clinical informatics approachcwmtafmorgannwg.wales/docs/board_papers/2019-2020... · clinical...
TRANSCRIPT

1
Clinical Informatics Approach
Author(s): David Rawlinson
Distributed to: Wales Major Trauma Network
Date: 20/09/2019 Version: 1.6
Review History:
Draft Number & version Author/ Editor Date
1 1.0 David Rawlinson 09/06/2019
1.1 David Rawlinson 11/06/2019
1.2 David Rawlinson 20/06/2019
1.3 David Rawlinson 26/06/2019
1.4 David Rawlinson 27/06/2019
1.5 David Rawlinson 30/06/2019
1.6 David Rawlinson 20/09/2019

2
Clinical Informatics approach
Informatics support is essential to improving patient outcomes through both direct support for patient
care and indirectly through improving efficiency of the administration of the patient pathway. Making
use of existing systems, and harnessing ongoing developments and the future plans of NHS Wales, the
informatics programme seeks to reduce the burden of data entry on clinicians and administrative staff,
and ensure timely, accurate information is available to patients, clinicians, and management
structures, as well as commissioners.
The work stream will seek to work with health boards, trusts, and NWIS to assess the current situation,
including mapping information flows relating to major trauma patients, and look at the short,
intermediate and long term expectations of the network and how informatics can support this. It will
also reach out to the wider UK and internationally to look at best practice and the lessons learned.
This approach has been presented to Trauma Governance Sub-committee.
In the context of Wales informatics, significant progress has been made recently with the roll out and
expansion of national systems allowing cross boundary access to patients records. This provides a
unique opportunity to build on existing technologies, and use routinely collected data to track trauma
patients in the network.
Some of the systems are listed below, and will be important in supporting the patient pathway:
MIS C3 Ambulance control system
WAST Anoto e-Pen system, Corpuls live monitor telemedicine capability
EMRTS Clinical database, RDT Telemedicine capability
Emergency department systems
Welsh Care Records Service (WCRS)
National Data Repository (NDR)
Welsh Clinical Portal (WCP)
Welsh Patient Referral Service (WPRS)
Welsh Results Reports Service (WRRS)
Welsh GP Record
Patient Knows Best (PKB)
National PROMS/ PREMS programme
Unscheduled Care Dashboard
NCCU Benchmarking toolkit

3
In addition Wales also has access to unparalleled health informatics research and evaluation support
from Swansea University including the Swansea Anonymised Information Linage (SAIL).
A brief overview of how informatics can support the various stages of the patient journey are outlined
below, and it is intended that all will be integrated to provide a seamless electronic record.
In addition to the membership of the trauma network working groups, the following organisations and individuals have been consulted during the development of this document
NAME ROLE ORGANISATION
MATTHEW JOHN Associate Director of Informatics
SBU
RACHAEL POWELL Assistant Director of Research, Audit and Service Improvement
WAST
KEVIN WEBB Head of Clinical Audit & Effectiveness
WAST
CRAIG GARNER Information Governance Manager
WAST
MARIA STOLZENBERG Assistant Head of Risk and Assurance, Patient Feedback Team
SBU
MARTIN DAVIS IM&T Development CAV
KATE BLACKMORE Area Manager for EMS CCC (Interim)
WAST
DANIEL PHILLIPS Director of Informatics Planning Management
Velindre
RHIDIAN HURLE MD/ CCIO NWIS LEE MORGAN Head of Information
Services SBU

4
Contents Clinical Informatics approach ................................................................................................................. 2
An overarching trauma informatics system ........................................................................................ 5
Pre-hospital – WAST/EMRTS ............................................................................................................... 7
Emergency Departments .................................................................................................................... 7
In-hospital ........................................................................................................................................... 8
E-discharge .......................................................................................................................................... 8
Implementation .................................................................................................................................. 9
Other areas for Network Support ..................................................................................................... 11
Central Incident Reporting ............................................................................................................ 11
Call recording ................................................................................................................................ 12
Welsh Patient Referral Service (WPRS)............................................................................................. 12
Network development and dissemination of information ............................................................... 12
Notes on specific areas ..................................................................................................................... 13
WCP ................................................................................................................................................... 13
Research ............................................................................................................................................ 13
Patient held records .......................................................................................................................... 13
Trauma tool App ............................................................................................................................... 14
Information App ................................................................................................................................ 14
Pre-hospital providers ........................................................................................................................... 16
WAST requirements .......................................................................................................................... 16
EMRTS requirements ........................................................................................................................ 17
Operational ................................................................................................................................... 17
EMRTS Informatics/ clinical audit ................................................................................................. 17
NWIS / CAV/ SBU .............................................................................................................................. 17
Estimated resource requirements & ROM costs .................................................................................. 18
Appendix 1 ............................................................................................................................................ 19
Appendix 2 – Trauma informatics system proof of concept ................................................................. 22
Appendix 3 – PKB proposal ................................................................................................................... 32

