clinical guideline on the assessment of the airway
TRANSCRIPT

Clinical Guideline on the Assessment of the AirwayFor Use in: Trust Wide
By: Anaesthetists / Airway trained staffFor: Airway Management in AdultsDivision responsible for document: Anaesthetics
Key words: Airway Assessment in Adults, Anaesthetic Pre-assessment, Intubation, Difficult Airway
Name and job title of document author’s:Dr Karan Verma, Specialist Trainee AnaesthesiaDr Edmund Quak, Consultant Anaesthetist
Name and job title of document author’s Line Manager:
Dr Michael Irvine, Consultant Anaesthetist, Clinical Director
Supported by:Dr Rocio Ochoa-Ferraro, Consultant Anaesthetist
Anaesthesia Governance Lead
Assessed and approved by the:
Airway Committee
Clinical Guidelines and Assessment Panel
If approved by committee or Governance Lead Chair’s Action; tick here
Date of approval: 29/12/2020
Ratified by or reported as approved to: Clinical Safety and Effectiveness Sub-Board
To be reviewed before:
This document remains current after this date but will be under review
29/12/2023
To be reviewed by: AuthorsReference and / or Trust Docs ID No: 14757Version No: 2
Description of changes:Addition of Quick Reference Guide flowchart
Updated literature referencesCompliance links: (is there any NICE related to guidance)
Difficult Airway Society (DAS)
If Yes - does the strategy/policy deviate from the recommendations of NICE?
If so why?No
Clinical Guideline for: Assessment of Airway in Adults Author/s: Dr Karan Verma, Specialist Trainee Anaesthesia, Dr Edmund Quak, Consultant AnaesthetistApproved by: CGAP and Airways Committee Date approved: 29/12/2020 Review date: 29/12/2023
Available via Trust Docs Version: 2 Trust Docs ID: 14757 Page 1 of 18

This guideline has been approved by the Trust's Clinical Guidelines Assessment Panel as an aid to the diagnosis and management of relevant patients and clinical circumstances. Not every patient or situation fits neatly into a standard guideline scenario and the guidelinemust be interpreted and applied in practice in the light of prevailing clinical circumstances, the diagnostic and treatment options availableand the professional judgement, knowledge and expertise of relevant clinicians. It is advised that the rationale for any departure from relevant guidance should be documented in the patient's case notes.
The Trust's guidelines are made publicly available as part of the collective endeavour to continuously improve the quality of healthcare through sharing medical experience and knowledge. The Trust accepts no responsibility for any misunderstanding or misapplication of this document.
Clinical Guideline for: Assessment of Airway in Adults Author/s: Dr Karan Verma, Specialist Trainee Anaesthesia, Dr Edmund Quak, Consultant AnaesthetistApproved by: CGAP and Airways Committee Date approved: 29/12/2020 Review date: 29/12/2023
Available via Trust Docs Version: 2 Trust Docs ID: 14757 Page 2 of 18

Clinical Guideline on the Assessment of the Airway
Version and Document Control:
VersionNumber
Date of Update
Change Description Author
2 29/12/2020Addition of Quick Reference Guide flowchart, Updated literature references
Dr Karan Verma, Dr Edmund Quak
This is a Controlled Document
Printed copies of this document may not be up to date. Please check the hospital intranet for the latest version and destroy all previous versions.Contents Page number1 Definitions of Terms Used 22 Quick Reference Guide 33 Objectives 64 Rationale 65 Scope 76 Processes to be followed 87 Clinical audit standards / audit standards / monitoring
compliance 11
8 Summary of development and consultation process undertaken before registration and dissemination
11
9 References 11Appendices
1 Example of a conventional airway pre-assessment 132 Difficult facemask ventilation 143 Difficult SAD insertion 144 Difficult laryngoscopy 145 Difficult front of neck access 146 Non-reassuring airway assessment features (adapted
from ASA Task Force on Management of the Difficult Airway, 2013)
15
7 Modified Mallampati classification 158 Wilson’s risk-sum index 169 Upper lip bite test 16
1. Definitions of Terms UsedBMI Body Mass IndexCTM Cricothyroid MembraneDAS Difficult Airway SocietyFONA Front of Neck Access - cannula or surgical cricothyroidotomyLMA Laryngeal Mask AirwayODP Operating Department PractitionersOSA Obstructive Sleep ApnoeaSAD Supraglottic Airway Device
Clinical Guideline for: Assessment of Airway in Adults Author/s: Dr Karan Verma, Specialist Trainee Anaesthesia, Dr Edmund Quak, Consultant AnaesthetistApproved by: CGAP and Airways Committee Date approved: 29/12/2020 Review date: 29/12/2023
Available via Trust Docs Version: 2 Trust Docs ID: 14757 Page 3 of 18

