clinical safety & effectiveness - ut health san antoniouthscsa.edu/cpshp/cseproject/increasing...
TRANSCRIPT

Clinical Safety & EffectivenessIncreasing Palliative Care Consultations
in the Medical Intensive Care Unit
DATEEducating for Quality Improvement & Patient Safety
Deborah Villarreal, MDJenifer Healy, DOLinda May, MD

Why Is Palliative Care Essential in the ICU?
After receiving ICU treatment many patients:
Die in ICU or soon after ICU care 1/5 dies following treatment in an ICU, 20%, 500,000 US/year
Remain “chronically critically ill” 100,000 ICU “survivors” in the US at any point in time who continue
with critical illness on a chronic basis
Nelson JE et al. Am J Respiratory Crit Care Med 2010 Angus DC et al. Crit Care Med 2004; 32: 6380-643.

DeathBereavement
Disease Modifying TherapyCurative, or Restorative intent
Critical CareLifeClosure
Diagnosis Palliative Care Hospice
Conceptual Model:
Palliative Care in the MICU

Care plan matches patient’s
goals
Focus
Dedicated Team
Follow Through
Decision MakingClarity
Time
Shouldn’t all clinicians be good at Palliative Care?
Of Course!Primary Palliative CareSecondary Palliative CareTertiary Palliative Care
Von Gunten, MD, PhD JAMA 2002
What Defines Quality?RWJ Critical Care Peer Workgroup:
Domains of ICU Palliative Care Quality
Symptom management and comfort careCommunication within team and with
patients/familiesPatient- and family-centered decision makingEmotional and practical support for patients and
familiesSpiritual support for patients and familiesContinuity of careEmotional and organizational support for ICU
clinicians
Clarke et al. Crit Care Med 2003; 31:2255-2262.

Selecky PA et al. Chest 2005;128:3599-610. (American College of Chest Physicians)
Lanken PN et al. Am J Respir Crit Care Med 2008;177:912-27. (American Thoracic Society)
Truog RD et al. Crit Care Med 2008;36:953-63. (American College of Critical Care Medicine)
Institute of Medicine (IOM)
Veterans Administration Healthcare System
Institute for Healthcare Improvement
Commercial insurers
Palliative Care in the ICU has been prioritized
Clinical Practice is lagging…
Much is now known about effective strategies for ICU Palliative Care quality improvement.
These methods can be applied to improve ICU Palliative Care.
Palliative Care is linked to ”Giving Up”: a major barrier to providing quality care for our pat/families

Palliative Care Publications 2010

Palliative Care Media Highlights 2010

► Communication by Clinicians: -timely, ongoing, clear, complete, sensitive
-addressing condition, prognosis, treatment
► Patient-Focused Decision-Making:-aligned with values, goals, preferences
► Clinical Care of the Patient:-comfort, dignity, personhood, privacy
► Care of the Family:-proximity/access, support including bereavement care
Nelson JE, Puntillo KA, Pronovost PJ, Walker AS, McAdam JL, Ilaoa D, Penrod J. Crit Care Med 2010;38:808.
N=48 subjects (15 pts, Fam); Focused group
What do our patients/families want? Define High-Quality ICU Palliative Care

And What They Get …
Not enough contact with MD: 78%Not enough emotional support (pt): 51%Not enough emotional support (family): 38%
Not enough information about whatto expect with the dying process: 50%
Not enough help with pain/SOB: 19%
Teno et al. JAMA 2004;291:88-93.N=1578 descendents (NH, hosptial)

More Medical Care Leads to LowerEmotional Satisfaction With Care
Family members of decedents in high-intensity hospital service areas report lower quality of: Inadequate Emotional support decedent (RR=1.2, 95%, CI=1.0–1.4)
Concerns Shared decision-making (RR=1.8, 95% CI=1.0–2.9),
Information about what to expect(RR=1.5, 95% CI=1.3–1.8)
Teno et al. JAGS 2005;53:1905-11. High (n=365) vs low (n=413)