5
An overarching trauma informatics system
As part of the MTC preparations the Major Trauma Project Board in Cardiff & Vale UHB are developing
a bespoke database system in house, and have offered the system to the wider network as a way of
improving data collection and tracking patients through the pathway (Appendix 1). A proof of concept
is also included in Appendix 2. This has been well received by the network board, and it has been
identified that for this to be achieved a number of areas will need to be considered:
1. The hosting of the system (separate instances vs CAV vs national infrastructure vs cloud etc..)
2. Development required including
a. Integrations with varied systems across LHB’s
b. Integrations with national systems such as NDR, WCRS, RADIS, WLIMS etc..
3. Information governance arrangements
4. User access control and administration (who adds and removes users from the system across
the network)
5. System training arrangements
6. Access audit and surveillance (NIASS)
7. Service management including routine business, change requests and future developments
(whole network approach)
A work programme will be established to implement a central trauma specific electronic patient
administration system. The system will aim to identify patients at the earliest opportunity, ideally pre-
hospital, or in the emergency department, and start to track the patient’s journey through the
pathway. It will integrate with local and national systems in use across NHS Wales, and provide the
relevant near real time information to all involved in the management of the pathway. This includes
clinicians, managers, clinical audit and administrative staff. It will also link with systems used to
communicate with patients to facilitate PROMS/ PREMS. A cohort of the patients who are TARN
eligible will then be fed into the TARN database. This approach will allow Wales to hold its own
trauma registry for operational management, with potential for service evaluation, additional audits
and research. With a scope wider than the TARN criteria, it will provide unique opportunities to
improve service delivery and facilitate injury prevention activities. The system will also support clinical
governance process through tracking of case reviews.

6
Key features of the system will include:
Provider model allowing each HB to integrate with systems where the differ from the national
landscape, allowing for the varying stages of transition and developments.
Hosting on the national infrastructure
Federated development model to ensure all partners are involved in the development and
reduce the reliance on any one health board or organisation.
It should be highlighted that for pre-hospital providers, and TU/ MTC, there are not new data flows
relating to this project, but the system aims to improve accessibility of the data to improve patient
care. e.g. a patients ambulance record is currently handed over to hospital staff and ultimately forms
part of the hospital record. It may also be scanned into a document management system and enter
onto national systems, as well as be manually audited by TARN audit staff.
A high level overview of the anticipated landscape of the systems is included in Figure 1
Figure 1 Overview

7
The following stages of the patient pathway are detailed below, with brief discussion a about how
they will interact with the information systems:
Pre-hospital – WAST/EMRTS
As the majority of major trauma patients first access health care via the 999 system, it is important
any informatics approach starts with the pre-hospital providers WAST and EMRTS. This can provide
and early record of a candidate major trauma patient entering the system, and should ideally aim to
identify patients where possible at the time of call or first clinical contact. Retrospective matching of
patients should take place in cases where the patient is unknown. Starting at this point facilitates a
multitude of potential actions such as use of trauma triage tools, senior clinical decision making
support, logistical support, clinical apps, accurate pre-alerting of primary and secondary receiving
centres, efficient radiology (such as direct to CT), early blood product transfusion and remote advise
to clinicians. There is also opportunity to improve the enhanced pre-hospital TARN dataset here, and
also reduce the burden on TARN coordinators.
It is important to remember that the majority of this data is already routinely shared with secondary
care through the transfer of paper records and printouts or scans of records and so the data flow is
not new. The information forms part of the patients health records. In addition operational metrics
are also available through data linkages to the individual health boards for performance management
purposes.
Emergency Departments
Identification of candidate patients in ED is important to continue tracking the patient’s journey, and
may be achieved through the use of routinely collected data. An analysis of systems in use, and
mapping of datasets will be required within the network, and where gaps exist, the programme will
seek to supplement these ensuring high compliance with a core dataset. In some cases this may be
achievable with routinely collected data from existing systems, in others it may require manual data
collection, or development of existing systems. Through use of already available systems such as WCP,
there are already opportunities to improve the care delivered to patients through access to patient’s