2. Quick Reference Guide
This is a rapid airway assessment framework to aid airway management planning and decision-making. It is a summary and should be used in conjunction with more detailed information provided later in this document.
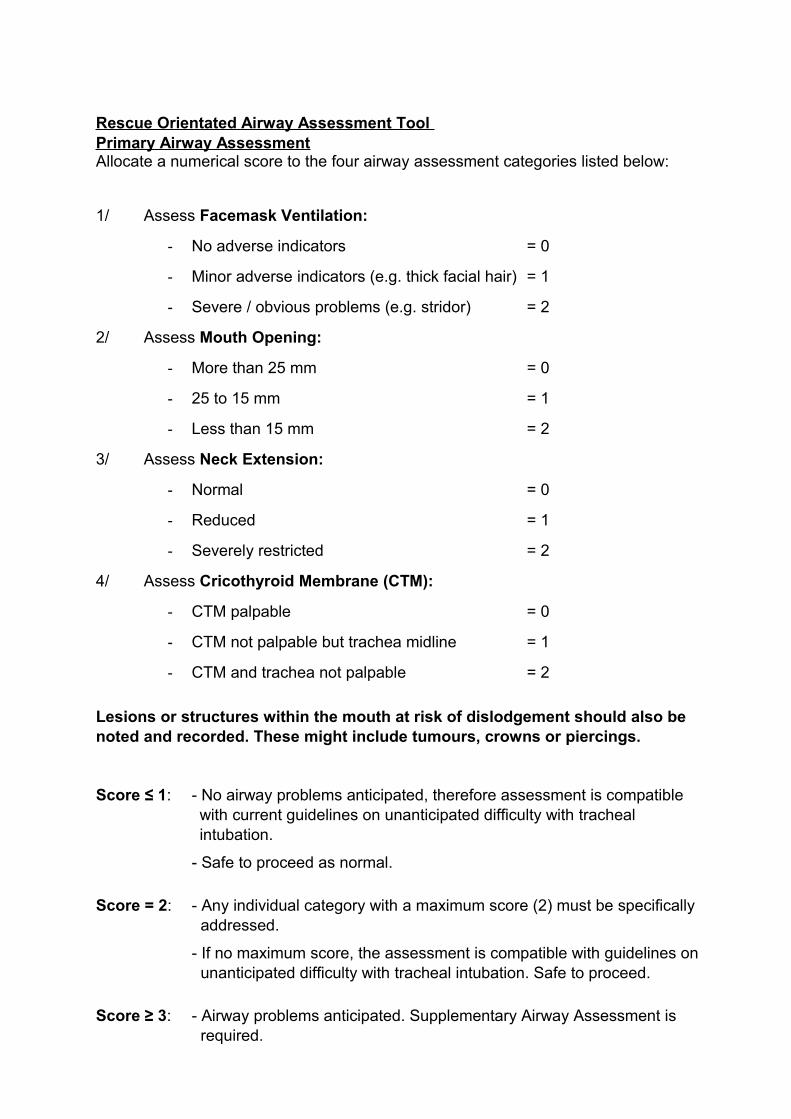
Rescue Orientated Airway Assessment Tool Primary Airway AssessmentAllocate a numerical score to the four airway assessment categories listed below:
1/ Assess Facemask Ventilation:
- No adverse indicators = 0
- Minor adverse indicators (e.g. thick facial hair) = 1
- Severe / obvious problems (e.g. stridor) = 2
2/ Assess Mouth Opening:
- More than 25 mm = 0
- 25 to 15 mm = 1
- Less than 15 mm = 2
3/ Assess Neck Extension:
- Normal = 0
- Reduced = 1
- Severely restricted = 2
4/ Assess Cricothyroid Membrane (CTM):
- CTM palpable = 0
- CTM not palpable but trachea midline = 1
- CTM and trachea not palpable = 2
Lesions or structures within the mouth at risk of dislodgement should also be noted and recorded. These might include tumours, crowns or piercings.
Score ≤ 1: - No airway problems anticipated, therefore assessment is compatible with current guidelines on unanticipated difficulty with tracheal intubation.
- Safe to proceed as normal.
Score = 2: - Any individual category with a maximum score (2) must be specifically addressed.
- If no maximum score, the assessment is compatible with guidelines on unanticipated difficulty with tracheal intubation. Safe to proceed.
Score ≥ 3: - Airway problems anticipated. Supplementary Airway Assessment is required.

