clinical podiatry and pharmacy - in1touchmpha.in1touch.org/uploaded/38/web/clinical podiatry and...
TRANSCRIPT
Clinical Podiatry and Pharmacy
Conflicts of Interest
• None to disclose.
Objectives
• To understand basic pathophysiology foot.
• 5 most common foot pathologies that present to pharmacists.
• To recognize and recommend products to:
a) Men & Women
b) Children
c) Pregnant women
• Myths about podiatric treatment.
• The role of podiatry and POM’s in Manitoba.
Acknowledge
• Kim McIntosh, Assistant Registrar to MPhA.
• Advit Shah, B.Sc. Pharmacy
Dr. Amar M. Gupta, Podiatrist
• Graduated from University of Winnipeg ’96 – BSc. Biology
• Graduated from University of Brighton, UK ‘2000 – B.Sc. (Hons) Podiatric Medicine.
• Currently attending University of Glasgow, UK. 2010- PgCert. Theory Podiatric Surgery M.Sc. Theory Podiatric Surgery.
Positions Held:
• College of Podiatrists of Manitoba (COPOM)- treasurer (3 terms).
• Canadian Podiatric Medical Association (CPMA)
• Task force for Surgical regulations committee (SRC)
Research Interest within surgery
• To evaluate accuracy of percutaneous release of the deep transverse metatarsal ligament (DTML) from the web space for Morton’s neuroma using fresh cadavers under diagnostic ultrasound.
Foot & Ankle Clinic, 1365 Grant Ave.
• www.winnipegfootclinic.com
• Interest in MSK problems, DxUS, surgery.
Phillips, I. Foot Injury. [online image] Available from: www.cartoonstock.com/cartoonview.asp?start=&search=main&catref=wstn27&MA_Artist=&MA_Category=&ANDkeyword=Podiatry. [Accessed on April 26 2012].
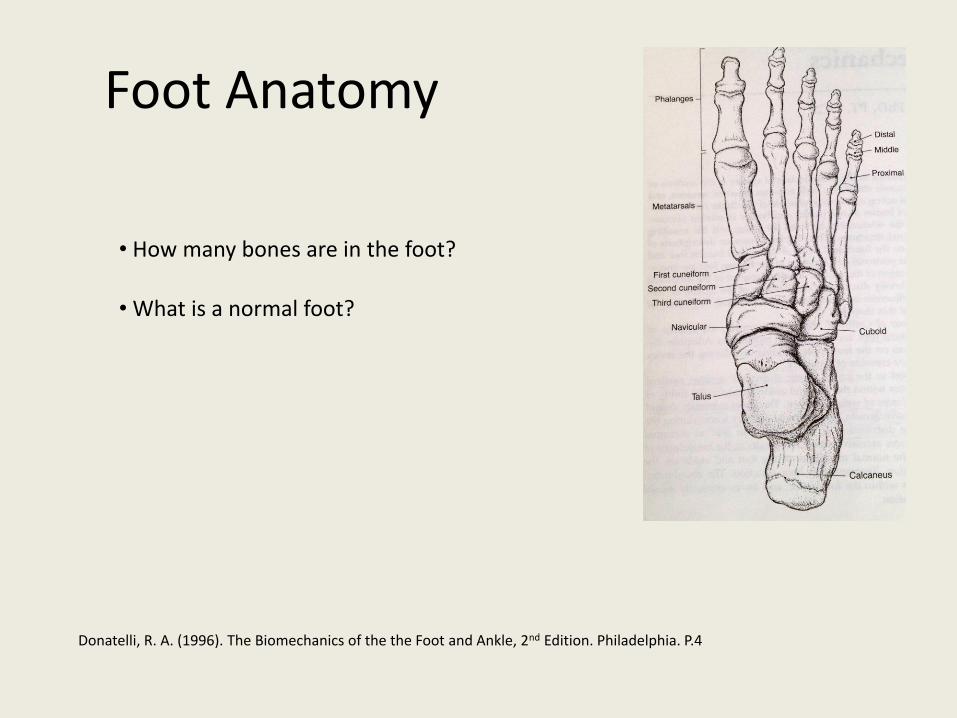
Foot Anatomy
Donatelli, R. A. (1996). The Biomechanics of the the Foot and Ankle, 2nd Edition. Philadelphia. P.4
• How many bones are in the foot?
• What is a normal foot?
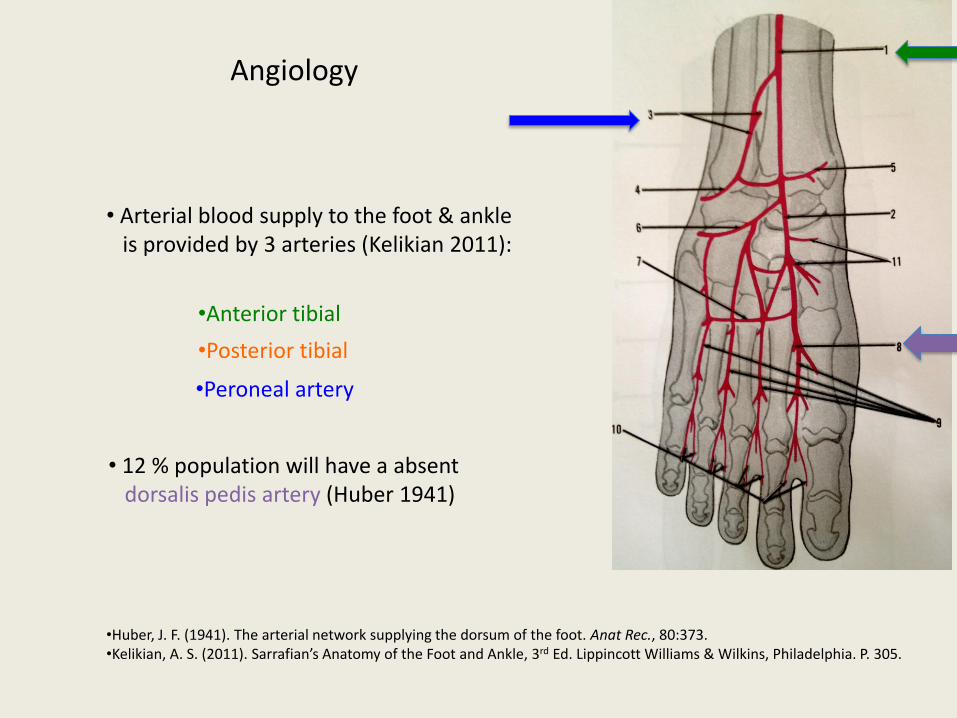
Angiology
• Arterial blood supply to the foot & ankle is provided by 3 arteries (Kelikian 2011):
•Anterior tibial
• 12 % population will have a absent dorsalis pedis artery (Huber 1941)
•Huber, J. F. (1941). The arterial network supplying the dorsum of the foot. Anat Rec., 80:373. •Kelikian, A. S. (2011). Sarrafian’s Anatomy of the Foot and Ankle, 3rd Ed. Lippincott Williams & Wilkins, Philadelphia. P. 305.
•Posterior tibial
•Peroneal artery
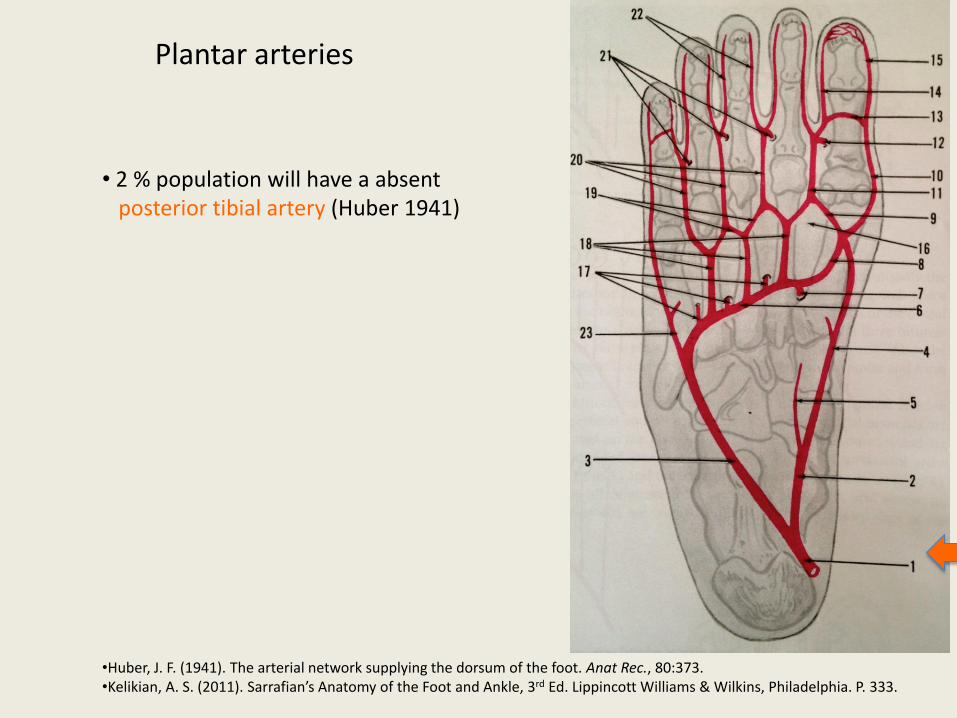
Plantar arteries
• 2 % population will have a absent posterior tibial artery (Huber 1941)
•Huber, J. F. (1941). The arterial network supplying the dorsum of the foot. Anat Rec., 80:373. •Kelikian, A. S. (2011). Sarrafian’s Anatomy of the Foot and Ankle, 3rd Ed. Lippincott Williams & Wilkins, Philadelphia. P. 333.
