clinical decisions in cataract surgery · adapted from fda clinical data: ... –sia (surgical...
TRANSCRIPT

h

Clinical Decisions in Cataract Surgery
H. Jellie MD FRCS, June CE 2016

Financial Interest Disclosure
• I have provided surgical services at TLC Waterloo since 1999
• I do not have any financial interest or receive and remuneration from any company that distributes ophthalmic products, devices or drugs

Beginning of Modern Lens Based Surgery

Cataract Surgery Confusion
• What is a cataract, when does it start?
• Who defines what a cataract is?
• Where is the line between cataract surgery and refractive surgery?

SU121259
The Changing Face of Cataract Surgery
- Large, rapidly growing demographic
- Educated, financially secure
- Increased life expectancy
- Longer working careers
- Demand high quality vision (reading, distance,
night vision)
- New requirement for near vision (computers)
- Unwilling to compromise active lifestyle
- Embracing demand driven healthcare
The Baby Boomer Generation
3

SU121259
The Need for Improvement
5
Adapted from FDA Clinical Data: Crystalens and Wavelight® Trials


Ophthalmology Times April 11 2015, by Dr. Mark Packer
1) Refractive Lens Exchange means that the primary purpose of surgery is to reduce or eliminate the need for eyeglasses.2) Cataract Surgery means that the primary purpose of surgery is to improve functional vision impaired by lenticular opacification. 3) Refractive Cataract Surgery means that the primary purpose of surgery is to improve functional vision impaired by lenticular opacification and the secondary purpose of surgery is to reduce or eliminate the need for eyeglasses. 4) Dysfunctional Lens Surgery means that the primary purpose of surgery is to improve functional vision impaired by lenticular aberrations.5) Refractive Dysfunctional Lens Surgery means that the primary purpose of surgery is to improve functional vision impaired by lenticular aberrations and the secondary purpose of surgery is to reduce or eliminate the need for eyeglasses.

Steps of Phaco
• Patient selection
• Preoperative assessment and counseling
• Incision
• Rhexis
• Hydrodissection
• Phaco / Cortex removal
• IOL Insertion

My Routine Case

Preop Cataract Surgery Considerations
• Preop Factors– Surface– BMD, Stromal or Endothelial Dystrophies
• Previous Refractive Surgery– Flap related issues– Radial Keratotomy– Hyperopia vs Myopia
• Retinal Abnormalities– Diabetes Stabilization– ARMD– Epithelial membranes / Lamellar holes

2 mm pterygium 3 mm pterygium

5 mm Pterygium

Salzmann Nodular Degeneration

Epithelial Ingrowth Post Lasik Trauma

Lasik flap trauma / Lamellar Transplant

Fuchs’ Corneal Dystrophy
• 62 female: R 20/50 L 20/80
• Pachs: 635/675 microns
• NS Cataract 2/4, Fuchs 2/4
• Left Cataract Sx with IOL
• 1 wk. po, 20/70, Pachs: 722
• 2 months po, CF 2 ft.
• 3 months po, Left DSAEK

Fuchs and CataractStaged or Combined Procedure
Staged
• Decreased risk for intraoperative complications
• DSAEK alone allows for easier to insert graft
• If complication with cataract surgery alone, just deal with it and come back later when eye quiet
Combined
• It only makes sense to do both if warrants surgery
• Saves patients surgery and travel time
• Patients get vision back more rapidly

Retinal Abnormalities

IOL Calculations
• Current Methods
– Spherical
• Wang-Koch
– Toric
• Other Considerations
– SIA (Surgical Induced Astigmatism)
– SA Matching (Spherical Aberration)

Spherical Calculations

Holladay 2 vs SRK/T

Toric Calculation Factors
• Incision location and SIA
– Surgically Induced Astig
• Need to know
– Correct steep meridian
– Power difference between principal meridians

Surgically Induced Astigmatism (SIA)

#1 Correct steep meridian
• Topographic axial power map is the primary instrument to determine steep meridian
• Regular astigmatism has a pair of symmetric astigmatic power lobes aligned along same meridian

#2 Correct Power Difference
• Best done using small zone autokeratometry, not Sim-Ks.
• Manual keratometer ( B&L or Javal)
• Use steep meridian from previous step and rotate drum for a second reading

Sphere IOL Power First

Alcon Toric Calculator

Barrett Toric Calculator

What is SPHERICAL ABERRATION (SA)?
In a lens system, peripheral rays are refracted more than central rays
(positive SA).
Blur interval
Correction of SA can improve contrast sensitivity, as much as 32%.1,2
Reduction of SA is optimal for visual quality when approaching 20/20.3
1.Piers et al IOVS 2004
2.Beiko JCRS 2007
3.Levy et al AJO 2005

In the Human Eye
Young Eye:
Corneal SA & Lens SA
cancels each other
Old Eye:
Corneal & Lens SA
additive
CorneaLens

With cataract surgery…
Cataract removed:
Left with + ve Corneal SA
Intraocular lens implant (IOL):
If matching IOL’s SA with
corneal SA – can cancel each
other!