Supplementary Airway Assessment (if primary assessment score is ≥ 3 )
The airway cannot be considered in isolation. Aspiration risk, haemodynamic instability and increased oxygen demand put a patient at higher risk of complications ifairway management is also delayed or complicated.
Therefore, if the primary airway assessment score is 3 or more, two additional assessments are required.
5/ Assess Aspiration Risk:
- Low = 0
- Moderate = 1
- High = 2
6/ Assess Physiological Derangement:
- None = 0
- Mild hypoxaemia, cardiovascular instability,
morbid obesity, or third trimester of pregnancy = 1
- Severe hypoxaemia or shock = 2
Completing the supplementary airway assessment will provide a cumulative score range (for all six categories) of 3 – 12. Any category with a maximum score (2) needs to be specifically addressed before induction of anaesthesia.
Score 3: - Increased difficulty with airway management is expected but the patient remains compatible with guidelines on unanticipated difficulty with tracheal intubation, therefore proceed as normal.
Score 4 – 6: - Accumulating probability of airway complications.
- Junior trainees should locate and inform a senior colleague.
- Inform ODP of management and escape plans.
- Assemble appropriate equipment.
Score 7 – 12:- Very high risk of airway complications.
- Senior anaesthetist should be involved and decision to proceed carefully weighed, including consideration of alternative anaesthetic techniques.
- Inform ODP of management plan, assemble equipment required.
- Consider need for surgical stand-by for emergency surgical airway.
3. Objectives
The aim of this guideline is to provide:
1. A systematic assessment to identify patients incompatible with the NNUH unanticipated difficulty with tracheal intubation guidelines.
2. A structured framework to enable the detection of potential problems leading to selection of the most appropriate airway management techniques, particularly outside of the theatre complex.
3. A source of information to aid airway management and planning.
4. A resource for training and discussion.
5. A framework for communication of airway problems between professionals.
4. Rationale
The 4th National Audit Project looking at ‘Major Complications of Airway Management in the United Kingdom’ highlighted significant deficiency in airway assessment as a factor in many of the cases of airway complications. Out of 133 reports, difficulty in airway management was anticipated in 66 cases but subsequent management strategy was not always matched to the initial assessment1.
Conventional practice of airway assessment relies on trying to predict a difficult airway. There are however two fundamental flaws with this concept. Firstly, the term ‘difficult airway’ is poorly defined with huge variation in definitions used in different scientific literatures2. Secondly, to predict difficult airway, this infers that there are reliable assessment tests available. Accurate prediction of difficult laryngoscopy is generally regarded as being flawed4,5. An editorial by Yentis eloquently explains why even the best airway assessment tests have very low positive predictive value for difficult airway due to the relatively low number of cases of ‘truly difficult airway’6. Predicting patients with difficult airway is therefore, unlikely to ever be reliable.
For discussion and training purposes, some of these airway assessment tests have been included in this document as Appendices.
On the contrary however, a guideline for the management of unanticipated difficulty with mask ventilation and tracheal intubation already exists in the Trust with four proposed rescue plans – A) facemask ventilation, B) tracheal intubation, C) use of supraglottic airway device and D) front of neck access3. However, for these rescue plans to be viable, they rely on the assumption that each of these options is a credible proposition in the first place.
For example, if a patient with severely restricted mouth opening develops an airway complication on induction of anaesthesia, the use of a supraglottic airway device, although recommended in the guideline, is not actually a feasible rescue strategy because it would not be possible to introduce the device into the mouth.