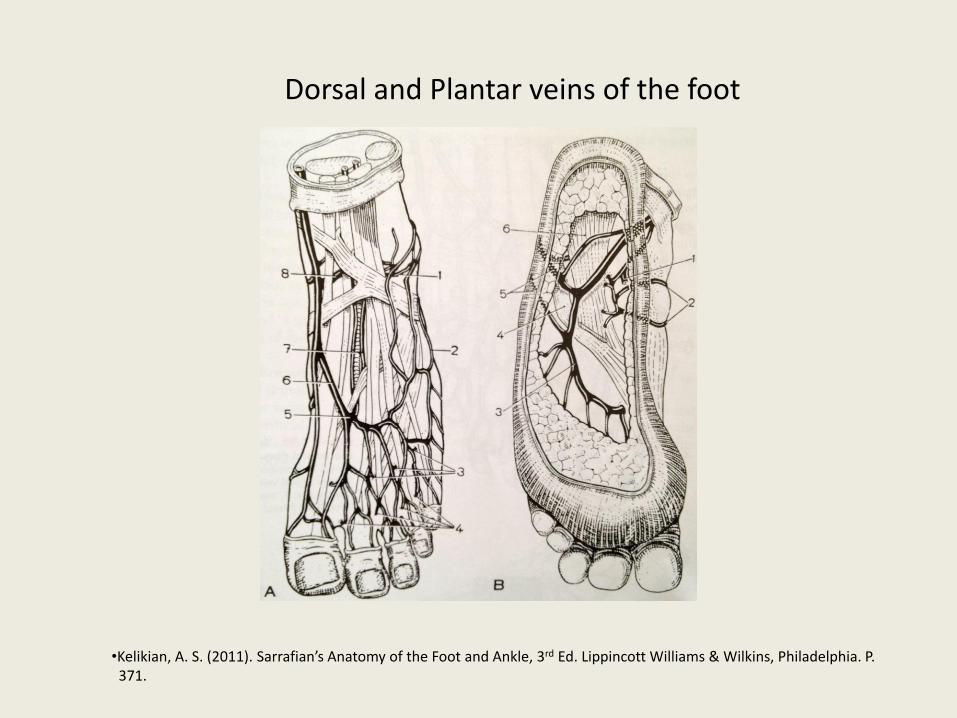
Dorsal and Plantar veins of the foot
•Kelikian, A. S. (2011). Sarrafian’s Anatomy of the Foot and Ankle, 3rd Ed. Lippincott Williams & Wilkins, Philadelphia. P. 371.
Nerves
• The nerve supply to the foot & ankle is provided by the branches of the sciatic n.
• The branches are: Sural n., Superficial peroneal n., Accessory deep peroneal n., Deep peroneal n., posterior tibal n. (MPN & LPN).
• The Saphenous n., a branch of the femoral n., gives limited contribution.
pathophysiology
• Most difficult management scenario for pharmacists and health care professionals is Diabetes and foot problems.
• Diabetes world wide will increase 366 million by 2030 (Wild et al. 2004).
• Diabetic patient has 25 % risk of developing foot ulcer in their lifetime (Singh et al. 2005).
• Annual incidence of diabetic foot ulcer 3%-10% (Reiber et al. 1999).
• Diabetic ulceration has shown to proceed amputation in up to 85% of cases (Reiber et al. 1999).
• Wild S, Roglic G, Green A, Sicree R,King H (2004) Global prevalence of diabetes: estimates for the year 2000 and projections for 2030. Diabetes Care 27:1047–1053. • Singh N, Armstrong DG, Lipsky BA (2005). Preventing foot ulcers in patients with diabetes. JAMA 293:217–228. • Reiber GE, Vileikyte L, Boyko EJ, del Aguila M, Smith DG, Lavery LA, Boulton AJ (1999). Causal pathways for incident lower extremity ulcers in patients with diabetes from two settings. Diabetes Care 22:157–162
4 Principal pathophysiologic factors responsible for foot ulcers:
• Neuropathy
• Ischemia
• Peripheral vascular disease
• Infection (Clayton & Elasy 2009).
• Clayton W. & Elasy, T. A. (2009). A Review of the Pathophysiology, Classification, and Treatment of Foot Ulcers in Diabetic Patient. Clinical Diabetes (27)2:52-58.
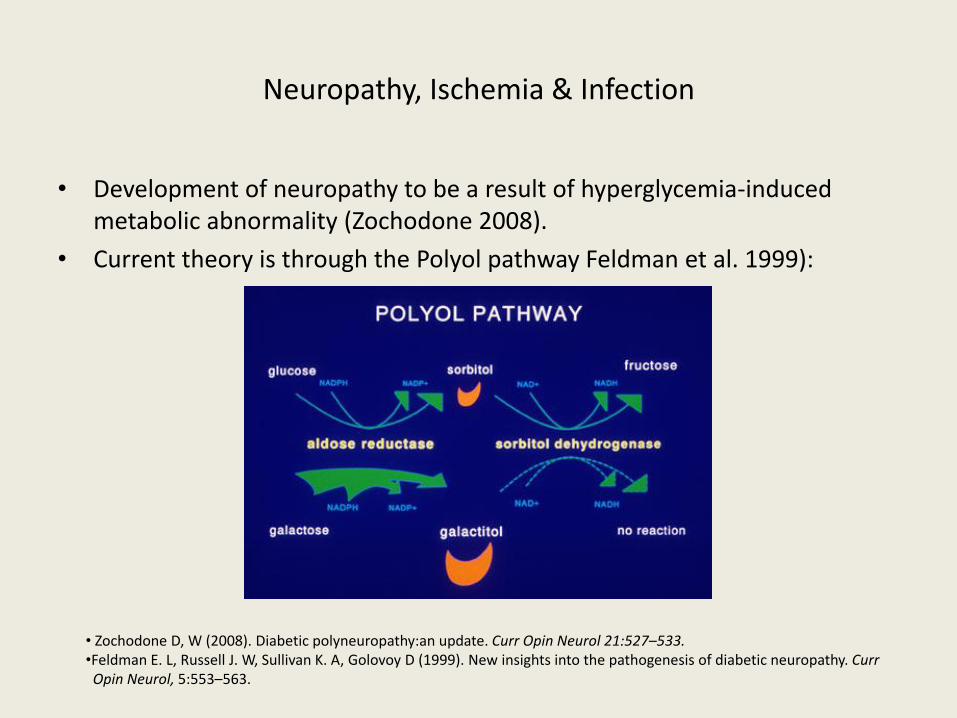
Neuropathy, Ischemia & Infection
• Development of neuropathy to be a result of hyperglycemia-induced metabolic abnormality (Zochodone 2008).
• Current theory is through the Polyol pathway Feldman et al. 1999):
• Zochodone D, W (2008). Diabetic polyneuropathy:an update. Curr Opin Neurol 21:527–533. •Feldman E. L, Russell J. W, Sullivan K. A, Golovoy D (1999). New insights into the pathogenesis of diabetic neuropathy. Curr Opin Neurol, 5:553–563.
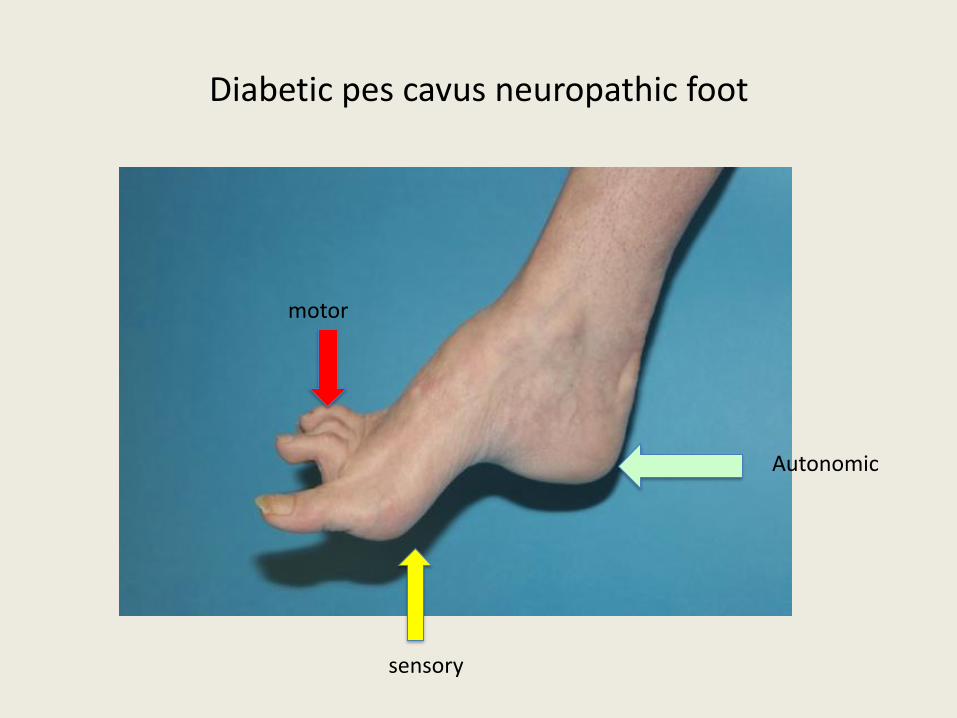
Diabetic pes cavus neuropathic foot
motor
sensory
Autonomic
Peripheral Arterial Disease (PAD)
• PAD is a contributing factor to ulcers in 50% of cases (Boulton et al. 2008).
