clinical management: hormonal contraception · 2018-04-04 · clinical management: hormonal...
TRANSCRIPT


Clinical Management: Hormonal Contraception
Kathleen Besinque, PharmDLoma Linda University School of [email protected] to disclose
Sarah McBane, PharmD, CDE, BCPS, FCCPUCSD Skaggs School of Pharmacy & Pharmaceutical [email protected] to disclose

Disclosure
The presenters have no conflicts of interest to disclose.

Handout resources for session
To facilitate your participation in today’s program, you may want to print or have available the following documents:
The California Board of Pharmacy Approved Protocol for Hormonal Contraception◦ http://www.pharmacy.ca.gov/licensing/homonal_contraception.shtml
The MEC Chart for hormonal contraceptives (2016)◦ http://www.cdc.gov/reproductivehealth/contraception/pdf/summary-chart-us-
medical-eligibility-criteria_508tagged.pdf

Pharmacists Role in Contraception Care
Provide contraceptives within the scope of practice (SB493 authorized changes)◦ Pharmacists may furnish self-administered hormonal contraceptives pursuant to a
statewide protocol (4502.3)◦ The statewide protocol must be approved by the Boards of Pharmacy, ACOG, CPhA and the Medical Board
◦ Applies to all pharmacists who have received the training
A resource for information and advice ◦ Manage side effects
◦ Provide advice re: drug interactions and missed pills
◦ Source of information regarding new methods
◦ Applies to all pharmacists
5
Contraceptive Methods in US
•Hormonal methods• Combined hormonal contraceptives
• Progestin-only contraceptives
• Emergency contraceptive pills
• Progestin Intrauterine devices
• Implants
•Non-hormonal methods• Barrier contraceptive methods
• Fertility Awareness-Based Methods
• Lactational Amenorrhea Method
• Coitus Interruptus
• Copper Intrauterine device
• Female and Male Sterilization


Protocol for Pharmacists Furnishing Self-Administered Hormonal Contraception
(a) A pharmacist furnishing self-administered hormonal contraception pursuant to Section 4052.3 of the Business and Professions Code shall follow the protocol specified in subdivision (b) of this section.
(b) Protocol for Pharmacists Furnishing Self-Administered Hormonal Contraception
(1) Authority: Section 4052.3(a)(1) of the California Business and Professions Code authorizes a pharmacist to furnish self-administered hormonal contraceptives in accordance with a protocol approved by the California State Board of Pharmacy and the Medical Board of California. Use of the protocol in this section satisfies that requirement.
(2) Purpose: To provide timely access to self-administered hormonal contraception medication and to ensure that the patient receives adequate information to successfully comply with therapy.
(3) Definition of Self-Administered Hormonal Contraception: Hormonal contraception products with the following routes of administration are considered self-administered:
◦ Oral;
◦ Transdermal;
◦ Vaginal;
◦ Depot Injection.
8
http://www.pharmacy.ca.gov/publications/hormonal_contraception_protocol_rphs.pdf

HC Protocol RequirementsTraining before implementation• complete one hour of continuing education program from a board-approved provider regarding HC and application of US MEC
(graduates from California School after 2014 excepted)
•A self-screening questionnaire with specific questions must be used
•Assessments required by the pharmacist• Review of self-assessment questionnaire and application of the Medical Eligibility Criteria (MEC)
• BP measurement before providing estrogen-containing products
•Patient Education required of the pharmacist• For the method selected including administration instructions
• Written patient education ( a “Fact Sheet”)
•Documentation of services and notification to woman primary care provider • Medication profile
• Patient to provide PCP contact info or may decline
•Referral as needed• for preventative care & screenings
• for ineligible patients
• for long-acting reversible contraceptives

http://www.pharmacy.ca.gov/publications/patient_screening_tool_consumers_english.pdf
Note to patient: print out and complete this questionnaire and bring to your pharmacy if you seek self‐ administered hormonal contraception. You may wish to call your pharmacy first to make certain they are able to provide this service at this time. You may also obtain the form from participating pharmacies.
All questions on this form must be used. The form may be modified/branded provided all required information is included.


Fact Sheets:The pharmacist should provide the patient with a copy of a current, consumer-friendly, comprehensive birth control guide such as that created by the Food and Drug Administration (FDA).
The pharmacist shall provide the patient with the FDA-required patient product information leaflet included in all self-administered hormonal contraception products. The pharmacist shall answer any questions the patient may have regarding self-administered hormonal contraception.
The pharmacist should provide the patient with a copy of an administration specific factsheet.
Examples of appropriate factsheets are available on the Board of Pharmacy’s website.

Documentation and NotificationThe pharmacist shall notify the patient’s primary care provider of any drug(s) or device(s) furnished to the patient, or enter the appropriate information in a patient record system shared with the primary care provider, as permitted by that primary care provider.
If the patient does not have a primary care provider, or is unable to provide contact information for his or her primary care provider, the pharmacist shall provide the patient with a written record of the drug(s) or device(s) furnished and advise the patient to consult an appropriate health care professional of the patient’s choice.
Each self-administered hormonal contraceptive furnished by a pharmacist…. shall be documented in a patient medication record and securely stored within the originating pharmacy or health care facility for a period of at least three years from the date of dispense.

New Recommendations2016 MEC
• 4 New conditions
• Cystic fibrosis
• Multiple sclerosis
• Women using selective serotonin reuptake inhibitors (SSRIs)
• Women using St.John’swort
• 1 new contraceptive method
• Ulipristal acetate (UPA) for emergency contraception

Changesto Existing Recommendations
• Migraine headaches
• Superficial venousdisease
• Gestational trophoblasticdisease (IUD)
• Women using antiretroviral therapy
• Postpartum and breastfeeding women (IUD)
• Women with known dyslipidemia
• Human immunodeficiency virus(IUD)
• Factorsrelated to sexually transmitted diseases (IUD)



