clinical image removed from presentation 25 final.pdf · reticularis (cutis marmorata) - primary...
TRANSCRIPT

BSD Workshop: Case 25 RAC5556
Clinical Image removed from Presentation

• F49 • Migraine • Single
miscarriage • 1 year history
gradually progressive skin discolouration
Clinical Image removed from Presentation
BSD Workshop: Case 25 RAC5556
Initial investigations (2008)
IgG anticardiolipin antibodies (IgG aCL): 190.8 GPL kU/L → 75mg aspirin od commenced
2010 • Odd sensory disorder right arm • Nerve conduction studies:
– Non-specific sensori-motor neuropathy • Ongoing sensory disorder in hands and
leg cramps
Investigations: June 2011
Atypical p-ANCA detected and Myeloperoxidase (MPO) < 1 kU/L → identical results in September 2011 IgG aCL: 2.7 GPL kU/L

In July 2011, she developed crops of necrotic papules within areas of livedo racemosa on her ankles
Clinical Image removed from Presentation








Differen+al Diagnosis for BSD Workshop
• Polyarteri+s nodosa • Livedoid vasculopathy • Microscopic polyarteri+s • Chrug Strauss syndrome • Cholesterol emoblism
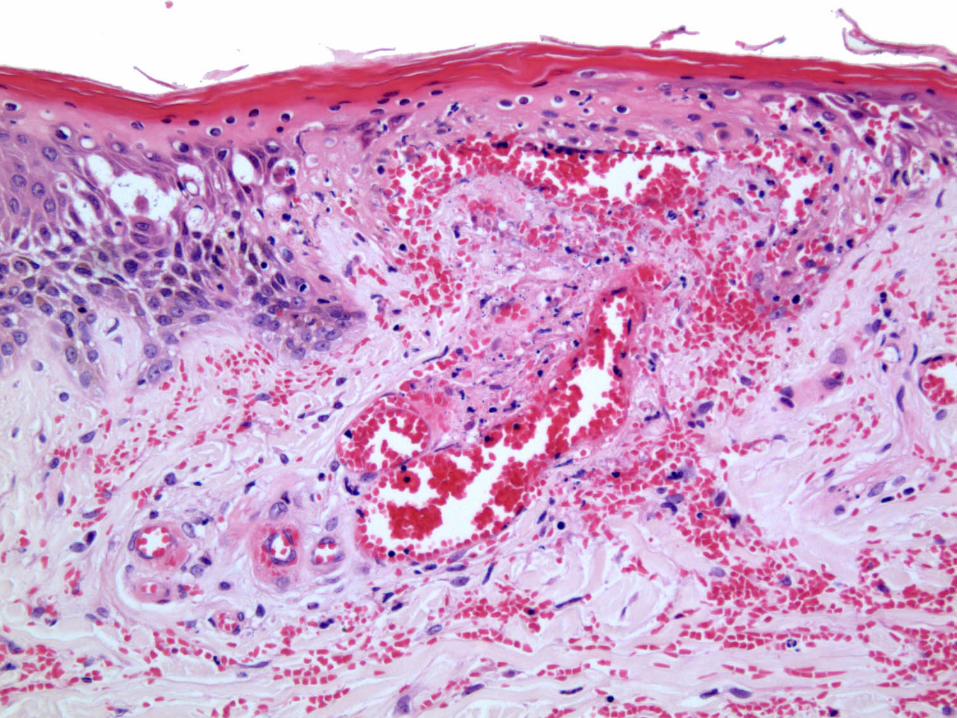
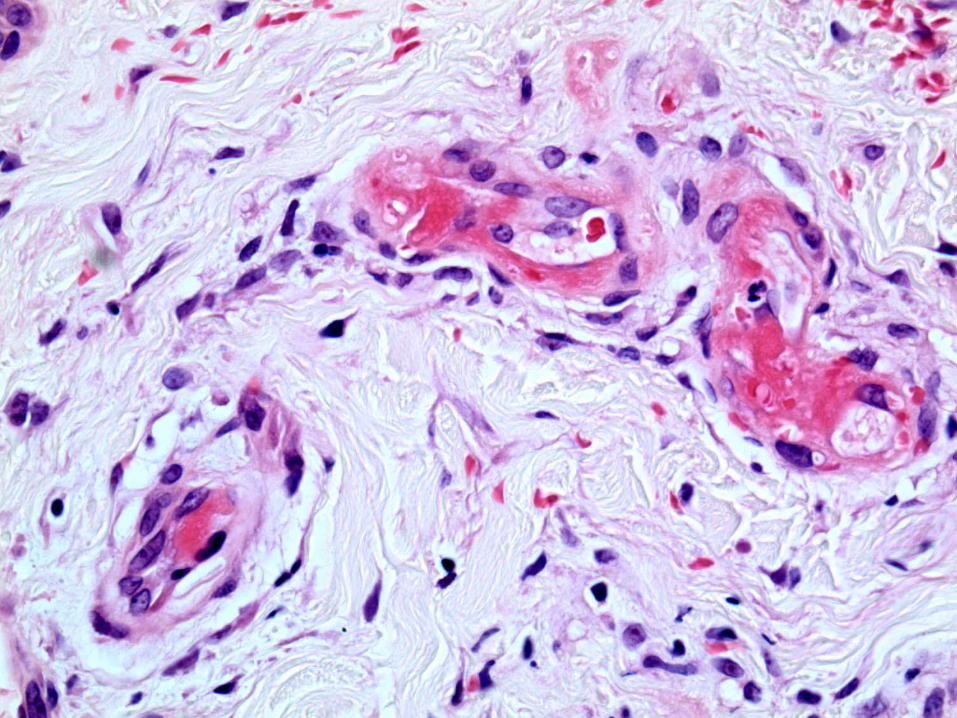
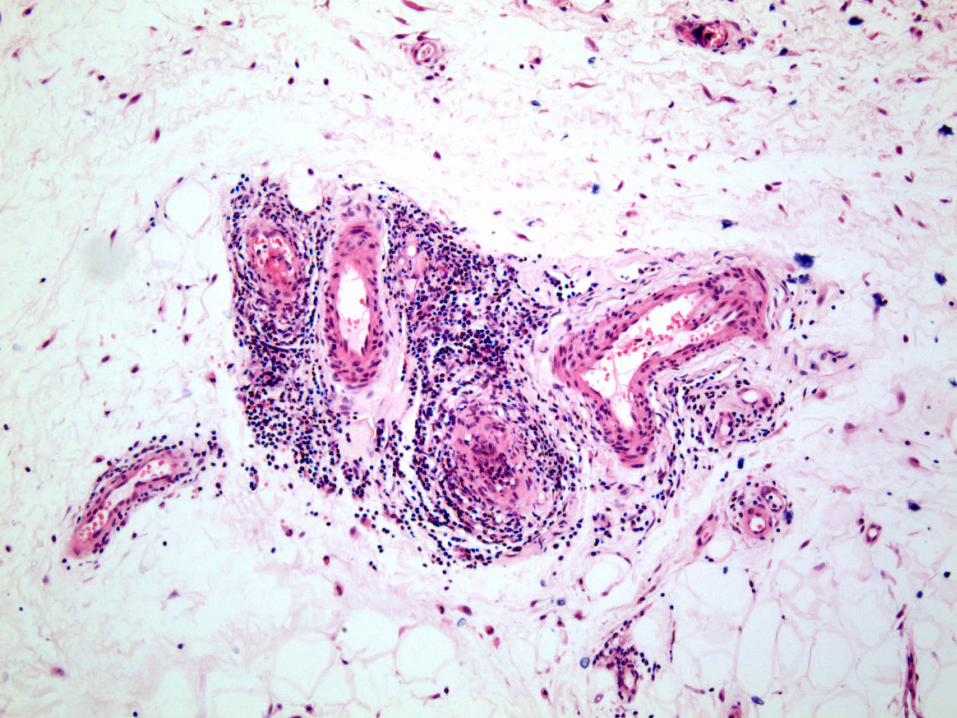
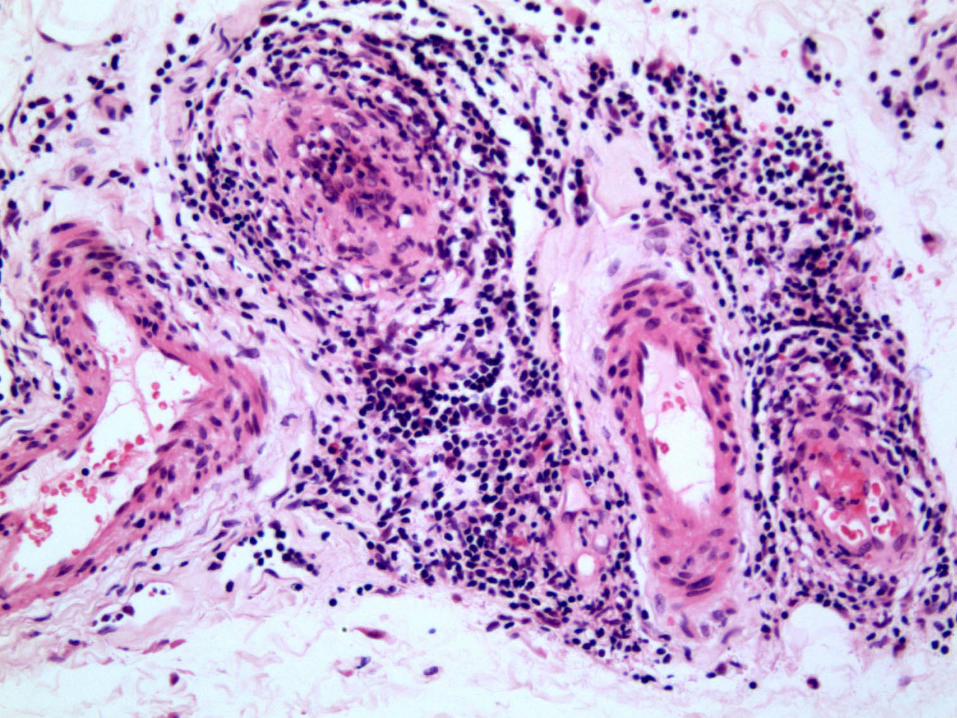
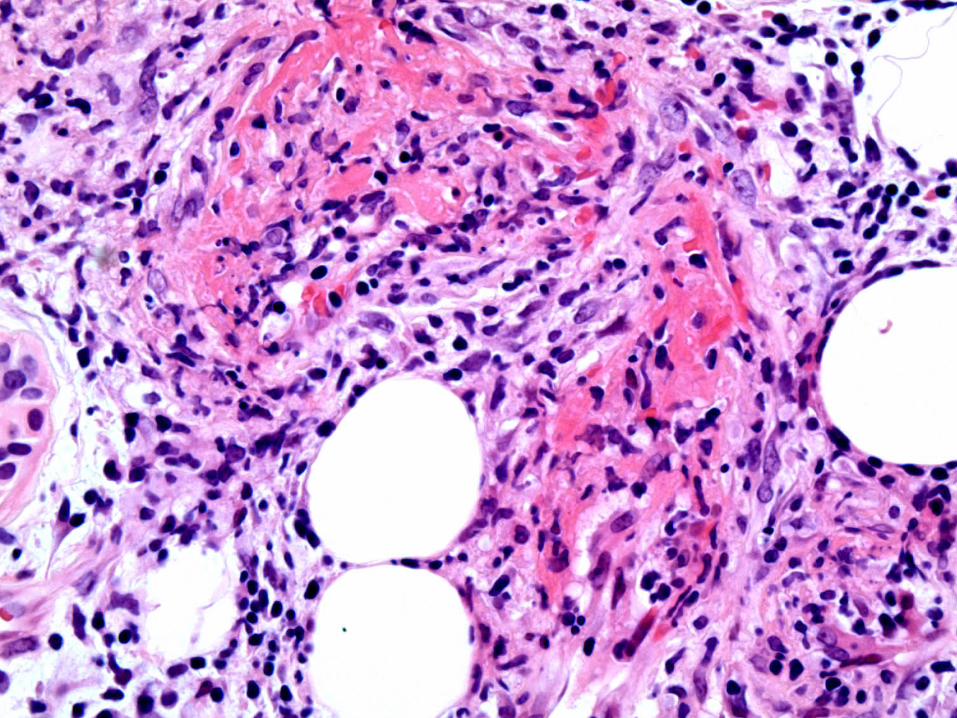
Histology Report: Lymphocytic true vasculitis including muscular vessels in the subcutis with widespread thrombosis of superficial vessels. Appearances in keeping with a systemic vasculitis, such as polyarteritis nodosa. In view of the widespread thrombotic element, suggest ruling out additional coagulopathy including cryoglobulins.