• Generally affects tibial and peroneal arteries of the gastrocnemius.
• Endothelial cell dysfunction and smooth cell abnormalities develop in peripheral arteries as a consequence of the persistent hyperglycemic state (Zochodone 2008).
• There is a resultant decrease in endothelium-derived vasodilators.
• Boulton A. J, Armstrong D. G, Albert S. F, Frykberg R. G, Hellman R, Kirkman M. S, Lavery L. A, LeMaster J. W, Mills J. L Sr, Mueller M. J, Sheehan P, Wukich D. K (2008). Comprehensive foot examination and risk assessment. Diabetes Care 31:1679– 1685. • Zochodone D, W (2008). Diabetic polyneuropathy:an update. Curr Opin Neurol 21:527–533.
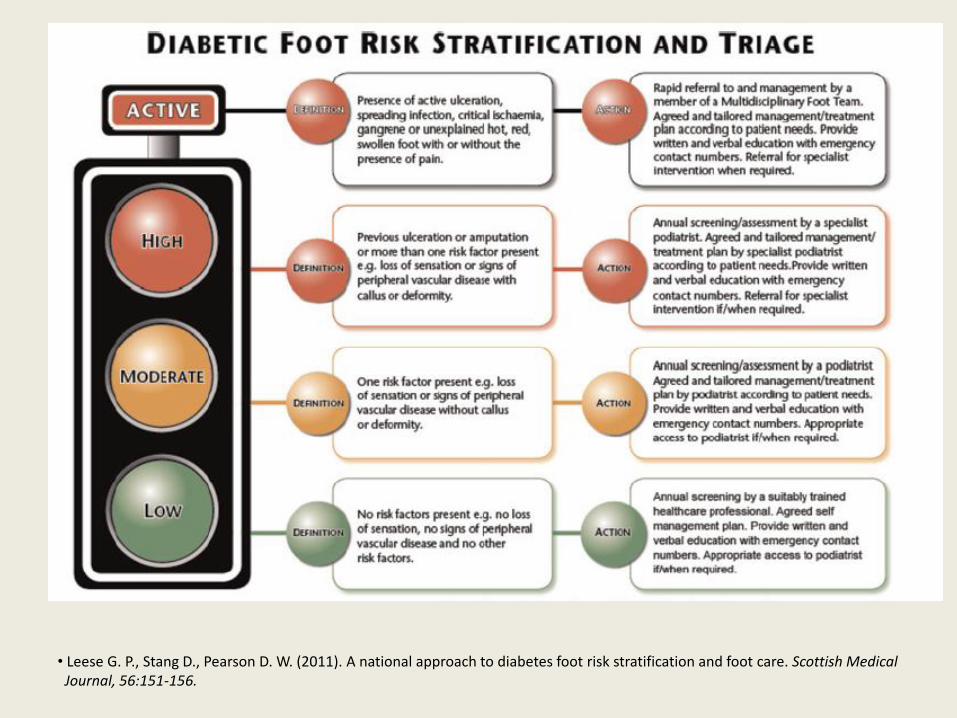
• Leese G. P., Stang D., Pearson D. W. (2011). A national approach to diabetes foot risk stratification and foot care. Scottish Medical Journal, 56:151-156.
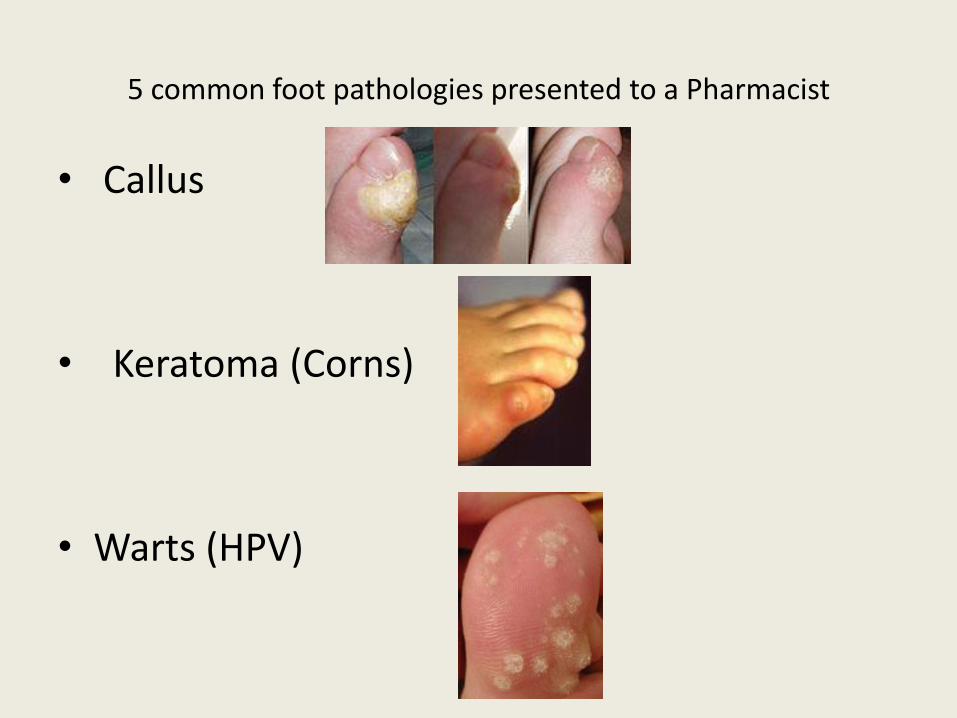
5 common foot pathologies presented to a Pharmacist
• Callus
• Keratoma (Corns)
• Warts (HPV)

• Athlete’s Foot / Fungal nail
•Heel Pain Syndrome
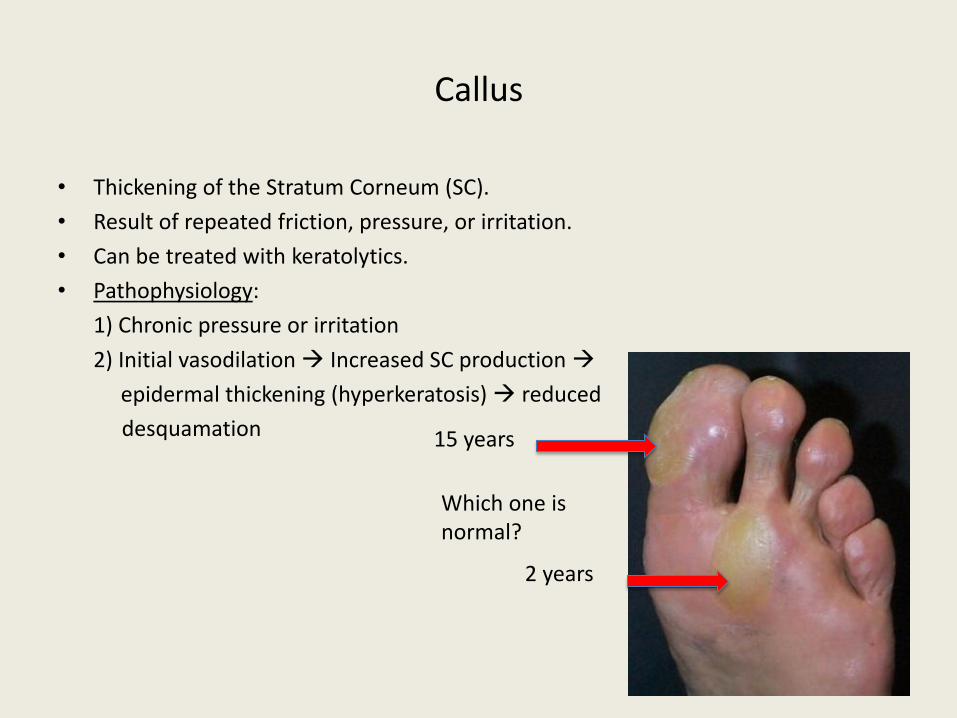
Callus
• Thickening of the Stratum Corneum (SC).