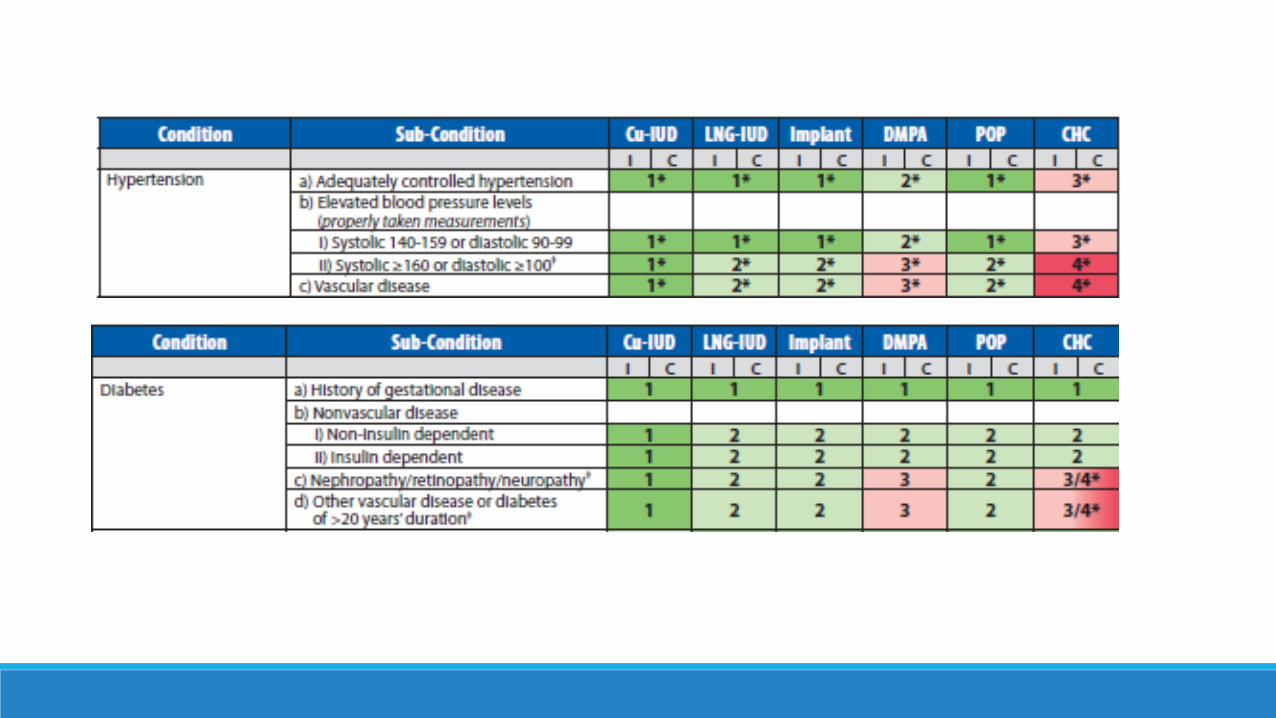
United States Medical Eligibility Criteria for Contraceptive Use : Organization
• Criteria are organized according to:
• Contraceptive method
• Patient characteristics (age, smoking status, etc.)
• Preexisting conditions (hypertension, epilepsy, etc.)
• Criteria use a numeric scheme to provide the recommendations for contraceptives being used for contraceptive purposes only, not for treatment of medical conditions
20

US Medical Eligibility Criteria
• Criteria are organized according to:
– Contraceptive method
– Patient characteristics (age, smoking status, etc.)
– Preexisting conditions (hypertension, epilepsy, etc.)
• Criteria use a numeric scheme to provide
the recommendations for contraceptives
being used for contraceptive purposes
only, not for treatment of medical
conditions
21
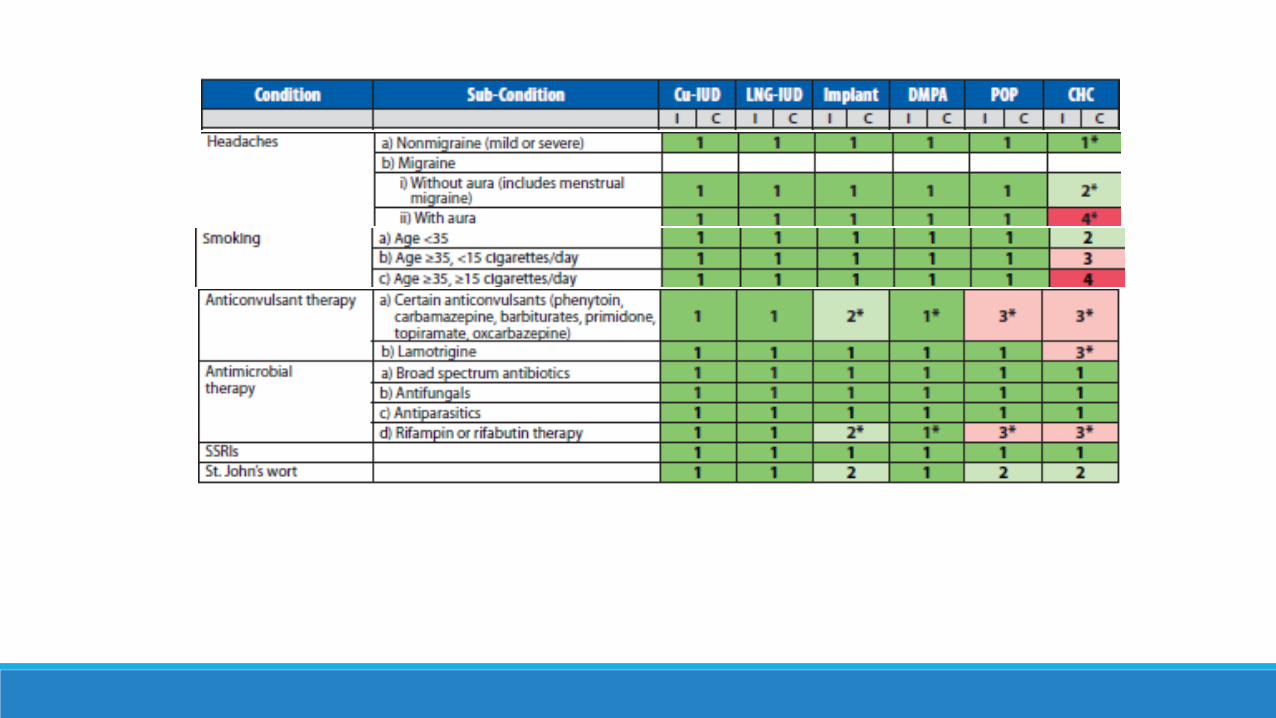
Safety/Risk Categories
1 Method can be used without restriction
2Advantages generally outweigh theoretical or proven risk
3Method usually not recommended unless other, more appropriate methods are not available or not acceptable
4 Method not to be used


