clinical evaluation of multifocal electroretinogram. / neurosa res. 1993; 35:530-539. 11. kadomalsu...
TRANSCRIPT

2146 Investigative Ophthalmology & Visual Science, September 1995, Vol. 36, No. 10
those agents are suggested to have therapeutic poten-tial, the degree of anatomic rescue of photoreceptorsis variable among agents. Further studies are war-ranted to assess survival-prornoting agents for the pres-ervation of retinal function, whereby recording ofERG responses provides a relatively simple, fast, reli-able test.
Key Words
basic fibroblast growth facotr (bFGF), electroretinographicresponse, light damage, midkinc, rat, retinal degeneration
References
1. Faktoiovich EG, Steinberg RH, Yasumura D, MatthesMT, LaVail MM. Phoioreceptor degeneration in in-herited retinal dystrophy delayed by basic h'broblasigrowth factor. Nature. 1990; 347:83-86.
2. Faktorovich EG, Steinberg RH, Yasumura D, MatthesMT, LaVail MM. Basic fibroblast growth factor andlocal injury protect photoreceptors from light damagein the rat. / Nmrosci. 1992; 12:3554-3567.
3. LaVail MM, Unoki K, Yasumura D, Matthes MT, Yanu-copoulos GD, Steinberg RH. Multiple growth factors,cytokines and neurotrophins rescue photoreceptorsfrom the damaging effects of constant light. Proc NailAmd Sri USA. 1992;89:11249-11253.
4. Unoki K, LaVail MM. Protection of the retina fromischemic injury by BDNF, CNTF and bFGF. Invest Oph-thalmol Vis'Sa. 1994;35:907-915.
5. Unoki K, Ohba N, Arimura H, Muramat.su H, Mura-matsu T. Rescue of photoreceptors from the damag-
ing effects of constant light by midkine, a retinoicacid-responsive gene product. Invest Ophthalviol Vis Sri.1994; 35:4063-4068.
6. Muramat.su H, Muramat.su T. Purification of recombi-nant midkine and examination of its biological activi-ties: Functional comparison of new heparin bindingfactors. Biochem Biophys Res Commun. 1991; 177:652—658.
7. Watanabe I, Toyama K. The effects of anesthetics onthe ERG and EOG. Doc Ophthalmol Proc Ser.1978; 15:21-30.
8. Watanabe I, Toyama K. Luminance-duration relation-ship in the electroretinogram. Ada Soc Ophthalmol/pn'.1981; 85:1449-1455.
9. Nurcombe V, Fraser N, Herlaar E, Heath JK. MK, apluripotential embryonic cell-derived neuroregula-tory factor. Develofmient. 1992; 116:1175-1183.
10. Michikawa M, Kikuchi S, Muramatsu T, MuramatsuH, Kim SU. Retinoic acid responsive gene product,midkine (MK), has neurotrophic functions for mousespinal cord and dorsal root ganglion neurons in cul-ture. / Neurosa Res. 1993; 35:530-539.
11. KadomaLsu K, Huang RP, Suganuma T, Murata F,MuramaLsu T. A retinoic acid responsive gene MKfound in the teratocarcinoma system is expressed inspatially and temporally controlled manner duringmouse embryogenesis. / Cell Biol. 1990; 110:607-616.
12. Gaur VP, De Lceuw AM, Milam AH, Saari JC. Localiza-tion of cellular retinoic acid-binding protein to ama-ci ine cells of rat retina. Kxp Eye Res. J990; 50:505-511.
13. Edwards RB, Adlcr AJ, Dev S, Claycomb RC. Synthesisof retinoic acid from retinol by cultured rabbit Mullercells. Kxp Eye Res. 1992;54:481-490.
Clinical Evaluation of MultifocalElectroretinogramMineo Kondo, Yozo Miyake, Masayuki Horiguchi,Satoshi Suzuki, and Atsuhiro Tanikawa
Purpose. To compare the multifocal electroretinogram(ERG) system to conventional gan/feld and focal ERGsobtained from patients with known retinal diseases toassess its clinical applicability.
