clinical experiences of boron neutron capture therapy to recurrenced rectal cancers hironobu...
TRANSCRIPT
Clinical Experiences of Boron Neutron Capture Therapy
to Recurrenced Rectal Cancers
Hironobu Yanagie*, Kazuyuki Oyama, Ryo Hatae, Syoji Maruyama, Yasuo Ohno, Shinichi Kurokawa, Yasumasa Nonaka,
Hirotaka Sugiyama, Yoshitaka Furuya, Keiko Taniike, Minoru Suzuki, Shin-ichiro Masunaga, Tomoko Kinashi, Yoshinori Sakurai, Natsuko Kondo, Masaru Narabayashi, Hiroki Tanaka, Akira
Maruhashi, Koji Ono, Jun Nakajima, Minoru Ono, Hiroyuki Takahashi, and Masazumi Eriguchi
*Dept. of Innovative Cancer Therapeuticis, Alpha particle & Immunotherapeutics,
Meiji Pharmaceutical UniversityE-mail: [email protected]
16th International Conference on Neutron Capture Therapy15th June 2014, Helsinki, FINLAND

Our proceeding BNCT Clinical Studies
•BNCT to Recurrenced / Advanced Cancer which is resistant to combinational Therapy •BNCT with Intra-arterial infusion of BSH-WOW emulsion to Recurrenced Hepatocellular Carcinoma
•BNCT to Recurrenced / Advanced Breast Cancer

Clinical Study Design 1ObjectWe perform pilot clinical study of boron neutron capture therapy to cancers that had been no effective or no indication of standard therapies using intra-veneous injection of 10Boronophenylalanine (10BPA) for evaluate its effeciency and safety.
Indication for Registration of patients 1. Over 20 years old2. No efectiveness by standard therapies
(chemotherapy, immunotherapy, or hormonal therapy,)
3. The patients whom is difficult to perform operations in advanced or recurrenced cancer stages, the patients who had rejected to be performed the operations, the patients will be able to lose the QOL by operations
4. The patients whom had not cured by iradiation therapy, or had no indication of iradiation therapy in cause of irradiation field.
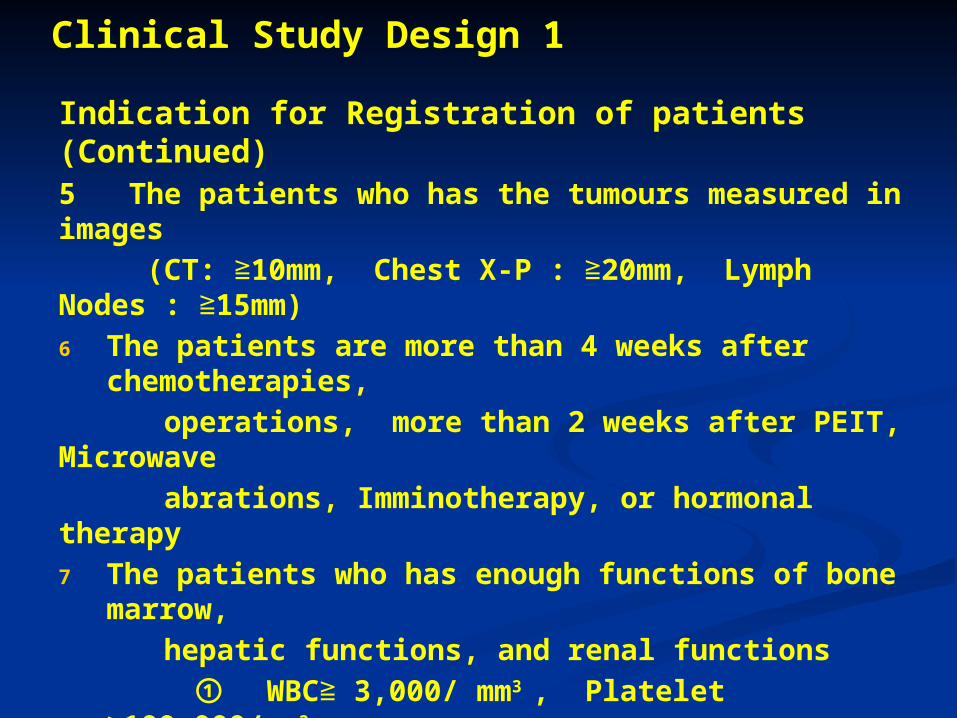
Clinical Study Design 1
Indication for Registration of patients (Continued) 5 The patients who has the tumours measured in images (CT: ≧10mm, Chest X-P : ≧20mm, Lymph Nodes : ≧15mm)6 The patients are more than 4 weeks after
chemotherapies, operations, more than 2 weeks after PEIT, Microwave abrations, Imminotherapy, or hormonal therapy7 The patients who has enough functions of bone
marrow, hepatic functions, and renal functions
① WBC≧ 3,000/ mm3 , Platelet ≧100,000/mm3
② GOT / GPT : ≦ 120 IU / l, Total Bilirubin : ≦ 2.0 mg / dl ③ Creatinine : ≦2 mg/dl
8 The patients who had accepted the Informed Concent with
contract
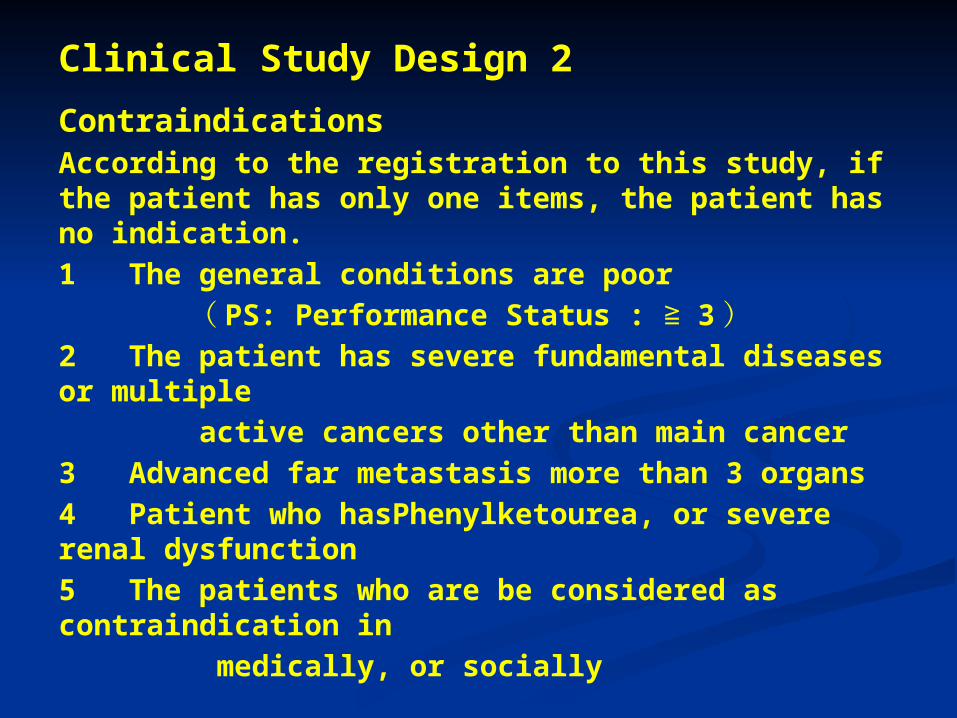
Clinical Study Design 2
Contraindications According to the registration to this study, if the patient has only one items, the patient has no indication.1 The general conditions are poor ( PS: Performance Status : ≧ 3 )2 The patient has severe fundamental diseases or multiple active cancers other than main cancer3 Advanced far metastasis more than 3 organs4 Patient who hasPhenylketourea, or severe renal dysfunction5 The patients who are be considered as contraindication in medically, or socially
Registered Patients Number n = 10

