position andstabilized with either suture, wire, or metal orresorbable plates, according to the surgeon’sdesire and the patient’s age (Figs. 2 and 3).Smaller bone fragments should not be re-placed; any residual gaps can be filled withcranial bone grafts. Anterior frontal sinus wallfractures alone do not merit sinus obliterationprocedures. The forehead region does nothave a thick subcutaneous tissue; thus, anymetal hardware can be easily palpated andeven becomes visible once the edema from thetrauma and surgery subsides. Currently, we fa-vor resorbable plating systems for stabilizingbone segments, to avoid further interventions
to remove the hardware. Moreover, theseplates do not cause any artifact effect duringfollow-up computed tomographic scans, as oc-curs with their metal counterparts, which ob-scures the fine details of the sinus lining. Re-cently, endoscopic reduction and fixation ofisolated, simple anterior wall fractures hasbeen popularized, with encouraging short-term results.14,15 This technique avoids a bi-coronal flap and reduces operative time andrecovery time. However, the efficacy of the en-doscopic approach in exploration of the pos-terior wall and frontonasal duct has not yetbeen clarified. In addition, there are someother factors, such as difficulty in complicatedfracture reduction and fixation, that limit itswidespread use.
Frontonasal Duct Fracture
Assessment of frontonasal duct injury is cru-cial, as surgical treatment will change signifi-cantly in the event of frontonasal duct involve-ment. Ideally, the preoperative coronal sectioncomputed tomographic scan will help to revealthe duct injury. However, with any frontal sinusfracture, we highly recommend an intraopera-tive exploration focusing on the continuity ofthe duct. In our series, approximately 55 per-cent of all frontal sinus fractures had frontona-sal duct injury to some extent. Intraoperatively,methylene blue or fluorescein tests may also beperformed to assess the drainage of the sinusthrough the duct. This is not necessary most ofthe time, because the fractured segments caneasily be seen during the operation. The diag-nosis of frontonasal duct injury necessitates si-nus obliteration. First, sinus mucosa is removedand mucosal curettage is performed with sharpperiosteal elevators. Curettage can also be per-formed by drilling the sinus walls with a high-speed burr.3,5 This method is preferred bysome authors to effectively clear the mucosalfragments from fracture lines and the foramenof Breschet. The frontonasal duct is pluggedwith a pericranium graft, which can easily beharvested from the surgical field. Recently, wehave been using fibrin glue to secure the plugin place. Bone grafts can also be used for thisprocedure.33,34
For sinus obliteration, there are several graftoptions. Some of the most commonly usedones are autogenous fat, dermal fat, muscle,cartilage, bone, pericranium grafts, and allo-plastic materials such as Surgicel (Ethicon Sarl,Neuchatel, Switzerland), silicone, hydroxyapa-
82e PLASTIC AND RECONSTRUCTIVE SURGERY, May 2005

tite, methyl methacrylate, and even bonewax.6,7,9,34–36 Another method of sinus oblitera-tion is osteoneogenesis).34,37 In spontaneous os-teoneogenesis, the denuded posterior wall ofthe sinus promotes the formation of fibroustissue, which is subsequently replaced to someextent by cancellous bone. With this tech-nique, one can avoid any donor areas for au-togenous grafting and also eliminate the use of
alloplastic material. However, it is not knownhow much new bone formation takes place, asthe volume of the frontal sinus can vary over awide range. In addition, the amount of timerequired for spontaneous osteoneogenesis toobliterate the sinus and whether the sinus ismore prone to infectious complications be-cause of that nonobliterated period have notbeen clearly documented. Despite these issues
FIG. 2. (Above, left) Preoperative view of a 22-year-old woman who was involved in a motorvehicle accident. (Above, right) Clinical examination revealed slight depression (arrows) of theright forehead, and a preoperative computed tomographic scan demonstrated a displacedanterior sinus wall fracture (center, right). (Below, left) Through a bicoronal approach, the fracturewas exposed. As the exploration failed to reveal frontonasal duct or posterior wall injury, the sinuswas preserved and the anterior wall was reconstructed using a resorbable mesh plate (below, right).
Vol. 115, No. 6 / FRONTAL SINUS FRACTURES 83e
that need to be addressed, good results can beachieved with osteoneogenesis, making it oneof the most reliable alternatives for sinus oblit-eration. Among the various graft options, fathas been the most widely used. Both propo-nents and opponents of autogenous fat graftsare found in the literature.13–15 Animal andclinical studies by Montgomery and Pierce sug-gested fat grafts as a reasonable choice in thesinus obliteration procedure.12,38 They alsostate that fat grafts are relatively resistant toinfection. To ensure the separation of the neu-rocranium from the contaminated external en-vironment and the upper airways, a tissue thatwill stay viable after obliteration of the sinus isneeded. Weber et al.39 showed that the amountof fat tissue placed in the sinus decreased sig-nificantly with time. In that study, postopera-tive magnetic resonance imaging performed ata mean 24.1 months after the operation re-vealed less than 20 percent of the initiallyplaced fat graft in more than half of the cases.
None of the above-mentioned autogenousobliteration methods provide vascularity to thesinus. The alloplastic materials cannot preventinfection, which is the leading cause of frontalsinus complications in both the early and latepostoperative periods. Thus, when obliterationof the frontal sinus is indicated, the galeal fron-
talis myofascial flap is the technique preferredby the authors.
