clinical policy title: corneal transplants (keratoplasty) · as medical advice or to direct...
TRANSCRIPT
Clinical Policy Title: Corneal transplants (keratoplasty) Clinical Policy Number: 10.03.04 Effective Date: April 1, 2015 Initial Review Date: November 19, 2014 Most Recent Review Date: November 16, 2016 Next Review Date: November 2017 Related policies: CP# 10.03.06 Corneal implants ABOUT THIS POLICY: AmeriHealth Caritas Pennsylvania has developed clinical policies to assist with making coverage determinations.
AmeriHealth Caritas Pennsylvania’s clinical policies are based on guidelines from established industry sources, such as the Centers for Medicare & Medicaid Services (CMS), state regulatory agencies, the American Medical Association (AMA), medical specialty professional societies, and peer-reviewed professional literature. These clinical policies along with other sources, such as plan benefits and state and federal laws and regulatory requirements, including any state- or plan-specific definition of “medically necessary,” and the specific facts of the particular situation are considered by AmeriHealth Caritas Pennsylvania when making coverage determinations. In the event of conflict between this clinical policy and plan benefits and/or state or federal laws and/or regulatory requirements, the plan benefits and/or state and federal laws and/or regulatory requirements shall control. AmeriHealth Caritas Pennsylvania’s clinical policies are for informational purposes only and not intended as medical advice or to direct treatment. Physicians and other health care providers are solely responsible for the treatment decisions for their patients. AmeriHealth Caritas Pennsylvania’s clinical policies are reflective of evidence-based medicine at the time of review. As medical science evolves, AmeriHealth Caritas Pennsylvania will update its clinical policies as necessary. AmeriHealth Caritas Pennsylvania’s clinical policies are not guarantees of payment.
Coverage policy AmeriHealth Caritas Pennsylvania considers corneal transplants (keratoplasty) to be clinically proven
and, therefore, medically necessary when the following criteria are met:
Vision cannot be corrected by eyeglasses, therapeutic contact lenses, or medical therapies.
There is documentation of corneal diseases that cause functional impediment of job
performance or ability to carry out activities of daily living, such as:
Scarring from infections (e.g., eye herpes or fungal keratitis).
Hereditary conditions (e.g., Fuchs’ endothelial corneal dystrophy [FECD]).
Eye diseases (e.g., advanced keratoconus, which is a common corneal disorder
where the central or paracentral cornea undergoes progressive thinning and
steepening, causing irregular astigmatism).
Thinning of the cornea and irregular corneal shape (e.g., with keratoconus).
Chemical burns of the cornea or damage from an eye injury.
Excessive edema (swelling) of the cornea.
Graft rejection following a previous corneal transplant.
Corneal failure due to cataract surgery complications.
Policy contains:
Corneal transplant.
Penetrating keratoplasty (PK).
Lamellar (partial thickness) keratoplasty (LK).
Endothelial keratoplasty (EK).

2
The following procedures are medically necessary for the following indications (including
but not limited to):
Procedures Indications and treatment of corneal diseases that obstruct
visual acuity, such as:
Penetrating (full thickness) keratoplasty (PK): removal and replacement of the entire thickness of the cornea with full thickness donor corneal tissue (corneal transplant).
Opaque cornea.
Persistent severe bacterial, fungal, or amebic inflammation (keratitis) if failure of antibiotic therapy.
Failure or rejection of a previous corneal transplant.
Bullous keratopathy (BK), keratoconus.
Full-thickness (penetrating) corneal transplant in a phakic patient.
Aphakic patient (with no native lens).
Pseudophakic patient (with an artificial lens).
FECD.
Herpes simplex keratitis.
Lamellar (partial thickness) keratoplasty (LK): replacement of the outer two-thirds of the cornea with donor cornea (nonpenetrating keratoplasty).
Scarring.
Corneal edema.
Keratoconus.
Corneal dystrophies, degenerations.
Thinning, distortion.
*Endothelial keratoplasty (EK) using the following techniques:
Posterior lamellar keratoplasty (PLK)/deep lamellar endothelial keratoplasty (DLEK).
Descemet’s stripping endothelial keratoplasty (DSEK).
Descemet’s stripping (automated) endothelial keratoplasty (DSAEK).
Descemet‘s membrane (automated) endothelial keratoplasty (DMAEK).
