clinical aspects of cancer staging and pathologystaging and … · 2019-02-26 · clinical aspects...
TRANSCRIPT

Clinical Aspects of Cancer Staging and PathologyStaging and Pathology
Simon J Hall MDChairman Department of UrologyChairman, Department of Urology Director, Deane Prostate Health & Research CenterMount Sinai School of MedicineMount Sinai School of MedicineNew York, New York

Wh t i C n r?What is Cancer?
Local Behavior Local Behavior Lack of contact inhibition Invade surrounding organsg g
Metastasis The ability to grow outside home environment So called “seed and soil phenomenon”
Lymphatic spread Hematogenous spread
Stage & Grade TerminologyStage & Grade Terminology
Staging: Clinical Measure of Disease Physical Exam Radiographic Imaging Pathology: depth of invasion –metastases
Pathologic Grading: Marker of Behavior Based on pathologist Based on pathologist Novel molecular markers

R di r phi St inRadiographic Staging
44M with obesity and type II DM referred 44M with obesity and type II DM referred for incidentally found left renal mass.
PMHx: DM, Dyslipidemia, ys p de a SurgHx: Hydrocelectomy Medications: Glipizide Medications: Glipizide Allergies: NKDA Social: 1-2 PPD x 20 years Social: 1 2 PPD x 20 years




















12/21/07L i R di l NLaparoscopic Radical Nx Clear cell RCC, grade 2. Clear cell RCC, grade 2. 6.0cm in greatest dimension. Invasion of the Renal Vein Invasion of the Renal Vein. Negative surgical margins.
pT3NxM0 Excellent correlation of Clinical and Excellent correlation of Clinical and
Pathological staging

MS-05-08360 3/3/05P il L iPenile Lesion
62 year old male presents with a penile lesion of 6 months duration. No pain.PMH & PSH i PMH & PSH negative
Medication: None PE: uncircumsized with some tightness;
2cm red raised lesion on glans of penis.




P il S C ll C rPenile Squamous Cell Cancer Pathology: Squamous cell carcinoma in Pathology: Squamous cell carcinoma in
situ (Bowen’s disease) with foci of invasive squamous well differentiated SCC.
Clinical Dx: SCC – unable to stageg Pathological Dx: Stage T1 SCC

U l i P th l P t t DiUrologic Pathology: Prostate Disease

Pathologic Upstaging: Prostate DiseaseI li ti f P iti M iImplications of Positive Margins
Types of Positive ypmargins True extracapsular
extensionextension Iatrogenic – surgeon
cut into prostate Focal vs broad Focal vs broad
Natural History of Positive margins PSA recurrence
30-50% by 5 years 30 50% by 5 years
Urologic Pathology: Prostate Disease T t t f P iti M iTreatment of Positive Margins
Surveillance Surveillance Radiation Therapy
60-64 Gy to prostate bed 60 64 Gy to prostate bed
EORTC 22911 SWOG8794 EORTC 22911 SWOG8794 74% vs 52% 73 vs 44% (PSA progression free)
Ganswindt et al EUR Urol 2008

U l i P th l R l MUrologic Pathology: Renal Masses
Incidental Renal Masses
Urologic Pathology: Renal Masses
Pathology of Small Incidental Masses (2cm) Pathology of Small Incidental Masses (2cm) 25% Oncocytoma 20% Chromophobe RCCsp
Treatment Options Surveillance Cryotherapy Partial nephrectomy

Urologic Pathology: Renal MassesE l i P diEvolving Paradigm
Indications for Biopsy Indications for Biopsy History other cancer
Esp. if other ? Mets seen
Enlarged Lymph Nodes Unclear if Resectable
Treatment OptionsS i t Surgery mainstay
Observation vs MIS Need for pathologic diagnosis. Need for pathologic diagnosis.

Urologic Pathology: Renal MassesC Bi S ffiCan a Biopsy Suffice

C r M h i f I d tiCancer: Mechanism s of Induction Genetics Genetics
Knudsen’s 2 hit theory Inherited disorders vs sporadicp
Risk factors: Smoking Chronic inflammation UV radiation

C P i F il S dCase Presentation: Family Syndromes Pt is a 33 y.o male who presented to the Pt is a 33 y.o male who presented to the
ER 10/28 with c/o headache and dizziness for two months.
Difficulty walking, “feeling unsteady” No nausea or vomitingg No change in vision or hearing.
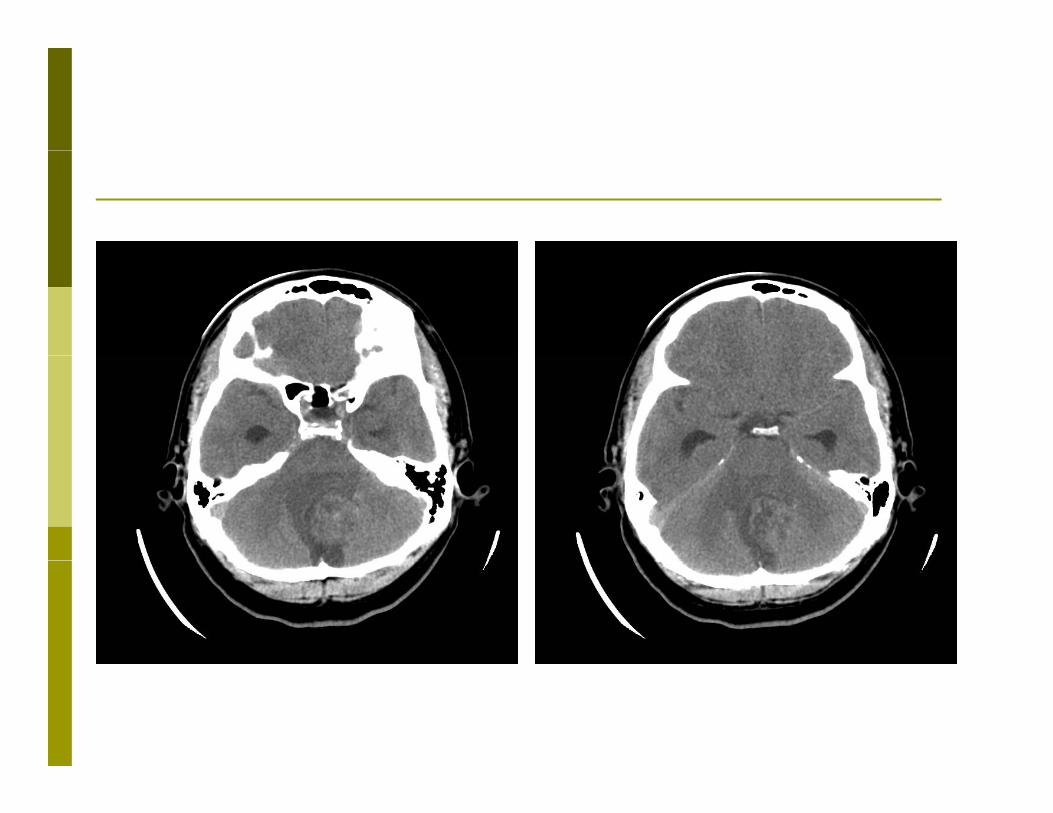
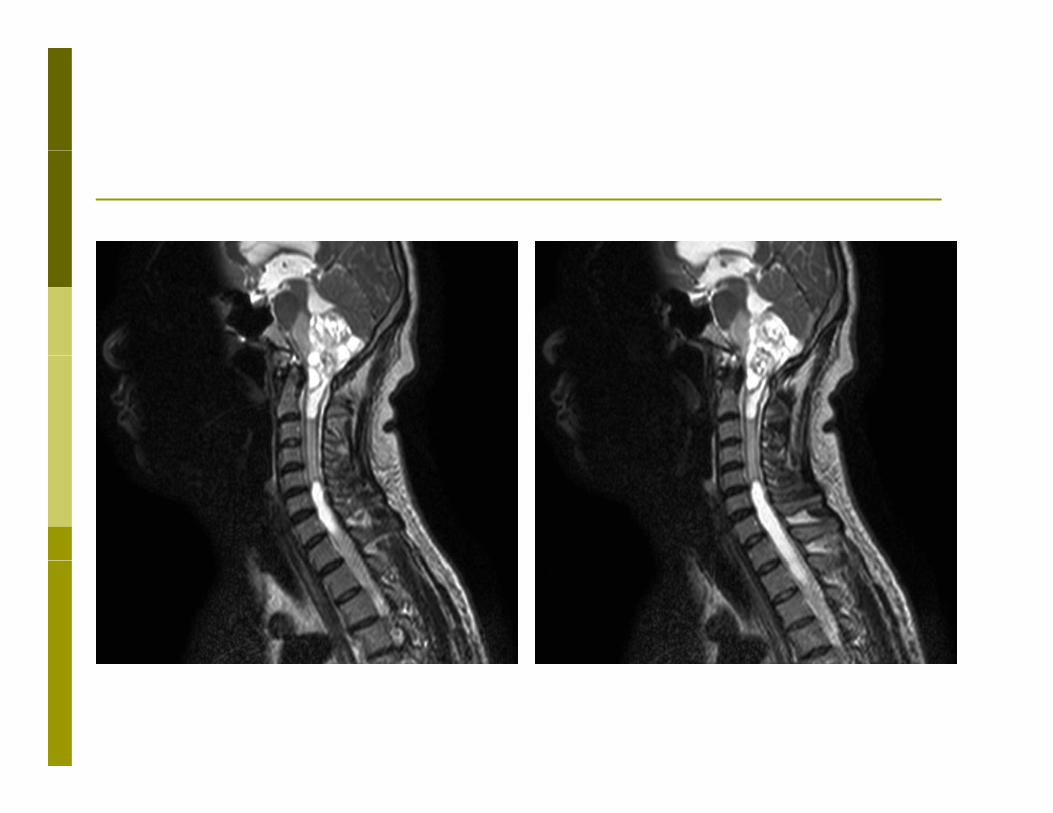
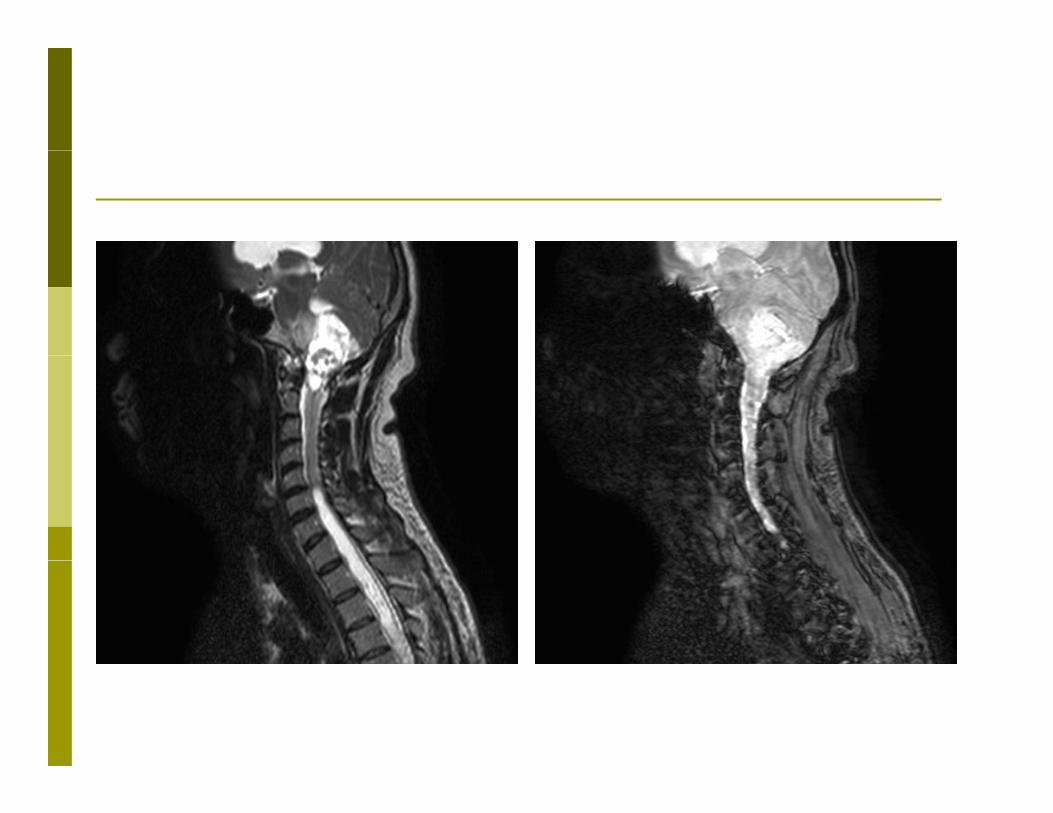

Br i T r C r b llBrain Tumor: Cerebellum Patient with large foramen Patient with large foramen
magnum/cerebellar tumor with obstruction of the ventricular outflow foramen and hydrocephalus.
Enhancing lesions at C5 and C6 Large syringomyelia type cystic cavity at
C1 and C2 and a second larger l dsyringomyelia type cystic cavity extending
from C5 to thoracic spinal cord.
Abd i l S r i f r VHLAbdominal Screening for VHL

Abd i l S r i f r VHLAbdominal Screening for VHL

Abd i l S r i f r VHLAbdominal Screening for VHL
Abd i l S r i f r VHLAbdominal Screening for VHL

Abd i l S r i f r VHLAbdominal Screening for VHL
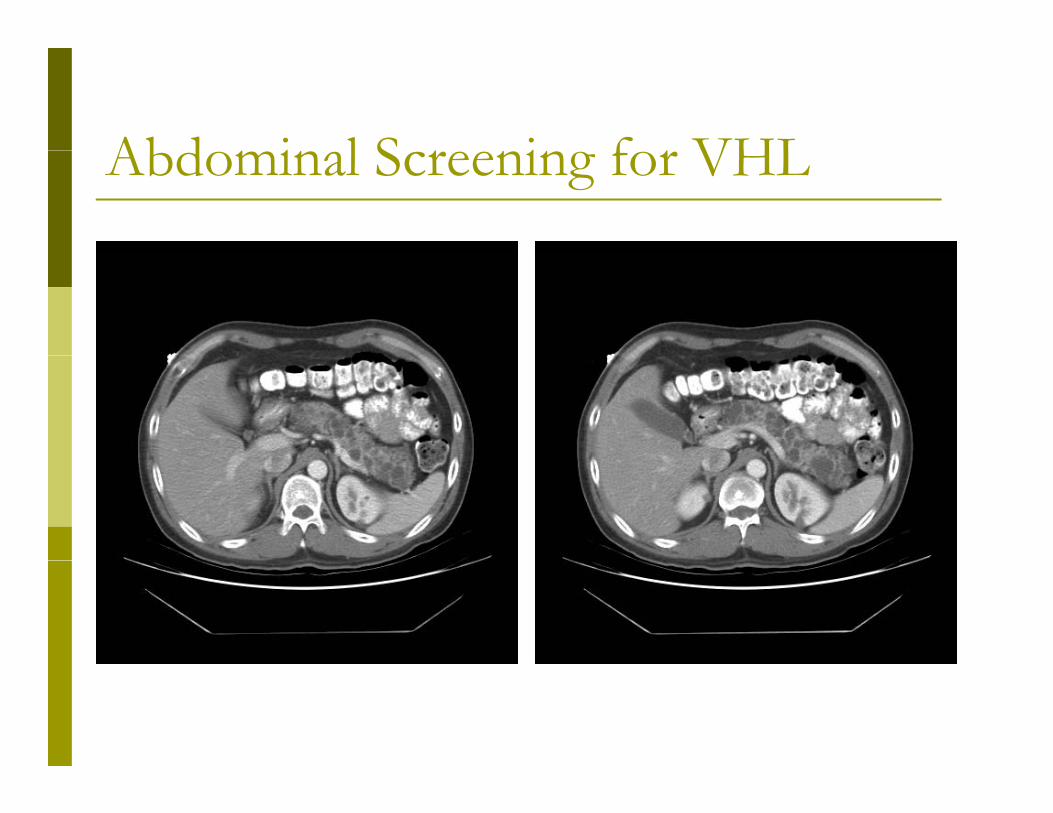
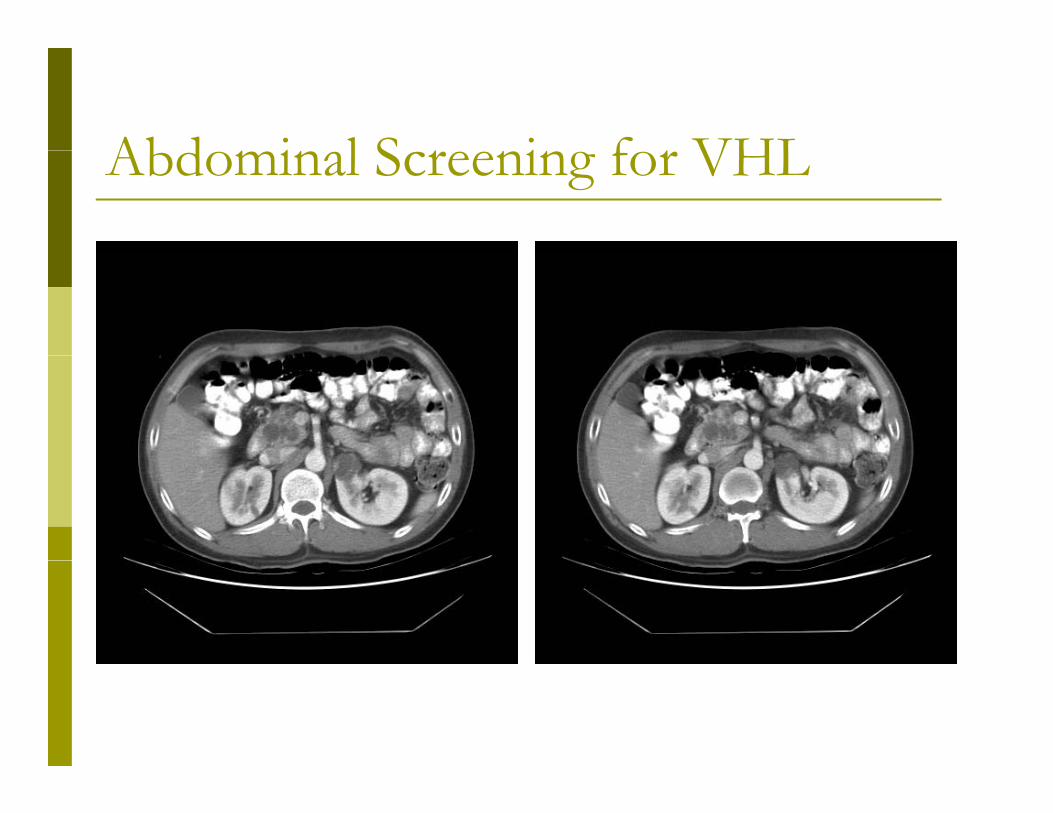
I i R ltImaging Results Enhancing 2 x 2 cm right lateral upper Enhancing 2 x 2 cm right lateral upper
pole renal mass. 3 cm medial enhancing rt mid pole mass3 c ed a e a c g t d po e ass 2 cm complex cyst left upper pole w/
enhancing mural nodule and septal g penhancment.
Multiple bil renal cysts Multiple cystic pancreatic lesions Normal Adrenals

P ti t Hi t rPatient History 10/31 –Given the large extent of CNS 10/31 Given the large extent of CNS
disease, Neurosurgery placed a VP shunt with no plans for surgical excision of the tumors.
2/2/06 – Pt seen by genetics Heterozygous for a T to C mutation at
nucleotide 479 if the VHL gene.

VHL Ur l i l W rk pVHL Urological Work up referred for bilateral renal masses and referred for bilateral renal masses and
diagnosis of VHL Patient reports no more HA, dizziness.at e t epo ts o o e , d ess Family history – sister with similar cysts in
pancreas and kidney “being followed in p y gNJ”

V Hipp l Li d S drVon Hippel Lindau Syndrome Genetic Disorder Genetic Disorder
Brain Tumors: cerebellum Brain Tumors: cerebellum Cystic lesions: liver, pancreas, kidney Pheochromocytomas Pheochromocytomas Renal Cell Cancers Cystadenomas of epididymis Cystadenomas of epididymis

PT CHPT CH Pt is a 74 Y Female with a long history of Pt is a 74 Y Female with a long history of
gross hematuria. Pt ignored symptoms for 1-2 years.t g o ed sy pto s o yea s Pt has no definite risk PMHx significant for arthritis and macular PMHx significant for arthritis and macular
degeneration. Pt reported to Elmhurst ER for evaluation Pt reported to Elmhurst ER for evaluation
during an episode of gross hematuria.

Pt CHPt CH Pt was hemodynamicly stable.y y Abd: soft. No CVAT Gyn: palpable but mobile mass appreciated
anterior to vaginal wall with out evidence of anterior to vaginal wall with out evidence of cervical disease
Creatinine 1.4 Hct 29.5 UA: blood Ucx: no significant growth Ucx: no significant growth CT obtained





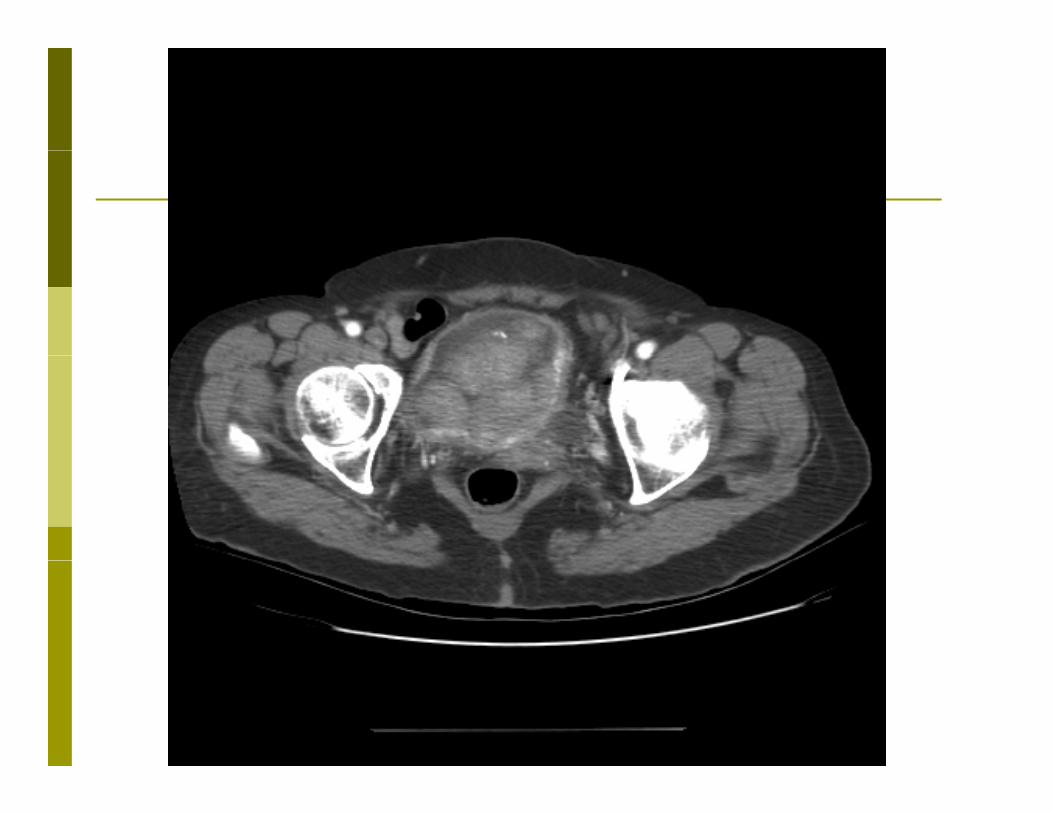


TURBTTURBT Given CT findings pt was brought for TURBT after g p g
cardiac clearence. Extensive tumor was found that:
Obscured the UOs and trigone Obscured the UOs and trigone Involved the left and right lateral bladder wall Circumferential bladder neck involvement Involvement of the proximal urethra Involvement of the proximal urethra
Partial resection was performed for tissue diagnosisl dd k d h d Bladder neck and urethra were not resected to
preserve sphincter.
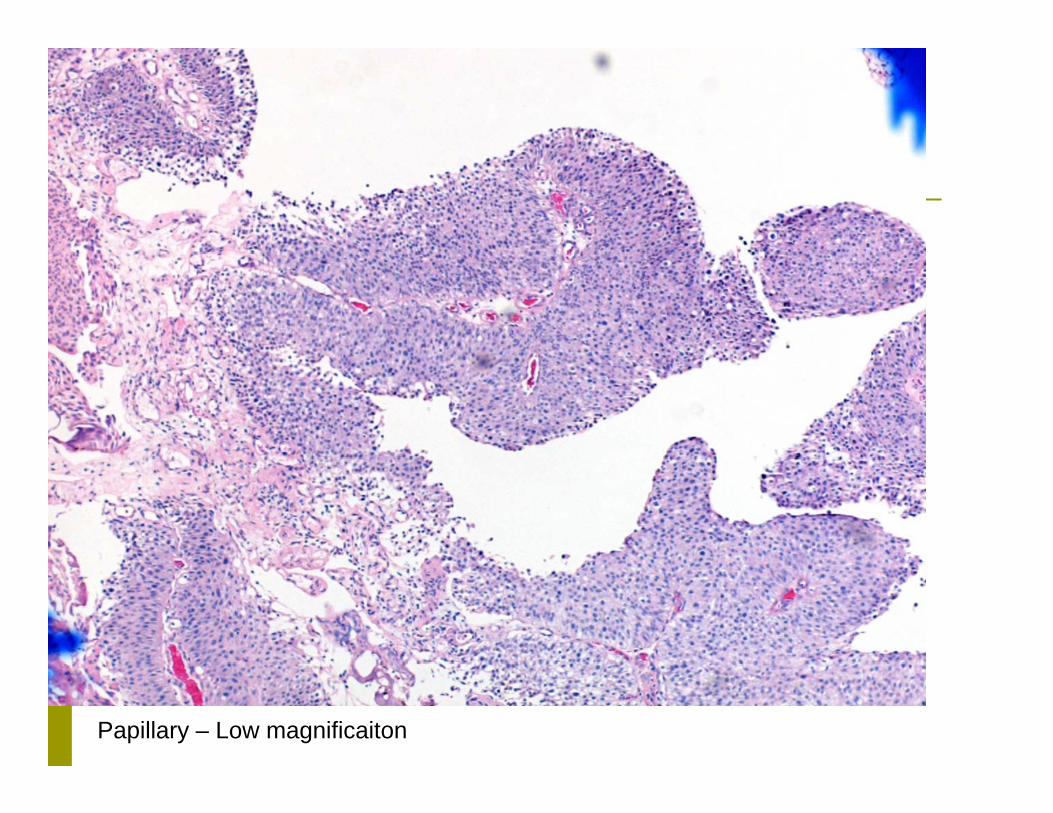
Papillary – Low magnificaiton

Invasion into lamina propria

Atypical Nuclei
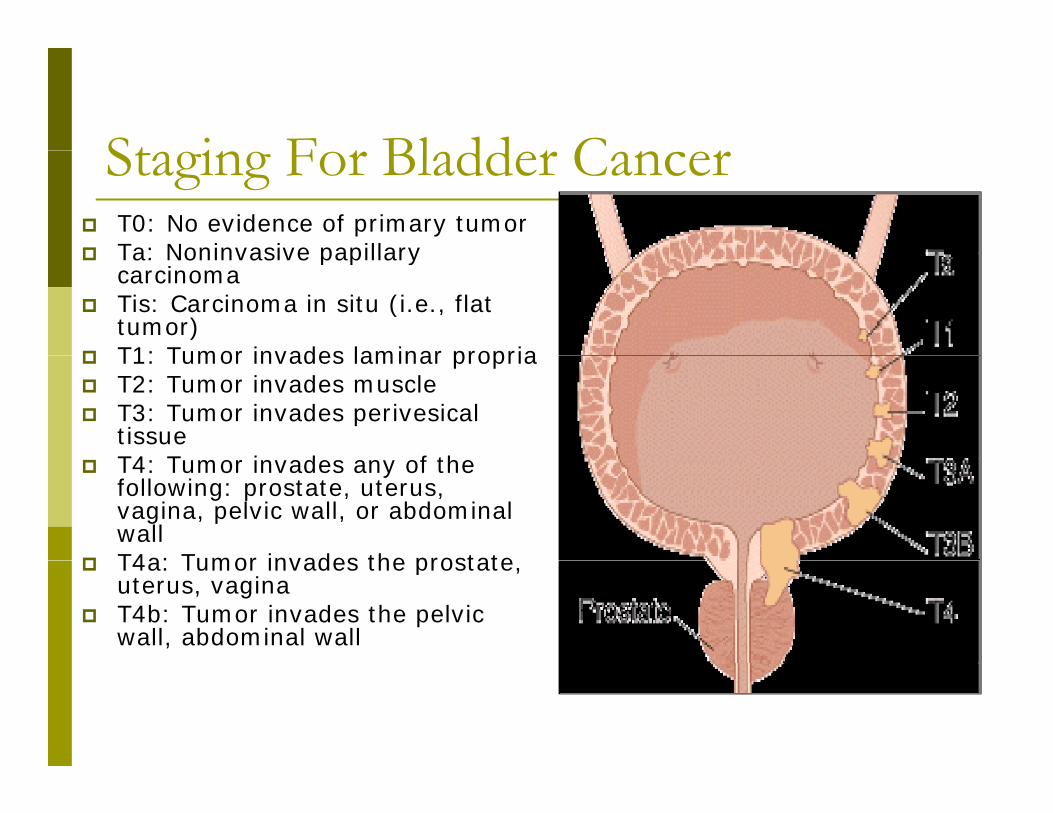
St i F r Bl dd r C rStaging For Bladder Cancer T0: No evidence of primary tumor Ta: Noninvasive papillary Ta: Noninvasive papillary
carcinoma Tis: Carcinoma in situ (i.e., flat
tumor) T1: Tumor invades laminar propria T1: Tumor invades laminar propria T2: Tumor invades muscle T3: Tumor invades perivesical
tissueT4 T i d f th T4: Tumor invades any of the following: prostate, uterus, vagina, pelvic wall, or abdominal wall
T4a: Tumor invades the prostate T4a: Tumor invades the prostate, uterus, vagina
T4b: Tumor invades the pelvic wall, abdominal wall

N I i Bl dd r C rNon-Invasive Bladder Cancer Approximately 70-80 % of bladder cancer pp y
present as superficial cancer About 10-20 % of superficial cancers progress to
l i i l imuscle invasive lesions Grade and stage influence recurrence and
progressionprogression Low grade Ta: 50-70 % recur, 5 % progress High grade T1: 80 % recur, 50 % progress (3y)
CIS 50% develop muscle invasive disease (5y) CIS- 50% develop muscle invasive disease (5y)

I iti l M tInitial Management Most patients with localized disease undergo a p g
TUR for diagnosis and staging The efficiency of the TUR may be less than
ll dgenerally presumed Residual disease may be seen in up to 40-70% of cases
if repeat TUR is done with weeks
T1 tumors may show worsening prognosis in up to 25 % on repeat TUR, and repeat TUR should be done if no muscle is identified on initial be done if no muscle is identified on initial pathology
FAFA 21 M presents to ER with cc of abdominal 21 M presents to ER with cc of abdominal
pain HPI:
vague abdominal pain x 3 weeks (dull, worsening)
Mild R flank pain, no fever, no N/V, possible 5 lb weight loss last month
slowly growing L testicular mass x 2 months slowly growing L testicular mass x 2 months. No other c/o

FAFA PMHx: No cryptoorchidism PSurgHx: none FHx: N/C Meds: tylenol for pain Meds: tylenol for pain
PEGeneral: no cachexia, thin, NADGeneral: no cachexia, thin, NADPulm: slight expiratory wheeze b/lAbd: mass R lateral/superior to umbilicus. NT/ND,
+BS. Minimal + R flank

FAFA GU:
normal DRE L testicle superior pole/ epididymal mass – well
circumscribed, indurated, not mobile. No masses b/l testes, small transilluminating area inferior
R testes
Labs: WBC, chem WNL. Crea 0.7 UA: nitrate neg, LE neg, blood neg LFT’s: wnl
ER CT scan obtained
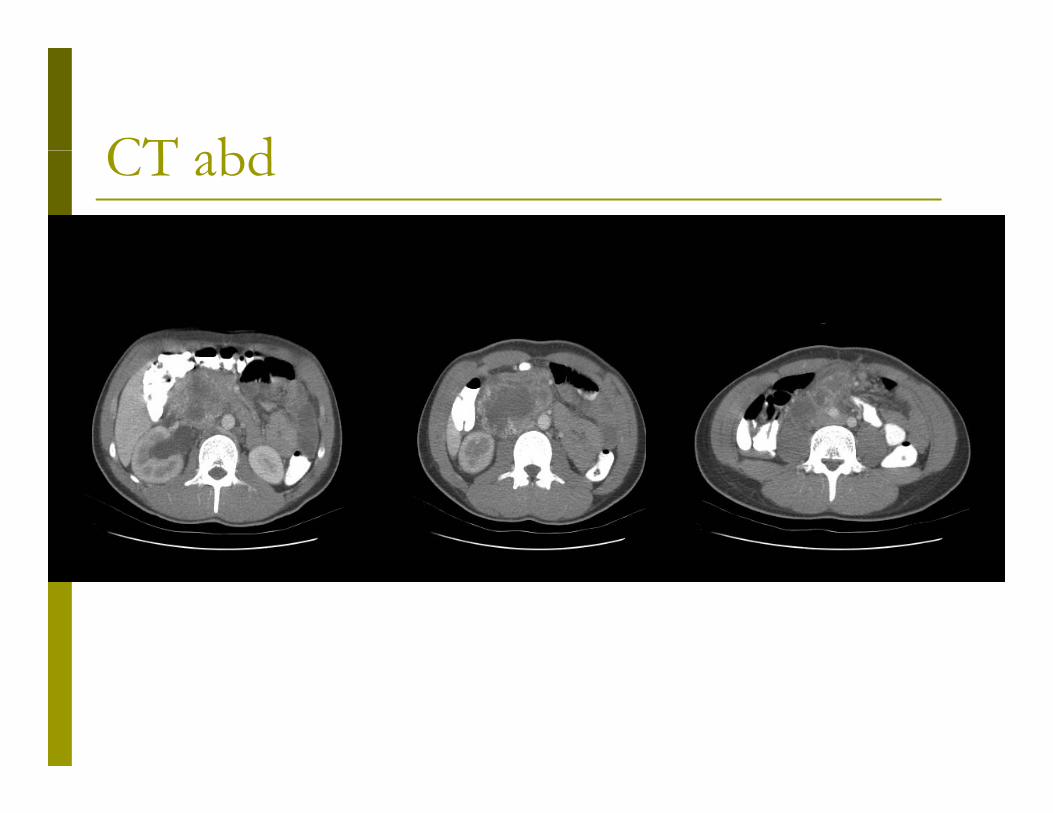
CT bdCT abd

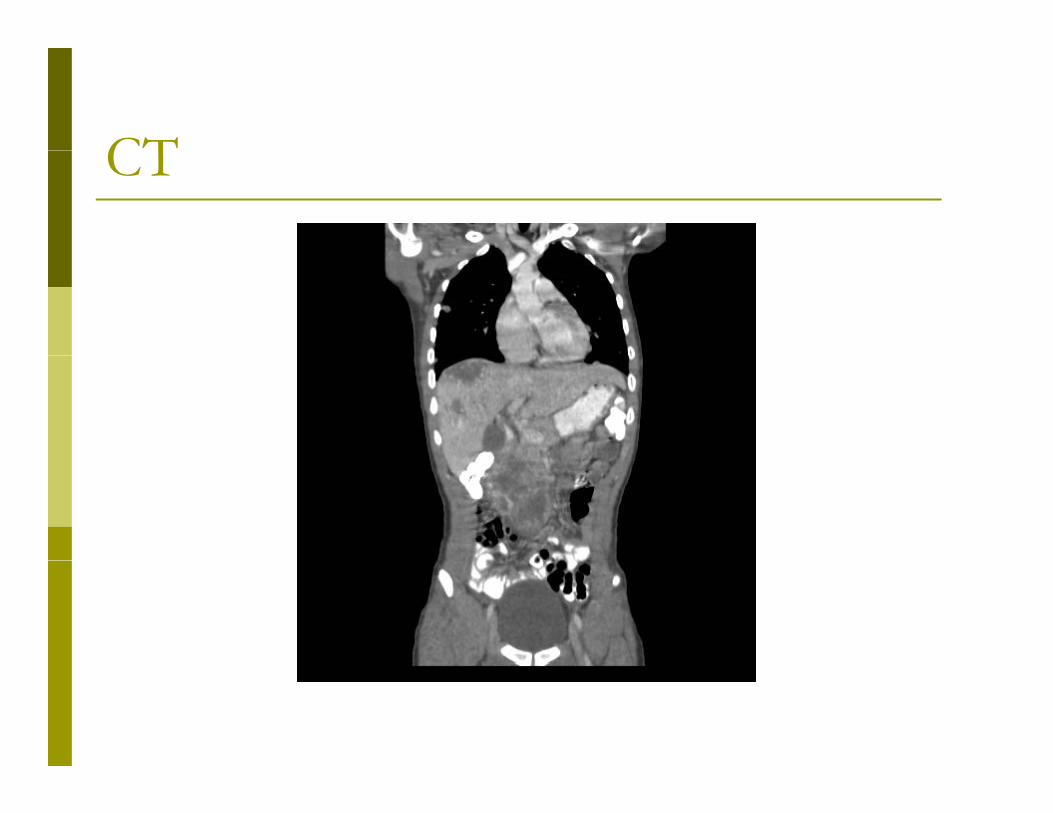
CTCT
CTCT

FAFA CT: CT:
multiple b/l lung masses massive necrotic retroperitoneal p
lymphadenopathy causing R renal obstrxn Massive hypodense liver lesions

GUGU Tumor markers Tumor markers
BhCG: >200,000 LDH: 648 AFP: 3
Possible L inguinal orchiectomy pending U/S

U/SU/S

U/SU/S No discrete testicular mass No discrete testicular mass R-sided microlithiasis b/l hydroceles R>L b/l hydroceles R>L Small varicoceles b/l
FAFA Surgery cancelled on presumptive Dx of Surgery cancelled on presumptive Dx of
extragonadal GST CT-guided biopsy:C gu ded b opsy
Choriocarcinoma
JJ stent on R Pt started on chemotherapy
T ti l r MTesticular Mass 24 yo male graduate student noted a 24 yo male graduate student noted a
painless mass in right testis. No increase in size since noted; no h/o trauma
or STDs
PE: firm nodule on lower pole of testis USG: tumor in lower pole of Testis Markers: AFP, HCG and LDH negative





Fi l Di iFinal Diagnosis Sertoli cell tumor Sertoli cell tumor
• 0.6 cm cm circumscribed• Limited to the testis• No vascular or lymphatic invasion• Resection margin negative for tumor• Adjacent testicular tissue with reduced spermatogenesis

Methods of Disease ScreeningMethods of Disease ScreeningA Two Part ProcessA Two Part Process
Di ti T t Diagnostic Test Picks up disease before clinically apparent
Treatment Intervention Prolongs Survivalg Impacts on Pain and Suffering
Prostate Cancer ScreeningProstate Cancer ScreeningDiagnostic test: PSADiagnostic test: PSA
Intervention: RRP or Radiation Therapy
If cure is possible is it necessary?If cure is possible, is it necessary? - if cure necessary, is it possible?
Willet Whitmore 1988

PSA & Prostate CancerPSA & Prostate Cancer Levels of PSA Levels of PSA
Catalona WJ et al, JAMA, 1998

Specificity & Sensitivity (ROC) of PSA f D t ti P t t CPSA for Detecting Prostate Cancer
ROCs comparing percent free prostate-specific antigen (PSA) to total PSA in reflex range subset of 4.1 to 10.0 ng/mL. Areas under the receiver operating characteristic curves for percent free PSA and total PSA are 0.71 and 0.52, respectively (P<0.05).
Vashi et al Urology 1997

Cancer Detection in PCPT R dl f PSARegardless of PSA
15% PSA <4.0 had cancer24% PSA 2.1-3.027% PSA 3.1-4.0 Thompson et al NEJM 2004

PSA Screening: Threat of Over DiagnosisThreat of Over Diagnosis Definition of Over Diagnosis Definition of Over Diagnosis
Disease which will not yield symptoms before death
Disease in those who die prior to clinical diagnosis
Over diagnosis in 18-44%
Draisma G et al JNCI, 2003Yao & Yao, JNCI, 2003

Has Use of PSA Affected Mortality?Has Use of PSA Affected Mortality?
Chu KC et al, Cancer, 2003
White males: 27% decrease A A males: 17% decrease

Underlying Cause of Lower Mortality in PSA EraMortality in PSA Era
D d M t lit M t t ti DiDecreased Mortality - Metastatic DiseaseLinked to
Decreased Incidence not Survival of Patients with Metastatic Disease
Chu KC, Cancer, 2003
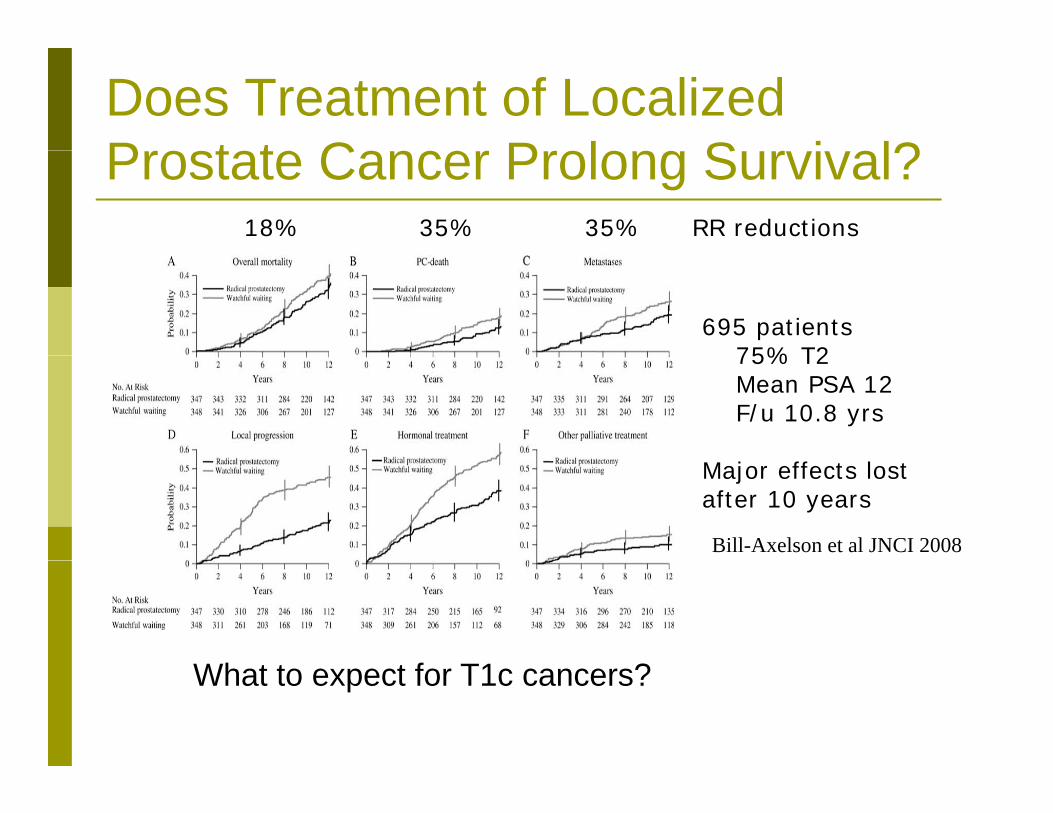
Does Treatment of Localized P t t C P l S i l?Prostate Cancer Prolong Survival?
18% 35% 35% RR reductions
695 patients75% T275% T2Mean PSA 12F/u 10.8 yrs
Major effects lost after 10 years
Bill-Axelson et al JNCI 2008
Wh f T1 ?What to expect for T1c cancers?

C # 1Case # 1 54 yo man with PSA 5.8 (16% free) 54 yo man with PSA 5.8 (16% free)
Last year it was 3.5 Has IPSS 18 Normal DRE
TRUS + PNB 52cc gland Gleason 3+3 - <5% one core
L Ri k T1Low Risk T1c Expectant Management Expectant Management Radical Prostatectomy Seed Implant Seed Implant External Beam Radiation Therapy
Repeat Biopsy: 2 months later <5% Gleason’s 3+3 <5% Gleason s 3+3

S d Opi iSecond Opinion
Expectant Management + Uroxatral (afluzosin)
7/03 8/03 5/04 8/04 11/04 3/05 6/05 9/05 1/06 4/06 7/06 11/06 1/07
PSA 5.9 4.1 4.39 5.9 3.6 5.7 5.7 5.4 5.29 5.25 4.36
%Free 16% 25% 19% 19
Biopsy 3+3 <5%
3+3 <5%
BPHBPH

More Conservative AS CriterionM nt Sin i E p ri nMount Sinai Experience
More Conservative Biopsy Criterion 50 patients: 60+/-7.4
yrs’ PSA 5 8 47 T1c
Confirmatory Biopsy Results (n=50)
2225
yrs PSA 5.8, 47 T1c 44 had 1 core involved;
6 had 2 cores 40 <5% 8 5 10% 1
17
15
20
40 <5%, 8 5-10%, 1 15%, 1 20%
All re-biopsied before moving to AS
64
0
5
10
moving to AS 0No CancerSampled
No Change orvolume
decrease
VolumeIncrease
GradeIncrease

Active SurveillanceTh M t Si i E p riTheMount Sinai Experience
1st Surveillance Biopsy Results (n=22)Table 3.Review of Outcomes
50%
36%
30%
40%
50%
60% # of Patients % Treated
F/U (mont
hs)
Mount Sinai 36 8 24
9% 9%
0%
10%
20%
No CancerSampled
No Change orvolume
decrease
VolumeIncrease
GradeIncrease
UCSF 321 21 24
Klotz et al. 299 34 64
Warlick et al. 320 31 23
Hardie 2005 80 14 42decrease
25
30
12
14
0.3
0.35
Predictors of Treatment
Patel 2004 88 35 44
10
15
20
Perc
ent F
ree
PSA
(%)
19.618.1
4
6
8
10
PSA
(ng/
ml)
5.9
4.6
0.1
0.15
0.2
0.25
PSA
Den
sity
(ng/
ml/c
c)
0.12
0.15
Predictors of Treatment
0
5
No Treatment Treatment0
2
No Treatment Treatment 0
0.05
P
TreatmentNo Treatment