Procedure of Pilot Study
1. The patient come to the registrated hospital from the other hospital with introduction form
2. Pre performanced diagnosis(Detect the indication) with discussion with KUR stuff by checking the CT images of recurrenced tumours
3. Checking the uptake of Boron by 18F –BPA-PET
4. Informed Concent of the pilot study of BNCT 5. Order for BNCT at KUR (Neutron dosimetry
by SERA)6. Simulational CT imaging in the same position
at BNCT with marking of the tumour sites 1 week before BNCT

7. BNCT procedure at KUR Intra-veneous injection of 10Boronophenylalanine – Fructose complex (10BPA-F) 3hours before BNCT (400mg /kg) The boron concentrations in blood are measured by γ- Telescopy (KUR). After BNCT : Stay at the hosted hospital
8. After CareThe effects of tumour suppression is
evaluate with the decreasing rate of the tumour by images of CT scan and MRI, and data of tumour markers. We also evaluate according to the RECIST cliteria of Japan Clinical Oncology Groups.
7. BNCT procedure at KUR Intra-veneous injection of 10Boronophenylalanine – Fructose complex (10BPA-F) 3hours before BNCT (400mg /kg) The boron concentrations in blood are measured by γ- Telescopy (KUR). After BNCT : Stay at the hosted hospital
8. After CareThe effects of tumour suppression is
evaluate with the decreasing rate of the tumour by images of CT scan and MRI, and data of tumour markers. We also evaluate according to the RECIST cliteria of Japan Clinical Oncology Groups.
Procedure of Pilot Study (continued)

