clinical research conotruncal defects associated … · clinical research conotruncal defects...
TRANSCRIPT
A
C
Cp
Cp
1d
rchives of Cardiovascular Disease (2009) 102, 105—110
LINICAL RESEARCH
onotruncal defects associated with anomalousulmonary venous connections
ardiopathies intéressant la région conotroncale et retour veineuxulmonaire anormal associés
Fanny Bajollea,b, Stéphane Zaffranb,c, Jean Losayd,Phalla Oua, Margaret Buckinghamb, Damien Bonneta,∗
a Service de cardiologie pédiatrique, centre de référence malformations cardiaquescongénitales complexes M3C, hôpital Necker-Enfants—Malades, AP—HP,149, rue de Sèvres, 75015 Paris, Franceb Département de biologie du développement, Institut Pasteur, Paris, Francec Institut de biologie du développement de Marseille-Luminy, Marseille, Franced Centre chirurgical Marie-Lannelongue, Le Plessis-Robinson, France
Received 27 March 2008; received in revised form 25 April 2008; accepted 29 April 2008Available online 25 February 2009
KEYWORDSConotruncal defects;Anomalouspulmonary venousconnection;Second heart field
SummaryBackground. — Conotruncal defects constitute one of the major categories of congenital heartdisease. Our understanding of how these defects develop has been derived from knowledge ofthe role of neural crest cells in heart development. However, recent studies have revealed arole for the myocardium in the formation of both the arterial and venous poles of the heart.Aim. — To identify congenital heart defects that associate anomalies of the arterial and venouspoles.Methods. — From a database spanning 27 years, we identified those patients with conotruncaldefects associated with an anomalous pulmonary venous connection (APVC; total or partial).Patients with atria isomerism or atrioventricular septal defects were excluded. Patient fileswere reviewed for clinical presentation, family history, diagnostic and surgical procedures, andoutcome.Results. — We identified 23 patients with conotruncal defects and APVC. Conotruncal defects
were as follows : common arterial trunk, n = 7; tetralogy of Fallot, n = 5; discordant ventriculoar-terial connections, n = 4; interrupted aortic arch, n = 2; subarterial ventricular septal defect,n = 2; double outlet right ventricle, n = 2; and right pulmonary artery from ascending aorta,n = 1. Nine patients had total APVC and 14 patients had partial APVC. Recurrence of the cardiacdefects in siblings was observed in three families.∗ Corresponding author. Fax : +33 1 44 49 43 40.E-mail address: [email protected] (D. Bonnet).
875-2136/$ — see front matter © 2008 Elsevier Masson SAS. All rights reserved.oi:10.1016/j.acvd.2008.04.010

106
MOTS CLÉSCardiopathiesconotroncales ;Retour veineuxpulmonaire anormal ;Second champcardiaque
Conclusion. — Notre étude suggère que les cardiopathies congénitales complexes associant desanomalies des pôles artériel et veineux puissent avoir une origine embryologique commune
onna. All
AAACIPPTT
B
Cdgtanncdd2lctdg
tchropgccoptabo
M
WfmwiP
dérivée du myocarde embry© 2008 Elsevier Masson SAS
bbreviationso aortaPVC anomalous pulmonary venous connectionAT common arterial trunk
V innominate veinA pulmonary trunk (artery)APVC partial anomalous pulmonary venous connectionAPVC total anomalous pulmonary venous connectionbx1 T-box transcription factor 1
ackground
ongenital heart disease affecting the arterial pole is oftenescribed as a conotruncal defect [1]. Ablation of premi-ratory neural crest cells from chick embryos has shownhat conotruncal defects (such as tetralogy of Fallot, CATnd double outlet right ventricle) are caused by cardiaceural crest defects [2]. However, abnormal migration ofeural crest cells may not be the sole cause of abnormalonotruncal development. In clinical practice, conotruncalefects are often observed in patients with DiGeorge syn-rome, who have deletions on the long arm of chromosome2 (specifically at region 22q11), which include the Tbx1
ocus [1,3]. Studies indicate that DiGeorge syndrome andonotruncal defects share common embryological perturba-ions, although the resultant anatomical abnormalities areifferent. Tissue-specific ablation of Tbx1 in the pharyn-eal mesoderm named the second heart field [4] was foundtooco
ire.rights reserved.