The galeal frontalis flap is elevated from theuninjured side; this will leave intact periosteumover the fractured anterior wall segments to aidin fracture healing. If this is not available be-cause of a full-thickness skin laceration on theforehead, the injured side is used. The galealaponeurosis is outlined on the previously dis-sected scalp flap based on the supratrochlearartery, the supraorbital artery, or both. Thegaleal layer is then carefully elevated from thesubcutaneous tissue without injuring the hairfollicles. Dissection proceeds in a cranial tocaudal direction and the frontalis muscle isincluded in the flap. The base of the flap re-quires careful dissection to avoid injury to thesupraorbital and supratrochlear vessels wherethey exit the frontal bone. Transilluminationaids in visualization of the vessels. They mustbe included because this is an axial patternflap. The flap is then rotated into the sinus andsecured using absorbable sutures placedthrough holes drilled on the edge of the frac-ture. For the past 3 years, fibrin glue has alsobeen used for flap inset; this is a later additionto the time-honored technique. In that case,the floor of the sinus and previously pluggedfrontonasal duct are covered with fibrin glue.
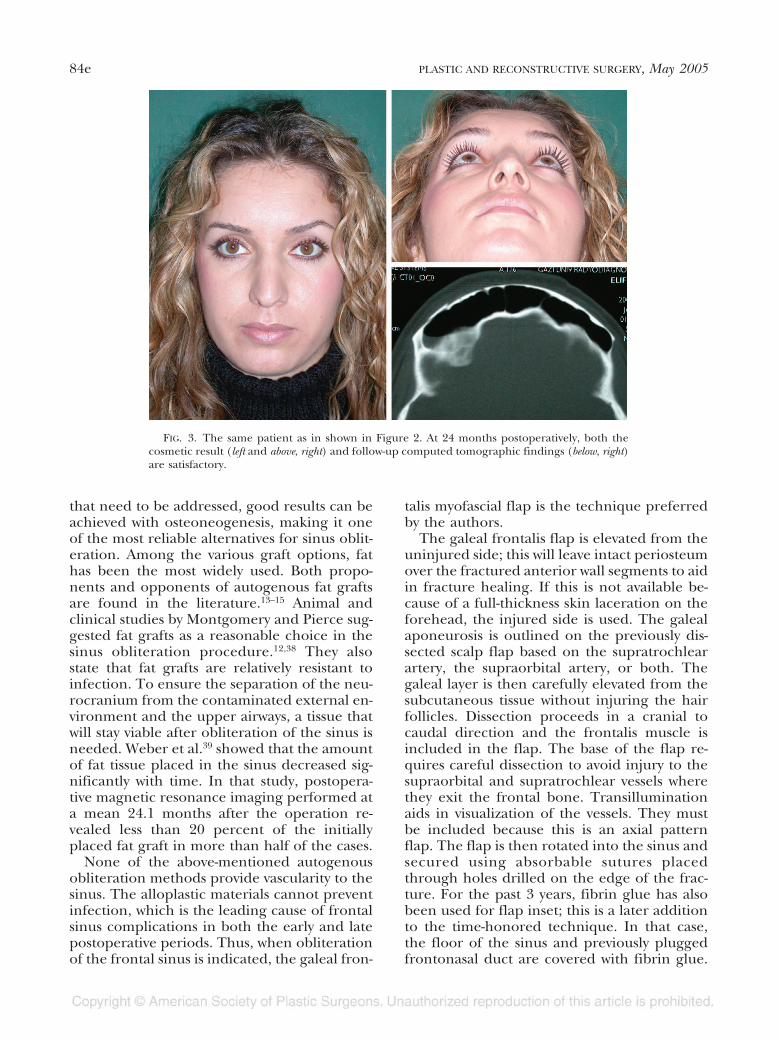
FIG. 3. The same patient as in shown in Figure 2. At 24 months postoperatively, both thecosmetic result (left and above, right) and follow-up computed tomographic findings (below, right)are satisfactory.
84e PLASTIC AND RECONSTRUCTIVE SURGERY, May 2005
Before it is allowed to set, the galeal frontalisflap is placed to fill the entire sinus cavity. Ifone flap is not enough to obliterate the sinusor when both sinuses are injured, two flaps areused. After galeal frontalis flap obliteration,the anterior wall of the sinus is reconstructedby using either native bone fragments or split-or full-thickness cranial bone grafts as re-quired. These grafts are either harvested fromadjacent noninjured areas of the skull or sup-plied as commercially available cadaveric allo-grafts. A defect is left at the edge of the bonegrafts so that the pedicle of the galeal frontalisflap will not be compressed. Either titanium orresorbable plates and screws can be used to fixthe bone grafts (Figs. 4 and 5).