For these reasons, the purpose of this airway assessment framework as described in the Quick Reference Guide is not to predict a difficult airway but instead, to assess theviability of the rescue / escape strategy in the event of an unanticipated difficult airway.Where problems are detected in the primary airway assessment, this should prompt an alternative, individualised airway management plan. Patients who are deemed to be incompatible with the DAS/NNUH unanticipated difficulty with tracheal intubation guidelines should NOT be treated in the usual standard manner. To do so may mean that in the event of an actual airway complication, the DAS/NNUH unanticipated difficult intubation rescue strategies are unlikely to be successful at salvaging the situation (Fig 1).
It is worth emphasising that in cases of airway complications, failure to look for problems, lack of knowledge, and reluctance to change behaviour are some of the reasons identified for the failure of anaesthetists to anticipate and manage difficult airways1,2,3,.
Fig 1: Implications of adverse features identified in airway pre-assessment
5. Scope
This guide is intended for the airway practitioners managing airway in and outside of the theatre complex. Although primarily aimed at anaesthetists, it may also be used byODPs, nurses and clinicians involved in the occasional airway management.
This guide is strictly for use in assessing the airway of adult patients only, including in obstetrics.
Airway assessment and management for the neonatal and paediatric population are outside the scope of this guideline.

6. Processes to be followed
This document is intended for use in conjunction with the following Trust Guidelines:
Trust Guidelines for the ‘Management of Unpredicted Difficult Ventilation and Unpredicted Difficult Intubation in Adults’
Joint Trust Policy for the ‘Management of Pre-operative Food, Drink and Oral Medications in Adult and Paediatric Patients Prior to Surgery’
6.1 History
A history of airway problems makes subsequent airway complications more likely. Steps should be taken to identify patients who have had previous airway problems during general anaesthesia and their previous anaesthetic records interrogated in order to understand the precise problem encountered. History of radiotherapy to the neck should also be noted. Similarly, certain genetic syndromes and cranio-facial deformities are known to be associated with difficult airway. This should be enquired as part of an airway history taking. Relevant imaging of the airway especially in head and neck cases should be reviewed.
6.2 Facemask Ventilation
Ability to facemask ventilate is a core component of any airway management. Difficultyin mask ventilation may result from factors involving patients, operators and equipment. Minor features associated with difficult facemask ventilation are listed in Table 1:
Age >57 years Facial trauma Mallampati III/IV
Thick facial hair Snoring/Obstructive Sleep Apnea (OSA)
Nasal deformity
Limited mandibular protrusion
BMI > 30kg/m2 Edentulous

