classification of endothelial dysfunction
TRANSCRIPT

Classification of Endothelial Dysfunction
Stefano TaddeiDepartment of Internal Medicine
University of Pisa, Italy

endothelial
dysfunction
stimuli-induced
vasodilation(e.g, to shear stress)
PGI EDHF NO
plaque growth
clinical
manifestations
acute
coronary
syndrome
ischemia /
angina pectoris
remodeling/
proliferation
Pathogenesis of atherosclerosisfrom endothelial dysfunction to clinical disease
Vasodilation
Platelet aggregation
VSMC migration and
proliferation
Monocyte adhesion
Adhesion molecules
expression
ET1
NO
Vasoconstriction
NO breakdown:
Platelet aggregation
VSMC migration and
proliferation
Monocyte adhesion
Adhesion molecules
expression
EDCFs(ET-1; A-II; TXA2; PGH2; ·O2
-)
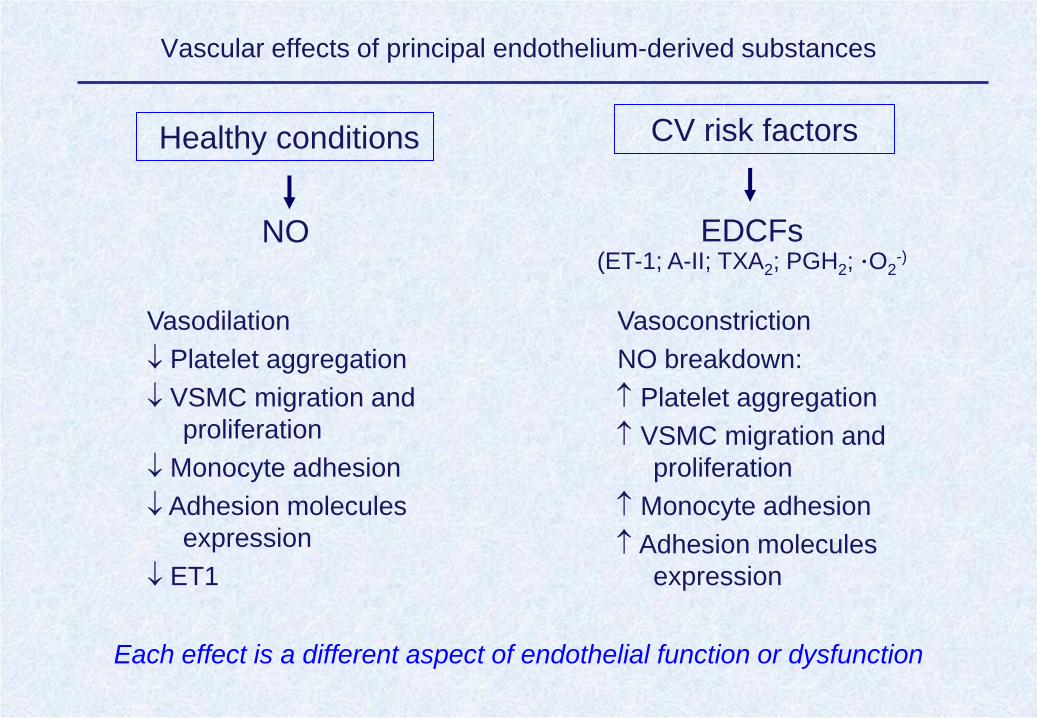
Vascular effects of principal endothelium-derived substances
Healthy conditions CV risk factors
Each effect is a different aspect of endothelial function or dysfunction

• Endothelial Dysfunction
reduced NO availability (vascular reactivity)
• Endothelial Activation
acquisition of flogistic activity
• Endothelial Injury and Repair
anathomical disruption and rigeneration of endothelial cells
Endothelial Pathology

• ENDOTHELIAL DYSFUNCTION– NO
– NO2/NO3 and other plasma nitrosylated species
– ADMA
• ENDOTHELIAL ACTIVATION– adhesion molecules: E-selectin, P-selectin, ICAM-1, VCAM-1
– Regulators of thrombosis: tPA, PAI-1
• ENDOTHELIAL DAMAGE– vWF
– soluble thrombomodulin
– circulating endothelial cells
– endothelial microparticles
• ENDOTHELIAL REPAIR– circulating endothelial progenitor cells
Markers and clinical significance of endothelial pathology
Evaluation of vascular
reactivity