Necrotic plaques resolved with a course of high dose prednisolone

Investigations: February 2012
ANCA negative MPO: < 0.2 kIU/L IgG aCL: 0.8 GPL kU/L
Other Normal investigations: 2008 - 12
FBC U&E LFT ESR CRP
Vasculitis screen including: - Proteinase 3 antigen - Lupus anticoagulant antibody - ß-2-glycoprotein-1 antibody - Clotting - Cryoglobulin & cryofibrinogen - Hepatitis B serology
Favoured Clinicopathological Diagnosis
Cutaneous polyarteritis
nodosa (c-PAN)

Current daily treatment
5mg prednisolone (on reducing dose since Aug
‘11): No further ulcers or chilblains
300mg aspirin (dose increased from 75mg in
Aug ‘11) – but livedo racemosa progressing
50mg losartan (started in April ‘12)
45mg amitriptyline & 10mg rizatriptan
Omeprazole & Calcichew
Livedo racemosa • First introduced by
Ehrmann in 19071
• Originates from the Latin word racemus (bunch / cluster of grapes)
• No effective treatment for livedo racemosa & may extend despite antiplatelets or anticoagulants
Ehrmann S. Ein Gefaessprozess Bei Lues. Wien Med Wochenschr 1907;57:777-82
Biopsy of livedo racemosa2,3
• Biopsy uninvolved skin at the centre of a livedo racemosa area and affected area
• Obtain deep, adequate size biopsies (1-2cm) • More than 1 biopsy:
– Sensitivity of biopsy increases from 27% (1 biopsy) to
80% (3 biopsies)
• Obtain serial sections of the biopsies
2. Zelger B et al. Life history of cutaneous vascular lesions in Sneddon’s syndrome. Hum Pathol 1992;23:668-75 3. Wohlrab J et al. Diagnostic impact and sensitivity of skin biopsies in Sneddon’s syndrome. A report of 15 cases. Br J Dermatol 2001;145:285-8
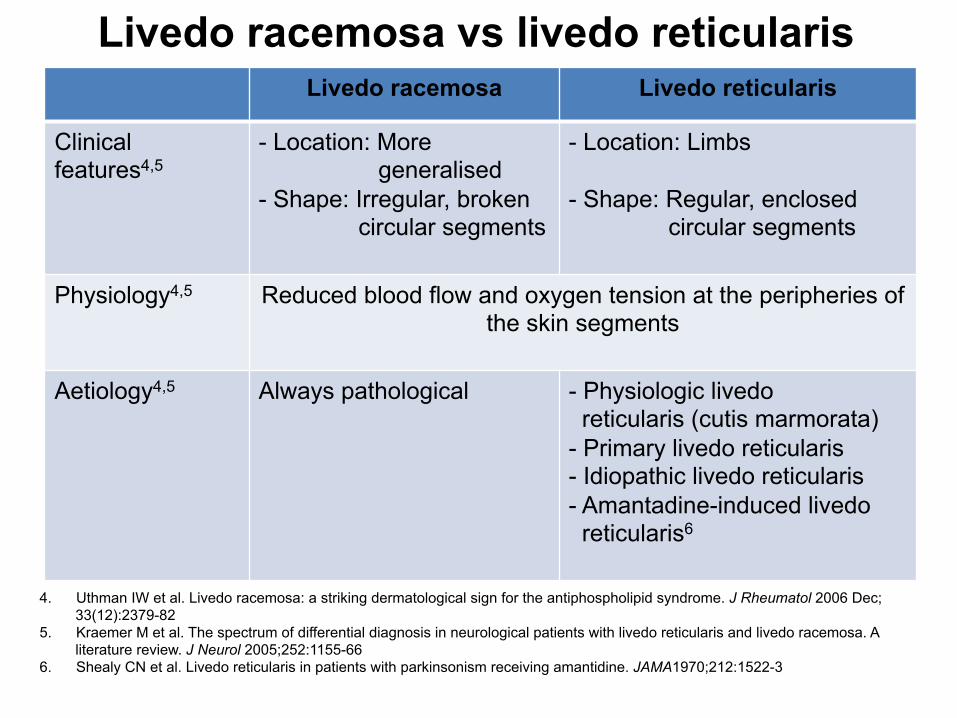
Livedo racemosa vs livedo reticularis Livedo racemosa Livedo reticularis
Clinical features4,5
- Location: More generalised - Shape: Irregular, broken circular segments