Descemet’s membrane endothelial keratoplasty (DMEK).
BK.
Corneal edema.
Posterior corneal dystrophies.
Rupture in Descemet’s membrane.
Endothelial corneal dystrophy and other posterior corneal dystrophies.
Mechanical complications due to corneal graft or ocular lens prostheses.
Iridocorneal (ICE) syndrome.
*Note: EK should not be used in place of PK for conditions with concurrent endothelial disease and
anterior corneal dystrophies. These situations include anterior corneal scars from trauma or prior
infection, and ectasia after previous laser vision correction surgery (American Academy of
Ophthalmology [AAO] recommendation).
Limitations:
The following corneal transplant (keratoplasty) procedures are not medically necessary:
Collagen cross-linking, not approved by the U.S. Food and Drug Administration
(FDA).

3
The use of DMEK, DSEK, DSAEK, and DMAEK to treat disease or injury of the corneal
stroma (for example, keratoconus, corneal ulcers caused by infection and traumatic
corneal injuries).
PK when performed solely to correct astigmatism or other refractive errors.
Corneal transplants are considered outpatient procedures and do not require an
inpatient stay (InterQual Clinical Guidelines, 2014).
Note: Keratoplasty procedures primarily for refractive correction and radial keratotomy are not covered
by Medicare (CMS Manual System, Pub. 100-03, Medicare National Coverage Determinations Manual,
Section 80.7, Refractive Keratoplasty). The CPT manual (at 65710) gives an instruction to use other
codes for refractive keratoplasty, such as CPT codes 65760, 65765, and 65767.
Alternative covered services:
Conservative treatment designed to reduce the fluid accumulation in corneal degeneration, or
treatment ordered by the treating specialist for a specific disorder.
Background
The cornea forms the transparent anterior part of the eye. It protects the contents of the eye and serves
as the major refractive element in it. The principal layers of the cornea are the epithelium, Bowman
layer, stroma, Descemet’s membrane, and the endothelium.
Corneal eye disease is the fourth most common cause of blindness (after cataracts, glaucoma, and age-
related macular degeneration) and affects more than 10 million people worldwide (Wachler, 2015).
Corneal transplantation removes the scarred, damaged, or diseased cornea and replaces it with a
human donor cornea. Corneal transplant surgery is also called PK, or corneal grafting.
An eye bank provides the donor tissue for corneal transplant surgery. In 2015, 79,304 corneas were
available for transplantation in the U.S (Eye Bank Association of America [EBAA], 2016). Since 1961,
more than 1.5 million people have had restored vision through corneal transplants. The success of
corneal transplantation may be attributed in part to the normal cornea lacking blood vessels, which may
prevent the body from recognizing the “foreign” donor cornea (EBAA, 2016).
Efforts are aimed at maintaining the current eye bank system and enhancing its effectiveness, while
simultaneously supporting the efforts to improve vital organ procurement and transplantation (AAO,
1996). Recent advances in techniques for storing donor corneas in fluid for several days have improved
the chances of successful surgery. This also allows for better planning and timing of surgery.
Corneal transplant procedures:

4
Corneal transplants are performed on an outpatient basis under local anesthesia. The surgeon performs
the surgery while looking at the eye through a microscope. A cookie-cutter-like knife called a trephine is
used to cut and remove a circular piece from the recipient’s scarred cornea. A similar knife is used to cut
and remove a piece from the donor cornea, which is sewn into place with very fine sutures that are
smaller in diameter than a human hair.
PK is the standard procedure for treating cornea disease. Most PKs are performed to improve poor
visual acuity caused by an opaque cornea. PK is used to remove active corneal disease, such as
persistent severe bacterial, fungal, or amebic inflammation of the cornea (keratitis), after appropriate
antibiotic therapy. The most common indications for PK are: BK, keratoconus, corneal scar with opacity,
keratitis, corneal transplant rejection, FECD, corneal degeneration, other corneal dystrophies, corneal
edema, and herpes simplex keratitis. PK is not used solely to correct astigmatism or other refractive
errors. Surgically-induced astigmatism is a potential complication of PK that may require refractive
surgery.