Serious adverse outcomes for bereaved caregivers
Wright et al. JCO 2010: Sept 13 Place of death: Correlation with QOL of pats with cancer and predictors of bereaved CG mental health.
-Death in ICU and Hospital vs. Death at home/Hospice N=342, enrollment, 2 wks, 6 mo, QOL, psychiatric
-Death in ICU associated with 5X family risk of PTSD-Death in hospital associated with 8.8 X family risk of prolonged grief disorder
Anderson WG et al. J Gen Intern Med 2008; 23:1872. N=50 families-Anxiety/depression in ICU and 1 mo and 6 months later. (42% - 15%; 16%-6%)-PTSD and complicated grief at 6 months. (35%)
Paparrigopoulos T et al. J Psychosom Res 2006; 61:719. N=32 families-High rates of anxiety, depressive (87%), and posttraumatic stress symptoms (81%)
within a week of ICU admission.-At 3-2 days prior ICU discharge PTSD persisted in families (59%).
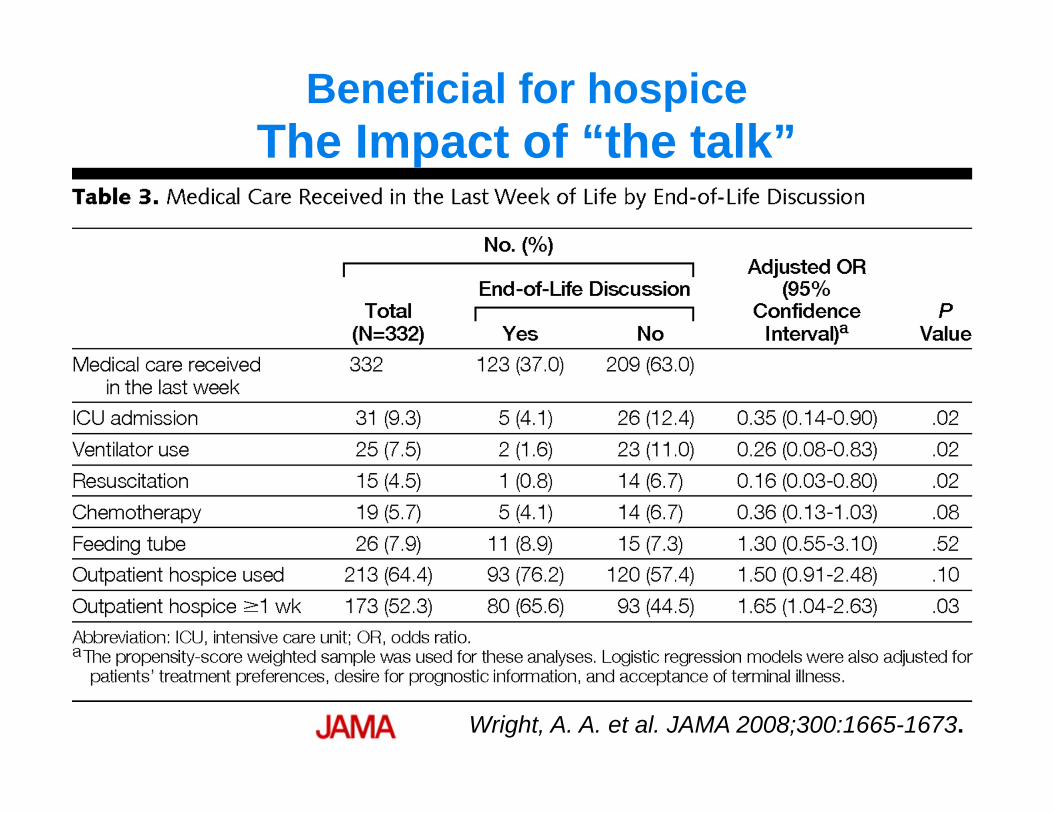
Wright, A. A. et al. JAMA 2008;300:1665-1673.
Beneficial for hospice The Impact of “the talk”

OutcomesOutcome Study↓ ICU/Hospital Length of Stay Norton, Quill et al. 2007 n=191,
Criteria, 8 to 16 d p=.0001
↓ Time from Poor Prognosis to Comfort‐ Focused Goals (Proactive Palli C/S)
Campbell 2003n=332, 7.3 to 2.2 d 6.3 to 3.5 d for MOF, CVp=<.05; No MDD in families
↑ Family Satisfaction/Comprehension Curtis 2004 n=214 FM; MD 71%, FM 29%
↓ Conflict over Goals of Care Curtis 2004↑ Symptom Assessment↑ Patient Comfort
Erdek 2003; SICU QI, 10 pt/wk for 5 wks, Q4h, 42% to 71% pain assessment,59%- 97% pain management, VAS