Posterior Wall Fractures
Almost all posterior wall fractures are accom-panied by anterior wall fractures. With posteriorwall fractures, again, frontonasal duct injury andcerebrospinal fluid leakage play the major rolesin surgical decisions. Nondisplaced posterior wallfractures do not require surgical intervention.Nondisplaced posterior wall fractures with cere-
brospinal fluid leakage should be treated expect-antly for up to a week, provided that the above-mentioned antibiotic coverage is provided.During this period, to facilitate spontaneous res-olution of the cerebrospinal fluid leak, bed rest,30 degrees of head elevation, and, for those casesthat persist beyond the first 4 days, spinal drain-age are recommended. With these nonoperativemeasures, more than half of the cases have asatisfactory outcome. Prolonged cerebrospinalfluid leakage beyond 10 days necessitates crani-otomy, repair of the dural laceration with a peri-cranial patch graft, and either obliteration of thesinus or cranialization, depending on the natureof the posterior wall fracture (Fig. 6). If duralrepair is performed before anterior wall recon-struction, the patient is placed in the Trendelen-burg position and the anesthetist is asked to tem-porarily increase the intracranial pressure toverify that the repair is watertight. If there is aleak with this maneuver, the dural repair site isreinforced with a larger graft. Once secure clo-sure has been confirmed, the patient is returnedto the normal position and the rest of the proce-dure is carried out.
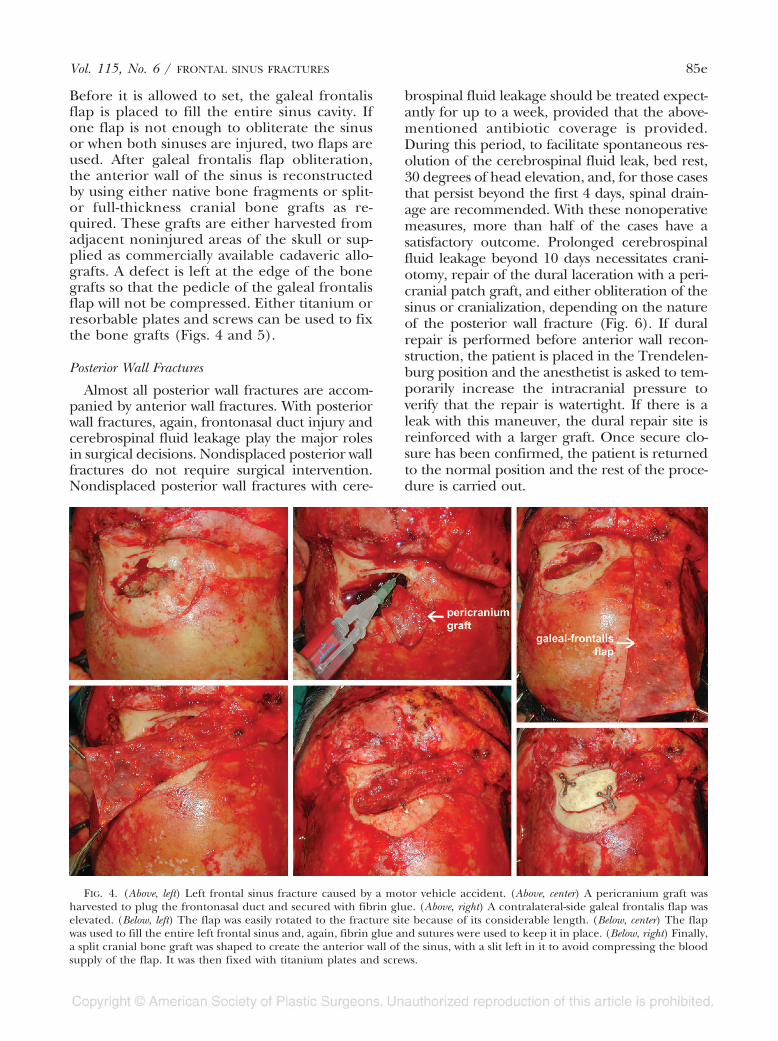
FIG. 4. (Above, left) Left frontal sinus fracture caused by a motor vehicle accident. (Above, center) A pericranium graft washarvested to plug the frontonasal duct and secured with fibrin glue. (Above, right) A contralateral-side galeal frontalis flap waselevated. (Below, left) The flap was easily rotated to the fracture site because of its considerable length. (Below, center) The flapwas used to fill the entire left frontal sinus and, again, fibrin glue and sutures were used to keep it in place. (Below, right) Finally,a split cranial bone graft was shaped to create the anterior wall of the sinus, with a slit left in it to avoid compressing the bloodsupply of the flap. It was then fixed with titanium plates and screws.
Vol. 115, No. 6 / FRONTAL SINUS FRACTURES 85e

Posterior wall fractures with no involvement ofthe frontonasal duct and no evidence of cerebro-spinal fluid leakage can be treated with eitherpreservation of the sinus or obliteration, depend-ing on the fracture. Severely contaminatedwounds or comminuted posterior wall fracturesare better treated with sinus obliteration with thegaleal frontalis flap or cranialization. Posteriorwall fractures with frontonasal duct injury or du-ral tear and cerebrospinal fluid leakage aretreated with sinus obliteration as outlined aboveor with cranialization. As a proponent of sinusobliteration with grafts, Luce recommended cra-nialization procedures for sinus ablation whennecessary.13 Cranialization involves removal ofthe entire posterior wall of the sinus after thefrontonasal duct is plugged, and any dural lacer-ation is repaired followed by separation of theintracranial cavity from the aerodigestive tractusing a galeal frontalis flap. The frontal lobe isthen expected to expand and fill the previous
sinus cavity. Cranialization procedures may bethe treatment of choice when a craniotomy forneurosurgical indications is combined with theneed for frontal sinus obliteration.40 In our opin-ion, which is supported by Wolfe and Johnson,6cranialization for sinus ablation without concur-rent neurosurgical indications is somewhat ex-tensive and increases the risk of postoperativemorbidity. In fact, it is a procedure that we haverarely ever performed.