- Location: Limbs - Shape: Regular, enclosed circular segments
Physiology4,5 Reduced blood flow and oxygen tension at the peripheries of the skin segments
Aetiology4,5 Always pathological - Physiologic livedo
reticularis (cutis marmorata) - Primary livedo reticularis - Idiopathic livedo reticularis - Amantadine-induced livedo reticularis6
4. Uthman IW et al. Livedo racemosa: a striking dermatological sign for the antiphospholipid syndrome. J Rheumatol 2006 Dec;33(12):2379-82
5. Kraemer M et al. The spectrum of differential diagnosis in neurological patients with livedo reticularis and livedo racemosa. A literature review. J Neurol 2005;252:1155-66
6. Shealy CN et al. Livedo reticularis in patients with parkinsonism receiving amantidine. JAMA1970;212:1522-3
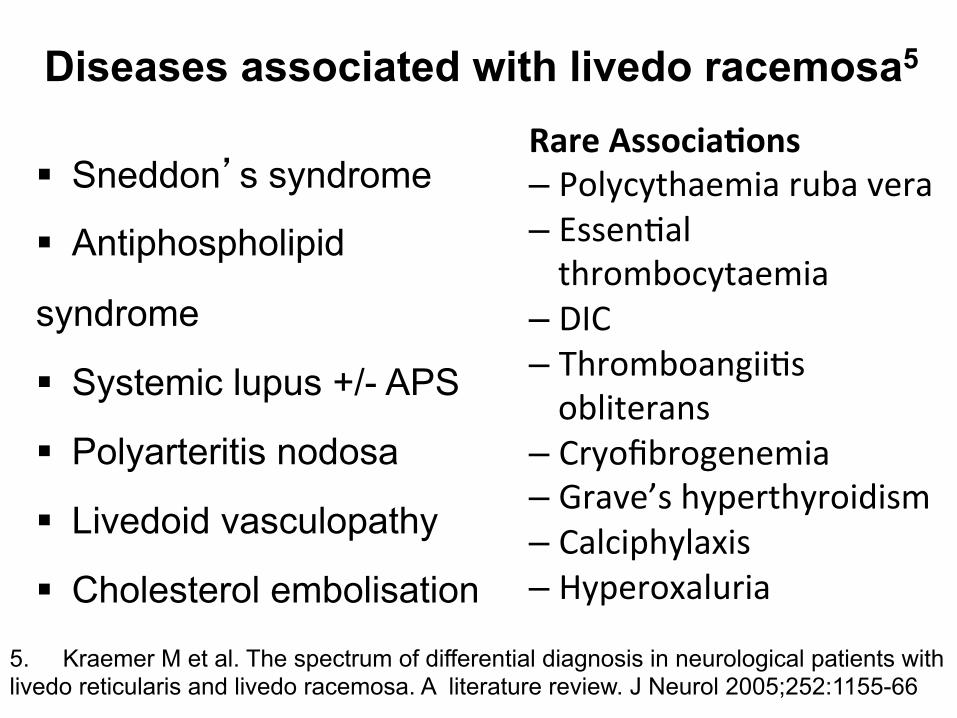
Diseases associated with livedo racemosa5
Sneddon’s syndrome
Antiphospholipid
syndrome
Systemic lupus +/- APS
Polyarteritis nodosa
Livedoid vasculopathy
Cholesterol embolisation
Rare Associa+ons – Polycythaemia ruba vera – Essen+al thrombocytaemia
– DIC – Thromboangii+s obliterans
– Cryofibrogenemia – Grave’s hyperthyroidism – Calciphylaxis – Hyperoxaluria
5. Kraemer M et al. The spectrum of differential diagnosis in neurological patients with livedo reticularis and livedo racemosa. A literature review. J Neurol 2005;252:1155-66

Sneddon’s syndrome
Diagnostic hallmark: Generalised livedo racemosa and ischaemic
stroke 1st described by Champion and Rook in 19607
1st characterised as a separate and distinct disease process by Sneddon in 19658
7. Champion RH, Rook A. Livedo reticularis. Proc R Soc Med 1960;53:961-2 8. Sneddon IB. Cerebrovascular lesions and livedo reticularis. Br J Derm 1965;77:180-5

Cutaneous polyarteritis nodosa (c-PAN)9,10
Rare form of vasculitis involving medium sized arteries