Methods. A multi-input system analysis was used to ex-plore the field topography of ERG responses to localluminance modulation in patients with retinitis pig-
i'utm the Depaitme-nt oj Ophthalmology, Naffrya Vnwn\ity School oj Medicine,Ntiffiyn. JapanSubmitted fin publutUion Dnrmlm 22, 1994, unused May I. 1995. wiejited May3. 1995.I'uyjmetnry nitnest (alegary i\Reprint ieque\t\ Mineo Kondo, Drpaitmenl oj Ophthalmology, Nagayn Unnieiut)School oj Medicine, 65 Tsiinimn-tho. Shmua-ku, Naffiya 466, Japan
mentosa, pencentral pigmentary retinal dystrophy,branch retinal arterial occlusion, or idiopathic macularhole.
Results. The dysfunctional areas measured by multifocalERG were compatible with those assumed by combinedfindings of gan/feld and focal ERGs. However, the waveshapes of multifocal ERG in the retina with arterialocclusion differed from those of conventional focalERG, suggesting that the negative and positive deflec-tions shown in the first-order kernel of multifocal ERGmay not correspond to conventional a- and b-waves ofERG.
Conclusions. The multifocal ERG system is available forelectroretinographic field mapping at the clinical level.Invest Ophthalmol Vis Sci. 1995;36:2146-2150.
Although many authors1"'1 have applied focal elec-troretinogram (ERG) to detect focal retinal abnormal-ities, the averaging technique used to improve thesignal-to-noise ratio permits testing of a single local
Downloaded From: https://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933182/ on 08/29/2018

Reports 2147
area at a time. Recently, Sutter et al' introduced a"multifocal ERG system" that can stimulate multipleretinal areas simultaneously and detect each responseindependently by applying the multi-input systemanalysis technique.1' Using this system, they have suc-ceeded in constructing an "ERG topography" of fineresolution. The technique, however, is in a prelimi-nary stage, and few studies have evaluated the systemfor clinical application.' It is important to determinewhether this system may be clinically applicable. Theauthors have compared the results obtained bymultifocal ERG to those acquired by ganzfcld and fo-cal ERGs from patients with known retinal diseases.
SUBJECTS AND METHODS. Methods. The sys-tem used for recording multifocal ERG has been de-scribed by Sutler et al.' The stimulus matrix consistedof 103 hexagonal elements displayed on a CRT colormonitor (Sony [Tokyo, Japan J GDM 2038) driven ata 75-Hz frame rate. These hexagons were scaled witheccentricity to elicit approximately equal signal ampli-tude at all locations (Fig. 1A). At a viewing distanceof 27 cm, the radius of stimulus array subtended ap-proximately 25° high and 30° wide. Each hexagon wasindependently alternated between black and white ac-cording to a pseudorandom sequence called binarym-sequence:>(> at a rate of 75 Hz. This stimulation tech-nique allowed extraction of the response from eachstimulus element. The high luminance was 138.0 cd/m2, and the low luminance was 3.5 cd/m2, resultingin a mean screen luminance of approximately 70.8cd/m2. A small red fixation spot was placed at thecenter of the stimulus matrix. A Burian-Allen bipolarcontact lens electrode was used for signal derivation,and a ground electrode was attached to the carlobe.Subjects' pupils were fully dilated with a combinationof 0.5% tropicamidc and 0.5% phcnylephrine hydro-chloride. The opposite eye was occluded. After sub-jects were optically corrected to their best visual acu-ities, they were asked to look at the fixation spot. Thesignal amplification was 50,000, and the filter settingwas bandpass 6 Hz to 100 Hz (Nihon Koden [Tokyo,Japan] AB-620G). An artifact rejection technique wasused.'*' The total recording took 4 minutes and weredivided into eight segments. Local responses were ex-tracted from the raw data by computating cross-corre-lation between the m-scquence and the response cy-cle.1' The amplitude of each local response was esti-mated as the dot product between the normalizedresponse template and each local response (scalarproduct method).' Electroretinographic topographieswere constructed to visualize the retinal response den-sity (amplitude per unit retinal area). The array oflocal responses and ERG topography were plotted inthe same manner as the visual field.
