clinical practice guideline forhealth professsionals · pdf filelegal note regarding ... jaime...
TRANSCRIPT

Libert y Orden
Clinical Practice Guideline Diagnosis and treatment of adult patients with severe Traumatic Brain InjuryGeneral System of Social Security in Health–Colombia
Guide for Health Professionals 2014-Guide No. GPC-2014-30
Foundation for Medical and Technical Research and Education in Emergencies and Disasters (MEDITECH)

© Ministry of Health and Social Protection - Colciencias
Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain InjuryGuide No. GPC-2014-30
ISBN: 978-958-8903-24-8Bogotá. ColombiaNovember 2014
Legal noteRegarding intellectual property, refer to the provisions of paragraph 12 of announcement 563 of 2012 and the twelfth clause - intellectual property “In the event that intellectual property rights are generated on the results that are obtained or may be obtained in the development of this announcement and the resulting fi nancing contract, these will belong to COLCIENCIAS and the Ministry of Health and Social Protection” and in accordance with the clauses of the contracts signed to this eff ect.
Financing: National Program for Science, Technology and Innovation in Health. Administrative Department of Science, Technology and Innovation in Health (COLCIENCIAS), announcement 563/2012, Contract 455 (2012), Project code 360056335262. The points of view of the fi nancial entity have had no infl uence on the content of the guideline.
This document should be referenced as: Colombia. Ministry of Health and Social Protection, Colciencias, MEDITECH Foundation. Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury. GSSSH – 2014. Guide No. 30 CPG-TBI. Bogotá, 2014.

ALEJANDRO GAVIRIA URIBEMinister of Health and Social Protection
FERNANDO RUIZ GÓMEZDeputy Minister of Health and Service Provision
NORMAN JULIO MUÑOZ MUÑOZDeputy Minister of Social Protection
GERARDO BURGOS BERNAL
General Secretary
JOSÉ LUIS ORTIZ HOYOSHead of the Quality Offi ce
Liberta y Orden

YANETH GIHA TOVAR General Director
ALICIA RÍOS HURTADO Deputy Director in Charge (e)
LILIANA MARÍA ZAPATA BUSTAMANTE General Secretary
ALICIA RIOS HURTADO Director of Knowledge Networks
LUCY GABRIELA DELGADO MURCIADirector for the Promotion of Research
JAIME EDUARDO CASTELLANOS PARRA Manager of the National Program of Science, Technology and
Innovation in Health
HILDA GRACIELA PACHECO GAITÁN Technical monitoring and auditing
DAVID ARTURO RIBÓN OROZCO Technical monitoring and auditing
HÉCTOR EDUARDO CASTRO JARAMILLO Executive Director
AURELIO MEJÍA MEJÍA Deputy Director for the Evaluation of Technology in Health
IVÁN DARÍO FLÓREZ GÓMEZDeputy Director for the Production of Clinical Practice Guidelines
JAVIER HUMBERTO GUZMANSub-Direction of Implementation and Dissemination
DIANA ESPERANZA RIVERA RODRÍGUEZ Deputy Director for Participation and Deliberation
SANDRA LUCÍA BERNALSub-Direction of Dissemination and Communication

TECHNICAL SUPPORT TEAM
INDIRA TATIANA CAICEDO REVELOQuality Offi ce
ABEL ERNESTO GONZALEZ VELEZQuality Offi ce
TECHNICAL SUPPORT TEAM
LORENA ANDREA CAÑÓN BETANCOURTEpidemiology
JAIME HERNAN RODRIGUEZ MORENO Research and Development
Libert y Orden

ESPERANZA ESCOBAR DONCEL Legal representative
ANDRES MARIANO RUBIANO ESCOBAR Medical and Research Coordinator
NAYA CAROLINA SOLANO RAMOSAdministrative Assistant
PAOLA ANDREA TEJADAJOSE DOMINGO ALARCONANGELA MAGNOLIA RIOS
JUAN CARLOS PUYANACentral Research Committee
JOSE DANIEL CHARRY CUELLAR JORGE HERNAN MONTENEGRO MUÑOZ
JOSE FERNANDO FERNANDEZ MARIA ALEJANDRA RIVAS
Technical Support Team

DEVELOPER GROUP OF THE GUIDELINE
Methodological group
Andrés Mariano Rubiano EscobarPrincipal Investigator– Thematic Leader and Coordinator of the Guide
Paola Andrea Tejada MoralesMethodological Leader and Project Manager for the Guide
José Domingo AlarcónMethodological Coordinator of the Guide
Ángela Magnolia Ríos Gallardo Coordinator of Patient Participation Component of the Guide
José Mauricio Ávila Rodríguez Coordinator of the Economic Evaluation Section
Pablo AlonsoMethodological Expert
Andrea Juliana SanabriaMethodological Expert
Gustavo PetroniMethodological Expert
Silvia Lujan Methodological Expert
Nancy Carney Methodological Expert
Juan Carlos Puyana Methodological and Thematic Expert
P. David AdelsonMethodological and Thematic Expert
M. Ross BullockMethodological and Thematic Expert
External thematic experts and representatives of scienti ic societies
Oswaldo Borráez Thematic Expert and Representative of the Colombian Society of Surgery and the Colombian Association of Trauma
Luis Eduardo JaramilloThematic Expert and Representative of the Colombian Society of Psychiatry

Nur Constanza VergaraThematic Expert and Representative of the Colombian Society of Physical Medicine and Rehabilitation
Milton MolanoThematic Expert
Oscar EcheverryThematic Expert, Representative of the Colombian Association of Prehospital Care
Ángela María OrtizThematic Expert, Representative of the Colombian Association of Infant Neurology
Norberto Navarrete AldanaThematic Expert, Representative of the Colombian Association of Emergency Medicine Specialists
Alexander NossaThematic Expert
José Nel Carreño Thematic Expert, Representative of the Colombian Neurosurgery Association
Juan Diego CiroThematic Expert, Representative of the Colombian Anesthesia and Reanimation Association
Jorge Humberto Mejía-MantillaThematic Expert, Representative of the Colombian Association Critical Medicine and Intensive Care
Luis Rafael Moscote SalazarThematic Expert, Representative of the Colombian Neurosurgery Association
Sandra Lucia Lozano ÁlvarezThematic Expert, Representative of Intensive Care Residents
Claudia Marcela Restrepo LugoThematic Expert, Representative of Neurosurgery Residents
Orlando PerdomoThematic Expert, Representative of the Colombian Medical College
Claudia Rodríguez TriviñoThematic Expert
Alejandro GómezThematic Expert
Jorge OteroThematic Expert
Editorial design and layoutDistribuna Publishers

Foundation for Medical and Technical Research and Education in Emergencies and Disasters10
Content
8 Developer Group for the Guide
20 Introduction
24 Background
25 Rationale
25 Con lict of Interest Declaration
26 Financing of the CPG
26 Editorial Independence
26 Scope of the topic of the CPG
27 Objectives of the CPG
27 Speci ic Objectives
28 Users
28 Population to whom the CPG is directed
28 Healthcare workers to whom the CPG is directed
28 Clinical aspects covered by the Guide
28 Clinical aspects not covered by the Guide
29 Updating the CPG
29 References
Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 11
31 Summary of recommendations
42 Elaboration of questions
43 De inition and classi ication of outcomes
45 Construction of the set of evidence or de novo development
46 Inclusion process for articles
46 Quality assessment of studies for inclusion
47 Process of information extraction and evidence synthesis
47 Final assessment of the body of evidence
48 Formulation of recommendations
49 Patient participation
52 Questions, evidence and recommendations
52 Question 1a
52 Recommendation
53 Introduction
53 Summary of the evidence
55 From evidence to recommendation
55 Structural Requirements
55 Considerations on bene its and risks
55 Considerations on values and preferences of patients
55 Implications on resources
55 References
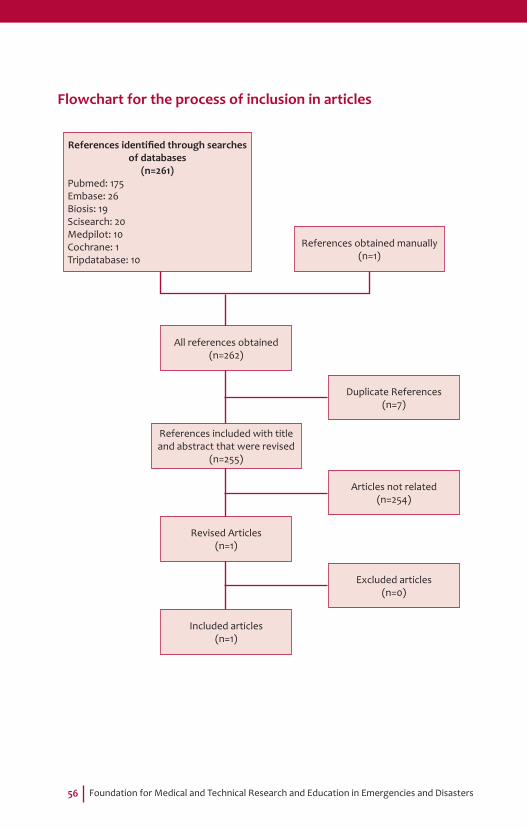
56 Flowchart for the process of inclusion in articles
57 Algorithm 1

Foundation for Medical and Technical Research and Education in Emergencies and Disasters12
58 Question 1b
58 Recommendation
59 Introduction
59 Summary of the evidence
61 From evidence to recommendation
61 Structural Requirements
62 Considerations on bene its and risks
62 Considerations on values and preferences of patients
62 Implications on resources
62 References
63 Flowchart for the process of inclusion in articles
64 Algorithm 1
65 Question 2
65 Recommendation
65 Introduction
66 Summary of the evidence
68 From evidence to recommendation
68 Structural Requirements
69 Considerations on bene its and risks
69 Considerations on values and preferences of patients
69 Implications on resources
70 References
71 Flowchart for the process of inclusion in articles
Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 13
72 Question 3
72 Recommendation
73 Introduction
74 Summary of the evidence
75 From evidence to recommendation
76 Structural Requirements
76 Considerations on bene its and risks
77 Considerations on values and preferences of patients
77 Implications on resources
77 References
78 Flowchart for the process of inclusion in articles
79 Algorithm 2
80 Question 4
80 Recommendation
80 Introduction
81 Summary of the evidence
82 From evidence to recommendation
82 Structural Requirements
82 Considerations on bene its and risks
82 Considerations on values and preferences of patients
83 Implications on resources
83 References
84 Flowchart for the process of inclusion in articles
Foundation for Medical and Technical Research and Education in Emergencies and Disasters14
85 Algorithm 3
86 Question 5
86 Recommendation
87 Introduction
87 Summary of the evidence
88 From evidence to recommendation
88 Structural Requirements
88 Considerations on bene its and risks
88 Considerations on values and preferences of patients
88 Implications on resources
89 References
89 Flowchart for the process of inclusion in articles
90 Question 6a
90 Recommendation
90 Introduction
90 Summary of the evidence
92 From evidence to recommendation
92 Structural Requirements
92 Considerations on bene its and risks
92 Considerations on values and preferences of patients
92 Implications on resources
93 Flowchart for the process of inclusion in articles
94 Algorithm 4

Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 15
95 Question 6b
95 Recommendation
95 Introduction
95 Summary of the evidence
97 From evidence to recommendation
97 Structural Requirements
97 Considerations on bene its and risks
97 Considerations on values and preferences of patients
97 Implications on resources
98 Flowchart for the process of inclusion in articles
99 Algorithm 4
100 Question 6c
100 Recommendation
100 Introduction
100 Summary of the evidence
101 From evidence to recommendation
101 Structural Requirements
101 Considerations on bene its and risks
102 Considerations on values and preferences of patients
102 Implications on resources
102 References
103 Flowchart for the process of inclusion in articles
104 Algorithm 4
Foundation for Medical and Technical Research and Education in Emergencies and Disasters16
105 Question 7
105 Recommendation
106 Introduction
106 Summary of the evidence
107 From evidence to recommendation
108 Structural Requirements
108 Considerations on bene its and risks
108 Considerations on values and preferences of patients
108 Implications on resources
108 References
109 Flowchart for the process of inclusion in articles
110 Algorithm 5
111 Question 8
111 Recommendation
111 Introduction
112 Summary of the evidence
112 From evidence to recommendation
113 Structural Requirements
113 Considerations on bene its and risks
113 Considerations on values and preferences of patients
113 Implications on resources
113 References
114 Flowchart for the process of inclusion in articles

Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 17
115 Algorithm 6
116 Question 9
116 Recommendation
116 Introduction
117 Summary of the evidence
118 From evidence to recommendation
118 Structural Requirements
118 Considerations on bene its and risks
119 Considerations on values and preferences of patients
119 Implications on resources
119 References
121 Flowchart for the process of inclusion in articles
122 Algorithm 7
123 Question 10
123 Recommendation
123 Introduction
124 Summary of the evidence
127 From evidence to recommendation
127 Structural Requirements
127 Considerations on bene its and risks
127 Considerations on values and preferences of patients
128 Implications on resources
128 References

Foundation for Medical and Technical Research and Education in Emergencies and Disasters18
129 Flowchart for the process of inclusion in articles
130 Algorithm 8
131 Economic Question
131 Objective
131 Methods
132 Results
132 Conclusions
132 Revision of economic evaluations present in the literature
136 Abbreviations and Glossary
144 Annexes
144 Annex 1
145 Annex 2
168 Annex 3
178 Annex 4
Ministry of Health and Social Protection - Colciencias 19
Tables
21 T 1. The Glasgow Coma Scale
23 T 2. Abbreviated injury scale (AIS) for head injuries, closed and penetrating
44 T 3. Glasgow Outcome Scale
44 T 4. Extended Glasgow Outcome Scale (GOS-E)
48 T 5. De inition of evidence levels
50 T 6. Report format of the participation of patients in the development of the CPG
54T 7. Summary of the results of the Pandor (2012) me-ta-analysis; indings of each clinical variable for the diagno-sis of intracranial injury in adults with mild TBI (sensitivity, speci icity, LR+ y LR- grouped)
60 T 8. Canadian CT Head Rule
61 T 9. Sensitivity and speci icity of the decision rules to identify injuries that require neurosurgical intervention
91 T 10. Group that made up the expert consensus for question 6a
96 T 11. Group that made up the expert consensus for question 6b
126 T 12. Group that made up the expert consensus for question 8
Foundation for Medical and Technical Research and Education in Emergencies and Disasters20
Introduction
Traumatic brain injury (TBI) is de ined as an condition characteri-zed by a brain disorder secondary to a traumatic injury produced
by the liberation of an external force, be it in the form of mechanical, chemical, thermal, electrical, radiant energy, or any combination the-reof. This transmission of energy to the cranial cavity causes structu-ral damage to its content, including brain tissue and the blood vessels that feed this tissue (Rubiano 2009). The TBI can be classi ied in many ways, including whether it is penetrating or closed and depending on the anatomical area that is affected. According to the consensus of gui-delines for the uni ication of variables in studies of neurotrauma, the Glasgow Coma Scale is one of the most appropriate scales for associa-ting the clinical presentation with the outcomes, taking into account that this classi ication was one of the irst that allowed the association of indings with clinical evaluation, imaging and post mortem macros-copic pathology (Saatman 2008). This is the most widely used classi i-cation in national and international environments, and selects patients according to the degree of severity. This scale has been developed ba-sed on the clinical evaluation of 3 parameters: eye opening, verbal res-ponse and motor response (see table 1).
Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 21
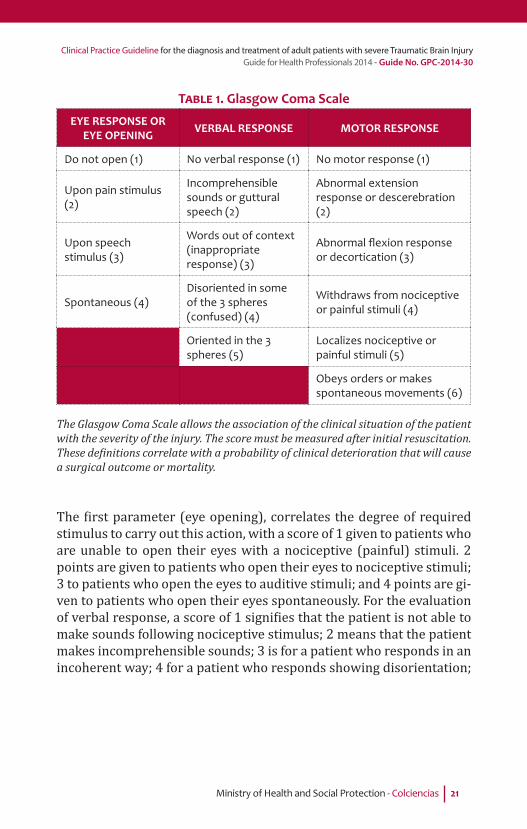
TABLE 1. Glasgow Coma Scale
EYE RESPONSE OR EYE OPENING VERBAL RESPONSE MOTOR RESPONSE
Do not open (1) No verbal response (1) No motor response (1)
Upon pain stimulus (2)
Incomprehensible sounds or guttural speech (2)
Abnormal extension response or descerebration (2)
Upon speech stimulus (3)
Words out of context (inappropriate response) (3)
Abnormal fl exion response or decortication (3)
Spontaneous (4)Disoriented in some of the 3 spheres (confused) (4)
Withdraws from nociceptive or painful stimuli (4)
Oriented in the 3 spheres (5)
Localizes nociceptive or painful stimuli (5)
Obeys orders or makes spontaneous movements (6)
The Glasgow Coma Scale allows the association of the clinical situation of the patient with the severity of the injury. The score must be measured after initial resuscitation. These de initions correlate with a probability of clinical deterioration that will cause a surgical outcome or mortality.
The irst parameter (eye opening), correlates the degree of required stimulus to carry out this action, with a score of 1 given to patients who are unable to open their eyes with a nociceptive (painful) stimuli. 2 points are given to patients who open their eyes to nociceptive stimuli; 3 to patients who open the eyes to auditive stimuli; and 4 points are gi-ven to patients who open their eyes spontaneously. For the evaluation of verbal response, a score of 1 signi ies that the patient is not able to make sounds following nociceptive stimulus; 2 means that the patient makes incomprehensible sounds; 3 is for a patient who responds in an incoherent way; 4 for a patient who responds showing disorientation;

Foundation for Medical and Technical Research and Education in Emergencies and Disasters22
and 5 indicates that the patient responds appropriately to questions from the examiner. The motor activity is the last parameter (which is considered one of the most important as it is not affected by the use of sedative or toxic medications). A score of 1 is assigned to patients that do not make any sort of movement following nociceptive stimuli; 2 is given to patients that respond with an abnormal extension move-ment (decerebration); 3 points are for patients who respond with an abnormal lexion movement (decortication); A score of 4 is given to patients who make withdrawal movements to stimuli; patients who can localize the stimulus receive a score of 5; and 6 for patients who make movements that are spontaneous or when induced to obey a ver-bal order. Therefore, adding up the scores for the 3 parameters, we can create categories:
• Mild TBI (Glasgow 13-15) • Moderate TBI (Glasgow 9-12) • Severe TBI (Glasgow 3-8)
These categories have been correlated to mortality, disability and the requirement for surgical intervention, all of which are greater in the severe TBI group.
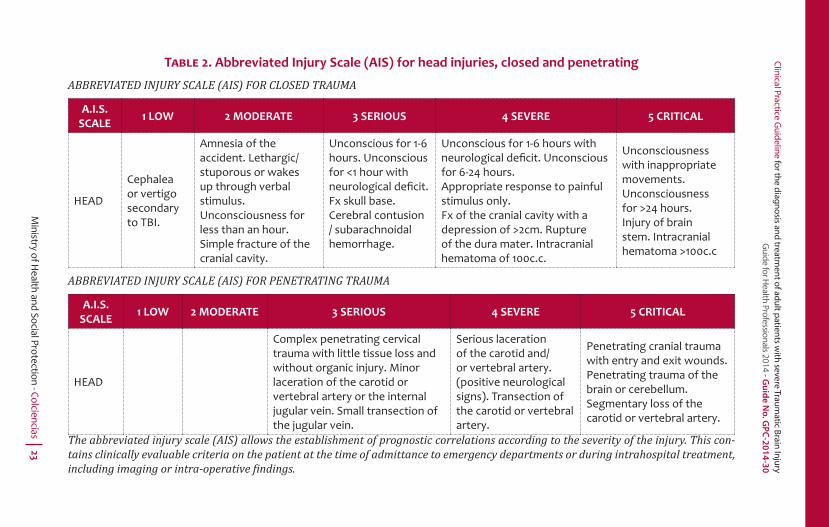
Additionally, a second severity classi ication method has been sugges-ted especi ically to compare the medical records of patients treated in specialized centers. Comparing these medical records allows us to establish differences in patients with multiple types of injury and to establish methods and mathematical models in order to determine survival rates. The most used score is the Abbreviated Injury Scale. This system has a range of 1 to 5, where 1 is for super icial and less complex injuries and 5 is for the most severe injuries (see table 2). It is considered that all head injuries with scores greater than 2 are severe and are associated with greater mortality and disability.
Clinical Practice Guideline for the diagnosis and treatm
ent of adult patients with severe Traum
atic Brain Injury G
uide for Health Professionals 2014 - G
uid
e N
o. G
PC
-20
14
-30
Ministry of H
ealth and Social Protection - Colciencias 23
TABLE 2. Abbreviated Injury Scale (AIS) for head injuries, closed and penetrating
ABBREVIATED INJURY SCALE (AIS) FOR CLOSED TRAUMA
A.I.S. SCALE 1 LOW 2 MODERATE 3 SERIOUS 4 SEVERE 5 CRITICAL
HEAD
Cephalea or vertigo secondary to TBI.
Amnesia of the accident. Lethargic/stuporous or wakes up through verbal stimulus.Unconsciousness for less than an hour.Simple fracture of the cranial cavity.
Unconscious for 1-6 hours. Unconscious for <1 hour with neurological defi cit. Fx skull base. Cerebral contusion / subarachnoidal hemorrhage.
Unconscious for 1-6 hours with neurological defi cit. Unconscious for 6-24 hours.Appropriate response to painful stimulus only.Fx of the cranial cavity with a depression of >2cm. Rupture of the dura mater. Intracranial hematoma of 100c.c.
Unconsciousness with inappropriate movements.Unconsciousness for >24 hours. Injury of brain stem. Intracranial hematoma >100c.c
ABBREVIATED INJURY SCALE (AIS) FOR PENETRATING TRAUMA
A.I.S. SCALE 1 LOW 2 MODERATE 3 SERIOUS 4 SEVERE 5 CRITICAL
HEAD
Complex penetrating cervical trauma with little tissue loss and without organic injury. Minor laceration of the carotid or vertebral artery or the internal jugular vein. Small transection of the jugular vein.
Serious laceration of the carotid and/or vertebral artery. (positive neurological signs). Transection of the carotid or vertebral artery.
Penetrating cranial trauma with entry and exit wounds.Penetrating trauma of the brain or cerebellum.Segmentary loss of the carotid or vertebral artery.
The abbreviated injury scale (AIS) allows the establishment of prognostic correlations according to the severity of the injury. This con-tains clinically evaluable criteria on the patient at the time of admittance to emergency departments or during intrahospital treatment, including imaging or intra-operative indings.

Foundation for Medical and Technical Research and Education in Emergencies and Disasters24
From the epidemiological point of view, TBI is one of the most impor-tant medical-surgical conditions at a global level. In the world, there are incidence estimates of near to 200 cases for every 100,000 inha-bitants, but the limited availability of epidemiological databases, es-pecially in countries with medium and low incomes (in which around 90% of the population with TBI are concentrated), means that these estimates are not very precise. It is clear, according to recent studies, such as the global burden of disease study performed by the WHO, that in areas such as Latin America, the impact of this condition is relatively high, with trauma in general being the most common cause of death and disability in the population between 10 and 24 years (Norton 2012). In Colombia, the data available, until 2008, allows the identi i-cation of trauma as the principal cause of death and disability in 12 to 45 year olds (WHO 2010). According to data from the National Institu-te of Legal Medicine and Forensic Sciences, for the year 2012, multiple trauma (including TBI) corresponded to 65.5% of the fatal injuries in traf ic accidents, followed by isolated TBI with 27.2% (Moreno 2012). Due to the above, it is clear that TBI as a condition is a public health problem and that it is vital to develop clinical practice guidelines in order to reduce variability in the treatment, oriented to the perfor-ming of an integral care of patients with the best scienti ic evidence and strengthened public policy towards a high quality health care.
Background
The Colombian Ministry of Health has made an important effort in the development of clinical practice and care guidelines since the 1990s. During that irst exercise, in a joint project with ASCOFAME, the Mi-nistry of Health and the Social Security Institute, the topic of TBI was identi ied as a priority, due to its high incidence in the population of Colombia. During the development of the second edition of the natio-nal emergency care guidelines (MPS 2004) and the irst edition of the prehospital medical care guidelines (MPS 2005), TBI was also consi-dered a priority topic, and speci ic chapters of reviews of the mana-gement of this condition were included. These care guides currently have revised and updated chapters on the topic in the latest edition of each one (MPS 2009) (MPS 2012). In the new phase of the creation of clinical practice guidelines, TBI continues to be a priority topic, recog-nizing its impact in the scenario of Colombian public health and due to

Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 25
this issue, it was made part of funding announcement 563-12, product of a joint effort between the Ministry of Health and Colciencias.
Rationale
The availability of a CPG for the diagnosis and treatment of severe TBI in adults implies a reduction in the variability of treatment and a high quality approach to diagnosis and treatment, based on the best available scienti ic evidence. Although there are different types of guidelines around the world, the methodological quality of their pro-duction has not been the most appropriate according to international standards (Alarcón 2013). Additionally, the great majority of the avai-lable guidelines are developed for contexts that are different to most of the countries in Latin America, were not all the technology availa-ble for advanced monitoring of patients with severe TBI is available all around. Adherence to the use of recommendations of guidelines with high methodological quality for the treatment of TBI has been linked to improvements in survival rates and cost reduction within health-care systems (Fakhry 2004) (Faul 2007) (Gerber 2013). Some of the most critical interventions are those that present greater variability in different scenarios, including the prehospital care phase and intrahos-pital treatment in terms of emergencies, surgery and intensive care. Therefore, the production of a CPG for the diagnosis and treatment of patients with severe TBI in Colombia is considered necessary, because in the country, this condition add an important burden of disease in the health system and additionally the care is heterogeneous due to the inexistence of this type of tools. Currently there is evidence availa-ble that allows the creation of recommendations based on a systematic and technically aseptic process. A preliminary review of the literature suggests that interventions such as early intubation in the prehospital phase, early surgical intervention, the use of speci ic neuromonitoring protocols at intensive care and the use of medications that can reduce the impact of secondary injuries, have been associated with a reduc-tion in mortality and disability.
Confl ict of interest declaration
The activities that may constitute con licts of interest are those circum-stances in which professional judgment on a primary interest, such as

Foundation for Medical and Technical Research and Education in Emergencies and Disasters26
the safety of patients or validity of research can be affected by another secondary interest, which could be a inancial bene it, prestige, perso-nal or professional promotion. An interest is considered speci ic if it is directly related to technologies or products being evaluated in a CPG. An unspeci ic interest is one that is not related directly to technolo-gies or products being evaluated in the CPG, but which may be related indirectly due to interactions with the manufacturer, marketer, users, etc., of these products. Con lict of interest declarations of each one of the members of the developer group can be found in annex 1 of the complete version of this guide.
Financing of the CPG
The development of this guide was funded by the Ministry of Health and Social Protection and the Administrative Department of Science, Technology and Innovation (COLCIENCIAS) through contract No. 455 of 2012 signed with the Foundation for Medical and Technical Educa-tion and Research in Emergencies and Disasters (MEDITECH), an ins-titution that was selected through the funding announcement 563 of 2012 for the developing of Clinical Practice Guidelines for the Diagnosis, Treatment and Rehabilitation of Patients with Traumatic Brain Injury.
Editorial Independence
The scienti ic work of research and production of the recommen-dations included in this document was made independently by the guide’s developer group. Funding institutions monitored the produc-tion of this document in order to guarantee the unconditional freedom of the contents of the guide.
Scope of the topic of the CPG
This CPG for the diagnosis and treatment of patients is designed for the adult population with severe Traumatic Brain Injury (TBI) in Co-lombia, considering as adults all persons over 15 years old, according to international standards for research into severe TBI; The recom-mendations are also directed at prehospital healthcare personnel, ge-neral physicians, paramedics, emergency surgeons, neurologists, neu-rosurgeons, intensive care doctors, patients and caregivers of patients.
Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 27
Objectives of the CPG
The objective of the CPG for the diagnosis and treatment of adult pa-tients with severe TBI is to reduce the heterogeneity in the diagno-sis and treatment of this kind of patients in Colombia, with the aim of improving the quality of care, reducing disabilities and increasing the survival rate for these patients.
Specifi c objectives
• To reduce the heterogeneity of prehospital and intrahospital care for severe TBI in Colombia in order to encourage evidence-based practice.
• To establish criteria for referral and transfer of adult patients with TBI in a trauma care system.
• To promote ef icient use of scans of the skull to focus the diagno-sis and treatment of TBI in adults.
• To establish criteria for the appropriate use of intravenous luids and management of the airway at prehospital and intrahospital levels in adult patients with severe TBI, reducing the hetero-geneity in treatment and with the aim of improving functional outcome.
• To establish criteria associated with the most appropriate time to carry out surgical procedures in adult patients with severe TBI, with the aim of improving the functional outcome of these patients.
• To establish criteria for the use of sedatives in the treatment of adult patients with severe TBI in intensive care units, reducing heterogeneity in their use.
• To decrease heterogeneity in the treatment of thrombopro-phylaxis, monitoring of intracranial pressure and treatment with selective hypothermia in adult patients with severe TBI treated in intensive care units, with the aim of improving functional outcome in these patients.
• To de ine the cost-effectiveness of the treatment with prehospi-tal intubation of adult patients with severe TBI compared with intra-hospital intubation.

Foundation for Medical and Technical Research and Education in Emergencies and Disasters28
Users
Prehospital healthcare personnel, nurses, general practitioners, spe-cialists in emergency medicine, emergency surgeons, neurologists, neurosurgeons, intensive care doctors, patients, caregivers, family members and decision makers.
Population to whom the CPG is directed
The people to whom the CPG for the diagnosis and treatment of severe TBI is directed are persons over 15 years old who have a traumatic brain injury.
Healthcare workers to whom the CPG is directed
Prehospital health care personnel, including nurses, technicians or te-chnologists in prehospital care and general physicians who work in this environment. Nurses and general practitioners from low-complexity le-vel institutions; In medium-complexity level institutions, nurses, general practitioners and medical specialists who assist in emergency services; In high-complexity level institutions, nurses, general practitioners and specialists in emergency medicine, emergency surgeons, neurologists, neurosurgeons and intensive care doctors who provide specialized ser-vices in emergency departments, surgery and intensive care.
Clinical aspects covered by the guide
The Guide refers to the diagnosis and interventions used to treat pa-tients over 15 years old with severe TBI. It addresses the following aspects of clinical treatment:
a) Aspect 1. Prehospital Treatmentb) Aspect 2. Emergency Treatmentc) Aspect 3. Treatment in Intensive Care Units
Clinical aspects not covered by the guide
The guide does not cover the following aspects of clinical treatment:a) Aspects of prevention and surveillance of injuries
Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 29
b) Aspects of rehabilitationc) Aspects of diagnosis and treatment of patients under 15 years oldd) Aspects related to alternative therapiese) Aspects of therapies in the experimentation phase
Updating the CPG
The recommendations of this guideline must be updated in the next three (3) years or earlier if there is new evidence that modify the re-commendations or any of the speci ic questions. The updating pro-cess must follow the previously established methodology and must be coordinated together with the Ministry of Health and the IETS.
References
1. Rubiano AM, Yepes R. Neurotrauma y Neurointensivismo. 1ª Ed. Editorial Distribuna. 2009.
2. Saatman KE, Duhaime AC, Bullock R, Maas AI, Valadka A, Manley GT; Workshop Scienti ic Team and Advisory Panel Members.J Neurotrauma. 2008 Jul;25(7):719-38.
3. Norton R, Kobusingye O: Injuries.N Engl J Med 2013; 368:1723-1730.4. World Health Organization. World Health Statistics. Geneva. 2010
(Disponible en:http://www.who.int/gho/publications/world_health_statistics/EN_WHS10_Full.pdf)
5. Ministerio de Protección Social – FEPAFEM. Guías de Atención en Urgencias 2ª Ed. Editorial Kimpres, Bogotá. 2004.
6. Ministerio de Protección Social de Colombia – ACAPH – Instituto de Ciencias de la Salud CES. Guías de Atención Básica Prehospitalaria. 2005.
7. Ministerio de Protección Social – FEPAFEM. Guías para Manejo de Urgencias. 3ª Ed. 2009.
8. Ministerio de Protección Social – Universidad de Antioquia. Guías de Atención Médica Prehospitalaria. 2ª Ed. 2012.
9. Alarcon JD, Rubiano AM, Chirinos MS, Valderrama A, Gich I, Bon ill X, Alonso-Coello P. Clinical practice guidelines for the care of patients with severe traumatic brain injury: a systematic evaluation of their quality.J Trauma Acute Care Surg. 2013;75(2):311-9.
10. Fakhry SM, Trask AL, Waller MA, Watts DD; IRTC Neurotrauma Task Force.Management of brain-injured patients by an evidence-

Foundation for Medical and Technical Research and Education in Emergencies and Disasters30
based medicine protocol improves outcomes and decreases hospital charges.J Trauma. 2004;56(3):492-9.
11. Faul M, Wald MM, Rutland-Brown W, Sullivent EE, Sattin RW.Using a cost-bene it analysis to estimate outcomes of a clinical treatment guideline: testing theBrain Trauma Foundation guidelines for the treatment of severe traumatic brain injury.J Trauma. 2007;63(6):1271-8.
12. Gerber LM, Chiu YL, Carney N, Härtl R, Ghajar J. Marked reduction in mortality in patients with severe traumatic brain injury. J Neurosurg. 2013;119(6):1583-90.
13. Moreno SL: Muertes y lesiones por accidentes detransporte, Colombia, 2012. Forensis (Datos o iciales sobre la violencia en Colombia en el 2012), 2012; pp: 351-402. Disponible en: http://www.medicinalegal.gov.co/images/stories/root/FORENSIS/2012/transporte%20forensis%202012.pdf)

Ministry of Health and Social Protection - Colciencias 31
Summary of recommendations
Question 1a
Which patients with TBI should have a computerized tomography (CT) of the head?
Recommendation
• It is recommended that every adult patient with TBI and who meet one or more of the following criteria must be have a CT scan: - Skull fracture (clinical or radiological) including signs of
basilar skull fracture (periorbital ecchymosis, retroauricu-lar ecchymosis, otorrhea, rhinorrhea).
- Post-traumatic seizure - Focal neurological de icit - Persistent vomiting (greater than or equal to two episodes) - Drop in the Glasgow Coma Scale of at least 1 point - Previous craniotomy - When the patient is a pedestrian who was hit by a car. - History of coagulopathy or pharmacologic anticoagulation - Patients suspected to be intoxicated. - Fall from height greater than 1.5 m - Retrograde Amnesia> 30 minutes and/or anterograde - Age greater than or equal to 60 years. - Severe headache - Blurred vision or diplopia
Foundation for Medical and Technical Research and Education in Emergencies and Disasters32
Question 1b
Which patients with TBI should be transferred from low-level of care hospitals to centers with neurosurgery and neuroimaging services?
Recommendation
• It is recommended that patients with moderate to severe TBI (Glasgow 3-12) should be transferred immediately to high-level of care hospitals with access to neuroimaging and neu-rosurgery.
• It is recommended that patients with mild TBI (Glasgow 13-15) who present one or more of the following criteria be re-ferred for evaluation at an institution that has access to neu-roimaging and neurosurgery: - Glasgow coma score under 15 up to 2 hours after injury - Severe headache - More than 2 episodes of vomiting - Skull fracture, including depressed fractures or clinical sig-
ns of fracture of the skull base (raccoon eyes, retro auricu-lar ecchymosis, otorrhea or rhinorrhea)
- Age greater than or equal to 60 years old - Blurred vision or diplopia - Post-traumatic seizure - Focal neurological de icit - Previous craniotomy. - Fall of over 1.5 meters. - Retrograde amnesia more than 30 minutes and/or antero-
grade amnesia. - Suspected intoxication with alcohol and/ or psychoactive
substances.• It is recommended that patients with mild TBI and who are
in active treatment with anticoagulants, have active coagula-pathies, or are pregnant should be transferred to centers with neurosurgery and neuroimaging services.
Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 33
Question 2
In adult patients with severe TBI, does the treatment in an organized trauma care center, compared to treatment in a general non-speciali-zed center reduce mortality?
Recommendation
• It is suggested that adult patients with severe TBI be trans-ferred directly to a leading high-complexity institution with emphasis on trauma care.
Weak recommendation in favor of intervention, low quality evidence.
Question 3
In adult patients with severe TBI, does prehospital orotracheal in-tubation, compared with orotracheal intubation in emergency de-partments, reduce neurological disability or mortality, evaluated at 6 months post-injury?
Recommendation
• It is recommended that adult patients with severe TBI need to be intubated in the trachea in a prehospital setting, using a ra-pid sequence intubation, which includes inductor medication and neuromuscular paralysis medication.
Strong recommendation in favor of intervention, moderate quality of evidence.
• The recommended dosages to be used are the following: - Fentanyl Dose: 1 μg/Kg - Midazolam Dose: 0.1mg/Kg - Succinylcholine Dose: 1 mg/Kg
Strong recommendation in favor of intervention, moderate quality of evidence.

