clinical spectrum of sick sinus syndrome -...
TRANSCRIPT

Clinical Spectrum of the Sick Sinus SyndromeBy JOEL J. RUBENSTEIN, M.D., CHARLES L. SCHULMAN, M.D.,
PETER M. YURCHAK, M.D., AND ROMAN W. DESANCTIS, M.D.
SUMMARYThe clinical spectrum of the sick sinus syndrome (SSS) is described in a series of
56 patients who demonstrated either persistent unexplained sinus bradyeardia (groupI: eight patients); sinus arrest (group II: 15 patients); or bradyeardia with episodicsupraventricular tachyarrhythmias (group III: 33 patients). Coronary disease was themost common form of heart disease where etiology could be determined, but in 25patients no clear etiologic diagnoses could be established. Thirty-three patients showedassociated electrocardiographic conduction disturbances. Symptoms were common
and were produced by both bradyeardia and tachycardia. Eight patients in thebradyeardia-tachyeardia group experienced cerebral embolization. Despite bother-some symptoms, only six of the 56 patients died over an average follow-up of 7 years,
and only one of these deaths appeared related to an arrhythmia. Drug therapy ofbradyeardia was generally ineffective, but digitalis was frequently helpful in patientswith tachycardia. Electrical pacing was uniformly successful in treating symptoms ofbradyeardia but was disappointing in preventing tachyarrhythmias.
Additional Indexing Words:Bradyeardia-tachyeardia syndromeSinus arrest Sinoatrial block
D EVELOPMENTS in electrical pacing ofthe heart during the past decade have
stimulated interest in mechanisms of brady-cardia in patients experiencing Adams-Stokessyncope. For the most part these attacks aredue to atrioventricular (A-V) block. However,an increasing number of patients have beendescribed in whom the basis of syncope hasbeen profound and unexplained sinus brady-cardia or sinus arrest. In addition to bradycar-dia, certain of these patients have recurrentepisodes of supraventricular tachyarrhyth-mias.
From the Department of Medicine, HarvardMedical School and Cardiac Unit, MassachusettsGeneral Hospital, Boston, Massachusetts.
Supported in part by U. S. Public Health ServiceGrants HE-5196 and HEP-06664.
Address for reprints: Dr. Joel J. Rubenstein,Cardiac Unit, Massachusetts General Hospital, Boston,Massachusetts 02114.
Received December 8, 1971; revision accepted forpublication March 8, 1972.
Circulation, Volume XLVI, July 1972
Conduction disturbances PacemakersSystemic embolism Sinus bradyeardia
The terms "sick sinus syndrome,"1-3 "inade-quate sinus mechanisms,"4 "sluggish sinusnode syndrome,"5 and "sinoatrial syncope"6have all been used to describe this phenome-non. When complicating supraventricular ar-rhythmias have been present, the conditionhas been termed "the syndrome of alternatingbradycardia and tachycardia,"7 or simply the"bradyeardia-tachyeardia syndrome" (BTS ).8We consider the sick sinus syndrome (SSS) tobe present in patients exhibiting otherwiseunexplained marked sinus bradyeardia orsinus arrest with or without associated supra-ventricular tachyarrhythmias. The mechanismof bradyeardia may be either disorderedimpulse generation within the sinus node orimpaired conduction of impulses from thesinus node into the atrium.Most previous reports have focused on the
necessity for and results of pacing in patientswith this type of bradyeardia.2 4 ' 9-lo Thepurpose of this communication is to describein broader terms the clinical spectrum of thesick sinus syndrome as observed in 56 patients
5
by guest on July 1, 2018http://circ.ahajournals.org/
Dow
nloaded from
RUBENSTEIN ET AL.
with this disorder encountered at the Massa-chusetts General Hospital. In addition totherapy, attention is called to etiology, symp-tomatology, and associated electrocardio-graphic abnormalities.