B
A-- -/— -A— A - A — A - ~
A ~ A— vV- A— A— A— A— A— -A—A-- A— A— v\— NA— A— -A— A— •/ A
A— A— A — ,A— ^— v w A — ^ ^ ^ _ ^ ^ ^ _A— A— 1[>A— A - v w A ~ A — A— A— A—
^- A — vv_ A — A - A - w - A— A— A— A—,/W- ,/\~ , / w A — </v- J V - A— A— A— A—
A - A - A - v - A - w - A — A— A— A— A—A— A— A ~ A— vw- vw- A — A— A— A—
A - A— A— A— A— A-- A— A— A—A— A— A— A— A— A—
FIGURE l. (A) Stimulus array of"103 hexagonal elements. (B)Array of 103 local responses of multifocal electroretinogramand (C) electroretinogram topography obtained from theleft eye of a normal subject. A low amplitude was seen atthe blind spot (arroiu).
Our system for recording the focal ERG has beendescribed.'1 Briefly, the subject's pupils were fully di-lated; an infrared television camera was positioned tomonitor the exact locus of stimulation on the fundusduring recordings, and a Burian-Allen bipolar con-tact lens electrode permitted clear observation of thefundus on the television monitor. The intensity of thewhite stimulus light (4°, 5°, 10°, 15° diameter) and thebackground light were 3.2 and 2.2 scotopic trolands(log), respectively. The ERG was recorded with 5-Hzrectangular stimuli for 100 msec with the light on and100 msec with the light off. A total of 512 responseswere averaged by a signal processor.
Ganzfeld ERGs were recorded according to a pre-viously described method.8 After 30 minutes of darkadaptation, a rod (scotopic) ERG was recorded witha blue light at an intensity of 5.2 X 10":< cd • m"2 • sec"1.
Downloaded From: https://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933182/ on 08/29/2018

2148 Investigative Ophthalmology & Visual Science, September 1995, Vol. 36, No. 10
A cone-rod mixed single bright-flash (bright white)ERG was recorded with a white stimulus at an intensityof 44.2 cd • m"2 • sec"1. A cone (photopic) ERG and a30-Hz flicker ERG were recorded with a white stimulusintensity of 4 cd-m~a*sec"' and 0.9 cd-m~2-sec~',respectively, under a background illumination of 21foot-lamberts. Four responses and 16 responses wereaveraged to record cone ERG and 30-Hz flicker ERG,respectively.
Subjects. Fifteen normal subjects (ranging in agefrom 21 to 63 years) and four patients with eitherretinitis piginentosa, pericentral pigmentary retinaldystrophy, branch retinal arterial occlusion, or idio-pathic macular hole were examined. The research fol-lowed the tenets of the Declaration of Helsinki. In-formed consent was obtained from all subjects andpatients after the nature and possible consequencesof the study were explained.
RESULTS. Normal Subjects. An array of 103 lo-cal responses of multifocal ERG and ERG topographyobtained from the left eye of a normal subject (24-year-old woman) are shown on Figures IB and 1C,respectively. A small response was seen at the blindspot (arrow), and this residual response can be ex-plained by die fact that the element size of the hexa-gon at the blind spot is larger than the blind spot.
Ten continuous recordings of multifocal ERGwere obtained from a normal subject to investigatethe reproducibility of this technique. Mean responsedensities (±1 SD) at two areas of central hexagon and15° temporal field hexagon (including the blind spot)were 11.4 ± 1.7 nV/deg-deg and 1.4 ± 0.3 nV/deg-deg, respectively, suggesting fine reproducibility. In-tersubject variability of multifocal ERG was investi-gated in 15 normal subjects at the same two areasmentioned. Mean response densities (±1 SD) were12.2 ± 2.7 nV/deg-deg and 1.7 ± 0.5 nV/deg-deg,respectively.
Patients. Retinitis pigmentosa. A 39-year-old womanhad a 2-year history of peripheral visual disturbance.Visual acuity was 1.5 in both eyes. Goldmann perime-try revealed constriction of die visual field (Fig. 2,top), and the fundus examination disclosed attenu-ated arteries, scattered pigmentary changes, and apale disc. Although ganzfeld ERG was nondetectablein rod and cone components (Fig. 3A), focal ERGwith 5°-, 10°-, and 15°-diameter spots at the fovea waswell preserved (Fig. 3B). The result of multifocal ERGshowed markedly reduced responses in the peripheralfield but relatively preserved responses in the centralfield (Fig. 4).