Why focus on MICU? FY10: # of Inpatient Deaths/Unit
UNIT # DEATHS5 MICU 68ECTC‐1 68KTC2B 255A MED 246 CCU 216B MED 15KTC3 142 SICU 13K5B MED 115 PCU 10ECTC‐2 94 SOUTH 7KTCC1 6KTC2A 57 BMT 3GLD SCI 1
“Slick Willie”Famous Bank
Robber
That where the money is ….

FY 10: % of MICU Patients who Died with a Geriatric Palliative Care Consultation
0.00%5.00%
10.00%15.00%20.00%25.00%30.00%35.00%40.00%45.00%50.00%
October December February April June
% MICU Deaths with PC Consult
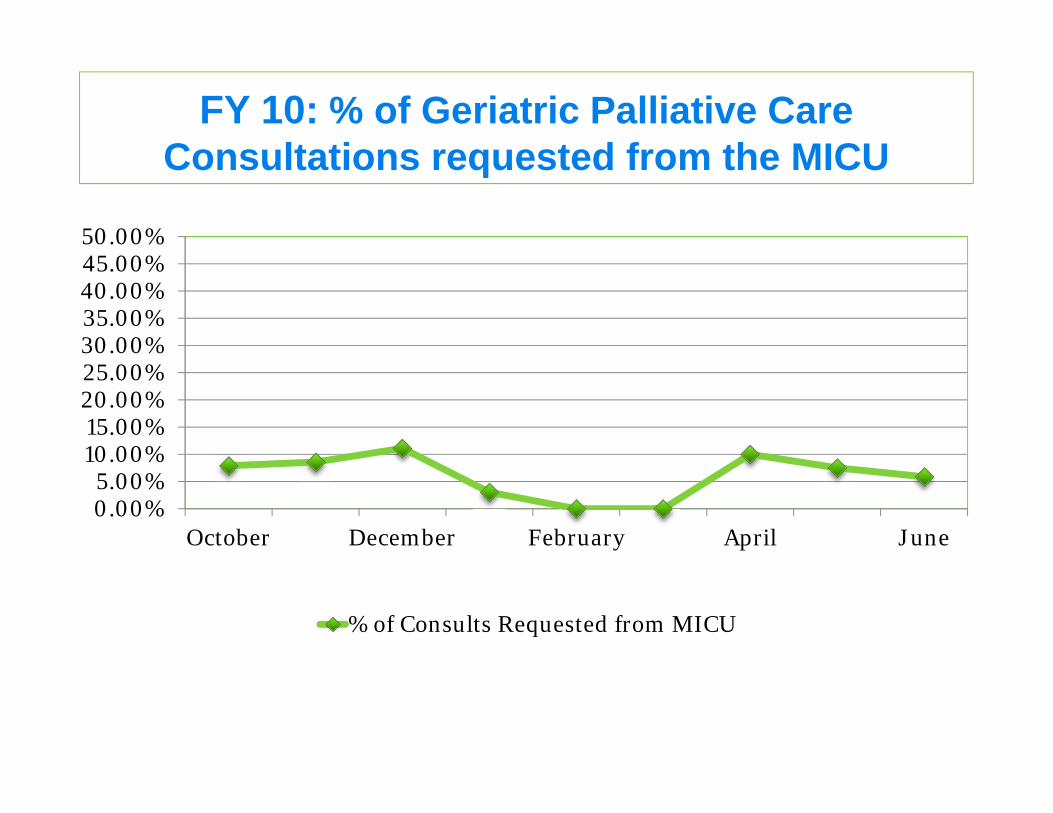
FY 10: % of Geriatric Palliative Care Consultations requested from the MICU
0.00%5.00%
10.00%15.00%20.00%25.00%30.00%35.00%40.00%45.00%50.00%
October December February April June
% of Consults Requested from MICU