• Result of repeated friction, pressure, or irritation.
• Can be treated with keratolytics.
• Pathophysiology:
1) Chronic pressure or irritation
2) Initial vasodilation Increased SC production
epidermal thickening (hyperkeratosis) reduced
desquamation
Which one is normal?
15 years
2 years
Products to recommend • Kerasal 15 g or 30 g (5% SCA + 10% urea)
• Uremol 20% (emollient) or 40% (keratolytic)
• UriSec 22% or 40%
• Lactic Acid (Lac-Hydrin 12%, Dermalac 12%)
• Mechanism: Urea works by enhancing the water-binding capacity
of the stratum corneum and long-term treatment with urea has
been demonstrated to decrease transepidermal water loss (TEWL)
(Flynn et al. 2001).
Flynn, T. C., Petros, J., Clark, R. E., Viehman, G. E. (2001). Dry skin and moisturizers. Clin Dermatol., 19(4):387-92.
Who to refer?
• Diabetics “Do not pass go” Podiatrist for risk assessment & treatment protocol
• Men & woman recommend OTC 20% urea-based products no improvement after 8 weeks refer for podiatry consult.
• Kids Normally should not have callus Refer before it becomes a chronic problem.
• When callus becomes painful? DDx: mechanical, plantar wart, foreign body granuloma, Porokeratosis, corns (hard, soft, ID) Podiatry dermatology.
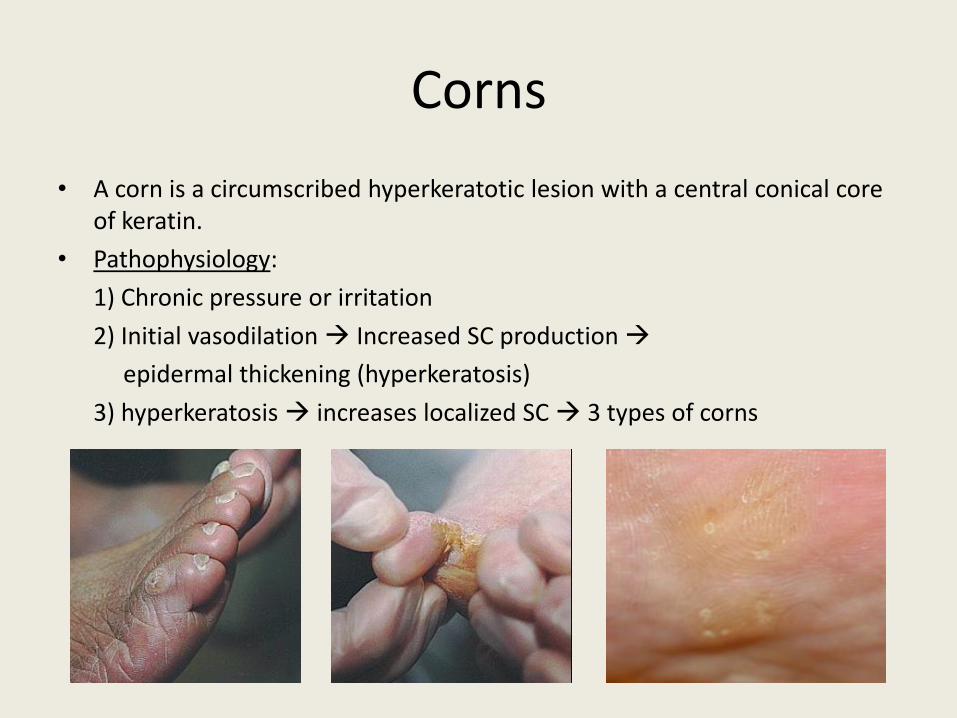
Corns
• A corn is a circumscribed hyperkeratotic lesion with a central conical core of keratin.
• Pathophysiology:
1) Chronic pressure or irritation
2) Initial vasodilation Increased SC production
epidermal thickening (hyperkeratosis)
3) hyperkeratosis increases localized SC 3 types of corns
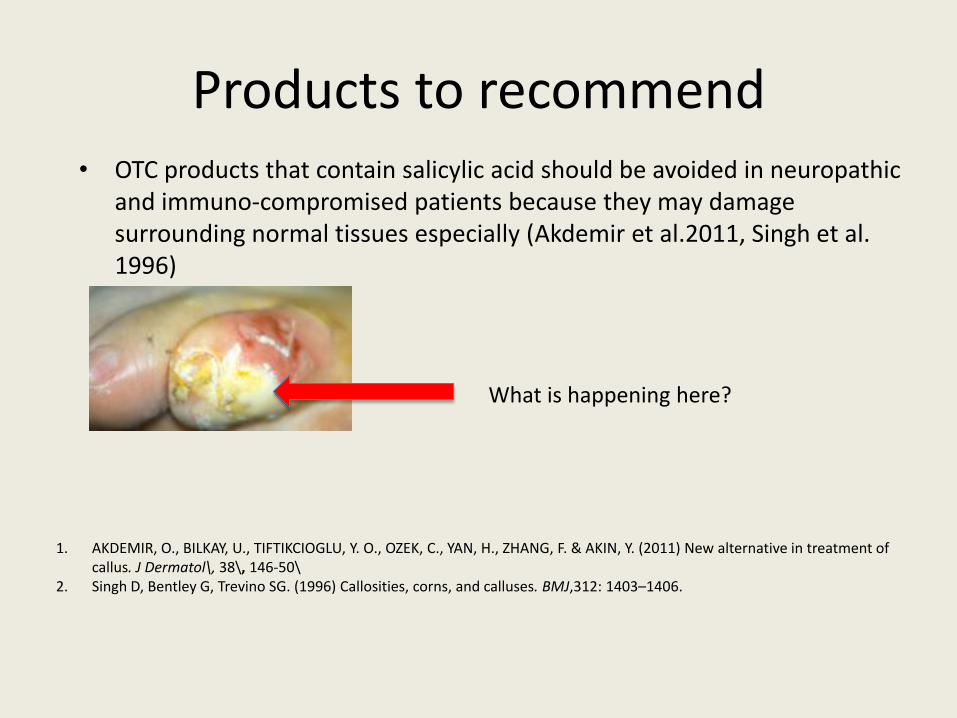
Products to recommend • OTC products that contain salicylic acid should be avoided in neuropathic
and immuno-compromised patients because they may damage surrounding normal tissues especially (Akdemir et al.2011, Singh et al. 1996)
1. AKDEMIR, O., BILKAY, U., TIFTIKCIOGLU, Y. O., OZEK, C., YAN, H., ZHANG, F. & AKIN, Y. (2011) New alternative in treatment of callus. J Dermatol\, 38\, 146-50\
2. Singh D, Bentley G, Trevino SG. (1996) Callosities, corns, and calluses. BMJ,312: 1403–1406.
What is happening here?
• Men & Woman Recommend digital cap versus
corn removers try for 4 weeks + change footwear
no improvement, refer to Podiatry.
• Kids Normally, should NOT get corns refer to
Podiatry for biomechanical examination.
• Diabetics recommend digital caps to prevent further mechanical injury Podiatry GP
Better alternative to corn removers

Warts
• Warts are common and benign epithelial growths caused by
human papillomavirus (HPV).
• Currently more than 100 types of HPV, with type 2, 4
(common wart) & type 1 (Palmoplantar wart).
• Pathophysiology: Thickening of stratum corneum
(hyperkeratosis), thickening of stratum spinosum
(acanthosis), thickening stratum granulosum, rete ridge, blood vessels at dermoepidermal junction.
• S.C.C., most common on the plantar surface that can resemble
warts.
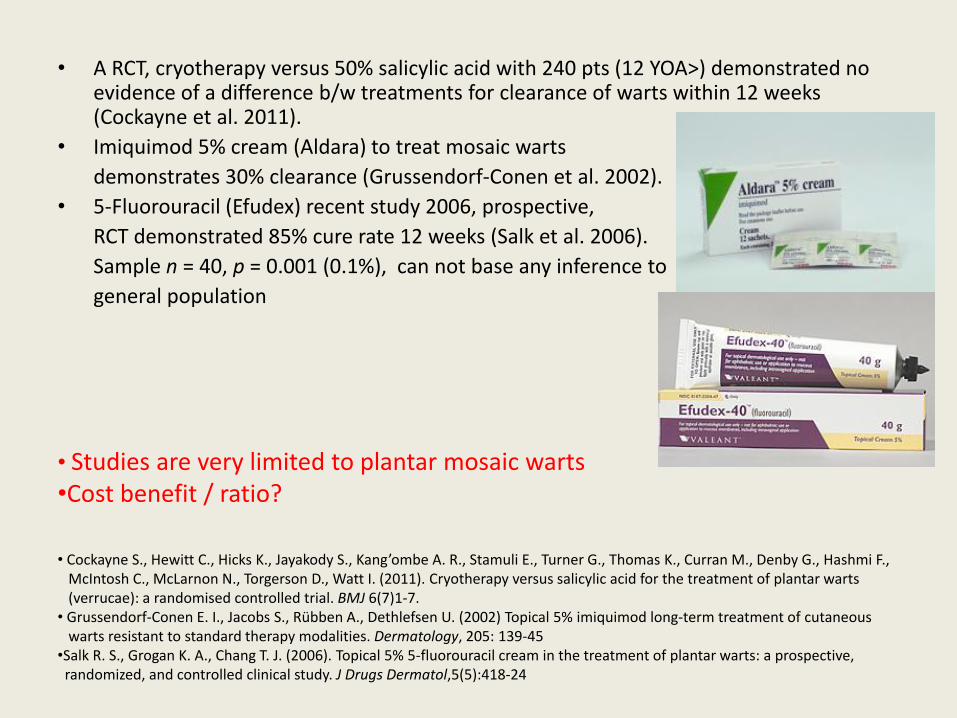
• A RCT, cryotherapy versus 50% salicylic acid with 240 pts (12 YOA>) demonstrated no evidence of a difference b/w treatments for clearance of warts within 12 weeks (Cockayne et al. 2011).