Complications
All patients with frontal sinus fractures re-quire a long-term follow-up of at least 5 years,during which yearly computed tomographicscan evaluations can be carried out. This willenable the surgeon to visualize the early stagesof complications before they present clinically.Early complications after frontal sinus fracturesare believed to be caused by dural layer disrup-tion and late complications by sinus malfunc-
FIG. 5. (Above, left) A motor vehicle accident resulted in a fracture involving the left and rightfrontal sinuses. (Above, right) The anterior walls of both sinuses were removed to inspect thefrontonasal duct and the posterior wall and to extract the injured sinus mucosa. (Below, left) Twogaleal frontalis flaps were designed to obliterate both sinuses. (Below, right) Both flaps wereelevated and are ready to be used for obliteration.
86e PLASTIC AND RECONSTRUCTIVE SURGERY, May 2005

tion caused by drainage problems. The mostcommon complications after surgery in pa-tients with frontal sinus injuries are chronicfrontal headaches, sinus infections with drain-age problems, and aesthetically unacceptablecontour deformities.2,3,5,6,41–43 Brain abscess for-mation and meningitis are less frequently seenand are disastrous outcomes of incorrectly han-dled sinus infection. In our series of frontalsinus fractures that had sinus obliteration withthe galeal frontalis flap, one minor infectionoccurred, and this resolved with antibiotictreatment. Therefore, even with the late-presenting infectious complications, we favoruse of the galeal frontalis flap most of the time.
In those cases, the sinus is filled with pus. Thepreferred treatment is radical débridement ofany remaining sinus contents together with un-healthy bone, followed by either galeal fron-talis flap obliteration (Fig. 7) or, rarely,cranialization.
Harvest of the galeal frontalis flap results intransient sensory loss over the frontal regionlasting from 4 to 12 months, with an averageduration of 6 months. Little or no significantcontour deformity of the donor area has beenseen. In the senior author’s series during afollow-up period ranging from 1 to 20 years,sinus obliteration was successfully achieved inall patients (Figs. 8 and 9).
FIG. 6. (Above, left) Through a bicoronal approach, a right frontal sinus fracture was seen. (Above, center) Once the anteriorwall was removed, a posterior wall fracture was also noted. (Above, right) An ipsilateral galeal frontalis flap was elevated. (Center,left) The flap was packed into the sinus. (Center, center) The anterior wall of the sinus was returned to its anatomical position aftera slit was created on its caudal edge. (Center, right) Resorbable mesh and screws were used to fix the replaced bone graft. (Below,left) A preoperative computed tomographic scan demonstrated a more severely damaged posterior wall (arrows) than the anteriorwall. (Below, right) At 13 months postoperatively, well-established frontal sinus obliteration and correction of the fracture siteswere noted.
Vol. 115, No. 6 / FRONTAL SINUS FRACTURES 87e
CONCLUSIONS
Although controversy remains regarding themanagement of frontal sinus fractures, it isobvious that if they are treated improperly orlate, a variety of complications can occur.Treatment principles emerging from pub-lished studies, especially those by Rohrich andHollier,1,10,34 and from our experience have re-
vealed some basic points to consider whendealing with frontal sinus fractures. The oper-ative indications in the management of frontalsinus fractures are as follows (Fig. 10):
Anterior wall fractures
• Isolated anterior wall fractures without de-pression do not require surgical treatment.
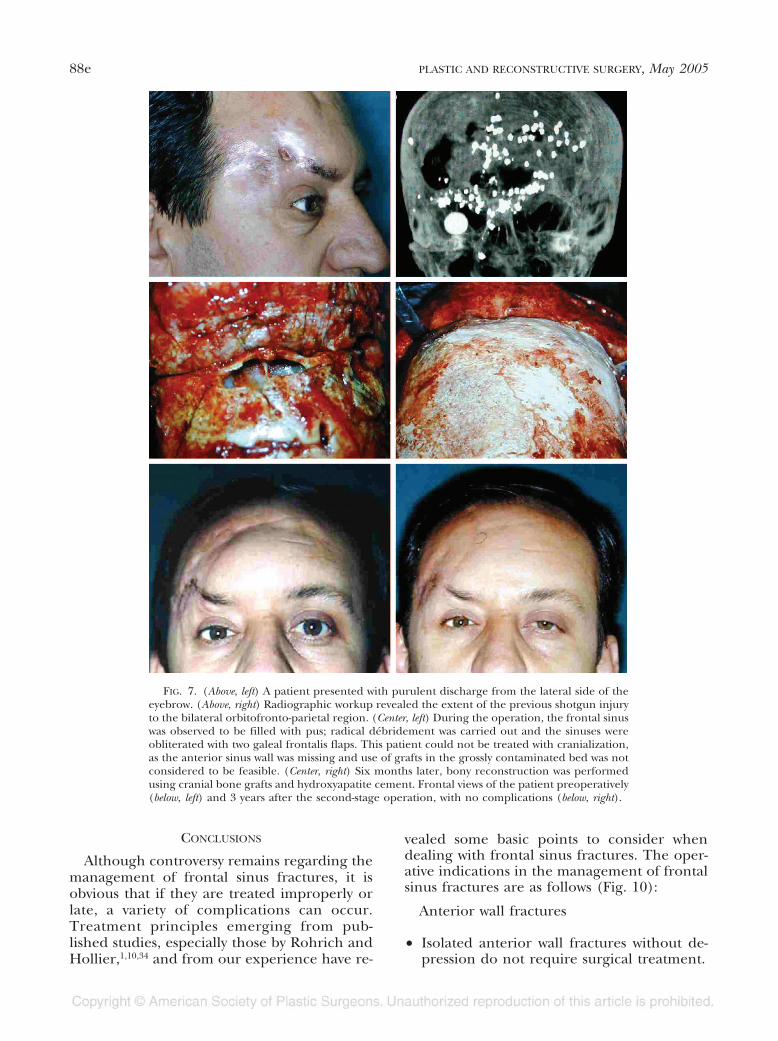
FIG. 7. (Above, left) A patient presented with purulent discharge from the lateral side of theeyebrow. (Above, right) Radiographic workup revealed the extent of the previous shotgun injuryto the bilateral orbitofronto-parietal region. (Center, left) During the operation, the frontal sinuswas observed to be filled with pus; radical débridement was carried out and the sinuses wereobliterated with two galeal frontalis flaps. This patient could not be treated with cranialization,as the anterior sinus wall was missing and use of grafts in the grossly contaminated bed was notconsidered to be feasible. (Center, right) Six months later, bony reconstruction was performedusing cranial bone grafts and hydroxyapatite cement. Frontal views of the patient preoperatively(below, left) and 3 years after the second-stage operation, with no complications (below, right).