Mortality Rate of Cancer in Japan
Colon Cancer
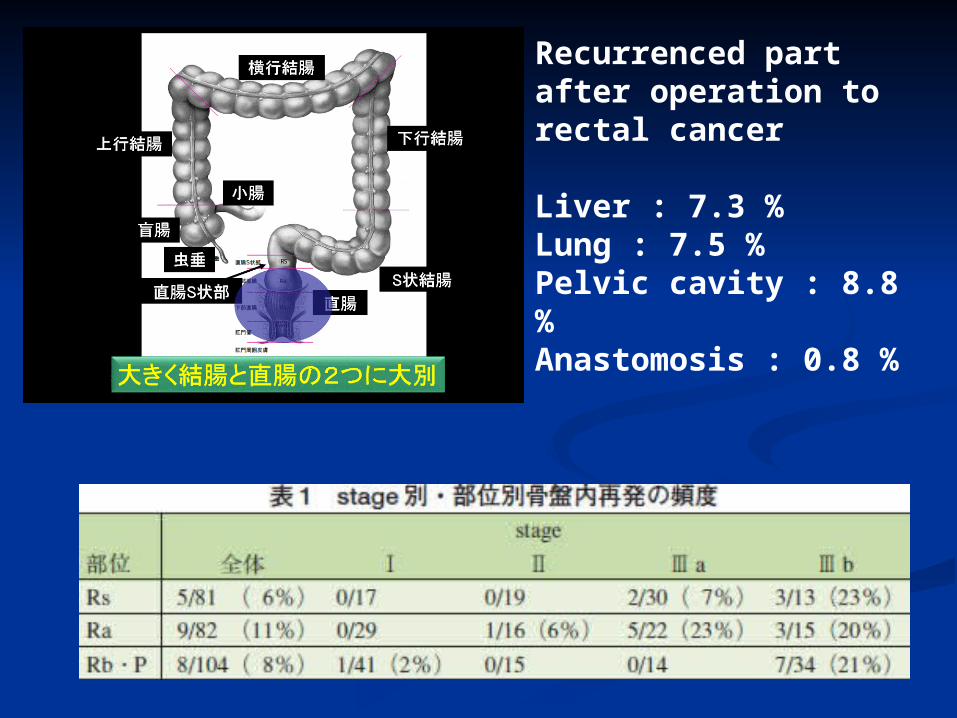
Recurrenced part after operation to rectal cancer
Liver : 7.3 %Lung : 7.5 %Pelvic cavity : 8.8 %Anastomosis : 0.8 %

Pilot Clinical Trial of Boron Neutron Capture Therapy
to Recurrenced Rectal Cancer using intraveneous injection of 10BPA

[ Case 1 ] 51y.o. Female, Rectal Cancer Clinical course1 16th .October.2006 : Low anterior resection Pathological findings: Adenocarcinoma of the rectum, tub2, type2, 6×7cm, AW(-), OW(-), n(+)(1/13)(#251) Postoperative staging : ( Ra ) pSE pN1 sH0 sP0 sM0 fStage aⅢ
2 June. 2009: Local recurrence in pelvic cavity & Invasion to Sacral bone
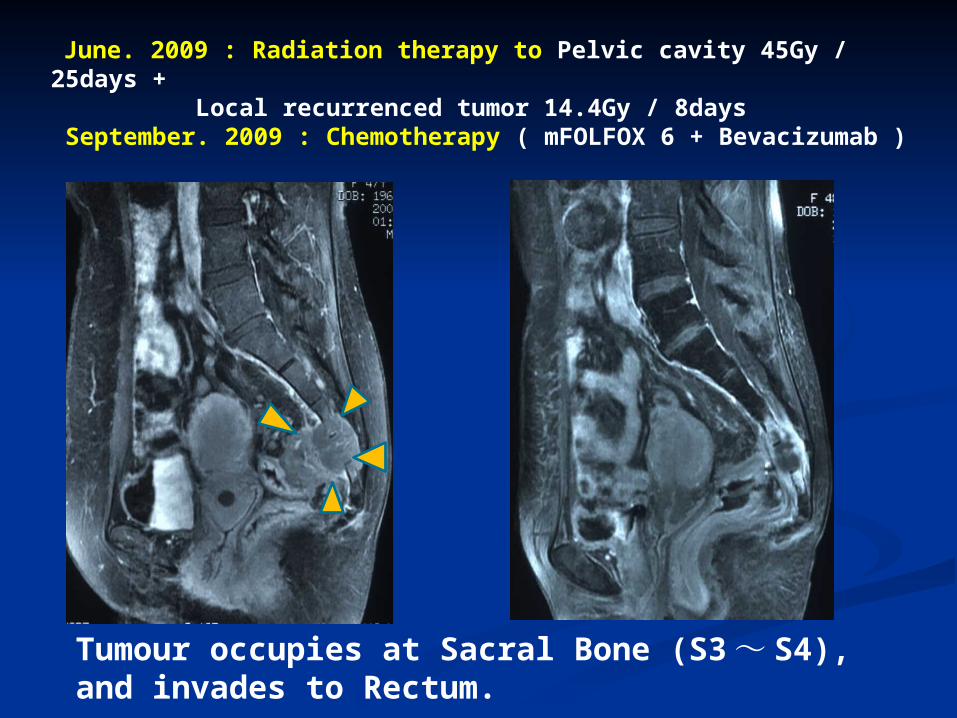
June. 2009 : Radiation therapy to Pelvic cavity 45Gy / 25days + Local recurrenced tumor 14.4Gy / 8days September. 2009 : Chemotherapy ( mFOLFOX 6 + Bevacizumab )
Tumour occupies at Sacral Bone (S3 ~ S4), and invades to Rectum.

