clinical considerations with silicone hydrogel...
TRANSCRIPT
1
Clinical Considerations with Silicone Hydrogel Lenses
Maurice J Wilson, OD
Agenda
The science behind the lensesOxygenSurfaceDesignLens care and silicone hydrogel lensesComfort & adaptation issues
The Science Behind the Lenses
HEMA-based materials– Positives
Easily fabricated into CL’sRelatively cheap to produceHighly flexibleDimensionally stable to changes in pH & temp.
– NegativesReliance on H2O to transport O2
– Limitation to amount of O2 transmitted to cornea– Corneal oxygen deficiency
O2 transport – HEMA materials
27
55
28
55
32
66
26
58
0
20
40
60
80
100
120
140
160
180
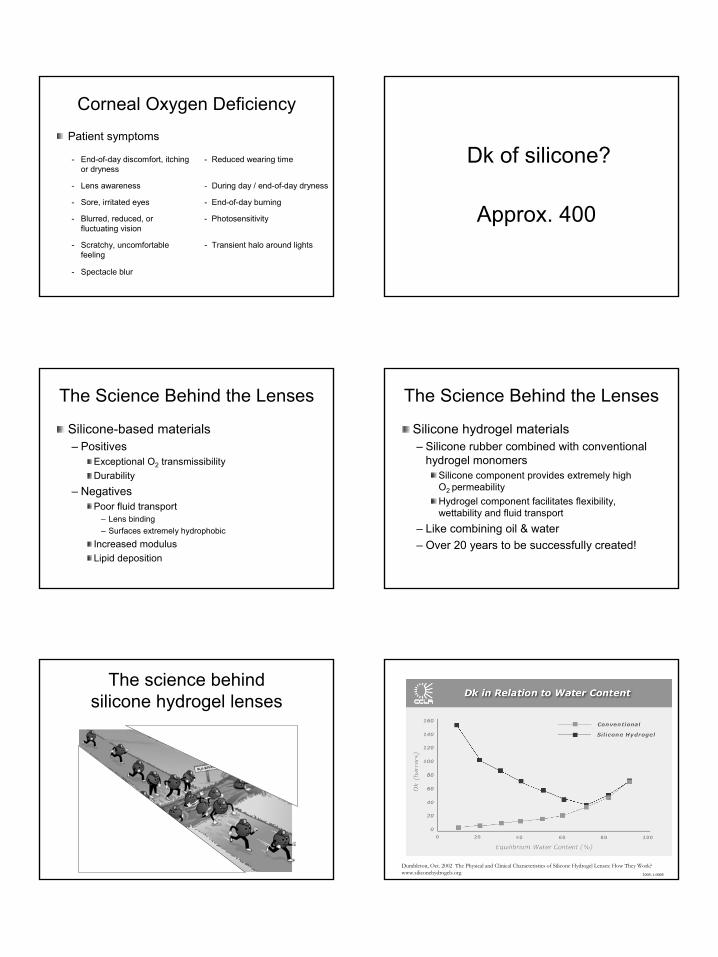
Dk/t H20
Dk/t and H2O
Frequen
cy®
55.
Biomedics
®
Soflens®
66
ACUVUE® 2
Primary means of ↑ Dk/t is to ↑ H2O
H2O has limited ability to dissolve & transport O2
Dk of H2O approx. 80– “100% H2O lens” Dk = 80
Corneal Oxygen DeficiencyClinical signs
- Conjunctival injection - Limbal redness
- Neovascularization - Corneal staining
- Refractive error shift - Corneal neovacularization (myopic shift of ≥ 0.50 D)
- Corneal edema - Corneal distortion
- Increased bacterial binding - Endothelial polymegethism, pleomorphism & ↓ cell density
- Keratometry/topographical - Increased corneal changes and distortion thickness
2
Corneal Oxygen Deficiency
Patient symptoms
- End-of-day discomfort, itching - Reduced wearing time or dryness
- Lens awareness - During day / end-of-day dryness
- Sore, irritated eyes - End-of-day burning
- Blurred, reduced, or - Photosensitivity fluctuating vision
- Scratchy, uncomfortable - Transient halo around lights feeling
- Spectacle blur
Dk of silicone?
Approx. 400
The Science Behind the Lenses
Silicone-based materials– Positives
Exceptional O2 transmissibilityDurability
– NegativesPoor fluid transport
– Lens binding – Surfaces extremely hydrophobic
Increased modulusLipid deposition
The Science Behind the Lenses
Silicone hydrogel materials – Silicone rubber combined with conventional
hydrogel monomersSilicone component provides extremely high O2 permeabilityHydrogel component facilitates flexibility, wettability and fluid transport
– Like combining oil & water – Over 20 years to be successfully created!
The science behind silicone hydrogel lenses
Dumbleton, Oct. 2002 The Physical and Clinical Characteristics of Silicone Hydrogel Lenses: How They Work? www.siliconehydrogels.org 2005-1-0005
3
27
55
28
55
32
66
26
58
86
47
101
36
138
33
147
38
175
24
020406080
100120140160180
Dk/t H20
Dk/t and H2O
Conventional Lenses Silicone Hydrogels
ACUVUE®
OASYS™
PureV
ision
®
NIGHT &
DAY
®
Frequen
cy®
55.
Biomedics
®
Soflens®
66
ACUVUE® 2
O 2OPTIX
™
ACUVUE®
Advance
™
18.9%20.0%
25.3%
26.8%
22.0%23.4%
17.6%16.7%
15.5%15.2%14.4%14.0%14.4%
13.8%12.8%11.4%
9.2%
7.5%
5%
10%
15%
20%
25%
30%
Jan04
Feb Mar Apr May Jun Jul Aug Sept Oct Nov Dec Jan05
Feb Mar Apr May Jun
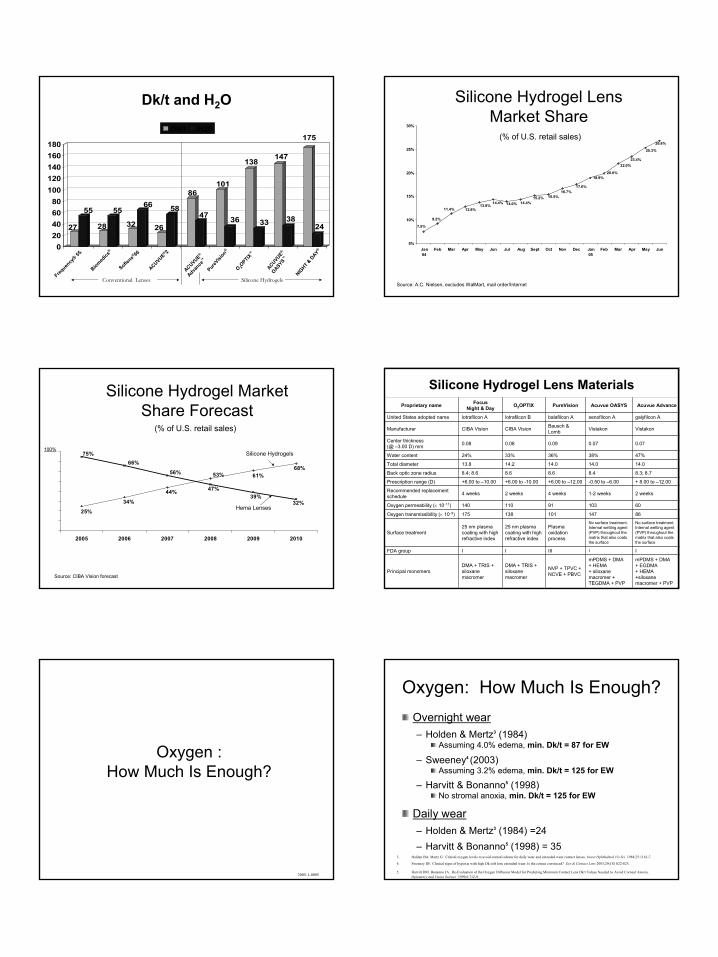
Source: A.C. Nielsen, excludes WalMart, mail order/Internet
Silicone Hydrogel Lens Market Share
(% of U.S. retail sales)
Silicone Hydrogel Market Share Forecast
25%
34%
44%
68%61%53%
47%
32%39%
56%
66%75%
2005 2006 2007 2008 2009 2010
Hema Lenses
Silicone Hydrogels100%
Source: CIBA Vision forecast
(% of U.S. retail sales)
Silicone Hydrogel Lens Materials
mPDMS + DMA + EGDMA + HEMA +siloxane macromer + PVP
mPDMS + DMA + HEMA + siloxane macromer + TEGDMA + PVP
NVP + TPVC + NCVE + PBVC
DMA + TRIS + siloxane macromer
DMA + TRIS + siloxane macromer
Principal monomers
IIIIIIIFDA group
No surface treatment.Internal wetting agent (PVP) throughout the matrix that also coats the surface
No surface treatment. Internal wetting agent (PVP) throughout the matrix that also coats the surface
Plasma oxidation process
25 nm plasma coating with high refractive index
25 nm plasma coating with high refractive index
Surface treatment
86147101138175Oxygen transmissibility (× 10–9)
6010391110140Oxygen permeability (× 10–11)
2 weeks1-2 weeks4 weeks2 weeks4 weeksRecommended replacement schedule
+ 8.00 to –12.00-0.50 to –6.00+6.00 to –12.00+6.00 to -10.00+6.00 to –10.00Prescription range (D)
8.3; 8.78.48.68.68.4; 8.6Back optic zone radius
14.014.014.014.213.8Total diameter
47%38%36%33%24%Water content
0.070.070.090.080.08Center thickness (@ –3.00 D) mm
VistakonVistakonBausch & LombCIBA VisionCIBA VisionManufacturer
galyfilcon Asenofilcon Abalafilcon Alotrafilcon Blotrafilcon AUnited States adopted name
Acuvue AdvanceAcuvue OASYSPureVisionO2OPTIXFocus Night & DayProprietary name
Oxygen :How Much Is Enough?
2005-1-0005
Oxygen: How Much Is Enough?Overnight wear– Holden & Mertz3 (1984)
Assuming 4.0% edema, min. Dk/t = 87 for EW
– Sweeney4 (2003)Assuming 3.2% edema, min. Dk/t = 125 for EW
– Harvitt & Bonanno5 (1998) No stromal anoxia, min. Dk/t = 125 for EW
Daily wear– Holden & Mertz3 (1984) =24– Harvitt & Bonanno5 (1998) = 35
3. Holden BA. Mertz G. Critical oxygen levels to avoid corneal edema for daily wear and extended wear contact lenses. Invest Ophthalmol Vis Sci 1984;25:1161-7.
4. Sweeney DF. Clinical signs of hypoxia with high Dk soft lens extended wear: Is the cornea convinced? Eye & Contact Lens 2003;29(1S) S22-S25.
5. Harvitt DM. Bonanno JA. Re-Evaluation of the Oxygen Diffusion Model for Predicting Minimum Contact Lens Dk/t Values Needed to Avoid Corneal Anoxia. Optometry and Vision Science 1999;6:712-9.
4
There Is Some Consensus
To achieve corneal swelling equivalent to no lens in EW2
To avoid corneal anoxia in overnight wear3
To avoid an increase in limbal hyperaemia in daily wearor extended wear4
– Implications for limbal stem cells which are critical for the long term growth and repair
To reduce bacterial binding for daily wear or extended wear5
3 Silicone Hydrogels, ed. Sweeney, page 93 (2000)4 Harvitt and Bonanno (1999): Re-evaluation of the oxygen diffusion model for predicting minimum contact lens Dk/t values to avoid corneal anoxia.5 Papas, E. On the relationship between soft contact lens oxygen transmissibility and induced limbal hyperemia. Exp Eye Res 1998;67(2):125-131.6 Cavanagh in Ghormley (2005): How Much Oxygen is Enough for Safe Lens Wear (CL Spectrum - March)
A minimum Dk/t is required:
Important Factors to Consider
These studies all represent the AVERAGE response– Average represents 50% of your patients
Patients exhibit widely different corneal swelling responses6
Corneal oxygen demand increases with age7
50% Pass 50% Fail
Dk, Dk/t and “Local Oxygen Transmissibility”
2005-1-0005
O2
O2
O2
O2
O2
Dk
Dk, Dk/t and “Local Oxygen Transmissibility”
2005-1-0005
O2
O2
O2
O2
O2
Dk Dk/t =
O2
O2
O2
O2
O2
?
?
?
?
?
thickness = “t” “t”
↑t → ↓Dk/t
material Dk divided by the local thickness (cm.)
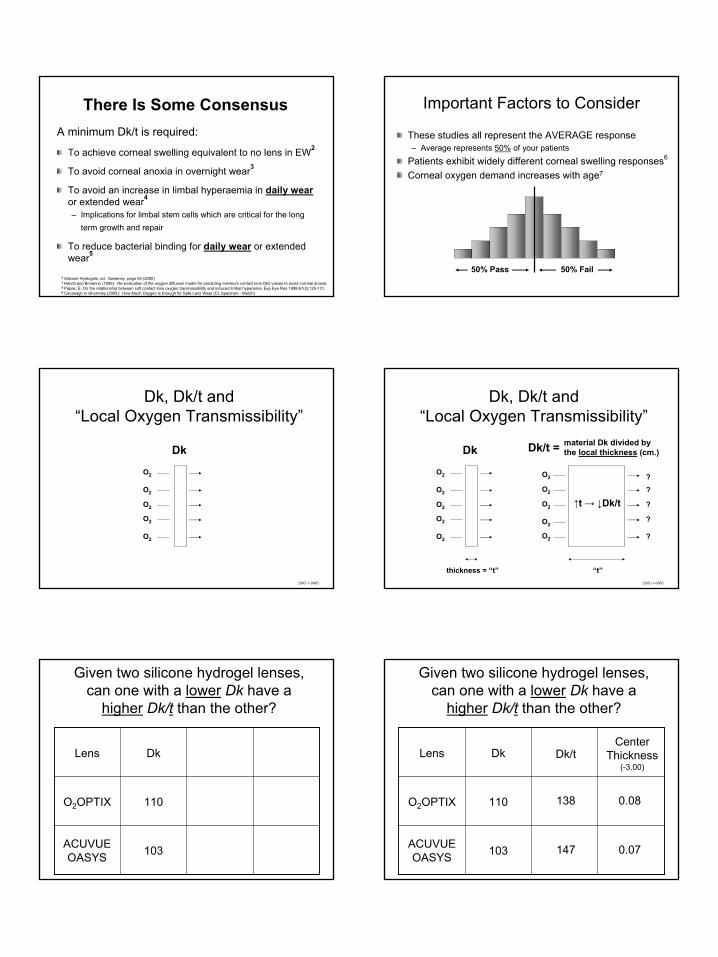
Given two silicone hydrogel lenses, can one with a lower Dk have a
higher Dk/t than the other?
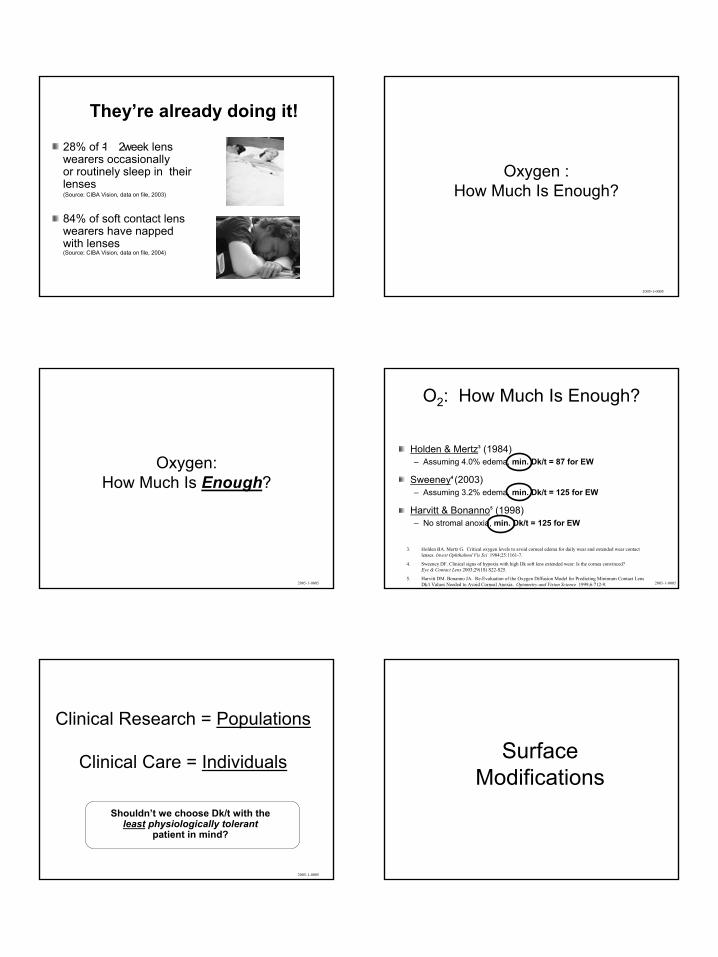
103ACUVUE OASYS
110O2OPTIX
DkLens
Given two silicone hydrogel lenses, can one with a lower Dk have a
higher Dk/t than the other?
103ACUVUE OASYS
110O2OPTIX
DkLens Dk/t
138
147
Center Thickness
(-3.00)
0.08
0.07
5
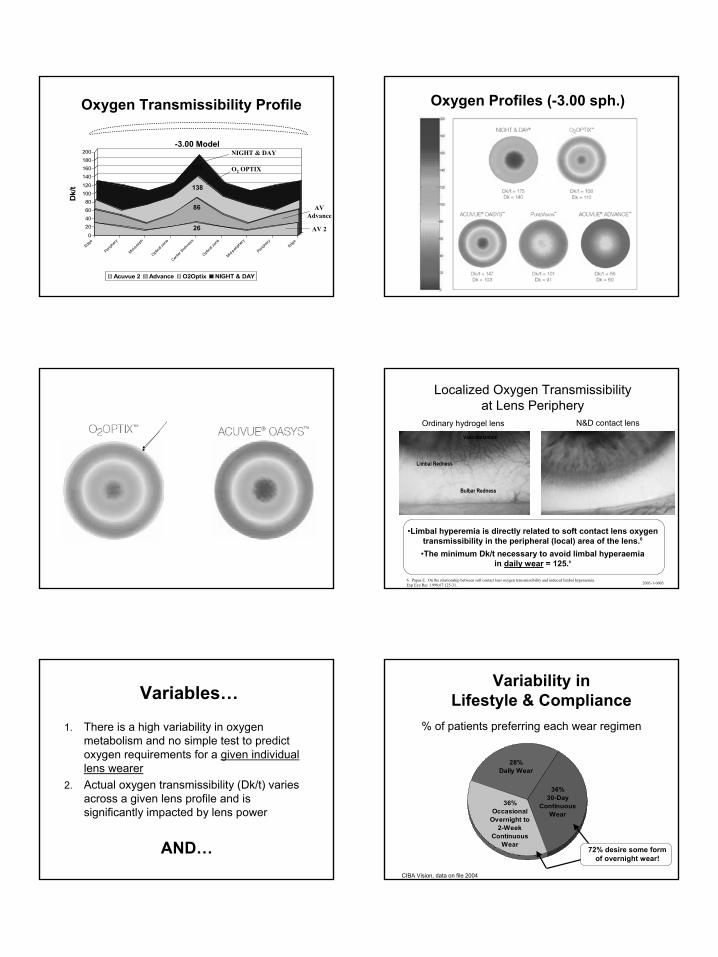
Oxygen Transmissibility Profile
-3.00 Model
0
20406080
100120
140160180200
Dk/
t
Edge
Periph
ery
Mid-peri
ph
Optica
l zon
e
Center
thick
ness
Optica
l zon
e
Mid-peri
phery
Periph
ery
Edge
Acuvue 2 Advance O2Optix NIGHT & DAY
175
138
86
26
NIGHT & DAY
O2 OPTIX
AV Advance
AV 2
Oxygen Profiles (-3.00 sph.)
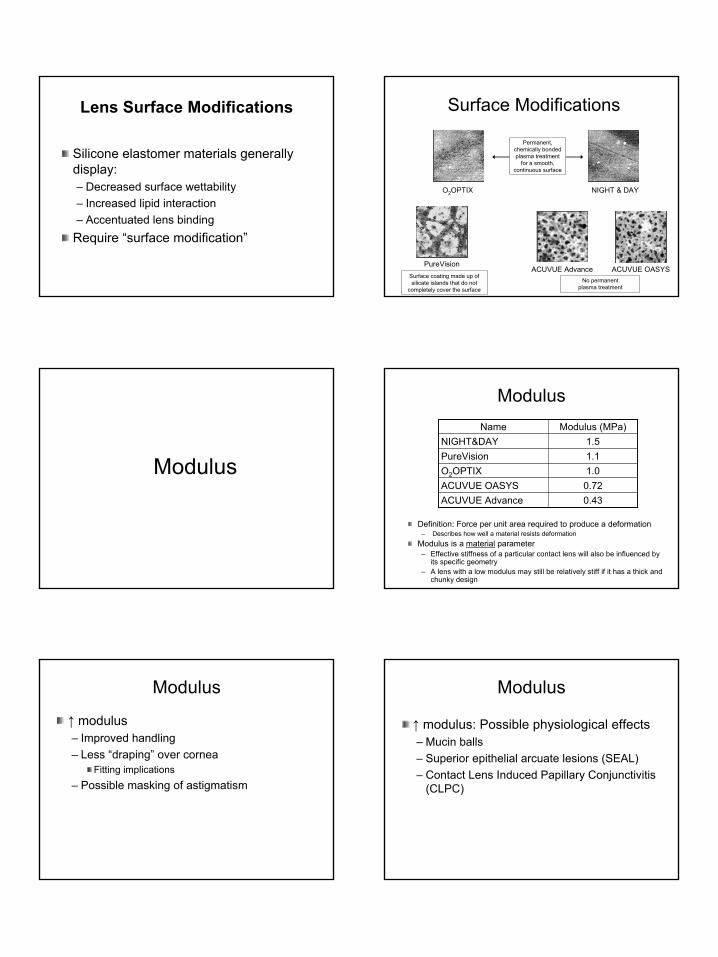
Ordinary hydrogel lens N&D contact lens
Bulbar Redness
Limbal Redness
Vascularization
•Limbal hyperemia is directly related to soft contact lens oxygentransmissibility in the peripheral (local) area of the lens.6
Localized Oxygen Transmissibility at Lens Periphery
6. Papas E. On the relationship between soft contact lens oxygen transmissibility and induced limbal hyperaemia. Exp Eye Res 1998;67:125-31. 2005-1-0005
•The minimum Dk/t necessary to avoid limbal hyperaemia in daily wear = 125.6
Variables…
1. There is a high variability in oxygen metabolism and no simple test to predict oxygen requirements for a given individual lens wearer
2. Actual oxygen transmissibility (Dk/t) varies across a given lens profile and is significantly impacted by lens power
AND…
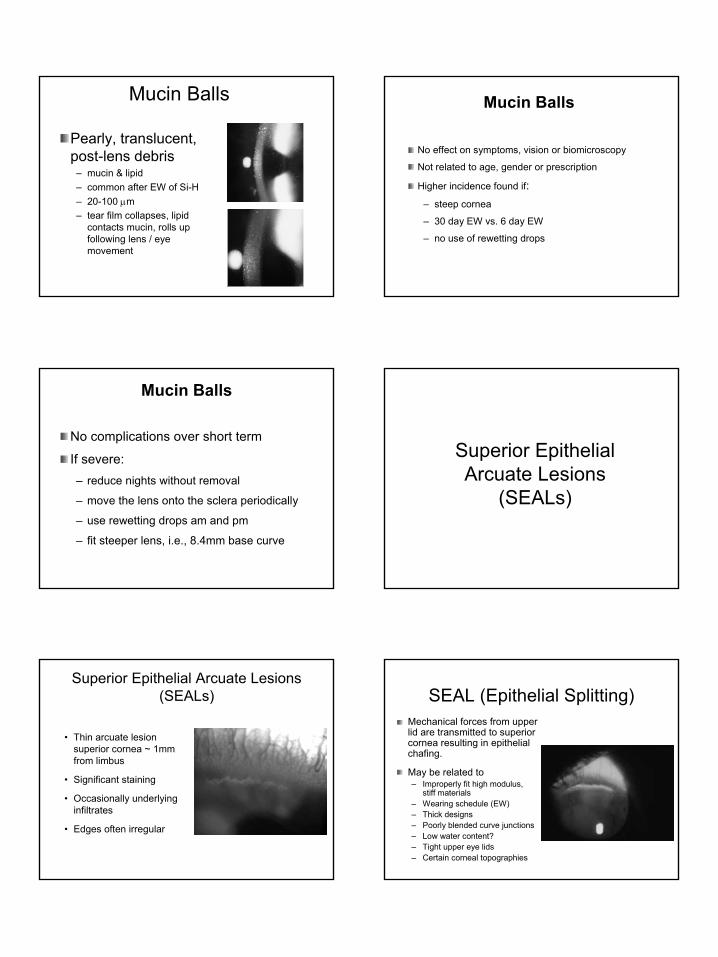
Variability in Lifestyle & Compliance
36% 30-Day
Continuous Wear
28% Daily Wear
36%Occasional
Overnight to 2-Week
Continuous Wear
% of patients preferring each wear regimen
CIBA Vision, data on file 2004
72% desire some form of overnight wear!
6
28% of 1- 2 week lens wearers occasionally or routinely sleep in their lenses(Source: CIBA Vision, data on file, 2003)
84% of soft contact lens wearers have napped with lenses (Source: CIBA Vision, data on file, 2004)
They’re already doing it!
Oxygen :How Much Is Enough?
2005-1-0005
Oxygen:How Much Is Enough?
2005-1-0005
O2: How Much Is Enough?
Holden & Mertz3 (1984) – Assuming 4.0% edema, min. Dk/t = 87 for EW
Sweeney4 (2003)– Assuming 3.2% edema, min. Dk/t = 125 for EW
Harvitt & Bonanno5 (1998) – No stromal anoxia, min. Dk/t = 125 for EW
3. Holden BA. Mertz G. Critical oxygen levels to avoid corneal edema for daily wear and extended wear contact lenses. Invest Ophthalmol Vis Sci 1984;25:1161-7.
4. Sweeney DF. Clinical signs of hypoxia with high Dk soft lens extended wear: Is the cornea convinced? Eye & Contact Lens 2003;29(1S) S22-S25.
5. Harvitt DM. Bonanno JA. Re-Evaluation of the Oxygen Diffusion Model for Predicting Minimum Contact Lens Dk/t Values Needed to Avoid Corneal Anoxia. Optometry and Vision Science 1999;6:712-9. 2005-1-0005
Clinical Research = Populations
Clinical Care = Individuals
Shouldn’t we choose Dk/t with theleast physiologically tolerant
patient in mind?
2005-1-0005
Surface Modifications
7
Lens Surface Modifications
Silicone elastomer materials generally display:– Decreased surface wettability– Increased lipid interaction– Accentuated lens binding
Require “surface modification”
Surface Modifications
O2OPTIX NIGHT & DAY
PureVisionACUVUE Advance ACUVUE OASYS
Permanent, chemically bonded plasma treatment
for a smooth, continuous surface
Surface coating made up of silicate islands that do not
completely cover the surfaceNo permanent
plasma treatment
Modulus
Modulus
Definition: Force per unit area required to produce a deformation– Describes how well a material resists deformation
Modulus is a material parameter– Effective stiffness of a particular contact lens will also be influenced by
its specific geometry – A lens with a low modulus may still be relatively stiff if it has a thick and
chunky design
0.43ACUVUE Advance0.72ACUVUE OASYS1.0O2OPTIX1.1PureVision1.5NIGHT&DAY
Modulus (MPa)Name
↑ modulus– Improved handling– Less “draping” over cornea
Fitting implications– Possible masking of astigmatism
Modulus
↑ modulus: Possible physiological effects– Mucin balls– Superior epithelial arcuate lesions (SEAL)– Contact Lens Induced Papillary Conjunctivitis
(CLPC)
Modulus
8
Mucin Balls
Pearly, translucent, post-lens debris
– mucin & lipid – common after EW of Si-H– 20-100 µm– tear film collapses, lipid
contacts mucin, rolls up following lens / eye movement
Mucin Balls
No effect on symptoms, vision or biomicroscopy
Not related to age, gender or prescription
Higher incidence found if:– steep cornea
– 30 day EW vs. 6 day EW
– no use of rewetting drops
Mucin Balls
No complications over short term
If severe:– reduce nights without removal
– move the lens onto the sclera periodically
– use rewetting drops am and pm
– fit steeper lens, i.e., 8.4mm base curve
Superior Epithelial Arcuate Lesions
(SEALs)
Superior Epithelial Arcuate Lesions (SEALs)
• Thin arcuate lesion superior cornea ~ 1mm from limbus
• Significant staining
• Occasionally underlying infiltrates
• Edges often irregular
SEAL (Epithelial Splitting)Mechanical forces from upper lid are transmitted to superior cornea resulting in epithelial chafing.
May be related to– Improperly fit high modulus,
stiff materials– Wearing schedule (EW)– Thick designs– Poorly blended curve junctions– Low water content?– Tight upper eye lids– Certain corneal topographies
9
SEAL (Epithelial Splitting)
Symptoms– Pt’s often
asymptomatic!– Most common
symptomsFBSIrritation
Contact Lens Papillary Conjunctivitis
(CLPC)
Contact Lens Papillary Conjunctivitis (CLPC)
General CLPC• Large, raised papillae of a
cobblestone appearance• Moderate to severe hyperaemia
across the entire tarsus • Moderate to severe patient
symptoms, including itching or irritation, a stringy or ropy discharge, excessive movement of the lens and blurred vision due to this movement or coatings/discharge on lenses.
Local CLPC• Involves papillae and hyperaemia
confined to one or two areas of the upper tarsus only, usually in the central region nearest the lid margin
• Symptoms typically much milder than in general CLPC, with slight irritation or foreign body sensation often the only symptom.
Contact Lens Papillary Conjunctivitis (CLPC)
Higher modulus?– SiHy: ↑ incidence of “local” CLPC
(≤ 2 zones involved)– Low Dk/t: ↑ incidence of “general” CLPC
(› 2 zones involved)– N&D: Lower incidence 8.4 BC vs. 8.6 BC
High recurrence rate if refit same SiHy material and continue EW
Recurrence rate significantly reduced with DW of same SiHy material
Optics Optics
NIGHT&DAY and O2OPTIX– Advanced aspheric lenses designed to
optimize visual clarity PureVision – Aspheric optical design to correct spherical
aberrationACUVUE Advance and OASYS– No asphericity
10
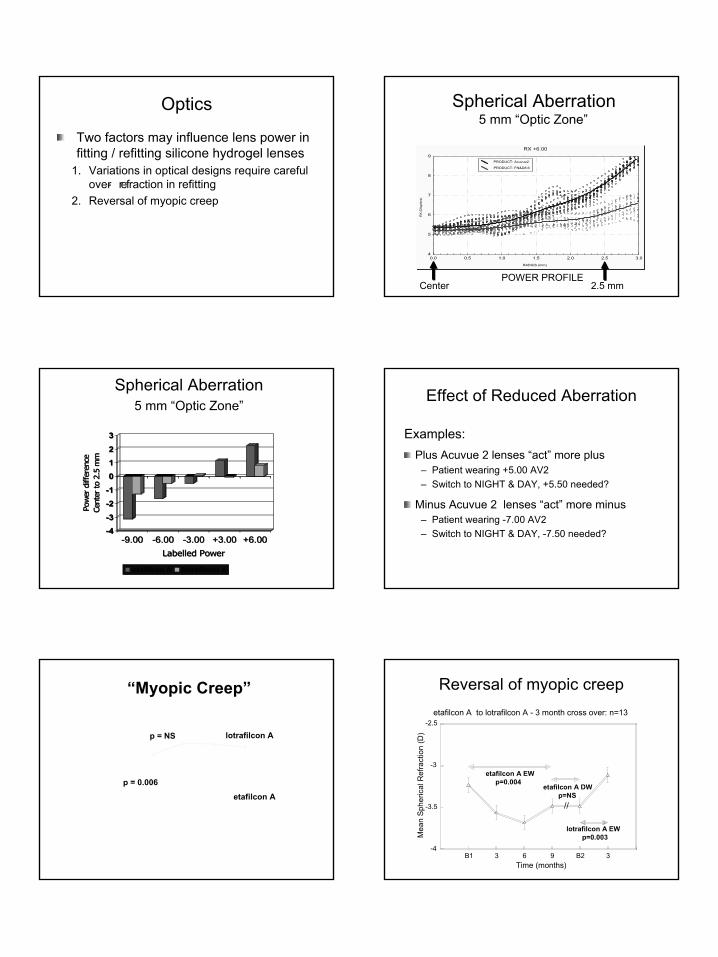
Optics
Two factors may influence lens power in fitting / refitting silicone hydrogel lenses
1. Variations in optical designs require careful over- refraction in refitting
2. Reversal of myopic creep
Spherical Aberration5 mm “Optic Zone”
POWER PROFILECenter 2.5 mm
RX +6.00
RADIUS (mm)
RX
(Dio
pter
s)
4
5
6
7
8
9
0.0 0.5 1.0 1.5 2.0 2.5 3.0
PRODUCT: Acuvue2
PRODUCT: FN&D8.6
RX +6.00
RADIUS (mm)
RX
(Dio
pter
s)
4
5
6
7
8
9
0.0 0.5 1.0 1.5 2.0 2.5 3.0
PRODUCT: Acuvue2
PRODUCT: FN&D8.6
Spherical Aberration5 mm “Optic Zone”
-4-3
-2-1
012
3
Pow
er d
iffer
ence
Cent
er to
2.5
mm
-9.00 -6.00 -3.00 +3.00 +6.00Labelled Power
etafilcon A lotrafilcon A
-4-3
-2-1
012
3
Pow
er d
iffer
ence
Cent
er to
2.5
mm
-9.00 -6.00 -3.00 +3.00 +6.00Labelled Power
etafilcon A lotrafilcon A
Effect of Reduced Aberration
Plus Acuvue 2 lenses “act” more plus– Patient wearing +5.00 AV2– Switch to NIGHT & DAY, +5.50 needed?
Minus Acuvue 2 lenses “act” more minus– Patient wearing -7.00 AV2– Switch to NIGHT & DAY, -7.50 needed?
Examples:
“Myopic Creep”
-1
-0.5
0
0.5
0 3 6 9
Mea
n C
hang
e in
Sph
eric
al R
efra
ctio
n (D
)
Time (months)
etafilcon A
lotrafilcon Ap = NS
p = 0.006
Reversal of myopic creepetafilcon A to lotrafilcon A - 3 month cross over: n=13
-4
-3.5
-3
-2.5
B1 3 6 9 B2 3
Mea
n Sp
heric
al R
efra
ctio
n (D
)
Time (months)
etafilcon A EWp=0.004
etafilcon A DWp=NS
lotrafilcon A EWp=0.003
//
11
Lens Care&
Silicone Hydrogel Lenses
Modern Lens Care Convenience
Current one- step, no- rub, multipurpose (MPS) systems generally contain one of three antimicrobial agents:– Hydrogen peroxide– Polyhexamethylene biguanide (PHMB)– Polyquaternium-1 (Polyquad)
2005-1-0005
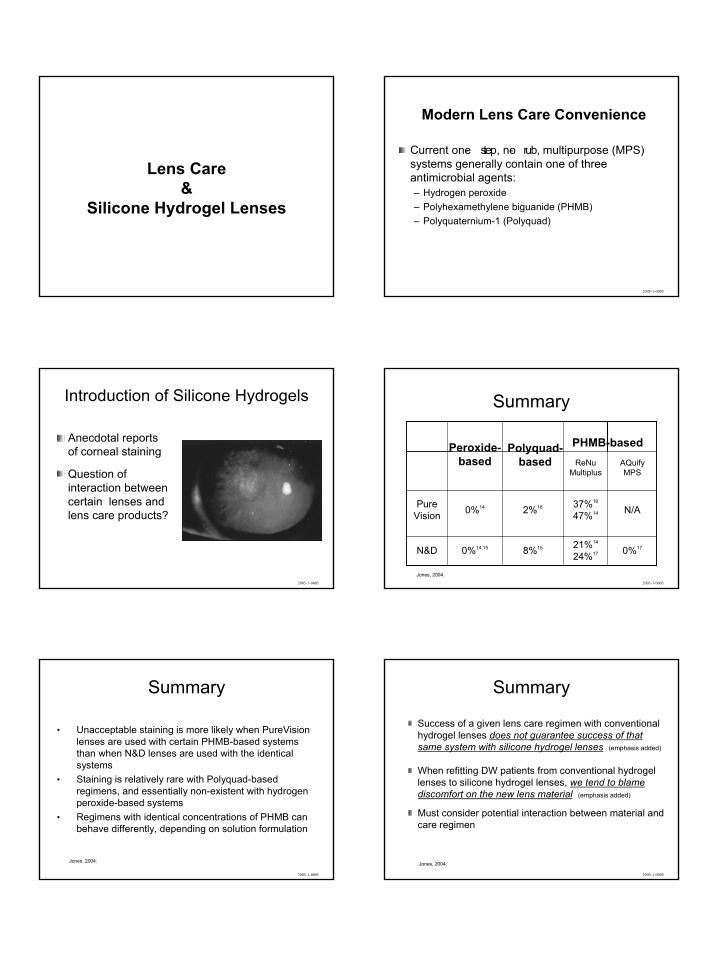
Introduction of Silicone Hydrogels
Anecdotal reports of corneal staining
Question of interaction between certain lenses and lens care products?
2005-1-0005
Summary
0%1721%14
24%178%150%14,15N&D
N/A37%16
47%142%160%14PureVision
AQuifyMPS
ReNuMultiplus
Polyquad-based
PHMB-basedPeroxide-based
Jones, 2004.2005-1-0005
Summary
• Unacceptable staining is more likely when PureVision lenses are used with certain PHMB-based systems than when N&D lenses are used with the identical systems
• Staining is relatively rare with Polyquad-based regimens, and essentially non-existent with hydrogen peroxide-based systems
• Regimens with identical concentrations of PHMB can behave differently, depending on solution formulation
Jones, 2004.
2005-1-0005
Summary
Success of a given lens care regimen with conventional hydrogel lenses does not guarantee success of that same system with silicone hydrogel lenses (emphasis added)
When refitting DW patients from conventional hydrogel lenses to silicone hydrogel lenses, we tend to blame discomfort on the new lens material (emphasis added)
Must consider potential interaction between material and care regimen
Jones, 2004.
2005-1-0005
12
“ The ultimate key to success with these novel contact lens materials is to make specific lens care recommendations to every patient …”
- Dr. Jennifer Smythe
Smythe J. A New Generation of Contact Lens Care. Optometric Management March, 2005.
Comfort &
Adaptation
Comfort?
Silicone hydrogel lenses are stiffer than conventional HEMA-based materialsMany patients will experience increased “awareness” when refit
Educate & Set Proper Expectations
Discuss up front!Awareness may increase before it gets better (PMMA RGP)
So how do I decide?
The “Pepsi Challenge”
vs.
13
The “Pepsi Challenge”
vs.
What’s going on?
Comfort and wettability
“Of the silicone hydrogel lenses used, balafilcon A (PureVision®) had the highest
contact angles; galyfilcon A (Acuvue®
Advance™) was the most wettable initially but rapidly developed contact angles similar to balafilcon A (Pure Vision); and lotrafilcon
materials (NIGHT & DAY® and O2OPTIX™) retained the most wettable surface overall.”1
1. Rogers R, Jones L. In vitro and ex vivo Wettability of Phema and Siloxane-Based Contact Lens Polymers. Invest Ophthalmol Vis Sci 2005;46; E-Abstract 918.
End of day comfort and dryness
Dumbleton2 (2004)– Group of successful long- term soft contact lens
wearers were refitted with silicone hydrogel lenses (CIBA Vision Night & Day™ )
DW basis and replaced monthly
2. Dumbleton KA, Keir N, Moezzi A, Jones L, Fonn D. Redness, dryness and comfort following refitting long term low Dk hydrogel wearers
with silicone hydrogels. Optom.Vis.Sci. 2004;81:31.
Dumbleton2 (2004)
– Results:Significantly better end-of-day comfort and less end of day dryness when compared with their habitual lensesWhile end-of-day comfort remained the same throughout the study, there was actually less end of day dryness as the study progressed The intensity of dryness symptoms at the end of the first month and throughout the second month was significantly lower than after the first day and first week wearing the silicone hydrogel lenses
End of day comfort and dryness
2. Dumbleton K. Daily wear performance of Silicone Hydrogel Lenses. www.siliconehydrogels.org June, 2005.
Limbal Hyperemia•“…showed a significant decrease in limbal hyperemia within one month of refitting conventional hydrogel lens.” 2 (emphasis added)
“Bulbar and limbal hyperemia decreased significantly during the study. The reduction … occurred mainly between the baseline and 1 month visits.3
(emphasis added)
2. Dumbleton K. Daily wear performance of Silicone Hydrogel Lenses. www.siliconehydrogels.org June, 2005. 3. Dumbleton et al. Redness, dryness and comfort following refitting long term low Dk hydrogel lens wearers with silicone hydrogel lenses. Optometry and Vision Science 81 (12S):31.
So how do I decide?
“Does this mean that the Pepsi Challenge was a fraud? Not at all. It just means that we have one reaction after taking a sip, and we have another reaction after drinking a whole can. In order to make sense of people’s cola judgments, we need to first decide which of those two reactions most interests us.” (emphasis added)
- Malcolm Gladwell As quoted in “blink”
14
“Most people have a desire to look for the exception instead of the desire to become exceptional.”
- John Maxwell
2005-1-0005
Questions &
Discussion
2005-1-0005
Thank you!
2005-1-0005