Aspheric IOLs
Tecnis Acrysof IQ SofPort Advanced
Optics
Manufacturer AMO Alcon Bausch & Lomb
Code Z9002 SN60WF LI61AO
Material Silicone Acrylic Silicone
SA at 6mm -0.27 -0.2 0
IOLs – used to be “spherical”…

Did IOL cancel out corneal SA?
-0.30
-0.20
-0.10
0.00
0.10
0.20
0.30
0.40
Pre-op Corneal SA Post-op Total Ocular SA
Tecnis
AcrySof IQ
All
P = 0.00
SA
(μ
m)

Corneal Spherical Aberration
Average cornea has positive spherical
aberration
Post myopic LASIK cornea has even more
positive spherical aberration
Post hyperopic LASIK cornea has negative
spherical aberration
This may be useful in choosing the type of IOL

Myopic vs Hyperopic Lasik

Targeting
• Normal / Mono / Mini-Mono
• Hyperopia
• Low Myopia / High Myopia

Learning Example #1
• 72 year old female referred for cataract Surgery
• OD: -3.00-0.50x103 20/30 OS: -2.75-1.00x100 20/30
• Grade III brunescent cataracts, Right partial macular hole
• Prefers to read with glasses off and adamant that must preserve her near vision at pre-op appointment
• Prior to OR this was confirmed with the patient and once again stated must preserve near vision at all costs

4 Hours Post Op Exam
• What did you do to me?
• But I cannot see far away!
• I could already read up close my problem was the distance
• I know we talked about this but you didn’t take enough time to explain fully
• This will not do, what are you going to do to fix it
Treatment
• What went wrong?
• Had patient return to her optometrist for a contact lens trial, distance vs mono
• Swallowed my pride and exchanged to IOL
• Also put in a distance IOL in the other eye
• Asked are you happy now?
• Well, it seems OK

Learning Example #2
• 59 year old female bilateral cataracts, myopic but also wears contacts
• Right: -3.75 + 0.50 x 11 Left: -3.75 + 0.75 x 157
• Discussed Preop about being less myopic but preserving reading
• Post Left cataract: -2.50 + 0.75 x 8 and disappointed
• Post Right cataract: -0.25 + 0.50 x 175
Learning Example #3• 53 year old female lawyer with right cataract
• Right: -21.00 + 2.25 x 103 Left: -20.25 + 3.25 x 134
• Myopic degeneration, Bilat CNVM, Lucentis also contact lens wearer
• Right eye was dominant eye and currently 20/400, discussed right target distance and wear a contact on left
• Patient at Preop appointment stated her Optometrist said she should be set at -10 D in right eye, this caused an hour long conversation, target was -1.00 spherical equivalent
• Results: -2.75 + 1.00 x 52, 20/70 sc, ph 20/40

Special Cases
• Keratoconus
• Post-Transplant
• DSAEK / DMEK
• Post Refractive Surgery

Keratoconus

Spheric vs. Toric High Astigmatism

Spheric vs. Toric IOL in Keratoconus

Keratoconus Severe but not Irregular

Keratoconus Example
• 69 year old female
• Severe right keratoconus, previous left PK
• Rx -17.75 + 3.75 x 131 20/80
• Right cornea iron line and slight haze
• Feb 2016, Right cataract / IOL /CTR
• IOL Power: 0.0 diopters
• One week post op 20/50 sc
• Auto Rx: -2.75 + 1.25 x 121

Post Refractive Surgery - RK
• 69 year old female
• Bilateral RK, 1996
• Vision OS was 20/20 now dropped to 20/40
• Nuclear Sclerosis 3/4
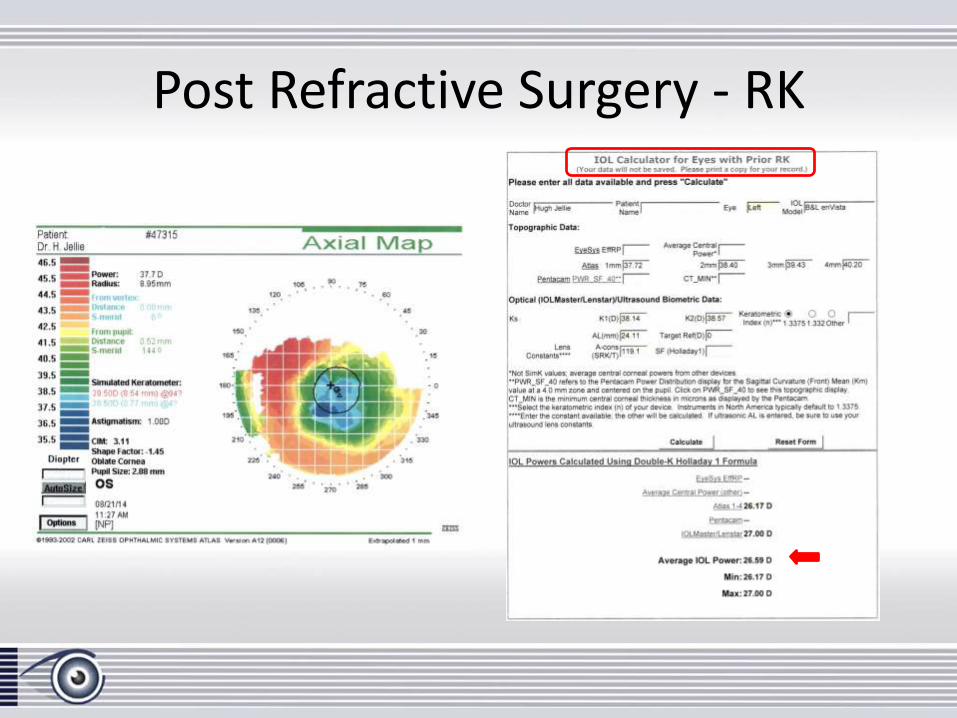
Post Refractive Surgery - RK