Self Administered Hormonal Contraceptive OptionsType of method desired
◦ Pill (oral)
◦ Vaginal ring
◦ Patch
◦ Injection
◦ Other
Regimen options◦ Type of regimen
◦ Monphasic
◦ Triphasic
◦ Multi-phasic
◦ Duration of a cycle
◦ 21 day, 28 day
◦ Extended cycle (91 day)
Formulary issues◦ What is covered?
◦ Cost
Hormone options◦ estrogen/progestin
◦ progestin only
Specific hormones available◦ estrogens:
◦ estradiol (mestranol)
◦ estradiol valerate
◦ progestins
◦ 1st generation estranes
◦ norethindrone
◦ 2nd generation gonanes
◦ levonorgestrel
◦ 3rd generation
◦ desogen
◦ norgestimate
◦ Other: drospirenone
23

How will you select HC products?
Creating your own “formulary”
◦ What products are commonly prescribed to women in your practice?
◦ Are there formulary limitations (quantity, product) with your most common insurance plans?
◦ How many products will you comfortably be able to maintain in stock?
Get comfortable with a handful of products that you can keep in stock.
◦ Select a monophasic and a triphasic product
◦ Select one product with each of the most commonly used progestinsnorethindrone, levonorgestrel, drospirenone
◦ Select a range of estrogen doses 10mcg to 35mcg
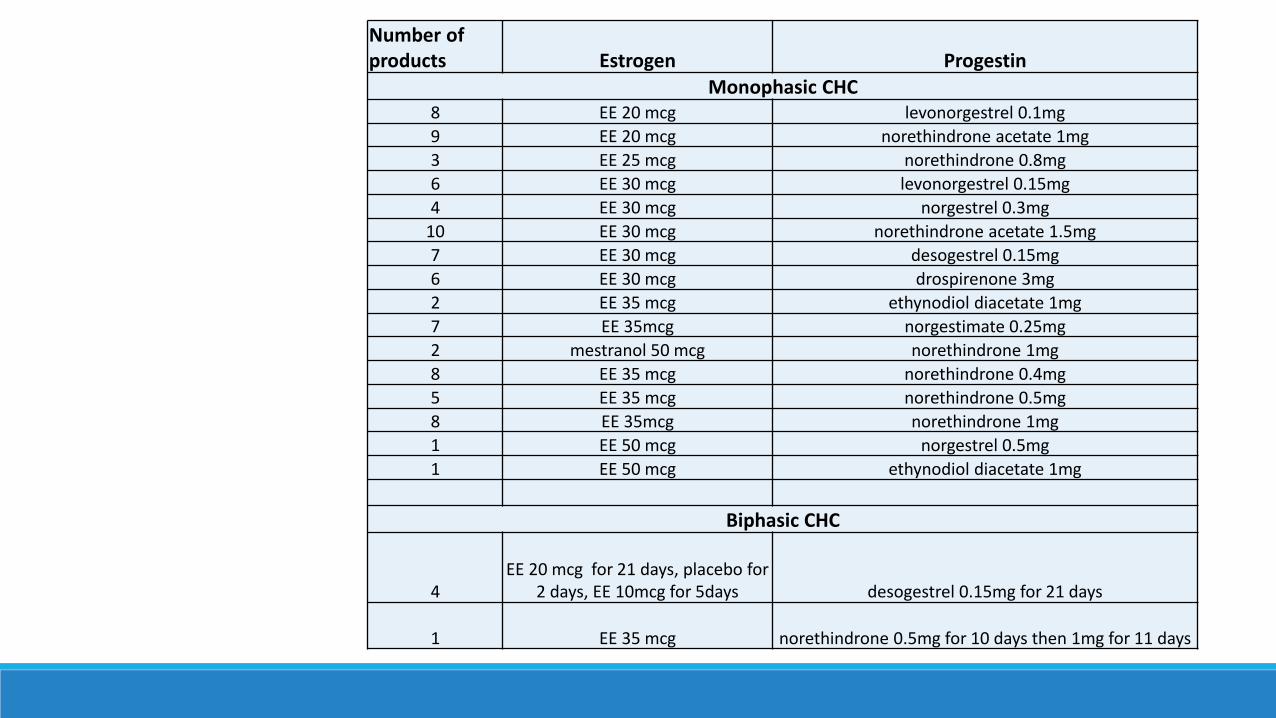
Number of products Estrogen Progestin
Monophasic CHC8 EE 20 mcg levonorgestrel 0.1mg
9 EE 20 mcg norethindrone acetate 1mg
3 EE 25 mcg norethindrone 0.8mg
6 EE 30 mcg levonorgestrel 0.15mg
4 EE 30 mcg norgestrel 0.3mg
10 EE 30 mcg norethindrone acetate 1.5mg
7 EE 30 mcg desogestrel 0.15mg
6 EE 30 mcg drospirenone 3mg
2 EE 35 mcg ethynodiol diacetate 1mg
7 EE 35mcg norgestimate 0.25mg
2 mestranol 50 mcg norethindrone 1mg
8 EE 35 mcg norethindrone 0.4mg
5 EE 35 mcg norethindrone 0.5mg
8 EE 35mcg norethindrone 1mg
1 EE 50 mcg norgestrel 0.5mg
1 EE 50 mcg ethynodiol diacetate 1mg
Biphasic CHC
4EE 20 mcg for 21 days, placebo for
2 days, EE 10mcg for 5days desogestrel 0.15mg for 21 days
1 EE 35 mcg norethindrone 0.5mg for 10 days then 1mg for 11 days