o cause severe defects in the conotruncal region, identi-al to those seen in DiGeorge syndrome [5]. The secondeart field provides most of the myocytes for the arte-ial pole, and for a portion of the venous pole [6]. Thesebservations suggest that conotruncal defects have multi-le embryological origins — an idea that is supported by theenetic heterogeneity of the malformations [7]. Conotrun-al defects can be associated with a wide variety of otherardiovascular defects [2]. For example, abnormal devel-pment of the conotruncal region is a regular feature inatients with isomerism, univentricular heart, and atrioven-ricular canal defects [8]. Several isolated examples of anssociation between a conotruncal defect and an APVC haveeen described [9—12]. In this study, we report on a seriesf 23 patients displaying this rare association.
ethods
e extracted all patients with conotruncal defects and APVCrom our database, which has had retrospective ascertain-ent from January 2006 to May 1979. We excluded patientsith atria isomerism and atrioventricular septal defects. We
ncluded patients with total or partial APVC (TAPVC andAPVC, respectively). With regard to conotruncal defects,
F. Bajolle et al.
Conclusion. — Our findings suggest that congenital heart defects that associate anomalies ofthe arterial and venous poles may have a common embryology, which results from a myocardialdefect.© 2008 Elsevier Masson SAS. All rights reserved.
RésuméIntroduction. — Les cardiopathies conotroncales constituent un des principaux groupes de car-diopathies congénitales. Leur origine embryologique a longtemps été attribuée à des anomaliesdes cellules de la crête neurale. Plus récemment, le rôle du myocarde dans le développementdes pôles artériel et veineux du cœur a été mis en exergue.But. — Identifier les patients ayant une cardiopathie congénitale affectant les pôles artérielset veineux simultanément.Méthodes. — Les patients ayant une cardiopathie conotroncale et une anomalie du retourveineux pulmonaire (RVPA) ont été identifiés à partir d’une base de données couvrant une péri-ode de 27 ans. Les patients ayant un isomérisme ou un canal atrioventriculaire ont été exclus. Laprésentation clinique, l’histoire familiale, les méthodes diagnostiques et thérapeutiques ainsique le devenir des patients ont été analysés.Résultats. — Vingt-trois patients ayant une cardiopathie conotroncale et un RVPA ont été iden-tifiés. Les cardiopathies conotroncales étaient les suivantes : tronc artériel commun, n = 7 ;tétralogie de Fallot, n = 5 ; discordance ventriculo-artérielle, n = 4 ; interruption de l’arche,n = 2 ; communication interventriculaire conoventriculaire, n = 2 ; ventricule droit à doubleissue, n = 2 ; et artère pulmonaire droite aberrante, n = 1. Neuf patients avaient un RVPA totalet 14 un RVPA partiel. Une récurrence de cardiopathies congénitales était notée dans troisfamilles.