Aetiology unknown Chronic condition with relapses and remission Good prognosis 9. Morgan AJ et al. Cutaneous polyarteritis nodosa: a comprehensive review. Int J Dermatol 2010 Jul;49(7):750-6 10. Ishiguro N et al. Cutaneous polyarteritis nodosa: a report of 16 cases with clinical and histopathological analysis and a
review of the published work. J Dermatol 2010 Jan;37(1):85-93
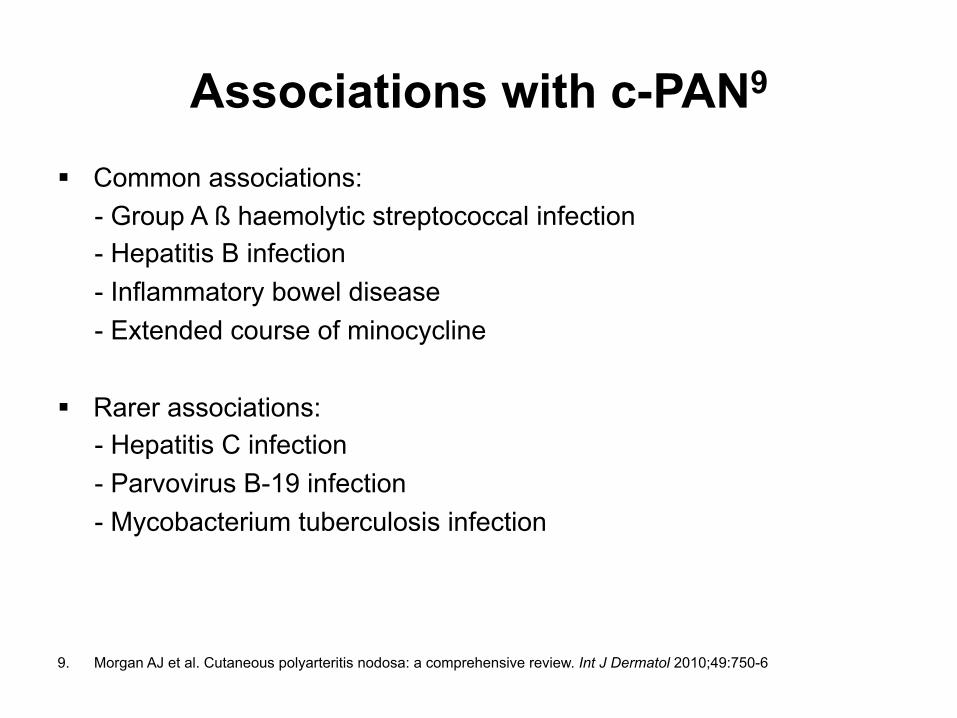
Associations with c-PAN9 Common associations: - Group A ß haemolytic streptococcal infection - Hepatitis B infection - Inflammatory bowel disease - Extended course of minocycline
Rarer associations: - Hepatitis C infection - Parvovirus B-19 infection - Mycobacterium tuberculosis infection 9. Morgan AJ et al. Cutaneous polyarteritis nodosa: a comprehensive review. Int J Dermatol 2010;49:750-6
Clinical features of c-PAN9,10 Cutaneous manifestations: - Tender subcutaneous nodules - Livedo racemosa - Tender indurated plaques - Necrosis - Punched-out ulcers - Purpura Extra-cutaneous manifestations: - Fever - Myalgia - Arthralgia - Neuropathy - Paraesthesia 9. Morgan AJ et al. Cutaneous polyarteritis nodosa: a comprehensive review. Int J Dermatol 2010 Jul;49(7):750-6 10. Ishiguro N et al. Cutaneous polyarteritis nodosa: a report of 16 cases with clinical and histopathological analysis and a
review of the published work. J Dermatol 2010 Jan;37(1):85-93
Laboratory abnormalities in c-PAN9 Frequently: - Mild anaemia - Moderate leukocytosis - Raised ESR - Anti-phosphatidylserine-prothrombin complex antibody (IgM >> IgG)11 Rare reported cases: - p-ANCA12
- Lupus anticoagulant antibody11
- Anticardiolipin antibody (IgG11,12 > IgM) 9. Morgan AJ et al. Cutaneous polyarteritis nodosa: a comprehensive review. Int J Dermatol 2010;49:750-6 11. Kawakami T et al. High titer of anti-phosphatidylserine-prothrombn complex antibodies in patients with cutaneous