Table 1: Minor features commonly associated with difficult mask ventilation
Examples of severe features of difficult facemask ventilation may include stridor or major facial trauma that prohibits the formation of a tight seal with a facemask.
Stridor is an audible indication of significant airway obstruction and this represents a high risk of difficulty with facemask ventilation and possibly ventilation by SAD or tracheal intubation. It is intended that a guideline for the peri-operative management ofpatients with airway obstruction and stridor will be developed but this has not yet beenachieved.
6.3 Mouth Opening
Restriction to mouth opening makes airway instrumentation, intubation and insertion ofSADs difficult. SADs may be used as a primary rescue or they can also be used as a conduit for fibre-optic intubation either electively or in an airway rescue situation. Few factors prevent SAD insertion. An iGel size 3 or a Proseal LMA 3 may be inserted through an inter-incisor distance of 15 mm7. For this reason 15 mm was selected as a suitable cut off limit in adults.
6.4 Oral Cavity
Dentition, piercings, dentures and tumours that may bleed or be dislodged should be noted and recorded during assessment of mouth opening.
6.5 Neck Extension
Head extension and jaw thrust are often used to relieve airway obstruction. It should be expected that limitation of neck extension might impair or prevent effective mask ventilation. Furthermore it will make it difficult to align the airway axis for laryngoscopy,tracheal intubation or insertion of SADs. In patients with severe neck flexion deformity,the cricothyroid membrane may lie within the chest or access to it may be blocked by the patient’s mandible.
A small reduction in neck extension on its own may not be problematic but severely reduced neck extension, including in trauma scenarios where the cervical spine has be to fully immobilised, may make direct laryngoscopy extremely challenging. A crude assessment of neck extension should suffice without the need for accurate measurements using special apparatus. Where significant restriction is detected, alternative airway management strategies should be instituted before induction of anaesthesia. The use of video-laryngoscopes and flexible fibre-optic scopes may be helpful in these situations.
6.6 Cricothyroid Membrane
Surgical cricothyroidotomy is the final recommended strategy for airway rescue by the DAS/NNUH unanticipated difficult intubation guideline. By the time this option is contemplated, the patient may be on the verge of a cardio-respiratory arrest and less invasive rescue strategies have been ineffective. Cricothyroidotomy is easiest when the CTM is clearly palpable and should therefore be routinely assessed pre-induction. Pre-operatively, an impalpable trachea and CTM may be identified using an ultrasound probe and the location marked.

In the event that a surgical cricothyroidotomy is required for a patient with impalpable CTM, a 10 cm vertical midline incision is recommended followed by finger dissection to identify the CTM3. The opportunity for regular practice of surgical cricothyroidotomy on a cricothyroidotomy trainer should be available.
6.7 Aspiration Risk
Aspiration is one of the commonest causes of death from airway problems during anaesthesia. Aspiration may complicate any airway management scenario and shouldform an integral part of an airway assessment. Assessment of aspiration risk should take into consideration the patient’s medical problems, medication, fasting status and current surgical pathology. Where possible, steps should be taken before surgery to reduce the volume and pH of gastric contents by fasting, pharmacological means and mechanical drainage by nasogastric tube. The latter is of particular benefit in those patients with severely delayed gastric emptying or intestinal obstruction. Table 2 lists the factors commonly associated with an increased risk of aspiration.

Patient factors Surgical factors Anaesthetic factors
Full stomach Upper GI surgery Light anaesthesia
Delayed gastric emptying Lithotomy SAD (especially 1st Gen)
Intestinal obstruction/ acute abdomen
Head down position Positive pressure ventilation
Incompetent lower oesophageal sphincter
Laparoscopy Surgery > 2 hours
Oesophageal diseases Gastric distention
Obesity Incomplete reversal of neuromuscular blockade
Autonomic dysfunction (e.g. due to diabetes)
Neuromuscular diseases
Table 2. Risk factors for aspiration
6.8 Physiological Derangement
Physiological derangement has the effect of either reducing the available oxygen reserve in a patient or increasing their oxygen demand. Both have the effect of diminishing the apnoea time before the patient begins to desaturate at induction of anaesthesia. In the event of a difficult airway, this represents a greater hazard as hypoxaemia and complications are likely to arise sooner compared to an otherwise physiologically normal patient. It is crucial therefore that any formulated airway management plan takes this into consideration.
6.9 Pre-Oxygenation
All patients benefit from routine pre-oxygenation but particularly so in the event of an unexpected airway management problem. In addition to conventional pre-oxygenation practice, the use of supplemental oxygen via nasal cannulas using the NO DESAT (nasal oxygen during efforts securing a tube) and High Flow Nasal Oxygenation (HFNO) techniques have been described with reported success in prolonging the apnoea time in many cases8-10. However, HFNO requires a specific humidified oxygen delivery system.
6.10 Airway Management Plan
It is beyond the scope of this guideline to propose the exact management plan for each airway problem. Clearly, the airway management plan has to be individualised taking into consideration the specific airway concern, available skills mix, equipment, etc.
Any individual category identified with a maximum score (2) during airway assessmenthighlights a significant airway concern and must therefore be specifically addressed before induction of anaesthesia.
Early senior involvement is crucial. In the case of an elective operation, alternative anaesthetic techniques, and perhaps even postponing the surgery until the

