clinical applications of cbct
TRANSCRIPT
Clinical Aspect and Applications of
CBCT
Author: Lokender Yadavwww.lokender.in

What is CBCT or DVT ? A cone beam CT scanner uses x-rays and computer graphic interfaces to produce 3D cross sectional images of the
jaws and teeth. Through the use of a cone shaped x-ray beam, and ultra low dose function, the time needed forscanning and radiation exposure are all much reduced, compared to traditional methods.
The machine moves around the patient’s head in a circular motion in a similar way to the panoramic radiographyunits.
www.lokender.in
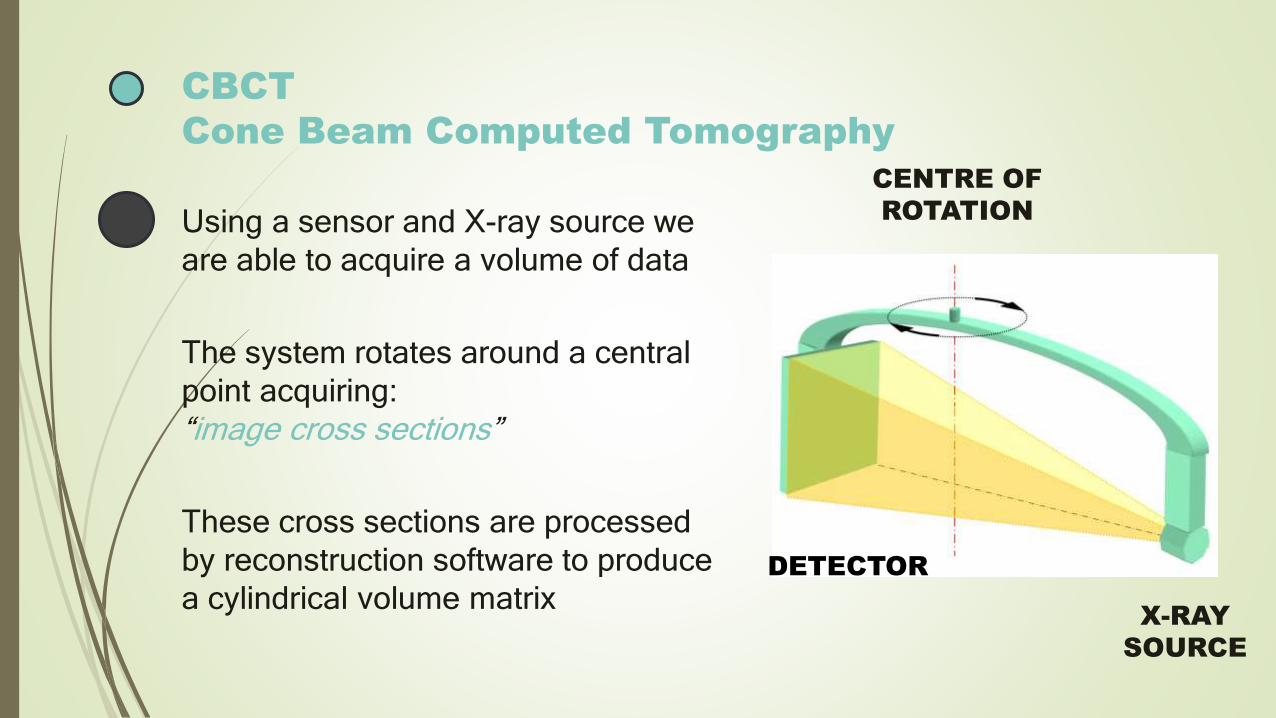
CBCT
Cone Beam Computed Tomography
X-RAY
SOURCE
DETECTOR
CENTRE OF
ROTATIONUsing a sensor and X-ray source we
are able to acquire a volume of data
The system rotates around a central
point acquiring:
“image cross sections”
These cross sections are processed
by reconstruction software to produce
a cylindrical volume matrix

The resulting volume is a cylinder of data,
◦ whose height would equal the height of the
detector
◦ and whose radius would equate the width of
the detector
“WOULD”
If magnification factor did not come into the
play
◦ this is the difference between detector size
and field of view
The reconstruction algorithm should take into
account the magnification factor thus ensuring
objects are represented as “true” size
FOCAL
POINT
DETECTOR SIZE IS GREATER THAN
FIELD-OF-VIEW SIZE