Foundation for Medical and Technical Research and Education in Emergencies and Disasters34
• The use of half the dose of inductor medications suggested above is recommended if the patient has systolic blood pres-sure <100mmHg, or is >60 years old.
Strong recommendation, moderate quality of evidence
• Orotracheal intubation in a prehospital setting should be ca-rried out by skilled medical personnel or prehospital techno-logists (who have an adequate level of training). Technologists must carry out the procedure under direct or indirect super-vision of a doctor with experience in handling prehospital and in-hospital emergencies.
Weak recommendation in favor of intervention, low quality of evidence.
• We suggest that adequate training as part of intubation train-ing programs should be considered to be at least 16 hours of theoretical-practical training in rapid sequence intubation, in-cluding at least 4 hours of theory, 8 hours of experience in in-tubation in operating theaters under the supervision of an an-esthesiologist and at least 4 hours of evaluation in simulators.
Weak recommendation, moderate quality of evidence.
• It is recommended that if the attempt to intubate is not suc-cessful, patients should continue to be ventilated with a bag valve mask system, together with an oropharyngeal airway, until they return to spontaneous respiration. If this method is insuf icient to achieve a pulse oximetry >90%, we recommend the use of a laryngeal mask, as a rescue device.
Strong recommendation in favor of intervention, moderate quality of evidence.
• It is suggested that in the case that the patient is being moved by a basic ambulance, and there is no technologist or medic on board, ventilation should be carried out with a bag valve mask system, together with an oropharyngeal airway in order to achieve a pulse oximetry of >90%.
Good clinical practice

Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 35
Question 4
In adult patients with severe TBI, does the use of 7.5% hypertonic so-lutions for resuscitation in prehospital setting, compared with the use of isotonic resuscitation solutions, reduce neurological disability or mortality, evaluated at 6 months post-injury?
Recommendation
• It is recommended that adult patients with severe blunt TBI without hypotension can be treated at a prehospital level with 250ml of saline solution at 0.9%
Strong recommendation in favor of intervention, moderate quality of evidence
• It is recommended that patients with penetrating TBI or with hypotension can be treated at a prehospital level with 250ml of saline solution at 0.9%.
Good clinical practice.
Question 5
In adult patients with severe TBI and intracranial hypertension, does the use of hypertonic saline at 7.5%, compared with mannitol, as a hy-perosmolar initial therapy reduce mortality at discharge?
Recommendation
• It is suggested that adult patients with severe TBI and refrac-tory intracranial hypertension (ICP> 25 mmHg for more than 5 minutes, measured with an intracranial pressure measuring device) be treated with a bolus of 2 ml/kg of 7.5% hypertonic saline solution or mannitol at 20%.
Weak recommendation in favor of intervention, moderate quality of evidence.

Foundation for Medical and Technical Research and Education in Emergencies and Disasters36
• If the irst dose is not effective in reducing ICP, a second bolus of 7.5% hypertonic saline solution or mannitol at 20% may be administered 10 minutes after inishing the irst bolus.
Weak recommendation in favor of the intervention, moderate quality of evidence.
• It is considered that adult patients with severe TBI and non-refractory intracranial hypertension (20-25mmHg, measured using an intracranial pressure device) requiring hyperosmolar therapy should be treated with a bolus of 2 cc/kg of 7.5% hy-pertonic saline solution or mannitol at 20%.
Good clinical practice
• It is considered that for the preparation of the 7.5% hyperto-nic saline solution, a mixture of (40%) 0.9% saline solution plus (60%) ampoules of sodium chloride should be used. To prepare 250cc of the solution, 100cc of normal saline so-lution and 15 ampoules of sodium chloride (20meq/10ml) would be mixed.
Good clinical practice
• It is considered that the use of mannitol at 20% should be performed only in normotensive patients with systolic blood pressure greater than 90 mmHg.
Good clinical practice
Question 6a
In adult patients with severe TBI and acute subdural hematoma with surgical indication, does early drainage surgery (within 4 hours), com-pared with late surgery (after 4 hours), reduce mortality at discharge?

Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 37
Recommendation
• It is recommended that surgical treatment be performed in the irst 4 hours post-trauma in patients with severe head trauma
with acute subdural hematoma with surgical indication. Recommendation by strong consensus in favor of the intervention.
Question 6b
In adult patients with severe TBI, and an epidural hematoma with sur-gical indication, does early drainage surgery (within 4 hours), compa-red with late surgery (after 4 hours), reduce mortality at discharge?
Recommendation
• It is recommended that patients with severe TBI and an epidu-ral hematoma with surgical indication for drainage be taken to surgery immediately.
Recommendation by strong consensus in favor of the intervention.
Question 6c
In adult patients with severe TBI and surgical indication for cerebral edema, does early decompression craniectomy (within 24 hours), compared with late craniectomy (after 24 hours), reduce mortality at discharge?
Recommendation
• It is suggested that patients with severe TBI and surgical indi-cation for cerebral edema be taken to surgery within 24 hours.
Weak recommendation in favor of the intervention, low qua-lity of evidence.
Foundation for Medical and Technical Research and Education in Emergencies and Disasters38
Question 7
In adult patients with severe TBI being treated in an ICU, does seda-tion with propofol, compared to sedation using Midazolam, reduce neurological disability or mortality, assessed at 3 months post-injury?
Recommendation
• It is suggested that adult patients with severe TBI be sedated during their stay in the ICU using midazolam. Doses of 0.1-0.3 mg/kg/h are suggested.1
Weak recommendation in favor of the intervention, moderate quality of evidence
• As a second choice after midazolam, propofol 1% can be used at a dose of 1.5 to 5 mg/kg/h1.
Weak recommendation in favor of the intervention, moderate quality of evidence
• It is suggested that a triglyceride measurement be perfor-med on patients sedated with propofol 1% within the irst 24 hours. If the initial sample of triglycerides is lower than 350 mg/dl, periodic checks should be performed every 72 hours. If the value is greater than 350 mg/dl, repeat the sample within 24 hours. If the second sample is also above 350 mg/dl, treatment should be discontinued immediately. Patients should be closely monitored for the possible occurrence of propofol infusion syndrome (hyperkalemia, metabolic aci-dosis, cardiac arrhythmia, cardiovascular collapse and multi-organ failure).
Weak recommendation in favor of the intervention, moderate quality of evidence
• Patients should be closely monitored for the possible occu-rrence of propofol infusion syndrome (hyperkalemia, meta-bolic acidosis, cardiac arrhythmia, cardiovascular collapse and multi-organ failure).
Good clinical practice.
1The use of the Richmond Agitation-Sedation Scale (RASS) for the evaluation and control of sedation is suggested because it is the most widely used scale.
Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 39
Question 8
In adult patients with severe TBI treated in an ICU, does thrombo-pro-phylaxis with low molecular weight heparin (LMWH), compared with thrombo-prophylaxis with unfractionated heparin, reduce the presen-ce of thrombotic events and mortality at discharge?
Recommendation
• It is recommended that adult patients with severe TBI receive antithrombotic prophylaxis with low molecular weight hepa-rin (enoxaparin). The suggested dose is 30mg/SC/day.
Weak recommendation for intervention, low quality of evidence.
• The recommendation is to start antithrombotic therapy as soon as possible; as long as the patient is not receiving trans-fusions, is stable in the neurological examination (no reduc-tion in GCS) and that the CT scan shows evidence that the bleeding is controlled (no expansion in the area of bleeding).
Weak recommendation for intervention, low quality of evidence
• Start pneumatic compression stockings in patients with seve-re TBI immediately after admission to the ICU.
Good clinical practice.
Question 9
In adult patients with severe TBI being treated in an ICU, does guided therapy with monitoring of intracranial pressure (ICP), compared with treatment without ICP monitoring, reduce mortality at discharge?
Foundation for Medical and Technical Research and Education in Emergencies and Disasters40
Recommendation
• It is suggested that adult patients with severe TBI need to be monitored with intracranial pressure measurement devices when they meet the following criteria: Glasgow Coma Scale greater than or equal to 3 and less than or equal to 8 after re-suscitation and an abnormal CT (hematoma, contussion, ede-ma, herniation or compression of basal cisterns).
Weak recommendation in favor of intervention, very low qua-lity of evidence.
• It is suggested that treatment of intracranial hypertension be initiated when the value measured in the patient is greater than 20mmHg in a single measurement.
Weak recommendation in favor of intervention, Very low qua-lity of evidence.
Question 10
In adult patients with severe TBI being treated in an ICU, does selec-tive head cooling, compared to normothermia, decrease neurological disability and mortality at discharge?
Recommendation
• It is suggested that adult patients with severe TBI have selec-tively and non-invasively cooled their skulls using a recircu-lating-water system or tapes chilled to 4 degrees centigrade, ensuring that intracerebral temperature can be measured.
Weak recommendation in favor of the intervention, moderate quality of evidence.

Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 41
• It is suggested that patients should be maintained at a body temperature above 36 degrees and below 38 degrees, measu-red rectally, in order to avoid systemic hypothermia.
Weak recommendation in favor of the intervention, moderate quality of evidence.
• It is not recommended to perform the intervention in institu-tions that do not have a recirculating-water system or tapes chilled to 4 degrees centigrade.
Recommendation by strong consensus in favor of the intervention.

Foundation for Medical and Technical Research and Education in Emergencies and Disasters42
Elaboration of questions
The development process began with a selection of questions raised on international guidelines that discuss the same condition and
have the same scope, in order to create a starting point for discussion with different actors in the system and discuss priorities adjusted to the Colombian context. The working group made a careful review of the questions included in the most internationally recognized guideli-nes and made a list of about 34 options of questions on critical issues involving aspects of diagnosis, treatment and rehabilitation of adult patients with severe TBI. These questions took into account that the Colombian guideline would be implemented in an environment with different resources from those in the analyzed literature, since all these came from countries with greater resources in their health sys-tems, especially in such aspects as available technology for advanced monitoring in intensive care units. The aspects related to emergency care system were also taken into account, especially in relation to the care within organized trauma systems. Three surveys aimed at gene-ral practitioners, emergency physicians, neurosurgeons and intensi-vists were performed. From these surveys, the topics, which had most variability in the answers and to which most emphasis was given by respondents, were:
• Prehospital and Emergency Care: - Prehospital intubation - Resuscitation using luid at prehospital level - Use of hyperosmolar solutions in emergency departments - Suggested time for surgical interventions - Sedation in the emergency department
• Surgery and Intensive Care - Times and indications for neurotrauma surgery - Hyperosmolar solutions in the ICU
Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 43
- Use of glycemia in the ICU - Managment of hyperthermia in the ICU - Systemic and selective hypothermia in the ICU - Thromboprophylaxis in the ICU - ICP monitoring
With the questions from the guides, in addition to the questions prio-ritized by surveys, an initial core set of questions was developed; this core set was discussed with different thematic panels including mee-tings with members of the Colombian Association of Prehospital Care, the Colombian Association of Specialists in Emergency Medicine, the Colombian Association of Neurosurgery and the Colombian Associa-tion of Critical Care and Intensive Care Medicine. In two of these mee-tings, surveys were conducted with speci ic methods for prioritizing questions in populations of 30 and 20 participants respectively. Fo-llowing these discussions and in parallel with the work done with the Ministry of Health and the Institute for the Assessment of Technology in Health (IETS) to focus the scope and objectives, the process reached a inal number of ten questions, in order to work, using the PICO model, whilst adding an economic question. These questions where focused on aspects of prehospital treatment (intubation and use of resuscita-tion luid in prehospital situations) emergency care (use of hyperos-molar solutions), surgery (optimal timing for surgery in subdural & epidural hematoma and for cerebral edema) and intensive care (se-dation, thromboprophylaxis, monitoring of intracranial pressure and selective hypothermia). By request of the Ministry of Health and Social Protection, two open (non PICO) questions related to the organization of the health system were included (indications for performing a brain scan on patients with TBI, and reference criteria for these same pa-tients from centers with lower levels of specialization to those with specialized level of care).
Defi nition and classifi cation of outcomes
Given that an extensive literature review of guidelines and articles rela-ted to the diagnosis and treatment of adult patients with severe TBI was carried out, the most important outcomes were established considering the methodology suggested by GRADE, including their suggested classi-ication in critical, important but not critical, and low importance. After
Foundation for Medical and Technical Research and Education in Emergencies and Disasters44
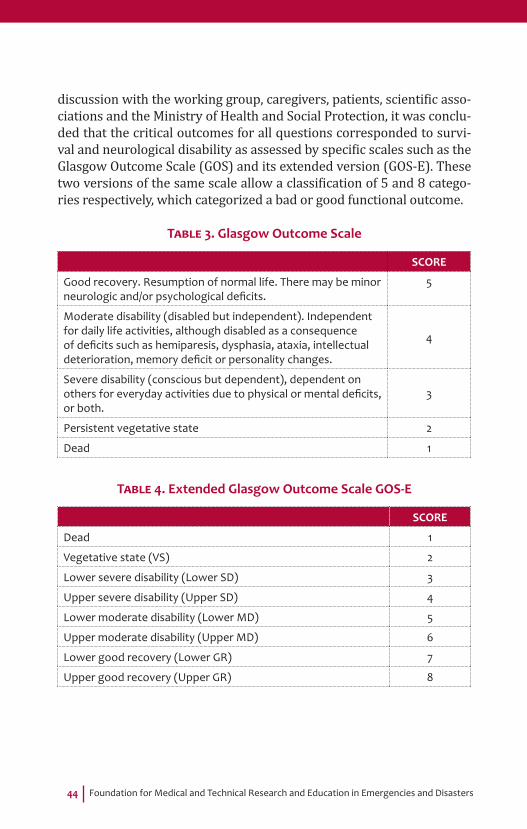
discussion with the working group, caregivers, patients, scienti ic asso-ciations and the Ministry of Health and Social Protection, it was conclu-ded that the critical outcomes for all questions corresponded to survi-val and neurological disability as assessed by speci ic scales such as the Glasgow Outcome Scale (GOS) and its extended version (GOS-E). These two versions of the same scale allow a classi ication of 5 and 8 catego-ries respectively, which categorized a bad or good functional outcome.
TABLE 3. Glasgow Outcome Scale
SCORE
Good recovery. Resumption of normal life. There may be minor neurologic and/or psychological defi cits.
5
Moderate disability (disabled but independent). Independent for daily life activities, although disabled as a consequence of defi cits such as hemiparesis, dysphasia, ataxia, intellectual deterioration, memory defi cit or personality changes.
4
Severe disability (conscious but dependent), dependent on others for everyday activities due to physical or mental defi cits, or both.
3
Persistent vegetative state 2
Dead 1
TABLE 4. Extended Glasgow Outcome Scale GOS-E
SCORE
Dead 1
Vegetative state (VS) 2
Lower severe disability (Lower SD) 3
Upper severe disability (Upper SD) 4
Lower moderate disability (Lower MD) 5
Upper moderate disability (Upper MD) 6
Lower good recovery (Lower GR) 7
Upper good recovery (Upper GR) 8
Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 45
Other critical outcomes for decision making (failed intubation, serum concentrations of triglycerides, deep vein thrombosis and pulmonary embolism) and important, but not critical outcomes for decision ma-king (success rate of intubation at the irst attempt, systemic compli-cations in hospitals, progression of neurological damage) were also considered. Due to the above, and thinking that severe TBI is a con-dition with high rates of mortality and neurologic disability, critical outcomes (mortality/survival and neurological disability), regardless of intermediate outcomes, were prioritized, considering also that any of the interventions that improve survival and neurological disabilities were the most important (especially due to the importance expressed by patients and caregivers regarding the negative results in their qua-lity of life, including the associated disability that may occur as result of severe TBI).
Construction of the set of evidence or de novo development
It was decided to conduct a de novo development taking into account the mechanism suggested by the Methodological Guide for the El-laboration of Clinical Practice Guidelines with Economic Evaluation in the Colombian General Social Security System in Health. As the scope and objectives (adult patients with severe TBI) were focused, searches were aimed at speci ic PICO questions in this population. The two open questions (indications for performing a brain scan in patients with TBI and criteria for referral of these same patients, from less specialized levels to more specialized centers of care) were an-swered through speci ic searches that covered adult patients with mild to moderate trauma. The search strategy included international data-bases in English and Spanish, gray literature searches and discussions with experts in order to search for additional sources of scienti ic asso-ciations and summaries of academic events specialized in the subject. This literature search included studies from 1 January 2000 to July 7 of 2013. Once the search syntax was designed, this was sent to the Iberoamerican Cochrane Centre for review, where suggestions were made to adjust them. The databases searched were PUBMED, EMBASE, COCHRANE LIBRARY, Tripdatabase, and DIMDI (MedPilot, SCISEARCH and BIOSIS). Other searches included, Google Scholar, unindexed Latin American biomedical journals and pages of national and international

Foundation for Medical and Technical Research and Education in Emergencies and Disasters46
scienti ic associations in the area. General search criteria for inclusion considered: patients older than 15 years with severe TBI, scoring less than 9 on the Glasgow Coma Scale (GCS) or with an Injury Severity Score (AIS) for the head higher than 2. Articles that included patients under 16 years old and patients with mild to moderate trauma (with the exception the criterion of severity in question 1) were excluded. The ilters used were the following: Article Types: Clinical Trial, Com-parative Study, Controlled Clinical Trial, Evaluation Studies, Guideline, Meta-Analysis, Multicenter Study, Practice Guideline, Randomized Controlled Trial, Review, Systematic Reviews, Technical Report, Vali-dation Studies. Publication dates: 01/01/2000 to 07/07/2013. Spe-cies: Humans. Languages: English, Spanish. Sex: Female, Male. Journal categories: Core clinical journals and MEDLINE.
Inclusion process for articles
Articles were included if they had recommendations for clinical practi-ce in the treatment of severe TBI according to the selected PICO ques-tions. Articles that did not consider the speci ied population were ex-cluded, as were articles addressing other issues, editorials, letters to editors, non-systematic reviews, studies being developed but without published results, case reports and reviews of articles. If multiple ver-sions of the same article were available, the latest version was selec-ted. Once the criteria for inclusion and exclusion of studies for each question were de ined, the evaluators performed a review of titles and abstracts.
Quality assessment of studies for inclusion
For the assessment of the methodological quality of the selected stu-dies, the formats proposed by SIGN (Scottish Intercollegiate Guideli-nes Network) were used. They were translated into Spanish following the Methodological Guideline for the Ellaboration of Clinical Practice Guidelines with Economic Evaluation in the Colombian General Social

Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 47
Security System for Health. Within these formats, checklists were in-cluded for each question, according to the type of study selected (sys-tematic review and meta-analysis, controlled clinical studies, cohort studies, case studies and controls).
Process of information extraction and evidence synthesis
The exercise of evidence extraction was performed with clinical ex-perts from the working group whose topic of expertise matched the speci ic subject. The same exercise was conducted in parallel with methodological group of the working group. In this way, it was pos-sible to double check the extraction process in order to subsequently access the data required for making the tables of evidence.
Final assessment of the body of evidence
The GRADE approach was used to de ine levels of quality of evidence (high, moderate, low and very low). The parameters used after initial evaluation of the body of evidence according to the study design were: risk of bias, inconsistency, direct or indirect evidence, inaccuracy and risk of selective publication of outcomes. The magnitude of the effect, the dose-response relationship and any possible residual confusion and residual bias were also taken into account. Following the GRADE recommendations, randomized trials were considered of high quality while observational studies were considered of low quality. The type of articles found did not allow the realization of meta-analyses for any questions. The ratings of the evidence with their meaning and graphi-cal interpretation are presented in Table 5:

Foundation for Medical and Technical Research and Education in Emergencies and Disasters48
TABLE 5. Defi nition of levels of evidence
LEVEL OF EVIDENCE DEFINITION GRAPHIC
REPRESENTATION
HighSe tiene gran confi anza en que el verdadero efecto se encuentra cerca al estimativo del efecto.
Moderate
There is moderate confi dence in the estimate of the eff ect: it is likely that the true eff ect is close to the estimate of the eff ect, but the possibility exists that it is substantially diff erent.
LowConfi dence in the estimate of the eff ect is limited: the true eff ect may be substantially diff erent from the estimate of the eff ect.
Very Low
One can have very little confi dence in the estimate of the eff ect: it is likely that the true eff ect is substantially diff erent from the estimate of the eff ect.
The inal rating of the body of evidence was made by the metodologi-cal experts of the working group together with the working group of the Iberoamerican Cochrane Center in Spain.
Formulation of recommendations
For the formulation of the recommendations, the GRADE methodolo-gy, which identi ies four determinants for the direction and strength of recommendations, was used. These are:
• Balance between desirable and undesirable results (estimated effects), with consideration of the values and preferences. The smaller the difference is, the less likely it is that a strong recom-mendation will be made.
• Con idence in the magnitude of the estimated effect of the in-tervention on important outcomes. If con idence is low, it is less likely that a strong recommendation will be made.
• Con idence in values, preferences and variability. The lower the con idence or the greater the variability, the less likely it is that a strong recommendation will be given.

Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 49
• Use of resources. When resource use is higher, it is less likely that a strong recommendation will be made.
Each recommendation that was made was given a strength (strong, weak) and directionality (in favor of making an intervention or against making it). The evidence on which it is based was described as high, moderate, low or very low according to the GRADE system.
Patient participation
In the development process of the guideline, patients and their families were invited to two meetings (Table 6). Both patients and caregivers mentioned the importance that health professionals make decisions in a timely manner and using appropriate clinical criteria in order to cau-se a better outcome. Detailed information regarding the preferences of patients for each of the questions is addressed in the discussion of each question, including its effect on the recommendations.

Foundation for Medical and Technical Research and Education in Em
ergencies and Disasters
50 TABLE 6. Format of the report into patient participation in the development of the CPG
STAGE IN THE DEVELOPMENT
OF THE CPG
STRATEGIES FOR PATIENT PARTICIPATION
RESULT: SUMMARY OF INFORMATION FOUND
INCORPORATION: DESCRIPTION OF THE INFORMATION INCLUDED AND NOT INCLUDED, AND THE REASONS
FOR NOT DOING SO.
Defi nition of the scope of the CPG Questionnaire
The scope of the guide was briefl y described, in terms of the topics that were found to be of relevance to patients.
Formulation of questions Questionnaire
The potential questions were included and those that resulted being too technical and that could distort the information for patients were explained more simply.
Identifi cation and evaluation of outcomes.
Questionnaire
This stage addressed the outcomes produced by the working group and that were found to be of relevance for patients and relatives.
Formulation of recommendations Questionnaire
Patients and their carers made contributions that helped or modifi ed the recommendations made by the working group.

Clinical Practice Guideline for the diagnosis and treatm
ent of adult patients with severe Traum
atic Brain Injury G
uide for Health Professionals 2014 - G
uid
e N
o. G
PC
-20
14
-30
Ministry of H
ealth and Social Protection - Colciencias 51
STAGE IN THE DEVELOPMENT
OF THE CPG
STRATEGIES FOR PATIENT PARTICIPATION
RESULT: SUMMARY OF INFORMATION FOUND
INCORPORATION: DESCRIPTION OF THE INFORMATION INCLUDED AND NOT INCLUDED, AND THE REASONS
FOR NOT DOING SO.
Revision of the preliminary documents of the CPG.
Participation: The document was socialized with patients and their families.
Questionnaire: this was done through a survey and sending the document to a group of patients and relatives.
By consulting with patients through a survey, it was shown that for them it is very important that skilled professionals are responsible for patients with severe TBI and they are told about the techniques of coping with this situation.
The elements that are of most relevance to patients and their relatives are included, taking into account: The accompaniment and the role to be performed by the family as part of in-hospital and post-discharge treatment.
Construction of the guide for patients.
Participation: both family and patients were invited to help with the structuring of the document.
Questionnaire: the mechanism was an informal interview since there is a database of patients who have suff ered severe TBI and have been treated at Neiva hospital during the last 5 years
The entire contents of the patients’ version of the CPG obeyed the need that patients and their relatives have for information.
Aspects of the treatment of patients prehospital, as inpatients and after discharge were included.
No technical information was included regarding specifi c clinical procedures due to the lack of understanding of this information by patients and family.
Formulation of indicators and implementation
Questionnaire: the mechanism was an informal interview.
The contributions of the patients did not generate any changes to the indicators proposed by the working group.

Foundation for Medical and Technical Research and Education in Emergencies and Disasters52
Questions, evidence and recommendations
Question 1a
Which patients with TBI should have a computerized tomography (CT) of the head?
Recommendation
• It is recommended that every adult patient with TBI and who meet one or more of the following criteria must be have a CT scan: - Skull fracture (clinical or radiological) including signs of
basilar skull fracture (periorbital ecchymosis, retroauricu-lar ecchymosis, otorrhea, rhinorrhea).
- Post-traumatic seizure - Focal neurological de icit - Persistent vomiting (greater than or equal to two episodes) - Drop in the Glasgow Coma Scale of at least 1 point - Previous craniotomy - When the patient is a pedestrian who was hit by a car. - History of coagulopathy or pharmacologic anticoagulation - Patients suspected to be intoxicated. - Fall from height greater than 1.5 m - Retrograde Amnesia> 30 minutes and/or anterograde - Age greater than or equal to 60 years. - Severe headache - Blurred vision or diplopia
Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 53
IntroductionIntracranial injuries following a TBI can be detected using imaging, even before the manifestations of clinical signs. If a patient with mild TBI (Glasgow 13-15) arrivers at a health institution that does not have the facilities to perform imaging (CT scan), there is an important di-fference in the clinical practice in terms of decision making so that pa-tients who require this scan can be transferred promptly. Furthermore, even in institutions that have these facilities, there are discrepancies in the criteria for carrying out the exam on patients with mild TBI. There-fore, it is considered important to ask this question.
Summary of the evidenceThrough the search strategy described in annex 6, only one study with acceptable methodological quality was found, and this was evalua-ted through the SIGN meta-analysis instrument. This meta-analysis (Pandor 2012) included 71 studies analyzed in two separate groups (a group of 42 adults and a group of 29 children), evaluating the sen-sitivity, speci icity and positive and negative likelihood ratio for 32 cli-nical variables including injury mechanism and its relationship with a positive outcome after an intracranial injury or one that requires neurosurgery. According to the results of the mentioned imaging, the clinical elements were divided into those with greater possibility of association with injury (skull fracture and post-traumatic seizure) mo-derate possibility of association with injury (focal de icit, persistent vomiting, fall on the Glasgow scale, previous neurosurgery) and low possibility of association with injury (high fall, coagulopathy, chronic use of alcohol, age over 60, injury due to being struck by a car, vomiting and retrograde amnesia).
The sensitivity, speci icity and likelihood ratio results for each of the clinical variables, speci ically for indings of intracranial injury on the scans, are summarized in Table 7.

Foundation for Medical and Technical Research and Education in Emergencies and Disasters54
TABLA 7. Summary of the results of the meta-analysis made by Pandor 2012; fi ndings of each clinical variable for a diagnosis of
intracranial injury in adults with mild TBI (sensitivity, specifi city, LR+ and LR- grouped).
CLINICAL CHARACTERISTIC
NO. OF STUDIES
NO. OF PATIENTS SENSITIVITY SPECIFICITY LR(-) LR(+)
Over 60 years old 7 20.514 23,9c 88,0c 0,868 1,97
Anterograde or postraumatic amnesia
6 16.965 16,2c 91,9c 0,912 1,95
Basilar skull fracture 8 27.717 21,1c 98,4c 0,80 54,070
Coagulopathy 8 35.567 4,9c 98,2c 0,968 3,27
Depressed fracture of the skull
2 2680 9,1c 99,9 0,967 102,15
Fall from height 1 1064 28,0 87,8 0,820 2,29
Neurological focal defi cit 8 21.729 6,6c 98,6c 0,95 9,671
Reduction on the Glasgow Coma Scale
3 6365 27,3c 95,7c 0,763 6,39
Intoxication 10 31.156 21,4c 84,6c 0,931 1,38
Collision with vehicle 6 6716 15,9 95,4c 0,882 3,43
Persistent vomiting 4 29.556 16,1c 97,2c 0,871 5,53
Post-traumatic seizure 2 11.076 7,9c 99,4c 0,921 12,39
Previous neurosurgery 3 19.056 1,9 99,8c 0,985 8,67
Fracture on skull x-ray 8 6502 29,8c 97,4c 0,720 14,26
Retrograde amnesia 4 14.023 44,3c 81,6c 0,687 2,41
Persistent or severe cefalea 2 15.871 19,4c 80,5c 1,028 1,00
Visual problems (diplopia) 3 664 2,4 94,2c 1,033 0,39
c: signi icant heterogeneity, Value of P <0.05

Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 55
From evidence to recommendationThe discussion with the members of the working group considered all the criteria associated with risk of intracranial injury considering the importance of this study for the referral process for patients within the health system. It took into account the availability and importance of the CT scan at a national level.
Structural requirementsThis guide considers that, in order to carry out this recommendation, it is vital to have personnel who are suitably trained in the identi ication of these risk factors. These same factors must be considered during the development of clinical history forms in emergency departments at any level of complexity.
Considerations on benefi ts and risksIt is considered that the bene it of opportune identi ication and treatment of an intracranial injury outweighs the risk of the ionizing radiation associated with the taking of a brain scan.
Considerations on values and preferences of patientsPatients and their caregivers stated a clear preference for the oppor-tunity for early access to a de initive care center, one which has a level of specialization that is suitable for all the interventions that are requi-red, as soon as possible after the injury.
Implications on resourcesIt is considered that the bene it of applying the recommendation can be cost effective, taking into account that the cost of a brain scan is less than the cost of an unidenti ied, untreated intracranial injury. It should be taken into account that in Colombia there are no economic studies on the implications of this intervention.
References1. Pandor A, Harnan S, Goodacre S, Pickering A, Fitzgerald P, Rees A.
Diagnostic accuracy of clinical characteristics for identifying CT abnormality after minor brain injury: a systematic review and meta-analysis. J Neurotrauma 2012; 29: 707-718.
Foundation for Medical and Technical Research and Education in Emergencies and Disasters56
Flowchart for the process of inclusion in articles
References identifi ed through searches of databases
(n=261)Pubmed: 175Embase: 26Biosis: 19Scisearch: 20Medpilot: 10Cochrane: 1Tripdatabase: 10
References obtained manually(n=1)
Duplicate References(n=7)
Articles not related(n=254)
Excluded articles(n=0)
All references obtained(n=262)
References included with title and abstract that were revised
(n=255)
Revised Articles(n=1)
Included articles(n=1)

Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 57
Algorithm 1Transfer to high-level centers (questions 1a and 1b)
Mild13-15
*Criteria of CT
• Skull fracture (clinical or radiological) including signs of fracture of the skull base (periorbital ecchymosis and ecchymosis headpiece, otoliquia, rinoliquia).
• Traumatic seizure• Focal neurologic defi cit• Persistent vomiting (greater than or equal to two
episodes)• Fall of the Glasgow of at least 1 point• Previous Craniotomy• Mechanism of the trauma produced by runover in
condition of pedestrian• History of coagulopathy or pharmacological
anticoaugulacion• Patient with suspected poisoning• Fall from height greater than 1.5 meters• Retrograde Amnesia > 30 minutes and/or
anterograde• Age greater than or equal to 60 years• Severe headache• Blurred vision or diplopia
**Transfer criteria
• Glasgow under 15 up to 2 hours after the injury• Severe headache• Persistent vomiting (greater than or equal to two
episodes)• Skull fracture (clinical or radiological) including signs
of fracture of the skull base (periorbital ecchymosis and ecchymosis headpiece, otoliquia, rinoliquia).
• Age greater than or equal to 60 years• Blurred vision or diplopia• Traumatic seizure• Focal neurologic defi cit• Previous Craniotomy• Fall from height greater than 1.5 meters• Retrograde Amnesia > 30 minutes and/or
anterograde• Suspicion of intoxication with alcohol and/or
psychoactive substances
Transfer to high complexity center with emphasis on
trauma care
Continue management in Center of low to
medium complexity
Meets criteria of CT*
Moderate-Severe3-12
Adult patient with TBI
Perform Glasgow Coma Scale
Meets criteria for transfer**
Yes
Yes
No
No
Foundation for Medical and Technical Research and Education in Emergencies and Disasters58
Question 1b
Which patients with TBI should be transferred from low-level of care hospitals to centers with neurosurgery and neuroimaging services?
Recommendation
• It is recommended that patients with moderate to severe TBI (Glasgow 3-12) should be transferred immediately to high-level of care hospitals with access to neuroimaging and neu-rosurgery.
• It is recommended that patients with mild TBI (Glasgow 13-15) who present one or more of the following criteria be re-ferred for evaluation at an institution that has access to neu-roimaging and neurosurgery: - Glasgow coma score under 15 up to 2 hours after injury - Severe headache - More than 2 episodes of vomiting - Skull fracture, including depressed fractures or clinical sig-
ns of fracture of the skull base (raccoon eyes, retro auricu-lar ecchymosis, otorrhea or rhinorrhea)
- Age greater than or equal to 60 years old - Blurred vision or diplopia - Post-traumatic seizure - Focal neurological de icit - Previous craniotomy. - Fall of over 1.5 meters. - Retrograde amnesia more than 30 minutes and/or antero-
grade amnesia. - Suspected intoxication with alcohol and/ or psychoactive
substances.• It is recommended that patients with mild TBI and who are
in active treatment with anticoagulants, have active coagula-pathies, or are pregnant should be transferred to centers with neurosurgery and neuroimaging services.

Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 59
IntroductionCurrently, several health institutions in Colombia do not have a spe-cialized trauma department for evaluation and decision-making in relationship with the heterogeneous group that involves patients with TBI. Usually patients with moderate to severe TBI (Glasgow 3-12) are transferred immediately due to the clear need for diagnos-tic imaging of the brain. The greatest variability in the criteria for transfer of patients is in those with mild TBI (Glasgow 13-15). The vast majority of low and medium complexity centers, especially rural hospitals, do not have a scanner available which could support prog-nostics or therapeutic decisions and for this reason it is important to establish what clinical criteria correlate with the presence of in-tracranial injury in patients with mild TBI. Because of this reality in terms of disparity of resources, this situation raises the need to de i-ne which patients should be transferred to a higher level of care cen-ter and when. For this reason, it was considered important to analyze the current evidence to establish clinical and imaging criteria for re-ferring patients with TBI to neurosurgical services.
Summary of the evidenceThrough the search strategy described in Annex 6, a meta-analysis was identi ied (Dunning 2004) that evaluated studies on prognostic factors, indicating the relative risk that a person with certain clinical indings has of developing any intracranial pathology. Additionally, a
systematic review was found (Harnan 2011), which included analyses of diagnostic accuracy of different clinical rules for decision making in patients with mild TBI who are at risk of intracranial injury. After the analysis of the two studies, the inal recommendation was made based on a systematic review of Harnan, 2011. The reason for choosing this study (which assesses more recent evidence than the meta-analysis and which presents an acceptable methodological quality evaluated using the AMSTAR methodology) was based on that fact that the clini-cal decision algorithms discussed in this paper can be used in our envi-ronment, in accordance with the technology available in Colombia and the characteristics of the care system. This review examined 19 studies that reported accurate data regarding 25 decision rules. Of these, 9, which all speci ied neurosurgical outcomes, were reported including groups of high and medium risk. The decision rules were intended to identify those adult patients with TBI who are at risk of an injury requiring neurosurgical intervention (considered high risk) and tho-
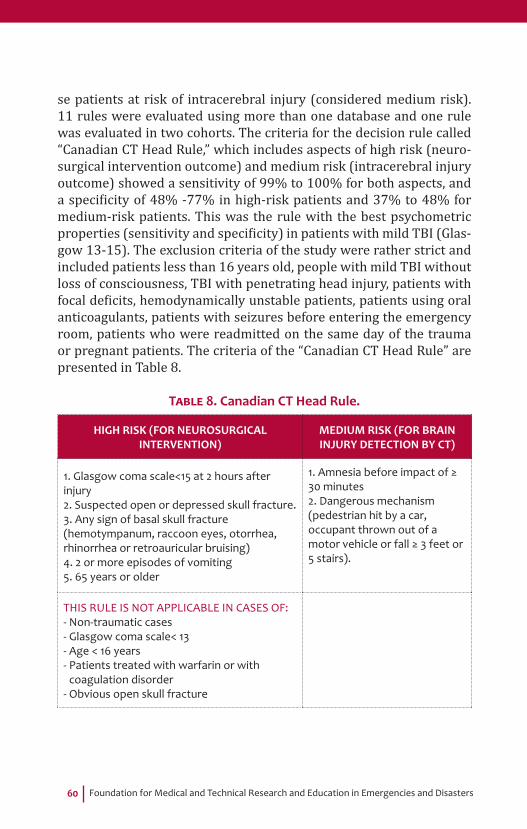
Foundation for Medical and Technical Research and Education in Emergencies and Disasters60
se patients at risk of intracerebral injury (considered medium risk). 11 rules were evaluated using more than one database and one rule was evaluated in two cohorts. The criteria for the decision rule called “Canadian CT Head Rule,” which includes aspects of high risk (neuro-surgical intervention outcome) and medium risk (intracerebral injury outcome) showed a sensitivity of 99% to 100% for both aspects, and a speci icity of 48% -77% in high-risk patients and 37% to 48% for medium-risk patients. This was the rule with the best psychometric properties (sensitivity and speci icity) in patients with mild TBI (Glas-gow 13-15). The exclusion criteria of the study were rather strict and included patients less than 16 years old, people with mild TBI without loss of consciousness, TBI with penetrating head injury, patients with focal de icits, hemodynamically unstable patients, patients using oral anticoagulants, patients with seizures before entering the emergency room, patients who were readmitted on the same day of the trauma or pregnant patients. The criteria of the “Canadian CT Head Rule” are presented in Table 8.
TABLE 8. Canadian CT Head Rule.
HIGH RISK (FOR NEUROSURGICAL INTERVENTION)
MEDIUM RISK (FOR BRAIN INJURY DETECTION BY CT)
1. Glasgow coma scale<15 at 2 hours after injury2. Suspected open or depressed skull fracture.3. Any sign of basal skull fracture (hemotympanum, raccoon eyes, otorrhea, rhinorrhea or retroauricular bruising)4. 2 or more episodes of vomiting5. 65 years or older
1. Amnesia before impact of ≥ 30 minutes2. Dangerous mechanism (pedestrian hit by a car, occupant thrown out of a motor vehicle or fall ≥ 3 feet or 5 stairs).
THIS RULE IS NOT APPLICABLE IN CASES OF:- Non-traumatic cases- Glasgow coma scale< 13- Age < 16 years- Patients treated with warfarin or with
coagulation disorder- Obvious open skull fracture

Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 61
The full group of evaluated rules is presented in table 9.
TABLA 9. Sensitivity and specifi city of the decision rules to identify injuries that require neurosurgical intervention
STUDY SENSITIVITY SPECIFICITY
CCHR High Risk 0,99 - 1,00 0,48 - 0,77
New Orleans Criteria 0,99 - 1,00 0,04 - 0,31
New Orleans Criteria adapted to cohort 1.00 0.03
CCHR High and Medium Risk 0,99 - 1,00 0,37 - 0,48
CCHR High and Medium Risk adapted to cohort 1.00 0.37
NCWFNS High and Medium Risk 0,94 - 0,99 0,03 - 0,44
NICE lenient criteria 0,94 - 0,98 0,29 - 0,67
Scandinavian lenient criteria 0,94 - 0,99 0,20 - 0,50
Miller criteria 0,50 - 1,00 0,61 - 0,66
CCHR (Canadian CT head rule), NCWFNS (Neurotraumatology Committee of the World Federation of Neurosurgical Societies).
From evidence to recommendationThe discussion with the working group took into account the system of reference and counter-reference established within the legal fra-mework of the General System of Social Security in Colombia and the aspects of cost and availability of resources together with the compo-nent of patient safety. It was considered important to combine the evi-dence recommended in order to make neurological scans with those recommended for assessment for neurosurgery. Two groups were es-tablished according to the level of severity of the injury (Glasgow 3-12 and Glasgow 13-15) and speci ic recommendations were constructed based on these.
Structural requirementsIt is considered that to carry out this recommendation, there is a need to have personnel properly trained in identifying these risk factors. These same factors must be taken into account during the development of me-dical history formats in emergency services of any complexity.

Foundation for Medical and Technical Research and Education in Emergencies and Disasters62
Considerations on benefi ts and risksIt is considered that the bene it of the identi ication and prompt treatment of an intracranial lesion outweighs the risk that a process of referral to a higher level of complexity might implicate.
Considerations on the values and preferences of patientsThe patients and their caregivers expressed a clear preference for the opportunity for early access to a de initive care center, which includes the appropriate level of complexity for all interventions that may be required, as soon as possible after injury.
Implications on resourcesIt is considered that the bene it of implementing the recommendation may be cost effective, given that the cost of an unidenti ied intracra-nial injury without appropriate treatment can be much higher than the cost of the referral process. It is important to keep in mind that there are no economic studies on the implications of this recommendation in Colombia.
References1. Dunning J, Stratford-smith P, Lecky F, Batchelor J, Hogg K, Browne
J, et al. A Meta-Analysis of clinical correlates that predict signi icant intracranial injury in adults whit minor head trauma. J Neurotrauma. 2004; 21 (7): 877-885.
2. Harnan SE, Pickering A, Pandor A, Goodacre SW. Clinical decision rules for a adults with minor head injury: a systematic review. J Trauma. 2011; 71 (1): 245-251.
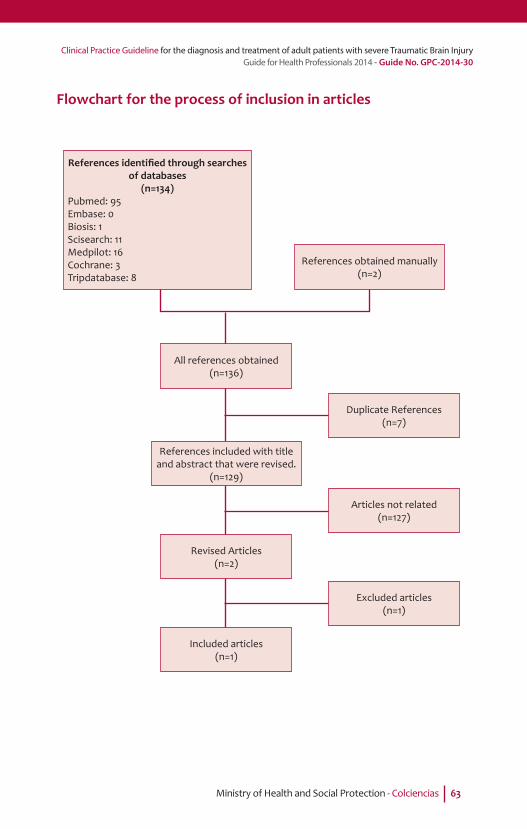
Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 63
Flowchart for the process of inclusion in articles
References identifi ed through searches of databases
(n=134)Pubmed: 95Embase: 0Biosis: 1Scisearch: 11Medpilot: 16Cochrane: 3Tripdatabase: 8
References obtained manually(n=2)
Duplicate References(n=7)
Articles not related(n=127)
Excluded articles(n=1)
All references obtained(n=136)
References included with title and abstract that were revised.
(n=129)
Revised Articles(n=2)
Included articles(n=1)
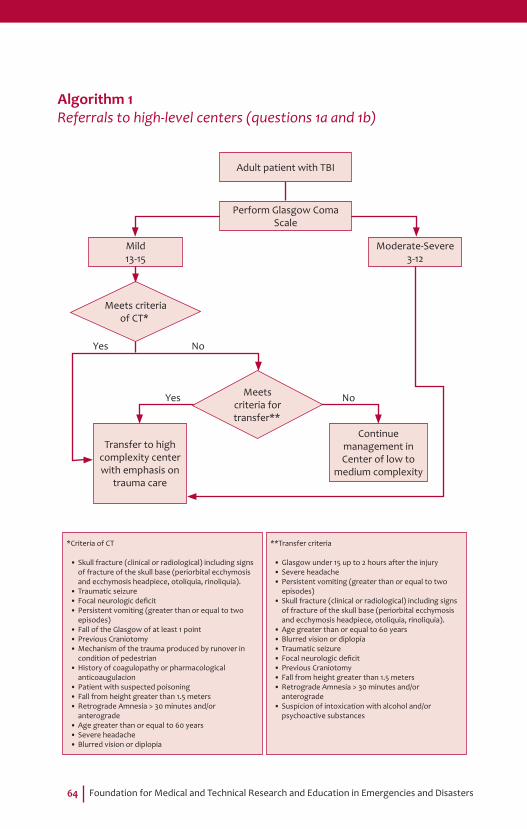
Foundation for Medical and Technical Research and Education in Emergencies and Disasters64
Algorithm 1Referrals to high-level centers (questions 1a and 1b)
Mild13-15
*Criteria of CT
• Skull fracture (clinical or radiological) including signs of fracture of the skull base (periorbital ecchymosis and ecchymosis headpiece, otoliquia, rinoliquia).
• Traumatic seizure• Focal neurologic defi cit• Persistent vomiting (greater than or equal to two
episodes)• Fall of the Glasgow of at least 1 point• Previous Craniotomy• Mechanism of the trauma produced by runover in
condition of pedestrian• History of coagulopathy or pharmacological
anticoaugulacion• Patient with suspected poisoning• Fall from height greater than 1.5 meters• Retrograde Amnesia > 30 minutes and/or
anterograde• Age greater than or equal to 60 years• Severe headache• Blurred vision or diplopia
**Transfer criteria
• Glasgow under 15 up to 2 hours after the injury• Severe headache• Persistent vomiting (greater than or equal to two
episodes)• Skull fracture (clinical or radiological) including signs
of fracture of the skull base (periorbital ecchymosis and ecchymosis headpiece, otoliquia, rinoliquia).
• Age greater than or equal to 60 years• Blurred vision or diplopia• Traumatic seizure• Focal neurologic defi cit• Previous Craniotomy• Fall from height greater than 1.5 meters• Retrograde Amnesia > 30 minutes and/or
anterograde• Suspicion of intoxication with alcohol and/or
psychoactive substances
Transfer to high complexity center with emphasis on
trauma care
Continue management in Center of low to
medium complexity
Meets criteria of CT*
Moderate-Severe3-12
Adult patient with TBI
Perform Glasgow Coma Scale
Meets criteria for transfer**
Yes
Yes
No
No
Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 65
Question 2
In adult patients with severe TBI, does the treatment in an organized trauma care center, compared to treatment in a general non-speciali-zed center reduce mortality?
Recommendation
• It is suggested that adult patients with severe TBI be trans-ferred directly to a leading high-complexity institution with emphasis on trauma care.
Weak recommendation in favor of intervention, low quality evidence.
IntroducciónThe organization and development of trauma care systems have been related to a reduction in the rates of mortality and disability for this condition (Mendelof 1991, Sampallis 1997, Maconel 2005, MacKenzie 2006, Rubiano 2013). Patients with severe TBI bene it equally from the organization and development of trauma care systems. Therefore, this type of recommendation has been established in consensus docu-ments and treatment guidelines in different parts of the world (Mass 1997, BTF 2007, Shima 2010). Regional hospitals and clinics with or-ganized trauma care systems (including intensive care units speciali-zed in trauma, residency programs with emphasis on trauma, active processes of education and research in trauma and surgical teams with training in trauma) and high volumes of patients admitted per year (more than 1200 admissions of trauma patients per year or at least 240 admissions with injury severity scores greater than 15), have been associated with a reduction in complications in the treatment of patients with severe TBI. The presence of neurosurgeons and neuroin-tensive care units within these organizations generate additional be-ne its for patients who have been transferred from institutions that do not have this resource, especially related to the proper management of the airway, early correction of hypotension and early management of intracranial hypertension. Due to the high variability in healthcare re-sources because of the lack of organization of speci ic trauma care sys-tems in Colombia, it was considered very important to de ine whether

Foundation for Medical and Technical Research and Education in Emergencies and Disasters66
the treatment of adult patients with severe TBI in organized trauma care centers vs the treatment of adult patients with severe TBI in cen-ters with lower level of organization reduces mortality and associated complications.
Summary of the evidenceThere are few international rankings for determining characteristics of organized trauma care systems. One of the most used rankings is the classi ication suggested by the Committee on Trauma of the American College of Surgeons (2006). They have developed a system to classify institutions by their ability to serve trauma patients with the aim of helping communities in the organization and development of these sys-tems. In accordance with this classi ication, this guide recognizes three levels. The highest level of specialization corresponds to a renowned institution or a center of greater specialization that serves as a reference point for other levels of care. Medium specialized levels are centers that serve as the starting point for referrals, especially from rural areas, and the low level of specialization is the closest point of care to where the event occurred. Each of these levels has been assigned characteristics, which are as follows:
High-specialized level• In house 24 hours a day for general surgery and immediate avai-
lability of other specialists such as orthopedics, neurosurgery, anesthesiology, emergency medicine, radiology, internal medi-cine, plastic surgery, maxillofacial surgery, and adult and pedia-tric intensive care. - A referral center for the community from nearby regions. - A leading center in prevention and public education for the
community. - Provides continuing education to members of the trauma
team. - Includes a trauma quality improvement program.
• Performs organized activities in teaching and research that help to innovate in trauma care. - Has screening programs for substance abuse and intervention.
• Meets minimum requirements in terms of the annual volume of admissions of severely traumatized patients.
Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 67
Medium-specialized level• Immediate 24-hour coverage by general surgeons, and coverage
of specialties such as orthopedics, neurosurgery, anesthesiolo-gy, emergency medicine, radiology and intensive care.
• Other services such as cardiac surgery, hemodialysis and micro-vascular surgery should be referred to the high-specialized level institutions.
• Provide trauma prevention services and have continuing educa-tion programs for their staff. - Has a trauma quality improvement program.
Low-specialized level• Immediate 24-hour coverage by emergency doctors and imme-
diate availability of surgeons and anesthesiologists. - Has a trauma quality improvement program.
• Has an organized referral system for patients requiring trans-fers to medium and high-specialized level institutions. - Serves as a support center for rural and community hospitals.
• Provides continuing education for nurses and other members of the trauma team. - Engages in prevention programs for their community.
A literature search revealed only one observational database analysis study that could give an answer to the PICO question (DuBose 2008). Additionally, an ongoing randomized study was found (HITS-NS), but being an ongoing study, no preliminary data had been published. This study compares adult patients with moderate to severe TBI who are transported to the nearest center vs those transferred to specialist neurosurgical centers and is in the pilot feasibility phase, waiting to randomize 350 patients in each arm of the study. The DuBose study analyzed 16,035 patients with severe TBI, de ined by having a head AIS greater than or equal to 3 without severe injuries to other body parts. These patients were treated in 71 high-specialized trauma ins-titutions and 55 medium specialized institutions. The study found hig-her rates of mortality and complications in medium specialized insti-tutions. Mortality was 9.6% in the high-specialized centers and 13.9% in medium specialized centers. The rate of complications in more complex centers was 10.6% and in medium complexity centers it was 15.5%. It was found that the progression of neurologic injury (given
Foundation for Medical and Technical Research and Education in Emergencies and Disasters68
by progression of secondary injury mechanisms such as hypotension and hypoxemia) was higher in medium specialized institutions (2% vs 1%). In the analysis of independent risk factors for mortality, it was found that the simple fact of being admitted to a medium specialized institution was a risk factor as important as the fact of being admitted with a penetrating mechanism, having a higher rate of severity, suffe-ring from hypotension or having a low Glasgow score.
From evidence to recommendationDuring the meeting with the working group, it was considered that this is a weak recommendation for intervention because the balance between the desired result (reduction in mortality and complications at discharge) vs unwanted effects (increased mortality and complica-tions at discharge) is slightly in favor of the irst one. The discussion took into account the aspects of cost and availability in the General System of Social Security in Health (GSSSH) and the integration of cu-rrent evidence from organized trauma care systems within the natio-nal system was considered to be an important aspect. Therefore, crite-ria for good clinical practice, which should be met by high-specialized centers with emphasis on trauma care, were established. It was felt that renowned public and private centers that handle high volumes of patients with trauma could therefore be de ined as organized care centers if they meet the criteria associated with good clinical practice.
Structural requirementsGiven that the Colombian GSSSH currently organizes health care faci-lities as having low, medium or high complexity, and there are some eligibility criteria for each of these levels, it is considered that to carry out this recommendation, there is already an organizational structure, supported by current regulations, that is equivalent to the criteria set earlier. The criteria recommended and established in the studies that were reviewed include:
• Permanent presence (24 hours) of general surgeons with trai-ning in trauma, immediate availability of specialists in orthope-dics, neurosurgery, anesthesiology, emergency medicine, radio-logy, internal medicine, plastic surgery, oral and maxillofacial surgery and critical care.
• Being a center of reference for hospitals with lower level of complexity.
Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 69
• Providing a leading process in prevention and public education for the region.
• Providing permanent continuing education for members of the trauma care team.
• Including a quality improvement program in trauma care, in-cluding review panels for preventable deaths and periodic mee-tings on morbidity and mortality in trauma; Leading processes in education and research in trauma that generate innovation in the topic.
• Having screening programs for substance abuse and interven-tion for these patients.
• Meets minimum requirements in terms of the annual volume of admissions of severely traumatized patients (more than 1200 admissions of trauma patients per year or at least 240 admis-sions with AIS greater than 15).
Considerations on benefi ts and risksIt is considered that the bene it of prompt and comprehensive treatment of an intracranial injury does not carry any risk that should be assumed by the care system.
Considerations on the values and preferences of patientsPatients and their caregivers expressed a clear preference for the op-portunity to access advanced comprehensive care, including that the personnel performing the procedures have an appropriate level of tra-ining for all interventions that are required, as soon as possible after injury. There was for this reason, no consideration that amended the recommendations.
Implications on resourcesIt is considered that the bene it of implementing the recommendation can be cost effective, considering that the cost of an intracranial lesion without proper treatment can be much greater than the cost involved in any minimum changes in the regulations of the system. It is impor-tant to keep in mind that there are no economic studies on the implica-tions of this recommendation in Colombia.

Foundation for Medical and Technical Research and Education in Emergencies and Disasters70
References1. Mendeloff JM, CaytenCG.Trauma systems and public policy. Annu Rev
Public Health.1991;12:401-24.2. Sampallis JS, Denis R, Fréchette P, Brown R, Fleiszer D, Mulder D.Direct
transport to tertiary trauma centers versus transfer from lower level facilities: impact on mortality and morbidity among patients with major trauma. J Trauma. 1997; 43(2): 288-95.
3. McConnell J, Newgard C,MullinsR, Arthur M, Hedges J. Mortality Bene it of Transfer to Level I versus Level II Trauma Centers for Head-Injured Patients. Health Services Research. 2005;40(2):435–458.
4. Rubiano AM, Puyana JC, Mock CN, Bullock R, Adelson D. Strengthening neurotrauma care systems in low and middle income countries. Brain Injury. 2013; 27 (3): 262-272.
5. Maas AI, Dearden M, Teasdale M, Braakman R, Cohadon F, Lannotti F. et all. EBIC- Guidelines for management of severe head injury in adults. Acta Neurochirurgica. 1997; 139(4): 286-294
6. Brain Trauma Fundation. Guidelines for the management of severe traumatic brain injury. Journal of Neurotrauma, 2007; 24 (1): S-1 – S-106.
7. Shima K, Aruga T, Onuma T, Shigemori M, et all. Guidelines for the Management of Severe Head Injury. Asian J Neurosurg. 2010; 5 (1): 15-23.
8. American College of Surgeons. Resources for optimal care of the injured patient. Committee on Trauma. 2006
9. DuBose JJ, Browder T, Inaba K, Teixeira PG, Chan LS, Demetriades D. Effect if trauma center designation on outcome in patients with severe traumatic brain injury. Arch Surg. 2008; 143(12):1213-1217.

Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 71
Flowchart for the process of inclusion in articles
References identifi ed through searches of databases
(n=256)Pubmed: 192Embase: 41Biosis: 2Scisearch: 4Medpilot: 13Cochrane: 3Tripdatabase: 1
References obtained manually(n=1)
Duplicate References(n=4)
Articles not related(n=252)
All references obtained(n=257)
References included with title and abstract that were revised
(n=253)
Revised Articles(n=1)
Included articles(n=1)

Foundation for Medical and Technical Research and Education in Emergencies and Disasters72
Question 3
In adult patients with severe TBI, does prehospital orotracheal in-tubation, compared with orotracheal intubation in emergency de-partments, reduce neurological disability or mortality, evaluated at 6 months post-injury?
Recommendation
• It is recommended that adult patients with severe TBI need to be intubated in the trachea in a prehospital setting, using a ra-pid sequence intubation, which includes inductor medication and neuromuscular paralysis medication.
Strong recommendation in favor of intervention, moderate quality of evidence.
• The recommended dosages to be used are the following: - Fentanyl Dose: 1 μg/Kg - Midazolam Dose: 0.1mg/Kg - Succinylcholine Dose: 1 mg/Kg
Strong recommendation in favor of intervention, moderate quality of evidence.
• The use of half the dose of inductor medications suggested above is recommended if the patient has systolic blood pres-sure <100mmHg, or is >60 years old.
Strong recommendation, moderate quality of evidence
• Orotracheal intubation in a prehospital setting should be ca-rried out by skilled medical personnel or prehospital techno-logists (who have an adequate level of training). Technologists must carry out the procedure under direct or indirect super-vision of a doctor with experience in handling prehospital and in-hospital emergencies.
Weak recommendation in favor of intervention, low quality of evidence.

Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 73
• We suggest that adequate training as part of intubation training programs should be considered to be at least 16 hours of theo-retical-practical training in rapid sequence intubation, including at least 4 hours of theory, 8 hours of experience in intubation in operating theaters under the supervision of an anesthesiologist and at least 4 hours of evaluation in simulators.
Weak recommendation, moderate quality of evidence.
• It is recommended that if the attempt to intubate is not suc-cessful, patients should continue to be ventilated with a bag valve mask system, together with an oropharyngeal airway, until they return to spontaneous respiration. If this method is insuf icient to achieve a pulse oximetry >90%, we recommend the use of a laryngeal mask, as a rescue device.
Strong recommendation in favor of intervention, moderate quality of evidence.
• It is suggested that in the case that the patient is being moved by a basic ambulance, and there is no technologist or medic on board, ventilation should be carried out with a bag valve mask system, together with an oropharyngeal airway in order to achieve a pulse oximetry of >90%.
Good clinical practice
IntroductionHypoxia, de ined as a lack of oxygen in the organism is identi ied by episodes of absence of breathing (apnea), purple coloration of the skin (cyanosis) or hypoxemia (established by measuring the oxygen level in the peripheral arterial blood) and has been strongly associated as a harmful factor in the evolution of patients with severe TBI. Diverse clinical studies have identi ied hypoxia at a prehospital level as one of the predictive elements strongly associated with the presence of neu-rological disability and mortality in these patients after being dischar-ged. This has been associated with the physiological mechanisms that trigger so-called secondary brain injuries, especially the changes rela-ted to ischemia, necrosis and brain swelling. Advanced management of airways through orotracheal intubation is one of the fundamental principles when treating patients with severe TBI in emergency de-partments of low, medium and high level health centers. Observational

Foundation for Medical and Technical Research and Education in Emergencies and Disasters74
studies have been inconsistent in trying to identify if the use of this procedure in prehospital care (before arriving at health centers) redu-ces neurological disability and mortality in patients with severe TBI, or not. This is mainly due to heterogeneity in the management protocols, evaluation of heterogeneous populations and evaluations of monito-ring being limited to the stay in hospital. All these studies have been made in environments different to Latin America. There has only been one controlled and randomized clinical study that compared prehos-pital orotracheal intubation with in-hospital orotracheal intubation in adult patients with severe TBI. It was published in 2010, and evaluated the results in terms of neurological disability and mortality in the 6 months following the injury in an Australian population. All the clini-cal studies published on the topic between 1990 and 2013 in English and Spanish were evaluated to determine the level of evidence pre-sented by the studies, in order to conclude if prehospital orotracheal intubation reduces neurological disability and mortality in patients over 15 years old with severe TBI, compared with situations where it is carried out in the emergency departments of health centers.
Summary of the evidenceA total of 14 observational studies together with 1 randomized contro-lled clinical study were evaluated (See Annex 6). After reviewing these studies, the recommendation was based on the only randomized and controlled clinical study, in patients over 15 years old with severe TBI (Bernard 2010). This study randomized 312 patients to prehospital orotracheal intubation with a rapid sequence of medication, or to ma-nual ventilation until the patient arrived at the hospital for orotracheal intubation in the emergency department. In this study, adequate trai-ning as part of training programs was considered to be at least 16 hours of theoretical-practical training in the rapid sequence of intubation, in-cluding at least 4 hours of theory, 8 hours of experience in intubation in operating theaters under the supervision of an anesthesiologist and at least 4 hours of evaluation in simulations. Mortality after 6 months was 33.8% in patients intubated before arriving at hospital and 38.7% for patients’ intubated in-hospital in the emergency department. The suc-cess rate of pre-hospital intubation was 97%. After six months, the per-centage of patients with a favorable outcome (GOSe 5–8) was 51% in the group intubated in the ambulance, compared with a favorable outcome (GOSe 5-8) of 39% in the group that were intubated in-hospital. Upon analyzing the available literature, it was found that the great majority of
Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 75
studies that supported this intervention were made in environments in which training of prehospital personnel has a suitable academic certi i-cation for carrying out the procedure, which is renewed periodically. For this reason, an additional search was made in order to look for evidence on the success rate in the procedure of intubation by paramedics and if there is any relationship between this and the level of experience of the person who performs the procedure.
The recommendation was made based on one randomized study, which compared the success rate of intubation made by paramedics in training with that of expert pre-hospital laryngoscopists (medics and paramedics) in a model of dif icult intubation (Woollard 2008). The rate of intubation at the irst attempt for paramedics in training was 0⁄23 (0%) and for expert laryngoscopists was 14⁄56 (25%). The esophageal intubation rate for paramedics in training was 15⁄23 (65%) and for expert laryngoscopists was 9⁄56 (16%). The failure rate for dif icult intubation was 57.1% for expert laryngoscopists and 69.6% for paramedics in training, after 3 attempts.
From evidence to recommendationDuring the meeting with the GDG it was considered that this is a strong recommendation in favor of intervention, because the balance between the desired results (improvement in disability and reduction in mortality after 6 months) versus the undesired (injury to airways, esophageal intubation and adverse reaction to medication during the procedure) is highly in favor of the irst group. The group took into account the study of cost-effectiveness made in the economic section of this guide and discussed the aspects of availability of resources and safety of the intervention. For this reason, and taking into account the quality of the evidence, speci ic recommendations were established that are directed towards offering quality care with aspects that must be strengthened with evaluation of compliance by the respective or-ganizations. This compliance must be evaluated speci ically in aspects of training in protocols of rapid intubation and alternative methods of management of airways in the case that the intubation process fails. The development group discussed the importance of suggesting doses of medication adjusted to the average weight of the Colombian popu-lation, taking into account the medication used in the evaluated study.

Foundation for Medical and Technical Research and Education in Emergencies and Disasters76
Structural requirementsWe consider that to bring about this recommendation, there is a need for appropriately trained personnel in the procedure of intubation with a rapid sequence of medication. The current programs of study in medi-cine and technology in prehospital care have speci ic modules for trai-ning in orotracheal intubation. Additionally, and taking into account the Colombian standards for habilitation of health care transport units, it is considered that the necessary resources to carry out the procedures are the following:
Basic Care Transport Unit• Personnel: Technologist in PHC (Pre-hospital care) or profes-
sional technician in PHC or nursing assistant with certi icate of training in the skill of basic life support.
• Equipment: Pulse oximeter, medicinal oxygen system.• Medication, medical devices or supplies: self-in latable bag-valve-
mask device with oxygen tanks for adults, supraglottic airway devices in different sizes.
Unidad de Traslado Asistencial Medicalizado• Personnel: Doctor, Nurse or Technologist in PHC, with certi icate
of at least 48h of training in advanced life support.• Equipment: Pulse oximeter, medicinal oxygen system, portable
mechanical ventilator, adult laryngoscope with 3 valves of diffe-rent sizes, laryngeal masks of different sizes, intubation guide and capnograph.
• Medication, medical devices or supplies: Vials of midazolam (5mg or 15mg), vials of fentanyl (500μg or 1.000μg), vials of succin-ylcholine (100mg or 250mg), endotracheal tubes of different sizes.
The abovementioned items must be considered during the develop-ment of formats of clinical histories in transport and emergency servi-ces of any level of complexity.
Considerations regarding benefi ts and risksIt is considered that the bene it of prehospital orotracheal intubation in patients with compromised oxygenation associated with an intra-

Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 77
cranial injury outweighs the risk associated with late intubation in the health center that initially manages the patient. The risks associated with a problem during the process of intubation with a rapid sequence of medication are equal in both situations (prehospital and in-hospi-tal). These risks will be minimized if each unit has the recommended equipment and the suggested training process.
Considerations regarding values and preferences of patientsPatients and their caregivers show a clear preference for the opportu-nity to have access to advanced comprehensive care, which includes the fact that the personnel who carry out the procedures have a sui-table level of training in order to perform the interventions that are required, as soon as possible after the injury. Therefore, there was no consideration that changes the recommendations.
Implications regarding resourcesIt is considered that the bene it of applying the recommendation is cost effective, considering that the cost of complications associated with ce-rebral hypoxia due to not receiving suitable treatment can be much greater than the cost that could result from the use of appropriate re-sources to carry out the procedure. It must be taken into account that that this guide makes the irst study of cost-effectiveness in Colombia for this speci ic question. The study clearly shows that intervention is cost-effective.
References1. Bernard SA, Nguyen V, Cameron P, Masci K, Fitzgerald M, Cooper
DJ, Prehospital Rapid Sequence Intubation Improves Functional Outcome for Patients With Severe Traumatic Brain Injury. Annals of Surgery.2010; 252(6):959-965.
2. Woollard M, Lighton D, Mannion W, Watt J, McCrea C, Johns I, Hamilton L, O’Meara P, Cotton C, Smyth M. Airtraq vs standard laryngoscopybystudentparamedics and experienced prehospital laryngoscopistsmanaging a model of dif icultintubation. Anaesthesia. 2008;63(1):26-31.