polyarteritis nodosa. Arthritis Rheum 2007;57:1507-13 12. Pereira BAF et al. Cutaneous polyarteritis nodosa in a child with positive antiphospolipid and p-PANCA. Scand J Rheumatol
1995;24:386-8

Treatment of c-PAN9,10 NSAIDS Colchicine Aspirin Steroids Steroid sparing agents Dapsone IV Ig Perilesional injections of granulocyte-macrophage colony-stimulating factor13 9. Morgan AJ et al. Cutaneous polyarteritis nodosa: a comprehensive review. Int J Dermatol 2010 Jul;49(7):750-6 10. Ishiguro N et al. Cutaneous polyarteritis nodosa: a report of 16 cases with clinical and histopathological analysis and a review of the published work. J Dermatol 2010 Jan;37(1):85-93 13. Tursen U et al. Rapid healing of chronic leg ulcers during perilesional injections of granulocyte-macrophage colony-
stimulating factor therapy in a patient with cutaneous polyarteritis nodosa. JEADV 2006;20:1341-3
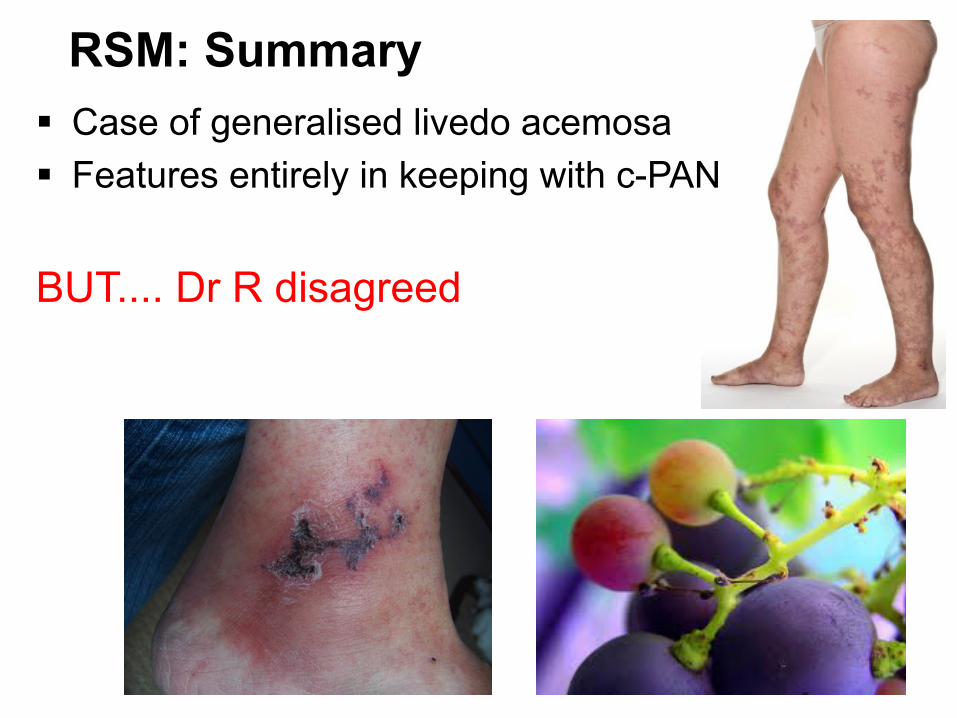
RSM: Summary Case of generalised livedo acemosa Features entirely in keeping with c-PAN BUT.... Dr R disagreed

s/b Bernhard Zelger Dear X and other colleagues involved in this lady`s case
This is a case of antiphospholipid-syndrome and as such no vasculitis, but a coagulopathy. Clinically, livedo (in this case racemosa) is characteristic of a coagulopathy and on the lower legs there is in addition also livedo vasculopathy (by others in my experience wrongly called livedo vasculitis).
As I showed in my presentation in Oxford this disease shows in stage II beside presence of fibrin thrombi (which would be stage I when present alone) plentiful lymphocytes accentuated around a superficial defect (as shown here in your series of histologies), but also involving deeper and larger vessels. This is yet an expected finding of reorganisation of stage I and will end as restitutio ad integrum or scar formation, atrophy blanche clinically and fibrosis, stage III livedo vasculopathy histologically.