he following abnormalities were considered: CAT, tetral-gy of Fallot, tetralogy of Fallot with pulmonary atresiar absent pulmonary valve, discordant ventriculoarterialonnections, subarterial ventricular septal defect, doubleutlet right ventricle, right pulmonary artery from ascending
Conotruncal defects associated with anomalous pulmonary venous connections 107
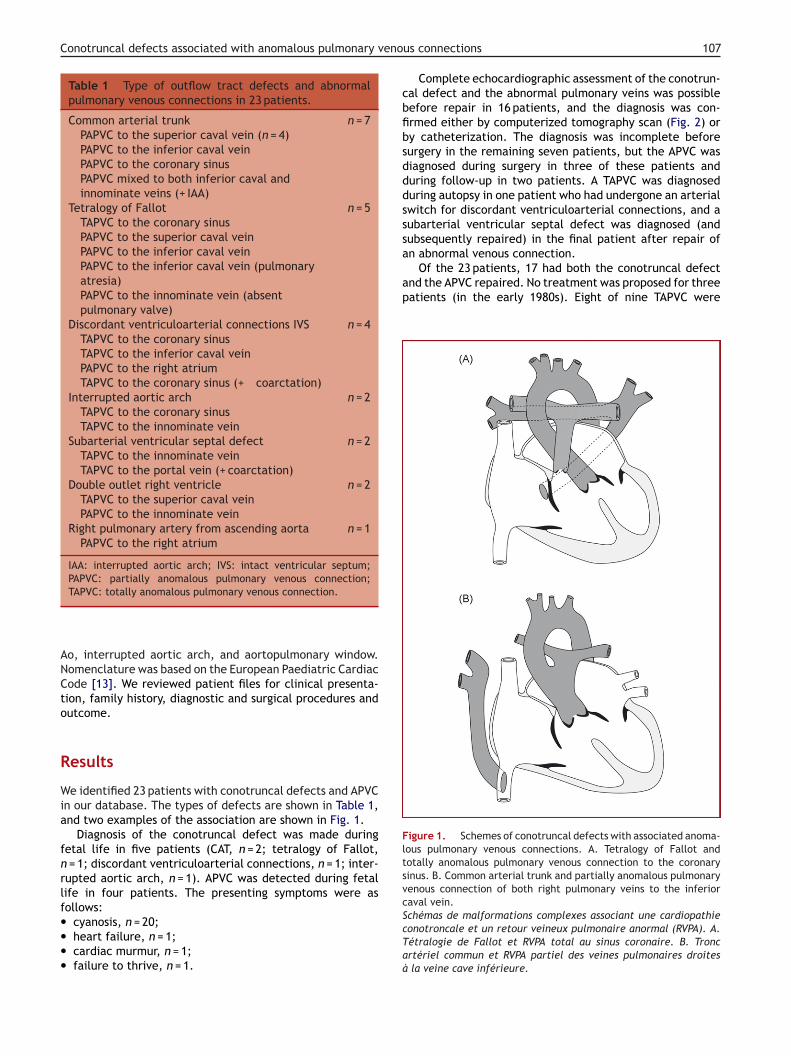
Table 1 Type of outflow tract defects and abnormalpulmonary venous connections in 23 patients.
Common arterial trunk n = 7PAPVC to the superior caval vein (n = 4)PAPVC to the inferior caval veinPAPVC to the coronary sinusPAPVC mixed to both inferior caval andinnominate veins (+ IAA)
Tetralogy of Fallot n = 5TAPVC to the coronary sinusPAPVC to the superior caval veinPAPVC to the inferior caval veinPAPVC to the inferior caval vein (pulmonaryatresia)PAPVC to the innominate vein (absentpulmonary valve)
Discordant ventriculoarterial connections IVS n = 4TAPVC to the coronary sinusTAPVC to the inferior caval veinPAPVC to the right atriumTAPVC to the coronary sinus (+ coarctation)
Interrupted aortic arch n = 2TAPVC to the coronary sinusTAPVC to the innominate vein
Subarterial ventricular septal defect n = 2TAPVC to the innominate veinTAPVC to the portal vein (+ coarctation)
Double outlet right ventricle n = 2TAPVC to the superior caval veinPAPVC to the innominate vein
Right pulmonary artery from ascending aorta n = 1PAPVC to the right atrium
IAA: interrupted aortic arch; IVS: intact ventricular septum;PAPVC: partially anomalous pulmonary venous connection;
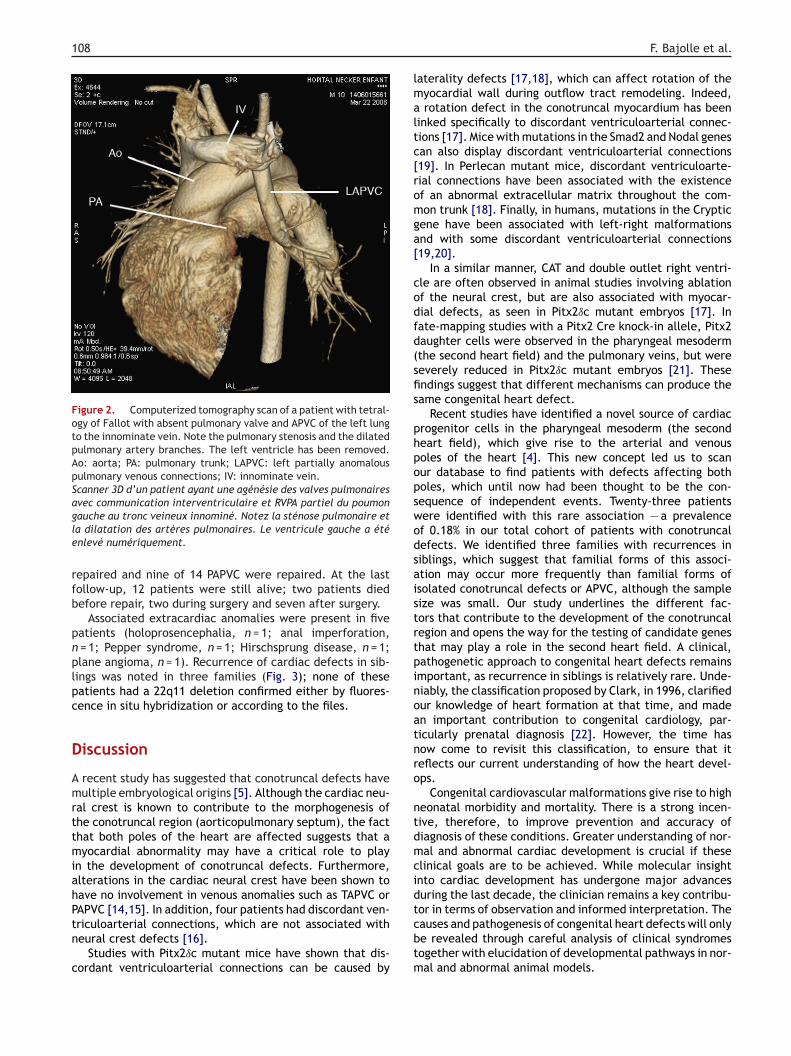
Complete echocardiographic assessment of the conotrun-cal defect and the abnormal pulmonary veins was possiblebefore repair in 16 patients, and the diagnosis was con-firmed either by computerized tomography scan (Fig. 2) orby catheterization. The diagnosis was incomplete beforesurgery in the remaining seven patients, but the APVC wasdiagnosed during surgery in