Foundation for Medical and Technical Research and Education in Emergencies and Disasters78
Flowchart for the process of inclusion in articles
References identifi ed through searches of databases
(n=95)Pubmed: 65Embase: 0Biosis: 10Scisearch: 11Medpilot: 3Cochrane: 2Tripdatabase: 4
References obtained manually(n=9)
Duplicate References(n=6)
Articles not related(n=88)
All references obtained(n=104)
References included with title and abstract that were revised.
(n=98)
Revised Articles(n=10)
Included articles (n=1)
Excluded articles(n=9)
Not adequately show the results: 2

Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 79
Algorithm 2Prehospital intubation (question 3)
*The recommended dosages to be used are the following: • Fentanyl Dose: 1 μg/Kg• Midazolam Dose: 0.1mg/Kg• Succinylcholine Dose: 1 mg/Kg
**In verifi ed, tracheal Intubation with pulse oximetry >90 %.Orotracheal intubation in a prehospital setting, should be performed by skilled medical personnel or prehospital technologists (who have an adequate level of training). Technologists must carry out the procedure under direct or indirect supervision of a physician with experience in the management of prehospital and in-hospital emergencies.
SBP<100 mmHg or age >60
years
Orotracheal Intubation
successful**
Pulse oximetry is
higher than 90%
Pulse oximetry is less
than 90%
PSBP>100 mmHg or age <60
years
Adult patient with severe TBI in ambulance
Evaluate systolic blood pressure (SBP) and age range
Provide 250 cc of normal salineIf the patient has
not been intubated (OTI), perform rapid sequence intubation.
It is recommended that you use half of the
conventional-dose of the induction drugs. *
Continue transfer to emergency room (see
Algorithm Question No. 6, Surgery time)
If the patient has not been intubated (OTI), perform rapid sequence intubation.
It is recommended that you use the
conventional-dose of the induction drugs. *
Continue ventilation system with a bag-valve-mask (BVM)
along with oropharyngeal cannula
Place laryngeal mask
Yes
Yes
Yes
Yes
No
No
No
No

Foundation for Medical and Technical Research and Education in Emergencies and Disasters80
Question 4
In adult patients with severe TBI, does the use of 7.5% hypertonic so-lutions for resuscitation in prehospital setting, compared with the use of isotonic resuscitation solutions, reduce neurological disability or mortality, evaluated at 6 months post-injury?
Recommendation
• It is recommended that adult patients with severe blunt TBI without hypotension can be treated at a prehospital level with 250ml of saline solution at 0.9%
Strong recommendation in favor of intervention, moderate quality of evidence
• It is recommended that patients with penetrating TBI or with hypotension can be treated at a prehospital level with 250ml of saline solution at 0.9%.
Good clinical practice.
IntroductionSevere TBI generates cellular responses that increase the likelihood of injury including ischemia associated with hypoxia and hypoten-sion inducing more cell injury. It has been shown that ischemia and in lammation following head trauma start from the moment of injury (Gaetz 2004, Miller 1978). Early and timely control of physiological variables such as oxygenation and blood pressure has been associated with a decrease in mortality and disability in patients with severe TBI (Chestnut 1993, Chestnut 1995, Stocheti 1996). Prehospital treatment of patients with severe TBI has been a controversial topic because of the dif iculty to perform appropriate studies in this type of scenario. There is signi icant variability in the type of solutions used in the pre-hospital environment and there are even discussions about the useful-ness or otherwise of the use of resuscitation solutions during the ini-tial care of these patients starting at the accident site (Sampalis 1997, Geeraerts 2007). In Colombia, there is great variability in prehospital
Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 81
care and there are even cases of prolonged transportation of patients with severe TBI when they are from rural areas. There is currently a trend towards the use of hypertonic solutions in patients with severe TBI as these solutions generate a double effect as both a hyperosmolar solution for the reduction of ICP and due to the expansion effect of the intravascular space due to the high concentration of sodium in the spa-ce. For these reasons and because of the great variability that exists in the management of prehospital luids in Colombia, it was considered important to compare the solution most used in our country, Normal Saline (NS) versus that suggested by the recent literature, Hypertonic Saline (HS).
Summary of the evidenceA total of 10 randomized trials on the use of prehospital resuscitation solutions in patients with severe TBI were found (See Annex 6). Only one study met the criteria for the PICO question by comparing sali-ne (7.5%) with NS in adult patients with severe head trauma (Bulger 2010). This study randomized 1331 patients with severe TBI. Com-plete monitoring was performed on 1087 of them for the 6 months fo-llowing discharge. Of these, 302 were included in the group receiving hypertonic saline and dextran, 293 were included in the group of hy-pertonic saline (7.5%) and 492 in the group receiving NS. The charac-teristics of the groups were similar, predominantly type II diffuse inju-ries and mass injuries. More than 58% of the patients in both groups were intubated in prehospital situations and the average transfer time was close to 50 minutes. In total, 650 milliliters of solution were admi-nistered in each of the groups. 40.8% of patients treated with hyperto-nic saline were transferred by air, compared to 37.4% of those treated with NS. The group receiving hypertonic saline, presented levels above 145 meq/l of sodium, a much higher percentage compared to the NS group; these levels remained high, especially in the irst 12 hours. The groups had similar results in terms of mortality and severe disability. The group treated with hypertonic saline (7.5%) had a survival rate of 58.4% and the group treated with NS had a rate of 56.1%. Disability (GOS-E <4) for the hypertonic saline (7.5%) group was 50.1%, and in the NS group this was 47.4%.

Foundation for Medical and Technical Research and Education in Emergencies and Disasters82
From evidence to recommendationDuring the meeting with the working group, it was considered that the balance of desired outcomes (improved survival and disability at 6 months) vs unwanted outcomes (increased mortality or disabili-ty at six months) is equal for the two interventions. Considering the aspect of the availability of hypertonic saline in Colombia (not found commercially) and risks that may occur during preparation (variation in concentrations, contamination of sterile solutions, biological acci-dents with needles, etc) it was considered important to establish a re-commendation for normal saline, as this is available and does not re-quire additional preparations or mixtures with other medications. The working group discussed the speci ic situation of patients with severe penetrating TBI or patients with hypotension and it was considered important to use the same recommendation as good clinical practice, since there are no studies that respond speci ically to this type of pa-tients, comparing normal saline with 7.5% hypertonic solution. Addi-tionally, the only studies made in general trauma patients comparing normal saline (0.9%) and hypertonic solutions (7.5%) or in patients with severe TBI comparing hypertonic saline with Ringer Lactate so-lution, showed no differences between the used solutions.
Structural requirementsIt is considered that to carry out this recommendation, no infrastruc-ture is required in addition to that, which is already available within the Colombian system of social security in health.
Considerations on benefi ts and risksIt is believed that the bene it of implementing the recommendation does not imply any risk associated with the use of the solution, especially sin-ce the recommendation is for the use of a small volume (250ml), which is not associated with the risk of luid overload and/or overhydration in patients.
Considerations on the values and preferences of patientsFor this recommendation in particular, no values or preferences were expressed. The patients and their caregivers expressed a clear prefe-rence for the opportunity to have appropriate prehospital treatment immediately after the injury.
Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 83
Implications on resourcesIt is considered that the bene it of applying the recommendation may be cost effective, given that the cost of an intracranial injury without appropriate treatment can be much greater than the cost of the use of a 250ml bolus of Normal Saline. It is important to bear in mind that there are no economic studies on the implications of this recommen-dation in Colombia.
References1. Gaetz M.Theneurophysiology of brain injury. ClinicalNeurophysiology.
2004;(115)1, 4–183.2. Miller JD, Sweet RC, Narayan R, Becker DP.Early insults to the injured
brain. JAMA. 1978;240(5):439-42.3. Chesnut RM, Marshall LF, Blunt BA, Baldwin N, Eisengberg HM, Jane
JA, et al. The role of secundary brain injury in determining outcome from severe head injury. J Trauma. 1993; 34: 216-222.
4. Chesnut, R.M, Secondary brain insults to the injured brain : clinical perspectivs. New Horiz. 1995; 3: 366-375.
5. Stocchetti N, Furlan A, Volta F.Hypoxemia and arterial hypotension at the accident scene in head injury.J Trauma. 1996;40(5):764-7.
6. Sampalis JS, Denis R, Fréchette P, Brown R, Fleiszer D, Mulder D.Direct transport to tertiary trauma centers versus transfer from lower level facilities: impact on mortality and morbidity among patients with major trauma.J Trauma. 1997;43(2):288-95.
7. Geeraerts T, Friggeri A, Mazoit JX, Benhamou D, Duranteau J, Vigué B.Posttraumatic brain vulnerability to hypoxia-hypotension: the importance of the delay between brain trauma and secondary insult.Intensive Care.2007; 34(3):551-60
8. Bulger EM, May S, Brasel KJ, Schreiber M, Kerby JD, Tisherman SA, et al. Out of hospital hypertonic resuscitation following severe traumatic brain injury: a randomized controlled trial. JAMA. 2010; 304(13): 1455-1464.
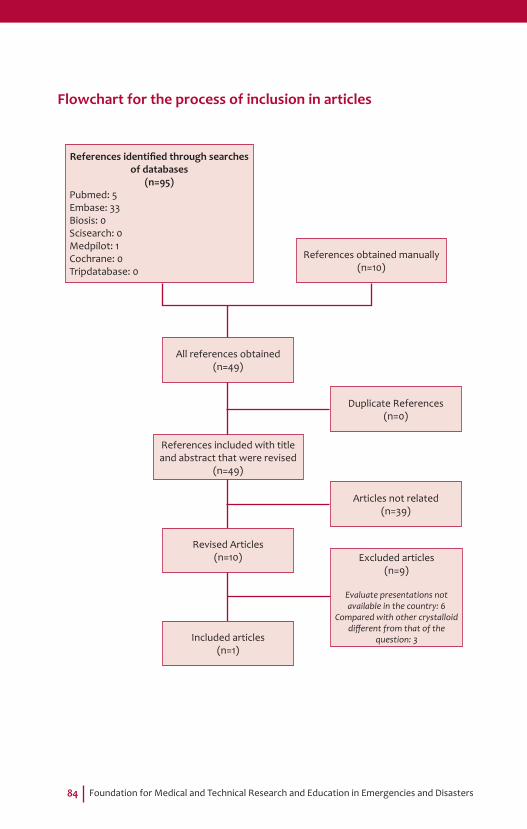
Foundation for Medical and Technical Research and Education in Emergencies and Disasters84
Flowchart for the process of inclusion in articles
References identifi ed through searches of databases
(n=95)Pubmed: 5Embase: 33Biosis: 0Scisearch: 0Medpilot: 1Cochrane: 0Tripdatabase: 0
References obtained manually(n=10)
Duplicate References(n=0)
Articles not related(n=39)
All references obtained(n=49)
References included with title and abstract that were revised
(n=49)
Revised Articles(n=10)
Included articles(n=1)
Excluded articles(n=9)
Evaluate presentations not available in the country: 6
Compared with other crystalloid diff erent from that of the
question: 3

Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 85
Algorithm 3Prehospital Fluids (question 4)
Is ICP decreased?
Adult Patient with severe TBI with intracranial hypertension (IHT) measured with ICP> 20 mmHg
Continue sedation algorithm (see question no. 7,
Sedation)Provide a bolus of 2 cc/kg of
hypertonic saline solution 7.5 % or
mannitol 20%
Continue sedationProvide a second bolus
of hypertonic saline solution 7.5 % or mannitol
20%, 10 minutes after you have completed
the fi rst bolus. Do not use mannitol if SBP <90
mmhg.
Consider hypothermia (see algorithm question No. 10), consider surgery
for cerebral edema before 24 hours (see
algorithm question No. 6)
Provide a bolus of 2 cc/kg of
hypertonic saline solution 7.5 %
Yes
Yes
Yes
Yes
No
No
No
No
SBP>90 mmHg
Is ICPdecreased?
Refractory IHT >25 mmHg by more than
5 minutes

Foundation for Medical and Technical Research and Education in Emergencies and Disasters86
Question 5
In adult patients with severe TBI and intracranial hypertension, does the use of hypertonic saline at 7.5%, compared with mannitol, as a hyperos-molar initial therapy reduce mortality at discharge?
Recommendation
• It is suggested that adult patients with severe TBI and refrac-tory intracranial hypertension (ICP> 25 mmHg for more than 5 minutes, measured with an intracranial pressure measuring device) be treated with a bolus of 2 ml/kg of 7.5% hypertonic saline solution or mannitol at 20%.
Weak recommendation in favor of intervention, moderate quality of evidence.
• If the irst dose is not effective in reducing ICP, a second bolus of 7.5% hypertonic saline solution or mannitol at 20% may be administered 10 minutes after inishing the irst bolus.
Weak recommendation in favor of the intervention, moderate quality of evidence.
• It is considered that adult patients with severe TBI and non-refractory intracranial hypertension (20-25mmHg, measured using an intracranial pressure device) requiring hyperosmolar therapy should be treated with a bolus of 2 cc/kg of 7.5% hy-pertonic saline solution or mannitol at 20%.
Good clinical practice
• It is considered that for the preparation of the 7.5% hypertonic saline solution, a mixture of (40%) 0.9% saline solution plus (60%) ampoules of sodium chloride should be used. To prepare 250cc of the solution, 100cc of normal saline solution and 15 ampoules of sodium chloride (20meq/10ml) would be mixed.
Good clinical practice
• It is considered that the use of mannitol at 20% should be performed only in normotensive patients with systolic blood pressure greater than 90mmHg.
Good clinical practice

Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 87
IntroductionIn patients with severe TBI, between 60% and 70% of patients ap-proximately have abnormalities in the tomography upon admission (concussion, intracerebral, extradural or subdural hematoma and/or signs of cerebral edema). A high percentage of these patients present intracranial hypertension associated with low perfusion of brain tis-sue. One of the medical therapies that have proved to be effective in reducing intracranial pressure (ICP) is the infusion of hyperosmolar solutions (osmotherapy). Two of the most commonly used solutions for osmotherapy are mannitol (20%) and hypertonic saline at various concentrations including 3%, 7.5% and 23.4% preparations. Therefo-re, there is variability in the decision of the solution to be infused and its concentration. Two of the most used solutions both in emergency and intensive care are mannitol and hypertonic saline (7.5%). There-fore, it is necessary to determine whether or not there is a difference in mortality associated with the use of one or another of the solutions.
Summary of the evidenceSix observational studies were analyzed, inding great variability in concentrations of the solutions used; the vast majority of these stu-dies did not assess mortality but physiological changes in monitored parameter values including ICP. The study from Vialet (2003), besides being a randomized controlled study was the only one that precisely answered the PICO question by including only adult patients with se-vere TBI and comparing the two solutions at the concentrations stated in the question. Furthermore, it evaluated mortality and neurological disability as outcomes. In this study, two groups were randomized for treatment of refractory endocranial hypertension by 2 cc/kg hypertonic saline (7.5%) vs 2cc/kg of mannitol (20%). The group treated with hy-pertonic saline presented a better control of intracranial pressure and lower requirement for drainage of cerebrospinal luid (CSF) through a ventriculostomy catheter. Mortality evaluated at 3 months after hospital discharge showed no signi icant difference between the two groups. In the group treated with hypertonic saline (7.5%) it was 40%, and for the group treated with mannitol (20%) it was 50%. There were no differen-ces in electrolyte changes or hemodynamic changes either.

Foundation for Medical and Technical Research and Education in Emergencies and Disasters88
From evidence to recommendationIn the discussion of the working group, the quality of the evidence presented was con irmed and it was considered important to make a suggestion for how to prepare hypertonic saline (7.5%) due to hetero-geneity in its preparation and the scarce availability of its commercial presentation in Colombia. Emphasis was placed on the appropriate hemodynamic status of patient (no hypotension) prior to use of man-nitol as hyper-osmolar therapy. Both interventions were considered low-cost.
Structural requirementsIt is considered that to carry out this recommendation, no infrastructure is required in addition to that already available within the Colombian system of social security in health. Although there is no commercial ver-sion of 7.5% saline, it can be prepared in intensive care units, mixing a solution of 60% normal saline and 40% sodium chloride.
Considerations on benefi ts and risksIt is considered that the bene it of applying the recommendation to either of the two substances outweighs the risk of not correcting an episode of refractory intracranial hypertension, which may be associa-ted with higher mortality and disability rates.
Considerations on the values and preferences of patientsFor this recommendation in particular, no value or preference was expressed.
Implications on resourcesIt is considered that the bene it of applying the recommendation may be cost effective, given that the cost of the complications asso-ciated with refractory intracranial hypertension without appropriate treatment (brain herniation, cerebral infarction, brain death), can be much greater than the cost that may arise from the use of the above solutions. It is important to bear in mind that there are no economic studies on the implications of this recommendation in Colombia.
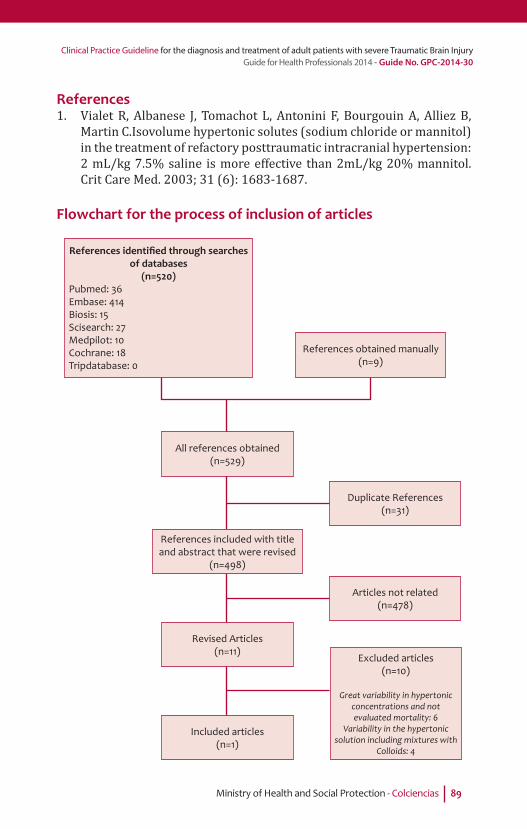
Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 89
References1. Vialet R, Albanese J, Tomachot L, Antonini F, Bourgouin A, Alliez B,
Martin C.Isovolume hypertonic solutes (sodium chloride or mannitol) in the treatment of refactory posttraumatic intracranial hypertension: 2 mL/kg 7.5% saline is more effective than 2mL/kg 20% mannitol.Crit Care Med. 2003; 31 (6): 1683-1687.
Flowchart for the process of inclusion of articles
References identifi ed through searches of databases
(n=520)Pubmed: 36Embase: 414Biosis: 15Scisearch: 27Medpilot: 10Cochrane: 18Tripdatabase: 0
References obtained manually(n=9)
Duplicate References(n=31)
Articles not related(n=478)
All references obtained(n=529)
References included with title and abstract that were revised
(n=498)
Revised Articles(n=11)
Included articles(n=1)
Excluded articles(n=10)
Great variability in hypertonic concentrations and not evaluated mortality: 6
Variability in the hypertonic solution including mixtures with
Colloids: 4
Foundation for Medical and Technical Research and Education in Emergencies and Disasters90
Question 6a
In adult patients with severe TBI and acute subdural hematoma with surgical indication, does early drainage surgery (within 4 hours), com-pared with late surgery (after 4 hours), reduce mortality at discharge?
Recommendation
• It is recommended that surgical treatment be performed in the irst 4 hours post-trauma in patients with severe head trauma
with acute subdural hematoma with surgical indication. Recommendation by strong consensus in favor of the intervention.
IntroductionAcute subdural hematoma is one of the most critical injuries associated with high mortality in patients with severe TBI. It often requires surgi-cal intervention and mortality rates are highly variable but may be as high as 70% depending on the institution where patients arrive. Time-to-surgery has been proposed as one of the prognostic factors given that the presence of this lesion is often associated with the mass effect, which generates a signi icant midline shift and compression of vital structures such as the brainstem. There are currently no treatment guidelines that establish a speci ic time of intervention for these patients in Colombia. Therefore, there is great variability in the time of surgery for patients with severe TBI having a subdural hematoma upon admission and hen-ce the need to respond to this question.
Summary of the evidenceFor this question, eight observational studies were found, none of which responded to the PICO question. Therefore, it was necessary to use a formal consensus of experts. Studies identi ied in the search, but which did not meet all the criteria of the PICO question were sent to all participants. They later attended a two-hour face-to-face meeting. The group was composed of experts working in prehospital care, emergen-cy care, intensive care and neurosurgery services in different regions of the country, both in public and private institutions (Table 10).
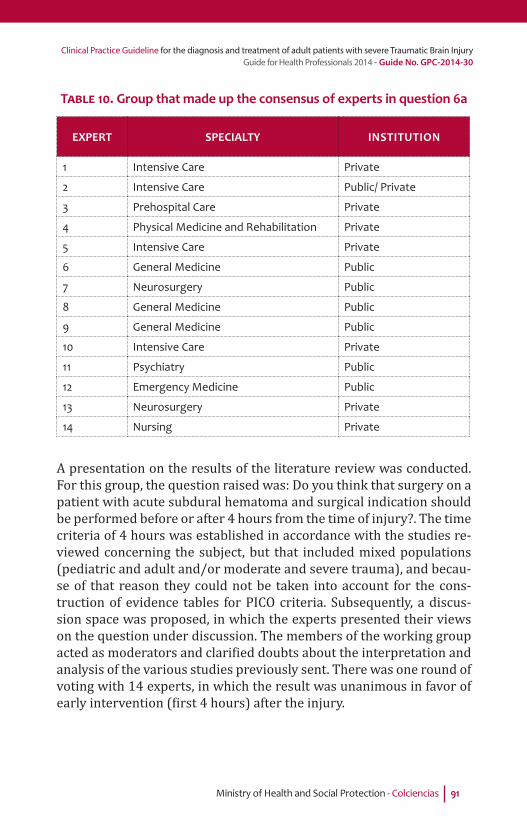
Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 91
TABLE 10. Group that made up the consensus of experts in question 6a
EXPERT SPECIALTY INSTITUTION
1 Intensive Care Private
2 Intensive Care Public/ Private
3 Prehospital Care Private
4 Physical Medicine and Rehabilitation Private
5 Intensive Care Private
6 General Medicine Public
7 Neurosurgery Public
8 General Medicine Public
9 General Medicine Public
10 Intensive Care Private
11 Psychiatry Public
12 Emergency Medicine Public
13 Neurosurgery Private
14 Nursing Private
A presentation on the results of the literature review was conducted. For this group, the question raised was: Do you think that surgery on a patient with acute subdural hematoma and surgical indication should be performed before or after 4 hours from the time of injury?. The time criteria of 4 hours was established in accordance with the studies re-viewed concerning the subject, but that included mixed populations (pediatric and adult and/or moderate and severe trauma), and becau-se of that reason they could not be taken into account for the cons-truction of evidence tables for PICO criteria. Subsequently, a discus-sion space was proposed, in which the experts presented their views on the question under discussion. The members of the working group acted as moderators and clari ied doubts about the interpretation and analysis of the various studies previously sent. There was one round of voting with 14 experts, in which the result was unanimous in favor of early intervention ( irst 4 hours) after the injury.

Foundation for Medical and Technical Research and Education in Emergencies and Disasters92
From evidence to recommendationIt was considered important that this surgical procedure be perfor-med as recommended within the limit of four hours, as this has been considered in many observational studies, and their correlation with outcome shows a clear trend between early intervention and survival. It was also important to consider the opinions given by the patients and their caregivers, who consider early surgery crucial if there are indications for intervention. The most common indications for surgery include: acute subdural hematoma greater than 10mm thick, subdural hematoma causing a midline shift of more than 5 mm, and an acute subdural hematoma causing obliteration of basal cisterns.
Structural requirementsIt is considered that to carry out this recommendation, no infrastructu-re is required in addition to that, which is already available within the Colombian system of social security in health. A neurosurgeon must be available to determine surgical criteria when the patient arrives at the emergency department.
Considerations on benefi ts and risksIt is considered that the bene it of implementing the recommendation of early intervention does not imply risks for the patient, and decrea-ses their risk of disability and mortality associated with the injury.
Considerations on the values and preferences of patientsFor this recommendation in particular, patients and their caregivers emphasized a preference for early intervention, perceiving it as a more effective intervention for improving chances of a better outcome.
Implications on resourcesIt is considered that the bene it of implementing the recommendation may be cost effective, given that the cost of the complications associa-ted with late intervention (brain herniation, cerebral infarction, brain death, etc.), can be much greater than the cost which might be caused by early surgical intervention. It is important to bear in mind that the-re are no economic studies on the implications of this recommenda-tion in Colombia.

Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 93
Flowchart for the process of inclusion of articles
References identifi ed through searches of databases
(n=319)Pubmed: 147Embase: 127Biosis: 1Scisearch: 2Medpilot: 20Cochrane: 21Tripdatabase: 1
References obtained manually(n=8)
Duplicate References(n=23)
Articles not related(n=296)
All references obtained(n=327)
References included with title and abstract that were revised
(n=304)
Revised Articles(n=8)
Included articles(n=0)
The question was answered by expert
consensus
Excluded articles(n=8)
Did not respond exactly the question: 8

Foundation for Medical and Technical Research and Education in Emergencies and Disasters94
Algorithm 4Time-to-surgery (question 6)
*Criteria of indication of surgery for subdural hematoma (SH) in adult patients with severe TBI:
• SH >10 mm of thickness measured at its larger diameter • SH that produces mid line shift > 5 mm • SH that produce compression of the basal cisterns
(perimesencephalic cisterns)
***Criteria of indication of surgery for cerebral edema in adult patients with severe TBI:
• Cerebral edema with mid line shift > 5 mm• Cerebral edema that produces compression of the
basal cisterns (perimesencephalic cisterns)
**Criteria of indication of surgery for epidural hematoma (EH) in adult patients with severe TBI:
• EH volume greater than 30 cc• EH that produces mid line shift >5 mm
§ It is considered that the patients with brain contusions (intracerebral hemorrhage) must be brought to surgery, if they meet the same criteria for surgical indications from cerebral edema or if the volume of the hemorrhage is bigger than 50 cc
It has a subdural
hematoma with surgical indication?
*It
has an epidural
hematoma with surgical indication? **
It has a cerebral edema with surgical
indication? ***
Adult Patient with severe TBI intubated in the emergency room.
CT fi ndings at Emergency Room
Surgical management
should be performed in
the fi rst 4 hours post-trauma
The patient should be taken to surgery
immediately
The patient should be taken to surgery in the fi rst
24 hours
Transfer to ICU § (see
algorithm No. 7, Sedation)
Yes
Yes
Yes No
No
No

Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 95
Question 6b
In adult patients with severe TBI, and an epidural hematoma with sur-gical indication, does early drainage surgery (within 4 hours), compa-red with late surgery (after 4 hours), reduce mortality at discharge?
Recommendation
• It is recommended that patients with severe TBI and an epidu-ral hematoma with surgical indication for drainage be taken to surgery immediately.
Recommendation by strong consensus in favor of the intervention.
IntroductionIt is considered that an epidural hematoma may be present in up to 30% of patients with severe TBI. In these patients, the hematoma is associated in a high percentage of cases with the mass effect, midline shift and compression of vital structures such as the brainstem. Cu-rrently in Colombia there are no management guidelines that esta-blish a speci ic time of intervention for these patients.
Summary of the evidenceFor the answer to this question, ive studies related to surgical mana-gement of acute epidural hematoma were reviewed. None responded exactly to the PICO question. Therefore, it was necessary to use a for-mal consensus of experts. Studies identi ied in the search, but which did not meet all the criteria of the PICO question were sent to all par-ticipants. Subsequently, they attended a face-to-face meeting lasting two hours. The group was composed of experts working in prehos-pital care, emergency departments, intensive care and neurosurgery services in different regions of the country, both in public and private institutions (Table 11).
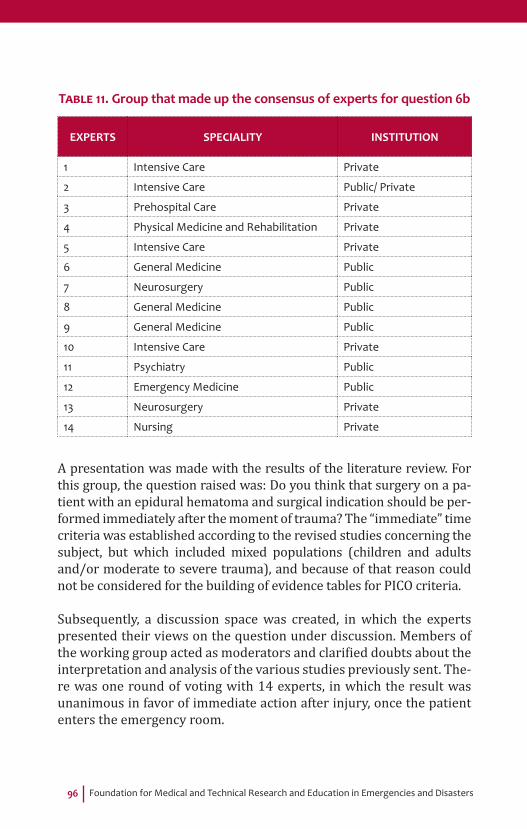
Foundation for Medical and Technical Research and Education in Emergencies and Disasters96
TABLE 11. Group that made up the consensus of experts for question 6b
EXPERTS SPECIALITY INSTITUTION
1 Intensive Care Private
2 Intensive Care Public/ Private
3 Prehospital Care Private
4 Physical Medicine and Rehabilitation Private
5 Intensive Care Private
6 General Medicine Public
7 Neurosurgery Public
8 General Medicine Public
9 General Medicine Public
10 Intensive Care Private
11 Psychiatry Public
12 Emergency Medicine Public
13 Neurosurgery Private
14 Nursing Private
A presentation was made with the results of the literature review. For this group, the question raised was: Do you think that surgery on a pa-tient with an epidural hematoma and surgical indication should be per-formed immediately after the moment of trauma? The “immediate” time criteria was established according to the revised studies concerning the subject, but which included mixed populations (children and adults and/or moderate to severe trauma), and because of that reason could not be considered for the building of evidence tables for PICO criteria.
Subsequently, a discussion space was created, in which the experts presented their views on the question under discussion. Members of the working group acted as moderators and clari ied doubts about the interpretation and analysis of the various studies previously sent. The-re was one round of voting with 14 experts, in which the result was unanimous in favor of immediate action after injury, once the patient enters the emergency room.
Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 97
From evidence to recommendationIt was considered important that this surgical procedure be performed as recommended, since in many observational studies a clear trend between early intervention and survival is evident. This was also in line with the views of patients and their caregivers, who consider early surgery crucial if there are indications for intervention. The most fre-quent indications for surgery include: an epidural hematoma greater than 30cc, an epidural hematoma that causes a midline shift of more than 5 mm, and an epidural hematoma causing obliteration of basal cisterns.
Structural requirementsIt is considered that to carry out this recommendation, no infrastructu-re is required in addition to that, which is already available within the Colombian system of social security in health. A neurosurgeon must be available to determine the criteria for surgery when the patient arrives at the emergency department.
Considerations on benefi ts and risksIt is considered that the bene it of applying the recommendation of immediate action does not involve risks to patients, and decreases di-sability and mortality rates associated with the injury.
Considerations on the values and preferences of patientsFor this recommendation in particular, patients and their caregivers emphasized a preference for early intervention, perceiving it as more effective at improving chances of a better outcome.
Implications on resourcesIt is considered that the bene it of implementing the recommendation may be cost effective, given that the cost of the complications associa-ted with late intervention (brain herniation, cerebral infarction, brain death, etc.), can be much greater than the cost which might arise from early surgical intervention. It is imperative to keep in mind that there are no economic studies on the implications of this recommendation in Colombia.

Foundation for Medical and Technical Research and Education in Emergencies and Disasters98
Flowchart for the process of inclusion in articles
References identifi ed through searches of databases
(n=323)Pubmed: 147Embase: 127Biosis: 1Scisearch: 2Medpilot: 20Cochrane: 21Tripdatabase: 5
References obtained manually(n=5)
Duplicate References(n=23)
Articles not related(n=300)
All references obtained(n=328)
References included with title and abstract that were revised
(n=305)
Revised Articles(n=5)
Included articles(n=0)
The question was answered by expert
consensus
Excluded articles(n=5)
Did not respond exactly the question: 8

Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 99
Algorithm 4Time-to-surgery (question 6)
*Criteria of indication of surgery for subdural hematoma (SH) in adult patients with severe TBI:
• SH >10 mm of thickness measured at its larger diameter • SH that produces mid line shift > 5 mm • SH that produce compression of the basal cisterns
(perimesencephalic cisterns)
***Criteria of indication of surgery for cerebral edema in adult patients with severe TBI:
• Cerebral edema with mid line shift > 5 mm• Cerebral edema that produces compression of the
basal cisterns (perimesencephalic cisterns)
**Criteria of indication of surgery for epidural hematoma (EH) in adult patients with severe TBI:
• EH volume greater than 30 cc• EH that produces mid line shift >5 mm
§ It is considered that the patients with brain contusions (intracerebral hemorrhage) must be brought to surgery, if they meet the same criteria for surgical indications from cerebral edema or if the volume of the hemorrhage is bigger than 50 cc
It has a subdural
hematoma with surgical indication?
*It
has an epidural
hematoma with surgical indication? **
It has a cerebral edema with surgical
indication? ***
Adult Patient with severe TBI intubated in the emergency room.
CT fi ndings at Emergency Room
Surgical management
should be performed in
the fi rst 4 hours post-trauma
The patient should be taken to surgery
immediately
The patient should be taken to surgery in the fi rst
24 hours
Transfer to ICU § (see
algorithm No. 7, Sedation)
Yes
Yes
Yes No
No
No
Foundation for Medical and Technical Research and Education in Emergencies and Disasters100
Question 6c
In adult patients with severe TBI and surgical indication for cerebral edema, does early decompression craniectomy (within 24 hours), compared with late craniectomy (after 24 hours), reduce mortality at discharge?
Recommendation
• It is suggested that patients with severe TBI and surgical indi-cation for cerebral edema be taken to surgery within 24 hours.
Weak recommendation in favor of the intervention, low qua-lity of evidence.
IntroductionIn patients with severe TBI, approximately 60 to 70% of cases present abnormalities in tomography at admission (concussion, intracerebral, extradural or subdural hematoma and/or signs of cerebral edema). Ap-proximately two thirds of these patients with imaging abnormalities present intracranial hypertension unresponsive to medical treatment (refractory intracranial hypertension) (Narayan 1982, Little 1998, Wardlaw 2002). The sustained elevated ICP is clearly correlated with increased mortality and increased functional sequelae after severe TBI (Vik 2008). Cranial decompression is an effective procedure to reduce ICP associated with severe TBI. The time to perform this surgery has been proposed as one of the predictors, but currently there are no ma-nagement guidelines that allow a speci ic time for this intervention to be established. Therefore, there is variability in the time elapsed from the moment of trauma to decompression surgery in patients with severe TBI who have indications for the procedure. This is why there is a need to answer this question.
Summary of the evidenceIn total, ive observational studies were analyzed. The table of eviden-ce was constructed for the sole observational study that responded exactly to the PICO question in terms of the population included and the measured results (Cianchi 2012). In this study, 186 patients with

Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 101
severe TBI admitted to the ICU of a tertiary hospital were analyzed. The patients were divided in 2 groups de ined as early decompression (within 24 hours) and late (after 24 hours). There was also a control group of patients with intracranial hypertension who were managed medically. 41 patients were included in the irst group, 21 in the se-cond and 124 in the control group. These patients were analyzed using the GOS scale at 6 months post-injury inding a mortality rate of 48.8% in early surgery patients and 42.2% of patients with late surgery. Di-sability at 6 months showed an average of 3.3 on the GOS in the early group and 3.0 in the late intervention group. This describes more mar-ked disability in the late intervention group.
From evidence to recommendationDuring the discussion with the working group, it was decided to give a weak recommendation for intervention because the balance bet-ween desired outcomes (reduced disability and increased survival at 6 months) vs unwanted (increased disability and higher mortality at 6 months) is low in favor of the irst outcome. It was considered im-portant, taking into account aspects of patient safety, that this surgi-cal procedure should be performed as recommended in the eviden-ce and that the limit of 24 hours should be considered the maximum time allowed to perform the procedure. The most widely used surgical criteria, which were found to be appropriate, include: cerebral edema with midline shift greater than 5mm, and cerebral edema that causes compression of the basal cisterns.
Structural requirementsIt is considered that to carry out this recommendation, no infrastructu-re is required in addition to that, which is already available within the Colombian system of social security in health. A neurosurgeon must be available to determine the criteria for surgery when the patient arrives at the emergency department.
Considerations on benefi ts and risksIt is considered that the bene it of applying the recommendation of immediate action does not involve risks to patients, and decreases di-sability and mortality rates associated with the injury.