Post Refractive Surgery - Lasik
• 64 year old female
• Lasik 1999, no enhancement
• OS Pre: -8.25-0.50-x70
• OS Post 1 mo., -0.25-0.25x140
• OS Now, -3.50+2.75x143, 20/50

What K’s to use?
• 64 patient, previous refractive surgery
• Pre-Lasik 43.37/43.25
• Atlas Sim K’s Post-Lasik 38.87/38.75
• Nidek OPDIII 41.25/40.50
• NIDEK APP 41.17
• IOL Master 40.47/40.86

Post Refractive Surgery - Lasik
• Patient 20/happy
• 1 week po 20/30 sc
Auto Rx: -1.75 + 1.00 x 141

Lens Options
• Who determines the lens choice?– Governments– Patients
• What lens to use?– Monofocal: Standard or
Aspheric– Toric – Multifocal

Who is the Salesman?

Torics Why?
• Candidates
• Calculations
• Available Technologies


Technology Advancements
• Toric Alignment
– Standard
– Advanced Intraoperative Toric Alignment
• Callisto: Computer Assisted Cataract Surgery (Zeiss)
• Verion: Image Guided System (Alcon)
• Aberrometry– ORA Intraoperative Aberrometry (Alcon)
– Holos: Continuous Real-time Intraop Wavefront Aberrometry

Standard Toric Alignment

Toric Classic 3 Step Marking
1. Marking horizontal axis preoperatively ………………….…. 2.4 degrees
2. Marking the limbus at the horizontal position ………….. 3.3 degrees
3. Use horizontal marks to position alignment axis ……… 2.6 degrees
Together the three errors led to a mean total error of in Toric alignment of 4.9 +/- 2.1 degrees , but an individual error could be as high as 10 degrees. A misalignment of more than 10 degrees is generally regarded as an indication for surgical repositioning.

Importance of Stability of Toric IOL’s
Degree of Rotation Percentage Cylinder Power
Loss
1° 3%
5° 17%
10° 35%
15° 52%
30° 100%
90° doubles astigmatism!

Toric Calculation Errors
• Candidate error
• Spherical calculation error
• Toric axis or power error
• SIA error
• Transcription error
• Marking error
• Surgical alignment error
• Surgical stability error

astigmatismfix.com

65
Image. Plan. Guide.
Pre-op Pre-op Intra-op
65
VERION™ Image Guided System
Designed to help you consistently hit your
cataract refractive target
65