88e PLASTIC AND RECONSTRUCTIVE SURGERY, May 2005

• Cases with solitary depressed anterior wallfractures require anterior wall restoration toobtain aesthetically acceptable contours.
• If there is frontonasal duct injury or poste-rior wall injury with dural tear or cerebro-spinal fluid leakage, the sinus mucosa is re-moved and the cavity is obliterated.
Posterior wall fractures
• Posterior wall fractures without displace-ment, cerebrospinal fluid leakage, or fron-tonasal duct injury do not require surgicaltreatment.
• Posterior wall fractures without displace-ment but with cerebrospinal fluid leakagerequire treatment with systemic antibiotics,head elevation, and spinal drainage whennecessary for up to 10 days.
• Posterior wall fractures without displace-ment but with cerebrospinal fluid leakagebeyond 10 days require craniotomy, duralrepair, and sinus obliteration.
• Displaced posterior wall fractures with fron-tonasal duct injury require either sinus oblit-eration or, rarely, cranialization.
If there is frontonasal duct injury or poste-rior wall injury with dural tear or cerebrospinalfluid leakage, the sinus mucosa is removed andthe cavity is obliterated. For cases requiringsinus obliteration, the frontonasal duct is oc-cluded with a pericranial graft. Then, thegaleal frontalis flap is used to obliterate thefrontal sinus, thus providing a good blood sup-ply to the contaminated open fracture. Apartfrom being a tissue more resistant to infection,the galeal frontalis flap with its proven vascu-
FIG. 8. (Above, left) A 28-year-old man was involved in a motor vehicle accident. (Below, left)His preoperative computed tomographic scan demonstrates a markedly displaced superiororbital rim and anterior sinus wall. (Above, right) The patient had no contour deformity or anyother sequelae after having his sinus packed with a galeal frontalis flap. (Below, right) Hispostoperative follow-up computed tomographic scan at 16 months revealed the corrected bonydeformity and obliterated left frontal sinus.
Vol. 115, No. 6 / FRONTAL SINUS FRACTURES 89e
larity makes even more sense as a filler becausethe anterior wall of the sinus is reconstructedwith bone grafts. When a contralateral galealfrontalis flap is used for sinus obliteration, thebone graft that is placed to reconstruct theanterior wall is supported by the overlying vas-cularized periosteum and the underlying vas-cular galeal flap. This is important for success-ful bone graft survival.
It is also obvious that, although avasculargrafts undergo some necrosis, revasculariza-tion occurs. During this avascular period, thehost immune system will not have the capabil-ity to counteract infection. In addition, thenecrotic debris of the graft cannot be drained,as the frontonasal passage is plugged; the over-lying bone graft will contact this nonvital tissue,which can act as a potential source of infection.