Recent advances in corneal surgery have enabled component surgery of the cornea to be performed,
replacing only the necessary tissue instead of the entire cornea. Modifications in surgical technique and
instrumentation also contributed to improved visual quality with LK surgery, making the procedures
more accessible and easier to perform, particularly posterior lamellar graft for endothelial dysfunction
— EK. These procedures include (Azur, 2001; Culbertson, 2003; Ehlers, 2000;Fernandez, 2010; Gorovoy,
2006; Ko, 1993; Sandup, 2001; Tappin, 2007):
Deep anterior lamellar keratoplasty (DALK).
DLEK.
Deep lamellar keratoplasty (DLKP).
DMAEK.
DMEK.
DSAEK.
Descemet's stripping automated keratoplasty (DSAK).
Ongoing research in compatibility testing between donor and recipient may lead to ways of increasing
the chance of a successful outcome in high-risk patients. Race, sex, blood type, eye color, and near- and
farsightedness are not considered in selecting the donor, because they do not affect the outcome of the
corneal transplant surgery.
Regulation:
Surgical procedures are not subject to FDA regulation, but the FDA Center for Devices and Radiological
Health (CDRH) does regulate instruments used during ophthalmic surgeries, including corneoscleral
punches, trephines, forceps, hooks, retrobulbar needles, and others (CDRH, 2016). There is a large
number of FDA-approved microkeratomes primarily for corneal dissection during (laser assisted in situ
keratomileusis (LASIK) eye surgery, but the EK procedures are not specifically referenced in the approval

5
documents. The FDA classifies these devices with the Product Code HNO. The FDA Center for Biologics
Evaluation and Research (CBER) regulates human cells or tissue intended for implantation,
transplantation, infusion, or transfer into a human recipient including cells or tissue from the cornea
(CBER, 2016).
Searches
AmeriHealth Caritas Pennsylvania searched PubMed and the databases of:
UK National Health Services Centre for Reviews and Dissemination.
Agency for Healthcare Research and Quality’s National Guideline Clearinghouse and other
evidence-based practice centers.
The Centers for Medicare & Medicaid Services (CMS).
We conducted searches on November 9, 2016. Search terms were: “corneal transplants,” “descemet
stripping,” “endothelial keratoplasty,” and “endothelial dysfunctions.”
We included:
Systematic reviews, which pool results from multiple studies to achieve larger sample sizes
and greater precision of effect estimation than in smaller primary studies. Systematic
reviews use predetermined transparent methods to minimize bias, effectively treating the
review as a scientific endeavor, and are thus rated highest in evidence-grading hierarchies.
Guidelines based on systematic reviews.
Economic analyses, such as cost-effectiveness, and benefit or utility studies (but not simple
cost studies), reporting both costs and outcomes — sometimes referred to as efficiency
studies — which also rank near the top of evidence hierarchies.
Findings
FECD and keratoconus are the primary indications for corneal transplantation among the elderly and
adolescents, respectively (Duman, 2013; Lowe, 2011). Keratoplasty for FECD is typically reserved until a
patient experienced a significant, persistent decrease in vision throughout the day, not simply in the
morning, when the cornea is most swollen. Keratoplasty for keratoconus in adolescents show excellent
survival (Lowe, 2011). Seventy-five percent of patients achieved 20/40 vision or better (some needed
eyeglasses, contact lenses, or vision-correcting surgery) and 90 percent still had viable corneas at their
10-year follow-up. However, less than 40 percent of infants (< age 5 years) had functional corneas at 16
years post-surgery, compared with 70 percent in the 5–12 year age group, at 22 years post-surgery.
Corneal graft survival and visual outcomes varied more by indication for graft than recipient age, but
presence of serious developmental disorders may have affected results.
The most suitable surgical candidates for EK would be patients with FECD or pseudophakic bullous
keratopathy (PBK). EK may also be valuable for some patients with a failed PK, particularly those without

6
significant stromal scarring, opacification, or vascularization of the anterior layers. Pseudophakic
patients with deep anterior chambers and posterior chamber intraocular lenses are the best candidates
for the novice surgeon, as there is adequate space to unfold the donor button without risk of trauma to
the lens. Similarly, for patients requiring both corneal transplantation and cataract removal, it is
advantageous to perform a triple procedure with removal of the cataract just before the EK portion of
the surgery. This allows the creation of a deeper anterior chamber and avoids the risk of damaging the
donor graft.