3 March.2010: Hartman operation + Sacral bones resection(belowS3)
May.2010: Chemotherapy : XELOX 4 February.2011 : Recurrenced Sacral bone S2 April. 2011: Chemotherapy : IRIS + Pmab July. 2011: Chemotherapy : SOX + Pmab
August. 2011 : Subcutaneous abscess at residual tumour at sacral bone December. 2011 : Tumour Regrowth, Abscess Disappeared, Walk disturbance was occurred with pain at sacral nerve area5 February.2012 : BNCT at Kyoto University Reactor

A Purpose of BNCT : Regulation of recurrenced rectal cancer in pelvic cavity by BNCTB Irradiation site : Recurrenced rectal cancer in pelvic cavity
C Boron compound : BPA400mg/kg (DIV by 150mg/kg/h x 3h, then perform irradiationD RBE CBE : ●Tumour (GTV) Dose : 30 > Gy-eq / 5cm depth ●Normal tissue Dose : < 10 Gy-Eq ●RBE & CBE
●T/B ratio by F-BPA PET = 2.6 ( 30th Jan. 2012 )
Boron compound, Irradiation ray
Tumour Skin Normal nerve Oral mucosa
BSH 2.5 0.8 0.37 0.3BPA 3.8 2.5 1.35 4.9
Neutron 3.0 3.0 3.0 3.0
Γ ray 1.0 1.0 1.0 1.0

fromBeam
port
From Beam port (Tumour)
Normal mucosal neutron flux (5Gy-Eq/hr)
Tumour neutron flux (5Gy-Eq/hr)
Two dimensional distribution of neutron flux (0cm)
BNCT position
16 cm
14 cm

Red : Tumour, Blue : Small Intestine, Green : Caudal nerve, Purple:Urinary Bladder
Urinary Bladder
Small Intestine
Caudal Nerve
Neutron Dosimetry
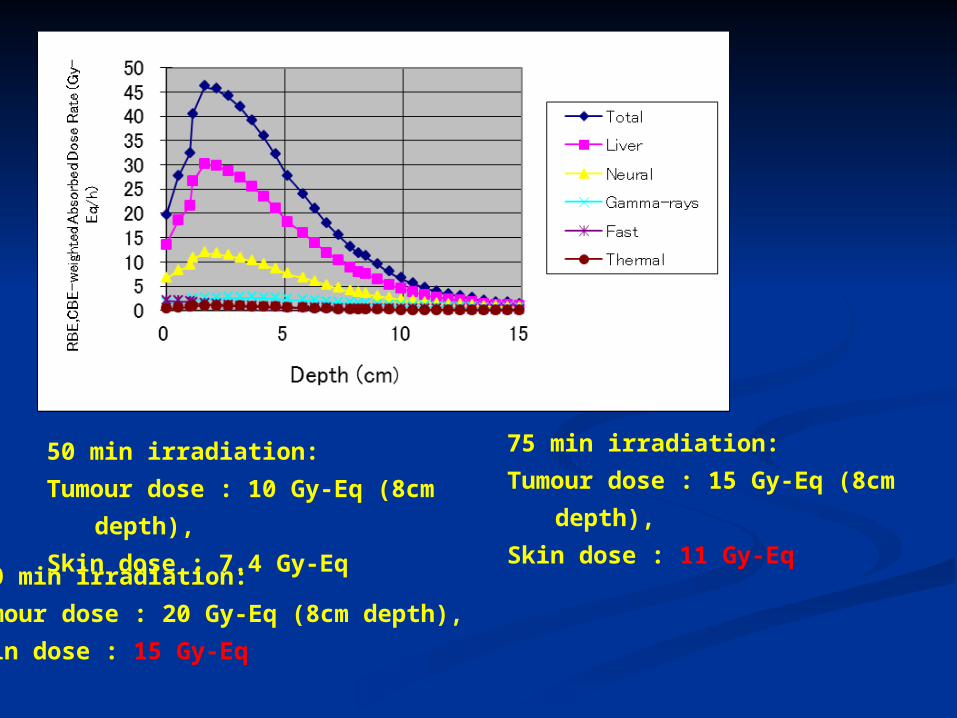
50 min irradiation:
Tumour dose : 10 Gy-Eq (8cm
depth),
Skin dose : 7.4 Gy-Eq
75 min irradiation:
Tumour dose : 15 Gy-Eq (8cm
depth),
Skin dose : 11 Gy-Eq100 min irradiation:
Tumour dose : 20 Gy-Eq (8cm depth),
Skin dose : 15 Gy-Eq