Patients and ClassificationPatients were collected from the clinical
material of the Massachusetts General Hospitaland from the private practices of the authors. Thecharts of 83 patients meeting the criteria of SSSwere reviewed. Of these, 56 were selected forinclusion, while 27 were excluded because of theprobability that the slow heart rates were theresult of medications (19 patients) or for lack ofsufficient clinical information (8 patients).The 56 patients were divided into three groups
on the basis of electrocardiographic manifesta-tions of SSS.Group I included eight patients with persistent
and otherwise unexplained extreme sinus brady-cardia at a heart rate of less than 50 beats/min.Generally the heart rate was between 40 and 50,though one patient had persistent bradyeardia of30 beats/min.Group II included 15 patients with at least one
documented episode of sinus arrest or sinoatrialblock, with A-V junctional or ventricular escapebeats. Of the 15 patients, five had sinusbradyeardia, nine were in regular sinus rhythm,and one exhibited permanent atrial arrest withA-V junctional rhythm.Group III included 33 patients with BTS. All
these patients exhibited either of the bradyeardicmechanisms of groups I and II. In addition, eachhad at least one documented episode of asupraventricular tachycardia, either paroxysmalatrial tachycardia (nine patients), atrial flutter(14 patients), or atrial fibrillation (27 patients).Thirteen patients exhibited more than one type oftachycardia, and in 28 the attacks were multiple.Mechanisms of bradyeardia included sinus brady-cardia in 14, intermittent sinus arrest in 16, andpermanent sinus arrest in three.
Table 1
Characteristics of the 56 Patients
GroupData I II III
Male (no.) 7 13Female (no.) 3 8 20Mean age (yr) 61 63 68Range 28-92 26-92 44-90
Age at onset (yr) 56 56 57Range 27-76 25-74 12-87
Follow-up (yr) 4 6 9
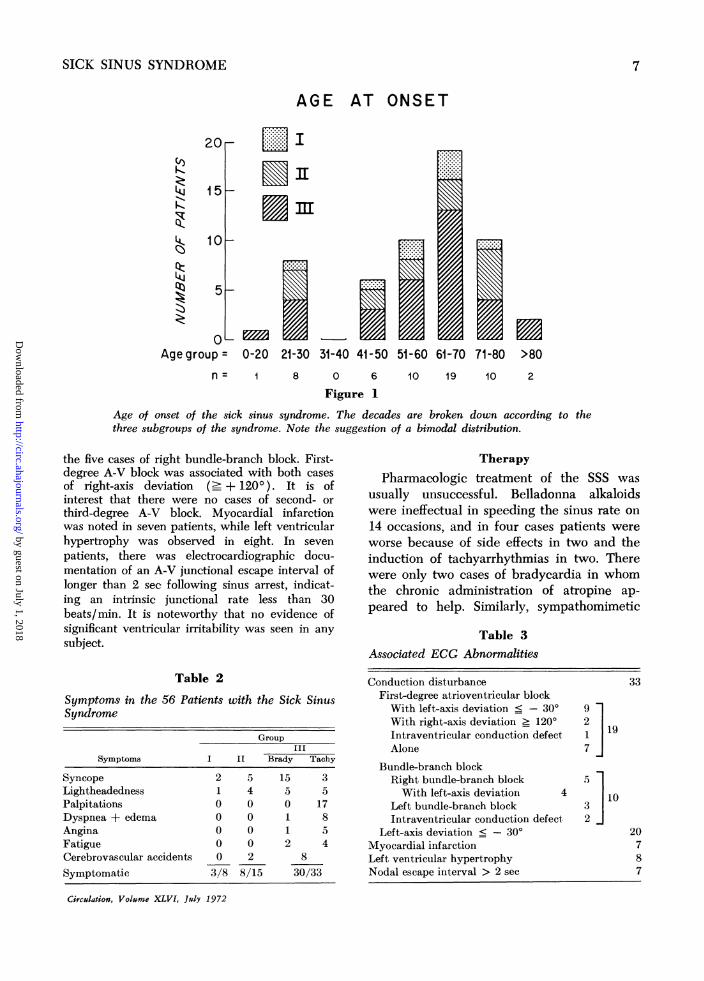
The series included 31 women and 25 menranging in age from 26 to 90 years with a meanage of 65 years. Table 1 shows the sex, age, ageof onset of either symptoms or electrocardiograph-ic diagnosis of the syndrome, and mean durationof follow-up for each of the three groups. Notethe female predominance in group III, the wideage ranges, and the long follow-up. Figure 1demonstrates a breakdown of the group by decileat age of onset of SSS. Although the numbers aresmall, there is a suggestion of a bimodaldistribution of the patients.
EtiologyThe diagnosis of coronary artery disease was
made in 20 patients on the basis of eitherhistorical or electrocardiographic evidence ofangina pectoris or myocardial infarction. Threepatients exhibited evidence of idiopathic cardi-omyopathy. Hypertensive heart disease waspresent in four. Single cases of luetic aorticinsufficiency, rheumatic heart disease, scleroder-ma, and congenital heart disease were noted. In25 patients no clear etiology could be determined.