No RCTs were found that directly compared DSEK or DSAEK with the reference standard of care, PK, or
with other EK techniques. Hayes (2011) reviewed seven studies, including three comparative trials that
evaluated the efficacy and safety of DSAEK and DSEK. DSAEK and DSEK improve visual acuity in the short
term with little effect on refractive astigmatism, although they are associated with mild hyperopic shifts.
Improvements in best-corrected visual acuity were achieved more quickly following DSAEK and DSEK
compared with PK, although the results of the two surgery types appear similar after one year.
Complication rates of dislocation following Descemet stripping procedures ranged from 2.6 percent to
23.0 percent, and graft failure rates ranged from 0 to 18 percent. Variation in surgical technique and
expertise complicated data interpretation. While promising, the long-term efficacy and safety of
Descemet stripping procedures compared with PK have not been established.
There is insufficient evidence to determine whether automating the procedure, using precut versus
fresh, surgeon-cut corneal grafts, or the presence of ECD of the donor cornea influences outcomes.
Variation in surgical technique and expertise between the studies further complicates data
interpretation. Definitive answers await the performance of RCTs with blinded assessment of health
outcomes (Hayes, 2011).
The main benefits of EK include a stronger wound (absence of a full thickness incision), more rapid
healing, and little or no change in refraction. Since the anterior layers remain undisturbed, there is no
need for the use of surface corneal sutures, as for traditional PK. The corneal curvature also remains
more stable over time and the large shifts in refraction that sometimes occur with corneal grafts do not
occur. Late suture-related complications, such as infection or vascularization, are prevented and the
absence of a full-thickness vertical interface in the cornea increases the safety of the procedure, both
during and after the operation.
The absence of penetrating corneal sutures and incisions results in reduced postoperative astigmatism,
normal corneal topography, faster wound healing, earlier visual rehabilitation, and a more stable globe.
In addition, rejection appears to be less frequent during the first two years after EK, and may be less
severe after EK than after PK.
Should rejection occur, aggressive treatment may be considered, as for conventional PK. The minimal
alteration in the contour of the cornea after surgery means that the predictability of intraocular lens
power calculations is enhanced. For DSEK, the entire recipient cornea is left intact; thus, subsequent
LASIK or other procedures may still be applied. In areas where donor grafts are scarce, the benefit of
multiple recipients for one donated eye is also important. The main disadvantages to EK include the
7
need for specific instrumentation, a steeper learning curve, and the need for excellent surgical
technique. EK requires a different skill set than that required for standard full thickness PK, so
experienced PK surgeons may initially find the EK maneuvers awkward and unfamiliar. It is strongly
recommended that EK should be extensively practiced in the laboratory before embarking on clinical
treatment of patients.
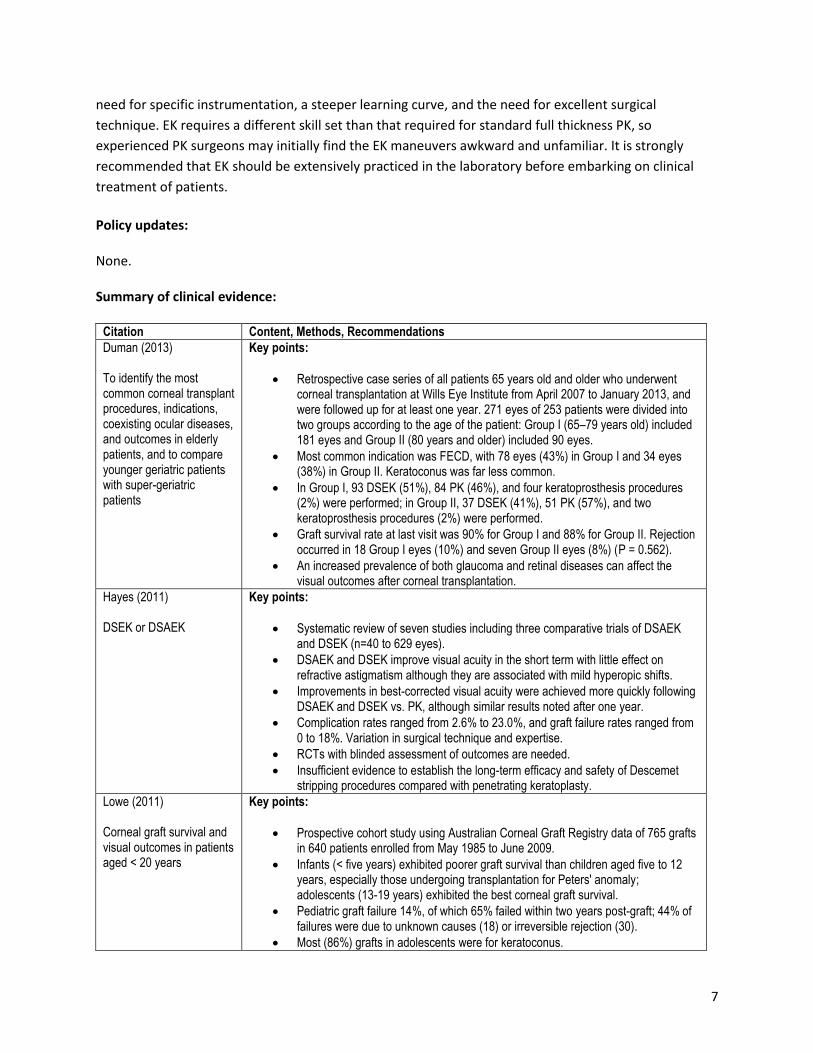
Policy updates: None. Summary of clinical evidence:
Citation Content, Methods, Recommendations
Duman (2013) To identify the most common corneal transplant procedures, indications, coexisting ocular diseases, and outcomes in elderly patients, and to compare younger geriatric patients with super-geriatric patients
Key points:
Retrospective case series of all patients 65 years old and older who underwent corneal transplantation at Wills Eye Institute from April 2007 to January 2013, and were followed up for at least one year. 271 eyes of 253 patients were divided into two groups according to the age of the patient: Group I (65–79 years old) included 181 eyes and Group II (80 years and older) included 90 eyes.
Most common indication was FECD, with 78 eyes (43%) in Group I and 34 eyes (38%) in Group II. Keratoconus was far less common.
In Group I, 93 DSEK (51%), 84 PK (46%), and four keratoprosthesis procedures (2%) were performed; in Group II, 37 DSEK (41%), 51 PK (57%), and two keratoprosthesis procedures (2%) were performed.
Graft survival rate at last visit was 90% for Group I and 88% for Group II. Rejection occurred in 18 Group I eyes (10%) and seven Group II eyes (8%) (P = 0.562).
An increased prevalence of both glaucoma and retinal diseases can affect the visual outcomes after corneal transplantation.
Hayes (2011) DSEK or DSAEK
Key points:
Systematic review of seven studies including three comparative trials of DSAEK and DSEK (n=40 to 629 eyes).
DSAEK and DSEK improve visual acuity in the short term with little effect on refractive astigmatism although they are associated with mild hyperopic shifts.
Improvements in best-corrected visual acuity were achieved more quickly following DSAEK and DSEK vs. PK, although similar results noted after one year.
Complication rates ranged from 2.6% to 23.0%, and graft failure rates ranged from 0 to 18%. Variation in surgical technique and expertise.
RCTs with blinded assessment of outcomes are needed.
Insufficient evidence to establish the long-term efficacy and safety of Descemet stripping procedures compared with penetrating keratoplasty.
Lowe (2011) Corneal graft survival and visual outcomes in patients aged < 20 years
Key points:
Prospective cohort study using Australian Corneal Graft Registry data of 765 grafts in 640 patients enrolled from May 1985 to June 2009.
Infants (< five years) exhibited poorer graft survival than children aged five to 12 years, especially those undergoing transplantation for Peters' anomaly; adolescents (13-19 years) exhibited the best corneal graft survival.
Pediatric graft failure 14%, of which 65% failed within two years post-graft; 44% of failures were due to unknown causes (18) or irreversible rejection (30).
Most (86%) grafts in adolescents were for keratoconus.

8
Factors significantly affecting corneal graft survival were indication for graft, graft inflammation, history of intraocular surgery, vascularization, rejection episodes, post-graft operative procedures, and refractive surgery.
Price (2010) The Cornea Donor Study: DSEK vs. PK
Key points:
Two surgeons performed DSEK on 173 patients at three-year follow up: clear grafts (64%) ; clear grafts on last examination but lost to follow up (25%); death (6.4%); graft failure (4%).
Cumulative probability of a DSEK graft survival at three years (94%): DSEK and PKP eyes with FECD (96%); DSEK eyes (86%); PKP eyes with other preoperative diagnoses (84%).