Pericentral pigmentary retinal dystrophy. A 47-year-oldwoman had a 3-year history of bilateral paracentralvisual loss. Visual acuity was 1.0 in both eyes. Gold-
Case 1
Case 2
Case 3 —
FIGURE 2. Goldmann perimetries in the left eye of patient 1(top), patient 2 (middle), and patient 3 (bottom).
mann perimetry showed annular scotoma (Fig. 2, mid-dle), and the fundus examination disclosed depig-mented spots along the vascular arcade. There wereneither attenuated arteries nor pigmentary changes.Focal macular ERG within 15° was preserved (Fig. 3B),but ganzfeld ERG was moderately decreased in coreand rod components (Fig. 3A). Multifocal ERG re-vealed reduced responses in the area approximatelycorresponding to the annular scotoma presented byGoldmann perimetry (Fig. 4).
Branch retinal artery occlusion. A 51-year-old mannoticed sudden visual loss in the upper visual field ofthe left eye. Visual acuity was 1.5 in both eyes. Gold-mann perimetry revealed a small superior scotoma inthe left eye (Fig. 2, bottom), and the fundus examina-tion disclosed a branch occlusion in the inferotem-poral artery of the left eye. Whitening retinal edemawas seen along the artery. Ganzfeld ERG was normal
Downloaded From: https://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933182/ on 08/29/2018
Reports 2149
Ganzfeld ERG
Case 1 Case 2 Case 3
Scotopic
Bright —iWhilo •
Photopic
J-
J-
_ ] , * .
B
10'
Focal ERG
Case 1 Case 2
A
Case 3
Upper
(Normal)
Lower
(Involved)
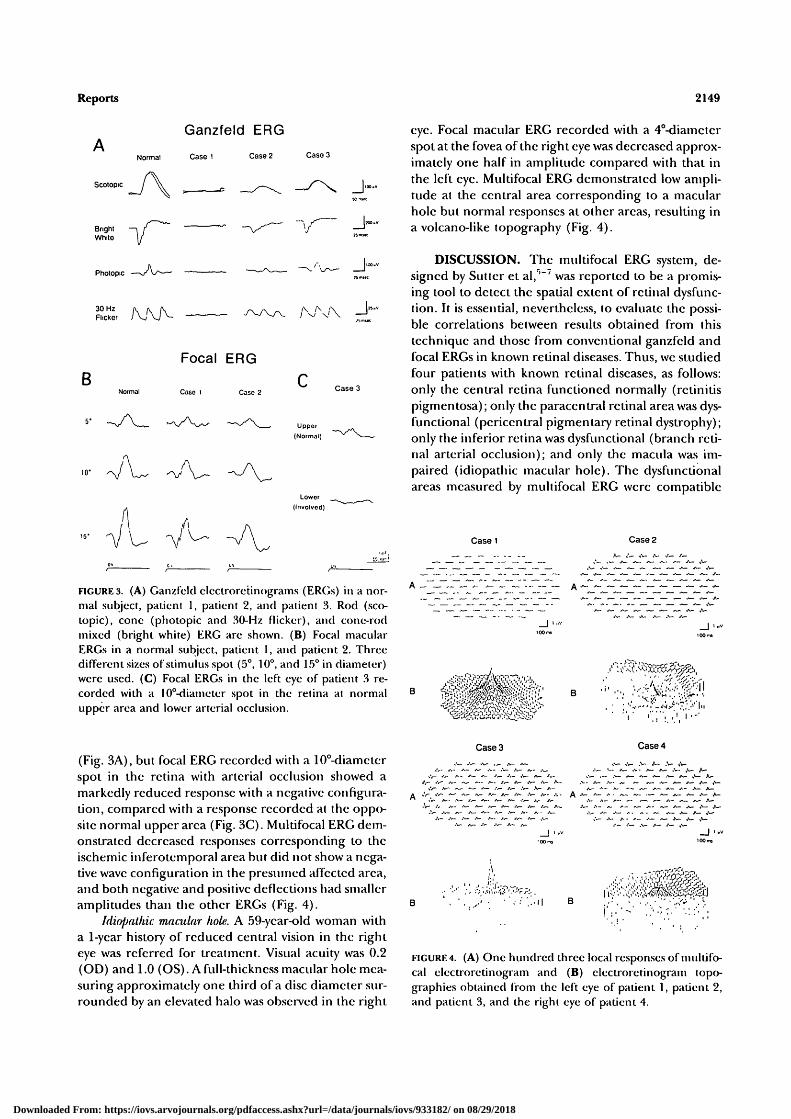
FIGURES. (A) Ganzfeld clectroretinograms (ERGs) in a nor-mal subject, patient 1, patient 2, and patient 3. Rod (sco-topic), cone (photopic and 30-Hz flicker), and cone-rodmixed (bright white) ERG are shown. (B) Focal macularERGs in a normal subject, patient 1, and patient 2. ThreedifFerentsi7.es of stimulus spot (5°, 10°, and 15° in diameter)were used. (C) Focal ERGs in the left eye of patient 3 re-corded with a 10°-diameter spot in the retina at normalupper area and lower arterial occlusion.