s/b Bernhard Zelger (Cont)
Laboratory work up (it is typical that some coagulopathic parameters may become positive and negative in due course of disease showing undulation/roller-coaster of coagulation cascade) and previous history (abortion, misscarriage) excellently fit APS. The question is if patient will develop lupus erythemathodes or another collagenosis/systemic disease in due course which is well established in the literature. Previously, such cases would have been considered in the field of Sneddon syndrome, but this was before the respective laboratory parameters were worked out. And these laboratory parameters nicely parallel the ulcers, i.e. in livedo racemosa with livedo vasculopathy one has a much greater chance to find a causative coagulation factor than without ulcers.
Many thanks for sharing this case with me
Best greetings, from Innsbruck, Bernhard (zelger)

Just as an attachment / addition to my previous email. Classic PN (panarteriitis nodosa) characteristically affects arteries (or arterioles) at the border dermis-subcutis only, very rarely there is superimposed livedo vasculopathy which might then be difficult to differentiate histologically.
Clinically, in classic PN nodules are present beside livedo racemosa which is then also more starry sky-like (i.e. inflammatory) and shows in addition severe arthropathy of ankle region the latter of which by the way is mostly the earliest clinical finding.
Microscopic PN is (completely) different. It accentuates postcapillary venules and may also involve larger vessels. In your case accentuation is on capillaries.
Best greetings
Bernhard
Learning Points
• Always be prepared to re-‐assess a diagnosis • Don’t be afraid to get it wrong • Don’t be afraid to ask for help!
Thank You