• Imiquimod 5% cream (Aldara) to treat mosaic warts
demonstrates 30% clearance (Grussendorf-Conen et al. 2002).
• 5-Fluorouracil (Efudex) recent study 2006, prospective,
RCT demonstrated 85% cure rate 12 weeks (Salk et al. 2006).
Sample n = 40, p = 0.001 (0.1%), can not base any inference to
general population
• Cockayne S., Hewitt C., Hicks K., Jayakody S., Kang’ombe A. R., Stamuli E., Turner G., Thomas K., Curran M., Denby G., Hashmi F., McIntosh C., McLarnon N., Torgerson D., Watt I. (2011). Cryotherapy versus salicylic acid for the treatment of plantar warts (verrucae): a randomised controlled trial. BMJ 6(7)1-7. • Grussendorf-Conen E. I., Jacobs S., Rübben A., Dethlefsen U. (2002) Topical 5% imiquimod long-term treatment of cutaneous warts resistant to standard therapy modalities. Dermatology, 205: 139-45 •Salk R. S., Grogan K. A., Chang T. J. (2006). Topical 5% 5-fluorouracil cream in the treatment of plantar warts: a prospective, randomized, and controlled clinical study. J Drugs Dermatol,5(5):418-24
• Studies are very limited to plantar mosaic warts •Cost benefit / ratio?
Products to recommend
• Men & Woman, Teenagers SCA products (27% >) because of the thick stratum corneum.
• Kids <27% due to no thickening SC.
When to refer?
• HPV (verruca vulgaris) – Men/Woman If no improvement with OTC after 8 weeks Podiatry (Cryotherapy, electrosurgery, Laser surgery)
• Pregnant woman no caustics or acids (SCA)Podiatry (Cryotherapy)
• Kids no pain with single lesion < 0.5 cm No treatment
pain present with single lesion Treat with OTC and wait 6-to-8 weeks
pain with multiple lesions Podiatry review of options
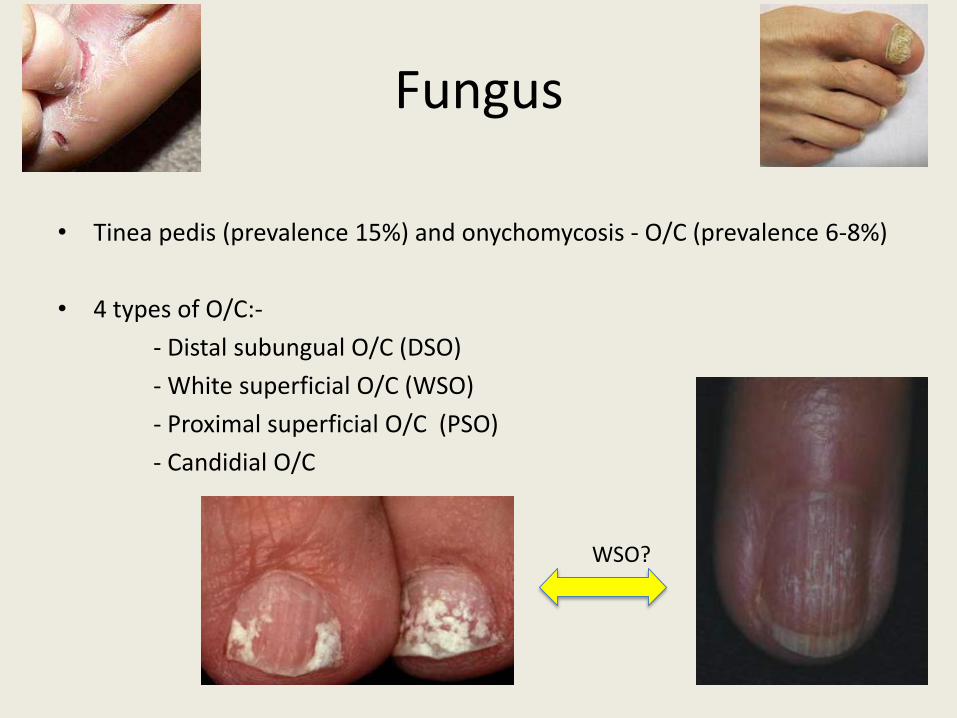
Fungus
• Tinea pedis (prevalence 15%) and onychomycosis - O/C (prevalence 6-8%)
• 4 types of O/C:-
- Distal subungual O/C (DSO)
- White superficial O/C (WSO)
- Proximal superficial O/C (PSO)
- Candidial O/C
WSO?
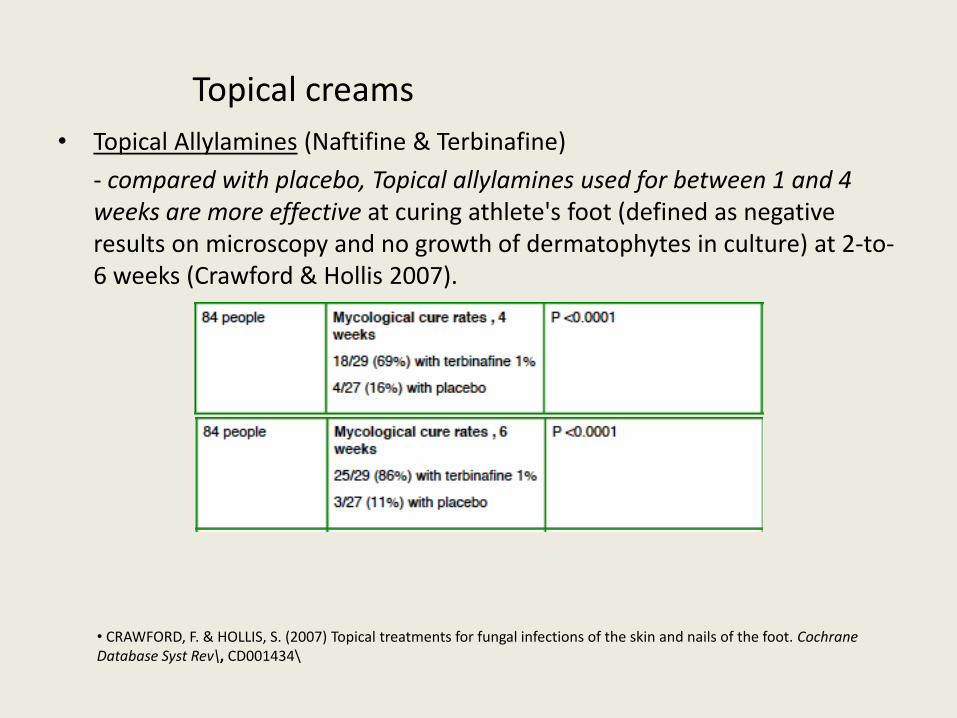
Topical creams
• Topical Allylamines (Naftifine & Terbinafine)
- compared with placebo, Topical allylamines used for between 1 and 4 weeks are more effective at curing athlete's foot (defined as negative results on microscopy and no growth of dermatophytes in culture) at 2-to-6 weeks (Crawford & Hollis 2007).
• CRAWFORD, F. & HOLLIS, S. (2007) Topical treatments for fungal infections of the skin and nails of the foot. Cochrane Database Syst Rev\, CD001434\
• Meta-analysis of 11 trials comparing allylamines and azoles showed a risk ratio of treatment failure RR 0.63 (95% CI 0.42 to 0.94) in favour of allylamines (Crawford & Hollis 2007).
• Allylamines cure slightly more infections than azoles.
• CRAWFORD, F. & HOLLIS, S. (2007) Topical treatments for fungal infections of the skin and nails of the foot. Cochrane Database Syst Rev\,
CD001434\ • Zuvela, T. Got any super-strength fungus creams? [online image] Available from: www.cartoonstock.com/cartoonview.asp?start=32&search=main&catref=tzun633&MA_Artist=Not+Selected&MA_Category=Not+Selected&ANDkeyword=Pharmacist+and+herbs&ORkeyword=&TITLEkeyword=&NEGATIVEkeyword= [Accessed Apri 26 2012]
Antifungals
• An open non-comparative study of Ciclopirox 8% demonstrated 36% cure rate of 40 patients in 9-months (Shemer et al. 2010).