(Fig. 3A), but focal ERG recorded with a 10°-diamclerspot in the retina with arterial occlusion showed amarkedly reduced response with a negative configura-tion, compared with a response recorded at the oppo-site normal upper area (Fig. 3C). Multifocal ERG dem-onstrated decreased responses corresponding to theischemic inferotemporal area but did not show a nega-tive wave configuration in the presumed affected area,and both negative and positive deflections had smalleramplitudes than the other ERGs (Fig. 4).
Idiopalhic macular hole. A 59-ycar-old woman witha 1-ycar history of reduced central vision in the righteye was referred for treatment. Visual acuity was 0.2(OD) and 1.0 (OS). A full-thickness macular hole mea-suring approximately one third of a disc diameter sur-rounded by an elevated halo was observed in the right
eye. Focal macular ERG recorded with a 4°-diamctcrspot at the fovea of the right eye was decreased approx-imately one half in amplitude compared with that inthe left eye. Multifocal ERG demonstrated low ampli-tude at the central area corresponding to a macularhole but normal responses at other areas, resulting ina volcano-like topography (Fig. 4).
DISCUSSION. The multifocal ERG system, de-signed by Sutter et al,'"' was reported to be a promis-ing tool to detect the spatial extent of retinal dysfunc-tion. It is essential, nevertheless, to evaluate the possi-ble correlations between results obtained from thistechnique and those from conventional ganzfcld andfocal ERGs in known retinal diseases. Thus, we studiedfour patients with known retinal diseases, as follows:only the central retina functioned normally (retinitispigmentosa); only the paracentral retinal area was dys-functional (pcriccntral pigmentary retinal dystrophy);only the inferior retina was dysfunctional (branch reti-nal arterial occlusion); and only the macula was im-paired (idiopathic macular hole). The dysfunctionalareas measured by multifocal ERG were compatible
Case 1 Case 2
/- „•— A -
Case 3
'"', I'-J-J.-.1
i I . I I
Case 4
>_ , ^ / . . ,v-
• ' • - • ? ' . • . ' • -
! , ' ' • • •
i'li..
,v- „•- A-
^ < - f - f -
A -V:.V- /.
.-.- A -
FIGURE 4. (A) One hundred three local responses of multifo-cal electroretinogram and (B) electroretinogram topo-graphies obtained from the left eye of patient 1, patient 2,and patient 3, and the right eye of patient 4.
Downloaded From: https://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933182/ on 08/29/2018

2150 Investigative Ophthalmology & Visual Science, September 1995, Vol. 36, No. 10
with those assumed by combined findings of ganzfeldand focal ERGs.