Number of products Estrogen Progestin
Triphasic CHC
2
EE 20 mcg x 5 days, 30 mcg x 7 days, 35 mcg x 9 days
norethindrone acetate1 mg x 21 days
2 EE 25 mcg x 21 days
norgestimate0.18 mg x 7 days,
0.215 mg x 7 days, 0.25 mg x 7 days.
3 EE 25 mcg x 21 days
desogestrel0.1 mg x 7 days,
0.125 mg x 7 days, 0.15 mg x 7 days.
4
EE 30 mcg x 6 days, 40 mcg x 5 days, 30 mcg x 10 days.
levonorgestrel0.05 mg x 6 days,
0.075 mg x 5 days, 0.125 mg x 10 days.
7 EE 35 mcg x 21 days
norgestimate0.18 mg x 7 days,
0.215 mg x 7 days, 0.25 mg x 7 days.
3 EE 35 mcg x 21 days
norethindrone0.5 mg x 7 days, 1 mg x 9 days,
0.5 mg x 5 days.
7 EE 35 mcg x 21 days
norethindrone0.5 mg x 7 days,
0.75 mg x 7 days, 1 mg x 7 days.
Number of products Estrogen Progestin
Four-phaisc CHC
1
Estradiol valerate 3 mg x 2 days, then 2 mg x 22
days, then 1 mg x 2 days, then 2-day pill-
free interval
dienogestnone x 2 days, then 2 mg x 5 days, then
3 mg x 17 days, thennone x 4 days
Extended cycle products
1 EE 10 mcg x 26 daysnorethindrone acetate 1
mg x 24 days
3 EE 20 mcg x 24 daysnorethindrone acetate 1
mg x 24 days
4EE 20 mcg x 84 days, 10
mcg x 7 days.levonorgestrel 0.1 mg x 84
days
4 EE 30 mcg x 84 dayslevonorgestrel 0.15 mg x
84 days
4EE 30 mcg x 84 days,
10 mcg x 7 days.levonorgestrel 0.15 mg x
84 days
1
EE 20 mcg x 42 days, 25 mcg x 21 days,
30 mcg x 21 days, then 10 mcg x 7 days
levonorgestrel 0.15 mg x 84 days
6 EE 20 mcg x 24 daysdrospirenone 3 mg x 24
days
1 EE 20 mcg levonorgestrel 90 mcg
Progestin only pills10 ************ norethindrone 0.35 mg
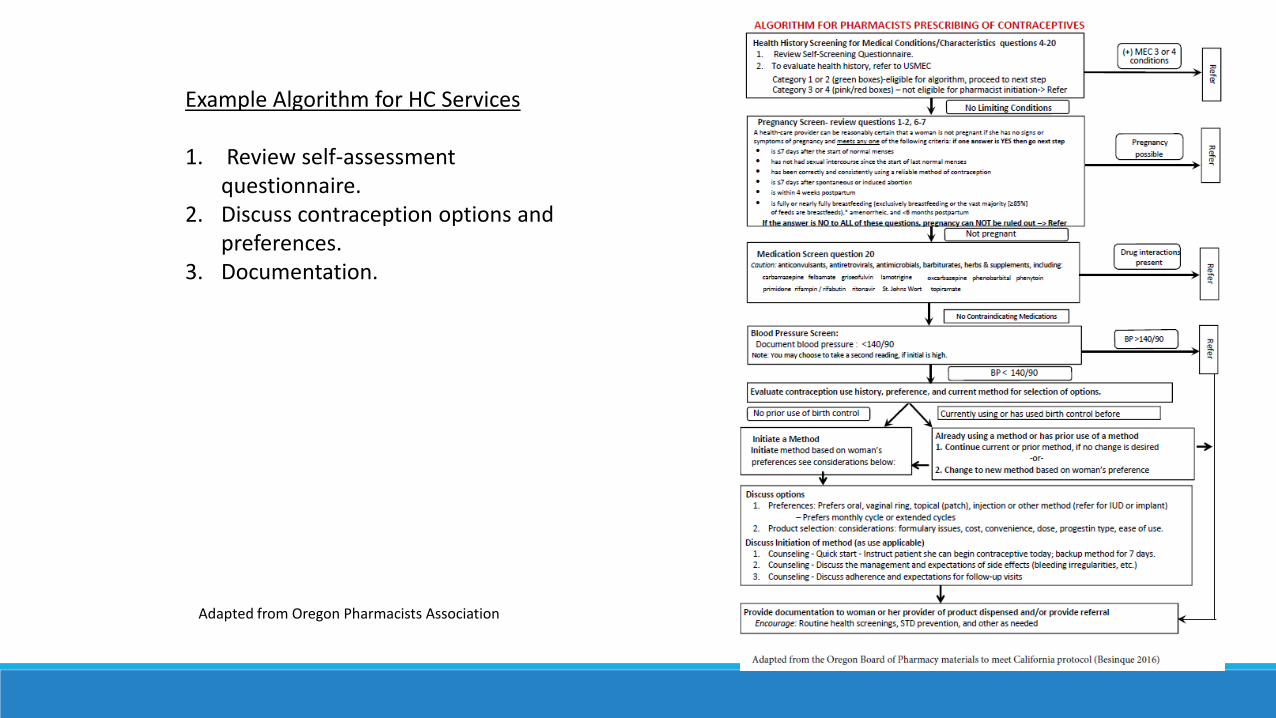
Adapted from Oregon Pharmacists Association
Example Algorithm for HC Services
1. Review self-assessment questionnaire.
2. Discuss contraception options and preferences.
3. Documentation.
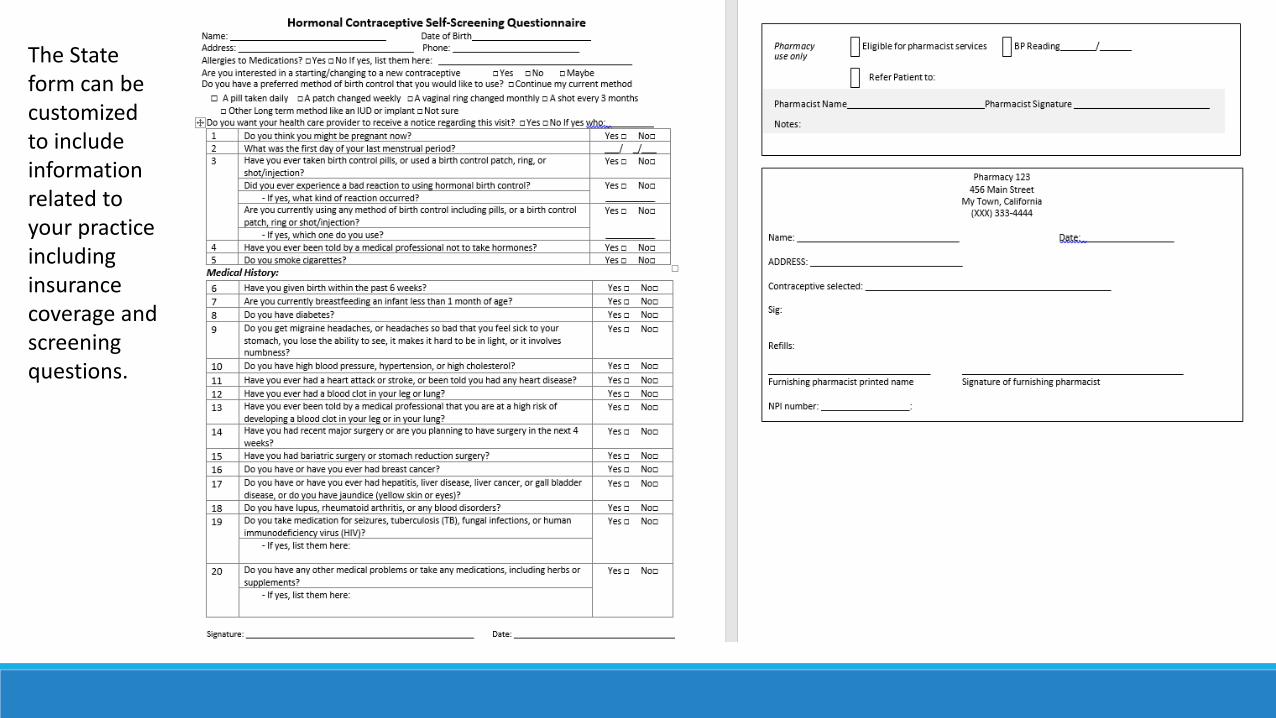
The State form can be customized to include information related to your practice including insurance coverage and screening questions.