SymptomsTable 2 lists symptoms noted in the three
groups. Forty-one of the 56 patients experiencedsymptoms related to the arrhythmias. Bradyeardiaalone was associated with symptoms in 19patients. In group III tachycardia alone causedsymptoms in 12 patients, and 10 patientsexperienced symptoms from both bradycardia andtachycardia.Syncope occurred in 25 patients and was
recurrent in 16. An additional 15 patientsreported a spectrum of symptoms varying fromlightheadedness to near-syncope.
There were 10 cerebrovascular accidents in theentire group, eight of them in the bradyeardia-tachycardia group, and two in group II. In eightcases, the strokes were thought to be due toemboli. Peripheral emboli were surgically re-moved from two patients in group III, one ofwhom had suffered a previous stroke.
Associated Electrocardiographic AbnormalitiesAbnormalities in addition to the rhythm were
encountered in the electrocardiograms of 37 ofthe 56 patients. These are documented in table 3.Some disturbance of conduction, either at thelevel of the A-V node or in the peripheral bundlebranches, was seen in 33 patients. First-degree A-V block (19 patients) and left-axis deviation
- 300) (20 patients) were most common.Complete bundle-branch block was nioted in 10patients. Combinations of disturbances frequenitlyoccurred. For example, left-axis deviationi ac-companied right bundle-branch block in foxur of
Circulation, Volumne XLVI. JulY 1972
6
by guest on July 1, 2018http://circ.ahajournals.org/
Dow
nloaded from
SICK SINUS SYNDROME
AGE AT ONSET
20(I)K
L. J
Qz~
15 -
10
5
Age gruAge group =
...............
L..I..I......--..--
......
,........,.........
0-20 21-30
-. -.............................
31-40 41-50 5i-60
. .....-.-.-.-.-.
.........
61-70 71-80 >808 0 6
Figure 110 19 10 2
Age of onset of the sick sinus syndrome. The decades are broken down according to thethree subgroups of the syndrome. Note the suggestion of a bimodal distribution.
the five cases of right bundle-branch block. First-degree A-V block was associated with both casesof right-axis deviation (': + 1200). It is ofinterest that there were no cases of second- orthird-degree A-V block. Myocardial infarctionwas noted in seven patients, while left ventricularhypertrophy was observed in eight. In sevenpatients, there was electrocardiographic docu-mentation of an A-V junctional escape interval oflonger than 2 sec following sinus arrest, indicat-ing an intrinsic junctional rate less than 30beats/min. It is noteworthy that no evidence ofsignificant ventricular irritability was seen in anysubject.
Table 2
Symptoms in the 56 Patients with the Sick SinusSyndrome
GroupIII
Symptoms I IL Brady Tachy
Syncope 2 5 15 3Lightheadedness 1 4 5 5Palpitations 0 0 0 17Dyspnea + edema 0 0 1 8Angina 0 0 1 5Fatigue 0 0 2 4Cerebrovascular accidents 0 2 8
Symptomatic 3/8 8/15 30/33
Circulation, Volume XLVI, July 1972
TherapyPharmacologic treatment of the SSS was
usually unsuccessful. Belladonna alkaloidswere ineffectual in speeding the sinus rate on14 occasions, and in four cases patients wereworse because of side effects in two and theinduction of tachyarrhythmias in two. Therewere only two cases of bradycardia in whomthe chronic administration of atropine ap-peared to help. Similarly, sympathomimetic
Table 3Associated ECG Abnormalities
Conduction disturbanceFirst-degree atrioventricular blockWith left-axis deviation < - 30°With right-axis deviation _ 120°Intraventricular conduction defectAlone
Bundle-branch blockRight bundle-branch blockWith left-axis deviation 4
Left bundle-branch blockIntraventricular conduction defect
Left-axis deviation _ - 30°Myocardial infarctionLeft ventricular hypertrophyNodal escape interval > 2 sec
33
9217I19
5
3 1032 j
20787
7
by guest on July 1, 2018http://circ.ahajournals.org/
Dow
nloaded from

RUBENSTEIN ET AL.