The technique also offered high-resolution map-ping of the retina in a very short time, which hadnever been achieved by conventional averaging ERGtechniques. Some problems must be considered, how-ever, when mapping the retina. The intersubject vari-ability of multifocal ERG may limit its sensitivity indetecting slightly impaired lesions. Therefore, an age-matched normal control is needed to evaluate theamplitude because a significant inverse correlation be-tween amplitude of local ERG response and age hasbeen reported. * Another problem is that steady eyefixation may be difficult to achieve in a patient withpoor visual acuity because of the inability to see thecentral fixating point and eye movement may result inconsiderable noise. For such patients, Sutter (personalcommunication) has suggested various fixation aids tobe displayed on the television monitor (for example, asmall cross placed at the center or eccentric spokes).A final problem is the analysis of each wave shaperecorded simultaneously from multiple retinal loca-tions using a high-frequency random stimulus. Themultifocal ERG discussed in this report (first-orderkernel) can be considered as the mean response to alocal flash. As presented in a normal subject (Fig. IB),it consists of a negative deflection followed by a posi-tive deflection, with a shape similar to that of conven-tional a- and b-waves. However, whether these deflec-tions have the same retinal origins as the a- and b-waves remains controversial. Because the physiologicalsubstrate of kernels is not well understood,110 compar-ing the wave shape of conventional focal ERG to thatof multifocal ERG is important. For example, in apatient with branch retinal arterial occlusion (patient3), conventional focal ERG showed a negative config-uration in the impaired retina. Although the a-wavewas preserved, the b-wavc and oscillatory potentialswere essentially absent when compared with ERG ob-tained from the upper normal retina (Fig. 3C). Thisfinding is reasonable because the retinal artery sup-plies the areas at the origin of the b-wave and oscilla-tory potentials, but the photoreceptors—the origin ofdie a-wave—are supplied by choroidal circulation. Onthe other hand, multifocal ERG in the presumablyaffected area did not show a negative configuration,and both negative and positive deflections showedsmaller amplitudes than the other ERGs. This resultsuggests that, the negative and positive deflectionsshown in the first-order kernel of multifocal ERG maynot correspond to conventional a- and b-waves of ERG.
Therefore, further studies are needed to identify theorigin of each component of multifocal ERG.
Key Words
electroretinogram, focal, ganzfeld, multifocal, topography
Acknowledgments
The authors thank Shinobu Awaya, MD, of the Ophthalmol-ogy Department, Nagoya University, for his revision of themanuscript. They also thank Erich E. Sutter, PhD, of theSmith-Kcttlewell Eye Research Institute (San Francisco,CA) for help constructing the multifocal electroretinogramsystem and valuable advice; Shiro Usui, PhD, of the Informa-tion and Computer Sciences Department, Toyohashi Uni-versity of Technology, for his helpful comments on themanuscript; and Eiichiro Nagasaka, and Hidetaka Kudo ofthe Tomey Corporation (Nagoya, Japan) for their excellenttechnical help.
References
1. Jacobson JH, Kawasaki K, Hirose T. The human elec-troretinogram and occipital potential in response tofocal illumination of the retina. Invest Ophthalmol VisSa. 1969; 8:545-556.
2. Biersdorf WR, Diller DA. Local electroretinogram inmacular degeneration. AmJ Ophthalmol. 1969; 68:296-303.
3. Birch DO, Fish GE. Focal cone electroretinograms:Aging and macular disease. Doc Ophthalmol. 1988; 69:211-220.
4. Miyake Y, Shiroyama N, Ota I, Horiguchi M. Localmacular electrorctinographic responses in idiopathiccentral serous chorioretinopathy. Am J Ophthalmol.1988; 106:546-550.
5. Sutter EE, Tran D. The field topography of ERG com-ponents in man: I: The photopic luminance response.Vision lies. 1992;32:433-446.
6. Sutter EE. A deterministic approach to nonlinear sys-tems analysis. In: Pinter RB, Nabet B, eds. NonlinearVision. Cleveland, OH: CRC Press; 1992:171-220.
7. Sutter EE, Dodsworth-Feldman B, Haegerstrom-Portnoy G. Simultaneous multifocal ERGs in diseasedretinas. ARVO Abstracts. Invest Ophthalmol V?.s Sa.1986; 27:301.
8. Miyake Y, Horiguchi M, Terasaki H, Kondo M. Sco-topic threshold response in complete and incompletetypes of congenital stationary night blindness. InvestOphthalmol Vis Sa. 1994;35:3770-3775.
9. Larkin RM, Klein S, Ogden TE, Fender DH. Nonlin-ear kernels of the human ERG. liiol Cyhern.1979;35:145-160.
10. Ogden TE, Larkin RM, Fender DF, Clcary PE, RyanSJ. The use of non-linear analysis oi the primate ERGto detect retinal dysfunction. Exp Eye Res. 1980;31:381-388.
Downloaded From: https://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933182/ on 08/29/2018