Various types of galeal flaps have been usedwith encouraging results for frontal sinus frac-tures.2,25,44–47 The galeal frontalis myofascialflap was used to separate the intracranial cavityfrom the aerodigestive tract in anterior cranial
base operations.48,49 The clinical success of itsapplication in cases possessing a possibility ofdirect intracranial nasopharyngeal communi-cation makes it a highly reliable flap. The com-plications arising after frontal sinus surgery aremainly caused by the presence of a contami-nated wound, either from the external envi-ronment or from the nasopharnyx. In a con-taminated wound, a good vascular supply is themainstay of resistance against infection. As de-scribed, the flap can be raised on the su-pratrochlear and the supraorbital arteries,which provide good vascularity. Cadaver stud-ies on the blood supply of the galea frontalisflap have shown that it is possible to perfusethe frontal, temporal, and parietal regionsfrom the supratrochlear and supraorbital arter-ies.50 Because of its dependable vascularity, theflap can also carry a large amount of bonewhen needed.51,52
Recently, fibrin glue has also been used inthe treatment of these cases for various rea-sons. First, fibrin glue helps to fix the pericra-
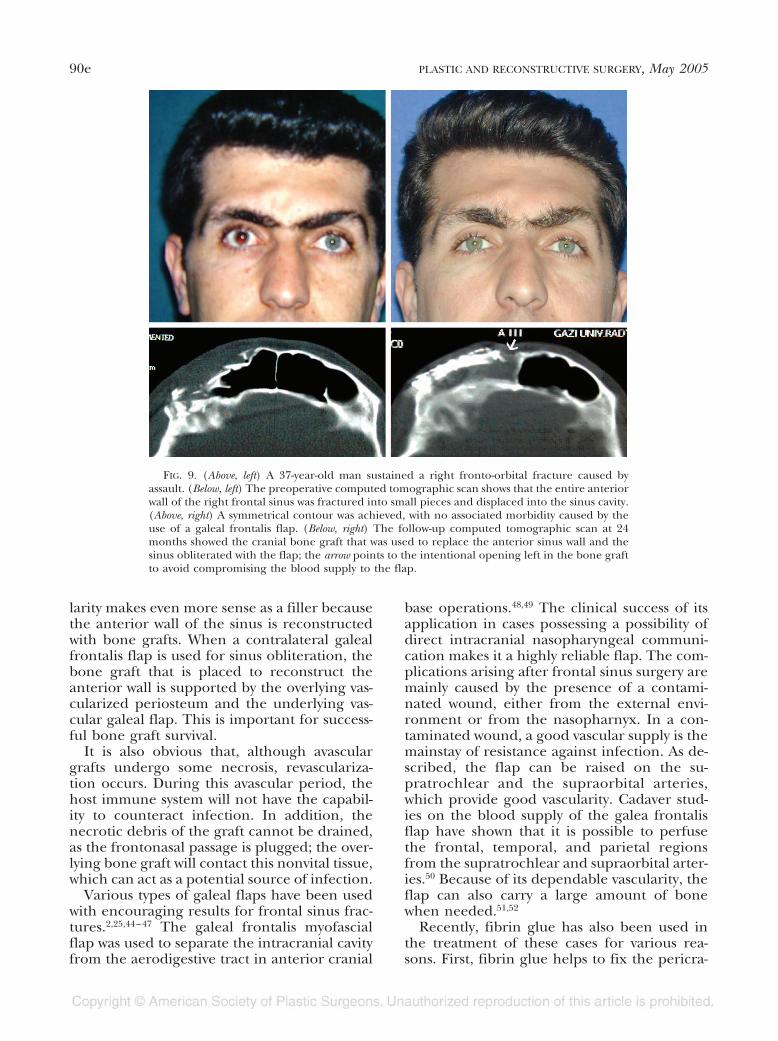
FIG. 9. (Above, left) A 37-year-old man sustained a right fronto-orbital fracture caused byassault. (Below, left) The preoperative computed tomographic scan shows that the entire anteriorwall of the right frontal sinus was fractured into small pieces and displaced into the sinus cavity.(Above, right) A symmetrical contour was achieved, with no associated morbidity caused by theuse of a galeal frontalis flap. (Below, right) The follow-up computed tomographic scan at 24months showed the cranial bone graft that was used to replace the anterior sinus wall and thesinus obliterated with the flap; the arrow points to the intentional opening left in the bone graftto avoid compromising the blood supply to the flap.
90e PLASTIC AND RECONSTRUCTIVE SURGERY, May 2005

nial patch in the frontonasal duct without anydifficulty. This technique can also be used forfixation of the galeal frontalis flap in additionto the sutures placed through the drill holes.Moreover, fibrin glue fills any residual spacebetween the galeal frontalis and the sinus,obliterating the entire frontal sinus. It also pro-vides hemostasis for the remaining frontal si-nus walls (especially when there is a fracture onthe posterior wall). Apart from fixing the softtissue, fibrin glue helps to hold the bone graftused to repair the anterior wall. However, wedo not currently feel secure enough with thisfixation alone and prefer to use resorbable ormetal plating systems. An osteoinductive prop-erty has been attributed to fibrin glue.53,54
Therefore, its use might have a positive effecton bone healing. This has not been analyzed,but in this series of patients, there was only onepartial bone resorption attributed to a localinfection. All the remaining bone grafts wereincorporated into the adjacent native bonewithout any problems whether fibrin glue wasused or not.
With its excellent blood supply, the galealfrontalis myofascial flap provides significant re-sistance to infection in acutely injured, con-taminated, or chronically complicated frontalsinus fractures. Cranial bone grafts provideone of the best—if not the best—reconstruc-tion option(s) for the severely damaged ante-rior or posterior frontal sinus wall. Therefore,
FIG. 10. Treatment algorithm for frontal sinus fractures. CSF, cerebrospinal fluid.
Vol. 115, No. 6 / FRONTAL SINUS FRACTURES 91e

the present clinical study suggests the combi-nation of a galeal frontalis flap and cranialbone graft as a good and reliable treatmentmethod in frontal sinus injuries that requiresinus obliteration.
Reha Yavuzer, M.D.Gazi University Medical FacultyCranioMaxilloFacial Surgery Working GroupDepartment of Plastic, Reconstructive, and
Aesthetic SurgeryGazi Hospital, 14th FloorBesevler 06500Ankara, [email protected]
REFERENCES
1. Rohrich, R. J., and Hollier, L. H. Management of fron-tal sinus fractures: Changing concepts. Clin. Plast.Surg. 19: 219, 1992.