amines were inieffective in 11 cases, and fivepatients were worse because of side effects orthe inductioni of tachyarrhythmias. However,onie patient from group III was improvedfrom the chronic administration of ephedrine,anid another in group III benefited fromchroniic isoproterenol administration.Drug therapy directed at episodes of
tachyarrhythmia in group III patients wassimilarly frustrating and unrewarding. At-tempts to increase the basic heart rate andthus to suppress the arrhythmias with bella-donna alkaloids on seven occasions, or sympa-thomimetic amines on seven occasions, wereuniformly without benefit. Antiarrhythmicagents alone, including quinidine, procaina-mide, and propranolol, were of little help in11 cases. Only four of 22 patients whoreceived these agents were improved. Sevenpatients were worse, five because of increasein symptoms related to bradyeardia, to sinusarrest, or to further depression of the A-Vjunctional escape focus. Digitalis glycosideswere employed in 17 patients for symptomatictachycardia and benefited 10 by either de-creasing the frequency of tachyarrhythmia orcontrolling the ventricular response. However,despite improvement with digitalis therapy,additional antiarrhythmic drugs were deemednecessary in six of the 10 cases. In all, digitalisglycosides were used in 34 of the 56 patientsfor treatment of congestive heart failure ortachyarrhythmia. These drugs were frequentlyemployed following development of SSS, butoccasionally had been administered severalyears preceding the diagnosis. Digitalis waswithdrawn from 14 patients in an effort toabolish the bradyeardia, but without effect inany.
Cardioversion was used uneventfully on fiveoccasions to convert arrhythmias. It wasgenerally avoided because of the fear of aninadequate sinus rate following cardioversion.
Pacing was employed in 23 of 56 patients-permanently in 18 and temporarily in five.Long-term pacing was undertaken in 18 forsymptomatic bradycardia. In 16 this wasmanifested as episodes of transient cerebralhypoxia secondary to long sinus pauses. Two
were paced primarily to increase cardiacoutput, which was considered depressed bybradyeardia. The original site of long-termpacing was the right ventricle in 14 cases andthe right atrium in four. However, it wasnecessary to change the electrode site on twooccasions. In one case erratic atrial pacingnecessitated changing to ventricular pacing.In the other case serious hypotension relatedto retrograde V-A conduction during demandventricular pacing was eliminated with de-mand atrial pacing. All 18 patients wereimproved.An additional two patients with bradyeardia
were paced temporarily in an effort toimprove cardiac output. In neither case wasthe clinical course altered, and the temporaryelectrode was withdrawn.Among those 18 patients permanently
paced primarily for symptoms related tobradyeardia, 13 also had episodes of tachyar-rhythmias. In only two patients did thetachyarrhythmias appear to be suppressed bythe addition of the pacemaker alone. One ofthe two patients has recently reverted topermanent atrial fibrillation following 24months of freedom from arrhythmia withventricular pacing. In three others the pace-maker allowed more aggressive administrationof antiarrhythmic drugs. This combinationeliminated or reduced the frequency oftachyarrhythmias. Three additional patientswere paced temporarily in an effort tosuppress episodic tachyarrhythmia. When itwas clear that the clinical course was unal-tered, the temporary electrode was with-drawn.There were six deaths in the series during
an average follow-up of 7 years. However, inonly one case was the arrhythmia closelyrelated to the terminal episode.Postmortem data were available in only four
cases and revealed a spectrum of coronaryartery disease. This ranged from sclerotic butwidely patent vessels to marked atherosclero-sis with severe focal obstruction of all majorcoronary vessels in a patient with seleroderma.The myocardial pathology reflected the severi-ty of coronary artery disease, ranging from
Circulation, Volume XLVI, July 1972
8
by guest on July 1, 2018http://circ.ahajournals.org/
Dow
nloaded from

SICK SINUS SYNDROME
mild cytoplasmic vacuolization of myocardialcells and small patches of myocardial sclerosisto severe, dense, and widespread myocardialfibrosis with particular involvement of atrialmyocardium. Detailed examination of thespecialized conduction system was not carriedout.