Immunological graft rejection: DSEK group (6.4%) vs. the PKP group (20%) at three years (P = 0.0005).
Median endothelial cell loss (ECL) at three years for DSEK vs. PKP groups (48% vs. 53%, respectively, P = 0.17): ECL with FECD < other preoperative diagnoses, but similar among DSEK and PKP eyes. Of note, more ECL with DSEK eyes than PKP eyes at one year, but less over the subsequent two years.
The two sites used different incision lengths: 3.2 mm and 5.0 mm. The significantly greater ECL observed in the 3.2-mm-incision eyes compared with the 5.0-mm-incision eyes at one year persisted at three years (60% vs. 33%, P = 0.0007). The 5.0-mm incision showed significantly less ECL in the DSEK eyes than in the PKP eyes at three years (33% vs. 53%, P = 0.0017). Compared with PK, DSAEK resulted in lower ECL with comparable cumulative graft survival rates for up to three years in patients with FECD and BK.
Basak (2008) Indications, operative problems, and postoperative complications of DSEK
Key points:
Prospective, nonrandomized, noncomparative, consecutive case series of 75 eyes of 75 patients with endothelial dysfunctions of different etiology, scheduled for DSEK. Healthy donor cornea with a cell count of > 2,000 cells/sq mm was considered. Best corrected visual acuity (BCVA), refractive and keratometric astigmatism, central corneal thickness (CCT), and ECD were analyzed for each patient after a minimum follow-up of three months.
Main indication was pseudophakic corneal edema and BK in 53 (70.7%) eyes. Seventeen (22.7%) cases had moderate to severe FECD with various grades of cataract, and DSEK was combined with manual small-incision cataract surgery (MSICS) with posterior chamber intraocular lens (PCIOL) in those cases.
After three months, best corrected visual acuity was 20/60 or better in 62 (82.7%) cases. Mean refractive and keratometric astigmatism were 1.10 ± 0.55 diopter cylinder (DCyl) and 1.24 ± 0.92 DCyl. The central corneal thickness and ECD were 670.8 ± 0.32 µm and 1485.6 ± 168.6/sq mm, respectively. The mean ECL after three months was 26.8 ± 4.24% (range: 13.3%–38.4%). Dislocation of donor lenticule occurred in six (8.0%) eyes. Graft failure occurred in one case.
DSAEK is a safe and effective procedure in patients with endothelial dysfunctions with encouraging surgical and visual outcomes. It can be safely combined with MSICS with PCIOL in patients with moderate to severe FECD with cataract.
References
Professional society guidelines/others:
American Academy of Ophthalmology. Automated lamellar keratoplasty. Ophthalmology. 1996; 103(5):
852 - 861.

9
American Academy of Ophthalmology. Corneal opacification. Preferred Practice Pattern No. 15. San
Francisco, CA: AAO; September 16, 1995. American Academy of Ophthalmology website.
http://www.aao.org/. Accessed November 22, 2016.
Center for Devices and Radiological Health (CDRH). 510k approvals. M3 microkeratome. K032836. June
18, 2004. FDA website. http://www.fda.gov/MedicalDevices/default.htm. Accessed November 22, 2016.
Center for Biologics Evaluation and Research. Tissues. Updated September 19, 2008. FDA website.
http://www.fda.gov/BiologicsBloodVaccines/TissueTissueProducts/default.htm . Assessed November
22, 2016.
InterQual Procedures Clinical Guidelines. 2014 McKesson Corporation.
National Institute for Health and Clinical Excellence (NICE). Corneal endothelial transplantation.
Interventional Procedures Consultation. London, UK: NICE; December 2008.
National Institute for Health and Clinical Excellence (NICE). Corneal implants for keratoconus.
Interventional Procedures Guidance 227. London, UK: NICE; July 2007.
National Keratoconus Foundation. National Eye Institute website. https://nei.nih.gov/content/national-
keratoconus-foundation. Accessed November 22, 2016.
Peer-reviewed references:
Allan BD, Terry MA, Price FW Jr, Price MO, Griffin NB, Claesson M. Corneal transplant rejection rate and
severity after endothelial keratoplasty. Cornea. 2007; 26: 1039 - 1042.