6666
Targeting Error Sources in the Current Process
VERION™ has the potential to reduce post-operative residual refractive error
at multiple steps of the cataract surgery process:
• Biometry
• Transcription
• Astigmatism Planning
• Manual marking
• Cyclorotation
• Incision
• Capsulorhexis
• IOL positioning
66
6767
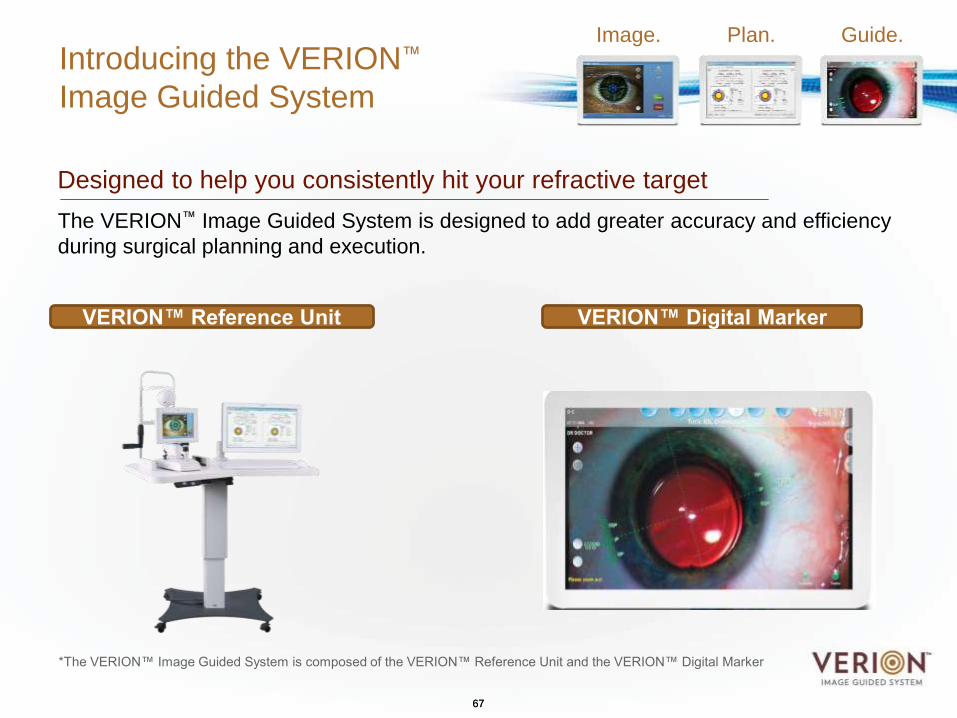
Introducing the VERION™
Image Guided System
Designed to help you consistently hit your refractive target
The VERION™ Image Guided System is designed to add greater accuracy and efficiency
during surgical planning and execution.
Image. Plan. Guide.
VERION™ Reference Unit VERION™ Digital Marker
*The VERION™ Image Guided System is composed of the VERION™ Reference Unit and the VERION™ Digital Marker
67

6868
VERION™ Digital Marker
Guide
To help optimize incision and IOL alignment,
the VERION™ Digital Marker displays patient
information and images from the VERION™
Reference Unit:
• Features a tracking overlay that enables
surgeons to see all incisions and
alignment in real time
• Accounts for cyclorotation
• Eliminates the need for manual toric
eye markings
• Automatically registers the patient for
accurate centering and alignment of
multifocal and toric IOLs
• Allows documentation of data to help
optimize procedures over time
Image. Plan. Guide.

6969
VERION Digital Marker
GUIDE: Incisional Plan
69

7070
VERION Digital Marker
GUIDE: Capsulorhexis Plan
70

7171
VERION Digital Marker
GUIDE: Toric Alignment Plan
71

727272
LENSX® LASERVERION™ IMAGE
GUIDED SYSTEM
CENTURION®
VISION SYSTEM
LUXOR™ LX3 WITH Q-VUE™
OPHTHALMIC MICROSCOPE
The Cataract Refractive Suite by Alcon
The Future of Cataract Refractive Surgery Has Arrived
Verion™ and LenSx® are the ONLY FULLY INTEGRATED
surgical planning – femtosecond – intraoperative marker system on the market

Callisto: Computer Assisted Cataract Surgery (Zeiss)

Multifocals
• Diffractive / Refractive
• Accommodative
• Extended Range (EDOF’s)
• Other Methods to increase depth of focus
• Virtually all say my lens sees better than your lens
• My lens has less halos and glare than your lens
• My lens has a better defocus curve than your lens
• My lens material is better than your lens material

Multifocal Trends
• Low Add MF-IOLs
– Benefits• Focal point moves out
• Less night vision symptoms
• EDOF IOLs
– Extended Depth of Focus

SU131137
Introducing the AcrySof ® IQ ReSTOR® +2.5 IOL
76
The +2.5 Patient• Distant dominant lifestyle
• Primary visual needs are at distance and intermediate • Not willing to compromise distance for a full range
• Desires more opportunity for a range of vision versus monofocal• Desires decreased spectacle use versus monofocal
Aspheric MonofocalAcrySof® IQ IOL
Aspheric Apodized
Diffractive Multifocal IQ ReSTOR® +2.5 IOL
Aspheric Apodized
Diffractive Multifocal IQ ReSTOR® +3 IOL

SU131137
The Growing AcrySof® IQ ReSTOR® Multifocal IOL Family Provides More Options to Cataract Patients
• Provides a range of vision with the same clarity of asphericity as the monofocal IOL
• Ideal for patients who decreased spectacle dependence and sharp distance vision
• Optimal for patients who desire decreased spectacle dependence for near, intermediate, and distance activities
• Offers the broadest range of vision at all distances
• For astigmatic patients who seek the benefits of multifocal technology plus the power of toric
+2.5 D +3.0 D
The growing number of AcrySof® IQ ReSTOR® Family IOL options:• Expands the number of patients who may fully benefit from a ReSTOR® IOL• Broadens the range of IOL options available for patients• Offers closer matches to the particular vision goals of each patient
77
Multifocal Toric +2.5 D Multifocal Toric +3.0 D

SU131137
The AcrySof® IQ ReSTOR® +2.5 D IOL
Most suitable for patients who:• Have distant dominant lifestyles
such as driving, watching TV, viewing and/or participating in live sporting events
• Seek sharper distance vision
• Desire reduced spectacle dependence
• Do not wish to compromise distance vision for a full range
− But, seek more opportunity for range and decreased spectacle use vs. monofocal options
78