8
medical history (primary and secondary care). For tertiary centres, access to live clinical information
from primary hospitals such as radiology and blood results can also be facilitated to aid planning and
assist with advice given by the centres. Radiology and clinical image transfer systems already exist but
improvements may be considered in the logistics and compatibility of these systems to ensure timely
image transfer. Future developments may also include telemedicine support for TU/ LEH.
In-hospital
As the patient’s journey continues, additional data collected such as radiology, operation and
procedure notes, as well as organ support information is collected and is vital to providing a complete
picture of the patient’s progress. There also exists opportunities to tie into other national work-
streams such as e-prescribing, e-flow, e-ICU (CCIS) and any other emerging technologies.
E-discharge
As the patient transitions between levels of care and subsequently home it is important that timely
and accurate transfer of information takes place. This includes communication with rehabilitation
services, primary care, and most importantly the patient. It is envisaged that in line with emerging
practices within wales, and the wider UK that patient held electronic records are used. Systems such
as PKB which are being used in Wales and across the UK provide such a platform, and when integrated
with national systems provide seamless transfer of information that the patient is in control of.
Evidence points to this improving compliance with rehabilitation, and also improved patient
satisfaction. It also provides an opportunity to collect data pertaining to PREMS and PROMS from
patients which can improve compliance with TARN PROMS, but also facilitate continuous service
improvement, reduce the administration burden for providers, and also provide data to support
economic evaluation of the service provided.

9
Implementation
It is recognised the work plan is ambitious given the short time frames to “go-live”, and ongoing
existing work streams in an already stretched informatics landscape. In addition, although important,
major trauma makes up a very small proportion of the overall workload in NHS Wales, and will be
competing with other established projects which impact far greater number of patients (e.g.
introduction of new emergency department systems, implementation of electronic records in WAST).
Thus, a phased approach will need to be taken, and phased over 5 years. An illustration of the essential
and desirable deliverables are included below, subject to change once formally handed over to the
ODN.

10
Year Essential Desirable
19/20 (in
place for
day 1)
Data sharing agreements in place
Pre-hospital patient reports from WAST & EMRTS to be available to TARN coordinators & Network office no more than 4 weeks following incident
WAST/EMRTS to be flagging potential major trauma cases on control systems
Up to date pre-hospital operational data available for interrogation and business intelligence dashboards
Network information “app” live
Trauma tool “app” live
All TU’s to upload trauma pro-forma to document management systems that interface with national repository
CAV to be using the network trauma information system pro-actively
Network incident reporting system short form live and process in place for handling cross boundary/ organisational incidents
Call recording available for non-emergency case discussions/ referrals
All TARN coordinators to have access to national instance of Welsh Clinical Portal
Network data analyst in post (training/ development with stakeholders)
Patient held records (for rehabilitation prescription) functioning
Capture of additional trauma cases in systems that are not TARN eligible, but of interest for injury prevention and service planning e.g. death at scene in HB’s that have capacity (i.e. are already up to date with retrospective data collection)
20/21 Integration with national systems complete (to include operation notes, emergency department systems, all radiology, pathology results)
Transition to electronic clinical data capture in emergency department (replacement of trauma paper pro-forma) CAV
Patient held records (for rehabilitation prescription) functioning for MTC patients
Transition of other TU’s to electronic data capture
Export of year 1 & year -1 data to SAIL
21/22 Patient held records (for rehabilitation prescription) functioning for MTC patients + 2 TU’s