Azar DT, Jain S, Sambursky R, Strauss L. Microkeratome assisted posterior keratoplasty. J Cataract
Refract Surg. 2001; 27: 353 - 356.
Basak SK. Descemet stripping and endothelial keratoplasty in endothelial dysfunctions: Three-month
results in 75 eyes. Indian J Ophthalmol. 2008; 56(4): 291 - 296.
Culbertson WW. Endothelial replacement: flap approach. Ophthalmol Clin North Am. 2003; 16: 113 -
118.
Duman F , Kosker M, Suri K, et al. Indications and Outcomes of Corneal Transplantation in Geriatric
Patients. Am J Ophthal. 2013;156(3):600 - 607.
Ehlers N, Ehlers H, Hjortdal J, Moller-Pedersen T. Grafting of the posterior cornea: description of a new
technique with 12-month clinical results. Acta Ophthalmol Scand. 2000; 78: 543 - 546.
10
Fernandez M., Afshari N. Endothelial Keratoplasty: From DLEK to DMEK. Middle East Afir J Ophthalmol.
2010, 17(1): 5 - 8.
Gorovoy MS. Descemet-stripping automated endothelial keratoplasty. Cornea. 2006; 25: 886 - 889.
Hayes Inc. Hayes Medical Technology Report. Descemet stripping with Manual or Automated Endothelial
Keratoplasty for Corneal Endothelial Degeneration. Hayes, Inc.; Lansdale, Pa. March 2011.
Kaufman HE, Barron, BA, McDonald, MB, eds. The Cornea, 2d ed. 1996. External Disease and Cornea,
Section 8. Basic and Clinical Science Course, AAO, 2006.
Ko W, Freuh B, Shield C, Costello M, Feldman S. Experimental posterior lamellar transplantation at the
rabbit cornea (abstract). Invest Ophthalmol Vis Sci. 1993; 34: 1102.
Kunimoto DY, Kanitkar KD, Makar M, eds. The Wills Eye Manual, 4th ed. Lippincott, 2004.
Lowe MT, Keane MC, Coster DJ, Williams KA. The outcome of corneal transplantation in infants,
children, and adolescents. Ophthalmology. 2011 Mar; 118(3): 492 - 497.
Price FW Jr, Price MO. Descemet’s stripping with endothelial keratoplasty in 200 eyes. J Cataract Refract
Surg. 2006; 32: 411 - 418.
Price FW, Price MO. Descemet’s stripping with endothelialkeratoplsty in 50 eyes: a refractive neutral
corneal transplant. J Refract Surg. 2005; 21: 339 - 345.
Price MO, Price FW Jr, Kruse FE, Bachmann BO, Tourtas T. Randomized comparison of topical
prednisolone acetate 1% versus fluorometholone 0.1% in the first year after descemet membrane
endothelial keratoplasty. Cornea. 2014; 33(8): 880 - 886.
Sandeep J, Azar DT. New lamellar keratoplasty techniques: posterior keratoplasty and deep lamellar
keratoplasty. Curr Opin Ophthalmol. 2001; 12: 262 - 268.
Tappin M. A method for true endothelial cell (Tencell) transplantation using a custom-made cannula for
the treatment of endothelial cell failure. Eye. 2007; 21: 775 - 779.
Terry MA, Ousley PJ. Deep lamellar endothelial keratoplasty (DLEK): early complications and their
management. Cornea. 2006; 25: 37 - 43.
Trousdale ER, Hodge DO, Baratz KH, et al. Vision-related quality of life before and after keratoplasty for
Fuchs’ endothelial dystrophy. Ophthalmology. 2014; 121(11): 2147 - 2152.

11
Vajpayee RB, Sharma N, Jhanji V, et al. One donor cornea for 3 recipients: a new concept for corneal
transplantation surgery. Arch Ophthalmol. 2007; 125: 552 - 554.
Wachler BB. Cornea Transplants: What to Expect. Allaboutvision.com website.
http://www.allaboutvision.com/conditions/cornea-transplant.htm. Accessed November 22, 2016.
Young AL, Rao SK, Cheng LL, Lam, PTH. Endothelial keratoplasty, HK. J Ophthalmol. 2013; 12(1): 25 - 32.