2. Gerbino, G., Roccia, F., Benech, A., and Caldarelli, C.Analysis of 158 frontal sinus fractures: Current surgicalmanagement and complications. J. Craniomaxillofac.Surg. 28: 133, 2000.
3. Wilson, B. C., Davidson, B., Corey, J. P., and Haydon,R. C., III. Comparison of complications followingfrontal sinus fractures managed with exploration withor without obliteration over 10 years. Laryngoscope 98:516, 1988.
4. Schultz, R. C., and de Camara, D. L. Athletic facialinjuries. J.A.M.A. 28: 252, 1984.
5. Larrabee, W. I., Jr., Travis, L. W., and Tabb, H. G. Fron-tal sinus fractures: Their suppurative complicationsand surgical management. Laryngoscope 90: 1810,1980.
6. Wolfe, S. A., and Johnson, P. Frontal sinus injuries:Primary care and management of late complications.Plast. Reconstr. Surg. 82: 781, 1988.
7. Ioannides, C., Freihofer, H. P., and Friens, J. Fracturesof the frontal sinus: A rationale of treatment. Br. J.Plast. Surg. 46: 208, 1993.
8. Levine, S. T., Rowe, L. D., Keane, W. M., and Atkins, J. P.Evaluation and treatment of frontal sinus fractures.Otolaryngol. Head Neck Surg. 95: 19, 1986.
9. Ioannides, C., and Freihofer, H. P. Fractures of thefrontal sinus: Classification and its implications forsurgical treatment. Am. J. Otolaryngol. 20: 273, 1999.
10. Rohrich, R. J., and Hollier, L. The role of the naso-frontal duct in frontal sinus fracture management.J. Craniomaxillofac. Trauma 2: 31, 1996.
11. Lee, T. T., Ratzker, P. A., Galarza, M., and Villanueva,P. A. Early combined management of frontal sinusand orbital and facial fractures. J. Trauma 44: 665,1998.
12. Montgomery, W. W., and Pierce, D. L. Anterior osteo-plastic fat obliteration for frontal sinus: Clinical ex-perience and animal studies. Trans. Am. Acad. Oph-thalmol. Otolaryngol. 67: 46, 1963.
13. Luce, E. A. Frontal sinus fractures: Guidelines to man-agement. Plast. Reconstr. Surg. 80: 500, 1987.
14. Chen, D. J., Chen, C. T., Chen, Y. R., and Feng, G. M.Endoscopically assisted repair of frontal sinus frac-ture. J. Trauma 55: 378, 2003.
15. Strong, E. B., Buchalter, G. M., and Moulthrop, T. H.Endoscopic repair of isolated anterior table frontalsinus fractures. Arch. Facial Plast. Surg. 5: 514, 2003.
16. Stevens, M., and Kline, S. N. Management of frontalsinus fractures. J. Craniomaxillofac. Trauma 1: 29, 1995.
17. Haug, R. H., Van Sickels, J. E., and Jenkins, W. S. De-mographics and treatment options for orbital rooffractures. Oral Surg. Oral Med. Oral Pathol. Oral Radiol.Endod. 93: 238, 2002.
18. Xie, C., Mehendale, N., Barrett, D., Bui, C. J., and Metz-inger, S. E. 30-year retrospective review of frontalsinus fractures: The Charity Hospital experience.J. Craniomaxillofac. Trauma 6: 7, 2000.
19. Constantinidis, J., Weber, R., Brune, M., Draf, W., andIro, H. Cranialization of the frontal sinus: Indica-tions, technique and results (in German). H.N.O. 48:361, 2000.
20. Gonty, A. A., Marciani, R. D., and Adornato, D. C. Man-agement of frontal sinus fractures: A review of 33cases. J. Oral Maxillofac. Surg. 57: 372, 1999.
21. Godin, D. A., and Miller, R. H. Frontal sinus fractures.J. La. State Med. Soc. 150: 50, 1998.
22. Stanley, R. B., Jr. Management of severe frontobasilarskull fractures. Otolaryngol. Clin. North Am. 24: 139,1991.
23. Helmy, E. S., Koh, M. L., and Bays, R. A. Managementof frontal sinus fractures: Review of the literature andclinical update. Oral Surg. Oral Med. Oral Pathol. 69:137, 1990.
24. Wallis, A., and Donald, P. J. Frontal sinus fractures: Areview of 72 cases. Laryngoscope 98: 593, 1988.
25. Ducic, Y., and Stone, T. L. Frontal sinus obliterationusing a laterally based pedicled pericranial flap. La-ryngoscope 109: 541, 1999.
26. Jacobs, J. B. 100 years of frontal sinus surgery. Laryn-goscope 107: 83, 1997.
27. Wright, D. L., Hoffman, H. T., and Hoyt, D. B. Frontalsinus fractures in the pediatric population. Laryngo-scope 102: 1215, 1992.
28. Locher, M. C., Sailer, H. F., Haers, P. E., Carls, F. R.,Oechslin, C. K., and Gratz, K. W. Development of thefrontal sinus following bilateral fronto-orbital osteot-omies. J. Craniomaxillofac. Surg. 26: 129, 1998.
29. Aydinlioglu, A., Kavakli, A., and Erdem, S. Absence offrontal sinus in Turkish individuals. Yonsei Med. J. 44:215, 2003.