Tumour dose ( 8cm depth ) was estimated to 15Gy-Eq, so iradiation time was
decided to 69 minutes.
Tumour dose was estimated to 54Gy-Eq at 1.8cm depth, and 35Gy-Eq at 5cm
depth. The dose of 90% tumour volume is more than 20Gy-Eq,
Maximum tumour dose is 59Gy-eq.
Surface skin dose was estimated to 10Gy-Eq.
Maximum dose : Caudal Nerve : 8.9Gy-eq, Small intestine : 7.3Gy-eq, Urinary
bladder : 4.3Gy-eq
BPA( 400mg/kg DIV before 3hr )
10BTumour conc.: 56.7ppm
Blood, SkinMucosa, Nerve: 27ppm

Kyoto University Research Reactor (KUR)

7th. Feb.2012BNCT
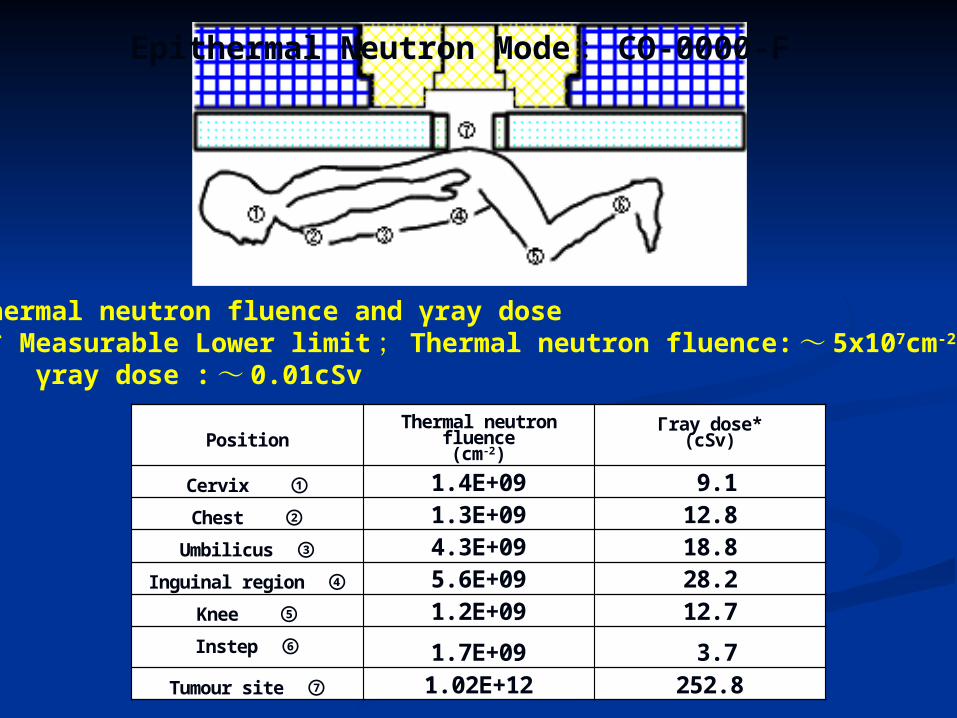
Epithermal Neutron Mode : CO-0000-F
Thermal neutron fluence and γray dose * Measurable Lower limit ; Thermal neutron fluence: ~ 5x107cm-2, γray dose : ~ 0.01cSv
Position Thermal neutron fluence(cm-2)
Γray dose*(cSv)
Cervix ① 1.4E+09 9.1 Chest ② 1.3E+09 12.8
Umbilicus ③ 4.3E+09 18.8 Inguinal region ④ 5.6E+09 28.2
Knee ⑤ 1.2E+09 12.7 Instep ⑥ 1.7E+09 3.7
Tumour site ⑦ 1.02E+12 252.8

There was no adverse event and side effects by BNCT.The walk disturbance and pain at sacral nerve area were especially improved at 1 month after BNCT.The tumour was not regrowth (Stable Disease) in size at 2 months after BNCT.
2nd Feb. 2012. Before BNCT
April. 2012
Marker 1/11 3/21 4/4CEA 2.3 1.6 2.1CA19-9 10.7 11.0 9.9