Education/ProcessFamily/Patient
.
Lack of understanding of what palliative care can add
MD/RN
No incentives for increasing palliative care utilization
No mandatory training for MD or nurses in palliative care/issues
No Policy or service agreement in place for patients who meet criteria
Lack of understanding of impact of the palliative care in the Intensive care
Lack of Advance Directives and discussions about the future
.Lack of education in palliative care
Nurses/Social work are not empowered to recommend palliative care to MDs
-Patients/Families die without palliative care services (SW, Chaplain, psychologist, Pharm D, MD) and Bereavement Services-PC is entered later inthe hospitalization
Problem Statement
Lack of understanding that palliative care does not mean giving up
Too many priority focus areas for the learners, so palliative care can be low priority
Fragmentation
Policy
Unrealistic GoalsLack of knowledge concerning appropriate criteria for trigger for consultation

The ParadigmIntegrate Geriatric Palliative Care in the ICU
beginning at ICU admission regardless of prognosis
part of the comprehensive critical care plan
Overall Goal: Increase the frequency/timeliness of Geriatric Palliative Care Medicine consultations

Aim Statement
To increase the percent of patients who are referred for a Geriatric Palliative Care Medicine consultation at the STVHCS MICU from 10% to 40% during October 2010 to Dec 2010.
Primary Measures
# MICU Patients with a GPC consult
# total MICU patients
# MICU Patients who Died with a GPC consult
# total MICU patients who Died
GPC: Geriatric Palliative Consultation

Measures
Demographics Diagnosis Discharge Location (Home, SNF, Hospice
(home/inpatient, Died, still in MICU/hospital) % Documented Social Work support and Spiritual
support

Patient Enters the
MICU
MICU staff assesses and manages the
patient
Is patient stable for transfer?
Patient is not stabilized despite aggressive
life-sustaining therapies
Patient leaves MICU
Yes
No
MICU staff recommends comfort care
Patient Dies or leaves MICU without Geriatric Palliative
Consult
Palliative/Hospice care ConsultProvides patient/family
additional support for decision making, symptom control and assistance with
disposition /f/u/bereavement
No
Family Yes
Patient Dies or leaves MICU
with Palliative care Consult
Mixed Model:“Clinical Triggers”
Engage MICU to discuss Case-by -Case
Flow ChartMICU staff places GP
C/S
Yes

“Clinical Triggers”Baseline patient characteristics Preexisting functional dependency with ≥1 chronic life-limiting conditions
(e.g.dementia) Advanced-stage malignancy Admission from a community hospice, or on “comfort measures only” ALS /neuromuscular disease considering mechanical ventilation/BIPAP,
feeding tube Recurrent admissions (>2/year) End Stage of COPD
Selected Acute diagnosis Global Cerebral ischemia Intra-cerebral hemorrhage requiring mechanical ventilation Status post cardiac or respiratory arrest Prolonged dysfunction of multiple organs (multi-system organ failure) Status Epilepticus > 24 hrs
Adapted from Mt Carmel, MSM, Nelson et al. 2010; Crit Care Med; 38: 1765-72

“Clinical Triggers”
Healthcare Use Prolonged or failed wean from the ventilator DNR and DNI status established or requested Decision to forego life-sustaining therapies with expected death
Family Characteristics Psychological or spiritual distress Family distress impairing surrogate decision-making, complex decision
making Family request for information regarding palliative care or hospice
appropriateness
Adapted from Mt Carmel, MSM, Nelson et al. 2010; Crit Care Med; 38: 1765-72

Interventions: Education/Collaboration
Interdisciplinary (IDT) Workgroup: -MICU Leaders: medical director Dr. Restrepo
nurse director Janet Tidwell-MICU IDT staff/champions: Chaplain Robert Bellin,
RN Robbie/Alodia, Clerk Tom Cardinal-GPC staff: Bonnie Howard, RN/CNS-GPC Fellow: Dr. Jennifer Healy -Incoming Resident: Dr. Linda May-Information systems (Karla Strawn), Statistician
(Shuko Lee), Dr. Linda May

Interventions: Education/Collaboration
Key Persons: Critical Care Fellows/Residents Social worker Jennifer Kelley,
Collaborators: Dr. Judith Nelson (VISN 3, VHA Inc., Comfort Bundle, IPAL-ICU NIA Grant)
UT Clinical Safety & Effectiveness Course (UT HSC: Dr. Jan Patterson, Amruta Patel, Edna Cruz, MD Anderson: Wayne Fisher )
Results“ Yo u C a n n o t I m p r o v e W h a t Yo u C a n n o t M e a s u r e . ”
- B u s i n e s s A d a g e , U s e d B y D o n B e r w i c k ( I H I )
Palliative Care in the ICU:Bringing the Evidence to the Bedside