11
22/23 Patient held records (for rehabilitation prescription) functioning for MTC patients + 4 TU’s
Patient held records (for rehabilitation prescription) functioning for 6 TU’s
23/24 TARN integration
1. TARN to have direct access to the network trauma information system data including all relevant linked data to complete a TARN submission.
2. Network to have direct link to TARN data to augment data already available within NHS held datasets e.g. addition of Ps, ISS etc… in operational dashboards.
3. PROMS data to be linked back into welsh systems, and in turn into National data repository
4. Export of dataset to SAIL with 3 complete years of network operation, and to include PROMS, and TARN metrics.
Patient held records (for rehabilitation prescription) functioning for all 8 TU’s
Other areas for Network Support
A number of areas have also been identified that will require support:
Central Incident Reporting
The development of a central incident reporting system (e.g. DATIX) that allows cross border
investigation of incidents and facilitates statuary reporting and escalation where required to WG.
Automatic population from the trauma system when cases are flagged e.g. M&M, critical
incident etc…
An easy to use short form for use by the network to log incidents

12
Discussions have taken place with the incident reporting manager in SBU who is also overseeing the
procurement of a national system, and these elements can be accommodated.
Call recording
Whilst early parts of the patient pathway e.g. trauma desk decisions and conference calls will be
routinely recorded, it has been identified that it would be advantageous to record calls between units
relating to repatriations to facilitate the governance process and improve accountability. On a basic
level this is the provision of a recorded line, and it is likely that this will require an office hours
administrative function to setup calls and log them against a patient in the trauma system to ensure
traceability. In the rare event of out of hours discussions then this could be conducted through the
trauma desk, recognising its primary responsibility is in the coordination of the emergency stages the
trauma pathway.
Welsh Patient Referral Service (WPRS)
As patients transition between stages of the pathway and institutions, if is desirable that any
communication relating to this is recorded on the trauma informatics system, but conducted through
existing e-referral process available via the national systems. This includes repatriations and
rehabilitation.
Network development and dissemination of information
An auditable document management system should be available for the development and version
control of network guidance e.g. Sharepoint
Tools for accessibility of network guidance, contacts, and communications should be available and
accessible through networked computers within the NHS and ideally on work and personal mobile
devices used by clinicians.

13
Notes on specific areas
WCP
The Welsh Clinical Portal provides a unique opportunity to provide a single point of access to trauma
patient’s records from pre-hospital through to rehabilitation. Any systems holding patient data should
provide data into the NDR and WCRS which will be consequently visible to users of WCP who may not
have access to the bespoke trauma systems. This would apply to the trauma informatics system where
it is implemented, but will also mitigate any delays e.g. in a TU, as any trauma related documentation
should be uploaded by them through existing systems. It is essential that all staff have access to this,
and specifically in respect of TARN coordinators, access to the national instance, which provides
enhanced visibility of information across health board boundaries.
Research
Swansea University has a long history of supporting trauma research on an international level, and
with existing data linkages through SAIL this provides an unparalleled opportunity to research trauma
in Wales. There is opportunity to benchmark against international services. The trauma informatics
system should be capable of providing an export to SAIL through the split file process. A key to
successfully matching patients in SAIL is ensuring a high compliance with NHS numbers being
recorded, and so this could be used as a measure of data quality in the day to day management of the
system.
Patient held records
In order to facilitate ongoing care of patients following their acute admission, there is growing
evidence that patient held records improve compliance with ongoing treatment plans. When in
electronic format they also enhance communication between clinicians and patients, and potentially
improve patient satisfaction. They also facilitate further contact to enhance collection of PROMS and

14
PREMS. An example of such a system is Patients Know Best (PKB). This is a patient held record system
that is now established in NHS Wales, and is integrated with the infrastructure, although not currently
used in Trauma care. It is however used to good effect in the south west of England and has proven
itself to be a valuable tool to improve quality discharge in trauma. The system is already in use in CAV
and SBUHB, which may represent a cost saving with regards to licencing. Additional licences would
need to be purchased to cover TU’s that enter patients onto the system
Some integration work would also be required to ensure the system functions efficiently with the
trauma informatics system.
Alternatively there are other providers, and scope for in house, or a hybrid approach. Further work is
required in the immediate term to determine the best approach, but for the purposes of financial
planning a worst case scenario is illustrated in the appendix and ROM costs.
Trauma tool App
There is a desire to produce an app that will allow clinicians to apply the trauma triage tool in both
the training environment and in clinical practice. This follows best practice exhibited elsewhere in the
UK (SCAS/ Wessex network, Scotland under development, North West). This supports ongoing work
to mobilise the pre-hospital workforce, and use technology to positively support the patient pathway.
In addition data relating to usage of the app can be use to support the operational management of
the network. This app can be produced in-house or commissioned from one of the existing providers
in the UK. An example of a proposal from a current provider, Volatile State Ltd is attached in Appendix
4.
Information App