Discussion
Altered function of the dominant pacemak-er of the heart, the S-A node, has long beenrecognized.16'8 Levine first described theelectrocardiographic features of S-A exit blockin 1916.'9 Most subsequent publications havedealt with electrocardiographic aspects of S-Ablock20 25 and atrial standstill.2>3' The firstreport of symptomatic sinus bradyeardia withAdams-Stokes attacks was that of Laslettin 1909.17 Other isolated case reportsfollowed.9' 32-34 A review of the subject ofsinus bradyeardia appearing in 1952 empha-sized exclusively the etiologic features.35 Therelationship between symptomatic bradyear-dia and paroxysmal supraventricular arrhyth-mias was first described by Short in 1954.7The term sick sinus syndrome was coined
by Lownl to describe rhythm disturbancesfollowing DC cardioversion of chronic atrialfibrillation. These phenomena included "cha-otic atrial activity, changing P wave contour,bradyeardia, interspersed with multiple andrecurrent ectopic beats, with runs of atrial andnodal tachycardia." Ferrer3 broadened thedefinition to include (1) persistent, severe,and unexpected sinus bradyeardia; (2) sinusarrest, brief or sustained, with escape atrial orA-V junctional rhythm; (3) prolonged sinusarrest with failure of subsidiary pacemakerresulting in total cardiac asystole; (4) chronicatrial fibrillation with slow ventricular re-sponse not due to drug therapy (she gave noexplanation for inclusion of this "non-sinus"rhythm in her definition.); and (5) inabilityof the heart to resume sinus rhythm followingelectroconversion for atrial fibrillation. Otherdescriptive terms have been applied to thisphenomenon, but sick sinus syndrome seemsthe simplest and most desirable.The clinical spectrum of SSS seen in our
Circulation, Volume XLVI, July 1972
material is wide, ranging from sinus bradyear-dia without symptoms to recurrent attacks ofsyncope or congestive failure. The questionarises whether asymptomatic sinus bradyear-dia (group I) can really be consideredabnormal, since sustained sinus bradyeardia isfound in association with many extracardiacfactors.35 It is regarded as physiologic in well-trained athletes. Although only three of the sixpatients in group I had symptoms related tobradyeardia, none was free of some evidenceof heart disease. Thus, we believe them tocomprise a portion of the spectrum of SSS, asdid Ferrer.3 Long-term follow-up of patientsin group I is not available, but it is very likelythat some may ultimately develop the rhythmdisturbances seen in groups II and III. In facta number of patients in our groups II and IIIhad sustained sinus bradyeardia for yearspreceding the documentation of sinus arrest ortachyarrhythmia. There is convincing evi-dence for derangements of S-A nodal functionin groups II and III. One patient in group IIand three in group III had permanent atrialarrest. Half of group III had intermittent sinusarrest as the mechanism of bradyeardia.Most recent descriptions2' 4, 6,9-15 of SSS
emphasize its frequent association with distur-bances of consciousness and the need for long-term pacing. It is not generally recognizedthat SSS may exhibit a wide range ofphenomena-from no symptoms at all, tofatigue and episodic lightheadedness, to franksyncope and/or congestive heart failure. Onefourth of our patients experienced no symp-toms, and those who were symptomatic haddisturbances of consciousness of variableseverity (40 of 56). A small number exhibitedcongestive heart failure as an importantcomplication of their disease. Bouvrain2 ana-lyzed a series of 63 cases of marked bradyear-dia, mostly related to recurrent S-A block. Ofthis number, 37 had chronic S-A block,unrelated to drug effects. Most patients wereelderly, and about one fourth had detectableunderlying coronary artery disease. Most wereasymptomatic, syncope occurring in 11 pa-tients but posing a problem in only five.Rasmussen15 reported 21 cases of chronic S-A
9
by guest on July 1, 2018http://circ.ahajournals.org/
Dow
nloaded from
RUBENSTEIN ET AL.
block, 15 of whom had Adams-Stokes attacks.Fourteen patients also had paroxysmal atrialarrhythmias. Seventeen of the group eventual-ly required permanent pacemaker implanta-tion. Easley et al.6 reported 13 patients withwhat they termed sinoatrial syncope. Eight ofthe group had other symptoms as well, chieflyangina pectoris and congestive failure. Theyclassified their series into two groups, thosewith only bradyarrhythmias, and those withalternating brady- and tachyarrhythmias.They emphasized, as have others, the difficulttherapeutic problem presented by the lattergroup.An unexpected and important feature of the
BTS noted by us is the occurrence of systemicembolization in eight of 33 patients. Presum-ably stasis in the atria associated with thetachyarrhythmias promoted mural thrombusformation. On the basis of our experience,anticoagulant therapy should be considered inthese patients if their general conditionwarrants it and if there is no contraindicationto such therapy.Remarkably absent from all patients report-
ed in our series and in those of others areserious ventricular arrhythmias. Although slowheart rates are known to promote appearanceof ventricular ectopic activity, this has notbeen a feature of SSS.The exact etiology of SSS remains obscure.