Field of View
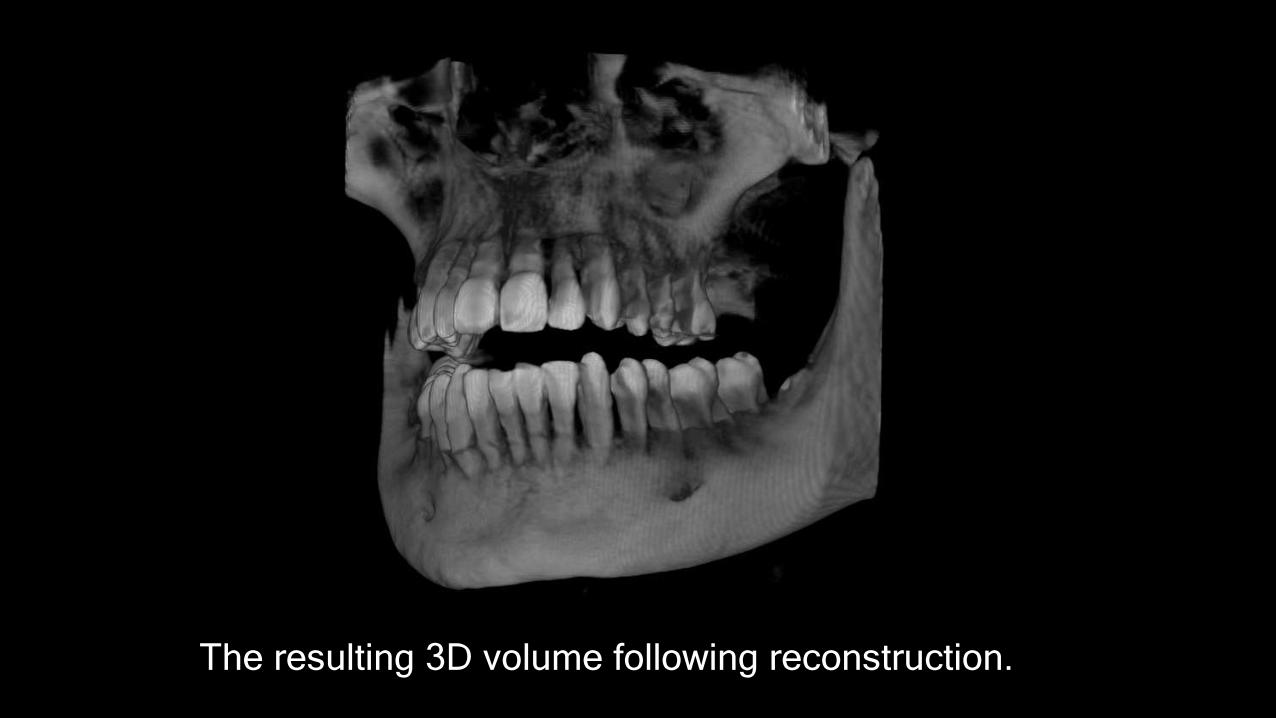
The resulting 3D volume following reconstruction.

Basic planes
AXIAL CORONAL SagittalGtIT
TALAxial Coronal

AXIAL CORONAL SAGITTAL

Displaying 3D aquisition
Following reconstruction the imaging software will show for example, the volume, projection
planes, MPR, simulated 2d, etc.
AXIALCORONAL
SAGITTAL2D


CBCT in dental Implantology..
◦ CBCT has revolutionized the way dental implant is
performed in dental clinics & hospitals.

Need of 3D in implant…
◦ To improve the overall success of implant therapy
with possible reduction in surgical and postoperative
implant complications, implantologist should 3D
information of :
◦ Bone volume
◦ Bone Topography
◦ Bone Density
◦ Proximity to anatomical structure

What doctor wanted to see as an implantologist?

Ridge Morphology :
◦ The Buccolingual ridge pattern cannot be viewed on 2D radiograph but CBCT come with advantage of showing the ridge pattern present.
◦ Ridge may be:
◦ Irregular
◦ Narrow Crestal
◦ Knife shape
◦ Case of Compromised jaw bone
◦ (quantity or quality)
◦ (2D is insufficient)

Quality of bone at site of implant
◦ The bone quality is most important marker/information for
implant planning(In determining the success of Implant),
◦ Type-1
◦ Type-2
◦ Type-3
◦ Type-4(higher chance of failure compare to other types of
bone)
◦ *Bone density is subjected to mineral density & bone
structure
CBCT-Guided Implant Surgery
Type and size of the planned implant, its position
with in the bone, its relationship to the planned
restoration can be determined before performing
surgery ,
◦ Implant Guide helps:
virtual planning
Allowing for more accurate and predictable implant
placement
Reduced Chances of Medical Errors

Requirement of Virtual Implant Planning
◦ Three or more implants in a row
◦ Proximity to vital anatomical structure
◦ Questionable bone volume
◦ Flapless implant placement
◦ Immediate placement
◦ Implant position that is critical to the planned
restoration
CBCT in oral and Maxillofacial surgery:

Third Molar Evaluation:
◦ Third molar removal in young adults reported frequently at
clinic's. IAN(Inferior Alveolar Nerve) is a serious complication in
third molar removal. So it becomes important to pre assess. In
case of overlapping impacted tooth with mandibular canal, IOPA
or Pano view provides a limited information

Maxillofacial Trauma
◦ Dentoalveolar fracture, Maxillary Bone fracture,Zygomatic fracture, Madibular Fracture, or gunshotinjuries .
◦ CBCT is more sensitive and accurate in imagingthe maxilla and mandible.
◦ It is reported that Mandibular Fractures that are notevident in conventional CT can be Identified usingCBCT.
◦ CBCT uniquely useful in the diagnosis of alveolarfractures.

Maxillofacial Region

Bone Graft Analysis:
◦ Volumetric analysis offers better prediction of defect
morphology(e.g. cleft palate) ,understanding the
morphology of a traumatic defect is critical in
developing the implant site before planned implant
placement.

Temporomandibular Joint Assessment
◦ TMJ disorders are often quite challenging.
◦ CBCT should be considered for:
◦ Limitation in mandibular movement and function
◦ Stiffness of jaw
◦ Pain in the TMJ upon palpation are present
◦ Evolution of bony changes of the TMJ

Craniofacial Surgery:
◦ Cleft lip and palate pose unique challenges to
dentists.
◦ Timely treatment is important , young age of
patient and concern surrounding radiation
exposure, Conventional CT is not always useful.
◦ CBCT is a reliable tool for volumetric assessment
of bone defects in alveolar and palatal regions.

Orthognathic Surgery
◦ Lateral Ceph view is a standard image modality
when diagnosing skeletal & dental deformities.
◦ Superimposition of right and left side along with
machine magnification ,accurate surgical
prediction and treatment planning become difficult.
◦ CBCT can be a better choice
◦ Cases: hemifacial microsomia , severe facial
asymmetries etc.

CBCT in Endodontics:

Assessment of root canal morphology
◦ Second Mesiobuccal canal(MB2) in maxillary first
molar vary from 70-90%, this variability occurs in
the Buccolingual plane, where the superimposition
of anatomical structures impedes the detection of
small structural density changes.

Dental Periapical Pathoses
Most common pathologic condition that involves teeth have inflammatory lesions of the pulp and periapical areas, lesions confined to cancellous bone with little or no cortical plate erosion is difficult to diagnose with intraoral modality


Root Fractures
◦ CBCT in diagnosis and management of specific
aspects of Dentoalveolar trauma, especially root
fractures, luxation, displacement and alveolar
fracture.

Root Resorption
◦ Root resorption is the loss of dental hard tissues
as a result of clastic activities(Int & Ex).

Postoperative Assessment
◦ Healing of apical lesions is an important aspect of
postoperative assessment in endo, adequacy of
root canal obturation is a important determinant of
endodontic success, integrity of root canal fillings,
precise nature of perforation etc.

CBCT in Orthodontics:
◦ CBCT images for Cephalometric analysis
◦ Tool for assessing facial growth ,age, airway function and disturbance in tooth eruption.
◦ Orthodontic assessment tools: Dolphin(USA), Invivo Dental (USA), allow dentist to work on CBCT images for orthodontic assessments.
◦ CBCT : proximity to impacted tooth, check for orthodontic movement space, assessing bone density before after during treatment

CBCT in Periodontics:

Assessment of bone loss amount and available bone due to
projection errors.
2D underestimate such assessments.
Other applications are
◦ Periodontal cyst
◦ Intrabony defects
◦ Small osseous defects

CBCT in Forensic Dentistry

◦ Age Estimation
◦ Pulpo-dential complex(Dentin ,cementum and pulp) shows
physiological and pathological changes with advancing
age
◦ (basically extraction and sectioning is required to quantify
but CBCT is a more viable option )
◦ Visualization of cervical vertebral morphology gives
footprint for skeletal age assessment, segmentation of
individual vertebrate is possible using CBCT
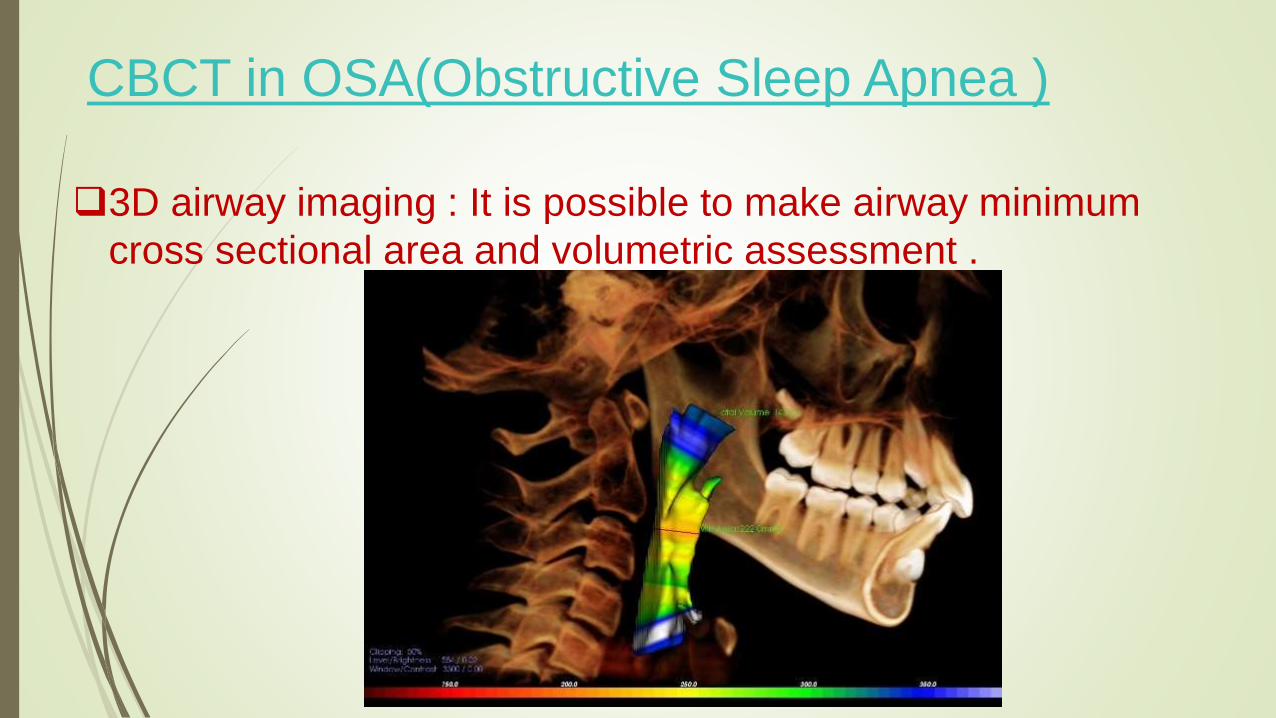
CBCT in OSA(Obstructive Sleep Apnea )
3D airway imaging : It is possible to make airway minimum
cross sectional area and volumetric assessment .

CBCT in ENT
◦ Inflammatory Pathology
◦ Fungal Sinusitis
◦ Tumoral Pathology(NC)
◦ Temporal Bone Assessment
◦ Sinuses and nasal fossae
T AH N K
OY U