Foundation for Medical and Technical Research and Education in Emergencies and Disasters102
Considerations on the values and preferences of patientsFor this recommendation in particular, patients and their caregivers emphasized a preference for early intervention, perceiving it as more effective at improving chances of a better outcome.
Implications on resourcesIt is considered that the bene it of applying the recommendation may be cost effective, given that the cost of the complications associated with late intervention (brain herniation, cerebral infarction, brain death, etc.), can be much greater than the cost which might arise from early surgical intervention. It is imperative to bear in mind that there are no economic studies on the implications of this recommendation in Colombia.
References1. Narayan R K, Kishore P R, Becker DP, Ward JD, Enas GG, Greenberg,
et al. Intracranial pressure: to monitor or not to monitor? A review of our experience with severe head injury . Journal of neurosurgery. 1982; 56(5): 650-659.
2. Poca MA, Sahuquillo J, Baguena M, Pedraza S, Gracia RM, Rubio E. Incidence of intracranial hypertension after severe head injury: a prospective study using the Traumatic Coma Data Bank classi ication. In: Intracranial Pressure and Neuromonitoring in Brain Injury. Springer Vienna. 1998: 27-30.
3. Wardlaw, J. M., Easton, V. J., & Statham, P. Which CT features help predict outcome after head injury? Journal of Neurology, Neurosurgery & Psychiatry.2002; 72(2): 188-192.
4. Vik A, Nag T, Fredriksli OA, Skandsen T, Moen KG., Schirmer-Mikalsen K, Manley GT. Relationship of “dose” of intracranial hypertension to outcome in severe traumatic brain injury. J of Neurosurgery 2008: 109; 678-684.
5. Cianchi G, Bonizzoli M, Zagli G, Valvasone S, Ciapetti M, Perreta L, Mariotti F, Peris A. Late decompressivecraniectomy traumatic brain injury: neurological outcome at 6 months after ICU discharge. J Trauma. 2012; 6 (8): 1-6.

Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 103
Flowchart for the process of inclusion in articles
References identifi ed through searches of databases
(n=325)Pubmed: 147Embase: 127Biosis: 1Scisearch: 2Medpilot: 20Cochrane: 21Tripdatabase: 7
References obtained manually(n=5)
Duplicate References(n=23)
Articles not related(n=302)
All references obtained(n=330)
References included with title and abstract that were revised
(n=307)
Revised Articles(n=5)
Included articles(n=1)
Excluded articles(n=4)
Did not respond exactly the question: 8

Foundation for Medical and Technical Research and Education in Emergencies and Disasters104
Algorithm 4Time-to-surgery (question 6)
*Criteria of indication of surgery for subdural hematoma (SH) in adult patients with severe TBI:
• SH >10 mm of thickness measured at its larger diameter • SH that produces mid line shift > 5 mm • SH that produce compression of the basal cisterns
(perimesencephalic cisterns)
***Criteria of indication of surgery for cerebral edema in adult patients with severe TBI:
• Cerebral edema with mid line shift > 5 mm• Cerebral edema that produces compression of the
basal cisterns (perimesencephalic cisterns)
**Criteria of indication of surgery for epidural hematoma (EH) in adult patients with severe TBI:
• EH volume greater than 30 cc• EH that produces mid line shift >5 mm
§ It is considered that the patients with brain contusions (intracerebral hemorrhage) must be brought to surgery, if they meet the same criteria for surgical indications from cerebral edema or if the volume of the hemorrhage is bigger than 50 cc
It has a subdural
hematoma with surgical indication?
*It
has an epidural
hematoma with surgical indication? **
It has a cerebral edema with surgical
indication? ***
Adult Patient with severe TBI intubated in the emergency room.
CT fi ndings at Emergency Room
Surgical management
should be performed in
the fi rst 4 hours post-trauma
The patient should be taken to surgery
immediately
The patient should be taken to surgery in the fi rst
24 hours
Transfer to ICU § (see
algorithm No. 7, Sedation)
Yes
Yes
Yes No
No
No
Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 105
Question 7
In adult patients with severe TBI being treated in an ICU, does sedation with propofol, compared to sedation using Midazolam, reduce neuro-logical disability or mortality, assessed at 3 months post-injury?
Recommendation
• It is suggested that adult patients with severe TBI be sedated during their stay in the ICU using midazolam. Doses of 0.1-0.3 mg/kg/h are suggested.1
Weak recommendation in favor of the intervention, moderate quality of evidence
• As a second choice after midazolam, propofol 1% can be used at a dose of 1.5 to 5 mg/kg/h1.
Weak recommendation in favor of the intervention, moderate quality of evidence
• It is suggested that a triglyceride measurement be perfor-med on patients sedated with propofol 1% within the irst 24 hours. If the initial sample of triglycerides is lower than 350 mg/dl, periodic checks should be performed every 72 hours. If the value is greater than 350 mg/dl, repeat the sample within 24 hours. If the second sample is also above 350 mg/dl, treatment should be discontinued immediately. Patients should be closely monitored for the possible occurrence of propofol infusion syndrome (hyperkalemia, metabolic aci-dosis, cardiac arrhythmia, cardiovascular collapse and multi-organ failure).
Weak recommendation in favor of the intervention, moderate quality of evidence
• Patients should be closely monitored for the possible occu-rrence of propofol infusion syndrome (hyperkalemia, meta-bolic acidosis, cardiac arrhythmia, cardiovascular collapse and multi-organ failure).
Good clinical practice.
1 The use of the Richmond Agitation-Sedation Scale (RASS) for the evaluation and control of sedation is suggested because it is the most widely used scale.

Foundation for Medical and Technical Research and Education in Emergencies and Disasters106
IntroductionPatients with severe TBI typically require sedative regimes for acute treatment with the aim of decreasing cerebral metabolic consumption, preventing episodes of agitation during mechanical ventilation and also as an anxiolytic effect during intensive care stay. Decreased intra-cranial pressure and improvement of cerebral perfusion pressure have been reported as bene icial effects of the use of these agents but some adverse effects, including hypotension and metabolic alterations, have also been reported. Different drugs have been used in these patients but currently there is signi icant variability in the protocols and re-commendations established in intensive care units. In Colombia, two of the most commonly used drugs are midazolam and propofol, which have pharmacodynamic and pharmacokinetic properties that produ-ce an appropriate response in the management of these patients. In Colombia benzodiazepines, and especially midazolam, are highly used due to their availability and cost. Internationally, it has been suggested that propofol is a more effective sedative and that it produces fewer adverse effects in patients with TBI. It is therefore necessary to deter-mine whether there is a difference in mortality and neurologic disabi-lity depending on which sedative is used.
Summary of the evidenceA total of three randomized controlled trials were evaluated (see an-nex 6). One of them (Ghori 2007) met the criteria of population, in-tervention and results formulated in the PICO question, so the table of evidence was constructed based on this study. The study randomi-zed 28 adult patients with severe TBI, of them, 15 received midazolam and 13 received propofol. This study found no differences between the use of midazolam or propofol as sedatives in the treatment of patients with severe TBI from the point of view of the neurological outcome, measured with the GOS at 3 months after hospital discharge. In the group of Midazolam, there was an outcome of GOS 4-5 (good neurolo-gical outcome) in 53.3% of cases, while for the Propofol group this was 53.8%. The study also analyzed plasma concentrations of neurological injury markers (S100 protein and nitric oxide) in the irst 5 days of hospitalization in the ICU and likewise there were no differences in the levels of these markers when comparing the two sedatives. Since the use of propofol has been associated with alterations in lipid me-tabolism, it was considered important to evaluate studies comparing metabolic complications associated with the use of the two drugs.

Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 107
Two randomized controlled clinical studies (Sanchez-Izquierdo 1998; Sandiumengue 2000) on populations of clinically ill trauma patients were reviewed. No such studies were found from populations speci-ically with severe TBI. The study by Sanchez-Izquierdo was used for
the table of evidence, as it included the analysis of a subpopulation of patients with severe TBI. This study compared the use of propofol 1% with midazolam in 150 patients who were divided into three groups with an average of 30% of patients with TBI in each group. The group of patients treated with propofol showed an increase in triglyceride levels, especially in patients treated for more than 72 hours, and grea-ter therapeutic failure associated to this cause (therapeutic failure was de ined as being when doses higher than 6 mg/kg/ho were required or if triglyceride levels increased above 350 mg/dl on two consecutive measurements within 24 hours or if there was one measurement grea-ter than 500 mg/dL).
From evidence to recommendationDuring the discussion with the working group, the grading of the qua-lity of evidence was con irmed. Both proposals for intervention were considered, considering them inexpensive, and furthermore there was no discussion regarding availability in the domestic environment. The most discussed aspects were regarding safety in the use of Propofol, as the evidence obtained in the analysis of studies of metabolic complica-tions when comparing the two drugs (in which hypertriglyceridemia was a cause for stopping use of the medication) showed a therapeutic failure of propofol, after which another sedative was required to con-tinue treating patients. The group of experts also discussed the impli-cations of propofol infusion syndrome, associated with hyperkalemia, arrhythmia and cardiovascular collapse, which, although not analyzed in the reviewed studies, has been described and is considered impor-tant by the group of experts. The last two points were taken into ac-count when making the recommendation, in which the working group considered Midazolam as a irst option as it is not associated with al-tered triglyceride levels or a risk of cardiovascular alterations induced by its infusion. The group also considered it important to use a scale for assessing the depth of sedation. This scale is the Richmond Agi-tation Sedation Scale, which is the scale that is most widely used in a standardized way for this purpose.
Foundation for Medical and Technical Research and Education in Emergencies and Disasters108
Structural requirementsIt is considered that to carry out this recommendation, no infrastruc-ture is required in addition to that, which is already available within the Colombian system of social security in health. Staff trained in the use of the Richmond Agitation Sedation Scale must be available to eva-luate depth of sedation.
Considerations on benefi ts and risksIt is considered that the bene it of applying the recommendation on the use of sedatives outweighs the risk caused by their adverse effects. Special precaution must be taken with monitoring of the adverse effects of propofol, given that the presence of hyperkalemia can be as-sociated with cardiac complications.
Considerations on the values and preferences of patientsFor this recommendation in particular, patients and their caregivers did not state any preference that would modify the recommendation.
Implications on resourcesIt is considered that the bene it of applying the recommendation may be cost effective, given that the cost of the complications associated with not using sedatives in patients with brain injuries during the acu-te treatment of intracranial hypertension can be much greater than the cost that might arise from their use. It is important to have in mind that there are no economic studies on the implications of this recom-mendation in Colombia.
References1. Ghori KA, Harmon DC, Elashaal A, Butler M, Walsh M, O’Sulliuvan
MGJ, Shorten DG, Effect of midazolam versus proporfol sedation on markers of neurological injury and outcome after severe head injury: a pilot study. Crit Care & Resuscitation. 2007; 9(2):166-171.
2. Sanchez-Izquierdo JA, Caballero CRE, Perez VJL, Ambros CA, Cantalapiedra SJA, Alted LE, Propofol versus midazolam: Safety and ef icacy for sedating the severe trauma patient. Crit Care & Trauma.1998;86: 1219-1224.
3. Sandiumenge CA, Sanchez-Izquierdo, RJA, Vazquez DT, Borges MS, Peinado R J, AtedLE.Midazolam and 2% proporfol in long-term
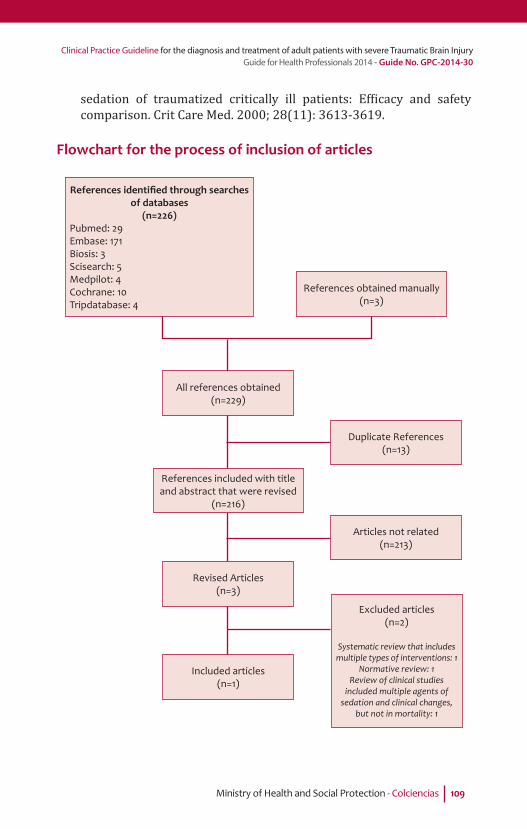
Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 109
sedation of traumatized critically ill patients: Ef icacy and safety comparison. Crit Care Med. 2000; 28(11): 3613-3619.
Flowchart for the process of inclusion of articles
References identifi ed through searches of databases
(n=226)Pubmed: 29Embase: 171Biosis: 3Scisearch: 5Medpilot: 4Cochrane: 10Tripdatabase: 4
References obtained manually(n=3)
Duplicate References(n=13)
Articles not related(n=213)
All references obtained(n=229)
References included with title and abstract that were revised
(n=216)
Revised Articles(n=3)
Included articles(n=1)
Excluded articles(n=2)
Systematic review that includes multiple types of interventions: 1
Normative review: 1Review of clinical studies
included multiple agents of sedation and clinical changes,
but not in mortality: 1

Foundation for Medical and Technical Research and Education in Emergencies and Disasters110
Algorithm 5Sedation (question 7)
Adult Patient with severe TBI in ICU
Start sedation with midazolam dose of 0.1 - 0.3 mg/kg/h or propofol 1% at dosis of 1.5 to 5 mg/
kg/h
In the event that management has been started with propofol perform measurement of
triglycerides (TGC) in the fi rst 24 hours
Repeat sample before 24 hours
Discard propofol and start midazolam
Continue ICU management (see algorithm question No.
9, Monitoring of ICP)
Perform control of TGC in 72 hours
Yes
Yes
No
No
TGC > 350 mg/dl
TGC > 350 mg/dl

Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 111
Question 8
In adult patients with severe TBI treated in an ICU, does thrombo-pro-phylaxis with low molecular weight heparin (LMWH), compared with thrombo-prophylaxis with unfractionated heparin, reduce the presen-ce of thrombotic events and mortality at discharge?
Recommendation
• It is recommended that adult patients with severe TBI receive antithrombotic prophylaxis with low molecular weight hepa-rin (enoxaparin). The suggested dose is 30mg/SC/day.
Weak recommendation for intervention, low quality of evidence.
• The recommendation is to start antithrombotic therapy as soon as possible; as long as the patient is not receiving trans-fusions, is stable in the neurological examination (no reduc-tion in GCS) and that the CT scan shows evidence that the bleeding is controlled (no expansion in the area of bleeding).
Weak recommendation for intervention, low quality of evidence
• Start pneumatic compression stockings in patients with seve-re TBI immediately after admission to the ICU.
Good clinical practice.
IntroductionDeep vein thrombosis is a clinical picture particularly associated with patients who have a prolonged stay in an ICU. Patients with severe TBI are generally treated in these units for long periods of time. The asso-ciation between severe TBI and deep vein thrombosis has been repor-ted on different occasions and can reach igures as high as 50% of the patients, including other complications such as the formation of a pul-monary embolus (Geerts 1994). The pulmonary embolisms, including smaller ones, are associated with important events of hypoxia and desaturation, which have been clearly associated with increased early mortality in patients with severe TBI (Chesnut 1993). The use of diffe-rent strategies to prevent thrombotic events in these patients has been proposed. Two of the most commonly used methods in Colombia are thromboprophylaxis with Low Molecular Weight Heparins (LMWH) and thromboprophylaxis with unfractionated heparin. Complications

Foundation for Medical and Technical Research and Education in Emergencies and Disasters112
such as intracerebral bleeding associated with the treatment have been described in both interventions. There is no consensus on the use of these drugs and therefore there is signi icant variability. The-refore there is a need to determine whether in patients with severe TBI, thromboprophylaxis with low molecular weight heparin versus unfractionated heparin reduces the occurrence of thrombotic events and mortality.
Summary of the evidenceAn observational study (Minshall 2011) of 386 patients with severe TBI, determined by a head abbreviated injury scale score> 3, analyzed and compared 158 patients treated with low molecular weight heparin with 171 patients treated with unfractionated heparin. It was the only study that met the inclusion criteria of the PICO question. The dose of enoxa-parin used was 30 mg subcutaneous twice daily and the dose of low molecular weight heparin was 5000 units subcutaneously three times a day. The mean time for starting therapy was 47 hours in patients with enoxaparin and 54 hours in patients receiving heparin. Mortality and thrombotic complications were higher in the group of unfractionated heparin, with a mortality assessed at discharge of 15.8% in this group, compared with a mortality of 5.1% in the group of low molecular weight heparin. Deep vein thrombosis occurred in 1.2% of the unfractionated heparin group and 0.6% in the group of low molecular weight heparin. The presence of pulmonary thromboembolism was 4.1% for the UFH group and 0% in the group receiving LMWH. Similarly, progression of intracerebral hemorrhage was greater in the second group.
From evidence to recommendationIn the group discussion, it was felt that there should be a weak recom-mendation to support the use of low molecular weight heparin (enoxa-parin) because the balance between desired outcomes (lower morta-lity and fewer thrombotic and thromboembolic events) vs unwanted (progression of intracerebral bleeding) is high in favor of enoxaparin but the quality of evidence is low. There was agreement on the avai-lability in our environment of the medication evaluated in the study. It was insisted that aspects related to safety (time of starting therapy and absence of active bleeding) were included and the group of ex-perts considered it important to suggest a lower dose than that used in the study (30mg/24h vs 60mg /24h), taking into account that the

Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 113
average weight of the North American population is higher than that of the Colombian population.
Structural requirementsIt is considered that to carry out this recommendation, no infrastruc-ture is required in addition to that, which is already available within the Colombian system of social security in health.
Considerations on benefi ts and risksIt is considered that the bene it of implementing the recommendation on the use of low molecular weight heparin outweighs the risk caused by their adverse effects. It is important to consider the criteria for the recommendation of starting time, especially after taking a control scan of the head.
Considerations on the values and preferences of patientsFor this recommendation in particular, patients and their caregivers did not state any preference that would modify the recommendation.
Implications on resourcesIt is considered that the bene it of applying the recommendation may be cost effective, given that the cost of the complications associated with not using thromboprophylaxis in patients with brain injuries can be much greater than the cost that might arise from their use. It is impor-tant to keep in mind that in Colombia there are no economic studies on the implications of this recommendation.
References1. Geerts W, Jay R, CodeK CE, SzalaiJ. A prospective study of venous
tromboembolism after major trauma. NEJM. 1994; 331(24): 1601-1606.
2. Chesnut RM, Marshall LF, Blunt BA, Baldwin N, Eisengberg HM, Jane JA, et al. The role of secundary brain injury in determining outcome from severe head injury. J Trauma. 1993; 34: 216-222.
3. Minshall CT, Erockson EA, Leon MS, Doben AR, Mckinzie BP, Fakhry SM. Safety and Ef icacy of heparin or enoxaparin prophylaxis in blunt trauma patients whit a head abbreviated injury severity score >2. J Trauma.2011; 71 (2): 396-400.

Foundation for Medical and Technical Research and Education in Emergencies and Disasters114
Flowchart for the process of inclusion in articles
References identifi ed through searches of databases
(n=190)Pubmed: 63Embase: 86Biosis: 4Scisearch: 6Medpilot: 5Cochrane: 24Tripdatabase: 2
References obtained manually(n=6)
Duplicate References (n=30)
Articles not related(n=160)
All references obtained(n=196)
References included with title and abstract that were revised
(n=166)
Revised Articles (n=6)
Included articles (n=1)
Excluded articles(n=5)
Not compared measurement of start times of
thromboprophylaxis, and the outcome did not correspond to
the question PICO: 5
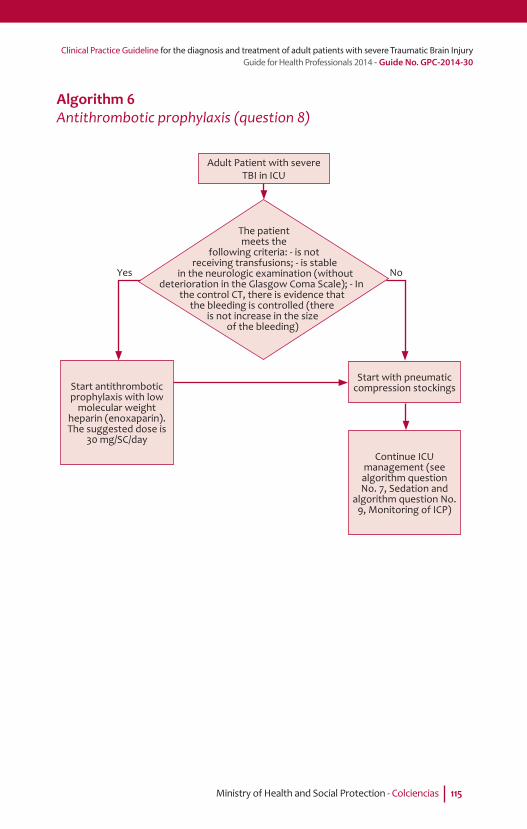
Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 115
Algorithm 6Antithrombotic prophylaxis (question 8)
The patient meets the
following criteria: - is not receiving transfusions; - is stable
in the neurologic examination (without deterioration in the Glasgow Coma Scale); - In
the control CT, there is evidence that the bleeding is controlled (there
is not increase in the size of the bleeding)
Adult Patient with severe TBI in ICU
Start antithrombotic prophylaxis with low
molecular weight heparin (enoxaparin). The suggested dose is
30 mg/SC/day
Start with pneumatic compression stockings
Continue ICU management (see algorithm question No. 7, Sedation and
algorithm question No. 9, Monitoring of ICP)
Yes No
Foundation for Medical and Technical Research and Education in Emergencies and Disasters116
Question 9
In adult patients with severe TBI being treated in an ICU, does guided therapy with monitoring of intracranial pressure (ICP), compared with treatment without ICP monitoring, reduce mortality at discharge?
Recommendation
• It is suggested that adult patients with severe TBI need to be monitored with intracranial pressure measurement devices when they meet the following criteria: Glasgow Coma Scale greater than or equal to 3 and less than or equal to 8 after re-suscitation and an abnormal CT (hematoma, contussion, ede-ma, herniation or compression of basal cisterns).
Weak recommendation in favor of intervention, very low qua-lity of evidence.
• It is suggested that treatment of intracranial hypertension be initiated when the value measured in the patient is greater than 20mmHg in a single measurement.
Weak recommendation in favor of intervention, Very low qua-lity of evidence.
IntroductionAfter severe TBI, patients can suffer alterations that lead to increases in ICP. These increases may be due to accumulation of blood in the epi-dural or subdural space, at intracerebral level and/or due to in lam-mation of the brain tissue. This increased pressure may be temporarily offset by the mobilization of cerebrospinal luid from the cranial com-ponent to the spinal space or by decreasing the volume of intracere-bral venous blood. When these mechanisms are exhausted, internal displacement of brain tissue (cerebral herniation or cerebellar) be-gins. This may cause death due to the compression of critical structu-res, especially in the brain stem. The increase in ICP occurs in the irst hours and its duration may vary depending on the type of injury that
Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 117
is causing it. Therefore, in patients with severe TBI, monitoring of ICP is considered an important tool in the acute care of patients. Several studies that have attempted to examine the relationship between the monitoring of ICP and functional outcome in patients have presented inconsistent results. A great majority of these studies were observatio-nal and the few clinical studies have biases that lower methodological quality. For this reason, it was considered important to perform this question for clinical practice guidelines in Colombia.
Summary of the evidenceA total of 11 studies were analyzed to answer the question, of which 10 were observational (Marmarou 1991, Lane 2000, Stiefel 2005, Bales-treri 2006, Mauritz 2008, Farahvar 2012, Barmparas 2012, Thompson 2008, Sha i 2008 and Alali 2007) and one was a randomized clinical study (Chesnut, 2012). The latter study was not included due to ha-ving a population below the stated range for this guideline (+15). The 2 studies selected to answer the question of the guide, despite being observational studies, strictly met the criteria of population, interven-tion and outcomes (mortality) established in the PICO question. The irst study (Sha i 2008) analyzed 1,646 patients over 20 years old with
severe TBI of whom 708 received ICP monitoring and 938 did not. The two groups were compared and it was found that there was improved survival in the group of patients that was not monitored. Mortality in the group whose ICP was monitored was 27.7%, and mortality in the non-monitored group was 11.9%. However, the group of monitored patients had a higher abbreviated injury scale score, having suffered more severe head injuries, which can clearly in luence the outcome. In the second study (Alali 2007) 10,628 adult patients in 155 trauma centers in the United States and Canada were analyzed. It was found that the institutions that monitored ICP had lower mortality rates at hospital discharge. A total of 1,874 patients were monitored and 8,754 were treated without monitoring. In this study, ICP monitoring was associated with lower mortality. Mortality in the monitored group of patients was 32% and mortality in the group of unmonitored patients was 36.2%.
Foundation for Medical and Technical Research and Education in Emergencies and Disasters118
From evidence to recommendationThe working group decided to give a weak recommendation for inter-vention, taking into account that the balance between desired outco-mes (reduction in mortality at discharge) versus unwanted results (intracerebral hemorrhage or infection of the central nervous system, during the procedure) wasa small in favor of the irst. Additionally, con idence in the magnitude of the estimated effect of the intervention on the important outcome (survival) is also low. Although both stu-dies showed different results, the group discussed the heterogeneity in practice and safety aspects, especially post-insertion treatment in the ICU. The importance of understanding the monitoring process as a marker of treatment intensity was discussed, because this monitoring integrates clinical monitoring and imaging with additional physiolo-gical data, enabling more aggressive and early medical or surgical in-terventions. Findings from CT scans that should be taken into account as indicators for ICP monitoring, were added to the recommendation.
Structural requirementsIt is considered that to carry out this recommendation, no infrastruc-ture is required in addition to that, which is already available within the Colombian system of social security in health. Current standards for the provision of intensive care units establish what is necessary for the monitoring of invasive pressure, and intracranial pressure monito-ring is established as one of the priority processes for intensive care units for adults. This measurement is usually performed in specialized centers that are referral centers for lower-level institutions. Given that care centers with emphasis on trauma are centers of high specializa-tion (see recommendation question 2), the necessary resources for ICP monitoring (including equipment, devices, supplies and trained human talent for the measurement and interpretation of monitoring data) must be available at these centers to provide comprehensive ma-nagement of adult patients with severe TBI.
Considerations on benefi ts and risksIt is considered that the bene it of implementing ICP monitoring (early identi ication of patients that require more aggressive medi-cal or surgical procedures and the evaluation of response to medical
Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 119
and/or surgical treatments) outweighs the risk caused by the inser-tion of the device (intracerebral bleeding and/or infection).
Considerations on the values and preferences of patientsFor this recommendation in particular, patients and their caregivers did not state any preference that would modify the recommendation.
Implications on resourcesIt is considered that the bene it of applying the recommendation may be cost effective, given that the cost of the complications associated with not using neuromonitoring devices in patients with brain injuries du-ring acute treatment of intracranial hypertension can be much greater than the cost that might arise from their use. It is important to bear in mind that in Colombia there are no economic studies on the implica-tions of this recommendation.
References1. Marmarou A, Anderson R L, Ward D, Choi SC, Young HF. Impact of ICP
instability and hypotension on outcome in patients with severe head trauma. J Neurosurg. 1991; 75: 1-8.
2. Lane P, Skoretz TG, Doig G, Girotti. Intracranial pressure monitoring and outcomes after traumatic brain injury. CMA.2000; 43 (6): 442-448.
3. Stiefel M, Spiota A, Gracias VH, Garuffe AM, Guillamondegui O, Wilensky EM, Et al. Reduced mortality rate in patients whit severe traumatic brain injury treated whit brain tissue oxygen monitoring. J of Neurosurg. 2005; 103: 805-811.
4. Balestreri, M., Czosnyka,M., Hutchinson, P., Steiner, L.A., Hiler, M., Smielewski, P., Pickard, D., (2006). Impact of intracranial pressure and cerebral perfusion pressure on severe disability and mortality after head injury. Neurocritical Care. 2006; 04:8–13.
5. MauritzW, stelzer H, Bauer P, Aghamanoukjan DL, Metnitz P. Monitoring of intracranial pressure in patients with severe traumatic brain injury: an Austrian prospective multicenter study. Intensive Care Med. 2008; 34: 1208-1215.
6. Farahvar A, Gerber LM, Chiu YL, Carney N, Hartl R, Ghajar J. Increased mortality in patients with severe traumatic brain injury treated without intracranial pressure monitoring. JNeurosurg. 2012; 117 (4): 729-34.

Foundation for Medical and Technical Research and Education in Emergencies and Disasters120
7. Barmparas G, Singer M, Ley E, Chung R, Malinoski D, Margulies D, Salim A, BukurM.Decreased intracranial pressure monitor use at level II trauma centers is associated with increased mortality. Am Surgeon. 2012: 78(10): 1166-1171.
8. Thompson HJ, Rivara FP, Jurkovich GJ, Wang J, Nathens AB, Mackenzie E. Evaluation of the effect of intensity of care on mortality after traumatic brain injury. Crit Care Med. 2008; 36 (1): 282-290.
9. Sha i S, Diaz-Arrastia R, Madden C, Gentilello L., Intracranial pressure monitoring in brain-injured patients is associated with worsening of survival. Journal of Trauma.2008; 64 (2): 335-40.
10. Alali AS, Fowler RA, Mainprize TG, Scales DC, Kiss A, de Mestral C, Ray JG, Nathens AB., Intracranial pressure monitoring in severe traumatic brain injury: results from the American College of Surgeons Trauma Quality Improvement Program. Journal of Neurotrauma. 2013; 30 (20): 1737-1746.
11. Chesnut RM, Temkin N, Carney N, Dikmen S, Rondina C, Videtta W, Petroni G, LujanS, Pridgeon J, BarberJ, Machamer J, Chaddock K, Celix JM, Cherner M, HendrixT. A Trial of Intracranial-Pressure Monitoring in Traumatic Brain Injury. NEJM. 367 (26).

Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 121
Flowchart for the process of inclusion in articles
References identifi ed through searches of databases
(n=320)Pubmed: 199Embase: 55Biosis: 2Scisearch: 12Medpilot: 10Cochrane: 19Tripdatabase: 23
References obtained manually(n=8)
Duplicate References(n=23)
Articles not related(n=294)
All references obtained(n=328)
References included with title and abstract that were revised
(n=305)
Revised Articles(n=11)
Included articles(n=2)
Excluded articles(n=9)
The results publication did not allow calculating the R-R: 1
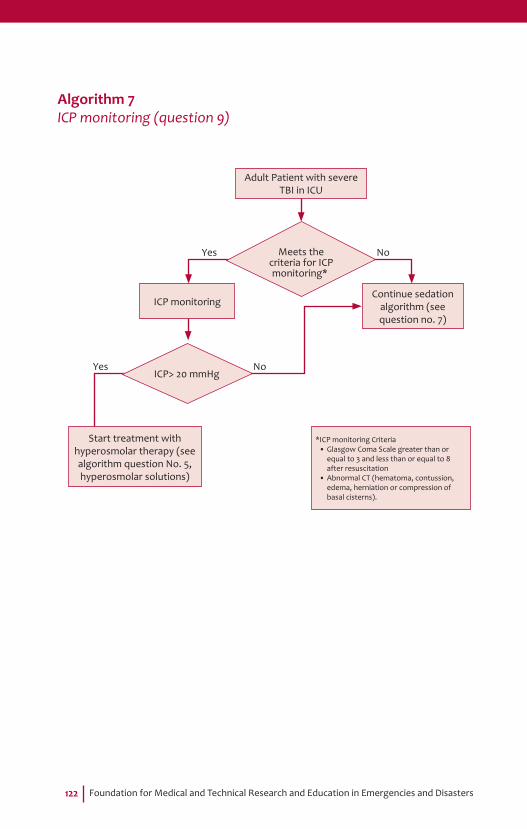
Foundation for Medical and Technical Research and Education in Emergencies and Disasters122
Algorithm 7ICP monitoring (question 9)
*ICP monitoring Criteria• Glasgow Coma Scale greater than or
equal to 3 and less than or equal to 8 after resuscitation
• Abnormal CT (hematoma, contussion, edema, herniation or compression of basal cisterns).
Adult Patient with severe TBI in ICU
ICP monitoring
Start treatment with hyperosmolar therapy (see algorithm question No. 5, hyperosmolar solutions)
Continue sedation algorithm (see question no. 7)
Yes
Yes
No
No
Meets the criteria for ICP monitoring*
ICP> 20 mmHg

Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 123
Question 10
In adult patients with severe TBI being treated in an ICU, does selective head cooling, compared to normothermia, decrease neurological disa-bility and mortality at discharge?
Recommendation
• It is suggested that adult patients with severe TBI have selec-tively and non-invasively cooled their skulls using a recircu-lating-water system or tapes chilled to 4 degrees centigrade, ensuring that intracerebral temperature can be measured.
Weak recommendation in favor of the intervention, moderate quality of evidence.
• It is suggested that patients should be maintained at a body temperature above 36 degrees and below 38 degrees, measu-red rectally, in order to avoid systemic hypothermia.
Weak recommendation in favor of the intervention, moderate quality of evidence.
• It is not recommended to perform the intervention in institu-tions that do not have a recirculating-water system or tapes chilled to 4 degrees centigrade.
Recommendation by strong consensus in favor of the intervention.
IntroductionHead cooling has been proposed as a model of neuroprotection in in-tensive care for patients with severe TBI. Cooling can be applied in-vasively and non-invasively, systemically or locally (Lazorthes 1958, Polderman 2004 Miñanbres 2008). The local non-invasive method (selective) may limit the secondary damage associated with systemic induction of hypothermia, which may be related to complications such as cardiac arrhythmia, abnormal coagulation and risk of systemic in-fections (Sahuquillo 2007). Therefore, selective head cooling is consi-dered a therapeutic alternative in patients with severe TBI in order to decrease the metabolic consumption of cerebral oxygen and reduce re-fractory intracranial pressure. Various studies have attempted to exa-mine the relationship between systemic hypothermia and functional