Information from pathologic examination ismeager. The basic process is presumablydegenerative change in the S-A node, eitherprimary or secondary to some vascular dis-ease. Myocardial biopsy in two family mem-bers with persistent atrial standstill showedamyloid deposits,31 but no parallel cases haveappeared. Rasmussen'5 believed the disease tobe a sequel of diphtheria in his patients fromScandinavia, but could offer only one exampleto support this thesis. Two patients reportedby Bouvrain et al.2 first developed SSS duringan attack of diphtheria. Winternitz andSelye36 reported a patient with sinus brady-cardia of 43-47 beats/min due to thrombosisof the artery to the S-A node. James37 haspointed out the vulnerability of the S-A node
to vascular damage by virtue of receiving itsentire blood supply from a single artery. TheS-A node artery also supplies the atria, anddisease of this vessel might be expected toaffect stability of the atrial rhythm, a possibleexplanation for the BTS.The most common etiology in our material
was coronary disease, seen in 20 patients. Yetno specific diagnosis could be established in astill larger number (25 patients). It isprobable that older subjects in this undiag-nosed group will prove to have coronarydisease, while some younger subjects willprove to have cardiomyopathy. It is worthpointing out that bradycardic rhythm distur-bances have only rarely been mentioned in thelarge reported series of patients with cardio-myopathy.3840 Some patients in either agegroup may have a primary degenerativeprocess involving the S-A node artery, or thespecialized conduction tissue. Detailed exami-nation of the S-A node in one of our fourpatients coming to autopsy showed degenera-tive changes, but no evidence of arteriopathyinvolving its artery.
Several authors have pointed out that notinfrequently more than the S-A node isdiseased in SSS.2, 41. 42 Electrocardiographicevidence for widespread abnormalities ofimpulse formation and conduction among ourpatients with the SSS is impressive (table 3).Nineteen subjects had some degree of A-Vblock, and 10 had intraventricular conductiondisturbances. Abnormal left-axis deviation in20 subjects can be offered as evidence of im-paired conduction in the anterior division ofthe main left bundle branch. Evidence ofgeneralized dysfunction of the conductionsystem has been demonstrated with Hisbundle recordings and with atrial pacing.41 42These abnormalities include impaired impulseformation by lower automatic centers. Ordi-narily pacemaker cells in the A-V junctionprovide escape beats at rates of 40-50 beats/min when the S-A node defaults. Seven of ourpatients failed to generate A-V junctionalescape beats at the usual rate, permittingsinus rates as low as 30 beats/min.
Circulation, Volume XLVI, July 1972
10
by guest on July 1, 2018http://circ.ahajournals.org/
Dow
nloaded from
SICK SINUS SYNDROME
With regard to therapy, none is indicatedfor bradycardia without symptoms. Bradycar-dia leading to disturbances of consciousness orfrank syncope is best treated with pacemakerimplantation. Drug therapy alone appears tohave little value, a conclusion voiced also byothers.6 14, 15 Nine of our series (16%) hadsyncope only once, and a solitary attack ofsyncope did not seem to merit pacemakerimplantation. Syncope occurred repeatedly in16 patients, all of whom required permanentpacemaker implantation. An average of 3Myears elapsed between onset of symptoms andthe need for pacemaker implantation. Onlyone of the six deaths in our series appearedrelated in any way to the arrhythmia. Thevariability in symptomatology and prognosisemphasizes the need to individualize therapy.
Bradycardia associated with evidence ofcongestive heart failure can be managed bydigitalis, with vigilance for any unexpectedeffects of this agent on the diseased S-A node.Should this occur, pacemaker implantationmay be necessary as an adjunct to drugtherapy of heart failure.Treatment of BTS merits special comment.
Previous authors have emphasized the difficulttherapeutic problem posed by patients withthis entity. 6, 10-13, 4 4 Therapy for tachyar-rhythmia with digitalis and/or conventionalantiarrhythmic agents may be associated withmarked bradycardia and syncope followingreversion to normal rhythm. This is presum-ably due to depression of endogenous pace-makers by the drugs. Atropine, given forbradyeardia, may promote the appearance oftachyarrhythmia. It was not until the adventof pacemakers that a satisfactory solution ofthe bradycardic aspect of the BTS was athand. Since the first report10 of a patientsuccessfully treated with a permanent pace-maker a number of reports have reiterated itsvalue.6' 3, 15
In general, pacing has failed to preventbouts of tachyarrhythmia. However, implanta-tion of a pacemaker may be of value bypermitting the addition of digitalis and/orantiarrhythmic preparations to the therapeuticprogram without fear of aggravating theCirculation, Volume XLVI, July 1972
effects of bradyeardia. Five of our patientswith BTS treated by combined pacing anddrugs have had a reduction in the frequencyof tachyarrhythmia. In the truly refractorycase of recurrent supraventricular tachycardia,consideration may be given to the veryaggressive procedure of sectioning the Hisbundle in combination with ventricularpacing.2With regard to the site of pacing, there is
theoretic advantage to atrial pacing becausethe contribution of atrial systole to cardiacoutput is preserved. In one of our cases, atrialpacing was successful when ventricular pacingfailed to maintain cardiac output. However,the lesser reliability of atrial pacing and thehigh incidence of A-V conduction distur-bances in these patients has led us to select aventricular site for pacing in the majority ofour cases.