30. Nambiar, P., Naidu, M. D. K., and Subramaniam, K. An-atomical variability of the frontal sinuses and theirapplication in forensic identification. Clin. Anat. 12:16, 1999.
31. Kirk, N. J., Wood, R. J., and Goldstein, M. Skeletal iden-tification using the frontal sinus region: A retrospec-tive study of 39 cases. J. Forensic Sci. 47: 318, 2002.
32. Yavuzer, R., and Jackson, I. T. Coronal incision ex-tending postauricularly. Plast. Reconstr. Surg. 103:1532, 1999.
33. Owens, M., and Klotch, D. W. Use of bone for obliter-ation of the nasofrontal duct with the osteoplastic flap:A cat model. Laryngoscope 103: 883, 1993.
34. Rohrich, R. J., and Mickel, T. J. Frontal sinus oblitera-tion: In search of the ideal autogenous material. Plast.Reconstr. Surg. 95: 580, 1995.
35. Petruzelli, G. J., and Stankiewicz, J. A. Frontal sinusobliteration with hydroxyapatite cement. Laryngoscope112: 32, 2002.
92e PLASTIC AND RECONSTRUCTIVE SURGERY, May 2005

36. Kalavrezos, N. D., Gratz, K. W., Warnke, T., and Sailer,H. F. Frontal sinus fractures: Computed tomographyevaluation of sinus obliteration with lyophilized car-tilage. J. Craniomaxillofac. Surg. 27: 20, 1999.
37. Mickel, T. J., Rohrich, R. J., and Robinson, J. B., Jr.Frontal sinus obliteration: A comparison of fat, mus-cle, bone and spontaneous osteoneogenesis in the catmodel. Plast. Reconstr. Surg. 95: 586, 1995.
38. Montgomery, W. W. The fate of adipose implants in abony cavity. Laryngoscope 74: 816, 1964.
39. Weber, R., Draf, W., Keerl, R., et al. Osteoplastic frontalsinus surgery with fat obliteration: Technique andlong-term results using magnetic resonance imagingin 82 operations. Laryngoscope 110: 1037, 2000.
40. Donald, P. J. Frontal sinus ablation by cranialization:Report of 21 cases. Arch. Otolaryngol. 108: 142, 1982.
41. Keay, D. G., Dale, B. A., and Murray, J. A. Long-termcomplications of frontal sinus fractures. J. R. Coll. Surg.Edinb. 33: 95, 1988.
42. Dee, K. E., Newell, D. W., and Cohen, W. A. Subduralempyema after depressed frontal sinus fracture. A.J.R.Am. J. Roentgenol. 170: 790, 1998.
43. Rath, S. A., and Knoringer, P. Late brain abscess yearsafter severe cerebrocranial trauma with fronto-orbito-basal fracture. Childs Nerv. Syst. 5: 121, 1989.
44. Parhiscar, A., and Har-El, G. Frontal sinus obliterationwith the pericranial flap. Otolaryngol. Head Neck Surg.124: 304, 2001.
45. Disa, J. J., Robertson, B. C., Metzinger, S. E., and Manson,P. N. Transverse glabellar flap for obliteration/iso-lation of the nasofrontal duct from the anterior cra-nial base. Ann. Plast. Surg. 36: 453, 1996.
46. Thaller, S. R., and Donald, P. The use of pericranialflaps in frontal sinus fractures. Ann. Plast. Surg. 32: 284,1994.
47. Baroudi, I. F. Obliteration of decompressed frontal si-nus by means of deepithelialized island forehead flap.Plast. Reconstr. Surg. 77: 824, 1986.
48. Jackson, I. T., Adham, M., and Marsh R. Use of thegaleal frontalis myofascial flap in craniofacial surgery.Plast. Reconstr. Surg. 77: 905, 1986.
49. Snyderman, C. H., Janecka, I. P., Sekhar, L. N., Sen, C. N.,and Eibling, D. E. Anterior cranial base reconstruc-tion: Role of galeal and pericranial flaps. Laryngoscope100: 607, 1990.
50. Fukuta, K., Potparic, Z., Sugihara, T., Rachmiel, A., Forte,R., and Jackson, I. T. A cadaver investigation of theblood supply of the galea frontalis flap. Plast. Reconstr.Surg. 94: 794, 1994.
51. Jackson, I. T., and Smith, A. W. Reconstruction of alarge mandible defect utilizing a full-thickness vascu-larized calvarial bone graft. Eur. J. Plast. Surg. 21: 257,1998.
52. Rinehart, G. C., Jackson, I. T., Potparic, Z., Tan, R. G., andChambers, P. A. Management of locally aggressivesinus disease using craniofacial exposure and thegaleal frontalis fascia-muscle flap. Plast. Reconstr. Surg.92: 1219, 1993.
53. Abiraman, S., Varma, H. K., Umashankar, P. R., and John,A. Fibrin glue as an osteoinductive protein in amouse model. Biomaterials 23: 3023, 2002.
54. Tholpady, S. S., Schlosser, R., Spotnitz, W., Ogle, R. C.,and Lindsey, W. H. Repair of an osseous critical-sizedefect using augmented fibrin glue. Laryngoscope 109:1585, 1999.
Vol. 115, No. 6 / FRONTAL SINUS FRACTURES 93e