Foundation for Medical and Technical Research and Education in Emergencies and Disasters124
outcome in these patients. Studies with systemic hypothermia have not shown a bene it of the procedure. Few studies have evaluated non-invasive selective hypothermia, but this intervention continues to be used with heterogeneity in different health institutions. For this rea-son it has been decided to include this question for clinical practice guidelines in Colombia.
Summary of the evidenceA total of three studies were reviewed to answer the question (Qiu 2006, Liu 2006, Harris 2009). All three studies were randomized cli-nical trials in which non-invasive selective cooling of the head using external devices were compared with the non-use of the same. The three studies included adult patients with severe TBI and for this reason were included in the analysis. In the irst study (Qiu 2006), 90 patients were analyzed and selective cooling was started in 45 of them between 0 and 5.6 hours after admission or emergency surgery, and cooling was maintained for three days. The system maintained a temperature in the skull and neck of around 4 degrees Celsius using an external water recirculation system and ice belts. Acquired ave-rage brain temperature was between 33 and 35 degrees centigrade, measured by an intraparenchymal temperature monitor. Rectal tem-perature was assessed to maintain a systemic temperature of no more than 37 degrees centigrade. Intracranial pressure was lower during the time of the procedure in the intervention group. Good functional outcome (de ined as having GOS 4-5) at 6 months was 73.3% in the intervention group, and 51.1% for the group whose heads were not cooled. There were more cases of pneumonia and thrombocytopenia in the intervention group. The platelet count was normalized after treatment ended. There were no abnormalities of heart rate, blood pressure or electrolytes. The second study (Liu 2006) analyzed 66 patients divided into 3 groups; 22 patients were given non-invasive selective cooling, 21 were given mild systemic hypothermia and 23 patients were treated with normothermia. All were adults with seve-re TBI. The authors evaluated outcome at discharge and at 2 years.
Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 125
Treatment was continued for 3 days. In the group of selective cooling, success (measured as GOS 4-5) at two years was 72.7%, and in the normothermia group it was 34.8%. There were no differences in in-fectious complications. The platelet count was found to be decreased in both groups that underwent hypothermia and cooling compared to the control group, but this decrease platelet returned to normal 3 days after completing treatment. Selective cooling was performed with a water recirculation system at 4 degrees centigrade and ice bars at neck level. Brain temperature, measured intraparenchyma-lly, fell to 33 degrees Celsius. There was a signi icant reduction in intracranial pressure in patients receiving the treatment and also an increase in serum sodium levels. The third study (Harris 2009) used a system called a “cooling cap” in adult patients with severe TBI. 25 patients were analyzed, of which 12 were assigned to treatment and 13 to the control group. The patients in the control group spent more time in the emergency department before being transferred to the ICU. In the group of selective cooling, mortality at hospital dischar-ge was 50%, and in the normothermia group, mortality was 30.8%. Intracranial temperature was reduced to 33 degrees Celsius and the body was heated to maintain a minimum of 36 degrees and avoid systemic hypothermia. Treatment was maintained for 3 days.
Given that the devices used in the three studies are not currently avai-lable in Colombia, the working group considered it important to make a consensus to establish a recommendation on selective cooling of adult patients with severe TBI in environments that do not have this equipment. All the participants of the consensus were sent the studies identi ied in the search, including those who did not meet all the cri-teria of the PICO question. Subsequently a face-to-face meeting lasting two hours was held. The group was composed of experts working in prehospital care, emergency departments, intensive care and neuro-surgery services in different regions of the country, both in public and private institutions (Table 12).
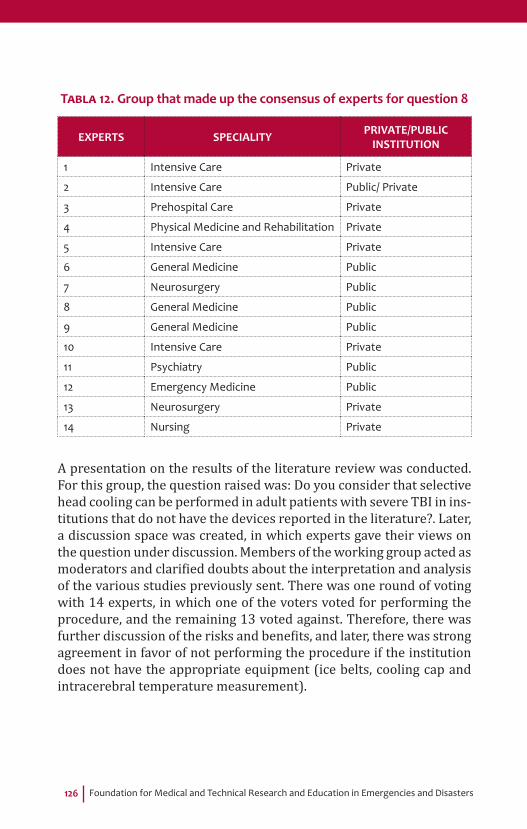
Foundation for Medical and Technical Research and Education in Emergencies and Disasters126
TABLA 12. Group that made up the consensus of experts for question 8
EXPERTS SPECIALITY PRIVATE/PUBLIC INSTITUTION
1 Intensive Care Private
2 Intensive Care Public/ Private
3 Prehospital Care Private
4 Physical Medicine and Rehabilitation Private
5 Intensive Care Private
6 General Medicine Public
7 Neurosurgery Public
8 General Medicine Public
9 General Medicine Public
10 Intensive Care Private
11 Psychiatry Public
12 Emergency Medicine Public
13 Neurosurgery Private
14 Nursing Private
A presentation on the results of the literature review was conducted. For this group, the question raised was: Do you consider that selective head cooling can be performed in adult patients with severe TBI in ins-titutions that do not have the devices reported in the literature?. Later, a discussion space was created, in which experts gave their views on the question under discussion. Members of the working group acted as moderators and clari ied doubts about the interpretation and analysis of the various studies previously sent. There was one round of voting with 14 experts, in which one of the voters voted for performing the procedure, and the remaining 13 voted against. Therefore, there was further discussion of the risks and bene its, and later, there was strong agreement in favor of not performing the procedure if the institution does not have the appropriate equipment (ice belts, cooling cap and intracerebral temperature measurement).
Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 127
From evidence to recommendationIn the discussion of the working group, it was decided that the recom-mendation for selective cooling is weak in favor of the intervention be-cause, although the balance between desired outcomes (improvement in disability and decreased mortality) vs unwanted results (coagulo-pathy, infection, hydro-electrolyte disturbance) is slightly in favor of cooling, it was recognized that the equipment evaluated in the studies is unavailable for intervention in most institutions in Colombia, and in the same way, the consensus of experts discussed the importance of hospitals having this equipment in order to make an appropriate intervention.
Structural requirementsIt is considered that to carry out this recommendation, no infrastructu-re is required in addition to that, which is already available within the Colombian system of social security in health. Current standards do not provide the necessary elements to establish a procedure of selec-tive head cooling in adult patients with severe TBI. Currently, the pro-cedure is performed without a device designed for this purpose and without measuring the intracerebral temperature, making it dif icult to maintain a speci ic target for the treatment. This inability to control this temperature can generate more complications than bene its.
Considerations on benefi ts and risksIt is considered that the bene it of implementing selective head cooling (reduction in cerebral metabolic consumption and anti-in lammatory effect) outweighs the risk caused by localized hypothermia (infection and coagulopathy). Keeping in mind that selective hypothermia poses fewer risks than systemic hypothermia, it is vital to control body tem-perature in order to prevent systemic hypothermia.
Considerations on the values and preferences of patientsFor this recommendation in particular, patients and their caregivers did not state any preference that would modify the recommendation.

Foundation for Medical and Technical Research and Education in Emergencies and Disasters128
Implications on resourcesIt is considered that the bene it of implementing the recommendation may be cost effective, given that the cost of the complications asso-ciated with not controlling intracranial hypertension in patients with brain injuries (Cerebral infarction, brain herniation, brain death) can be much greater than the cost that might arise from the use of these lo-cal cooling devices. It is important to remember that in Colombia there are no economic studies on the implications of this recommendation.
References1. Lazorthes G, Campan L. Hypothermia in the treatment of craniocerebral
traumatism. Neurosurg. 1958; 15(2):162-167.2. Polderman K H. Keeping a cool head: How to induce and maintain
hypothermia. J Med. 2004; 32(12): 2558-2560.3. Miñambres E, Holanda MS, Domínguez Artigas MJ, Rodríguez Borregán
JC. Therapeutic hypothermia in neurocritical patients. J MedIntensiva. 2008;32(5):227-35.
4. Sahuquillo J, Vilalta A.Cooling the injured brain: how does moderate hypothermia in luence the pathophysiology of traumatic brain injury. J Curr Pharm Des. 2007;13(22):2310-2322.
5. Qui W, Shen H, Zhang Y, Wang W, Liu W, Jiang Q, Luo M, Manou M. Noninvasive selective brain cooling by head and neck cooling is protective in sever traumatic brain injury. Journal clinical neuroscience. 2006; 13: 995-100.
6. Liu WG, Qiu WS, Zhang Y, Wang WM, Lu F, Yang XF. Effects of selective brain cooling in patients whit severe traumatic brain injury: a preliminary study. Journal of international medical research. 2006; 34: 58-64.
7. Harris OA, Muh CR, Surles MMC, Pan Y, Rozycki G, Macleod J, Et al. Discrete cerebral hypothermia in the management of traumatic brain injury: a randomized controlled trial, JNeurosurg. 2009; 110: 1256-1264.

Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 129
Flowchart for the process of inclusion in articles
References identifi ed through searches of databases
(n=352)Pubmed: 92Embase: 114Biosis: 27Scisearch: 70Medpilot: 18Cochrane: 27Tripdatabase: 4
References obtained manually(n=2)
Duplicate References(n=68)
Articles not related(n=283)
All references obtained(n=354)
References included with title and abstract that were revised
(n=286)
Revised Articles(n=3)
Included articles (n=3)
Excluded articles(n=0)

Foundation for Medical and Technical Research and Education in Emergencies and Disasters130
Algorithm 8Hypothermia (question 10)
Availability of cooling systems of recirculating water or frozen tapes to 4
degrees Celsius and a device for measuring brain temperature
Adult Patient with severe TBI in ICU and refractory intracranial hypertension
Start selective head cooling maintain a body temperature
above 36 degrees and below 38 degrees, measured by rectal
temperature, in order to avoid the systemic
hypothermia
Continue handling in ICU (see algorithm
question No. 7, Sedation), consider
indications for surgery from cerebral edema
before 24 h (see algorithm question
No. 6)
Yes No

Ministry of Health and Social Protection - Colciencias 131
Economic Question
Economic evaluation for rapid sequence intubation in patients with severe traumatic brain injury.
Objective
Determine if the Rapid Sequence Intubation (RSI) procedure applied early in prehospital care (PHC) on adult patients diagnosed with seve-re Traumatic Brain Injury (TBI), is more cost-effective compared with intubation in Hospital Emergency Department (ED).
Methods
A decision model was designed to compare the costs and outcomes related to two strategies for performing RSI (PHC or ED) on adult pa-tients with severe TBI. Costs were determined from Colombian prac-tice guidelines. Outcomes were measured using GOS-E adjusted to 3 states of health (neurological outcome level 1 and 2, plus death), at 6 months after the accident; the effectiveness of therapeutic alternatives was taken from existing clinical literature. Based on this information, the incremental cost-effectiveness ratio (ICER) was calculated. Finally, the model was calibrated using indicators of cost-utility (QALY), sce-narios of extreme values (univariate) and a Monte Carlo process with 10,000 iterations (multivariate).
Foundation for Medical and Technical Research and Education in Emergencies and Disasters132
Results
The RSI-PHC strategy is more cost effective than the RSI-ED strategy and generates signi icant savings for the GSSSH. In the base scenario, the ICER is estimated to be -$270 million; models used show that if more RSI procedures were carried out in PHC and fewer in ED, the GSSSH would get better levels of health for their bene iciaries and would use inancial resources more ef iciently.
Conclusions
Current clinical practice and especially the mechanism of reimburse-ment for emergency care related to TBI, make the costs of RSI-ED stra-tegy higher than those of RSI-PHC; furthermore, early treatment using RSI for a TBI emergency increases the likelihood of obtaining better neurological outcomes, so the RSI-PHC strategy becomes dominant over RSI-ED.
Revision of economic evaluations present in the literature
The economic question made above is taken as the basis for the sys-tematic review of existing literature, which is a complementary pro-cess to the search performed by the clinical team; for this reason the same databases and syntax were used as in the technology assessment process (discussed in the relevant section of the Clinical Practice Gui-deline of Severe TBI (CPG/TBI)), and the relevant economic terms were also used. Furthermore, the databases recommended by the methodological guideline (MG) were used: Econlit, Embase, MEDLI-NE/PUBMED, Database of Abstracts of Reviews of Effects (DARE), NHS Economic Evaluation Database (NHS EED) and the Health Technology Assessment (HTA) Database. The search process for economic eviden-ce in the literature yielded no results that speci ically answered the economic question (and neither did it obtain any results that answe-red it partially). Therefore, the evaluation used the reference on which the Clinical Team of the working group based their evidence: “Prehos-pital Rapid Sequence Intubation Improves Functional Outcome for Pa-tients with Severe Traumatic Brain Injury. A Randomized Controlled Trial “published by Bernard et al (2012), in which the authors sought

Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 133
to determine whether RSI in PHC applied to adult patients (> 16 years) diagnosed with Severe TBI (GCS < 9) improves neurological outcomes measured 6 months post-trauma, compared with intubation procedu-re made in hospitals.
CHART 1. Selection of Relevant Studies for the Literature Review. Source: Made by the working group based on CDR 2009.
References identifi ed through searches of databases
(n=95)Econlit: 0Embasse: 0Pubmed: 0Medline: 0CRD/DARE/NHSEED,HTA: 0 References obtained manually
(n=7)
Duplicate References(n=0)
Articles not related(n=7)
All references obtained(n=7)
References included with title and abstract that were revised
(n=7)
Revised Articles(n=0)
Included articles (n=0)
Excluded articles(n=0)
Foundation for Medical and Technical Research and Education in Emergencies and Disasters134
As indicated in the MG, the Economical Evaluation (EE) of the RSI pro-cedure in the CPG/TBI, due to a lack of economic evidence, must be made de novo based on existing data and/or data on clinical effecti-veness found by the clinical team of the working group, complemen-ted with data on costs that can be created from the description of the practices related to the treatment of TBI in Colombia and the innova-tion proposed by the CPG/TBI, such as the procedures described in the guideliness for PHC and emergencies of the Ministry of Health and Social Protection.
Conclusions
The inal recommendation after the economic assessment is that ambulances of Medicalized Assistance Transport (MAT), which rigo-rously apply the standard procedures for PHC, must attend to severe TBI events; evidence was found which makes more ef icient use of the resources of the GSSSH and helps improve health outcomes.
The economic assessment for the RSI procedure in the CPG/TBI shows that the RSI-PHC strategy, by making use of the resolution capabilities of ambulances or MATs is more cost-effective than the current RSI-ED practice, to the point of being totally dominant over this (negative incremental cost, positive incremental effectiveness); aditionally the ICER is located in quadrant VI and its value is optimally well below the WHO threshold of 1 GDP (approx -$270 million compared to $14.5 million.). This result happens basically because standard practice in Colombia loads the system with costs that can be saved; currently, emergencies related to TBI are attended through Basic Assistance Transport (BAT) procedures, but reimbursed at MAT rates, especially because there is a high probability (over 90%) that the cases are traf ic accidents and therefore the rate established in the 2013 SOAT (obli-gatory road insurance) manual applies. In this way the management of an emergency becomes a patient transfer to an ED, at PHC rates. Finally, it is important to clarify that the use of RSI in PHC, although it is regulated in Colombia by technical guides, requires a number of additional factors, some of a logistical nature (such as the effective and ef icient functioning of the Regulating Center for Emergencies) other operating (such as the standard number of hours of speci ic training in intubation required for staff in MAT), which together have implications
Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 135
in clinical outcomes. As mentioned in the Clinical Practice Guidelines for the Diagnosis and Treatment of Adult Patients with Severe TBI, in its chapter on early intervention by RSI, Colombia must make improve-ments in PHC so that the procedures applied in this instance reach the level of development seen in the clinical evidence. An example for this case is the Australian PHC system on which Bernard based his study. This whole set of elements would be the ideal base to design a compre-hensive and deep Budget Impact Analysis (BIA) from the perspective of the GSSSH, which would allow the system to have a tool that helps align the requirements of public investment in health with policies in PHC quality and the levels of health of the Colombian population.
The full economic study, including the references used in the produc-tion of this study, can be read in Chapter 4 of the full version of this guide.

Foundation for Medical and Technical Research and Education in Emergencies and Disasters136
Abbreviations and Glossary
Abbreviations
AIS: Abbreviated Injury Scale
AMSTAR: A Measurement Tool To Assess Systematic Reviews
ASCOFAME: Asociación Colombiana de Facultades de Medicina (Colom-bian Association of Medicine Faculties)
BIA: Budget Impact Analysis
BNEE: Brigade Nationale d’Enquêtes Économiques (French National Brigade of Economic Surveys)
BTF: Brain Trauma Foundation
CT: Computerized Tomography
CEA: Cost-Effectiveness Analysis
CENDEX: Centro de Proyectos para el Desarrollo (Center for Develop-ment Projects)
COLCIENCIAS: Departamento Administrativo de Ciencia, Tecnología e Innovación (Colombian Administrative Department of Science, Tech-nology and Innovation)
CPA: Cost and Pro it Analysis
CSF: Cerebrospinal luid
CUPS: Clasi icación Única de Procedimientos de Salud (Unique Classi i-cation of Health Procedures)
DANE: Departamento Administrativo Nacional de Estadística (Colom-bian National Administrative Department of Statistics)
Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 137
DIMDI: Deutsches Institut für Medizinische Dokumentation und Informa-tion (German Institute for Medical Documentation and Information)
EPS: Entidad Promotora de Salud (Colombian Healthcare Provider)
GCS: Glasgow Coma Scale
GDP: Gross Domestic Product
GOS: Glasgow Outcome Scale
GOS-E: Glasgow Outcome Scale -Extended
CPG: Clinical Practice Guideline
GRADE: Grades of Recommendation, Assessment, Development and Evaluation Working Group
GSSSH: General Social Security System in Health
HITS-NS: Health Information Technology Services of Nova Scotia
ICER: Incremental cost-effectiveness ratio
ICH: Intracranial Hypertension
ICP: Intracranial Pressure
ICU: Intensive Care Unit
ICUR: The Incremental Cost Utility Ratio
IETS: Instituto de Evaluación Tecnológica en Salud (Colombian Institu-te of Technological Evaluation in Health)
IPS: Instituciones Prestadoras de Servicios (Colombian Healthcare Services)
LMWH: Low Molecular Weight Heparin
MG: Management Group
MGEE: Methodological Guide for Economic Evaluations
MINSALUD: Ministerio de Salud y Protección Social (Colombian Minis-try of Health and Social Protection)
NPV: Net Present Value
NS: Normal Saline Solution
PHC: Pre Hospital Care
PICO: Population, Intervention, Comparator and Outcome
Foundation for Medical and Technical Research and Education in Emergencies and Disasters138
POS: Plan Obligatorio de Salud (Obligatory Health Plan)
QALY: Quality-Adjusted Life Years
RASS: Richmond Agitation Sedation Scale
RSI: Rapid Sequence Intubation
SIGN: Scottish Intercollegiate Guidelines Network
SISMED: Sistema Integrado de Suministros de Medicamentos e Insumos Quirúrgicos (Integrated System for the Provision of Medication and Surgical Supplies)
SISPRO: Sistema Integral de Información de la Protección Social (Inte-grated Information System for Social Protection)
SOAT: Seguro Obligatorio de Accidentes de Tránsito (Colombian Obliga-tory Insurance for Traf ic Accidents)
SPSS: Statistical Product and Service Solutions
TAB: Transporte Asistencial Básico (Basic Assistance Transport)
TAM: Transporte Asistencial Medicalizado (Medicalized Assistance Transport)
TBI: Traumatic Brain Injury
WHO: World Health Organization
Glossary
Advanced life support: Measures for the advanced management of patients in the emergency department, including invasive methods and use of medication
Advanced neurological monitoring: The use of devices to measure the brain´s physiological variables in the intensive care unit
Amnesia: Loss of memory
Bag-valve mask system: Device that supplies air through the airway to support spontaneous ventilation in patients with respiratory failure

Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 139
Basic care transfer unit: Motor vehicle manned by personnel trained in basic life support, used to transfer patients from the site of an emer-gency or between hospitals
Basilar skull fracture: Disruption of the cranial table in the region of the loor of the skull
Biosis: Biological Science Database
Brain death: Cessation of brain functional activities after irreversible damage of brain tissue
Brain drain surgery: A surgical procedure through which intracranial hematic collections are evacuated
Brain hernia: Squeezing of brain tissue through natural spaces in the skull
Brain in lammation: Phenomenon of brain tissue which occurs as a cellular response associated with trauma
Brain necrosis: Death of brain tissue due to lack of oxygenated blood low
Capnography: A device that allows measurement of carbon dioxide exhaled during respiration
Cephalea: Aches and pains located anywhere in the head
Coagulopathy: A group of disorders of the coagulation system of the blood, due to which bleeding is prolonged and excessive.
Cochrane Library Database: Database of systematic revisions in the Cochrane library
Controlled clinical trial: Scienti ic procedure commonly used in tes-ting medicines or medical procedures randomly
Computerized tomography (CAT) of the skull: Brain image made through a computerized system that integrates radiological images of the skull
Cranial descompression surgery: A surgical procedure through which a large portion of the skull bone is removed to relieve intracra-nial pressure

Foundation for Medical and Technical Research and Education in Emergencies and Disasters140
Craniotomy: Surgical opening of the cranial cavity
Cerebral infarction: Injury caused by lack of blood low within the brain tissue
Cerebral ischemia: brain state secondary to a reduction in oxygen supply to brain tissue
Diplopia: Visual impairment in which objects appear twice
Disability: A condition under which certain people have some phy-sical, mental, intellectual or sensory impairment that in the long run affects their way of interacting and participating fully in society
Depressed fracture: Depression of a fragment or section of the skull bone, which often compresses the brain and the dura beneath
Diagnostic heterogeneity: Variability in diagnoses
Endotracheal intubation (intratracheal): Action to introduce a si-licon tube through the trachea in order to facilitate the passage of air from outside into the lungs.
Extradural hematoma: A buildup of blood located between the skull and the dura mater
Focal neurological de icit: Abnormality of the nervous system detec-ted during physical examination
Forensis: Journal of the National Institute of Legal Medicine and Fo-rensic Sciences
Good clinical practice: International ethical and scienti ic standards for designing, conducting, recording and reporting studies that involve the participation of human standard.
Gray Literature: Any document that is not included in the main search databases
Hyperkalemia: Increased blood potassium levels above those accep-ted as normal
Hipervolemia: State of increased body intravascular volume
Hypertonic solution: Crystalloid or colloid solution with a high so-dium load
Hypotension: Blood pressure below the normal limit

Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 141
Injury severity index: Abbreviated injury scale created by the Ame-rican Medical Association, quantifying the severity of injury to each of the body regions
Inductor Medication: Medication associated with a state of hypnosis that is part of rapid sequence intubation
Intensive care: Medical specialty dedicated to providing life support or organ systems support in critically-ill patients
Intracranial hematoma: A buildup of blood inside the brain tissue
Intracranial hypertension: Increased pressure within the structures of the content of the cranial cavity
Intracranial pressure: Pressure that exists within the cranial cavity
Intravenous luids: Crystalloid solutions used for resuscitation that create volume within the intravascular space
Isotonic solution: Crystalloid or colloid solution with a sodium con-centration similar to blood plasma
Laryngeal Mask: Alternative airway management device used as part of rescue in case of unsuccessful intubation.
Laryngoscopy: Action of visualizing the airway through a laryngoscope
Level of Evidence: Hierarchical system, based on tests or research studies, which helps health professionals to assess the strength or so-lidity of evidence linked to the results of a therapeutic strategy
Meta-analysis: A set of statistical tools that is useful to synthesize data from a study group
Mortality: The number of deaths in a population
Neurologic sequelae: Cognitive, motor or sensory disturbance resul-ting from a brain injury
Neuromuscular relaxant: A drug that induces relaxation of skeletal muscle and that is part of rapid sequence intubation
Oropharyngeal airway: A device that keeps the air passage between the mouth and pharynx open
Otorrhea: Loss of cerebrospinal luid through the ear canal

Foundation for Medical and Technical Research and Education in Emergencies and Disasters142
Outcome: Final result of an event or occurrence that has been taking place for some time
Periorbital ecchymosis: Purplish discoloration of the tissue around the eye socket
Persistent vomiting: Emesis on more than two occasions
Pharmacological anticoagulation: Inhibition of the process of blood coagulation induced by medications
Postraumatic seizure: Abnormal movements generated by patholo-gical cerebral electric shock
Prehospital care: Operational and coordination service for urgent medical problems comprising rescue services, health care and trans-portation provided to sick or injured people outside the hospital
Pubmed: Search engine for the Medline database
Pulse-oximetry: Monitoring method which evaluates the percentage of oxygen in peripheral arterial blood
Rapid sequence intubation: Sequential use of drugs required to ca-rry out the process of intubation
Refractory intracranial hypertension: Increased intracranial pres-sure for more than 5 minutes above 25 mmHg
Retroauricular ecchymosis: Purple discoloration in tissue located behind the ear
Rhinorrhea: Loss of cerebrospinal luid through the nasal passage
Skull fracture: Disruption of the cranial bone
Subdural hematoma: A buildup of blood located between the dura mater and the brain
Selective hypothermia: A maneuver of decreasing temperature, applied to one segment of the body (eg head)
Secondary brain injury: Physiological disorder in the brain resulting from the body’s natural reaction to a brain injury that is treated inap-propriately.
Systolic blood pressure: Corresponds to the maximum blood pressu-re when the heart is contracting

Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 143
Sedation: Pharmacological induction of a state of decreased cons-ciousness
Search syntax: Combination of all descriptive terms designated for the study which will be used in article search engines
Survival: Time after treatment during which there is no mortality
Systematic review: Review of scienti ic articles that follow an expli-cit method to summarize information about a certain topic or health problem
Thromboprophylaxis: Method to prevent the formation of thrombus in peripheral or central veins
Trauma care system: Part of the health model designated for emer-gency trauma health care
TripDatabase: Medical search engine with an emphasis on medicine based on evidence, questions and clinical guidelines
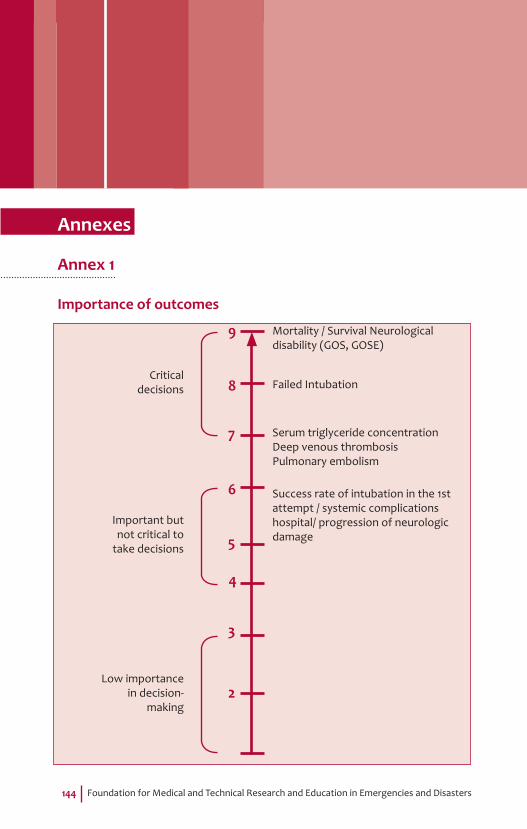
Foundation for Medical and Technical Research and Education in Emergencies and Disasters144
Annexes
Annex 1
Importance of outcomes
Mortality / Survival Neurological disability (GOS, GOSE)
Failed IntubationCritical
decisions
Serum triglyceride concentrationDeep venous thrombosisPulmonary embolism
Success rate of intubation in the 1st attempt / systemic complications hospital/ progression of neurologic damage
Important but not critical to
take decisions
Low importance in decision-
making2
3
4
5
6
7
8
9

Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 145
Annex 2
Inclusion and exclusion tables for full text articles
Question 1a
AUTHOR METHOD PARTICIPANTS INTERVENTION FINAL POINTS
MEETS REQUI-
REMENTS
Pandor 2012
Meta-analysis and systematic review
Mild TBI; Diagnostic cohorts
Clinical characteristics
CT FINDINGS Yes
References1. Pandor A, Harnan S, Goodacre S, Pickering A, Fitzgerald P, Rees A.
Diagnostic accuracy of clinical characteristics for identifying CT abnormality after minor brain injury: a systematic review and meta-analysis. J Neurotrauma 2012; 29: 707-718.
Question 1b
AUTHOR METHOD PARTICIPANTS FINAL POINTS MEETS REQUIREMENTS
Sue E. Harnan 2011
Systematic review Mild TBI Rules for clinical
decision making Yes
Dunning 2004
Meta-analysis Mild TBI
Factors for the prediction of intracranial hemorrhage
Yes
References1. Dunning J, Stratford-smith P, Lecky F, Batchelor J, Hogg K, Browne
J, et al. A Meta-Analysis of clinical correlates that predict signi icant intracranial injury in adults whit minor head trauma. J Neurotrauma. 2004; 21 (7): 877-885.
2. Harnan SE, Pickering A, Pandor A, Goodacre SW. Clinicaldecision rules for a adults with minor head injury: a systematic review. J Trauma. 2011; 71 (1): 245-251.
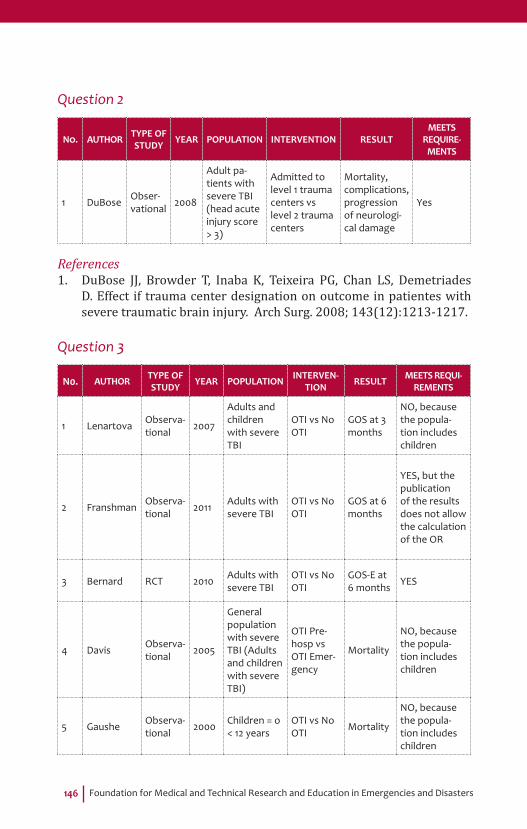
Foundation for Medical and Technical Research and Education in Emergencies and Disasters146
Question 2
NO. AUTHOR TYPE OF STUDY YEAR POPULATION INTERVENTION RESULT
MEETS REQUIRE-
MENTS
1 DuBose Obser-vational 2008
Adult pa-tients with severe TBI (head acute injury score > 3)
Admitted to level 1 trauma centers vs level 2 trauma centers
Mortality, complications, progression of neurologi-cal damage
Yes
References1. DuBose JJ, Browder T, Inaba K, Teixeira PG, Chan LS, Demetriades
D. Effect if trauma center designation on outcome in patientes with severe traumatic brain injury. Arch Surg. 2008; 143(12):1213-1217.
Question 3
N0. AUTHOR TYPE OF STUDY YEAR POPULATION INTERVEN-
TION RESULT MEETS REQUI-REMENTS
1 Lenartova Observa-tional 2007
Adults and children with severe TBI
OTI vs No OTI
GOS at 3 months
NO, because the popula-tion includes children
2 Franshman Observa-tional 2011 Adults with
severe TBIOTI vs No OTI
GOS at 6 months
YES, but the publication of the results does not allow the calculation of the OR
3 Bernard RCT 2010 Adults with severe TBI
OTI vs No OTI
GOS-E at 6 months YES
4 Davis Observa-tional 2005
General population with severe TBI (Adults and children with severe TBI)
OTI Pre-hosp vs OTI Emer-gency
Mortality
NO, because the popula-tion includes children
5 Gaushe Observa-tional 2000 Children = o
< 12 yearsOTI vs No OTI Mortality
NO, because the popula-tion includes children

Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 147
N0. AUTHOR TYPE OF STUDY YEAR POPULATION INTERVEN-
TION RESULT MEETS REQUI-REMENTS
6 Hartl Observa-tional 2006
General population with severe TBI (Adults and children with severe TBI)
OTI vs No OTI
Morta-lity at 2 weeks
NO, because the popula-tion includes children
7 Bochiccio Observa-tional 2003 14 to 56 year
old patients
Prehosp OTI vs emergen-cy OTI
Mortality
NO, because the popula-tion includes children
8 Davis Observa-tional 2010
Adults with moderate and severe TBI
OTI vs No OTI Mortality
NO, because the population includes mo-derate TBI
9 Bukur Observa-tional 2011
Adults with moderate and severe TBI and with AIS = >3
OTI vs No OTI Mortality
NO, because the population includes mo-derate TBI
10 Dowling Observa-tional 2008
Adults with severe TBI; AIS = >3
Prehosp OTI vs emergen-cy OTI
Mortality
NO, because the population includes mo-derate TBI
11 DAVIS Observa-tional 2005
Adults with major trauma
OTI vs No OTI Mortality
NO, because they evaluated mortality at 6 months
12 DAVIS Observa-tional 2003 Adults with
severe TBIOTI vs No OTI Mortality
NO, because GOS-E was evaluated at hospital discharge
13 MURRAY Observa-tional 2000
Patients with severe TBI
OTI vs No OTI Mortality
NO, because GOS-E was evaluated at hospital discharge
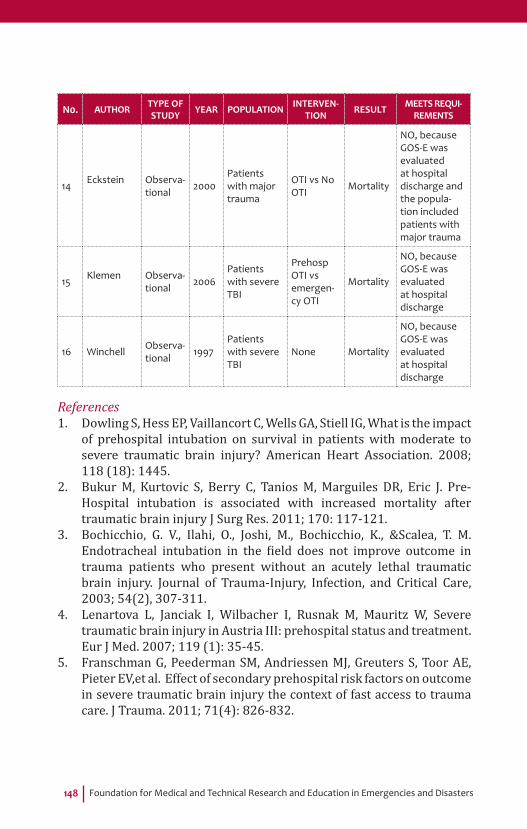
Foundation for Medical and Technical Research and Education in Emergencies and Disasters148
N0. AUTHOR TYPE OF STUDY YEAR POPULATION INTERVEN-
TION RESULT MEETS REQUI-REMENTS
14 Eckstein Observa-tional 2000
Patients with major trauma
OTI vs No OTI Mortality
NO, because GOS-E was evaluated at hospital discharge and the popula-tion included patients with major trauma
15 Klemen Observa-tional 2006
Patients with severe TBI
Prehosp OTI vs emergen-cy OTI
Mortality
NO, because GOS-E was evaluated at hospital discharge
16 Winchell Observa-tional 1997
Patients with severe TBI
None Mortality
NO, because GOS-E was evaluated at hospital discharge
References1. Dowling S, Hess EP, Vaillancort C, Wells GA, Stiell IG, What is the impact
of prehospital intubation on survival in patients with moderate to severe traumatic brain injury? American Heart Association. 2008; 118 (18): 1445.
2. Bukur M, Kurtovic S, Berry C, Tanios M, Marguiles DR, Eric J. Pre-Hospital intubation is associated with increased mortality after traumatic brain injury J Surg Res. 2011; 170: 117-121.
3. Bochicchio, G. V., Ilahi, O., Joshi, M., Bochicchio, K., &Scalea, T. M. Endotracheal intubation in the ield does not improve outcome in trauma patients who present without an acutely lethal traumatic brain injury. Journal of Trauma-Injury, Infection, and Critical Care, 2003; 54(2), 307-311.
4. Lenartova L, Janciak I, Wilbacher I, Rusnak M, Mauritz W, Severe traumatic brain injury in Austria III: prehospital status and treatment. Eur J Med. 2007; 119 (1): 35-45.
5. Franschman G, Peederman SM, Andriessen MJ, Greuters S, Toor AE, Pieter EV,et al. Effect of secondary prehospital risk factors on outcome in severe traumatic brain injury the context of fast access to trauma care. J Trauma. 2011; 71(4): 826-832.

Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 149
6. Bernard SA, Nguyen V, Cameron P, Masci K, Fitzgerald M, Cooper DJ, Prehospital Rapid Sequence Intubation Improves Functional Outcome for Patients With Severe Traumatic Brain Injury. Annals of Surgery.2010; 252(6):959-965.
7. Davis DP, Stern J, Ochs M, Sise MJ, Hoyt DB. A follow-up analysis of factors associated with head-injury mortality after paramedic rapid sequence intubation. J Trauma. 2005; 59 (2): 486-490.
8. Davis DP, Peay J, Sise MJ, Kennedy F, Simon F, Tominanga G, et al. Prehospital airway and ventilation management: A trauma score and injury severity score based analysis. J Trauma, 2010; 68 (2): 294-301.
9. Davis DP, Vadeboncoeur TF, Ochs M, Pste JC, Vilke GM, Hoyt DB. The association between ield glasgwow coma scale score and outcome in patients undergoing paramedic rapid sequence intubation. J Emerg Med. 2005; 24 (4): 391-397.
10. Murray JA, Demetriades D, Berne TV, Stratton SJ, Cryer HG, Bongard F, Fleming A, Gaspard D. Prehospital intubation in patients with severe head injury. J Trauma. 2000 Dec;49(6):1065-70.
11. Eckstein M, Chan L, Schneir A, Palmer R. Effect of prehospital advanced life support on outcomes of major trauma patients. J Trauma. 2000 Apr;48(4):643-8.
12. Klemen P, Grmec S. Effect of pre-hospital advanced life support with rapid sequence intubation on outcome of severe traumatic brain injury. Acta Anaesthesiol Scand. 2006 Nov;50(10):1250-4.
13. Winchell RJ, Hoyt DB. Endotracheal intubation in the ield improves survival in patients with severe head injury. Trauma Research and Education Foundation of San Diego. Arch Surg. 1997 Jun;132(6):592-7.
14. Gausche M, Lewis RJ, Stratton SJ, Haynes BE, Gunter CS, Goodrich SM, Poore PD, McCollough MD, Henderson DP, Pratt FD, Seidel JS. Effect of out-of-hospital pediatric endotracheal intubation on survival and neurological outcome: a controlled clinical trial. JAMA. 2000 Feb 9;283(6):783-90.
15. Davis DP, Hoyt DB, Ochs M, Fortlage D, Holbrook T, Marshall LK, Rosen P. Theeffect of paramedic rapid sequence intubation on outcome in patients with severe traumatic brain injury. J Trauma. 2003 Mar;54(3):444-53
16. Hartl R, Gerber LM, Iacono L, Ni Q, Lyons K, Ghajar J. Direct transport within an organized state trauma system reduces mortality in patients with severe traumatic brain injury. J Trauma. 2006 Jun;60(6):1250-6; discussion 1256.

Foundation for Medical and Technical Research and Education in Em
ergencies and Disasters
150 Question 4
N0. AUTHOR TYPE OF STUDY YEAR POPULATION INTERVENTION RESULT MEETS
REQUIREMENTS
1
Baker AJ, Rhind SG, Morrison LJ et al.
RCT 2009 Adults with severe skull trauma Glasgow < 8
250 ml of hyperto-nic saline solution 7.5% and dextran 70
Survival, GOS, GOS-E, FIM, DRS, Biomarkers
No, because it was not compa-red with normal saline solution
2
Bulger E, Jurkovich G, Nathens A et a
RCT 2008
Adults: subgroup of patients with closed skull trauma (Head AIS > 2) and at least 1 prehospital PAS 90 mmHg
250 ml hypertonic NaCl (7.5% NaCl in 6% dextran 70)
Acute respiratory distress syn-drome (ARDS) in the 28 days following the injury
No, because it was not compa-red with normal saline solution
3Bulger E, May S, Brasel K et al.
RCT 2010
Adult with closed skull trauma, GCS score <8 and PAS> 70 mmHg or 71-90 mmHg: cardiac rhythm >o= 108 bpm
Hypertonic saline solution and Dex-tran
Survival, GOS-E, DRS YES
4
Cooper DJ, Myles PS, McDermott FT et al
RCT 2004
Adult with closed skull trau-ma and GCS<9 and PAS <100 mmHg (includes polytrauma-tized patients)
250 ml of hyperto-nic saline solution 7.5%
Survival, GOS, GOS-E, GCS, FIM
No, because the intervention does not match requirements
5
Morrison LJ, Rizoli S, Schwartz B, Rhind S, Black S, Stuss DT
RCT 2006 Adult with closed skull trauma (GCS <9)
250 ml of hyperto-nic saline solution Survival, DRS, GOS-E
No, because it was not compa-red with normal saline solution
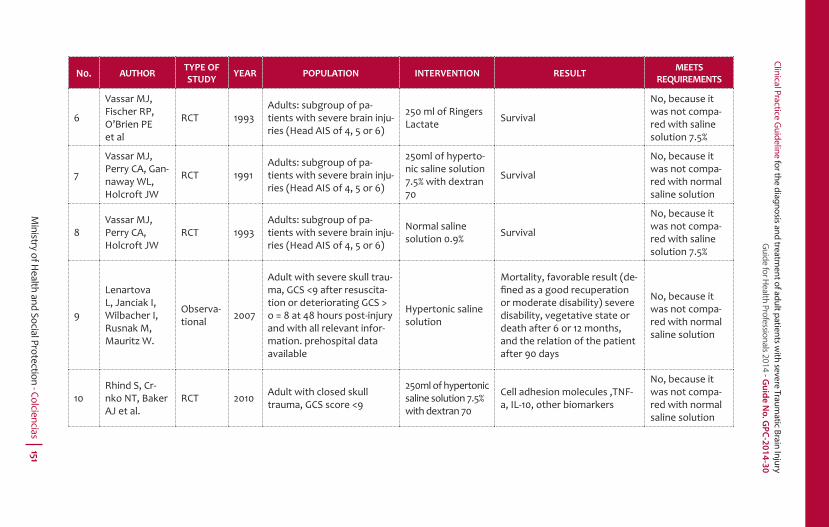
Clinical Practice Guideline for the diagnosis and treatm
ent of adult patients with severe Traum
atic Brain Injury G
uide for Health Professionals 2014 - G
uid
e N
o. G
PC
-20
14
-30
Ministry of H
ealth and Social Protection - Colciencias 151
N0. AUTHOR TYPE OF STUDY YEAR POPULATION INTERVENTION RESULT MEETS
REQUIREMENTS
6
Vassar MJ, Fischer RP, O’Brien PE et al
RCT 1993Adults: subgroup of pa-tients with severe brain inju-ries (Head AIS of 4, 5 or 6)
250 ml of Ringers Lactate Survival
No, because it was not compa-red with saline solution 7.5%
7
Vassar MJ, Perry CA, Gan-naway WL, Holcroft JW
RCT 1991Adults: subgroup of pa-tients with severe brain inju-ries (Head AIS of 4, 5 or 6)
250ml of hyperto-nic saline solution 7.5% with dextran 70
Survival
No, because it was not compa-red with normal saline solution
8Vassar MJ, Perry CA, Holcroft JW
RCT 1993Adults: subgroup of pa-tients with severe brain inju-ries (Head AIS of 4, 5 or 6)
Normal saline solution 0.9% Survival
No, because it was not compa-red with saline solution 7.5%
9
Lenartova L, Janciak I, Wilbacher I, Rusnak M, Mauritz W.
Observa-tional 2007
Adult with severe skull trau-ma, GCS <9 after resuscita-tion or deteriorating GCS > o = 8 at 48 hours post-injury and with all relevant infor-mation. prehospital data available
Hypertonic saline solution
Mortality, favorable result (de-fi ned as a good recuperation or moderate disability) severe disability, vegetative state or death after 6 or 12 months, and the relation of the patient after 90 days
No, because it was not compa-red with normal saline solution
10Rhind S, Cr-nko NT, Baker AJ et al.
RCT 2010 Adult with closed skull trauma, GCS score <9
250ml of hypertonic saline solution 7.5% with dextran 70
Cell adhesion molecules ,TNF-a, IL-10, other biomarkers
No, because it was not compa-red with normal saline solution
Foundation for Medical and Technical Research and Education in Emergencies and Disasters152
References1. Baker AJ, Rhind SG, Morrison LJ, Black S, Crnko NT, Shek NP, Rizolli
SB. Resusitacion with hypertronic saline – Dextran reduces serum biomarker levels and correlates with outcome in severe traumatic brain injury patients. J Neurotrauma. 2009; 26 : 1227-1240.
2. Bulger EM, May S, Brasel KJ, Schreiber M, Kerby JD, Tisherman SA, et al. Out of hospital hypertonic resuscitation following severe traumatic brain injury: a randomized controlled trial. JAMA. 2010; 304(13): 1455-1464.
3. Bulger EM, Jurkovich GJ, Nathens AB, Copass MK, Hanson S, Cooper C, et al. Hypertronic resuscitation of hypovolemic shock after blunt trauma, A Randomized Controlled Trial. Archsurg. 2008; 143 (2): 139148.
4. Cooper J, Myles PS, MCDermot FT, Murray LJ, Cooper G, Tremayne SS, et al. Prehospitalhypertronic saline resucitation of patients whit hypotension and severe traumatic brain injury, A randomized controlled trial. JAMA. 2004; 291(11): 1350-1357.
5. Morrison LJ, Rizoli S, Schwartz B, Rhind SG, Simitciu M, Perreira T, et al. The Toronto prehospital hypertronic resucitation-head injury and milti organ dysfunction trial (TOPHRHIT) - Methods and data collections tools. Trials. 2009; 10(105): 1-9
6. Vassar MJ, Perry CA, Holcroft JW. Analysis of potential risks associated with 7.5% sodium chloride resuscitation of traumatic shock. Arch Surg. 1990; 125: 1309-1315.
7. Vassar MJ, Perry CA, Gannaway PD, Holcroft JW. 7.5% sodium chloride/dextran for resicitation of trauma patients undergoing helicopter transport. Arch Surg. 1991; 126: 1065-1072.
8. Vassar MJ, Fischer RP, O’Brien PE, Bachulis BL, Chambers JA, Hoyt DB, et al. A multicenter trial for resuscitation of injured patients with 7.5% sodium chloride.Arch Surg. 1993; 128: 1003-1013.
9. Lenartova L, Janciak I, Wilbacher I, Rusnak M, Mauritz W. Severe traumatic brain injury in Austria III: Prehospital status and treatment. Eur J Med. 2007; 119 (1): 35-45.
10. Rhind SG, Cmko NT, Baker AJ, Morrison LJ, Shek PN, Scarpelli S, Rizoll SB. Prehospitalresucitacion with hipertronbic saline- Dextran modulates in lammatory, coagulation and endothelial activation marker pro iles in severe traumatic brain injured patients. J Neurin lamation. 2010; 7(5): 1-17.
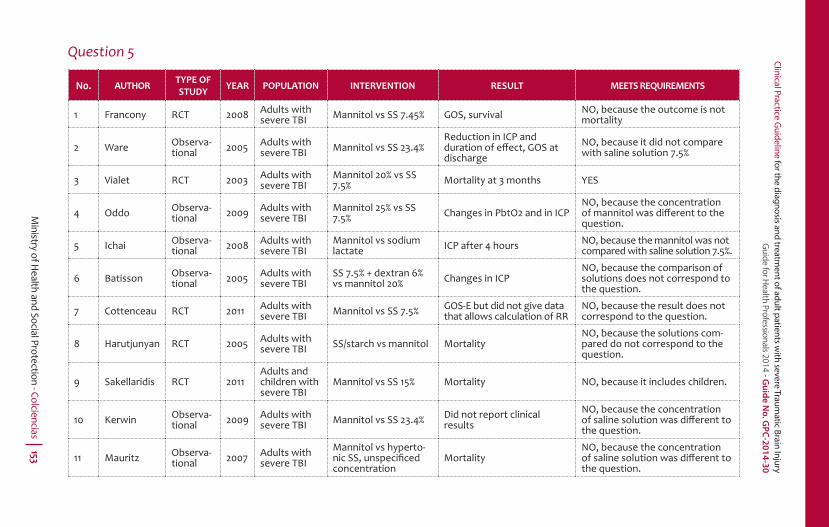
Clinical Practice Guideline for the diagnosis and treatm
ent of adult patients with severe Traum
atic Brain Injury G
uide for Health Professionals 2014 - G
uid
e N
o. G
PC
-20
14
-30
Ministry of H
ealth and Social Protection - Colciencias 153
Question 5
N0. AUTHOR TYPE OF STUDY YEAR POPULATION INTERVENTION RESULT MEETS REQUIREMENTS
1 Francony RCT 2008 Adults with severe TBI Mannitol vs SS 7.45% GOS, survival NO, because the outcome is not
mortality
2 Ware Observa-tional 2005 Adults with
severe TBI Mannitol vs SS 23.4%Reduction in ICP and duration of eff ect, GOS at discharge
NO, because it did not compare with saline solution 7.5%
3 Vialet RCT 2003 Adults with severe TBI
Mannitol 20% vs SS 7.5% Mortality at 3 months YES
4 Oddo Observa-tional 2009 Adults with
severe TBIMannitol 25% vs SS 7.5% Changes in PbtO2 and in ICP
NO, because the concentration of mannitol was diff erent to the question.
5 Ichai Observa-tional 2008 Adults with
severe TBIMannitol vs sodium lactate ICP after 4 hours NO, because the mannitol was not
compared with saline solution 7.5%.
6 Batisson Observa-tional 2005 Adults with
severe TBISS 7.5% + dextran 6% vs mannitol 20% Changes in ICP
NO, because the comparison of solutions does not correspond to the question.
7 Cottenceau RCT 2011 Adults with severe TBI Mannitol vs SS 7.5% GOS-E but did not give data
that allows calculation of RRNO, because the result does not correspond to the question.
8 Harutjunyan RCT 2005 Adults with severe TBI SS/starch vs mannitol Mortality
NO, because the solutions com-pared do not correspond to the question.
9 Sakellaridis RCT 2011Adults and children with severe TBI
Mannitol vs SS 15% Mortality NO, because it includes children.
10 Kerwin Observa-tional 2009 Adults with
severe TBI Mannitol vs SS 23.4% Did not report clinical results
NO, because the concentration of saline solution was diff erent to the question.
11 Mauritz Observa-tional 2007 Adults with
severe TBIMannitol vs hyperto-nic SS, unspecifi ced concentration
MortalityNO, because the concentration of saline solution was diff erent to the question.
Foundation for Medical and Technical Research and Education in Emergencies and Disasters154
References1. Francony G, Fauvage B, Falcon D, Canet C, Dilou H, Lavagne P. Equimolar
doses of manitol and hypertronic saline in the treatment of increased intracranial pressure. Crit Care Med. 2008; 36 (3): 795-800.
2. Ware M, Nemani V, Meeker M, Lee m, Morabito D, Manley G. Effects of 23,4% sodium choride solution in reducing intracranial pressure in patients whit traumatic Brain Injury: preliminary study. Neurosurgery. 2005; 57 (4); 727-736.
3. Vialet R, Albanese J, Tomachot L, Antonini F, Bourgouin A, Alliez B, Martin C. Isovolumhypertronic solutes (sodium chloride or manitol) in the Treatment of refactory posttraumatic intracranial Hypertension: 2 mL/kg 7.5% saline is more effective than 2mL/kg 20% mannitol. Crit Care Med. 2003 31 (6): 1683-1687.
4. Oddo M, Schimid M, Carrera E, Badjatia N, Connolly S, Presciutii M, et al. Impact of glycemic control on cerebral glucose metabolism after severe brain injury: a microdialysis study. Crit Care Med 2008: 36 (12); 3233 – 3238.
5. Battison C, Andrews P, Graham C, Petty T. Randomized controlled trial on the effect of a 20% mannitil solution and 7.5% saline dextran solution on increased intracranial pressure after brain injury. CritCare med. 2005; 33 (1): 196-202.
6. Harutjunyan, L., Holz, C., Menzel, M., Grond, S., Soukup, J., (2005); Ef iciency of 7.2% hypñertronic saline Hydroxyethlystarc 200/0.5 versus manitol 15% in the treatment of increased intracranial pressure in neurosurgical patients – a randomized clinical trial. critical care, 9 (5), pp 530-540. Doi: 10.1186/cc3767.
7. Sakelladiris N, Pavlou E, Karatzas S, Chroni D, Vlachos K, Chatzopoulos K. Comparison of manitol and hypertronic saline in the treatment of severe brain injuries. J Neurosurg. 2001; 114: 545-548.
8. Mauritz W, Janciak I, Wilbacher I, Rusnak, for the Austrian severe TBI study investigators. Wien KlinWochenschr. 2007; 119 (1-2): 46-55.
9. Cottenceau V1, Masson F, Mahamid E, Petit L, Shik V, Sztark F, Zaaroor M, Soustiel JF. Comparison of Effects of Equiosmolar Doses of Mannitol and Hypertonic Saline on Cerebral Blood Flow and Metabolism in Traumatic Brain Injury. J Neurotrauma. 2011 Oct;28(10):2003-12. doi: 10.1089/neu.2011.1929. Epub 2011 Sep 23.
10. Kerwin AJ, Shinco MA, Tepas JJ, Renfro WH, Pharm D. The use of 23.4% Hypertronic saline the management of elevated intracranial pressure in patients whit severe traumatic brain injury: a pilot study. J Trauma. 2009; 67: 277-282.
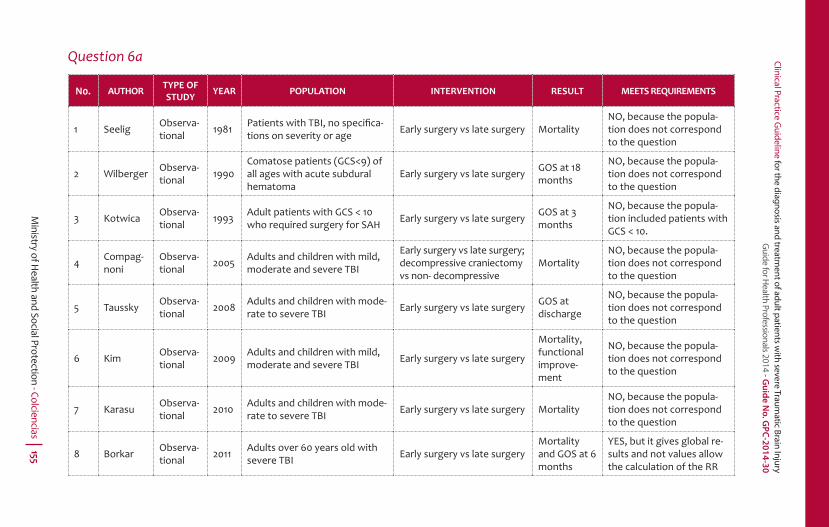
Clinical Practice Guideline for the diagnosis and treatm
ent of adult patients with severe Traum
atic Brain Injury G
uide for Health Professionals 2014 - G
uid
e N
o. G
PC
-20
14
-30
Ministry of H
ealth and Social Protection - Colciencias 155
Question 6a
N0. AUTHOR TYPE OF STUDY YEAR POPULATION INTERVENTION RESULT MEETS REQUIREMENTS
1 Seelig Observa-tional 1981 Patients with TBI, no specifi ca-
tions on severity or age Early surgery vs late surgery MortalityNO, because the popula-tion does not correspond to the question
2 Wilberger Observa-tional 1990
Comatose patients (GCS<9) of all ages with acute subdural hematoma
Early surgery vs late surgery GOS at 18 months
NO, because the popula-tion does not correspond to the question
3 Kotwica Observa-tional 1993 Adult patients with GCS < 10
who required surgery for SAH Early surgery vs late surgery GOS at 3 months
NO, because the popula-tion included patients with GCS < 10.
4 Compag-noni
Observa-tional 2005 Adults and children with mild,
moderate and severe TBI
Early surgery vs late surgery; decompressive craniectomy vs non- decompressive
MortalityNO, because the popula-tion does not correspond to the question
5 Taussky Observa-tional 2008 Adults and children with mode-
rate to severe TBI Early surgery vs late surgery GOS at discharge
NO, because the popula-tion does not correspond to the question
6 Kim Observa-tional 2009 Adults and children with mild,
moderate and severe TBI Early surgery vs late surgery
Mortality, functional improve-ment
NO, because the popula-tion does not correspond to the question
7 Karasu Observa-tional 2010 Adults and children with mode-
rate to severe TBI Early surgery vs late surgery MortalityNO, because the popula-tion does not correspond to the question
8 Borkar Observa-tional 2011 Adults over 60 years old with
severe TBI Early surgery vs late surgeryMortality and GOS at 6 months
YES, but it gives global re-sults and not values allow the calculation of the RR

Foundation for Medical and Technical Research and Education in Emergencies and Disasters156
References1. Seelig JM, Becker DP, Miller JD, Greenberg RP, Ward JD, Choi JC.
Traumatic Acute Subdural Hematoma, Major Mortality Reduction in Comatose Patients Treated within Four Hours. J Med 1981; 304:1511-1518.
2. Wilberger JE, Harris M, Diamond DL, Acute subdural hematoma: Morbidity and Mortality related to timing of operative intervention. J. Trauma. 1990; 30 (5): 733-736.
3. Kotwica Z, Brzezinski J, Acute subdural haematoma in adults: an analysis of otcome in comatose petients, ActaNeurochir. 1993; 121: 95-99.
4. Compagnone C, Murray GD, Teasdale GM, Maas AI, Esposito D, Princi P, et al. The management of patients whit intramural post-traumatic mass lesions: a multicenter Survey of current approaches to surgical management in 729 patients coordinated by the European brain injury consortium. Neurosurgery. 2005; 57 (6): 1183- 1192.
5. Taussky P, Widmer H, Takala J, Fandino J, Outcome after acute traumatic subdural and epidural hematoma in switzerland a single-centre experience. Swiss Med WKLY, 2008; 138 (19-20): 281-285.
6. Kim KH, Predictors for functional recovery and mortality of surgically treated traumatic acute subdural hematomas in 256 patients. J Korean Neurosurg. 2009: 45: 143-150.
7. Karasu A, Civelek E, Aras Y, Sabanci PA, Cansever T, Yanar H, et al. Analyses of clinical prognostic factors in operated traumatic acute subdural hematomas. Turkish journal of trauma & emergency surgery. 2010; 16 (3): 233-236.
8. Borkar SA, Sinha S, Agrawal D, Satyarthee GD, Gupta D, Mahapatra A M, Severe head injury in the ederly: risk factor assessment and outcome analysis in a series of 100 consecutive patients at level 1 trauma centre. IJNT. 2011; 8 (2): 77-82.

Clinical Practice Guideline for the diagnosis and treatm
ent of adult patients with severe Traum
atic Brain Injury G
uide for Health Professionals 2014 - G
uid
e N
o. G
PC
-20
14
-30
Ministry of H
ealth and Social Protection - Colciencias 157
Question 6b
N0. AUTHOR TYPE OF STUDY YEAR POPULATION INTERVENTION RESULT MEETS REQUIREMENTS
1 Lee Observational, retrospective 1998 Patients with epidural hematomas
requiring surgery, GCS 3-15Early surgery vs late surgery GOS at 1 year NO, because it included
patients with GCS >8.
2 Cohen Observational, prospective 1996 21 adult patients GCS < 8 Early surgery vs
late surgeryNot documen-ted
NO, because the results were not published
3 Kotwica Observational, retrospective 1993
Adult patients with GCS < 10 who required surgical treatment for SAH
Early surgery vs late surgery
GOS at 3 months
NO, because it included patients with GCS >8.
4 Sakas Observational 1995Patients with TBI who required craniectomy and were in a state of coma
Early surgery vs late surgery
Mortality, funcional recuperation
NO, because it was limited to patients in a coma
5 Taussky Observational, restrospective 2008 Adults and children with moderate
to severe TBIEarly surgery vs late surgery
GOS at dis-charge
NO, the population does not correspond to the question

Foundation for Medical and Technical Research and Education in Emergencies and Disasters158
References1. Lee, E., Hung, Y., Wang L., Chung, K., Chen, H., (1998). Factors
in luencing the functional outcome of patients whit acute epidural hematomas: analysis of 200 patients undergoing surgery. Journal Trauma. 45, pp. 48-57.
2. Cohen, J., Montero, A., Israel, Z., (1996).Prognosis and clinical relevance of anisicoria-craniotomy latency for epidural hematoma in comatose patients. J Trauma. 41, pp. 120-122.
3. Kotwica Z, Brzezinski J, Acute subdural haematoma in adults: an analysis of otcome in comatose petients, ActaNeurochir. 1993; 121: 95-99.
4. Sakas, D., Bullock, M., Teasdale, G., (1995). One- year outcome following craniotomy for traumatic hematoma in patients whit ixed dilated pupils. Journal Neurosurg. 82, pp. 961-965
5. Taussky P, Widmer H, Takala J, Fandino J, Outcome after acute traumatic subdural and epidural hematoma in switzerland a single-centre experience. Swiss Med WKLY, 2008; 138 (19-20): 281-285
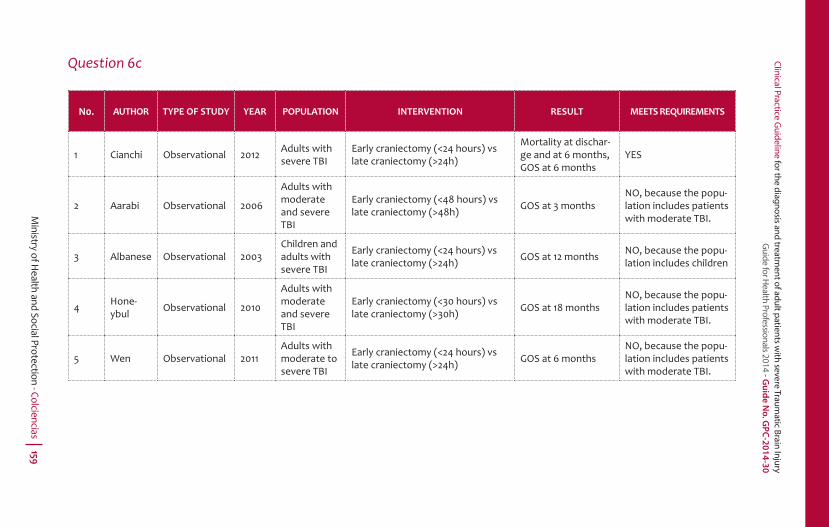
Clinical Practice Guideline for the diagnosis and treatm
ent of adult patients with severe Traum
atic Brain Injury G
uide for Health Professionals 2014 - G
uid
e N
o. G
PC
-20
14
-30
Ministry of H
ealth and Social Protection - Colciencias 159
Question 6c
N0. AUTHOR TYPE OF STUDY YEAR POPULATION INTERVENTION RESULT MEETS REQUIREMENTS
1 Cianchi Observational 2012 Adults with severe TBI
Early craniectomy (<24 hours) vs late craniectomy (>24h)
Mortality at dischar-ge and at 6 months, GOS at 6 months
YES
2 Aarabi Observational 2006
Adults with moderate and severe TBI
Early craniectomy (<48 hours) vs late craniectomy (>48h) GOS at 3 months
NO, because the popu-lation includes patients with moderate TBI.
3 Albanese Observational 2003Children and adults with severe TBI
Early craniectomy (<24 hours) vs late craniectomy (>24h) GOS at 12 months NO, because the popu-
lation includes children
4 Hone-ybul Observational 2010
Adults with moderate and severe TBI
Early craniectomy (<30 hours) vs late craniectomy (>30h) GOS at 18 months
NO, because the popu-lation includes patients with moderate TBI.
5 Wen Observational 2011Adults with moderate to severe TBI
Early craniectomy (<24 hours) vs late craniectomy (>24h) GOS at 6 months
NO, because the popu-lation includes patients with moderate TBI.
Foundation for Medical and Technical Research and Education in Emergencies and Disasters160
References 1. Albanese J, Leone M, Alliez JR, Kaya JM, Antonini F. Decompresive
craniectomy for severe traumatic brain injury evaluation of the effects at one year. Crit care Med. 2003; 31: 2535-2538.
2. Aarabi B, Hesdorfer DC, Ahn ES, Aresco C, Scalea TM, Eisengber HM. Outcome following decompressive craniectomy for malignant swelling due to severe head injury. J Neurosurg. 2006; 104: 469-479.
3. Wen H, Wang F, Wang JB, Gong GL, Huang R, Y Zhan, F Yang. A prospective study of early versus late craniectomy after traumatic brain injury. Brain Inj. 2011; 25 (13): 1318-1324.
4. Honeybul S, Ho K.M, Lind PC R, Guillett GR. Surgical intervention for severe head injury: ethical considerations when performing life-saving but non-restorative surgery. Actaneurochir. 2011;153: 1105-1110.
5. Cianchi G, Bonizzoli M, Zagli G, Valvasone S, Ciapetti M, Perreta L, Mariotti F, Peris A. Late decompressivecraniectomy traumatic brain injury: neurological outcome at 6 months after ICU discharge. J Trauma. 2012; 6 (8): 1-6.
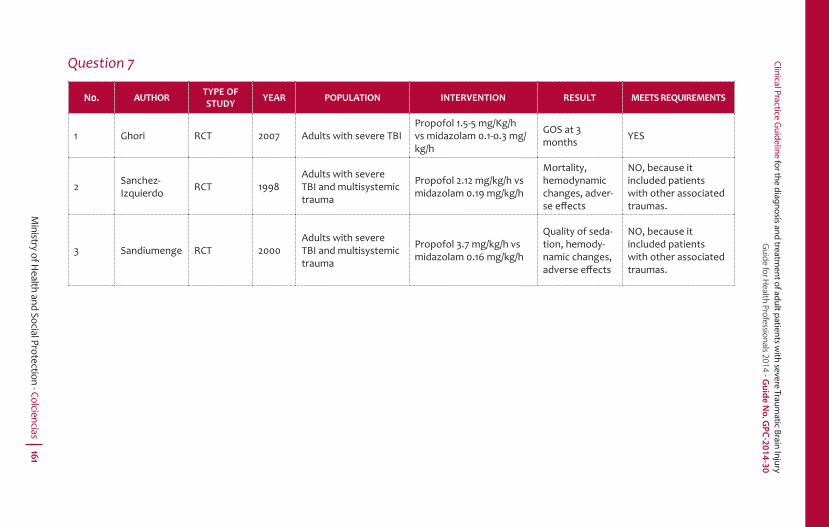
Clinical Practice Guideline for the diagnosis and treatm
ent of adult patients with severe Traum
atic Brain Injury G
uide for Health Professionals 2014 - G
uid
e N
o. G
PC
-20
14
-30
Ministry of H
ealth and Social Protection - Colciencias 161
Question 7
N0. AUTHOR TYPE OF STUDY YEAR POPULATION INTERVENTION RESULT MEETS REQUIREMENTS
1 Ghori RCT 2007 Adults with severe TBIPropofol 1.5-5 mg/Kg/h vs midazolam 0.1-0.3 mg/kg/h
GOS at 3 months YES
2 Sanchez-Izquierdo RCT 1998
Adults with severe TBI and multisystemic trauma
Propofol 2.12 mg/kg/h vs midazolam 0.19 mg/kg/h
Mortality, hemodynamic changes, adver-se eff ects
NO, because it included patients with other associated traumas.
3 Sandiumenge RCT 2000Adults with severe TBI and multisystemic trauma
Propofol 3.7 mg/kg/h vs midazolam 0.16 mg/kg/h
Quality of seda-tion, hemody-namic changes, adverse eff ects
NO, because it included patients with other associated traumas.
Foundation for Medical and Technical Research and Education in Emergencies and Disasters162
References 1. Ghori KA, Harmon DC, Elashaal, Walsh F, O’Sullivan M, Shorten G. Effect
of midazolam versus Propofol sedation on markers of neurological injury and outcome after isolated severe head injury: a pilot study. Crit Care Resusc. 2007; 9: 166-171.
2. Sanchez- Izquierdo JA, Caballero Cubedo RE, Perez VJL, Ambros CAA, Santadiago CJA, Alted LE. Propofol versus Midazolam: Safety and ef icacy for sedating the severe trauma patient. AnesthAnalg. 1998; 86: 1219-1224.
3. Sandiumenge A, Sanchez I JA, Vazques DT, Borges MS, Peinado R J, Alted LE. Midazolam and 2% Propofol in long-term sedation of traumatized critically ill patients: ef icacy and safety comparison. Crit Care Med. 2000; 28 (11): 3612- 3618.

Clinical Practice Guideline for the diagnosis and treatm
ent of adult patients with severe Traum
atic Brain Injury G
uide for Health Professionals 2014 - G
uid
e N
o. G
PC
-20
14
-30
Ministry of H
ealth and Social Protection - Colciencias 163
Question 8
N0. AUTHOR TYPE OF STUDY YEAR POPULATION INTERVENTION RESULT MEETS REQUIREMENTS
1 Ali Case studies and controls
2013 > 15 years with TBI and ICH
Lenox 30 mg sc two times per day (normal creatinine or Hepa-rin 5000 3 times per day TFG < 30 24 hours post-trauma
Group A without using protocol, group B followed protocol
NO, because it inclu-ded patients under 16 years old.
2 Scott Observational prospective
2002Cohorts
Adults with TBI and ICH. AIS> 3
Enoxaparin 30 mg sc every 12 hours, 24 hours of initial evalua-tion im emergency department
No control group
NO, because there was no comparison with unfractionated heparin.
3 ScottObservational, prospective study
2008 > 14 years old, blunt TBI
Enoxaparin 30 mg sc every 12 hours, 24 hours initially No control group
NO, because the population is under 16 years old.
4 Minshall Observational 2011 HAIS > 2, > 16 years old, TBI
Compared LMWH 30 mg sc every 12 hours with UFH 5000 u sc three times per day
YES
5 Salottolo Observational 2011 TBI , > 18 years old
External compression, LMWH 30 mg sc every 12 hours
Compared time of beginning thrombo prophylaxis
NO, because there was no comparison with unfractionated heparin.
6 Donald 2009Penetrating brain injury, sin TBI
UFH or LMWHNo prophylaxis, 0-24 hours, 24-48 hours, > 48 hours
NO, because the population does not correspond with the question.