We performed the chemotherapy (SOX + BV) in followed up periods on BNCT. The tumour size was decleased at 4 months after BNCT with chemotherapy compared with the tumour size at preBNCT.The tumour size was increased at 7 months after BNCT, and subcutaneous abscess is reoccured.
2012 年 2 月 BNCT 前
2012 年 6 月 2012 年 9 月

[ Case 2 ] 56y.o. Female, Rectal Cancer Clinical course1 December. 2006 : Low anterior resection Pathological findings: Adenocarcinoma of the rectum, ( Type2, tub2, se, ly2, v2, n1 )2 July. 2007: Hartman operation to recurrence lesion3 February.2008 : Local recurrence in pelvic cavity ( presacral bone area)4 April. 2008 : Radiation therapy to Pelvic cavity 57.8Gy / 25days5 January.2009: Local recurrence in pelvic cavity & Invasion to Sacral bone 6 February.2009: Chemotherapy ( FOLFORI )7 December. 2010 : Chemotherapy ( CPT-11 + Arbitax )8 April. 2012 : Tumour growth

2012.5.24 BPA-PETTmax/Bmean = 2.9
Recurrenced Rectal Cancer : Local recurrenced lesion was recognized at the pre-fat tissue of sacral bone after Hartomann’s operation. The tumour size was increased. No liver metastasis.

A Purpose of BNCT : Regulation of recurrenced rectal cancer in pelvic cavity by BNCTB Irradiation site : Recurrenced rectal cancer in pelvic cavity
C Boron compound : BPA400mg/kg (DIV by 150mg/kg/h x 3h, then perform irradiationD RBE CBE : ●Tumour (GTV) Dose : 30 > Gy-eq / 5cm depth ●Normal Skin Dose : < 8 Gy-Eq, Normal Mucosal Dose(Small intestine) : < 7 Gy-Eq ●RBE & CBE
●T/B ratio by F-BPA PET = 2.9 ( 24th May 2012 )
Boron compound, Irradiation ray
Tumour Skin Normal nerve Oral mucosa
BSH 2.5 0.8 0.37 0.3BPA 3.8 2.5 1.35 4.9
Neutron 3.0 3.0 3.0 3.0
Γ ray 1.0 1.0 1.0 1.0

照射体系
照射方向 照射孔から
照射孔から ( 腫瘍 )
二次元線量率分布 (-2.0cm)
神経線量 (×2Gy-eq/h)
腫瘍線量 (×5Gy-eq/
h) 小腸線量 (×5Gy-eq/h)

59 min irradiation:
Tumour dose : 30 Gy-Eq (5cm depth), Skin dose : 8.3 Gy-Eq
Small Intestine dose : 3.6Gy-eq, Kidney : 1.5Gy-eq
81 min irradiation:
Tumour dose : 15 Gy-Eq (8cm depth), Skin dose : 11.4 Gy-Eq
Small Intestine dose : 5.0 Gy-eq, Kidney : 2.1 Gy-eq
107 min irradiation:
Tumour dose : 20 Gy-Eq (8cm depth), Skin dose : 15.0 Gy-Eq
Small Intestine dose : 6-6 Gy-eq, Kidney : 2.8 Gy-eq
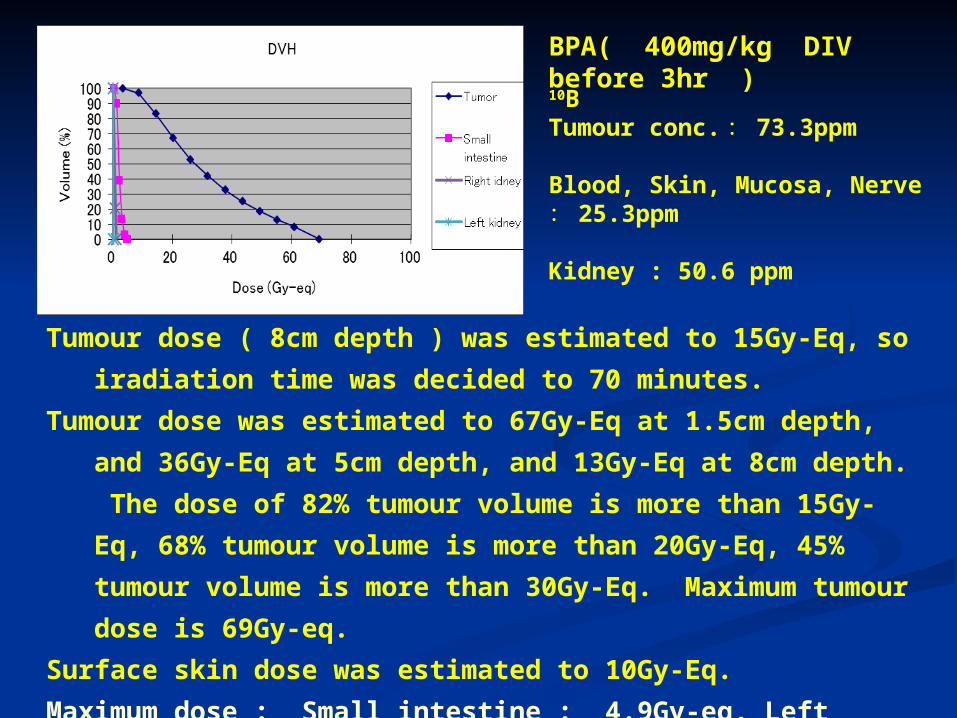
BPA( 400mg/kg DIV before 3hr )
10BTumour conc. : 73.3ppm
Blood, Skin, Mucosa, Nerve: 25.3ppm
Kidney : 50.6 ppm
Tumour dose ( 8cm depth ) was estimated to 15Gy-Eq, so iradiation time was
decided to 70 minutes.
Tumour dose was estimated to 67Gy-Eq at 1.5cm depth, and 36Gy-Eq at 5cm
depth, and 13Gy-Eq at 8cm depth. The dose of 82% tumour volume is
more than 15Gy-Eq, 68% tumour volume is more than 20Gy-Eq, 45%
tumour volume is more than 30Gy-Eq. Maximum tumour dose is 69Gy-
eq.
Surface skin dose was estimated to 10Gy-Eq.
Maximum dose : Small intestine : 4.9Gy-eq, Left Kidney : 1.2Gy-eq, Right
Kidney 0.2Gy-eq, Caudal Nerve : 9.5Gy-eq, Urinary bladder : 10.3Gy-eq