15
Distinct from the trauma tool app, which is a clinical decision making tool, there is a requirement to
make network documentation easily available to any clinician involved in accessing the network. This
must be accessible on multiple platforms, and content will be managed by the network office. A
potential solution already widely used by NHS staff in Wales is “Induction”. This is already established
in a number of English NHS major trauma networks, and provides ready access to guidance and
contact details. Alternatively an in-house app may be developed, or a mobile view of a website may
provide adequate functionality, and be managed by the communications manager.

16
Pre-hospital providers
WAST requirements
Trauma Desk/ Control staff
Flagging of cases on the CAD that are potential major trauma
Recording whether the trauma triage tool was used or not
Operational data access
Provision of a data SQL view relating to trauma cases to include fields such as incident number,
date, time, location, postcode, LHB, staff names and skill level, callsigns, time of resource
arrival/ left scene/ arrival at hospital, destination hospital and LHB, clinic attended, nature
description, call category, problem text, flag status, trauma triage tool used etc…
Clinical Audit & Health Records
Provision of un-redacted patient report form image to the network office, either via secure
email or direct upload to the trauma patient administration system (timeframes TBC)
Structured data view mapped to core TARN data fields and Welsh Trauma registry (TBC)
following clinical coding, on a monthly basis
Corpuls data (e.g. physiological trends) (desirable)
Identification of patients that are deceased outside of hospital where possible, to facilitate
post-mortem requests by the network office.
Overall, the aim would be to automatically “push” records into the trauma system at the earliest
opportunity, but it is recognised this will likely be tied into developments such as further phases of
CAD, and the ePCR project/ ePEN replacement and so a degree of manual data transfer is to be
expected initially. This may have additional staff resource requirements in the case of health records/
clinical audit departments workload.

17
EMRTS requirements
Operational
Air Support desk staff – working closely with the trauma desk (model TBC), and ensuring accurate data
entry into CAD and trauma system.
EMRTS Informatics/ clinical audit
Provision of an SQL view to link pre hospital records to the trauma system
Provision of unredacted exports from ePCR and digital copies of any associated paper records either
to the network office, either via secure email or direct upload to the trauma patient administration
system
NWIS / CAV/ SBU
Working with CAV and SBU to facilitate the following works, or providing an alternative solution
1. Hosting of the trauma informatics system SQL database and application
2. Integration with
a. NIASS
b. MPI
c. WCRS
d. NDR
e. RADIS
f. WLIMS
g. WEDS
h. Welsh Patient Referral Service (WPRS)
3. Service desk support
4. SAIL upload support through existing split file process
18
Estimated resource requirements & ROM costs
An estimate of resource requirement and ROM costs is provided here to aid financial planning, and is
subject to change as the work progresses with formal project management. It should be noted that
work is not in established work plans, and crosses multiple stakeholders with complex integration
work required in some areas. Each stakeholder may also incur additional resource requirements to
complete the work, not detailed here.
Other requirements
Other incidental expenses such as provision of computer and telecoms equipment for network
office staff are included in other areas of the business case.
ICT support costs and the organisation that incurs them will depend on the final architecture
of the network trauma information system
Network data analyst and TARN coordinators that are instrumental to high quality data
collection and analysis are covered elsewhere.
Education and training ICT requirements are covered elsewhere.