Foundation for Medical and Technical Research and Education in Emergencies and Disasters164
References1. Farooqui A, Hiser B, Barnes SL, Litofsky. Safety and ef icacy of early
thromboembolism chemoprophylaxis after intracranial hemorrhage from traumatic brain injury. J Neurosurg. 2013; 199: 1576- 1582.
2. Norwood SH, McAuley CE, Berne JD, Vallina VL, Kerns BD, Grahm TW. Prospective evaluation of safety of enoxaparin pro hylaxis for venous tromboembolism in patients with intracranial hemorrhagic injuries. Arch Surg. 2002; 137 : 696-702.
3. Norwood SH, Berne JD, Stephen A, Rowe SA, Villarreal DH, ledie JT. Early venous thromboembolism prophylaxis whit enoxaparin in patients with blunt traumatic brain injury. J Trauma. 2008; 65 (8): 1021-1027.
4. Minshall, C.T., Erockson, E.A., Leon M. S., Doben, A.R., Mckinzie, B.P., Fakhry, S.M., (2011). Safety and Ef icacy of heparin or enoxaparin prophylaxis in blunt trauma patients whit a head abbreviated injury severity score >2. Thejournal of trauma. 71 (2), pp. 396-400.
5. Salottolo K, offner P, Stewart L, Mains WC, Slone DS, Bar-Or D, Interrupted pharmacologic tromboprophylaxisicreases venous thromboembolism in traumatic brain injury. J Trauma. 2011; 70 (1): 19-26.
6. Reiff DA, Haricharan RN, BullingtonNM, Grif in RL, Rue WL. Traumatic brain injury is associated with the development of deep vein thrombosis independent of pharmacological prophylaxis. 2009; 66: 1436-1440.
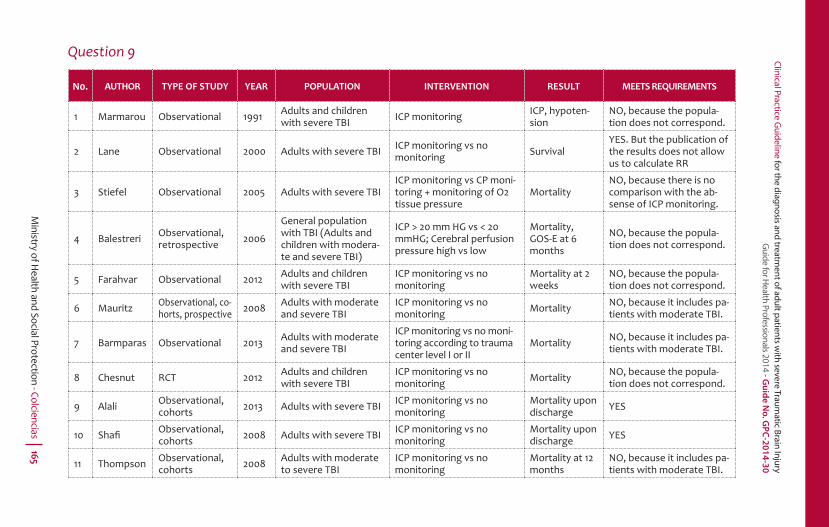
Clinical Practice Guideline for the diagnosis and treatm
ent of adult patients with severe Traum
atic Brain Injury G
uide for Health Professionals 2014 - G
uid
e N
o. G
PC
-20
14
-30
Ministry of H
ealth and Social Protection - Colciencias 165
Question 9
N0. AUTHOR TYPE OF STUDY YEAR POPULATION INTERVENTION RESULT MEETS REQUIREMENTS
1 Marmarou Observational 1991 Adults and children with severe TBI ICP monitoring ICP, hypoten-
sionNO, because the popula-tion does not correspond.
2 Lane Observational 2000 Adults with severe TBI ICP monitoring vs no monitoring Survival
YES. But the publication of the results does not allow us to calculate RR
3 Stiefel Observational 2005 Adults with severe TBIICP monitoring vs CP moni-toring + monitoring of O2 tissue pressure
MortalityNO, because there is no comparison with the ab-sense of ICP monitoring.
4 Balestreri Observational, retrospective 2006
General population with TBI (Adults and children with modera-te and severe TBI)
ICP > 20 mm HG vs < 20 mmHG; Cerebral perfusion pressure high vs low
Mortality, GOS-E at 6 months
NO, because the popula-tion does not correspond.
5 Farahvar Observational 2012 Adults and children with severe TBI
ICP monitoring vs no monitoring
Mortality at 2 weeks
NO, because the popula-tion does not correspond.
6 Mauritz Observational, co-horts, prospective 2008 Adults with moderate
and severe TBIICP monitoring vs no monitoring Mortality NO, because it includes pa-
tients with moderate TBI.
7 Barmparas Observational 2013 Adults with moderate and severe TBI
ICP monitoring vs no moni-toring according to trauma center level I or II
Mortality NO, because it includes pa-tients with moderate TBI.
8 Chesnut RCT 2012 Adults and children with severe TBI
ICP monitoring vs no monitoring Mortality NO, because the popula-
tion does not correspond.
9 Alali Observational, cohorts 2013 Adults with severe TBI ICP monitoring vs no
monitoringMortality upon discharge YES
10 Shafi Observational, cohorts 2008 Adults with severe TBI ICP monitoring vs no
monitoringMortality upon discharge YES
11 Thompson Observational, cohorts 2008 Adults with moderate
to severe TBIICP monitoring vs no monitoring
Mortality at 12 months
NO, because it includes pa-tients with moderate TBI.

Foundation for Medical and Technical Research and Education in Emergencies and Disasters166
References1. Marmarou A, Anderson R L, Ward D, Choi SC, Young HF. Impact of ICP
instability and hypotension on outcome in patients with severe head trauma. J Neurosurg. 1991; 75: 1-8.
2. Lane P, Skoretz TG, Doig G, Girotti. Intracranial pressure monitoring and outcomes after traumatic brain injury. CMA. 2000; 43 (6): 442-448.
3. Stiefel M, Spiota A, Gracias VH, Garuffe AM, Guillamondegui O, Wilensky EM, Et al. Reduced mortality rate in patients whit severe traumatic brain injury treated whit brain tissue oxygen monitoring. J Neurosurg. 2005; 103: 805-811.
4. 4) Balestreri, M., Czosnyka,M., Hutchinson, P., Steiner, L.A., Hiler, M., Smielewski, P., Pickard, D., (2006). Impact of intracranial pressure and cerebral perfusion pressure on severe disability and mortality after head injury. Neurocritical Care. 2006; 04:8–13.
5. Mauritz W, stelzer H, Bauer P, Aghamanoukjan DL, Metnitz P. Monitoring of intracranial pressure in patients with severe traumatic brain injury: an Austrian prospective multicenter study. Intensive Care Med. 2008; 34: 1208-1215.
6. Farahvar A, Gerber LM, Chiu YL, Carney N, Hartl R, Ghajar J. Increased mortality in patients with severe traumatic brain injury treated without intracranial pressure monitoring. J Neurosurg. 2012; 117 (4): 729-34.
7. Barmparas G, Singer M, Ley E, Chung R, Malinoski D, Margulies D, Salim A, Bukur M. Decreased intracranial pressure monitor use at level II trauma centers is associated with increased mortality. Division of Acute Care Surgery, Cedars-Sinai Medical Center. 2012: 78(10): 1166-1171.
8. Thompson HJ, Rivara FP, Jurkovich GJ, Wang J, Nathens AB, Mackenzie E. Evaluation of the effecte of intensity of care on mortality after traumatic brain injury. Crit Care Med. 2008; 36 (1): 282-290.
9. Sha i S, Diaz-Arrastia R, Madden C, Gentilello L., (2008). Intracranial pressure monitoring in brain-injured patients is associated with worsening of survival. J Trauma. 64 (2), pp. 335-40.
10. Alali AS, Fowler RA, Mainprize TG, Scales DC, Kiss A, de Mestral C, Ray JG, Nathens AB., (2013). Intracranial pressure monitoring in severe traumatic brain injury: results from the American College of Surgeons Trauma Quality Improvement Program. Journal of Neurotrauma. 30 (20), pp. 1737-46.
11. Chesnut, R.M., Temkin, N., Carney, N., Dikmen, S., Rondina, C., Videtta, W., Petroni, G., Lujan,S., Pridgeon, J., Barber,J., Machamer, J., Chaddock, K., Celix, J.M., Cherner, M., Hendrix,T., (2012). A Trial of Intracranial-Pressure Monitoring in Traumatic Brain Injury. NEJM. 367 (26).

Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 167
Question 10
N0. AUTHOR TYPE OF STUDY YEAR POPULATION INTERVENTION RESULT
MEETS REQUIRE-
MENTS
1 Harris RCT 2009 Adults, GCS < 8
Cooling cap vs no cooling cap
Mortality, GOS, FIM YES
2 Liu RCT 2006 Adults with severe TBI
Cooling head and neck vs mild system-atic hypother-mia vs not exposed to hypothermia
GOS YES
3 Qiu RCT 2006 Adults with severe TBI
Selective brain cooling vs nor-mothermia
GOS 6 months YES
References1. Harris OA, Muh CR, Surles MC, Pan Y, Rozycki G, Macleod J,
Easley K. Discrete cerebral hypothermia in the management of traumatic brain injury: a randomized controlled trial. J Neurosurg. 2009 Jun; 110(6):1256-64.
2. Liu WG, Qiu WS, Zhang Y, Wang WM, Lu F, Yang. Effects of selective brain cooling in patients with severe traumatic brain injury: a preliminary study. J IntMed Res. 2006;34(1):58-64.
3. Qiu W, Shen H, Zhang Y, Wang W, Liu W, Jiang Q, Luo M, Manou M. Non invasive selective brain cooling by head and neck cooling is protective in severe traumatic brain injury. J Clin Neurosci. 2006;13(10):995-1000.
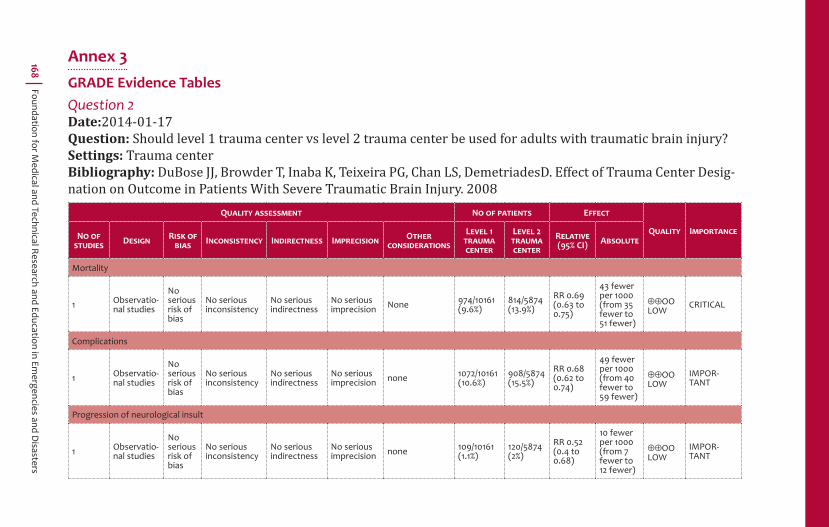
Foundation for Medical and Technical Research and Education in Em
ergencies and Disasters
168
Annex 3GRADE Evidence TablesQuestion 2Date:2014-01-17Question: Should level 1 trauma center vs level 2 trauma center be used for adults with traumatic brain injury?Settings: Trauma centerBibliography: DuBose JJ, Browder T, Inaba K, Teixeira PG, Chan LS, DemetriadesD. Effect of Trauma Center Desig-nation on Outcome in Patients With Severe Traumatic Brain Injury. 2008
QUALITY ASSESSMENT NO OF PATIENTS EFFECT
QUALITY IMPORTANCENO OF STUDIES DESIGN RISK OF
BIAS INCONSISTENCY INDIRECTNESS IMPRECISION OTHERCONSIDERATIONS
LEVEL 1 TRAUMA CENTER
LEVEL 2 TRAUMA CENTER
RELATIVE(95% CI) ABSOLUTE
Mortality
1 Observatio-nal studies
No serious risk of bias
No serious inconsistency
No serious indirectness
No serious imprecision None 974/10161
(9.6%)814/5874 (13.9%)
RR 0.69 (0.63 to 0.75)
43 fewer per 1000 (from 35 fewer to 51 fewer)
OOLOW
CRITICAL
Complications
1 Observatio-nal studies
No serious risk of bias
No serious inconsistency
No serious indirectness
No serious imprecision none 1072/10161
(10.6%)908/5874 (15.5%)
RR 0.68 (0.62 to 0.74)
49 fewer per 1000 (from 40 fewer to 59 fewer)
OOLOW
IMPOR-TANT
Progression of neurological insult
1 Observatio-nal studies
No serious risk of bias
No serious inconsistency
No serious indirectness
No serious imprecision none 109/10161
(1.1%)120/5874 (2%)
RR 0.52 (0.4 to 0.68)
10 fewer per 1000 (from 7 fewer to 12 fewer)
OOLOW
IMPOR-TANT

Clinical Practice Guideline for the diagnosis and treatm
ent of adult patients with severe Traum
atic Brain Injury G
uide for Health Professionals 2014 - G
uid
e N
o. G
PC
-20
14
-30
Ministry of H
ealth and Social Protection - Colciencias 169
Question 3Date: 2013-09-26Question: Should Prehospital intubation vs hospital intubation be used for adults with severe trauma brain injury?Settings: Bibliography: Bernard SA, Nguyen V, Cameron P, Masci K, Fitzgerald M, Cooper DJ et al. Prehospital rapid se-quence intubation improves functional outcome for patients with severe traumatic brain injury: a randomized controlled trial. AnnSurg. 2010;252(6):959-65.
QUALITY ASSESSMENT NO OF PATIENTS EFFECT
QUALITY IMPORTANCENO OF STUDIES DESIGN RISK OF
BIAS INCONSISTENCY INDIRECTNESS IMPRECISIONOTHER CONSIDE-RATIONS
PREHOSPITAL INTUBATION
HOSPITAL INTUBATION
RELATIVE(95% CI) ABSOLUTE
1. Mortality (follow-up 6 months; assessed with: Glasgow Outcome Scale (GOSe) score equal to one (1) at 6 months after injury)
1 Randomised trials
No serious risk of bias
No serious inconsistency
No serious indirectness Serious1 None 53/157
(33.8%)55/142 (38.7%)
RR 0.87 (0.64 to 1.18)
50 fewer per 1000 (from 139 fewer to 70 more)
OMODERATE
CRITICAL
2. Bad neurologic outcome (follow-up 6 months; assessed with: Glasgow Outcome Scale (GOSe) score between 2 and 4 at 6 months after injury)
1 Randomised trials
No serious risk of bias
No serious inconsistency
No serious indirectness Serious1 None 24/157
(15.3%)31/148 (20.9%)
RR 0.70 (0.43 to 1.13)
63 fewer per 1000 (from 119 fewer to 27 more)
OMODERATE
CRITICAL
3. Good neurologic outcome (follow-up 6 months; assessed with: Glasgow Outcome Scale (GOSe) score between 5 and 8 at 6 months after injury)
1 Randomised trials
No serious risk of bias
No serious inconsistency
No serious indirectness Serious2 None 80/157
(51%)56/142 (39.4%)
RR 1.29 (1 to 1.67)
114 more per 1000 (from 0 more to 264 more)
OMODERATE
CRITICAL
1 The 95% con idence appreciable bene it or appreciable harm.2 The 95% con idence interval included no bene it or appreciable bene it.
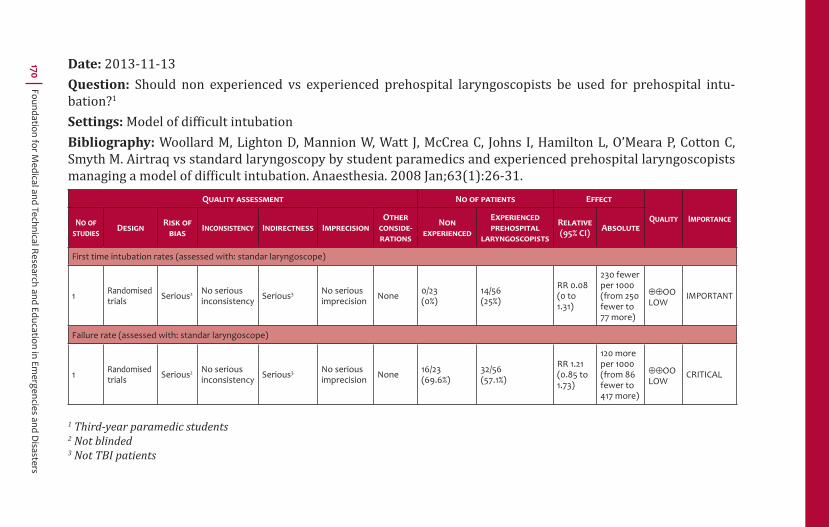
Foundation for Medical and Technical Research and Education in Em
ergencies and Disasters
170 Date: 2013-11-13Question: Should non experienced vs experienced prehospital laryngoscopists be used for prehospital intu-bation?1
Settings: Model of diffi cult intubationBibliography: Woollard M, Lighton D, Mannion W, Watt J, McCrea C, Johns I, Hamilton L, O’Meara P, Cotton C, Smyth M. Airtraq vs standard laryngoscopy by student paramedics and experienced prehospital laryngoscopists managing a model of dif icult intubation. Anaesthesia. 2008 Jan;63(1):26-31.
QUALITY ASSESSMENT NO OF PATIENTS EFFECT
QUALITY IMPORTANCENO OF STUDIES DESIGN RISK OF
BIAS INCONSISTENCY INDIRECTNESS IMPRECISIONOTHER CONSIDE-RATIONS
NON EXPERIENCED
EXPERIENCED PREHOSPITAL
LARYNGOSCOPISTS
RELATIVE(95% CI) ABSOLUTE
First time intubation rates (assessed with: standar laryngoscope)
1 Randomised trials Serious2 No serious
inconsistency Serious3 No serious imprecision None 0/23
(0%)14/56 (25%)
RR 0.08 (0 to 1.31)
230 fewer per 1000 (from 250 fewer to 77 more)
OOLOW
IMPORTANT
Failure rate (assessed with: standar laryngoscope)
1 Randomised trials Serious2 No serious
inconsistency Serious3 No serious imprecision None 16/23
(69.6%)32/56 (57.1%)
RR 1.21 (0.85 to 1.73)
120 more per 1000 (from 86 fewer to 417 more)
OOLOW
CRITICAL
1 Third-year paramedic students2 Not blinded3 Not TBI patients

Clinical Practice Guideline for the diagnosis and treatm
ent of adult patients with severe Traum
atic Brain Injury G
uide for Health Professionals 2014 - G
uid
e N
o. G
PC
-20
14
-30
Ministry of H
ealth and Social Protection - Colciencias 171
Question 4Date: 2013-10-21Question: Should hypertonic saline vs SS 0.9% be used for adults with severe TBI?Settings: PrehospitalBibliography: Bulger E, May S, Brasel K et al. Out of hospital hypertonic resuscitation following severe traumatic brain injury 2010
QUALITY ASSESSMENT NO OF PATIENTS EFFECT
QUALITY IMPORTANCENO OF STUDIES DESIGN
RISK OF BIAS
INCONSISTENCY INDIRECTNESS IMPRECISION OTHER CON-SIDERATIONS
HYPERTONIC SALINE SS 0.9% RELATIVE
(95% CI) ABSOLUTE
Survival at hospital discharge (follow-up 28 days; assessed with: survival (Bulger 2010))
1 Randomised trials
No serious risk of bias
No serious inconsistency
No serious indirectness Serious None 171/293
(58.4%)276/492 (56.1%)
RR 1.04 (0.91 to 1.17)
22 more per 1000 (from 50 fewer to 95 more)
OMODERATE
CRITICAL
Bad neurological outcome (follow-up 6 months; assessed with: GOSe< o igual a 4)
1 Randomised trials
No serious risk of bias
No serious inconsistency
No serious indirectness Serious1 None 171/341
(50.1%)276/582 (47.4%)
RR 1.05 (0.92 to 1.21)
24 more per 1000 (from 38 fewer to 100 more)
OMODERATE
CRITICAL
1 The 95% con idence appreciable bene it or appreciable harm
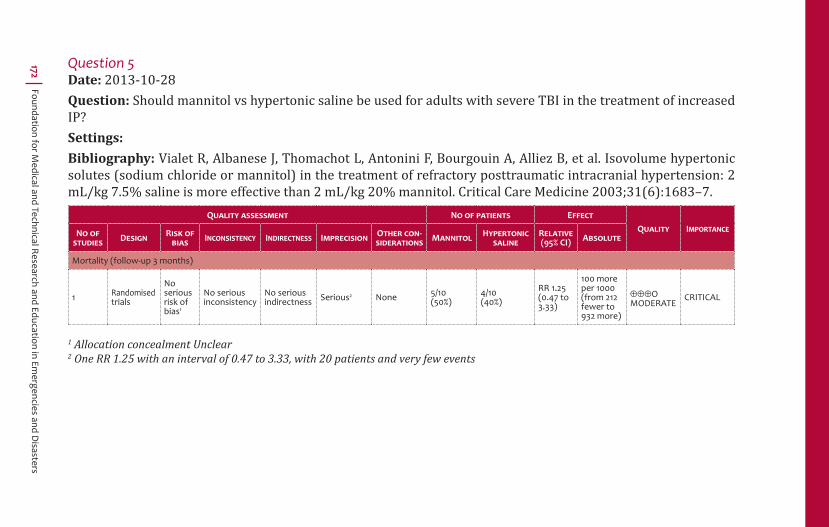
Foundation for Medical and Technical Research and Education in Em
ergencies and Disasters
172 Question 5Date: 2013-10-28Question: Should mannitol vs hypertonic saline be used for adults with severe TBI in the treatment of increased IP?Settings: Bibliography: Vialet R, Albanese J, Thomachot L, Antonini F, Bourgouin A, Alliez B, et al. Isovolume hypertonic solutes (sodium chloride or mannitol) in the treatment of refractory posttraumatic intracranial hypertension: 2 mL/kg 7.5% saline is more effective than 2 mL/kg 20% mannitol. Critical Care Medicine 2003;31(6):1683–7.
QUALITY ASSESSMENT NO OF PATIENTS EFFECTQUALITY IMPORTANCENO OF
STUDIES DESIGN RISK OF BIAS INCONSISTENCY INDIRECTNESS IMPRECISION OTHER CON-
SIDERATIONS MANNITOL HYPERTONIC SALINE
RELATIVE(95% CI) ABSOLUTE
Mortality (follow-up 3 months)
1 Randomised trials
No serious risk of bias1
No serious inconsistency
No serious indirectness Serious2 None 5/10
(50%)4/10 (40%)
RR 1.25 (0.47 to 3.33)
100 more per 1000 (from 212 fewer to 932 more)
OMODERATE
CRITICAL
1 Allocation concealment Unclear2 One RR 1.25 with an interval of 0.47 to 3.33, with 20 patients and very few events

Clinical Practice Guideline for the diagnosis and treatm
ent of adult patients with severe Traum
atic Brain Injury G
uide for Health Professionals 2014 - G
uid
e N
o. G
PC
-20
14
-30
Ministry of H
ealth and Social Protection - Colciencias 173
Question 6cDate: 2013-10-28Question: Should early craniectomy vs late craniectomy be used for adults with severe TBI in patients with re-fractory intracranial hypertension?Settings: Patients admitted to the ICU of the Emergency DepartmentBibliography: Cianchi G, Bonizzoli M, Zagli G, di Valvasone S, Biondi S, Ciapetti M, Perretta L, Mariotti F, Peris A. Late decompressive craniectomy after traumatic brain injury: neurological outcome at 6 months after ICU dis-charge. 2012.
QUALITY ASSESSMENT NO OF PATIENTS EFFECTQUALITY IMPORTANCENO OF
STUDIES DESIGN RISK OF BIAS INCONSISTENCY INDIRECTNESS IMPRECISION OTHER CON-
SIDERATIONSEARLY
CRANIECTOMYLATE
CRANIECTOMYRELATIVE(95% CI) ABSOLUTE
Mortality (assessed with: ICU mortality)
1 Observational studies1 Serious No serious
inconsistencyNo serious indirectness Serious2 None 12 cases 6 controls
OR 1.02 (0.44 to 2.34)
-OOOVERY LOW
CRITICAL
28.6%
4 more per 1000 (from 136 fewer to 198 more)
Good Neurological outcome (timing of exposure 6 months; assessed with: Glasgow Outcome Scale at 6 months)
1 Observational studies1
No serious risk of bias
No serious inconsistency
No serious indirectness
No serious imprecision none
41 cases 21 controlsOR 3.3 (0 to 0)
-OOLOW
CRITICAL 0% -
1 Case-control2 Small sample

Foundation for Medical and Technical Research and Education in Em
ergencies and Disasters
174 Question 7Date: 2013-10-10Question: Should Propofol vs Midazolam be used for sedation in patients with severe traumatic brain injury?Settings: Intensive careBibliography: Sanchez-Izquierdo-Riera JA, Caballero-Cubedo RE, Perez-Vela JL, Ambros-Checa A, Cantalapiedra-Santiago JA, Alted-Lopez E. Propofol versus midazolam: safety and ef icacy for sedating the severe trauma patient. Anesth Analg. 1998 Jun;86(6):1219-24. Ghori KA et al. Effect of midazolam versus propofol sedation on markers of neurological injury and outcome after isolated severe head injury: a pilot study. CritCareResusc 2007; 9: 166:171
QUALITY ASSESSMENT NO OF PATIENTS EFFECTQUALITY IMPORTANCENO OF
STUDIES DESIGN RISK OF BIAS INCONSISTENCY INDIRECTNESS IMPRECISION OTHER
CONSIDERATIONS PROPOFOL MIDAZOLAM RELATIVE(95% CI) ABSOLUTE
1. Serum triglyceride concentration (measured with: laboratory biochemical determination every third day; Better indicated by lower values)
1 Randomised trials None 33 34 -
MD 99.00 higher (16.4 to 181.6 higher)
Good neurological outcome (follow-up 3 months; assessed with: GOS 4-5)
1 Randomised trials Serious1 No serious
inconsistencyNo serious indirectness
No serious imprecision None 7/13
(53.8%)8/15 (53.3%)
RR 1.00 (0.50 to 2.01)
O fewer per 1000 (from 267 fewer to 539 more)
OMODERATE
CRITICAL
1 No blinding
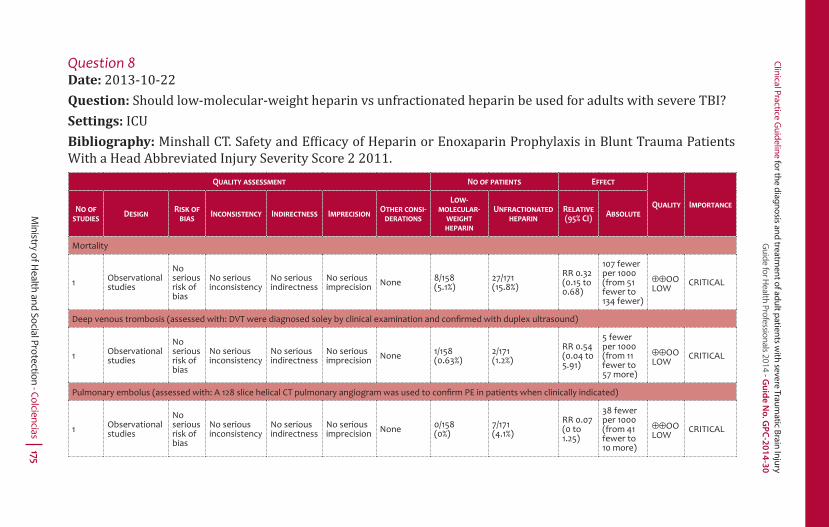
Clinical Practice Guideline for the diagnosis and treatm
ent of adult patients with severe Traum
atic Brain Injury G
uide for Health Professionals 2014 - G
uid
e N
o. G
PC
-20
14
-30
Ministry of H
ealth and Social Protection - Colciencias 175
Question 8Date: 2013-10-22Question: Should low-molecular-weight heparin vs unfractionated heparin be used for adults with severe TBI?Settings: ICUBibliography: Minshall CT. Safety and Ef icacy of Heparin or Enoxaparin Prophylaxis in Blunt Trauma Patients With a Head Abbreviated Injury Severity Score 2 2011.
QUALITY ASSESSMENT NO OF PATIENTS EFFECT
QUALITY IMPORTANCENO OF STUDIES DESIGN RISK OF
BIAS INCONSISTENCY INDIRECTNESS IMPRECISION OTHER CONSI-DERATIONS
LOW-MOLECULAR-
WEIGHT HEPARIN
UNFRACTIONATED HEPARIN
RELATIVE(95% CI) ABSOLUTE
Mortality
1 Observational studies
No serious risk of bias
No serious inconsistency
No serious indirectness
No serious imprecision None 8/158
(5.1%)27/171 (15.8%)
RR 0.32 (0.15 to 0.68)
107 fewer per 1000 (from 51 fewer to 134 fewer)
OOLOW
CRITICAL
Deep venous trombosis (assessed with: DVT were diagnosed soley by clinical examination and confi rmed with duplex ultrasound)
1 Observational studies
No serious risk of bias
No serious inconsistency
No serious indirectness
No serious imprecision None 1/158
(0.63%)2/171 (1.2%)
RR 0.54 (0.04 to 5.91)
5 fewer per 1000 (from 11 fewer to 57 more)
OOLOW
CRITICAL
Pulmonary embolus (assessed with: A 128 slice helical CT pulmonary angiogram was used to confi rm PE in patients when clinically indicated)
1 Observational studies
No serious risk of bias
No serious inconsistency
No serious indirectness
No seriousimprecision None 0/158
(0%)7/171 (4.1%)
RR 0.07 (0 to 1.25)
38 fewer per 1000 (from 41 fewer to 10 more)
OOLOW
CRITICAL

Foundation for Medical and Technical Research and Education in Em
ergencies and Disasters
176 Question 9Date: 2013-09-30Question: Should Intracranial pressure monitoring vs no intracranial pressure monitoring be used for adults with severe trauma brain injury?Settings: Intensive careBibliography: 1. Sha i S, Diaz-Arrastia R, Madden C, Gentilello L. Intracranial pressure monitoring in brain-injured patients is associated with worsening of survival. J Trauma. 2008;64(2):335-40. 2. Alali AS, Fowler RA, Mainprize TG, Scales DC, Kiss A, de Mestral C et al. Intracranial Pressure Monitoring in Severe Traumatic Brain Injury: Re-sultsfrom the American College of Surgeons Trauma Quality ImprovementProgram. J Neurotrauma. 2013 Jul 11.
QUALITY ASSESSMENT NO OF PATIENTS EFFECT
QUALITY IMPORTANCENO OF STUDIES DESIGN RISK OF
BIAS INCONSISTENCY INDIRECTNESS IMPRECISION OTHER CONSI-DERATIONS
INTRACRANIAL PRESSURE
MONITORING
NO INTRACRANIAL PRESSURE
MONITORINGRELATIVE(95% CI) ABSOLUTE
2. Hospital Mortality (Shafi 2008) (follow-up to discharge)
1 Observational studies Serious1 No serious
inconsistencyNo serious indirectness
No serious imprecision None 196/708
(27.7%)112/938 (11.9%)
RR 2.31 (1.87 to 2.86)
156 more per 1000 (from 104 more to 222 more)
OOOVERY LOW
CRITICAL
3. Mortality (Alali 2007) (follow-up to discharge)
1 Observational studies Serious1 No serious
inconsistencyNo serious indirectness
No serious imprecision None 599/1874
(32%)3170/8754 (36.2%)
RR 0.88 (0.82 to 0.94)
43 fewer per 1000 (from 22 fewer to 65 fewer)
OOOVERY LOW
CRITICAL
1 Selection bias, for blindness and execution.

Clinical Practice Guideline for the diagnosis and treatm
ent of adult patients with severe Traum
atic Brain Injury G
uide for Health Professionals 2014 - G
uid
e N
o. G
PC
-20
14
-30
Ministry of H
ealth and Social Protection - Colciencias 177
Question 10Date: 2013-12-04Question: Should selective brain cooling vs normothermia be used for severe TBI?Settings: ICUBibliography: Harris 2009; Qiu 2006; Liu 2006
QUALITY ASSESSMENT NO OF PATIENTS EFFECT
QUALITY IMPORTANCENO OF STUDIES DESIGN RISK OF
BIAS INCONSISTENCY INDIRECTNESS IMPRECISIONOTHER
CONSIDERA-TIONS
SELECTIVE BRAIN COOLING
NORMOTHER-MIA
RELATIVE(95% CI) ABSOLUTE
Mortality (assessed with: hospital mortality)
1 Randomised trials
No serious risk of bias
No serious inconsistency
No serious indirectness Serious1 None 6/12
(50%)4/13 (30.8%)
RR 1.62 (0.60 to 4.38)
191 more per 1000 (from 123 fewer to 1000 more)
OMODERATE
CRITICAL
Good neurological outcome (follow-up 6 months; assessed with: GOS score of 4 to 5)
1 Randomised trials
No serious risk of bias
No serious inconsistency
No serious indirectness Serious2 None 33/45
(73.3%)23/45 (51.1%)
RR 1.43 (1.02 to 2.00)
220 more per 1000 (from 10 more to 511 more)
OMODERATE
CRITICAL
Good neurological outcome (follow-up 2 years; assessed with: GOS score of 4 to 5)
1 Randomised trials
No serious risk of bias
No serious inconsistency
No serious indirectness
No serious imprecision2 None 16/22
(72.7%)8/23 (34.8%)
RR 2.09 (1.13 to 3.86)
379 more per 1000 (from 45 more to 995 more)
HIGH
CRITICAL
1 The 95% con idence interval included no bene it or appreciable bene it, this study was to small to be powered to detect a difference in mortality2 The 95% con idence interval included no bene it or appreciable bene it.

Foundation for Medical and Technical Research and Education in Emergencies and Disasters178
Annex 4
Richmond agitation/sedation scale (RASS)
POINTS CATEGORIES DESCRIPTION
+4 Combative Violent or combative, a risk for staff
+3 Very agitated Tries to remove tubes or catheters or is aggresive with staff
+2 Agitated Uncoordinated movements or fi ghts the respirator
+1 Restless Anxious but without aggressive or vigorous movements
0 Alert and calmTends to be asleep, but is able to be awake for more than 10 seconds (opens eyes to voice)
-1 Drowsy Awake (opens eyes) for less than 10 seconds in response to voice
-2 Light sedation Movements without opening eyes in response to voice
-3 Moderate sedation No response to voice, but moves or opens eyes to physical stimulation
-4 Deep sedation No response to voice or physical stimulation
-5 Unarousable Sin respuesta a la voz o estimulo físico
Procedure1. Observe the patient. Is (s)he alert and calm? (Score 0). Is (s)he
restless or agitated (score +1 to +4)?2. If the patient is not alert, call him/her by his/her name and see
if (s)he opens his/her eyes and makes eye contact.3. Repeat if necessary.4. The patient wakes up and opens eyes, maintaining visual con-
tact for more than 10 seconds: score -1.5. The patient wakes up and opens eyes, maintaining visual con-
tact for less than 10 seconds: score -2.6. The patient moves in response to voice but does not open eyes:
score -3.

Clinical Practice Guideline for the diagnosis and treatment of adult patients with severe Traumatic Brain Injury Guide for Health Professionals 2014 - Guide No. GPC-2014-30
Ministry of Health and Social Protection - Colciencias 179
7. If the patient doesn’t respond to voice, physically stimulate him/her by moving the shoulder or pressing the sternum.
8. If the patient moves after physical stimulation: score -4.9. If the patient doesn’t move after any physical stimulation:
score -5.
Reference: Sessler CN. Grap MJ, Brophy GM. Multidisciplinary management of seda-tion and analgesia in critical care. Semin Respir Crit Care Med. 2001; 22: 211-225.
Foundation for Medical and Technical Research and Education in Emergencies and Disasters180
Clinical Practice GuidelineDiagnosis and treatment of adult patients with severe Traumatic Brain InjuryGuide for Health Professionals
2014-Guide No. GPC-2014-30
gpc.minsalud.gov.co