Position Thermal neutron fluence(cm-2)
Γray dose*(cSv)
Cervix ① 1.8E+09 5.9 Chest ② 9.4E+08 11.8
Umbilicus ③ 1.4E+09 19.6 Inguinal region ④ 1.3E+09 23.5
Knee ⑤ 8.2E+08 12.5 Instep ⑥ 3.5E+09 10.4
Tumour site ⑦ 1.38E+12 268.8
Epithermal Neutron Mode : CO-0000-F
Thermal neutron fluence and γray dose * Measurable Lower limit ; Thermal neutron fluence: ~ 5x107cm-2, γray dose : ~ 0.01cSv

BNCT 線量シミュレーション 2012/06/11
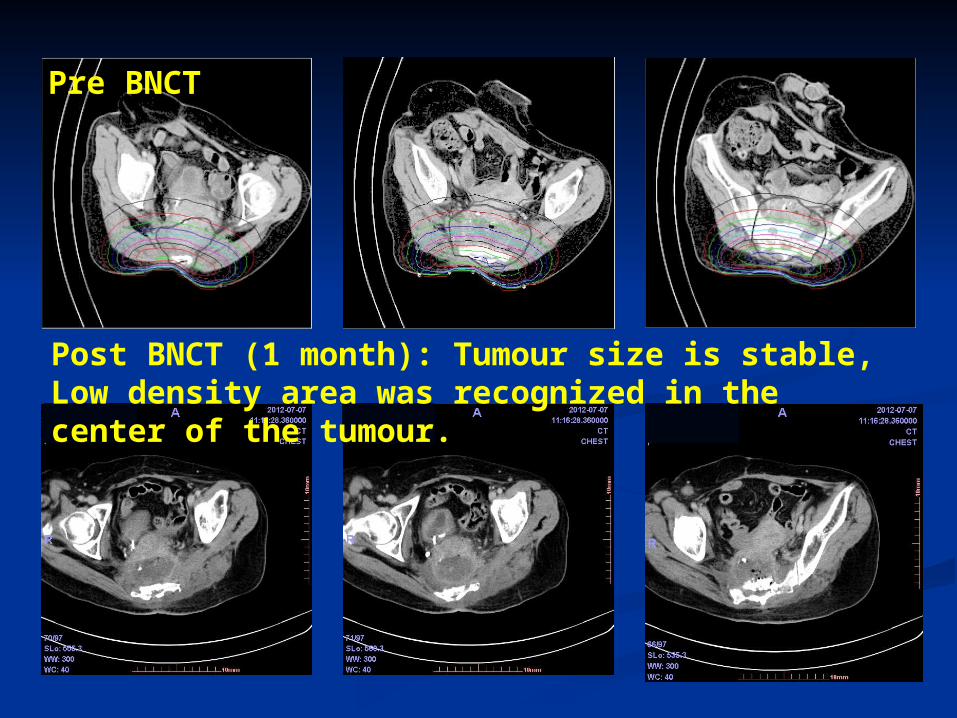
Post BNCT (1 month): Tumour size is stable, Low density area was recognized in the center of the tumour.
Pre BNCT

Post BNCT (2 month): Tumour size is stable, Low density area was recognized in the center of the tumour. Invasion was recognized to the surrounding tissue.
Post BNCT (3 month): Tumour size is stable, Low density area was recognized in the center of the tumour. Invasion was recognized to the surrounding tissue.