SU131137
Optic Design Differences: ReSTOR® +2.5 vs. ReSTOR® +3.0 IOLs
OuterDistance
Zone
Outer Distance
Zone
Center DistanceZone Apodized
DiffractiveMultifocal
Zone
Apodized DiffractiveMultifocal
Zone
ReSTOR® +2.5 IOL ReSTOR® +3.0 IOL
•Reduced the add power from 3.0 D to 2.5 D by:• Reducing diffractive rings from 9 to 7 and increasing spacing
• Altered the light distribution by:• Increasing the distance function of the center zone from 40% to 100% • Reducing apodized diffractive area by 18% (from 10.2mm2 to 8.4mm2)• Increasing the outer distance area by 6% (from 18.1mm2 to 19.9mm2)
79
Alcon Data on File TDOC -0015054

SU131137
Bench Headlight Image Simulation
AcrySof IQ IOL ReSTOR +2.5 IOL
Oculentis* MPlusCrystalens* HD500 Tecnis* ZMA00
ReSTOR +3.0 IOL
80
*Trademarks are property of their respective ownersAlcon Data on File TDOC -0009977

TECNIS PLATFORM: Wave Front DesignOptical Synergy

Optical Synergy
A patient’s visual outcome following cataract surgery is affected by a multitude of factors, many which are directly attributed to the IOL.
Multiple lens design and material attributes affect quality of vision, including:
1. Spherical aberration correction
2. Chromatic aberration correction
3. Light transmission
4. Material clarity
5. Lens epithelial cell (LEC) migration
– For multifocal lenses, these attributes are even more critical and there are further considerations such as pupil-independence
82
82

1. Spherical Aberration Correction
Residual spherical aberration of monofocal lenses (4 mm pupil)*
83
*Data on file. Abbott Medical Optics Inc.
Full correction of spherical aberration results in sharper focus of light
83

85
4. Incidence of Glistenings
AMO® IOLs are not associated with glistenings
– A study found that while the AMO®
acrylic material had no lens with glistenings higher than Grade 1, the AcrySof ® lenses had some Grade 2 glistenings7
– AMO’s proprietary cryo-lathing method limits microvoid formation and high temperature fluctuations that can cause glistenings8
7Tognetto D, et al. JCRS. 2002.8Miyata A, JCRS. 2004.
85
Glistenings in a competitive
acrylic IOL
Image courtesy of Randall J. Olson, MD

86
– It has been shown that a 360° sharp edge, including at the haptic-optic junction, plays the greatest role in limiting LEC migration*
– The TECNIS® 1-Piece IOL with ProTEC™ 360° edge design provides an uninterrupted barrier edge, designed to prevent LEC migration better than previous 1-piece lens designs**
5. Limiting LEC migration
*Kugelberg M, et al. JCRS. 2006.
**Nixon DR. Presented at ESCRS, 2007.
TECNIS® 1-Piece IOL AcrySof ® IOL
86
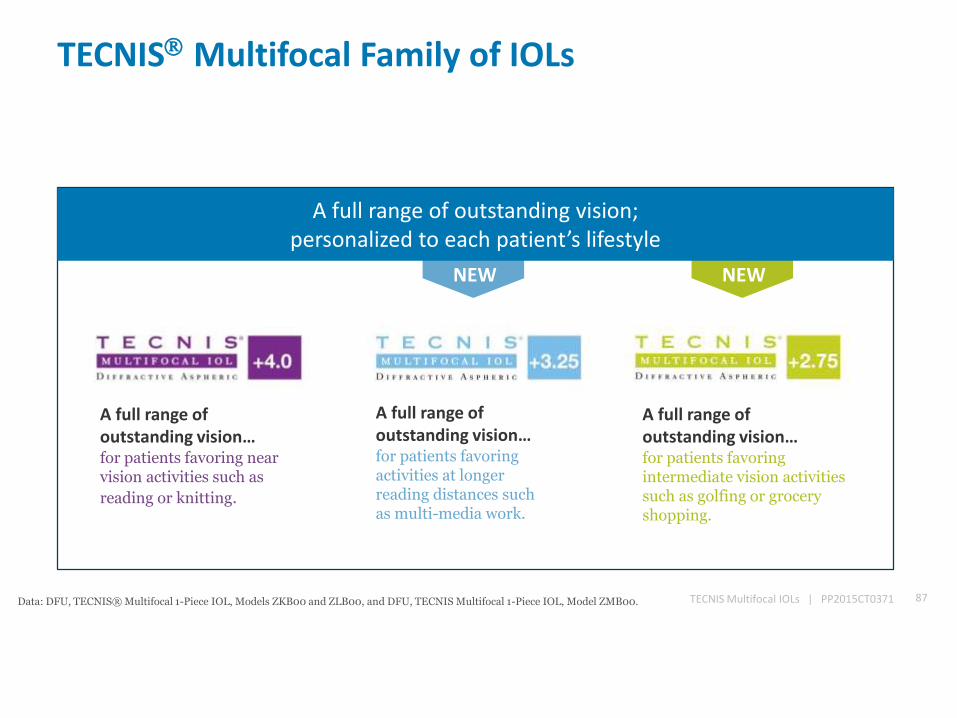
TECNIS Multifocal Family of IOLs
A full range of outstanding vision… for patients favoring activities at longer reading distances such as multi-media work.
A full range of outstanding vision… for patients favoring intermediate vision activities such as golfing or grocery shopping.
A full range of outstanding vision… for patients favoring near vision activities such as
reading or knitting.
TECNIS Multifocal IOLs | PP2015CT0371 87
NEW NEW
A full range of outstanding vision;personalized to each patient’s lifestyle
Data: DFU, TECNIS® Multifocal 1-Piece IOL, Models ZKB00 and ZLB00, and DFU, TECNIS Multifocal 1-Piece IOL, Model ZMB00.