Table: Patient Characteristics/LOS June, Aug-SeptN=85
Oct-Dec N=78
Age 65.4 ± 11.3 64.7 ± 11.0Gender (Male) 84 (97.7) 112 (96.6)
Ethnicity
WhiteHispanic/LatinoBlackAsianOther
4833 3 2 0
871951 4
Diagnosis
Cancer 4SepsisRFOther (MOF, ESLD, CV, ESRD)
16 4 10 56
6 11 1584
Length of Stay in Hospital 3.3 ± 4.0 5.4 ± 8.4Discharge Type
HomeSkilled Nursing Home/ECTCDeath in HospitalHospiceStill in Hospital
55 8 15 7 0
48 29 23 57

CL 0.044
0.265
UCL0.148
0.477
LCL
0.053
0.000
0.100
0.200
0.300
0.400
0.500
0.600
Jun Aug Sep Oct Nov Dec
# C
onsu
lts C
ompl
eted
from
MIC
U
Time Period
# of Paliative Care Consults Completed from MICU at STVHCS
Pre Interventiondata
Post intervention data

CL 0.083
0.938
UCL0.454
1.000
LCL
0.424
0.000
0.200
0.400
0.600
0.800
1.000
1.200
Jun Aug Sep Oct Nov Dec
#M
ICU
Dea
ths
with
Con
sult
Time Period
# MICU Deaths with Palliative Care Consult
Pre intervention data
Post intervention data

Conclusions
More MICU patients and families received GPC services:-We provided support for more patients who were expected to benefit from ICU treatment and those who died.
Aim: To increase the percent of patients who are referred for a Geriatric Palliative Care Medicine consultation at the STVHCS MICU from 10% to 40% during October 2010 to Dec 2010.

Lessons Learned
Work force is #1 Major Barrier Work processes and systems (rounding,
predictability, turnover) Sustainability Interval Management with stakeholders and
workgroup key BUY-IN is crucialCulture change-Still not viewed as standard of
care, goals of care conversations start early!

Lessons Learned
Defining a “Clinical Triggers” criteria Understanding what we can offer: Acute and
chronic have different needs, skills Fragmentation – RoundsOpportunities for Education: GPC is only for
when someone is actively dyingNeed for IT resources for data collection,
accessibility of data: lag time

Next Steps
PC team is working on new projects/collaboration
Education: Knowledge and skills needed clinicians and patients and families (Pocket Cards, RN/MD orientation, modules, videos, surveys, focus groups)
Increase IDT family meetings (MD/RN/SW), Templates
Bereavement/Anticipatory Grief Support Templates/Implementation/Interventions, “Bereavement Bags”

“Care and Communication Bundle” of ICU Palliative Care Quality Measures
Day 1(1) Identify Decision-Maker (2) Address AD status(3) Address CPR status(4) Distribute informational
pamphlet to family(5) Assess pain regularly(6) Manage pain optimally
Day 3(7) Offer Social Work support(8) Offer Spiritual support
Day 5(9) Family Meeting
Nelson and Pronovost 2006; Quality and Safety in Health Care; 15:264-271.www.qualitymeasures.ahrq.gov
Acknowledgements MICU MD, RN leaders (Marcos Restrepo MD, Janet
Tidwell RN), Jay I. Peters MD, RNs GPC team: Jennifer Healy MD, Bonnie Howard, RN Sandra Sanchez-Reilly, MD Mentor Jeanette Ross MD, Dr. Linda Gray GRECC Sara Espinosa, MD MSc, Karla Strawn Scotte Hartronft MD, Michael Lichtenstein MD MSc Collaborator Judith Nelson MD (ICU-IPAL, NIH grant) UT-Clinical Safety and Effectiveness (Jan Patterson MD,
Amruta Patel, Wayne Fisher) CAPC : Diane Meier MD, David Weismann MD,

40
Thank you!
Educating for Quality Improvement & Patient Safety