three of these patients andduring follow-up in two patients. A TAPVC was diagnosedduring autopsy in one patient who had undergone an arterialswitch for discordant ventriculoarterial connections, and asubarterial ventricular septal defect was diagnosed (andsubsequently repaired) in the final patient after repair ofan abnormal venous connection.
Of the 23 patients, 17 had both the conotruncal defectand the APVC repaired. No treatment was proposed for threepatients (in the early 1980s). Eight of nine TAPVC were
Figure 1. Schemes of conotruncal defects with associated anoma-lous pulmonary venous connections. A. Tetralogy of Fallot andtotally anomalous pulmonary venous connection to the coronarysinus. B. Common arterial trunk and partially anomalous pulmonaryvenous connection of both right pulmonary veins to the inferiorcaval vein.
TAPVC: totally anomalous pulmonary venous connection.
Ao, interrupted aortic arch, and aortopulmonary window.Nomenclature was based on the European Paediatric CardiacCode [13]. We reviewed patient files for clinical presenta-tion, family history, diagnostic and surgical procedures andoutcome.
Results
We identified 23 patients with conotruncal defects and APVCin our database. The types of defects are shown in Table 1,and two examples of the association are shown in Fig. 1.
Diagnosis of the conotruncal defect was made duringfetal life in five patients (CAT, n = 2; tetralogy of Fallot,n = 1; discordant ventriculoarterial connections, n = 1; inter-rupted aortic arch, n = 1). APVC was detected during fetallife in four patients. The presenting symptoms were asfollows:
• cyanosis, n = 20;• heart failure, n = 1;• cardiac murmur, n = 1;• failure to thrive, n = 1.Schémas de malformations complexes associant une cardiopathieconotroncale et un retour veineux pulmonaire anormal (RVPA). A.Tétralogie de Fallot et RVPA total au sinus coronaire. B. Troncartériel commun et RVPA partiel des veines pulmonaires droitesà la veine cave inférieure.