appropriate support is available must be considered. Surgical airway as the primary technique of choice may be the most appropriate in some situations.
7. Clinical audit standards / audit standards / monitoring compliance
Future mortality and morbidity cases should be presented regularly at the monthly Anaesthetic Clinical Governance meetings and used to test the recommendations made within these guidelines.
The output of Governance meetings will be reviewed by the chairman and Clinical Director and where measures are required, this will be communicated either directly tothe relevant parties, or by dissemination of the minutes of the governance meetings bythe Governance Lead. The Clinical Director has overall responsibility to ensure that agreed action plans are implemented.
Independent audit of airway assessment and documentation should also be performedagainst the recommendations in this guideline at intervals of no less than once every two years. This will be co-ordinated by the Lead Anaesthetist for Airway.
8. Summary of development and consultation process undertaken before registration and dissemination
During its development, the draft document was presented to the Anaesthetic body at the February 2017 departmental governance meeting for comments. It has been circulated for comment to: Consultant Anaesthetists (Drs Lindsay Barker, Helen Goddard, Robert Harwood, Paul Hutchings, Lorna Kerr and David Spackman). An abstract of this guideline was also presented at the Difficult Airway Society ASM 2017 for feedback and discussion.
Version 1 of this document was authored by Dr E Quak and Dr C Lopez-Soto, supported by Dr N Woodall in 2017. This current version has been endorsed by the Airway Committee.
9. References
1. Cook TM, Woodall N, Frerk C; Fourth National Audit Project. Major complications of airway management in the UK: results of the Fourth National Audit Project of the Royal College of Anaesthetists and the Difficult Airway Society. Part 1: Anaesthesia. Br J Anaesth 2011; 106:617–31
2. Apfelbaum JL et al. Practice guidelines for management of the difficult airway: an updated report by the American Society of Anesthesiologists Task Force on Management of the Difficult Airway. Anesthesiology Feb 2013; 118:251 – 270.
3. Frerk C et al. Difficult Airway Society 2015 guidelines for management of unanticipated difficult intubation in adults. Br J Anaesth 2015; 115 (6):827-48
4. Baker P. Assessment before airway management. Anesthesiology Clinics 2015;(33):257-278
5. Lewis MM, Keramati SM, Benumof JL et al. What is the best way to determine oropharyngeal classification and mandibular space length to predict difficult laryngoscopy? Anesthesiology 1994; 81:69-75
6. Yentis SM. Predicting difficult intubation—worthwhile exercise or pointless ritual? Anaesthesia 2002; 57:105–9