• Inclusion criteria NOT mentioned based on selection of fungus growth/penetration along proximal or distal part of nail;
• Selection bias
SHEMER A., NATHANSOHN N., TRAU H., AMICHAI B., GRUNWALD M. H. (2010). Ciclopirox nail lacquer for the treatment of onychomycosis: An open non-comparative study. The Journal of Dermatology,37(2)137-39.
Griseofulvin
• Griseofulvin first isolated from a Penicillium spp., used to treat ring worm.
• insoluble in water
• administered orally
• reaches the skin and hair
• it is deposited primarily in keratin precursor cells
• mainly effective against Trichophyton rubrum and T. mentagrophyte
• adverse reactions are uncommon
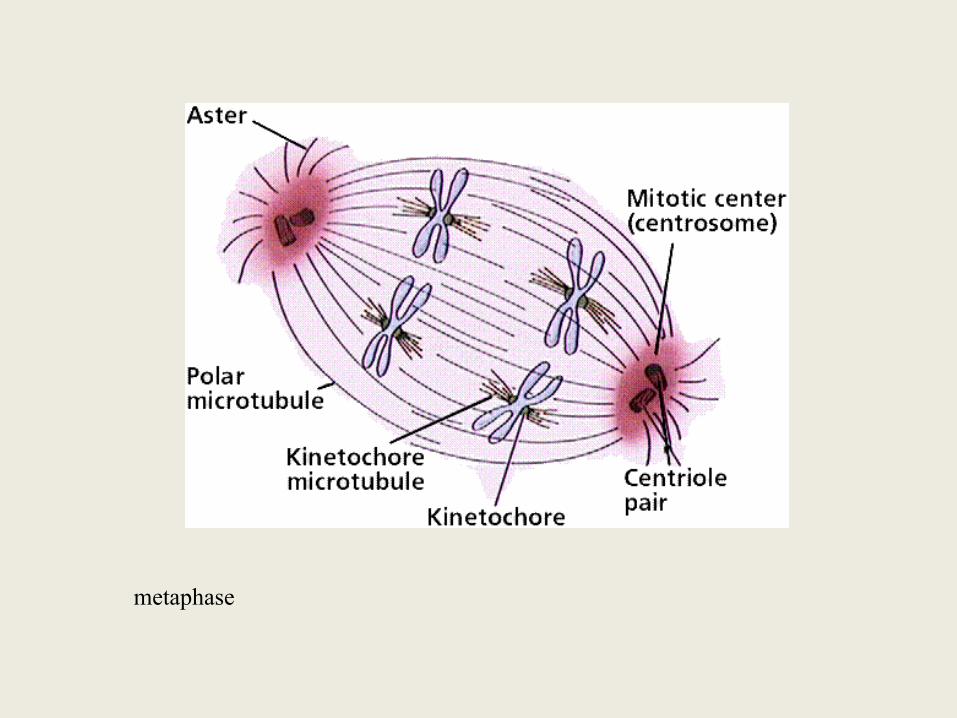
metaphase
Interactions:
• Nicotinamide (Vitamin B3), Alpha-tocopherol (Vitamin E) and dietary fat affect drug performance and toxicity
– Vitamin B3 and dietary fat increase griseofulvin solubility
– Vitamin E slows down the biotransformation rate of griseofulvin elevating its blood serum and skin concentrations
• Vitamin K levels are reduced by griseofulvin
• Affects Probiotic intestinal flora – overgrowth of nonsusceptible organisms particularly
Oral Terbinafine (L
• synthetic antifungal agent
– highly lipophilic
• accumulates in skin, nails, and fatty tissues
• effective against most Candida spp. Aspergillus spp. Trichosporon spp. Cryptococcus spp.
• more effective and significantly less toxic than griseofulvin
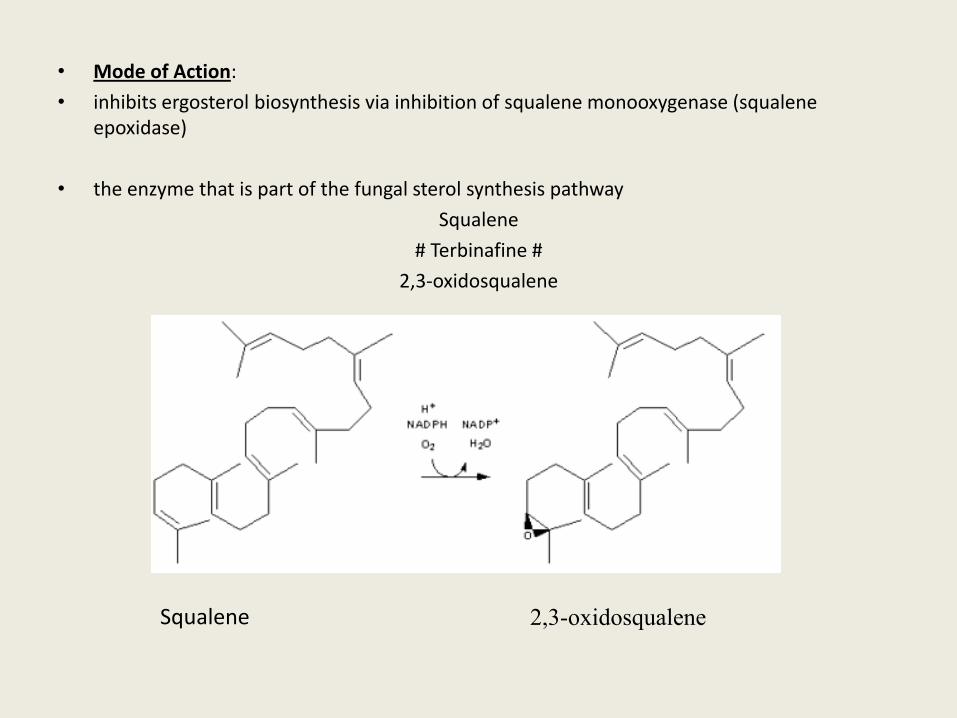
• Mode of Action:
• inhibits ergosterol biosynthesis via inhibition of squalene monooxygenase (squalene epoxidase)
• the enzyme that is part of the fungal sterol synthesis pathway
Squalene
# Terbinafine #
2,3-oxidosqualene
Squalene 2,3-oxidosqualene
What product to recommend?
• Nails No OTC products systemic
white superficial onychomycosis 1% Clotrimazole 6 weeks bid.
• Skin 1% Clotrimazole 60 g (Canestan),
Tolnaftate (Tinactin)
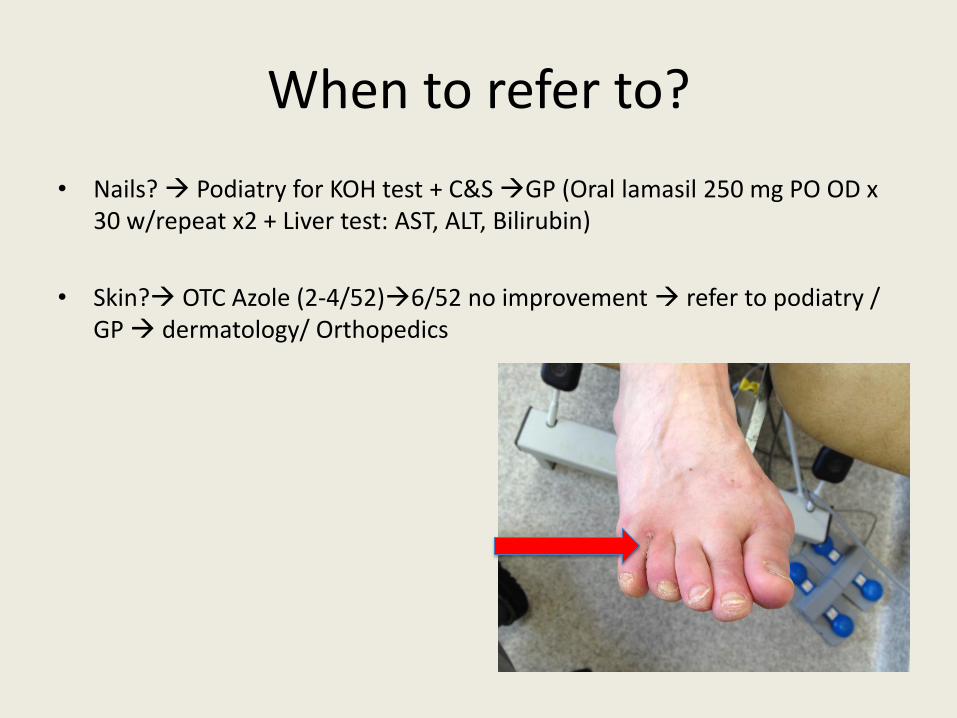
When to refer to?