TECNIS® Multifocal Family of IOLsBinocular Defocus Curve at 6 Months
88TECNIS Multifocal IOLs | PP2015CT0371Data: DFU, TECNIS® Multifocal 1-Piece IOL, Models ZKB00 and ZLB00, and DFU, TECNIS Multifocal 1-Piece IOL, Model ZMB00.Distances (cm) in the graph are approximate.
ZM900 (+4.0 D) data are historical from a separate clinical study using the same test methodology.

89
New Solution for Presbyopia Correction Extended Range of Vision IOLs
The first and only presbyopia-correcting extended range of vision IOL.
Delivers a continuous, full-range of high quality vision with reduced incidence of halos and glare comparable to a monofocal IOL.1,2
1. 168 Data on File_Symfony_Simulated Defocus Curves2. 166 Data on File_Extended Range of Vision IOL 3-Month Study Results (NZ)

90
A New Segment of IOLs –Extended Range of Vision IOLs
The TECNIS® Symfony Extended Range of Vision IOL represents a new segment in presbyopia-
correcting IOLs.
Multifocal and Tri-Focal IOLs
Accommodating IOLs
Extended Range of Vision IOLs

Diffraction in OphthalmologyDiffraction Gratings
A diffraction grating is a collection of diffracting elements1
91
Diffracting element or echelette
Step height
Area
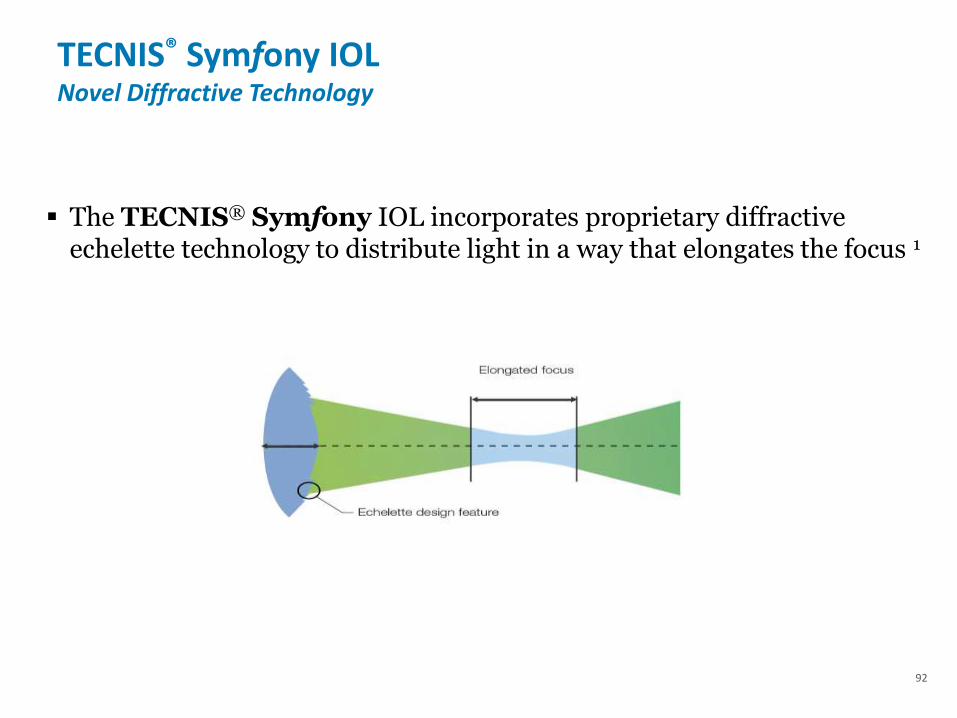
TECNIS® Symfony IOL Novel Diffractive Technology
The TECNIS® Symfony IOL incorporates proprietary diffractive echelette technology to distribute light in a way that elongates the focus 1
92


• Excellent far and intermediate vision
– Segment with higher refraction for intermediate distance
– good visual acuity from far to intermediate (until 60 cm) through
ADD +1.50 dpt within the segment
Design

• Comparison of monofocal IOL with Comfort IOL
– LENTIS Comfort
• Good far vision and within all intermediate distances
• Higher spectacle independency, spectacles only for distances
< 60 cm necessary
Spectacles only for distances
< 60 cm necessary
Good far vision without spectacles
Good intermediate vision without
spectacles!
Design

LENTIS Comfort – the future standard of care in cataract surgery
Market Trends
• EDOF = Extended Depth Of Focus
Novel and modern concept of creating a larger range of
functional vision with as little physical focal points as
possible
Refractive Cataract Surgery
Patients are very demanding and knowledgable
Market is polarizing in basic (public) care and special (private) care
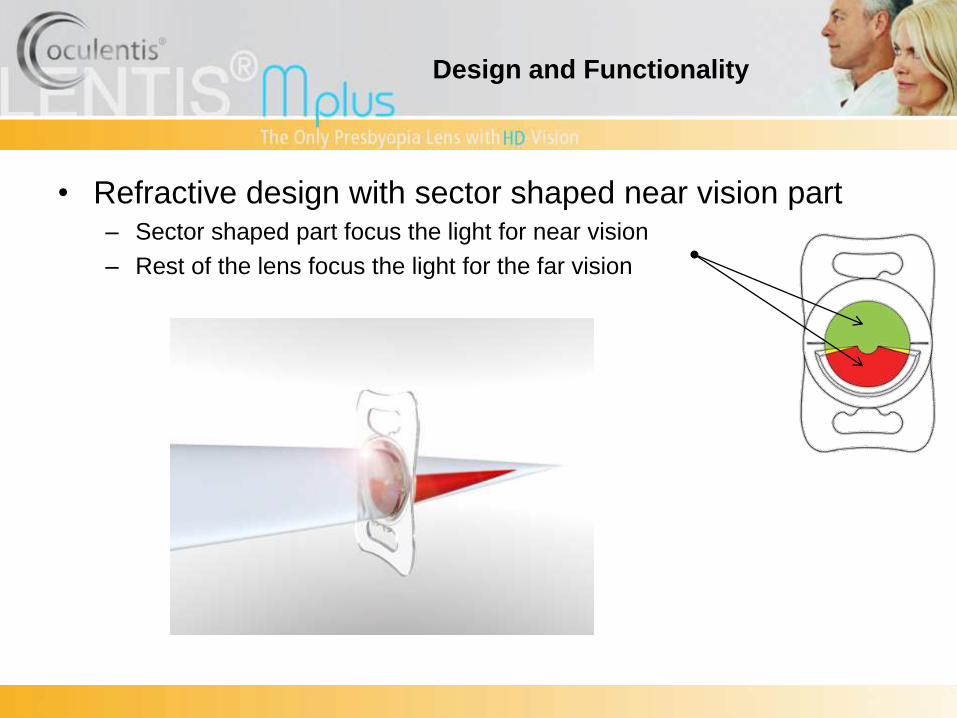
• Refractive design with sector shaped near vision part– Sector shaped part focus the light for near vision
– Rest of the lens focus the light for the far vision
Design and Functionality

Far Near
Interval
Far Near
Simplified Model Asymmetrical ray section at the image
planes
Small Blur Radius ±10 mµ
Interval
Far and Near. Each with his own reduced
aperture size function independently
For Far and Near objects a high quality
image is created by the 2 asymmetrical
optical zones
The Near part does not contribute to an
increased blur size and improve distance
vision quality.
At the lower boundary of the interval; the
central far part gives a high quality blur
radius; serving better intermediate vision.
The optical effect of the Near and Far part
is low frequency background illumination of
the retina in 180°
As a result the asymmetrical far and near
optical zone work with a dramatically
increased depth of focus resulting in good
distance, near and intermediate vision.

Additional Benefits for Patient
• Almost freedom from spectacles
• Fast adaption time (less than 4 weeks)
• Good contrast sensitivity
• Minimal halos and glares
• Pupil independent
• sph ±0.0 dpt till +36.0 dpt (0.5 dpt)
• LENTIS Mplustoric to correct astigmatism
• sph ±0.00 dpt till +36.00 dpt (0.01 dpt)
• cyl +0.25 dpt till +12.00 dpt (0.01 dpt)






Femtosecond Laser-Assisted Cataract Surgery (FLACS)

Laser vs Conventional Cataract Surgery:
real life data
• 2,814 prospective FLACS cases from 2013 to 2015
• 16 centres, 10 European countries
• Similar visual results (UDVA, CDVA, refractive target)
• More postoperative surgical complications FLACS
• More lost lines of vision with FLACS (3.3%) than CPS (1.3%)
• Improved astigmatism correction in FLACS (18.5%) over CPS (9%)

FLACS vs CPS
Metaanalysis
• 9 RCT, 15 cohort studies
• 4,903 eyes
• Slightly improved UDVA in FLACS
• Slightly improved refractive outcomes in FLACS
• Less postoperative complications with FLACS

Fig 5. Forest plot comparison of UDVA at final follow-up after treatment with FLACS and CPS.
Chen X, Chen K, He J, Yao K (2016) Comparing the Curative Effects between Femtosecond Laser-Assisted Cataract Surgery and Conventional
Phacoemulsification Surgery: A Meta-Analysis. PLoS ONE 11(3): e0152088. doi:10.1371/journal.pone.0152088
http://journals.plos.org/plosone/article?id=info:doi/10.1371/journal.pone.0152088

FLACS vs CPS: which is better?
• Why does the data conflict?
• FLACS appears to be safe
• Overall no significant clinical benefit of
FLACS over CPS in terms of safety,
visual quality, or refractive outcome.
• Significant cost difference currently

Current Opinion in OphthalmologyJanuary 2016 – Vol 27 (1): p76-81
• Recent findings: FLACS has several potential advantages over traditional phacoemulsification. However, although studies have demonstrated noninferiority of FLACS, there continues to be few data to support significantly improved visual outcomes. The literature does show a significantly higher cost for FLACS.

Wills Eye Alumni Conference: March 10-12, 2016Review of Visual Outcomes of Femtosecond Laser Assisted Cataract
Surgery by Novice Surgeons
• Conclusions: There is no significant difference in complication rates between FLACS and MCS for novice surgeons.

LenSx Video

Catalys Video

Ethics in Ophthalmology(is there such a thing?)
• What is our role and obligations when discussing surgical options with patients?
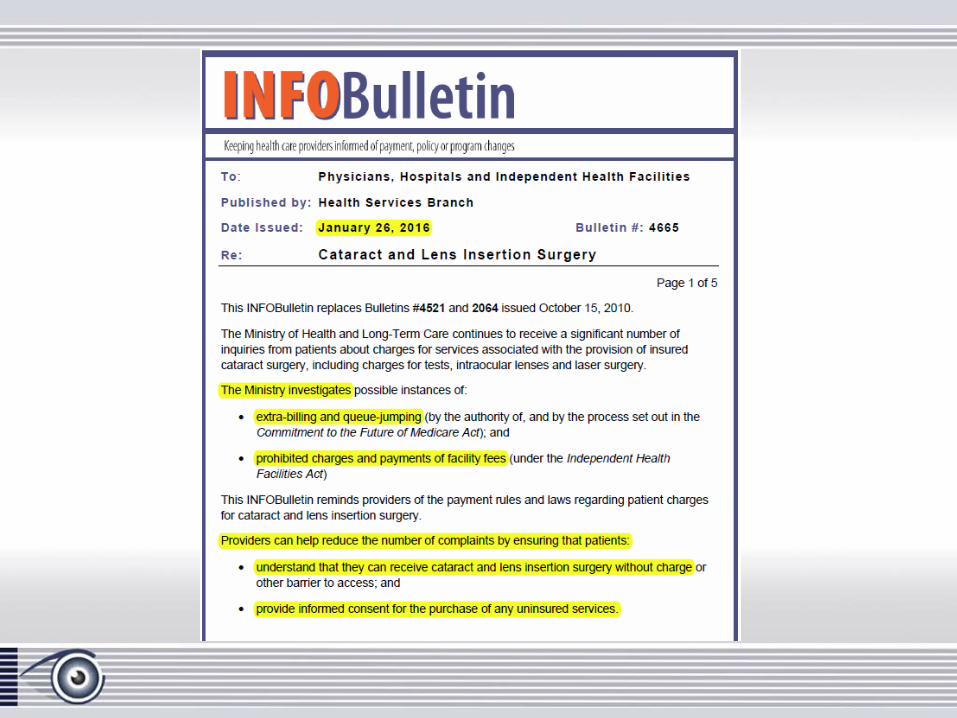
• MOH: INFO Bulletin, January 26, 2016





Femto / Toric Example
• 56 year old man presents for right cataract surgery
• Told at a private clinic he would be a good candidate for a Femto / Toric IOL
• Underwent a Right Toric IOL

Post Toric Lens
• Tecnis ZCT 100 implanted
• Post-op: 20/40, Mx: -0.50+1.25 x 160, IOL axis 60 degrees
• Patient very unhappy and told if he wishes to fix this astigmatism then a PRK is needed
• Seeks a second opinion

Second Opinion and Treatment
Second Surgery:IOL exchange with a Monofocal IOLVA: 20/25 Plano, patient happy with resultWhere did things go wrong?

Summary of What We Learned• We are in a constant environment of changing technologies,
some evolve and some are abandoned
• Monofocal lens is still the standard but there is an upswing in Torics
• Multifocal / Extended Range IOL’s are changing on almost a monthly basis but there is a trend to low add IOL’s
• Technologies in Alignment, Intraoperative Refraction and Lens Based Surgery will continue to evolve
• Governments can and do shape the interpretation and delivery of health care and how we interact with our patients

Thank You