19
Appendix 1
South, Mid & West Wales Major Trauma Network – Informatics & Database
Leigh Davies
Clinical Governance Lead – Major Trauma Network
Situation
The development and implementation of the major trauma network and major trauma centre, together
with a requirement for the collection and submission of TARN audit data from across the network area
has resulted in the need to develop a regional solution for the acquisition and management of data from
across the Major Trauma Network.
This will enable the network, MTC and trauma units to understand the work load for which they are
responsible, their outcomes and the patients across the network waiting for repatriation to their base
trauma unit. In addition, the submission of TARN data across the network will be improved and allow
the network to understand the workload across the network and changes over time which will allow the
network to amend and adjust the system to maximise outcomes and improve efficiency to ensure that
patients get the best system possible with minimum waste.
Background
The development of a South, Mid & West Wales trauma network has been in development for a number
of years and is now being implemented across the region with the project being led from the NHS wales
collaborative. Within this project are a number of Welsh Health Boards each with a designated trauma
unit and one with the Major Trauma Centre (Cardiff & Vale) the overarching body responsible for the
management of the South, Mid & West Wales major trauma service will be the Major Trauma network.
Further interactions with the Welsh ambulance service NHS Trust and the Emergency Medical

20
Retrieval and Transfer Service (EMRTS) will also play a significant part within the major trauma
service.
As a complex organisation with interactions between each of these bodies, there will be a requirement
for an over-arching data system which allows each organisation to understand it’s patient volumes, the
location of each of the patients it has responsibility for, the outcomes for those patients and support in
submitting each organisations data to the TARN audit.
Traditionally, each organisation in the Welsh NHS has maintained control of their own data
management as the need to interact between organisations has been limited. More recently, data
management has become more centralised as the utility of sharing data across the region has been
recognised as of increasing utility.
The development of the trauma network together with planning for trauma units in each Health Board
and the development of the Major Trauma Centre in Cardiff presents an opportunity for the development
of a single data management system across the network which will fulfil the needs of each of the
organisations involved to maximise data acquisition and allow use of that data to maximum effect.
Assessment
Currently, as part of the development of the Major Trauma Centre in Cardiff, it was recognised that
current data management for major trauma patients was lacking which resulted in a lack of clarity on
the volume of patients being treated for major trauma and their outcomes in a timely manner. TARN
data submissions were ultimately completed but not within the required timeframes and there was lack
of confidence across the network on the total volumes of patients and the severity of injuries and a poor
understanding of their total medical needs. As such, this makes the planning for the MTC more
challenging. As a result of this, an early decision by the Major Trauma Project Board in Cardiff & Vale
UHB was made to initiate a Major Trauma Database system which will acquire data on major trauma
patients in a prospective and timely manner, allowing early TARN data submission, an understanding
of the patient load/volumes and their needs, and to support outcome measures including PROMs.

21
Currently, C&VHB is developing this database system using their in-house IT department and the
system is being designed and built by the IT service as a bespoke package for the MTC to achieve the
needs stated above. This system will be based on a SQL server system which allows access from across
the health board on all NHS computers but protected from inappropriate access using appropriate
security to maintain data security as per Caldicott and GDPR principles.
It would seem that there are requirements for a similar system to manage patient data and outcomes
across the network.
Recommendation
There appears to be an opportunity to maximise data management and data sharing to allow best flow
of patient information and outcomes across the network if the network was to adopt a system of data
management that integrates across the network, the MTC and the trauma units simultaneously.
It would therefore be appropriate that the Major Trauma Network adopts the same system for MT data
management that is being developed by the MTC and this system is adapted for use across the network,
such that data is shared appropriately and at the same time maintained in a secure manner consistent
with current data protection principles.
The development of the current MTC system will allow the Trauma units to understand the patients in
the pipeline which are awaiting repatriation to local hospitals and facilitate their significant role in the
Major Trauma Network in “Pulling” their patients from the MTC in order to maximise patient flow and
allow patients to recover and rehabilitate as locally as possible to home once their treatment in the MTC
is completed.

22
Appendix 2 – Trauma informatics system proof of concept
The following is a demonstration of proof of concept of the trauma informatics system and is
subject to change. With thanks to Martin Davis, CAV IM&T development.
Patient Lists
This is the first screen that people will see once they’ve logged in; it shows a list of the patients
currently receiving care within the hospital/health board to which the users account has been
associated. Information presented includes basic demographics, the location of the patient within
the hospital, their current status (i.e. Inbound, Assessment, Critical, Stable, Awaiting Transfer,
Discharge Imminent, etc.), the date and mechanism of injury. A series of icons in the first column
can convey information stored about this patient in the underlying PAS (i.e. stroke, dementia, end of
life, etc.) if the PAS supports such things. The final column allows individual users to “star” a patient,
a convenient way to easily track patients that are under that individuals care.
In a busy hospital this could become a long list, so there are menu options on the left-hand side that
allow you to view categorised sub-sections of the list such as “Transfers In”, “Transfers Out” and
“Starred Patients”. There are other menu options for patients that are no longer receiving care, but
still require their record to be available, including “Awaiting TARN” (for patients that have been
discharged, but not yet uploaded to TARN) and “M&M Cases” for patients whose cases need to be
reviewed in an M&M scenario. “Search” and “Help” complete the options on the main navigation.