• Nails? Podiatry for KOH test + C&S GP (Oral lamasil 250 mg PO OD x 30 w/repeat x2 + Liver test: AST, ALT, Bilirubin)
• Skin? OTC Azole (2-4/52)6/52 no improvement refer to podiatry / GP dermatology/ Orthopedics
Heel Pain Syndrome/ Plantar Fasciitis
• “fasciitis” or “Fasciosis”??
– What clinical evidence would constitute “itis?”
• LEMONT, H., AMMIRATI, K. M. & USEN, N. (2003) Plantar fasciitis: a degenerative process (fasciosis) without inflammation. J
Am Podiatr Med Assoc, 93, 234-7
• To treat with NSAID’s or NOT??
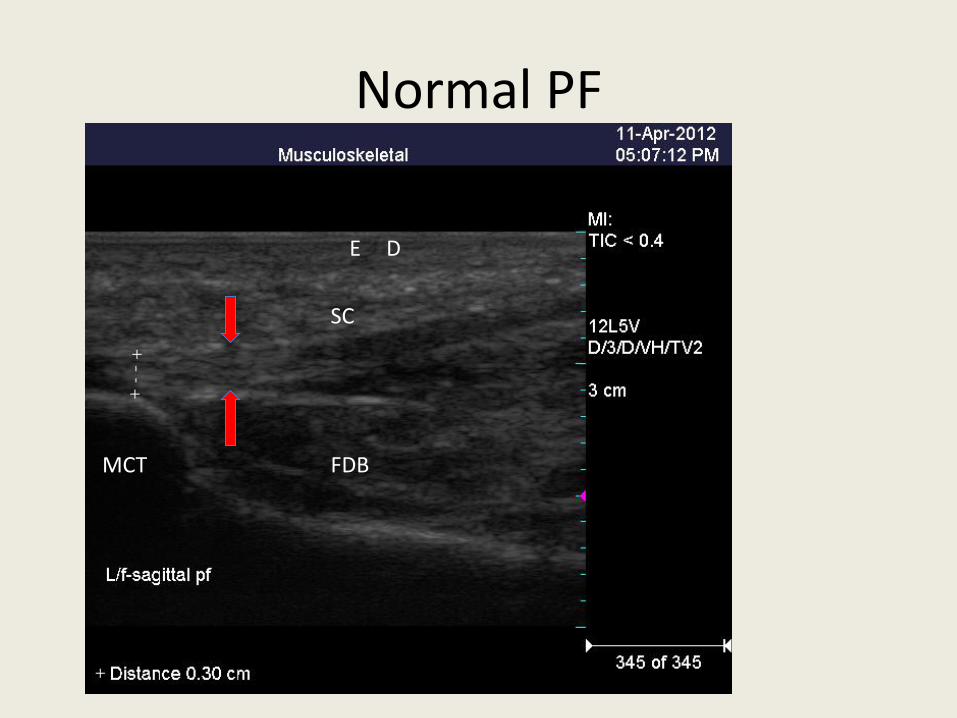
Normal PF
SC
FDB MCT
E D

Clinical Case
• 64 Female, worked in house keeping. •PMHx: Nil; •Current Meds: Voltaren gel 1%; •Allergy: NKA;

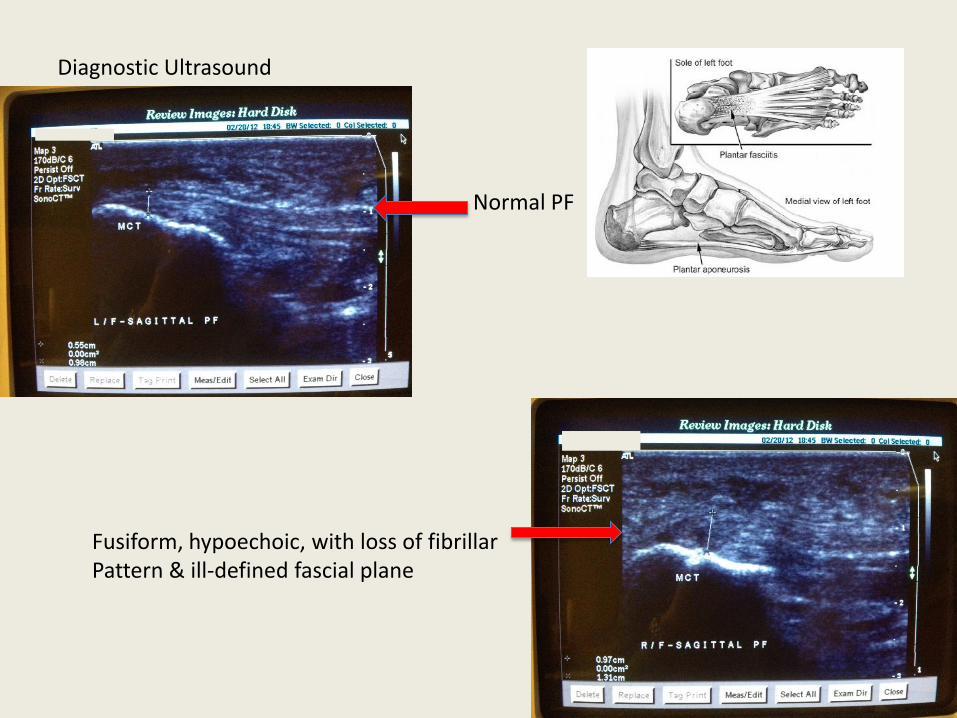
Diagnostic Ultrasound
Normal PF
Fusiform, hypoechoic, with loss of fibrillar Pattern & ill-defined fascial plane
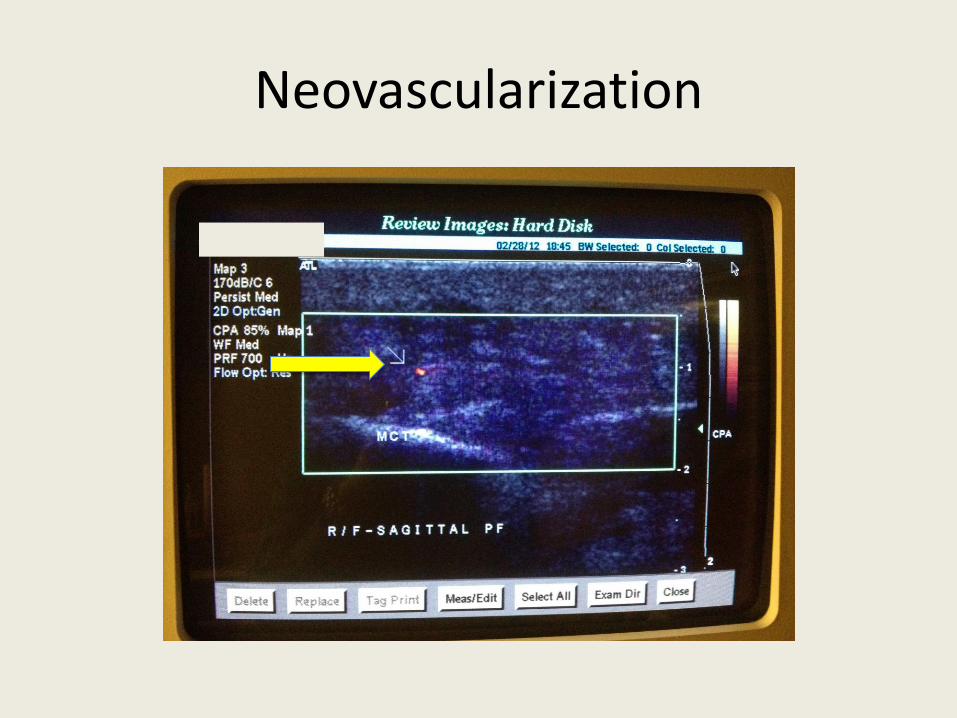
Neovascularization
To Rx NSAID’s or not to Rx ?
• Retrospective study, 27% patients reported significant
improvement with NSAID (Gill & Kiebzak 1996). • Randomized, prospective, placebo-controlled Celecoxib 200
mg (Donley et al 2007). Concluded: NSAID, may increase pain relief.
• Sample size was not sufficient to show statistical significance, n= 23, p = 0.05, statistical power = 0.8 ( n= 128), with p= 0.01 (n= 192).
• Gill, L. H., and Kiebzak, G. M.(1996) Outcome of nonsurgical treatment for plantar fasciitis. Foot Ankle Int. 17:527 – 532. • DONLEY, B. G., MOORE, T., SFERRA, J., GOZDANOVIC, J. & SMITH, R. (2007) The efficacy of oral nonsteroidal anti- inflammatory medication (NSAID) in the treatment of plantar fasciitis: a randomized, prospective, placebo-controlled study. Foot Ankle Int, 28, 20-3.
Celecoxib (Celebrex)
• Is a sulfa NSAID and a selective COX-2
• Used to treat OA (osteoarthrosis) and RA primarily.