108
Figure 2. Computerized tomography scan of a patient with tetral-ogy of Fallot with absent pulmonary valve and APVC of the left lungto the innominate vein. Note the pulmonary stenosis and the dilatedpulmonary artery branches. The left ventricle has been removed.Ao: aorta; PA: pulmonary trunk; LAPVC: left partially anomalouspulmonary venous connections; IV: innominate vein.Scanner 3D d’un patient ayant une agénésie des valves pulmonairesavec communication interventriculaire et RVPA partiel du poumongle
rfb
pnplpc
D
AmrttmiahPtn
c
lmaltc[romga[
codfd(sfis
phpopswodsaistrtpinoatnro
ntdmcid
auche au tronc veineux innominé. Notez la sténose pulmonaire eta dilatation des artères pulmonaires. Le ventricule gauche a éténlevé numériquement.
epaired and nine of 14 PAPVC were repaired. At the lastollow-up, 12 patients were still alive; two patients diedefore repair, two during surgery and seven after surgery.
Associated extracardiac anomalies were present in fiveatients (holoprosencephalia, n = 1; anal imperforation,= 1; Pepper syndrome, n = 1; Hirschsprung disease, n = 1;lane angioma, n = 1). Recurrence of cardiac defects in sib-ings was noted in three families (Fig. 3); none of theseatients had a 22q11 deletion confirmed either by fluores-ence in situ hybridization or according to the files.
iscussion
recent study has suggested that conotruncal defects haveultiple embryological origins [5]. Although the cardiac neu-
al crest is known to contribute to the morphogenesis ofhe conotruncal region (aorticopulmonary septum), the facthat both poles of the heart are affected suggests that ayocardial abnormality may have a critical role to play
n the development of conotruncal defects. Furthermore,lterations in the cardiac neural crest have been shown toave no involvement in venous anomalies such as TAPVC or
APVC [14,15]. In addition, four patients had discordant ven-riculoarterial connections, which are not associated witheural crest defects [16].Studies with Pitx2ıc mutant mice have shown that dis-ordant ventriculoarterial connections can be caused by
tcbtm
F. Bajolle et al.
aterality defects [17,18], which can affect rotation of theyocardial wall during outflow tract remodeling. Indeed,rotation defect in the conotruncal myocardium has been
inked specifically to discordant ventriculoarterial connec-ions [17]. Mice with mutations in the Smad2 and Nodal genesan also display discordant ventriculoarterial connections19]. In Perlecan mutant mice, discordant ventriculoarte-ial connections have been associated with the existencef an abnormal extracellular matrix throughout the com-on trunk [18]. Finally, in humans, mutations in the Cryptic
ene have been associated with left-right malformationsnd with some discordant ventriculoarterial connections19,20].
In a similar manner, CAT and double outlet right ventri-le are often observed in animal studies involving ablationf the neural crest, but are also associated with myocar-ial defects, as seen in Pitx2ıc mutant embryos [17]. Inate-mapping studies with a Pitx2 Cre knock-in allele, Pitx2aughter cells were observed in the pharyngeal mesodermthe second heart field) and the pulmonary veins, but wereeverely reduced in Pitx2ıc mutant embryos [21]. Thesendings suggest that different mechanisms can produce theame congenital heart defect.
Recent studies have identified a novel source of cardiacrogenitor cells in the pharyngeal mesoderm (the secondeart field), which give rise to the arterial and venousoles of the heart [4]. This new concept led us to scanur database to find patients with defects affecting botholes, which until now had been thought to be the con-equence of independent events. Twenty-three patientsere identified with this rare association — a prevalencef 0.18% in our total cohort of patients with conotruncalefects. We identified three families with recurrences iniblings, which suggest that familial forms of this associ-tion may occur more frequently than familial forms ofsolated conotruncal defects or APVC, although the sampleize was small. Our study underlines the different fac-ors that contribute to the development of the conotruncalegion and opens the way for the testing of candidate geneshat may play a role in the second heart field. A clinical,athogenetic approach to congenital heart defects remainsmportant, as recurrence in siblings is relatively rare. Unde-iably, the classification proposed by Clark, in 1996, clarifiedur knowledge of heart formation at that time, and maden important contribution to congenital cardiology, par-icularly prenatal diagnosis [22]. However, the time hasow come to revisit this classification, to ensure that iteflects our current understanding of how the heart devel-ps.