Post BNCT (1 month)
Post BNCT (1 week)
There was no skin necrosis.

Summary 1. We hope to apply the BNCT to the treatments for recurrenced metastatic cancer in gastro-intestinal legions on
one of the intensive combinational cancer therapies.
2. We have reported the pilot clinical studies of BNCT to and locally recurrenced tumour of rectal cancer. We performed BNCT with safety manner with no adverse event and side effects, and it is very impressive that we aquired the suppression effects.
3. We recognized the enhanced effect of targeted molecular therapy after BNCT. This result was speculated that the cancer cells were damaged by BNCT, and the cytotoxic effect was increased by targeted molecular therapy.

Summary (continued)4. These patients showed the recovery of quality of life (QOL) after BNCT. In Case 1, the tumour volume was slightly decreased by BNCT, and the walk disturbance and pain at sacral nerve area were especially improved at 1 month after BNCT. In Case 2, the main tumour volume was suppressed (stable disease), but, surrounding tumour was invaded at 3 month after BNCT. The pain at sacral nerve area were especially improved.
5. In these BNCT, we performed the F-10BPA-PET. According to the results of Tumour / Blood ratio, we evaluated the neutron dosimetry ( Case 1 : T/B ratio = 2.6, Case 2 : T/B ratio = 2.9 ).

Summary (continued)6. We used the CBE of oral mucosa (4.9) for estimation to CBE value of small intestine. In these cases, small intestine were existed in the anterior site in the abdomen compared to the tumour lesion in CT images, so we performed the BNCT with careful consideration of maximum neutron dose to small intestine.
7. The urine in the urinary bladder / blood ratio was 10 in F-BPA PET, so we must consider the dose to mucosa of urinary bladder in the BNCT to pelvic cavity. In this BNCT studies, there was no hematuria, inflamation signs after irradiation.
8. In these cases, we would like to perform second BNCT, but we do not have any budget, so we performed only single BNCT to check the neutron capture effect.

Summary (continued)9. We had performed the pilot clnical studies of BNCT to the
gastro-intestinal cancers in safety manner. Further investigations are necessary to increase the suppressive effect by BNCT with improving ① the regulation of the body in the irradiation time, ② administration of boron compound(DIV methods, combination of BPA and BSH), etc.
10. We hope that applications of accerelated BNCT will be opened to patients of gastro-intestinal cancers (included HCC etc.), breast cancer in near future.

Conclusion
We started pilot clinical studies BNCT to the treatments for recurrenced recurrenced & metastatic cancer in gastro-intestinal legions on one of the intensive combinational cancer therapies. We hope to accumulate the BNCT treated cases to evaluate the effects of treatment in these regions.
AcknowledgementThe University of TokyoDept. of Nuclear Engineering & Management, Cooperative Unit of Medicine & Engineering, U-Tokyo Hospital
Hiroyoki Takahashi, Minoru Ono, Jun Nakajima, Yuriko Sakurai, Kikue MouriGraduate School of Agricultural and Life Science, Laboratory of Veterinary Surgery
Ryohei Nishimura, Masashi Yanagawa, Tomoya IIzukaDept. of Molecular Pathology, Faculty of Medicine
Yasuyuki Morishita
Shin-Yamate Hospital, Anti-Tuberculosis AssociatonDept. of Surgery & Radiology Masazumi Eriguchi, Shoji Maruyama, Ryo Hatae, Morimasa Sekiguchi, Kazuyuki OyamaKojin-kai Medical City East Hospital, Dept. of Surgery Syushi Higashi, Koji SeguchiMiyakonojo Medical Association Hospital, Dept. of Radiology Ichiro Ikushima

AcknowledgementResearch Reactor Institute, Kyoto Universit Koji Ono, Akira Maruhashi, Shinichiro Masunaga, Minoru Suzuki, Yoshinori Sakurai, Tomoko Kinashi, Hiroki Tanaka, Natuko Kondo, Masaru NarabayashiJyuntendo University
Atsuko ShinoharaNihon University
Koichi Ogura, Syouji MikadoMitsubishi Chemical MedienceCorporation
Ryouji Mizumachi, Yuji MurataInstitute for Atomic Energy, Rikkyo University
Hisao Kobayashi Nikken Chemicals Co. Ltd.
Toshio MatsumotoDept. of Surgery, Keiai-kai Hoyo Hospital
Yasumasa NonakaSatukidai Hospital
Yoshitaka Furuya