• Review the self-screening questionnaire• What do you need to do before furnishing HC?• Does Lora meet eligibility for pharmacist furnishing HC?• Questions to ask regarding methods?


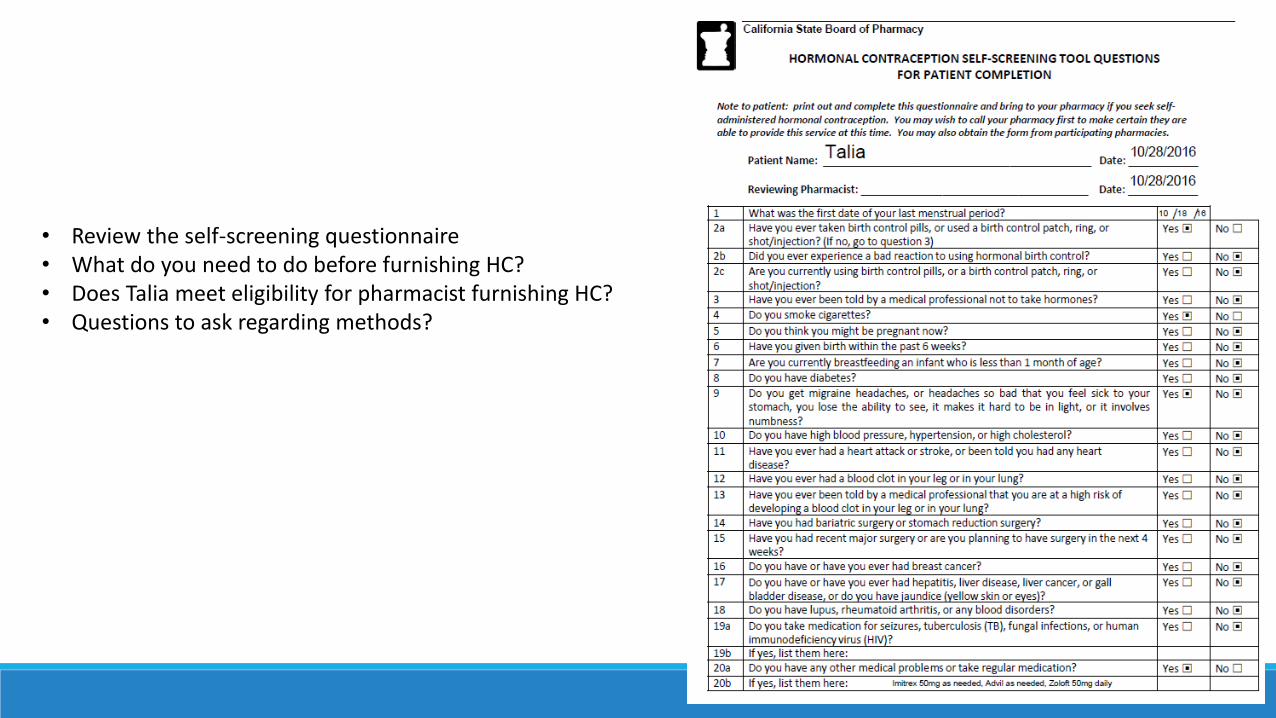
• Review the self-screening questionnaire• What do you need to do before furnishing HC?• Does Talia meet eligibility for pharmacist furnishing HC?• Questions to ask regarding methods?
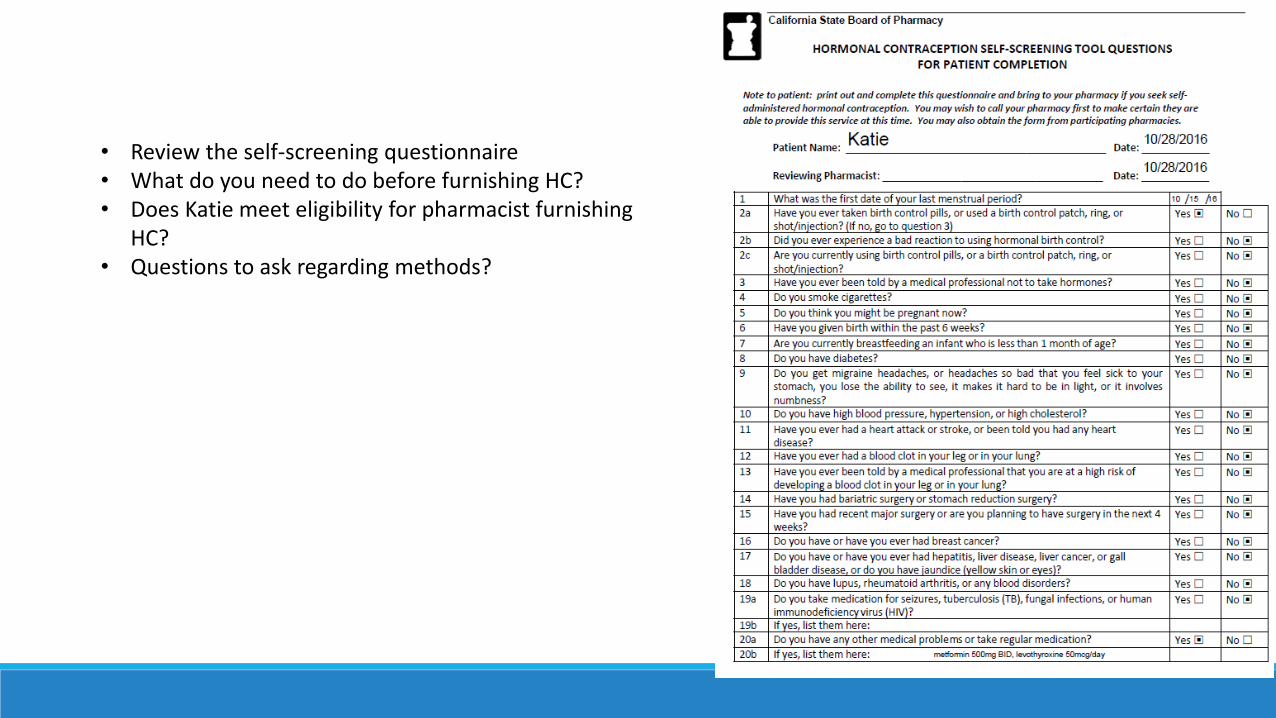
• Review the self-screening questionnaire• What do you need to do before furnishing HC?• Does Katie meet eligibility for pharmacist furnishing
HC?• Questions to ask regarding methods?