Congenital cardiovascular malformations give rise to higheonatal morbidity and mortality. There is a strong incen-ive, therefore, to improve prevention and accuracy ofiagnosis of these conditions. Greater understanding of nor-al and abnormal cardiac development is crucial if these
linical goals are to be achieved. While molecular insightnto cardiac development has undergone major advancesuring the last decade, the clinician remains a key contribu-
or in terms of observation and informed interpretation. Theauses and pathogenesis of congenital heart defects will onlye revealed through careful analysis of clinical syndromesogether with elucidation of developmental pathways in nor-al and abnormal animal models.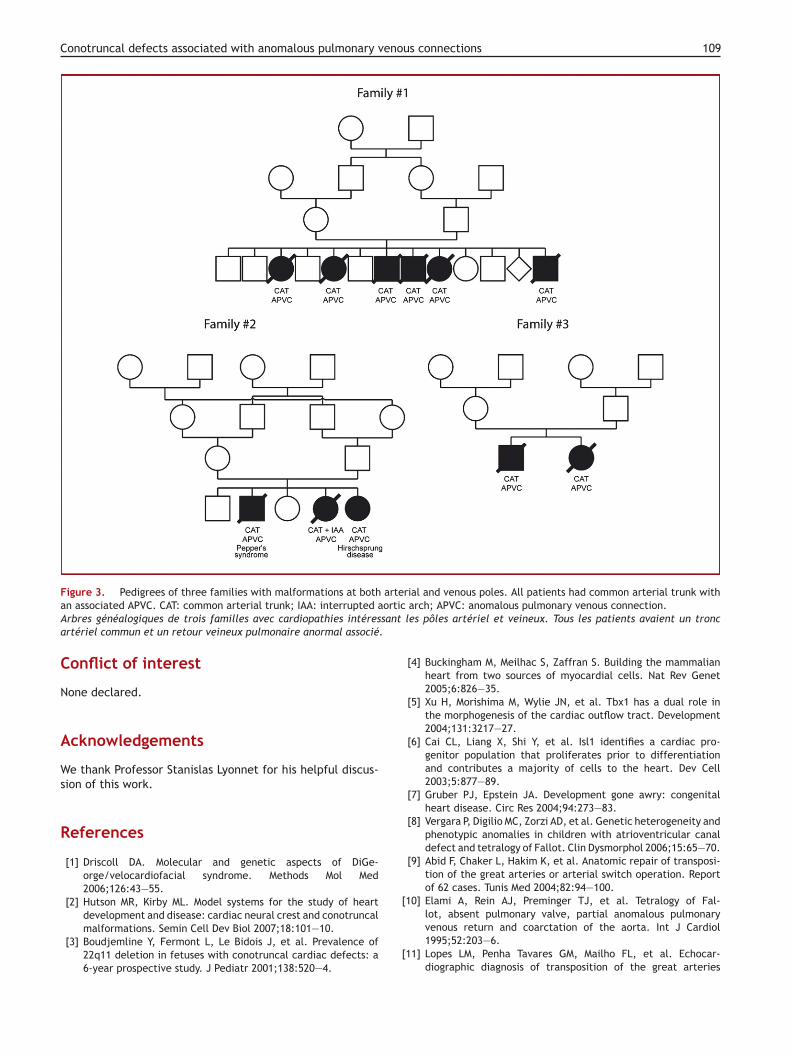
Conotruncal defects associated with anomalous pulmonary venous connections 109
arteorticsant.
[
Figure 3. Pedigrees of three families with malformations at bothan associated APVC. CAT: common arterial trunk; IAA: interrupted aArbres généalogiques de trois familles avec cardiopathies intéresartériel commun et un retour veineux pulmonaire anormal associé
Conflict of interest
None declared.
Acknowledgements
We thank Professor Stanislas Lyonnet for his helpful discus-sion of this work.
References
[1] Driscoll DA. Molecular and genetic aspects of DiGe-orge/velocardiofacial syndrome. Methods Mol Med2006;126:43—55.