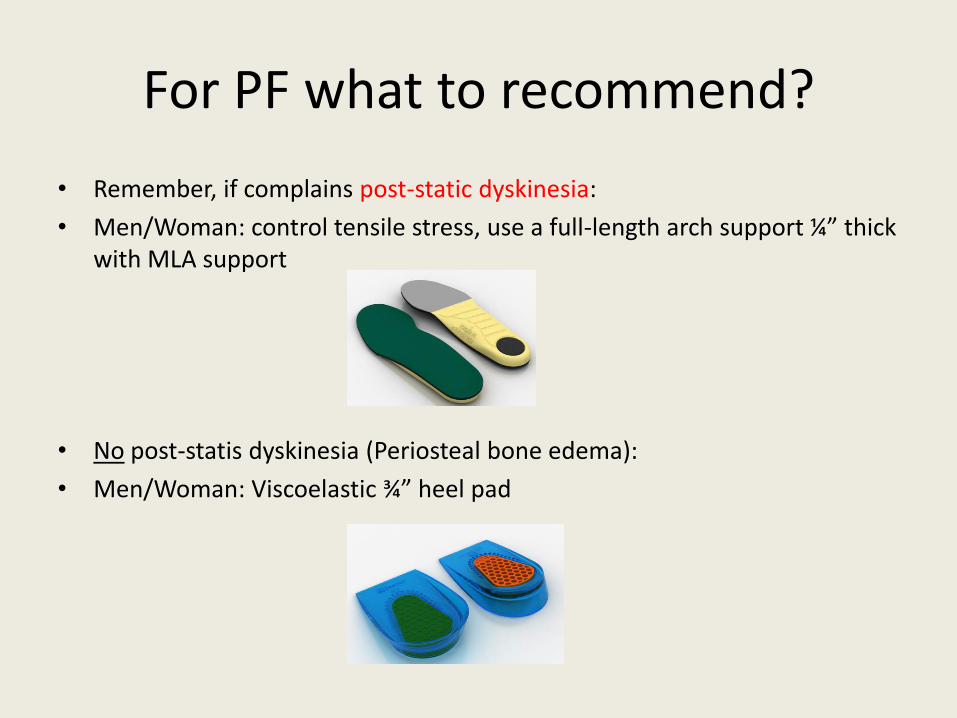
For PF what to recommend?
• Remember, if complains post-static dyskinesia:
• Men/Woman: control tensile stress, use a full-length arch support ¼” thick with MLA support
• No post-statis dyskinesia (Periosteal bone edema):
• Men/Woman: Viscoelastic ¾” heel pad
Who to refer to for PF?
• Heel pain syndrome referral (men/woman) if OTC product does not decrease symptoms 6/52 Podiatry.
• Heel pain syndrome + burning (men/woman) PodiatryNeurology (EMG)
• Kids (Sever’s disease, Calcaneal apophysitis) if OTC ¾” heel pad/ramp does not alleviate symptoms 6/52 Podiatry (DxUS) x-ray Pediatrician.
Good night bunions?
• Cohort study 30 patients with complaint hallux valgus • Randomly divided into two groups: Case group had a custom splint and control was given OTC splints. • Inclusion criteria for hallux valgus angles were mild or moderate
• p = case group < 0.001, no significance found in control group (Mirzashahi et al. 2012) • Night splints do not work for painful hallux valgus (Tehraninasr et al. 2008).
• MIRZASHAHI, B., AHMADIFAR, M., BIRJANDI, M. & POURNIA, Y. (2012) Comparison of designed slippers splints with the splints available on the market \ in the treatment of hallux valgus. Acta Med Iran\, 50\, 107-12\ • TEHRANINASR, A., SAEEDI, H., FOROGH, B., BAHRAMIZADEH, M. & KEYHANI, M. R. (2008) Effects of insole with toe-separator and night splint on patients with painful\ hallux valgus: a comparative study. Prosthet Orthot Int\, 32\, 79-83\
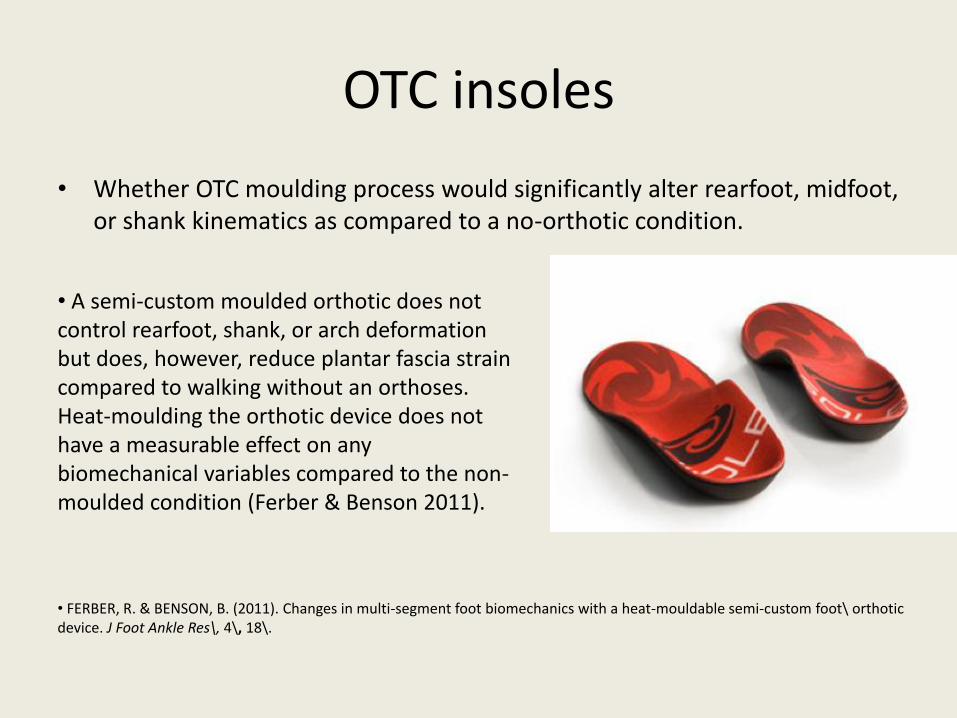
OTC insoles
• Whether OTC moulding process would significantly alter rearfoot, midfoot, or shank kinematics as compared to a no-orthotic condition.
• A semi-custom moulded orthotic does not control rearfoot, shank, or arch deformation but does, however, reduce plantar fascia strain compared to walking without an orthoses. Heat-moulding the orthotic device does not have a measurable effect on any biomechanical variables compared to the non-moulded condition (Ferber & Benson 2011).
• FERBER, R. & BENSON, B. (2011). Changes in multi-segment foot biomechanics with a heat-mouldable semi-custom foot\ orthotic device. J Foot Ankle Res\, 4\, 18\.
Baldwin, Mike. Arch support group.[online image] Available from: www.cartoonstock.com/directory/numbers/12_step_program.asp [Accessed on April 26 2012]
• Arch Pain Medium density to reduce tensile stress
• Heel Pain post-static dyskinesia Heel pain arch support
• Heel Pain No post-static dyskinesia Heel pad ¾”
• Forefoot pain metatarsal pad / Ball of foot
• Diabetic/ Rheumatoid foot Tridensity insole (memory fit)
Basic Algorithym

Podiatry
• MYTH 1: Banana peel, duct tape, nail polish, penny, and garlic are all efficient treatments for warts.
• Myth 2: Tea Tree oil (TTO) is efficient treatment for fungal nails.
Carson, C. F., Hammer, K. A., and Riley, T. V. (2006) Melaleuca alternifolia (Tea Tree) Oil: a Review of
Antimicrobial and Other Medicinal Properties. Clin. Microbiol. Rev. 19 (1) 50-62.
Myth 3: Does Ranitidine clear verruca vulgaris?
• Fit, K. E. and William, P. C. (2007). Use of histamine 2- antagonists for the treatment of verruca vulgaris. Ann. Pharmacother.,41(7)1222-6.
• Myth 4: Flat feet and high arches are bad?
• Myth 5: All babies have flat feet
• Madden, C. Our trials show that new drugs performs no better than placebo. [online image]. Available from: www.cartoonstock.com/cartoonview.asp?start=3&search=main&catref=cman369&MA_Artist=Not+Selected&MA_Category=Not+Selected&ANDkeyword=Pharmacist+and+herbs&ORkeyword=&TITLEkeyword=&NEGATIVEkeyword= [Accessed April 26 2012]
Podiatry and POM’s
• Pharmacy regulations will include Podiatry who have prescribing privileges.
• COPOM currently working on plan for independent prescribing within the RHP Act.
• Additional training will be required for U.K. Podiatrists (MSc. Program) and for DPM’s (from the United States).
McLlwaine, Randall. I’m the podiatrist around here. [online image]. Available from: www.cartoonstock.com/fullsearch.asp?ANDkeyword=Podiatry&ORkeyword=&TITLEkeyword=&NOTkeyword=&performSearch=TRUE&mainArchive=mainArchive&MA_Artist=&MA_Category= [Accessed on April 26 2012].