Blood Pressure
Initial BP reading high- ask to rest for 5 minutes and re-check.
If with-in normal range- then ok to continue, if not then refer
Other Practice Issues
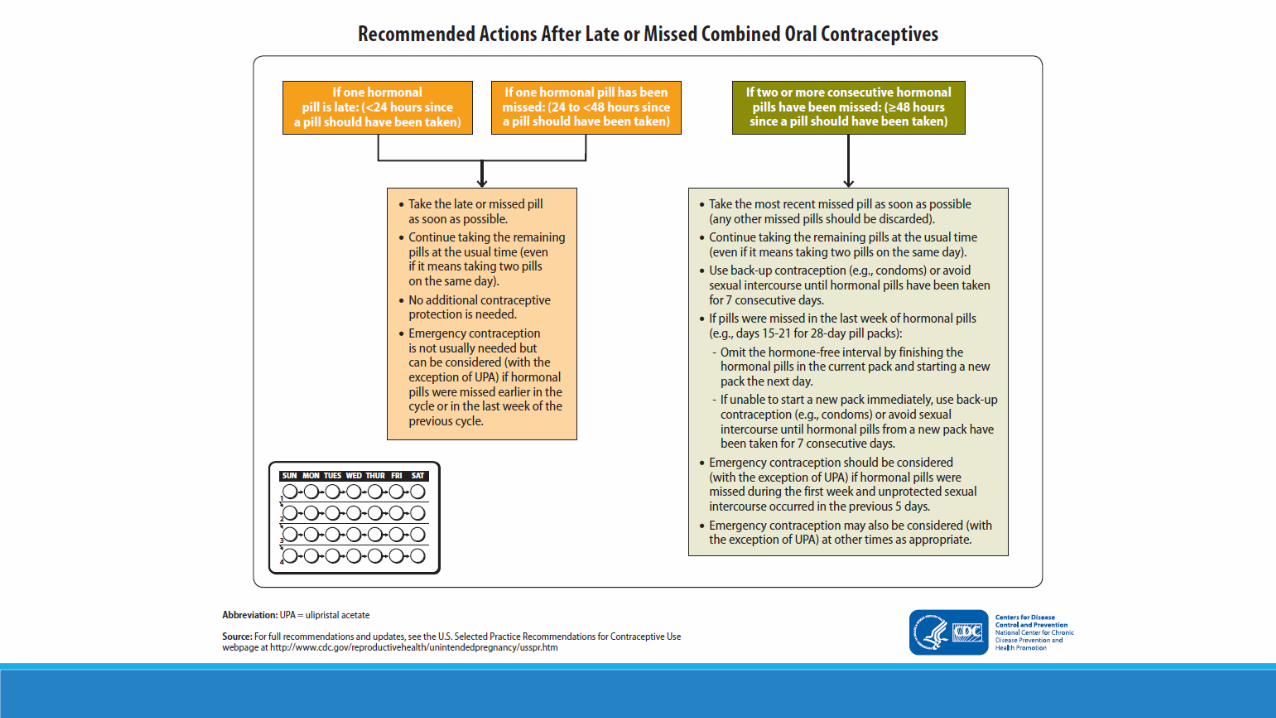
•Missed pills
•Emergency contraception
•Minors and consent

Emergency Contraception
•Can be provided with or without HC:
• Any time- in advance of need
• Within 5 days of unprotected intercourse with declining effectiveness over time
•EC options
• Copper IUD most effective
• Ulipristal (ella®) prescription only • included in California EC protocol for pharmacists
• Levonorgestrel 1.5mg tablets OTC, no age or other restrictions
41
http://www.pharmacy.ca.gov/consumers/emergency_cont.shtml
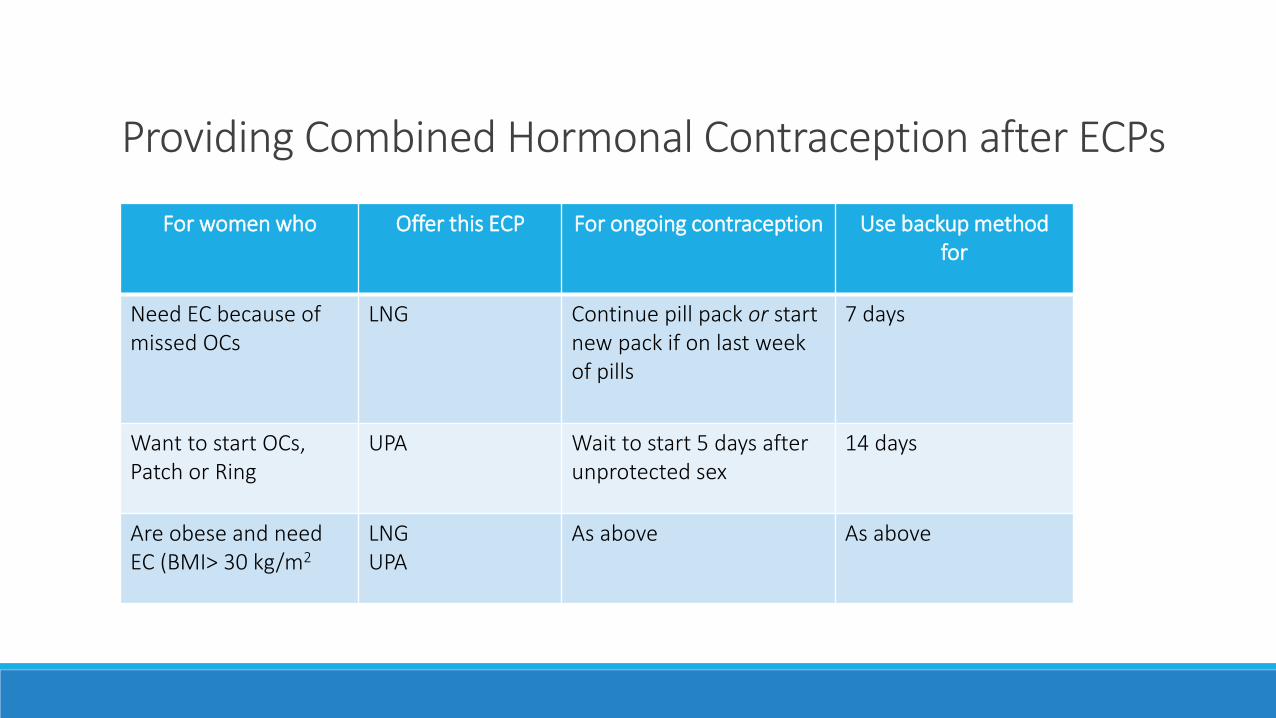
Providing Combined Hormonal Contraception after ECPs
For women who Offer this ECP For ongoing contraception Use backup method for
Need EC because ofmissed OCs
LNG Continue pill pack or start new pack if on last week of pills
7 days
Want to start OCs, Patch or Ring
UPA Wait to start 5 days after unprotected sex
14 days
Are obese and need EC (BMI> 30 kg/m2
LNGUPA
As above As above
MINORS RIGHTSA minor (person under 18 years of age) may consent to health care services that are related to prevention of or treatment of pregnancy
◦ Including prenatal vitamins, EC, contraception
A minor who is ≥12, may consent to medical care related to the diagnosis or treatment of infectious diseases
◦ Including STIs
A minor is competent to make their own decisions if they1. Understand the nature and consequences of his/her medical condition and proposed treatment
and
2. can communicate his/her decision to the provider
Instructions: Create no more than 3 questions per hour of CE. Review questions with attendees in whichever format you prefer. You MUST provide the correct answers to the attendees at this time. This is an ACPE requirement.
Test Questions