23
This is the “Transfers In” view – it shows the same information as the main view, but in addition
includes a clock in the first column to show how much time is left in the transfer window. This is
a “target” that is created by the system in response to a transfer request, similar targets are
initiated in other parts of the system, i.e. when a patient is discharged, a target is created to
ensure their TARN submission is completed on time. Users can also create bespoke targets to
remind them, for example, to check a patients observations every 2 hours.
Patient Record
24
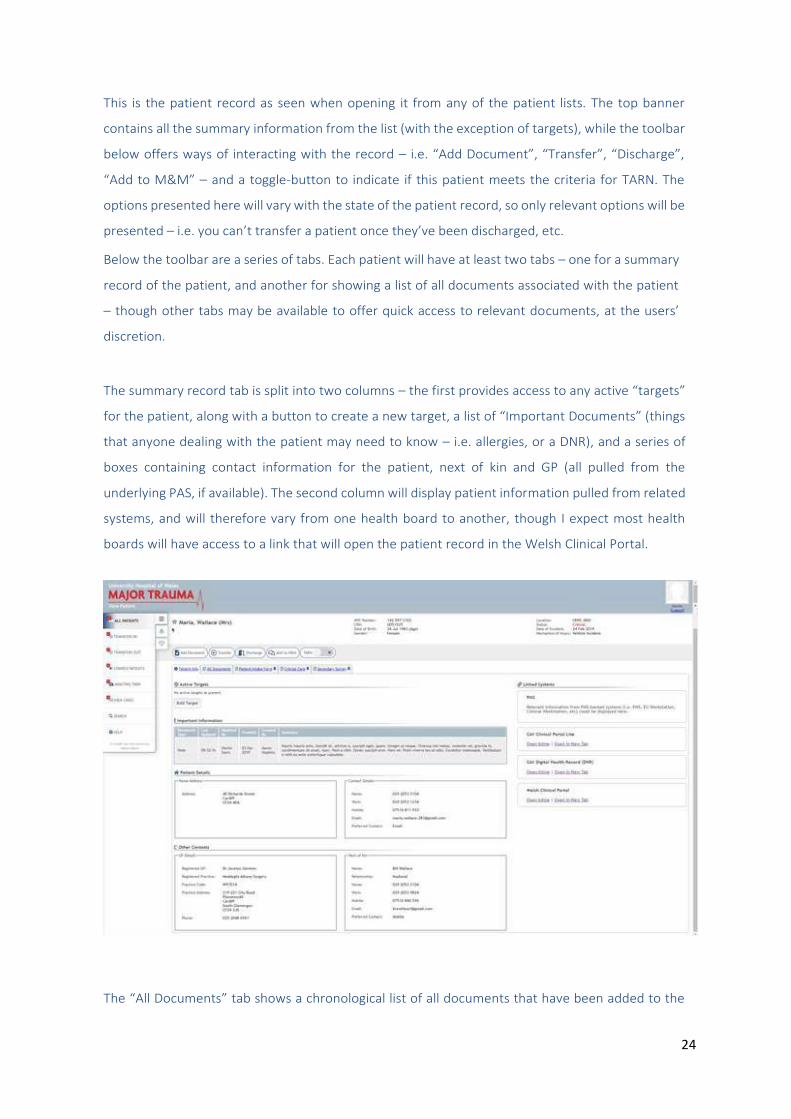
This is the patient record as seen when opening it from any of the patient lists. The top banner
contains all the summary information from the list (with the exception of targets), while the toolbar
below offers ways of interacting with the record – i.e. “Add Document”, “Transfer”, “Discharge”,
“Add to M&M” – and a toggle-button to indicate if this patient meets the criteria for TARN. The
options presented here will vary with the state of the patient record, so only relevant options will be
presented – i.e. you can’t transfer a patient once they’ve been discharged, etc.
Below the toolbar are a series of tabs. Each patient will have at least two tabs – one for a summary
record of the patient, and another for showing a list of all documents associated with the patient
– though other tabs may be available to offer quick access to relevant documents, at the users’
discretion.
The summary record tab is split into two columns – the first provides access to any active “targets”
for the patient, along with a button to create a new target, a list of “Important Documents” (things
that anyone dealing with the patient may need to know – i.e. allergies, or a DNR), and a series of
boxes containing contact information for the patient, next of kin and GP (all pulled from the
underlying PAS, if available). The second column will display patient information pulled from related
systems, and will therefore vary from one health board to another, though I expect most health
boards will have access to a link that will open the patient record in the Welsh Clinical Portal.
The “All Documents” tab shows a chronological list of all documents that have been added to the