• ENDOTHELIAL DYSFUNCTION– NO
– NO2/NO3 and other plasma nitrosylated species
– ADMA
• ENDOTHELIAL ACTIVATION– adhesion molecules: E-selectin, P-selectin, ICAM-1, VCAM-1
– Regulators of thrombosis: tPA, PAI-1
• ENDOTHELIAL DAMAGE– vWF
– soluble thrombomodulin
– circulating endothelial cells
– endothelial microparticles
• ENDOTHELIAL REPAIR– circulating endothelial progenitor cells
Markers and clinical significance of endothelial pathology
Evaluation of vascular
reactivity
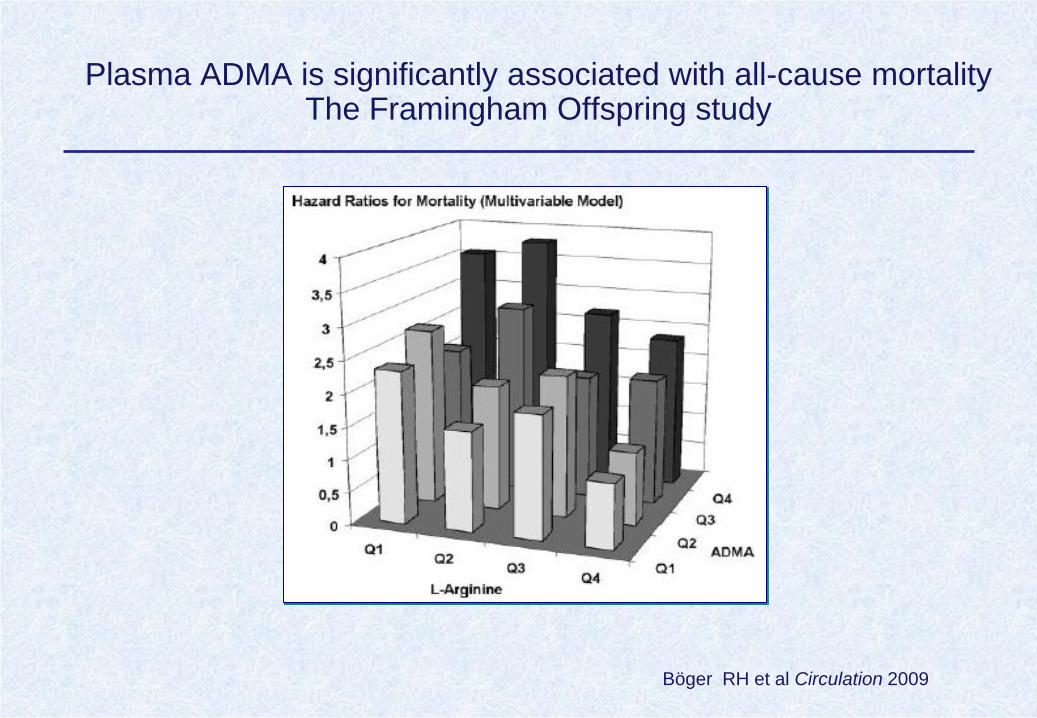
Plasma ADMA is significantly associated with all-cause mortality The Framingham Offspring study
Böger RH et al Circulation 2009

ADMA as a prospective marker of CV disease and mortality
Boger RH et al. Pharmacological Research 2009
High risk
Intermediate risk
Low risk –
general population

Vascular Reactivity
• Vascular response to stimulation or inhibition of endothelial function
• Selectivity for vessel type and vascular district
• Large availability of agonists and antagonists
• Strong association with intermediate organ damage and clinical end-
points

Taddei S et al. Circulation 1995
Effect of aging on endothelium-dependent vasodilation in
the forearm microcirculation
Normotensive Subjects
(N=43)

µg/100 ml/min
Taddei S et al Circulation 1999
0
100
200
300
400
500
600
700
BRADYKININ
0.005 0.015 0.05
Normotensive Subjects
saline
L-NMMA
Ouabain
*
*
* p<0.05
FBFD%
0.005 0.015 0.05
BRADYKININ
*
*
Vitamin C
0.005 0.015 0.05
Essential Hypertensive
Patients
BRADYKININ
**
Control

Solzbach U et al, Circulation 1997
Coronary endothelial dysfunction in hypertensive patients
Role of oxidative stress

Association between endothelial dysfunctionand atherosclerosis
Zeiher AM et al. Circulation 1994
CORONARY ARTERIES
Ghiadoni L et al. Hypertension 1998
0
1000
2000
0,6 0,9 1,2 1,5 1,8 2,1
INTIMA-MEDIAL THICKNING (mm)
Maxim
al
Ach
eti
lch
oli
ne-i
nd
uced
FB
F i
ncre
ase (D
%)
r = -.58
p<.0001
CAROTID ARTERIES

Endothelial Function Assessed by Vascular Reactivity and
Cardiac Events
Lerman A & Zeiher A Circulation 2005
Multivariant analysis of hazard ratio of present studies reporting association between
coronary or peripheral endothelial function and cardiovascular events

Vasodilation
Platelet aggregation
VSMC migration and
proliferation
Monocyte adhesion
Adhesion molecules
expression
ET1
NO
Vasoconstriction
NO breakdown:
Platelet aggregation
VSMC migration and
proliferation
Monocyte adhesion
Adhesion molecules
expression
EDCFs(ET-1; A-II; TXA2; PGH2; ·O2
-)
Vascular effects of principal endothelium-derived substances
Healthy conditions CV risk factors

Effect of NO-synthase blockade by L-NMMA on t-PA release in
normotensive subjects and essential hypertensive patients
Giannarelli C et al Hypertension 2007
t-P
A b
ala
nce
(ng/1
00
ml/m
in)
0
0.5
1.0
ACh ACh +
L-NMMA
ACh + L-
NMMA
*
ACh induced release
Normotensive
subjects
Hypertensive
patients

† p<0.01 vs BDK+saline
0
0.5
1
1.5
2
*
†tPA
rele
ase
ng/1
00m
L/m
in
Hypertensive Patients
Baseline Bradykinin
Sulfaphenazole
Saline
Giannarelli C et al Circulation 2009
Effect of bradykinin on tPA release in the presence of saline or
sulfaphenazole in hypertensive patients

Relaxation
Smooth muscle cells
t-PA release
Endothelial cells
NO EDHF
Bradykinin

• ENDOTHELIAL DYSFUNCTION– NO
– NO2/NO3 and other plasma nitrosylated species
– ADMA
• ENDOTHELIAL ACTIVATION– adhesion molecules: E-selectin, P-selectin, ICAM-1, VCAM-1
– regulators of thrombosis: tPA, PAI-1
• ENDOTHELIAL DAMAGE– vWF
– soluble thrombomodulin
– circulating endothelial cells
– endothelial microparticles
• ENDOTHELIAL REPAIR– circulating endothelial progenitor cells
Markers and clinical significance of endothelial pathology

Constans J et al Clinica Chimica Acta 2006
Endothelial activation represents a switch from a quiescent phenotype toward
one that involves the host defense response

Soluble e-selectin in essential hypertension: a correlate of vascular structural changes
De Caterina R et al Am J Hypertens 2001

Soluble adhesion molecules and prediction of coronary heart disease: a prospective study and meta-analysis
Malik I et al Lancet 2001
• The odds ratio for CHD were 1·68 (95% Cl
1·32–2·14) for ICAM-1 and 1·27 (1·00–1·61)
for E-selectin, but became not significant
after adjustment for some classic coronary
risk factors and indicators of socioeconomic
status.
•The measurement of adhesion
molecules is unlikely to add much
predictive information to that provided by
more established risk factors.

• ENDOTHELIAL DYSFUNCTION– NO
– NO2/NO3 and other plasma nitrosylated species
– ADMA
• ENDOTHELIAL ACTIVATION– adhesion molecules: E-selectin, P-selectin, ICAM-1, VCAM-1
– Regulators of thrombosis: tPA, PAI-1
• ENDOTHELIAL DAMAGE– Von Willebrand Factor
– soluble thrombomodulin
– circulating endothelial cells
– endothelial microparticles
• ENDOTHELIAL REPAIR– circulating endothelial progenitor cells
Markers and clinical significance of endothelial pathology

Von Willebrand Factor, Soluble P-Selectin, and TargetOrgan Damage in Hypertension
A Substudy of the Anglo-Scandinavian Cardiac Outcomes Trial (ASCOT)
Spencer CGC et al Hypertension 2002
* p<0.05
*
*
Hypertensive patients
** p<0.05

A comparison of FMD and VWF as markers of endothelial cell function in health and in hypertension
A substudy of the Anglo-Scandinavian Cardiac Outcomes Trial
r=0.517, p < 0.001
vWF and FMD both correlated with 10-year cardiovascular risk using the Framingham
equation (vWF, r=0.48, p< 0.001; FMD, r =0.624, p< 0.001).
Felmeden DC et al Blood Coagulation and Fibrinolysis 2003

Soluble thrombomodulin
• Thrombomodulin (TM) is specifically expressed by endothelial cells
• Soluble TM can be reliably measured by ELISA
• Controversial clinical significance:
– TM is released from injured endothelial cells high levels indicate a greater
extent of endothelial damage?
– TM plays a role as a protein C cofactor and has anticoagulant activity high
levels may be protective?

High Soluble thrombomodulin predicts recurrence after CAD and mortality after stroke
• 54 patients who had survived a myocardial infarction
• Soluble thrombomodulin was 65+/-24 ng/mL in patients who suffered an end-point
and was 49+/-19 ng/mL in patients who were free of an end-point (p=0.009).
• Using life tables, soluble thrombomodulin had a significant effect on survival free of
an end-point (p=0.011).Blann AD et al. Eur J Haematol. 1997
Olivot GM et al Stroke 2004
• 492 patients with previous brain
infarction
• 5 years follow up
• Soluble thrombomodulin among
the upper tertile confers risk of
recurrence of 2.04 (1.34–3.11),
as compared to the lower tertile

Low sTM predicts CHD in healthy individualsThe ARIC study
Possible explanation: In healthy people, concentrations of soluble thrombomodulin may reflect
the quantity of thrombomodulin expressed on the endothelial surface. Increased expression of
thrombomodulin will increase production of activated protein C, which suppresses the
coagulation reaction by degrading factors Va and VIIIa.
<24.7 24.8-30.6 30.7-40.2 40.3-66.2 >66.3
Quintiles of soluble thrombomodulin (ng/ml)
Ra
te r
atio
of in
cid
en
t co
ron
ary
he
art
dis
ea
se
Salomaa V et al Lancet 1999

Endothelial Dysfunction (FMD) and Damage (CEC) in Congestive Heart Failure
r=0.423, p=0.002
Chong AY et al. Circulation. 2004;110:1794-1798

Circulating endothelial cells and prognosis in 156 patients with acute coronary syndromes
Kaplan-Meier cumulative 1-year event-free survival curves
between more than median versus less than median values
of (A) CECs at 48 hours
Numbers of circulating endothelial cells (CECs) on
admission according to diagnosis and compared with
patients with stable angina and healthy control subjects.
STEMI indicates ST-segment elevation myocardial
infarction; NSTEMI, non-STEMI; UAP, unstable angina
pectoris; SA, stable angina.
Lee KW et al. Blood 2005;105:526–32

Circulating endothelial cells in hypertension and acute ischaemic stroke
•29 hypertensive patients with previous stroke, 30 hypertensive patients and 30 normotensive controls
•Patients with an acute ischaemic stroke had significantly higher numbers of CECs/ml of blood (p<0.001)
plasma vWf (p=0.008), soluble E-selectin (p=0.002) and higher SBP as compared to the other groups
•The number of CECs significantly correlated with soluble E-selectin (r=0.432, p<0.001) and vWf (r=0.349,
p=0.001) but not with SBP (r=0.198, p=0.069)
Nadar SK et al, Thromb Haemost 2005; 94: 707–12
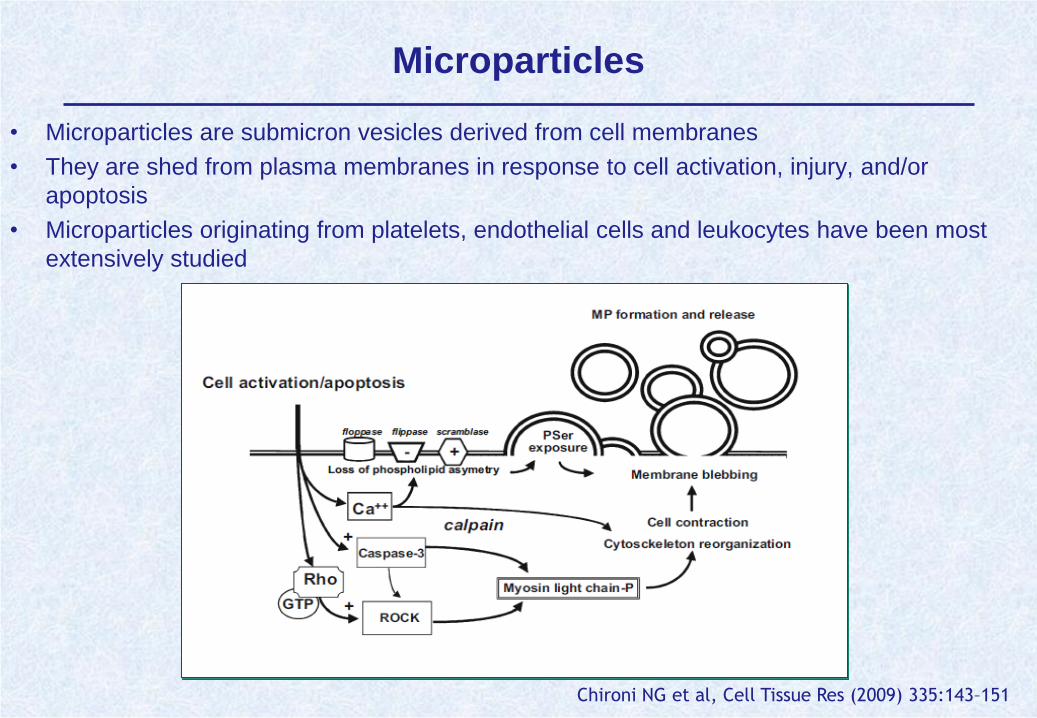
Microparticles
• Microparticles are submicron vesicles derived from cell membranes
• They are shed from plasma membranes in response to cell activation, injury, and/or
apoptosis
• Microparticles originating from platelets, endothelial cells and leukocytes have been most
extensively studied
Chironi NG et al, Cell Tissue Res (2009) 335:143–151

Circulating Endothelial Microparticles Are Associated with Vascular Dysfunction in Patients with End-Stage Renal Failure
• Flow cytometry analysis of platelet-free plasma from 44 patients with ESRF indicated that
circulating levels of Annexin V+ microparticles were increased compared with 32 healthy
subjects, as were levels of microparticles derived from endothelial cells (three-fold), platelets
(16.5-fold), and erythrocytes (1.6-fold).
Circu
latin
g m
icro
pa
rtic
les (
eve
nts
/µl)
End stage renal failure
Healthy subjects
Platelet-derived MP
Endothelium-derived MP
Endothelium-derived MP
Erythrocytes-derived MP
Amabile N et al. J Am Soc Nephrol 16: 3381-3388, 2005

• ENDOTHELIAL DYSFUNCTION– NO
– NO2/NO3 and other plasma nitrosylated species
– ADMA
• ENDOTHELIAL ACTIVATION– adhesion molecules: E-selectin, P-selectin, ICAM-1, VCAM-1
– Regulators of thrombosis: tPA, PAI-1
• ENDOTHELIAL DAMAGE– vWF
– soluble thrombomodulin
– circulating endothelial cells
– endothelial microparticles
• ENDOTHELIAL REPAIR– circulating endothelial progenitor cells
Markers and clinical significance of endothelial pathology
• Classification of endothelial dysfunction is important to understand
the pathophysiology of atherosclerotic disease and in the next
future might be useful for a better determination of CV risk and the
effectiveness of treatment.
Conclusions
• In addition, no large scale intervention trials are available to
consider endothelial dysfunction as a target of CV treatment.
• However, at the present time, the different aspects of endothelial
dysfunctions are not related to a specifc clinical significance.
Further investigation is necessary to establish the exact
relationship between the different types of endothelial alterations
and the development of CV disease.