Finally, the recently developed "bifocal"demand pacemaker may prove useful in thesepatients.45 This pacemaker involves the use oftwo electrodes, one positioned in the rightatrium and one in the right ventricle, withboth atrial and ventricular pacing circuits. Theventricular electrode senses the ventricularelectrocardiogram and sequentially paces theatrium and ventricle on demand. In thepresence of sinus bradyeardia and intact A-Vconduction, the atrium is paced and theventricular circuit is blocked by the conductedbeat.
References1. LOWN B: Electrical reversion of cardiac arrhyth-
mias. Brit Heart J 29: 469, 19672. BOUVRAIN Y, SLAMA R, TEMKINE J: Le bloc
sino-auriculaire et les "maladies du sinus":Reflexions a propos de 63 observations. ArchMal Coeur 60: 753, 1967
3. FERRER M: The sick sinus syndrome in atrialdisease. JAMA 206: 645, 1968
4. SILVERMAN LF, MANKIN HT, MCGOoN DC:Surgical treatment of an inadequate sinusmechanism by implantation of a right atrialpacemaker electrode. J Thorac CardiovascSurg 55: 264, 1968
5. 1TABATZNIK B, MOWER MM, SAMSON EB,PREMPREE A: Syncope in the "sluggish sinusnode syndrome." Circulation 40 (suppl III):III-200, 1969
11
by guest on July 1, 2018http://circ.ahajournals.org/
Dow
nloaded from

RUBENSTEIN ET AL.
6. EASLEY RM, GOLDSTEIN S: Sino-atrial syncope.Amer J Med 50: 166, 1971
7. SHORT DS: The syndrome of alternating brady-cardia and tachycardia. Brit Heart J 16: 208,1954
8. SCHULMIAN CL, RUBENSTEIN JJ, YURCHAK PM,DESANcrIS RW: The "sick sinus" syndrome:Clinical spectrum. Circulation 17 (suppl III):III-42, 1970
9. MIULLER OF, FINKELSTEIN D: Adams-Stokessyndrome due to sinoatrial block. Amer JCardiol 17: 433, 1966
10. COHEN HE, KAHN M, DONoso E: Treatment ofsupraventricular tachyeardias with catheter andpermanent pacemakers. Amer J Cardiol 20:735, 1967
11. CHENG TO: Transvenous ventricular pacing inthe treatment of paroxysmal atrial tachyar-rhythmias alternating with sinus bradyeardiaand standstill. Amer J Cardiol 22: 874, 1968
12. ADELMAN AG, WICLE ED: The bradyeardia,tachycardia, asystole syndrome: Treatment bya pacemaker. Canad Med Ass J 100: 75,1969
13. SANDOE E, FLENsTED-Jensen E: Adams-Stokesseizures in patients with attacks of both tachy-and bradyeardia, a therapeutical challenge.Acta Med Scand 186: 111, 1969
14. FOWLER NO, FENTON JC, CONWAY GF: Syncopeand cerebral dysfunction caused by bradyear-dia without atrioventricular block. Amer HeartJ 80: 303, 1970
15. RASMUSSEN K: Chronic sinoatrial heart block.Amer Heart J 81: 38, 1971
16. WENCKEBACH KF: Beitrage zur Kenntnis dermenschlichen Herztatigkeit. Arch Physiol(Leipzig) 297: 354, 1906
17. LAsLETT EE: Syncopal attacks, associated withprolonged arrest of the whole heart. Quart JMed 2: 348, 1909
18. BARLOW P: The clinical occurrence of sino-auricular block. Lancet 1: 65, 1927
19. LEVINE SA: Observations on sino-auricular heartblock, Arch Intern Med (Chicago) 17: 153,1916
20. DE ZARDAY I: Unusual features of two cases ofsino-auricular block. Amer Heart J 12: 339,1936
21. COWAN J: Some disturbances of the rhythm ofthe heart. Brit Heart J 1: 3, 1939
22. WINTON SS: Sino-auricular block: An analysis ofeleven cases. Acta Cardiol 3: 108, 1948
23. GREENWOOD RJ, FINKELSTEIN D, MONHEIT R:Sinoatrial heart block with Wenckebach phe-nomenon. Amer J Cardiol 8: 140, 1961
24. SCHAMROTH L, DovE E: The Wenckebach
phenomenon in sino-atrial block. Brit Heart J28: 350, 1966
25. NAKAMOTO K: Second degree sinoatrial blockwith the Wenckebach phenomenon associatedwith nodal escape and second degree atrio-ventricular block and its conversion to regularsinus rhythm by sympathetic stimulation:Report of a case. Jap Circ J 33: 553, 1969
