clinical analytics for quality improvement initiatives paul henchey october 5, 2015
TRANSCRIPT

Clinical Analytics for Quality Improvement Initiatives
Paul HencheyOctober 5, 2015

ABOUT ARBORMETRIX MISSION TO DELIVER THE MOST ADVANCED HEALTHCARE PERFORMANCE MEASUREMENT PLATFORM
ROOTSFOUNDED BY SURGEONS AND RESEARCHERSFUNDED BY VENTURE CAPITAL
FOCUSACUTE CARESCIENTIFICALLY RIGOROUS CLINICAL ANALYSISADVANCED CLOUD-BASED TECHNOLOGY
CLIENTSCOLLABORATIVES & SPECIALTY SOCIETIES HOSPITALS & HEALTH SYSTEMSACCOUNTABLE CARE ORGANIZATIONS

AGENDA
• Context for Quality Improvement– National – Regional– Local
• Implementing clinical analytics to– Drive quality improvement locally– Leverage national and regional initiatives
• Case Studies

CONTEXT FOR QUALITY IMPROVEMENT

COMPLEMENTARY INITIATIVES
NATIONALResearch Database
REGIONALCollaboration
LOCALProcess Improvement
National societies like ACS and STS have been successful in aggregating broad research databases. More specialized registries now being developed.
State-wide and regional CQI initiatives are big enough for data-driven learning and small enough that the players can know each other and can collaborate effectively on best practices.
Individual health systems are where quality improvements must ultimately be organized, funded and implemented.

EXAMPLE: BROAD NATIONAL INITIATIVE
American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP®)
• 50 clinical variables captured for surgical cases• Includes 30 day outcomes• 660 Participating Hospitals• Clinical abstraction of 1,680 sample cases per hospital per year• Semi-annual benchmarking reports

EXAMPLE: SPECIALIZED NATIONAL INITIATIVE
Americas Hernia Society Quality Collaborative (AHSQC)
• Focus on ventral hernia repair• Continuous data collection and online
benchmarking• Captures details of technique, mesh utilization• Patient outcomes including readmission • Quarterly QI meetings• Coaching on surgical technique
AHSQC Medical Director: Michael J. Rosen, MD, FACS Professor of Surgery, Cleveland Clinic Foundation, Comprehensive Hernia Center
AHSQC Director for Quality and Outcomes: Benjamin K. Poulose, MD, MPH, FACS Assistant Professor of Surgery, Vanderbilt University Medical Center

EXAMPLES: REGIONAL INITIATIVES
• 10 percent reduction in mortality• 34 percent reduction in sepsis• 29 percent reduction in pneumonia• 33 percent reduction in cardiac arrest• 15 percent reduction in length of stay• 18 percent reduction in surgical site infections
Saved $11 million statewide in total episode payments for Post-CQI treated patients in one year, through the Michigan Trauma Quality Improvement Program (MTQIP)
Saved $27.8 million statewide over four years, through the Michigan Bariatric Surgery Collaborative (MBSC)
$85.9 million saved statewide over two years by reducing adverse events, through the Michigan Surgical Quality Collaborative (MSQC)
Regional CQI model now being replicated in states such as Pennsylvania and North Carolina…

EXAMPLES: LOCAL INITIATIVES
VanderbiltSection of Surgical Sciences
• Surgeon-led Surgical Value Improvement Initiative
• Leveraging national registry data (NSQIP, AHSQC, etc.)
• Focus on unwanted variation in cost and quality
University of MichiganDepartment of Surgery
• Leadership for several regional initiatives
• Implementing process improvements internally
• Tracking ROI • Feedback loop for surgeons

IMPLEMENTING CLINICAL ANALYTICS

FRAGMENTED DATA
OPPE
RVUS
CFO
OR DIRECTORSECTION CHIEFBlock timeQuality
Supply cost
Revenue
Cost
DRG
CPT

COLLABORATIVE CLINICAL ANALYTICS
Integrated system provides credible, consistent performance metrics
Eliminates ‘spreadsheet wars’
Supports the alignment of goals, processes
Targeted Improvement
Strategic Planning
Monitoring & coaching

DATA MODELProfessional Claims
CPT
RVU
Surgeon
Facility Claims & Cost Accounting
ICD9
Facility Cost
LOS
OR System
Case Minutes
Supply Cost
CPT, RVU, Surgeon
ICD9, Facility Cost, LOS
Case Minutes, Supply Cost
Clinical Outcomes
Clinical Registries
Clinical Outcomes

CLINICAL SCOPE
National Surgical QIP (ACS)
Metabolic and Bariatric Surgery Accreditation and QIP (ACS)
American Hernia Society Quality Collaborative (AHSQC)
Collaborative Endocrine Surgery QIP
Michigan Surgical Quality Collaborative (MSQC)
Michigan Trauma QIP
Michigan Urological Surgery Improvement Collaborative (MUSIC)
CLINICAL REGISTRIES
Acute Care
Bariatric
Colorectal
Endocrine
HPB
Minimally Invasive
DEPARTMENTS
Surgical Oncology
Cardiac
Thoracic
Vascular
Urology
Orthopaedic

CORE METRICS
QUALITY PRODUCTIVITY
EFFICIENCY FINANCIAL
Post-operative complicationsMortalityReoperationsReadmissions
LOSSurgical cut-to-close timeSupply costHospital direct cost
Work RVUsProceduresVisitsCases
Net revenueNet incomeTotal costContribution margin

ARBORMETRIX RISK-ADJUSTMENT
Why Risk-Adjust? Because an 85-year-old female undergoing cardiac surgery is more likely to suffer adverse outcomes compared to an otherwise healthy 50-year-old male undergoing the same procedure.
Because some hospitals and physicians treat more high-risk patients than others.
Without Risk adjustment physicians will not trust your reports.