Based on the MEC criteria below, a 26 year old woman with normal blood pressure who has been taking a combination hormonal contraceptive and an SSRI and has developed migraine headaches without an aura and is seeking pharmacist HC should be:
1. Continued on her current method of cpntraception.
2. Be referred to her to a primary care provider for evaluation without providing HC.
3. Advised to change to a progestin only HC.

Based on the MEC criteria below, a 35 year old woman who has been taking a combination hormonal contraceptive and losartan for HTN is seeking pharmacist HC. Her BP is 136/70. The pharmacist should:
1. Continue her method.
2. Refer her to a primary care provider for evaluation. She is not eligible for pharmacist care.
3. Advise her to change to a progestin only HC .
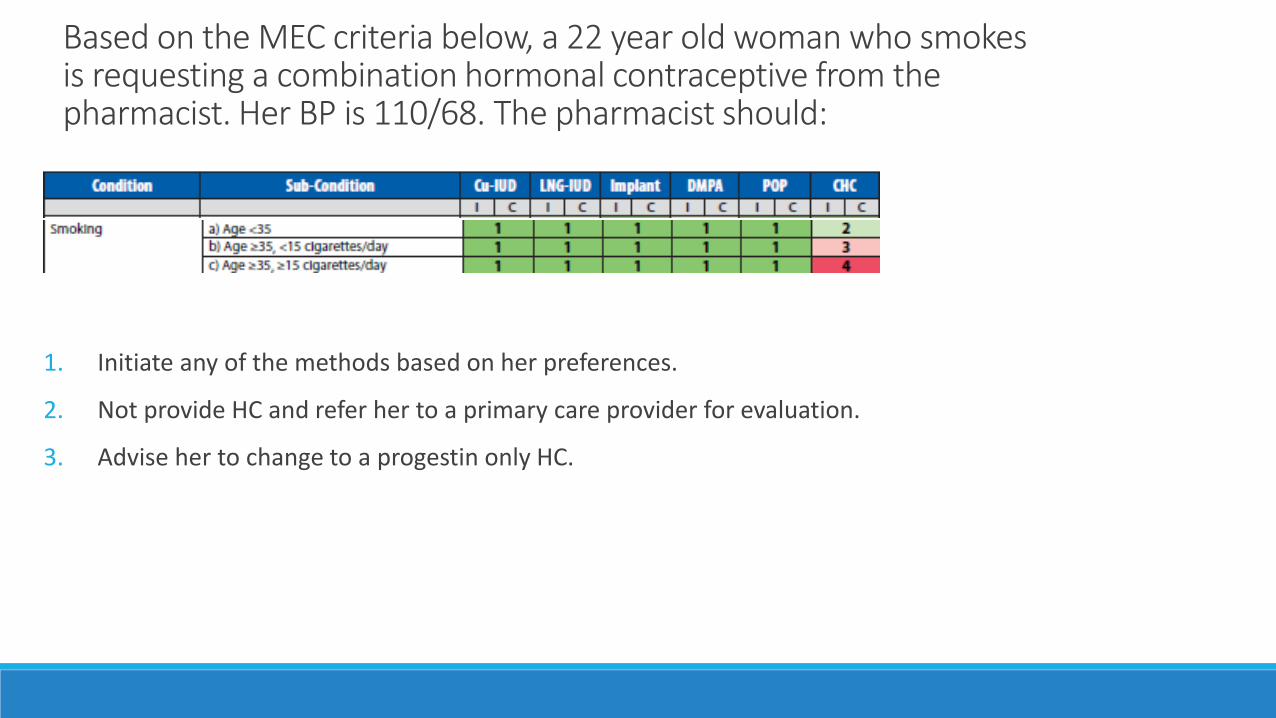
Based on the MEC criteria below, a 22 year old woman who smokes is requesting a combination hormonal contraceptive from the pharmacist. Her BP is 110/68. The pharmacist should:
1. Initiate any of the methods based on her preferences.
2. Not provide HC and refer her to a primary care provider for evaluation.
3. Advise her to change to a progestin only HC.
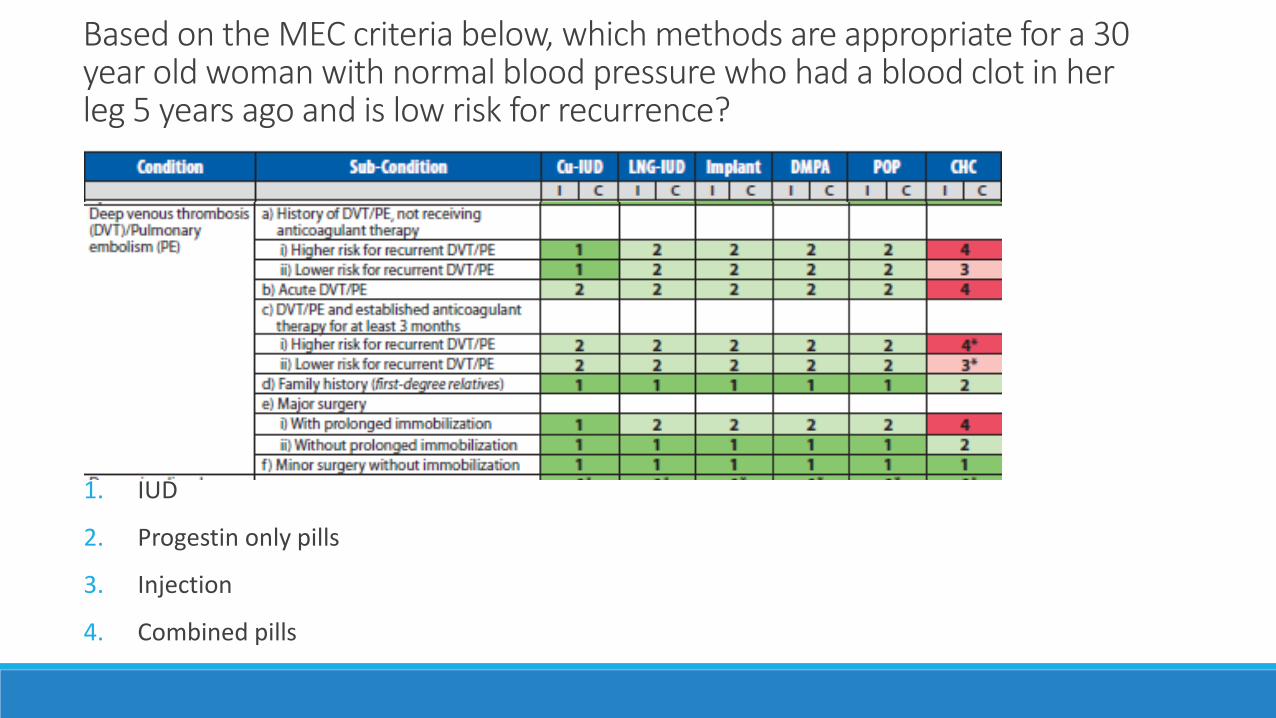
Based on the MEC criteria below, which methods are appropriate for a 30 year old woman with normal blood pressure who had a blood clot in her leg 5 years ago and is low risk for recurrence?
1. IUD
2. Progestin only pills
3. Injection
4. Combined pills