26. ROSENBAUM FF, LEVINE SA: Auricular stand-still: Its occurrence and significance. Amer JMed Sci 198: 774, 1939
27. MAGNUSSON P: Auricular standstill. Acta MedScand 123: 519, 1946
28. BLOOMFIELD DA, SINCLAIR-SMITH BC: Persis-tent atrial standstill. Amer J Med 39: 335,1965
29. WADA M, TAKADA C, MISE J: A case report ofatrial standstill. Jap Circ J 30: 543, 1966
30. MESSINGER WJ, MIRKINSON AM: Permanentatrial standstill. Arch Intern Med (Chicago)124: 211, 1969
31. ALLENSWORTH DC, RICE GJ, LOWE GW:Persistent atrial standstill in a family withmyocardial disease. Amer J Med 47: 775,1969
32. ANDERSEN MS: A case of sino-auricular heart-block with Stokes-Adams attacks. Acta MedScand 78: 216,1932
33. PEARSON RSB: Sinus bradyeardia with cardiacasystole. Brit Heart J 7: 85, 1945
34. TUNA N, SCOTT JW: Stokes-Adams attacks withsimultaneous auricular and ventricular stand-still. Circulation 4: 853, 1954
35. KIRK JE, KVORNING SA: Sinus bradyeardia: Aclinical study of 515 consecutive cases. ActaMed Scand (suppl 266): 625, 1952
36. WINTERNITZ M, SELYE H: Ein Fall von
Sinusbradykardie durch sinus-arterienthrom-bose. Wien Arch Med 16: 377, 1929
37. JAMES TN: Anatomy of the Coronary Arteries.New York, Paul B. Hoeber, Inc., 1961
38. DYE CL, ROSENBAUM D, LOWE JC, BEHNKE RH,GENOVESE PD: Primary myocardial disease: I.Clinical features. Ann Intern Med 58: 426,1963
39. MASsuMi RA, Rios JC, GOOcH AS, NUrrER D,DEVITA VT, DATLOW DW: Primary myocar-dial disease: Report of 50 cases and review ofthe subject. Circulation 31: 19, 1965
40. HAMBY RI, RAIA F: Electrocardiographic aspectsof primary myocardial disease in 60 patients.Amer Heart J 76: 316, 1968
41. ROSEN KM, LOEB HS, SINNO MZ, RAHIMTOOLASH, GUNNAR RM: Cardiac conduction inpatients with symptomatic sinus node disease.Circulation 43: 836, 1971
42. MANDEL W, HAYAKAWA H, DANZIG R, MARCUS
Circulation, Volume XLVI, July 1972
12
by guest on July 1, 2018http://circ.ahajournals.org/
Dow
nloaded from

SICK SINUS SYNDROME
HS: Evaluation of sino-atrial node function inman by overdrive suppression. Circulation 44:59, 1971
43. BIRCHFIELD RI, MENEFEE EE, BRYANT G.D.N.:Disease of the sinoatrial node associated withbradyeardia, asystole, syncope, and paroxysmalatrial fibrillation. Circulation 16: 20, 1957
44. BRADLOW BA: Supraventricular paroxysmaltachycardia interrupted by repeated episodes oftotal cardiac standstill with syncopal attacks.Chest 58: 122, 1970
45. CASTILLO CA, BERKOVITs BV, CASTELLANOS AJR, LEMBERG L, CALLARD G, JUDE JR: Bifocaldemand pacing. Chest 59: 360, 1971
Circulation, Volume XLVI, July 1972
13
by guest on July 1, 2018http://circ.ahajournals.org/
Dow
nloaded from

ROMAN W. DESANCTISJOEL J. RUBENSTEIN, CHARLES L. SCHULMAN, PETER M. YURCHAK and
Clinical Spectrum of the Sick Sinus Syndrome
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1972 American Heart Association, Inc. All rights reserved.
75231is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TXCirculation
doi: 10.1161/01.CIR.46.1.51972;46:5-13Circulation.
http://circ.ahajournals.org/content/46/1/5located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer
of the Web page under Services. Further information about this process is available in thewhich permission is being requested is located, click Request Permissions in the middle columnClearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service of the CopyrightCirculationoriginally published in Requests for permissions to reproduce figures, tables, or portions of articlesPermissions:
by guest on July 1, 2018http://circ.ahajournals.org/
Dow
nloaded from