CMS National Coverage Determinations (NCDs):
NCD for Refractive KERATOPLASTY (80.7). Effective date of this version: May 1, 1997. CMS website.
https://www.cms.gov/medicare-coverage-database/details/ncd-
details.aspx?NCDId=72&ncdver=1&SearchType=Advanced&CoverageSelection=Both&NCSelection=NCA
%7cCAL%7cNCD%7cMEDCAC%7cTA%7cMCD&ArticleType=SAD%7cEd&PolicyType=Both&s=All&KeyWor
d=keratoplasty&KeyWordLookUp=Doc&KeyWordSearchType=Exact&kq=true&bc=IAAAACAAAAAAAA%3
d%3d&. Accessed December 20, 2016.
Local Coverage Determinations (LCDs):
No LCDs identified at the writing of this policy.
Commonly submitted codes
Below are the most commonly submitted codes for the service(s)/item(s) subject to this policy. This is
not an exhaustive list of codes. Providers are expected to consult the appropriate coding manuals and
bill accordingly.
CPT Code Description Comments
65710 Keratoplasty (corneal transplant); anterior lamellar
65730 Keratoplasty (corneal transplant); penetrating except in aphakia or pseudophakia)
65750 Keratoplasty (corneal transplant); penetrating (in aphakia)
65755 Keratoplasty (corneal transplant); penetrating (in pseudophakia)
65756 Keratoplasty (corneal transplant); endothelial
ICD-10 Code Description Comments
E50.6 Vitamin A deficiency with xerophthalmic scars of cornea
H17.89 Other corneal scars and opacities
H17.9 Unspecified corneal scar and opacity
H18.001 Unspecified corneal deposit, right eye
H18.002 Unspecified corneal deposit, left eye
H18.003 Unspecified corneal deposit, bilateral
H18.009 Unspecified corneal deposit, unspecified eye
12
H18.009 Unspecified corneal deposit, unspecified eye
H18.20 Unspecified corneal edema
H18.20 Unspecified corneal edema
H18.221 Idiopathic corneal edema, right eye
H18.221 Idiopathic corneal edema, right eye
H18.222 Idiopathic corneal edema, left eye
H18.223 Idiopathic corneal edema, bilateral
H18.229 Idiopathic corneal edema, unspecified eye
H18.231 Secondary corneal edema, right eye
H18.232 Secondary corneal edema, left eye
H18.233 Secondary corneal edema, bilateral
H18.239 Secondary corneal edema, unspecified eye
H18.50 Unspecified hereditary corneal dystrophies
H18.51 Endothelial corneal dystrophy
H18.52 Epithelial (juvenile) corneal dystrophy
H18.53 Granular corneal dystrophy
H18.54 Lattice corneal dystrophy
H18.55 Macular corneal dystrophy
H18.59 Other hereditary corneal dystrophies
H18.601 Keratoconus, unspecified, right eye
H18.602 Keratoconus, unspecified, left eye
H18.603 Keratoconus, unspecified, bilateral
H18.609 Keratoconus, unspecified, unspecified eye
H18.621 Keratoconus, unstable, right eye
H18.622 Keratoconus, unstable, left eye
H18.623 Keratoconus, unstable, bilateral
H18.629 Keratoconus, unstable, unspecified eye
H18.811 Anesthesia and hypoesthesia of cornea, right eye
H18.812 Anesthesia and hypoesthesia of cornea, left eye
H18.813 Anesthesia and hypoesthesia of cornea, bilateral
H18.819 Anesthesia and hypoesthesia of cornea, unspecified eye
L76.81 Other intraoperative complications of skin and subcutaneous tissue
L76.82 Other postprocedural complications of skin and subcutaneous tissue
T26.11XA Burn of cornea and conjunctival sac, right eye, initial encounter
T26.12XA Burn of cornea and conjunctival sac, left eye, initial encounter
T26.60XA Corrosion of cornea and conjunctival sac, unspecified eye, initial encounter
T26.61XA Corrosion of cornea and conjunctival sac, right eye, initial encounter
T26.62XA Corrosion of cornea and conjunctival sac, left eye, initial encounter
T85.318A Breakdown (mechanical) of other ocular prosthetic devices, implants and grafts, initial encounter
T85.328A Displacement of other ocular prosthetic devices, implants and grafts, initial encounter
T85.398A Other mechanical complication of other ocular prosthetic devices, implants and grafts, initial encounter
T86.840 Corneal transplant rejection
T86.841 Corneal transplant failure