Association of Reproductive Health Professionals – Curricula Organizer for Reproductive Health Education (CORE). Available at: http://core.arhp.org.
CDC – U.S. Medical Eligibility Criteria (US MEC) for Contraceptive Use. Available at: http://www.cdc.gov/reproductivehealth/contraception/usmec.htm .
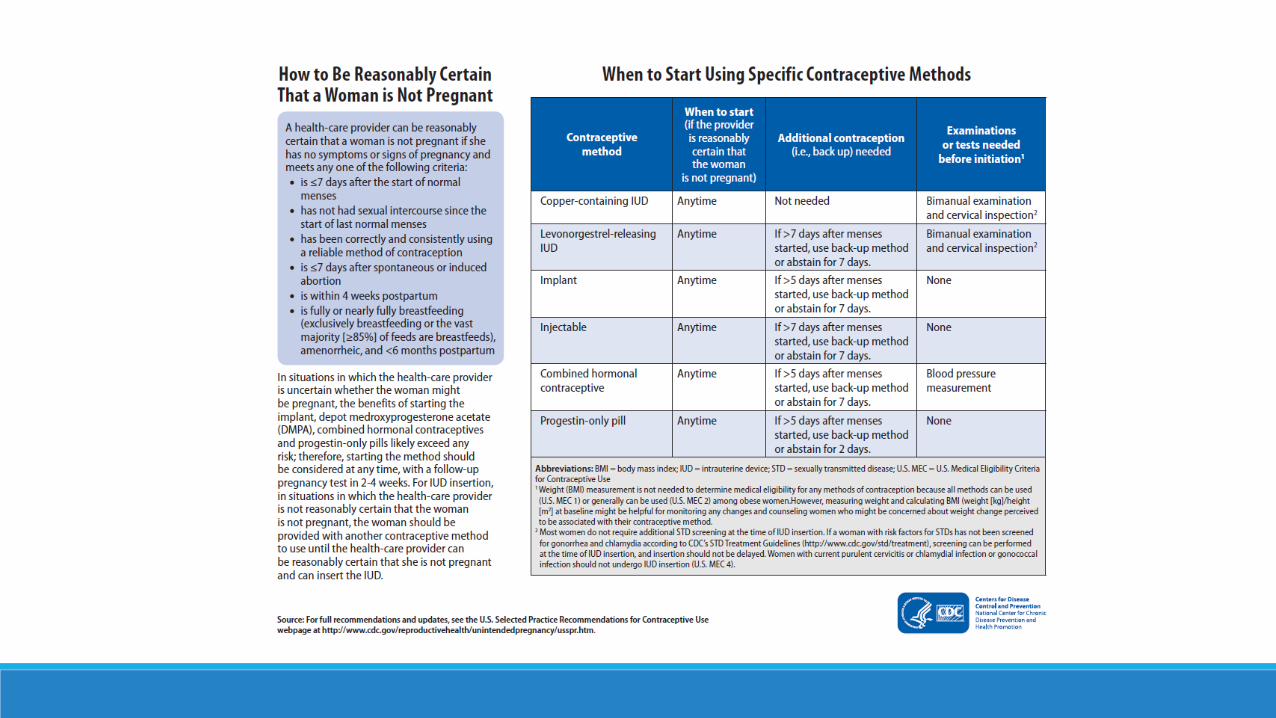
CDC – U.S. Selected Practice Recommendations (US SPR) for Contraceptive Use. Available at: http://www.cdc.gov/reproductivehealth/contraception/usspr.htm .
California State Board of Pharmacy: Protocol information Available at: http://www.pharmacy.ca.gov/licensees/hormonal_contraception.shtml
References

CDC Resources and Downloads

1. Write down the course code. Space has been provided in the daily program-at-a-glance sections of your program book.
2. To claim credit: Go to www.cshp.org/cpe before December 1, 2016.
Session Code: