clinical bph and its management a comprehensive slide kit professor kurt dreikorn director,...
Post on 18-Dec-2015
214 views
TRANSCRIPT

Clinical BPH and Its ManagementA Comprehensive Slide Kit
Professor Kurt DreikornDirector, Department of Urology
ZentralkrankenhausTeaching Hospital of the University of Gottingen
Bremen, Germany
Mark Speakman, MDConsultant Urologist
Musgrove Park HospitalTaunton, UK
PSC 2001-W-11666-SS

PSC 2001-W-11666-SS
This presentation is provided as a professional service by Merck & Co., Inc. The views expressed herein
represent the independent opinions and experience of the speakers and not necessarily those of Merck & Co., Inc., or its related affiliates.
Any product mentioned in this presentation should be used in accordance with the prescribing information issued by the manufacturer.
Definition, Pathophysiology, and Epidemiology of Clinical BPH
Section I
PSC 2001-W-11666-SS
PSC 2001-W-11666-SS
Definition of Terms
• LUTS Lower-urinary-tract symptoms
• BPE Benign prostatic enlargement(macroscopic)
• BOO Bladder-outlet obstruction
• BPH Benign prostatic hyperplasia (microscopic/histologic)
• BPO Benign prostatic obstruction (BOO caused by BPE)
• Clinical BPH LUTS + BPE + BOO
Slide I.1
PSC 2001-W-11666-SS
Adapted from Nordling J et al. In Benign Prostatic Hyperplasia. Plymouth, United Kingdom: Health Publication, 2001:107-166.
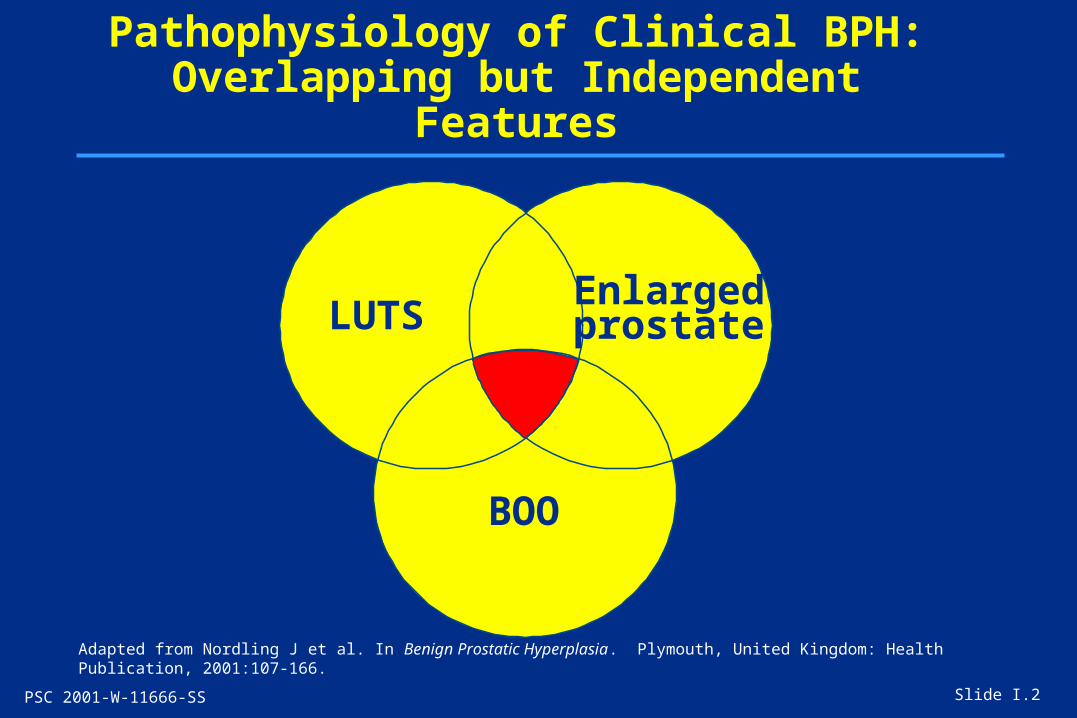
Pathophysiology of Clinical BPH:Overlapping but Independent Features
Slide I.2
LUTSEnlargedprostate
BOO

PSC 2001-W-11666-SS
Adapted from Nordling J et al. In Benign Prostatic Hyperplasia. Plymouth, United Kingdom: Health Publication, 2001:107-166.
Pathophysiology of Clinical BPH:Conditions Potentially Leading to LUTS
Slide I.3
Aging
Anoxia
Obstruc-tion
Highnocturnaldiuresis
Age-relateddiseases
Neuro-logic
diseases
Localdisease
Bladder
LUTS

PSC 2001-W-11666-SS
Pathophysiology of Clinical BPH:Predictive Risk Factors
Slide I.4
• Increasing age
• Prostatic enlargement
• Elevated prostate-specific antigen (PSA)
• Lower-urinary-tract symptoms (LUTS)
• Decreased urinary flow rate
PSC 2001-W-11666-SS
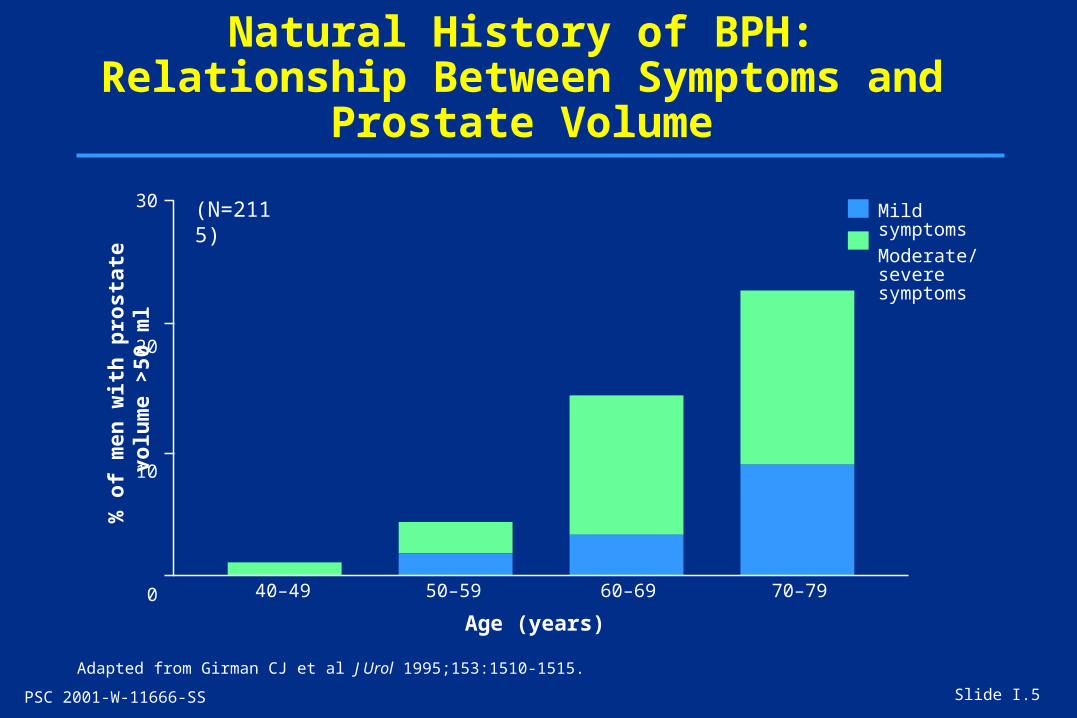
Natural History of BPH: Relationship Between Symptoms and Prostate Volume
Adapted from Girman CJ et al J Urol 1995;153:1510-1515.
Slide I.5
40–49 50–59 60–69 70–79
Age (years)
30
20
10
0
Mild symptoms
Moderate/severe symptoms
% o
f m
en w
ith
pro
stat
e vo
lum
e >
50 m
l (N=2115)

PSC 2001-W-11666-SS
Natural History of BPH: Relationship Between Symptoms and Peak Urinary Flow
Adapted from Girman CJ et al J Urol 1995;153:1510-1515.
Slide I.6
% o
f m
en w
ith
pea
k f
low
rat
e <
10 m
l/se
c
40–49 50–59 60–69 70–79
Age (years)
30
20
10
0
Mild symptoms
Moderate/severe symptoms
(N=2115)

PSC 2001-W-11666-SS
Natural History of BPH:PSA Is a Powerful Risk Factor for Clinical BPH
p<0.00001 for trend across odds ratiosFree PSA values adjusted for age and total PSA
Adapted from Meigs JB et al J Clin Epidemiol 2001;54(9):935-944.
Slide I.7
Od
ds
rati
o
5
4
3
2
1
0
1
1.91.8
4.4
0.0–0.07 0.08–0.10 0.11–0.17 0.18–2.43
Free PSA value
(N=1709)
PSC 2001-W-11666-SS
3.5
3
2.5
2
1.5
1
0.5
0
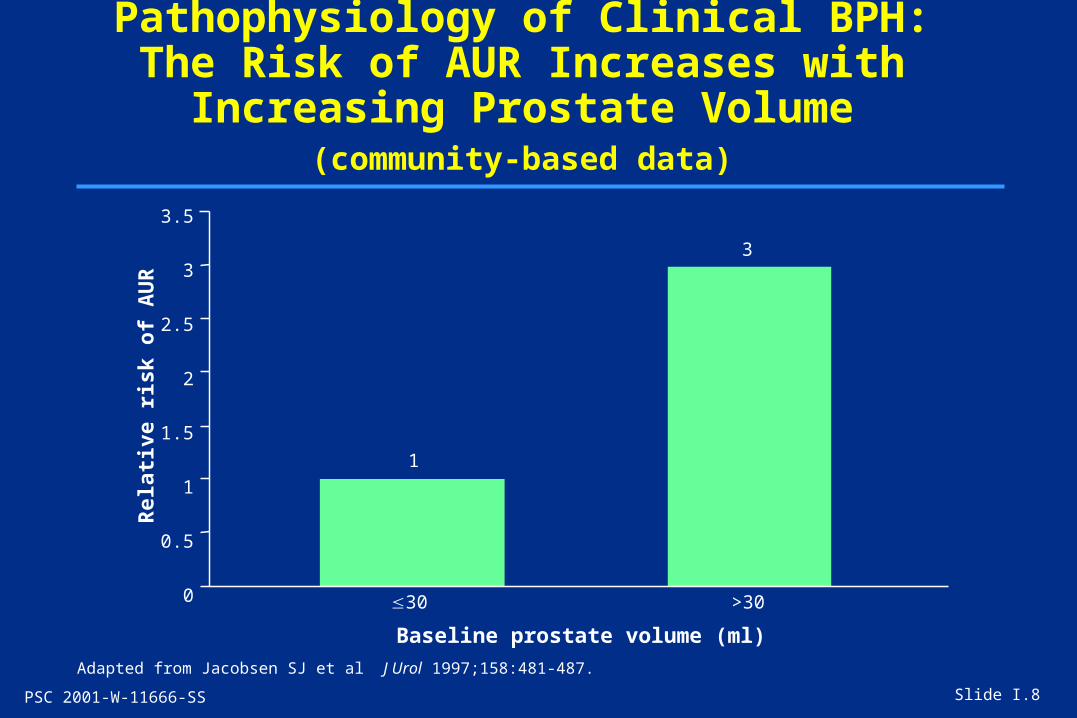
Pathophysiology of Clinical BPH:The Risk of AUR Increases with Increasing
Prostate Volume (community-based data)
Adapted from Jacobsen SJ et al J Urol 1997;158:481-487.
Slide I.8
1
3
30 >30
Baseline prostate volume (ml)
Rel
ativ
e ri
sk o
f A
UR
PSC 2001-W-11666-SS
10
8
6
4
2
0
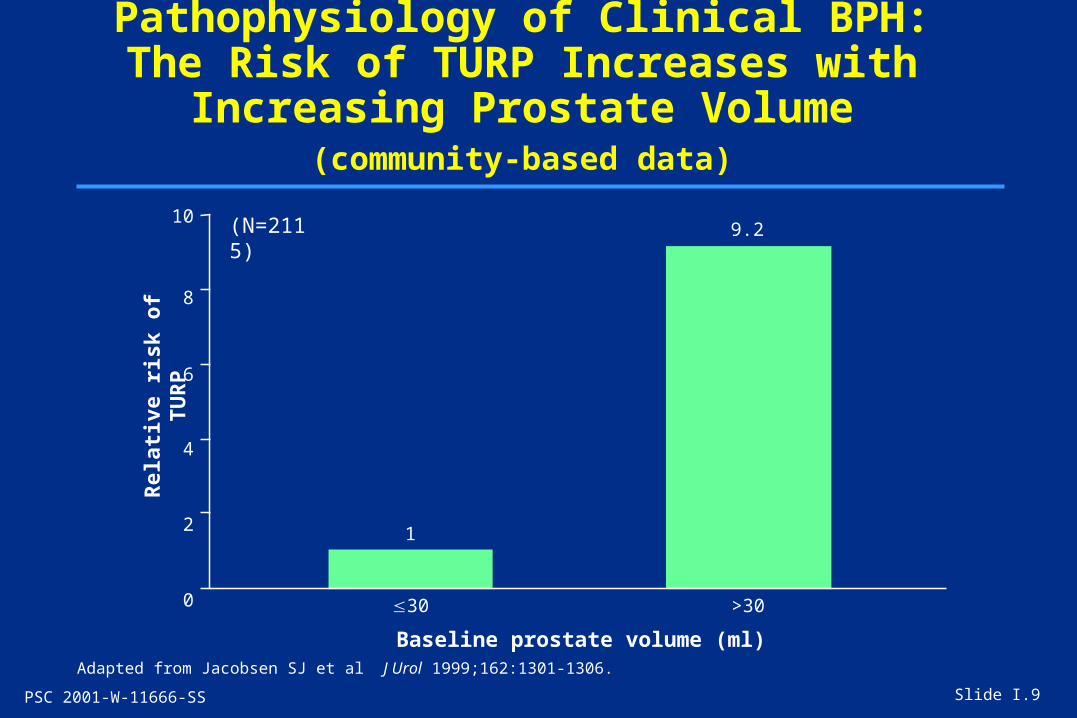
Baseline prostate volume (ml)Adapted from Jacobsen SJ et al J Urol 1999;162:1301-1306.
Slide I.9
Pathophysiology of Clinical BPH:The Risk of TURP Increases with Increasing
Prostate Volume (community-based data)
1
9.2
30 >30
Rel
ativ
e ri
sk o
f T
UR
P
(N=2115)

PSC 2001-W-11666-SS
Definition, Pathophysiology, and Epidemiology of Clinical BPH: Summary
Slide I.10
• Clinical BPH is a multifactorial disease composed mainly of prostatic enlargement, LUTS, and BOO
• Age, prostatic enlargement, elevated PSA, LUTS, and decreased urinary flow rate are major independent predictive risk factors – Elevated PSA levels powerfully predict clinical BPH and
subsequent outcomes
• Prostate volume correlates with BOO, severity of symptoms, and risk of serious outcomes
PSC 2001-W-11666-SS
Consequences of BPH
Section II

PSC 2001-W-11666-SS
Complications of UntreatedClinical BPH
Slide II.1
• Acute urinary retention
• Urinary tract infection
• Bladder calculi
• Bladder damage
• Renal impairment
• Hematuria

PSC 2001-W-11666-SS
Incidence of Serious Clinical Outcomes in Untreated Patients with BPH vs. Other Diseases
Slide II.2
Condition Clinical Outcome Incidence (%)*
Osteoporosis Vertebral fracture 1.5Hip fracture 18
Atherosclerosis Fatal/nonfatal MI 2.1
Superficial bladder cancer Recurrence 30–88
Kidney stones Recurrence 2–47
BPH AUR 7Surgery 10
*Annual incidence or rate per person-years
Adapted from Roehrborn CG et al Urology 2000;56:9-18. McConnell JD et al N Engl J Med 1998; 338(9):557-563.
PSC 2001-W-11666-SS
10
8
6
4
2
0
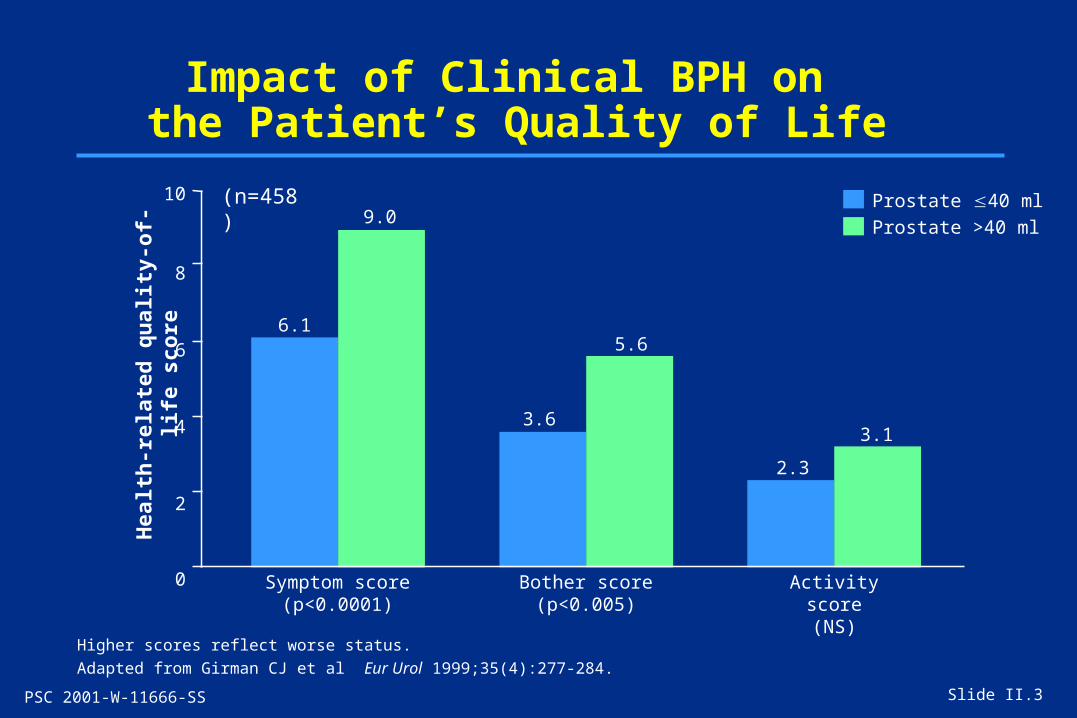
Impact of Clinical BPH on the Patient’s Quality of Life
Higher scores reflect worse status.
Adapted from Girman CJ et al Eur Urol 1999;35(4):277-284.
Slide II.3
6.1
9.0
3.6
5.6
2.3
Prostate 40 ml
Prostate >40 ml
Symptom score(p<0.0001)
Bother score(p<0.005)
Activity score(NS)
Hea
lth
-rel
ated
qu
alit
y-of
-lif
e sc
ore
3.1
(n=458)

PSC 2001-W-11666-SS
Impact of Clinical BPH on the Spouse’s Quality of Life
Adapted from Sells H et al Br J Urol Int 2000;85:440-445.
Slide II.4
80
70
60
50
40
30
20
10
0
47
6671
66
Adverse effects on social life
Adverse impact on
sex life
Worry aboutprostate cancer
Worry aboutpartner’s need
for surgery
% o
f sp
ouse
s
(n=90)

PSC 2001-W-11666-SS
Consequences of Untreated Clinical BPH:Summary
Slide II.5
• Serious clinical outcomes– AUR– BPH-related surgery
• Adverse impact on quality of life– For patients – For spouses

PSC 2001-W-11666-SS
Regulation of Prostate Growth
Section III

PSC 2001-W-11666-SS
Regulation of Prostate Growth:Intrinsic and Extrinsic Factors
Adapted from Lee C et al. In Benign Prostatic Hyperplasia. Plymouth, United Kingdom: Health Publication, 2001:79-106.
Slide III.1
Extrinsic factors Testicular• Androgens• Estrogens• Nonandrogenic
Nontesticular• Endocrine organs• Neurotransmitters• Immunologic
Epithelium• Luminal• Basal• Neuroendocrine
Genetic• Homeobox genes• Hereditary
diseases
Stroma• Fibroblast• Smooth muscle• Extracellular matrix
Environmental• Dietary• Micro-organisms
(immune response)
Urethra• Urine• Testis-epididymal fluid
Extrinsic factors
Intrinsic factors(prostate)

PSC 2001-W-11666-SS
• DHT is the principal androgen responsible for prostatic growth and BPH
• 5-reductase mediates the conversion of testosterone to DHT
Regulation of Prostate Growth:Role of Androgens
Slide III.2
Testosterone Dihydrotestosterone
O
OH
O
OH
H
5-reductase
Adapted from Bartsch G et al Eur Urol 2000;37(4):367-380.

PSC 2001-W-11666-SS
• Inherited 5-reductase deficiency results in male pseudohermaphroditism, characterized by
– Markedly reduced DHT and normal testosterone levels– Lack of prostatic development and/or enlargement (BPH)
• 5-reductase plays a key role in both normal and abnormal prostate growth
Regulation of Prostate Growth:Role of 5-Reductase
Slide III.3
In the 1980s, inhibitors that selectively blocked the action of 5-reductase were synthesized for the treatment of symptomatic BPH.

PSC 2001-W-11666-SS
Tissues in which type I and type II 5-reductase are predominant
Relative Roles of Type I and Type II 5-reductase
Slide III.4
Type I Type II
Skin (sebaceous glands)
Liver
Adrenal glands
Hair follicles
Liver
Seminal vesicles
Prostate gland
Epididymis
Internal/externalgenital tissues

PSC 2001-W-11666-SS
Regulation of Prostate Growth:Summary
• DHT is a key to the regulation of prostatic growth and BPH
• 5-reductase mediates the conversion of testosterone to DHT
• 5-reductase plays a key role in normal and abnormal prostate growth
• 5-reductase has two isoenzymes, type I and type II– Type II predominates in the prostate and other genital
tissues
• Agents that selectively block the action of 5-reductase have been synthesized for the treatment of symptomatic BPH – Finasteride is a selective inhibitor of type II 5-reductase
Slide III.5
PSC 2001-W-11666-SS
Management of BPH
Section IV

PSC 2001-W-11666-SS
Diagnosis of Clinical BPH: International Recommendations
Slide IV.1
Assessment ICBPH Guidelines
Quantification of symptoms–IPSS RecommendedQuantification of symptoms—bother score RecommendedDigital rectal examination RecommendedUrinalysis RecommendedPSA measurement RecommendedVoiding diary (frequency-volume charts) RecommendedUrinary flow-rate recording OptionalPostvoid residual urine volume studies OptionalPressure-flow studies OptionalProstate imaging (TRUS) OptionalUpper-urinary-tract imaging (US or IVU) OptionalLower-urinary-tract endoscopy OptionalSerum creatinine measurement Not recommendedAdapted from Fifth International Consultation 2001 on BPH. In Benign Prostatic Hyperplasia. Plymouth, United Kingdom: Health Publication, 2001:519-535.

PSC 2001-W-11666-SS
*Absolute indications for surgery include urinary retention; significant gross hematuria refractory to finasteride treatment; renal failure, bladder stones, or recurrent urinary tract infections due to BOO; or large bladder diverticulum.
Adapted from Fifth International Consultation 2001 on BPH. In Benign Prostatic Hyperplasia. Plymouth, United Kingdom: Health Publication, 2001:519-535; De la Rosette JJMCH et al Eur Urol 2001;40:256-263.
Treatment of Clinical BPH: International Recommendations
Slide IV.2
Findings RecommendationMinimal/not bothersome LUTS Watchful waitingNo absolute indication for surgery*
Bothersome LUTS Watchful waitingEnlarged prostate Medical treatmentNo absolute indication for surgery* • Finasteride
• Alpha blockerInterventional treatment
Bothersome LUTS Watchful waiting Normal prostate Medical treatmentNo absolute indication for surgery* • Alpha blocker
Interventional treatment
Bothersome LUTS SurgeryNormal or enlarged prostateAbsolute indication for surgery*

PSC 2001-W-11666-SS
ICBPH guidelines• Short term
– Improve symptoms
• Long term – Slow disease progression– Minimize adverse effects of treatment– Preserve quality of life
Treatment of Clinical BPH:Objectives
Adapted from Fifth International Consultation 2001 on BPH. In Benign Prostatic Hyperplasia. Plymouth, United Kingdom: Health Publication, 2001:519-535.
Slide IV.3
PSC 2001-W-11666-SS
Alpha Blockers:Mechanism of Action
• Improve urinary flow and reduce BOO and LUTS
• Do not affect prostate enlargement
• Established mechanisms– Blockade of sympathetic activity– Relaxation of prostatic and bladder-neck smooth
muscle– No effect on disease progression
Slide IV.4

PSC 2001-W-11666-SS
Type II 5-reductase
Type II 5-reductase
5-Reductase Enzyme Inhibitors: Mechanism of Action of PROSCAR™
• Significantly reduces serum and intraprostatic DHT• Treats the underlying cause of BPH
Slide IV.5
PROSCAR (finasteride) is a trademark of Merck & Co., Inc., Whitehouse Station, NJ, USA.
Testosterone
Conversion of Testosterone to Dihydrotestosterone
Testosterone
PROSCAR
Enzyme Inhibition
DHT
DHT

PSC 2001-W-11666-SS
Management of Clinical BPH:Summary
• International guidelines for the management of clinical BPH recommend– Diagnostic tests to characterize disease severity and rule
out other disorders– Treatment to relieve symptoms and prevent complications
• Alpha blockers relieve BPH symptoms primarily by relaxing smooth muscle
• PROSCAR™ relieves BPH symptoms primarily by reducing prostate volume
• PROSCAR slows the progression of BPH
Slide IV.6

PSC 2001-W-11666-SS
Time-Tested Clinical Benefitsof PROSCAR™
Section V

PSC 2001-W-11666-SS
Evidence-Based Medicine:Proven Treatment for Clinical BPH
• Evidence-based medicine is based on results of clinical research.
• Drugs in the same therapeutic class may exert different pharmacologic effects.
• Independent clinical studies must establish each drug’s efficacy, safety, and effect on outcomes.
• Outcome studies with drugs for clinical BPH should evaluate the effects of therapy on AUR and BPH-related surgery.
Slide V.1
PSC 2001-W-11666-SS
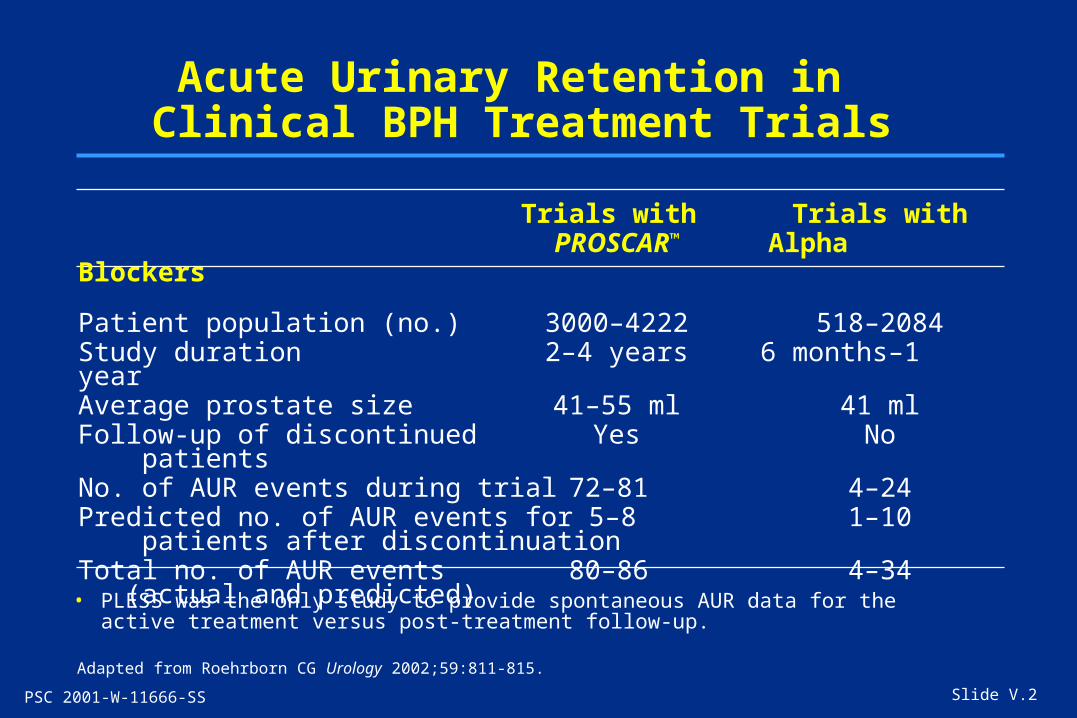
Acute Urinary Retention in Clinical BPH Treatment Trials
Slide V.2
Trials with Trials withPROSCAR™ Alpha Blockers
Patient population (no.) 3000–4222 518–2084Study duration 2–4 years 6 months–1 yearAverage prostate size 41–55 ml 41 mlFollow-up of discontinued Yes No patientsNo. of AUR events during trial 72–81 4–24Predicted no. of AUR events for 5–8 1–10 patients after discontinuationTotal no. of AUR events 80–86 4–34 (actual and predicted)
Adapted from Roehrborn CG Urology 2002;59:811-815.
• PLESS was the only study to provide spontaneous AUR data for the active treatment versus post-treatment follow-up.
PSC 2001-W-11666-SS
PROSCAR™:Treatment Goals
• Improves symptoms
• Reduces risk of AUR
• Reduces risk of BPH-related surgery
• Slows disease progression
Slide V.3
PROSCAR has been proved effective in the treatment of clinical BPH in men with an enlarged prostate.

PSC 2001-W-11666-SS
PROSCAR™:Durable Efficacy in Long-Term Trials
Duration Long-Term ImprovementStudy (years) Symptoms Prostate Volume Urinary Flow
North American 1 SCARP 2 PROSPECT 2 PROWESS 2 PLESS 4 North American Extension* Maintained Maintained MaintainedScandinavian Open Extension* Maintained Maintained Maintained
Slide V.4
= significant improvement from baseline vs. placebo (p0.05); SCARP = Scandinavian Study of Reduction of the Prostate; PROSPECT = Proscar Safety Plus Efficacy Canadian Two-Year Study; PROWESS = Proscar Worldwide Efficacy and Safety Study; PLESS = Proscar Long-term Efficacy and Safety Study
*Benefits achieved during double-blind therapy were maintained in extensions.

PSC 2001-W-11666-SS
Effects of PROSCAR™ on the Natural History of Clinical BPH: Reduced Risk of AUR
Slide V.5
Placebo
PROSCAR
57%risk
reductionp<0.001
15
10
5
0
41 2 30
Pro
bab
ilit
y of
AU
R
Years No. of AURs 36 25 20 18 No. at risk 1503 1454 1398 1347
No. of AURs 14 11 7 10 No. at risk 1513 1487 1449 1421
Placebo
PROSCAR
p<0.001 at 4 years PROSCAR vs. placebo
Adapted from McConnell JD et al N Engl J Med 1998;338(9):557-563.

PSC 2001-W-11666-SS
Effects of PROSCAR™ on the Natural History of Clinical BPH: Reduced Risk of Surgery
Slide V.6
55%risk
reductionp<0.001
15
10
5
01 2 30
Pro
bab
ilit
y of
su
rger
y
No. of surgeries 37 52 32 31No. at risk 1503 1454 1374 1314
No. of surgeries 18 22 9 20No. at risk 1513 1483 1438 1410
Years4
Placebo
PROSCAR
Placebo
PROSCAR
p<0.001 at 4 years, PROSCAR vs. placebo
Adapted from McConnell JD et al N Engl J Med 1998;338(9):557-563.
PSC 2001-W-11666-SS
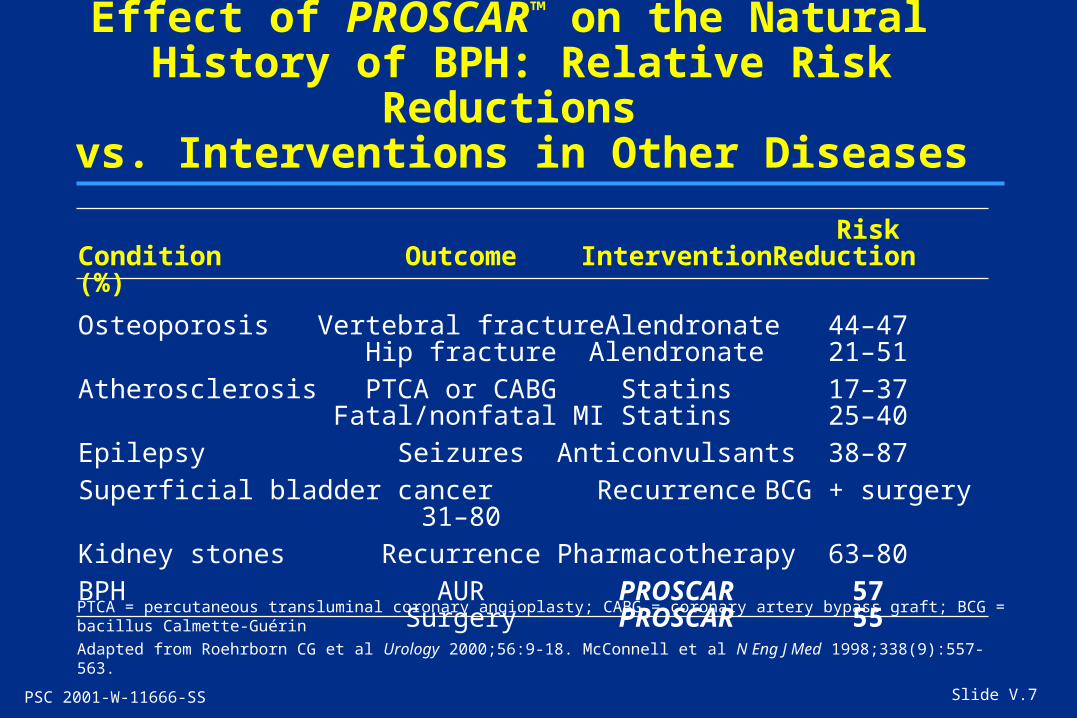
Effect of PROSCAR™ on the Natural History of BPH: Relative Risk Reductions
vs. Interventions in Other Diseases
RiskCondition Outcome Intervention Reduction (%)
Osteoporosis Vertebral fracture Alendronate 44–47Hip fracture Alendronate 21–51
Atherosclerosis PTCA or CABG Statins 17–37 Fatal/nonfatal MI Statins 25–40
Epilepsy Seizures Anticonvulsants 38–87
Superficial bladder cancer Recurrence BCG + surgery 31–80
Kidney stones Recurrence Pharmacotherapy 63–80
BPH AUR PROSCAR 57Surgery PROSCAR 55
Slide V.7
PTCA = percutaneous transluminal coronary angioplasty; CABG = coronary artery bypass graft; BCG = bacillus Calmette-Guérin
Adapted from Roehrborn CG et al Urology 2000;56:9-18. McConnell et al N Eng J Med 1998;338(9):557-563.

PSC 2001-W-11666-SS
PSA and PROSCAR™
• Predictably reduces PSA by 50% in men with BPH
• Multiplication of PSA values by 2 in men treated for 6 months preserves predictive value of PSA measurements
Slide V.8
In PLESS, PROSCAR did not mask prostate cancer detected by PSA

PSC 2001-W-11666-SS
Time-Tested Clinical Benefits of PROSCAR™: Summary
• Evidence-based medicine calls for clinical studies of individual drugs that investigate efficacy and disease outcomes.
• Outcomes studies with drugs for clinical BPH should evaluate effects on AUR and BPH-related surgery.
• Multicenter, double-blind, placebo-controlled trials of up to 6 years’ duration have established the effects of PROSCAR:– Durable improvements in symptoms, prostate volume,
and maximum urinary flow (p0.05) over 1 to 4 years vs. placebo
– Significant reductions in the risk of AUR and BPH-related surgery (p<0.001) at 4 years vs. placebo in PLESS
• No other therapy—including alpha blockers—proven to reduce AUR
Slide V.9

PSC 2001-W-11666-SS
New Data on the Long-Term Efficacy and Tolerability of PROSCAR™
Section VI

PSC 2001-W-11666-SS
Long-Term Experiencewith PROSCAR™
• Sustained improvements over 7 years of therapy– Reductions in symptom scores– Sustained reductions in prostate volume
25% reduction at year 7– Sustained increases in urinary flow
2.5 ml/sec increase at year 7
• Consistent safety and tolerability profile over 8 years of therapy
Slide VI.1
Data on file, MSD.

PSC 2001-W-11666-SS
Efficacy of PROSCAR™ in Younger vs. Older Men with Clinical BPH (PLESS Subanalysis)
Slide VI.2
Adapted from Kaplan SA et al Urology 2001;57(6):1073-1077.
Younger men(<65 years)
Placebo(n=774)
PROSCAR(n=786)
201816141210
86420F
our-
year
pro
bab
ilit
y of
AU
Ran
d/o
r n
eed
ing
surg
ery
0 1 2 3 4
Year
51% riskreduction(p<0.001)51% risk
reduction(p<0.001)
• PROSCAR significantly reduced the incidence of AUR and BPH-related surgery in younger and older patients at 4 years (p<0.001).
Older men(65 years)
Placebo(n=742)
PROSCAR(n=738)
Fou
r-ye
ar p
rob
abil
ity
of A
UR
and
/or
nee
din
g su
rger
y
201816141210
86420
0 1 2 3 4
Year

PSC 2001-W-11666-SS
Rapid and Sustained Reduction in the Risk of Long-Term Outcomes with PROSCAR™
Double-blind study Open-label extension
Slide VI.3
n values indicate number of patients completing each trial phase
Adapted from Roehrborn CG et al. Poster 419.
Placebo (n=1503)PROSCAR 5 mg (n=1513)
Placebo PROSCAR 5 mg (n=858)PROSCAR 5 mg PROSCAR 5 mg (n=979)
5
4
3
2
1
0
Yea
rly
% o
f A
UR
an
d/o
r B
PH
-rel
ated
su
rger
y
1 2 3 4 5 6
Study year
3.7
1.9
4.4
2.1
3.3
1.0
3.0
2.0
1.00.7
1.4 1.3

PSC 2001-W-11666-SS
PROSCAR™ Significantly Reduced Bother Over Long-Term Therapy (4 Years) (PLESS Substudy)
Slide VI.4
*p<0.05 PROSCAR vs. placebo at every time point after 4 months to 1 year and p<0.001 PROSCAR vs. placebo every 4 months, years 1 to 4**Significant improvement vs. baseline with PROSCAR and placebo at 4 years, p<0.001
PSA = prostate-specific antigen
Adapted from Bruskewitz R et al Urology 1999;54:670-678.
Overallbother score*,** By baseline PSA tertile (ng/ml)
Placebo(n=1503)
PROSCAR
5 mg(n=1513)
PSA: 0–12 PSA: 0–1.3 PSA: 1.4–3.2 PSA: 3.3–12
1 2 3 4 1 2 3 4 1 2 3 4 1 2 3 4
Year of follow-up
0
–1
–2
–3
–4
Mea
n (
±SE
) ch
ange
inb
oth
er s
core
fro
m b
asel
ine

PSC 2001-W-11666-SS
PROSCAR™ Had No Effect on Bone Mineral Density (BMD) (PLESS Substudy)
Slide VI.5
p = NS between treatments
Adapted from Matsumoto AM et al J Urol 2002;167:2105-2108.
1.12
1.10
1.14
1.13
1.15
1.14
1.13
1.12
1.11
1.10
1.09
1.08 Baseline End of study
BM
D (
g/cm
2 )
PROSCAR (n=63)
Placebo (n=54)

PSC 2001-W-11666-SS
New Data on the Long-Term Efficacy and Tolerability of PROSCAR™: Summary
• PROSCAR maintains clinical improvements over long-term therapy– Sustained reductions in symptom scores and prostate volume
and increases in urinary flow over 7 years – Durable effects up to 10 years – Similar effects in older vs. younger men– Reductions in risk of outcomes maintained over 6 years– Significant reductions in bother due to BPH symptoms at 4 years
(p<0.001 vs. placebo)
• PROSCAR is well tolerated over long-term therapy– Consistent safety/tolerability profile through year 7 – No effect on BMD
Slide VI.6

PSC 2001-W-11666-SS
The Patient-Physician Connection
Section VII

PSC 2001-W-11666-SS
Patient Satisfaction Is Important in the Treatment of Clinical BPH
• Treatment selection in BPH should take into account– Patient’s perception of the impact of BPH on
quality of life– Patient’s ability to deal with bother caused
by symptoms– Patient’s attitudes toward risk of possible
complications
Slide VII.1

PSC 2001-W-11666-SS
The Physician’s Rolein Patient Education
• Physicians should involve patients with BPH in the choice of therapy
• Patient education should include discussions of– The natural history of BPH (including potential
for serious complications)– Benefits, risks, and costs of alternative approaches
Slide VII.2

PSC 2001-W-11666-SS
Combination Therapyfor Clinical BPH
Section VIII

PSC 2001-W-11666-SS
Combined Therapy with PROSCAR™ and an Alpha Blocker (terazosin) for Clinical BPH
Slide VIII.1
p<0.05 PROSCAR + terazosin vs. either agent used alone at 12 months
Adapted from Savage SJ et al Can J Urol 1998;5(3):578-584.
20
18
16
14
12
10
8
0 2 4 6 8 10 12
Time (months)
Mea
n I
PS
S
PROSCAR 5 mg/day
Terazosin titrated to 5 mg
Combination

PSC 2001-W-11666-SS Slide VIII.2
Discontinuation of Alpha Blockade After Combined Therapy with PROSCAR™ and
an Alpha Blocker (doxazosin) for BPH
Adapted from Baldwin KC et al Urology 2001;58(2):203-209.
Su
cces
s ra
tes
afte
r d
isco
nti
nu
atio
n
(% o
f p
atie
nts
)
100
80
60
40
20
0 3 months 6 months 9 months 12 months
Doxazosin 2 mg (n=25)
Doxazosin 4 mg (n=20)
Doxazosin 8 mg (n=15)
2015 13
4845
40
8480
73
84 85 87
Time after discontinuation
PSC 2001-W-11666-SS
Combined Therapy with PROSCAR™ and an Alpha Blocker for Clinical BPH: Summary
Slide VIII.3
• Enhanced relief of symptoms
• After withdrawal of alpha blocker– Satisfaction (success) rates maintained
87% after 12 months in one study

PSC 2001-W-11666-SS
Other Emerging Usesof PROSCAR™
Section IX

PSC 2001-W-11666-SS
63
PROSCAR™ Decreases the Risk of Hematuria
Slide IX.1
*p<0.05 between groupsPROSCAR is not indicated for treatment of BPH-related hematuria.
Adapted from Foley SJ et al J Urol 2000;163:496-498.
Control (n=27)
PROSCAR (n=28)
70
60
50
40
30
20
10
0
% o
f m
en
Hematuria*at 1 year
Hematuria requiring surgery
at 1 year
14
0
26

PSC 2001-W-11666-SS
Pretreatment with PROSCAR™ Decreases Perioperative Bleeding Associated with TURP*
Slide IX.2
*PROSCAR was given 2–4 months before TURP.PROSCAR is not indicated for pretreatment before prostate surgery.
Adapted from Hagerty JA et al Urology 2000;55:684-689.
Total group <30 g resected 30 g resected
40
35
30
25
20
15
10
5
0
% o
f p
atie
nts
wit
h b
leed
ing
Placebo
PROSCAR
(n=25) (n=12)
8.3
0
4
(n=13)(n=50) (n=19)
14
36.8
0
(n=31)

PSC 2001-W-11666-SS
Other Emerging Usesof PROSCAR™: Summary
• Extended benefits of PROSCAR in men with BPH – Reduced risk of hematuria and hematuria-related
surgery– Improved outcomes when used prior to BPH-related
surgery
• PROSCAR is not currently indicated for these uses.
Slide IX.3
PROSCAR is not currently indicated for these uses.

PSC 2001-W-11666-SS
Summary
Section X

PSC 2001-W-11666-SS
Overall Summary and Conclusions
• BPH, a multifactorial disorder characterized by an enlarged prostate, LUTS, and BOO, can lead to serious clinical outcomes (AUR and BPH-related surgery).
• PROSCAR™ is a competitive and specific inhibitor of type II 5-reductase, which mediates the conversion of testosterone to DHT.
• PROSCAR reduces BPH symptoms and prostate size, improves urinary flow, and decreases the risk of AUR and BPH-related surgery.
• PROSCAR slows the progression of BPH.
• The clinical effects of PROSCAR have been established in clinical trials of up to 7 years’ duration.
Slide X.1

PSC 2001-W-11666-SS
Bibliography
• See Notes page

PSC 2001-W-11666-SS
Bibliography (cont’d)
• See Notes page

PSC 2001-W-11666-SS
Before prescribing any of the products mentioned
in this slide presentation, please consult the manufacturer’s
prescribing information.
Copyright © 2002 Merck & Co., Inc., Whitehouse Station, NJ, USA.
All rights reserved. 7-03 PSC 2001-W-11666-SS Printed in USA
VISIT US ON THE WORLD WIDE WEB AT http://www.merck.com
Clinical BPH and Its ManagementA Comprehensive Slide Kit