ARBORMETRIX RELIABILITY ADJUSTMENT
0 deaths out of 2 patients 0 deaths out of 200 patients
Which surgeon would you refer a family member to?


CASE STUDIES

REGIONAL EXAMPLE: MSQC
A statewide colectomy experience: the role of full bowel preparation in preventing surgical site infection.Ann Surg. 2014 Feb;259(2):310-4. doi: 10.1097/SLA.0b013e3182a62643.Kim EK1, Sheetz KH, Bonn J, DeRoo S, Lee C, Stein I, Zarinsefat A, Cai S, Campbell DA Jr, Englesbe MJ.
“In the state of Michigan, full bowel preparation is associated with decreased infectious complications after elective colectomy.
Within this context, the Michigan Surgical Quality Collaborative recommends full bowel preparation before elective colectomy.”

MICHIGAN SURGICAL QUALITY COLLABORATIVE
SCREEN SHOT Bundle 3way with Mech Bowel Prep selected.
Chart shows level of compliance with each of six best practices.
Wide variation in bundle compliance across hospitals.
Data altered to protect confidentiality

Chart shows correlation between bundle compliance and SSI rates.
Cases with 5 of 6 best practices have only 1/5th the complications compared to those with 0 or 1 best practices.
Data altered to protect confidentiality

LOCAL EXAMPLE: VANDERBILT SECTION OF SURGICAL SERVICES
“We have been able to gain new intelligence regarding value that we did not have prior to implementing the SurgicalMetrix solution.”
“We are able to evaluate each surgeon in their own clinical space and identify surgeons who deliver high quality care at low cost.”
“We are then planning to engage those surgeons and apply their processes to those who may not be performing as well.”

Reports quantify the financial impact of
surgical complications.
Here we see a $9,000 swing in net
income between complicated and uncomplicated
colorectal surgery cases.
Data altered to protect confidentiality

Chart shows correlation between poor quality and reduced margins
Surgeon in lower right quadrant has high complication rates and low net income per case
Data altered to protect confidentiality
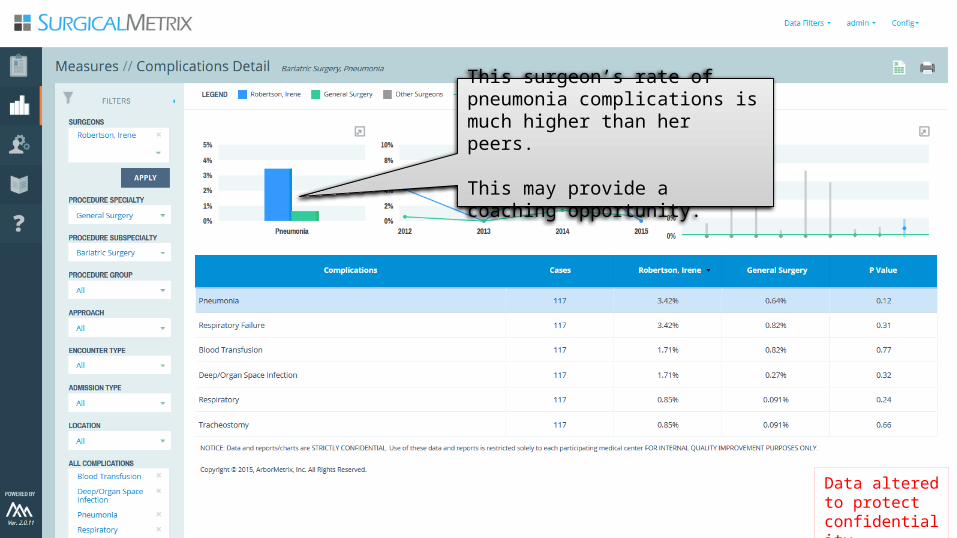
This surgeon’s rate of pneumonia complications is much higher than her peers.
This may provide a coaching opportunity.
Data altered to protect confidentiality

LOCAL EXAMPLE: MICHIGAN DEPARTMENT OF SURGERY
“How can we track the results from our investment in a new staffing model for Acute Care Surgery?”
New staffing model intended to improve quality and reduce cost per case.
SurgicalMetrix put in place to track actual impact over time.

Now using dedicated Acute Care surgeons in place of rotating staff for most Non-Trauma Emergency (NTE) cases.Data altered to
protect confidentiality

Dashboards track cost and quality for NTE cases:
• Complication rate has dropped from about 20% to 12%
• Direct Costs reduced from about $18,000 to $12,000 per case
• LOS also reduced by about 0.5
Data altered to protect confidentiality

COMPLEMENTARY INITIATIVES
NATIONALResearch Database
REGIONALCollaboration
LOCALProcess Improvement
National societies like ACS and STS have been successful in aggregating broad research databases. More specialized registries now being developed.
State-wide and regional CQI initiatives are big enough for data-driven learning and small enough that the players can know each other and can collaborate effectively on best practices.
Individual health systems are where quality improvements must ultimately be organized, funded and implemented.

ADDITIONAL INFORMATION
http://www.arbormetrix.com/whitepapers
http://www.arbormetrix.com/blog
https://twitter.com/ArborMetrix