7. Wild K, Woodall N. A bench test for determining the minimum access requirements for the insertion of four supraglottic airway devices currently available in the UK. Anaesthesia 2011; 66:237–238
8. Levitan RM. NO DESAT! Nasal oxygen during efforts securing a tube. Emergency Physicians Monthly. December 9, 2010. http://epmonthly.com/article/no-desat/
9. Weingart SD, Levitan RM. Preoxygenation and prevention of desaturation during emergency airway management. Ann Emerg Med. 2012; 59(3):165-175.
10. Patel A, Nouraei SA. Transnasal humidified rapid-insufflation ventilatory exchange (THRIVE): a physiological method of increasing apnoea time in patients with difficult airways. Anaesthesia 2015; 70(3):323-329.
11. Cattano D, Killoran PV, Iannucci D, et al. Anticipation of the difficult airway: preoperative airway assessment, an educational and quality improvement tool. Br J Anaesth 2013; 111:276–285.
12. Kheterpal S, Han R, Tremper KK, et al. Incidence and predictors of difficult and impossible mask ventilation. Anesthesiology 2006; 105:885–91
13. Mallampati SR, Gatt SP, Gugino LD, Desai SP, Waraksa B, Freiberger D, Liu PL: A clinical sign to predict difficult tracheal intubation: A prospective study. Can Anaesth Soc J 1985; 32:429–34.
14. Wilson ME, Spiegelhalter D, Robertson JA, Lesser P. Predicting difficult intubation. Br J Anaesth 1988; 61:211–6.
15. Khan ZH, Kashfi A, Ebrahimkhani E. A comparison of the upper lip bite test (a simple new technique) with modified Mallampati classification in predicting difficulty in endotracheal intubation: a prospective blinded study. Anesth Analg. 2003 Feb;96(2):595-9.
16. Roth D, Pace NL, Lee A, et al. Airway physical examination tests for detection of difficult airway management in apparently normal adult patients. Cochrane Database Syst Rev. 2018 May 15; 5(5).
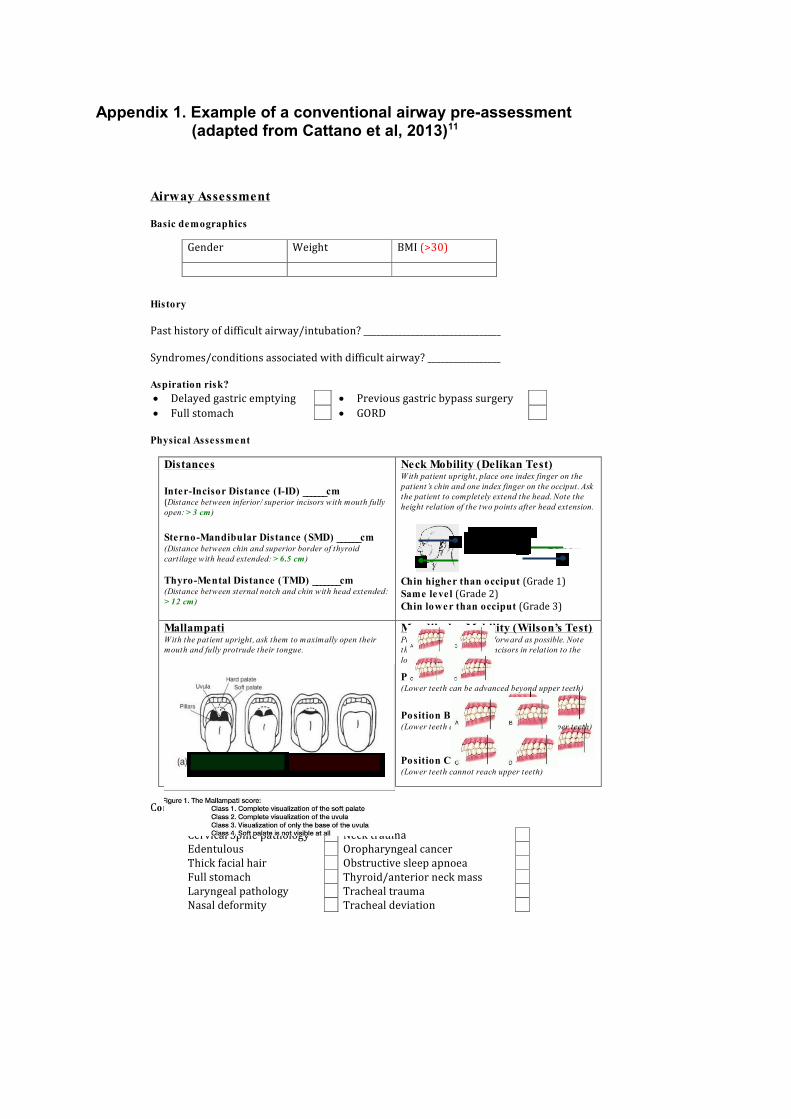
Appendix 1. Example of a conventional airway pre-assessment (adapted from Cattano et al, 2013)11
Airway Assessment
Basic demographics
History
Past history of difficult airway/intubation? ________________________________
Syndromes/conditions associated with difficult airway? _________________
Aspiration risk?· Delayed gastric emptying · Previous gastric bypass surgery· Full stomach · GORD
Physical Assessment
Conditions associated with difficult airway
Distances
Inter-Incisor Distance (I-ID) ______cm(Distance between inferior/ superior incisors with mouth fullyopen:> 3 cm )
Sterno-Mandibular Distance (SMD) ______cm(Distance between chin and superior border of thyroidcartilage with head extended:> 6.5 cm )
Thyro-Mental Distance (TMD) _______cm(Distance between sternal notch and chin with head extended:> 12 cm )
Neck Mobility (Delikan Test)With patient upright, place one index finger on thepatient’s chin and one index finger on the occiput. Askthe patient to completely extend the head. Note theheight relation of the two points after head extension.
Chin higher than occiput (Grade 1)Same level (Grade 2)Chin lower than occiput (Grade 3)
MallampatiWith the patient upright, ask them to maximally open theirmouth and fully protrude their tongue.
Mandibular Mobility (Wilson’s Test)Protrude mandible as far forward as possible. Notethe position of the upper incisors in relation to thelower.
Position A(Lower teeth can be advanced beyond upper teeth)
Position B(Lower teeth can be advanced even with upper teeth)
Position C(Lower teeth cannot reach upper teeth)
Gender Weight BMI (>30)
Cervical Spine pathology Neck traumaEdentulous Oropharyngeal cancerThick facial hair Obstructive sleep apnoeaFull stomach Thyroid/anterior neck massLaryngeal pathology Tracheal traumaNasal deformity Tracheal deviation
extension