[2] Hutson MR, Kirby ML. Model systems for the study of heart
development and disease: cardiac neural crest and conotruncalmalformations. Semin Cell Dev Biol 2007;18:101—10.[3] Boudjemline Y, Fermont L, Le Bidois J, et al. Prevalence of22q11 deletion in fetuses with conotruncal cardiac defects: a6-year prospective study. J Pediatr 2001;138:520—4.
[
rial and venous poles. All patients had common arterial trunk witharch; APVC: anomalous pulmonary venous connection.
les pôles artériel et veineux. Tous les patients avaient un tronc
[4] Buckingham M, Meilhac S, Zaffran S. Building the mammalianheart from two sources of myocardial cells. Nat Rev Genet2005;6:826—35.
[5] Xu H, Morishima M, Wylie JN, et al. Tbx1 has a dual role inthe morphogenesis of the cardiac outflow tract. Development2004;131:3217—27.
[6] Cai CL, Liang X, Shi Y, et al. Isl1 identifies a cardiac pro-genitor population that proliferates prior to differentiationand contributes a majority of cells to the heart. Dev Cell2003;5:877—89.
[7] Gruber PJ, Epstein JA. Development gone awry: congenitalheart disease. Circ Res 2004;94:273—83.
[8] Vergara P, Digilio MC, Zorzi AD, et al. Genetic heterogeneity andphenotypic anomalies in children with atrioventricular canaldefect and tetralogy of Fallot. Clin Dysmorphol 2006;15:65—70.
[9] Abid F, Chaker L, Hakim K, et al. Anatomic repair of transposi-tion of the great arteries or arterial switch operation. Reportof 62 cases. Tunis Med 2004;82:94—100.
10] Elami A, Rein AJ, Preminger TJ, et al. Tetralogy of Fal-
lot, absent pulmonary valve, partial anomalous pulmonaryvenous return and coarctation of the aorta. Int J Cardiol1995;52:203—6.11] Lopes LM, Penha Tavares GM, Mailho FL, et al. Echocar-diographic diagnosis of transposition of the great arteries

1
[
[
[
[
[
[
[
[
[
[
10
associated with anomalous pulmonary venous connection. ArqBras Cardiol 2001;77:63—8.
12] Nouet N, Doz F, Dessemme P, et al. Pepper syndrome, truncusarteriosus communis and abnormal pulmonary venous return:an unusual association. Eur J Pediatr 2002;161:114—5.
13] The European Paediatric Cardiac Code: the first revision. Car-diol Young 2002;12:1—211.
14] Anderson RH, Brown NA, Moorman AF. Development and struc-tures of the venous pole of the heart. Dev Dyn 2006;235:2—9.
15] Phillips 3rd MT, Waldo K, Kirby ML. Neural crest ablation doesnot alter pulmonary vein development in the chick embryo.
Anat Rec 1989;223:292—8.16] Kirby ML. Embryogenesis of transposition of the great arteries:a lesson from the heart. Circ Res 2002;91:87—9.
17] Bajolle F, Zaffran S, Kelly RG, et al. Rotation of themyocardial wall of the outflow tract is implicated in the
[
F. Bajolle et al.
normal positioning of the great arteries. Circ Res 2006;98:421—8.
18] Costell M, Carmona R, Gustafsson E, et al. Hyperplasticconotruncal endocardial cushions and transposition of greatarteries in perlecan-null mice. Circ Res 2002;91:158—64.
19] Gaio U, Schweickert A, Fischer A, et al. A role of the crypticgene in the correct establishment of the left-right axis. CurrBiol 1999;9:1339—42.
20] Goldmuntz E, Bamford R, Karkera JD, et al. CFC1 mutations inpatients with transposition of the great arteries and double-outlet right ventricle. Am J Hum Genet 2002;70:776—80.
21] Liu C, Liu W, Palie J, et al. Pitx2c patterns anterior
myocardium and aortic arch vessels and is required for localcell movement into atrioventricular cushions. Development2002;129:5081—91.22] Clark EB. Pathogenetic mechanisms of congenital cardiovascu-lar malformations revisited. Semin Perinatol 1996;20:465—72.