25
patient record, showing the type of document, when it was created and by whom, when it was last
updated and by whom, and a brief textual summary of the document. Clicking on an entry will open
the document in its entirety.
Document View
This shows a document in its default read-only state. There are a series of small icons on the left of
the document that allow you to interact with it…

26
…clicking on one opens a small side panel to show additional information. The first icon provides
a brief summary of the document activity – i.e. author, editors, number of versions, etc.:
The second allows you to control whether the document appears as a tab or important document
on the patient record:

27
The third shows you a list of all edits that have been made to the document, and allows you to
quickly view an older version so you can see what the document looked like at a given point in time.
The final icon allows you to open the document for editing.
Adding a Document

28
From the main patient record, the “Add Document” toolbar button allows you to add a new
document to the patient record. The expectation is that there will be many different document
types available in the system, so they will be presented in a hierarchical/grouped fashion to make it
easier to find what you’re looking for. Document types that you use a lot can be added to a
“favourites” list, which is presented first, to save you having to go hunt for them.
Selecting a document type will show you a small preview of that document along with a description
of what the document is and how it should be used. Clilcking the “Create” button will create a new
document of the selected type, and take you to it in edit mode.

29
The term “document” might make you think of flat word-type documents, but they don’t need to be
– a document can be anything that contains patient-related information, and can be as interactive
as needed. Below is an example of a “Scribe Sheet” document, which is used to capture activity in a
busy setting (i.e. in resus, which doctors attended, which medications were given, etc.). Activity is
written into the small text box on the left of the screen (which grows, as necessary, as you type in it)
and when the [Enter] key is pressed, the text is transferred to the right hand pane where it is
automatically time stamped and attributed to the author.

30
Add Patient
Adding a patient to the system (from a toolbar button on any patient list) also creates a document,
and shows how integration with other systems can be achieved within the document paradigm.
Initially presenting a simple form to capture the details of the patient and the circumstances
surrounding their injury, it can expand to show information from related systems.
If you’re adding the patient after the fact (i.e. the patient has already arrived in the emergency unit)

31
you can quickly view a list of patients currently recorded in the underlying EU system, and pull
across their demographics and other related information:
If you’re adding a patient in response to a call from the ambulance team, you can free-text in the
patient details that are known and use that to search the underlying PAS to find a matching record
(giving access to GP and next of kin information, etc.):

32
Pricing proposal for Wales Major Trauma Network
June 2019
Patients Know Best (PKB) standard price for departmental deployments would be £30,000 per
annum. For the Major Trauma Centres (MTC), PKB have agreed a price of £10,000 per annum. This
includes major trauma patients who are treated at a MTC who then may be
repatriated/transferred. Any receiving site within each network could also be set up with a
team for access to these transferred/repatriated patients.
Any major trauma unit also wishing to register their own patients on PKB would be charged an
additional £2,000 per annum.
The breakdown of this would be as follows:
All prices are exclusive of VAT.
St John’s Innovation Centre T: +44 1223 790708 Registered in England: No. 6517382
Cambridge CB4 0WS, UK E: [email protected] UK VAT registration: 944 9739 67
Site Price per unit total
MTC £10,000 £10,000
X8 Major Trauma Units £2,000 £16,000
Total - £26,000
Appendix 3 – PKB proposal