Appendix 2. Difficult facemask ventilation12
Factors Associated with Difficult Facemask VentilationAge >57 years Facial trauma Mallampati III/IVThick facial hair Snoring/OSA Nasal deformityLimited mandibular protrusion
BMI > 30kg/m2 Edentulous
Appendix 3. Difficult SAD insertion
Factors Associated with Difficult SAD InsertionMouth opening < 1.5cm Male Airway abnormalitiesGlotic/SupragloticExtraglotic/SubgloticPathology
Increased BMI Patient transport
Fixed cervical spine Poor dentition Upper airway obstructionCricoid pressure Rotation surgical table
during case
Appendix 4. Difficult laryngoscopy
Factors Associated with Difficult LaryngoscopyMallampati III/IV Neck circumference > 30cmMouth opening < 2cm Upper lip bite position CThyro-mental distance < 6cm Atlanto-occipital extension grades III/IVSterno-mental distance < 10cm
Appendix 5. Difficult front of neck access
Factors Associated with Difficult Front of Neck AccessFemale Thick/ overlying pathologyAge < 8 years old Fixed cervical spineThick neck Overlying pathologyDisplaced airway

Appendix 6. Non-reassuring airway assessment features (adapted from ASA Task Force on Management of the Difficult Airway, 2013)2
Appendix 7. Modified Mallampati classification13
This is assessed by asking the patient (in an upright position) to maximally open his/her mouth and protrude the tongue. Visibility of faucial pillars, soft palate and uvulainside the patient's mouth will result in a score of one to three. A Mallampati score of four was later added.
Mallampati FeaturesI Faucial pillars, soft palate and entire uvula can be visualised.II Faucial pillars and soft palate can be visualised. The uvula is masked
by the base of the tongue.III Only the soft palate is visible.IV The soft palate is not visible, i.e. only the hard palate can be visualised
at the roof of the mouth.
Mallampati in his original paper in 1985 demonstrated the relationship between his scoring system and ease of laryngoscopy. Most patients with a score of one would have a grade 1 Cormack-Lehane view during laryngoscopy. Most patients with a scoreof two would have a grade 2 view and so on.

Appendix 8. Wilson’s risk-sum index14
Risk Factor 0 1 2
Weight (kg) < 90 90 – 110 >110Head & Neck Movement (°)
> 90 ≈ 90 +/- 10 < 90
I-I Distance (cm)Mandible Subluxation
> 5 or> 0
= 5 and= 0
< 5 and< 0
Receding Mandible None Moderate SevereBuck Teeth None Moderate Severe
Risk sum score is out of 10. Score of ≥ 2 will correctly predict 75% of difficult airway but carries a 12.1% false positive rate (see Table A below).
Risk Sum Criterion
True Positive (%) False Positive (%)
≥ 6 8 0≥ 5 17 0.3≥ 4 42 0.8≥ 3 50 4.6≥ 2 75 12.1≥ 1 92 26.2
Appendix 9. Upper Lip Bite Test15
(Image adapted from Roth et.al, 201816)