classification of brain tumors and management og low grade glioma
TRANSCRIPT

CLASSIFICATION OF BRAIN TUMORS&
MANAGEMENT OF LOW GRADE GLIOMA
ABHIJIT DAS
IST YEAR PGT
DEPT. OF RADIATION ONCOLOGY
AHRCC
topics of discussion are
• Classification
• Glioma and its gradation
• What are low grade glioma?
• Usual clinical presentations
• Clinical signs on the basis of location
• discussion about them individually
• Treatment of glioma
• Follow up

Classification of brain tumors
• CNS tumors can primarily be divided into• primary -originates in the brain (solitary, nodular)
• Secondary-made up of cells that have spread (metastasized) to the brain from somewhere else in the body.
Multiple in number, prior h/o cancer , edema +, located at gray white interface.
may lodge into
- Brain parenchyma – most common area of metastases
- Leptomeninges – pia mater & arachnoid mater
- Dural space

WHO classification of brain tumors 2007
• Tumors of Neuroepithelial Tissue
• Tumors of Cranial and Spinal Nerves
• Tumors of the Meninges
• Lymphomas and Hematopoietic Neoplasm
• Germ Cell Tumor
• Tumors of the Sellar Regions( pituitary /craniopharyngioma)
• Metastatic Tumors

• Astrocytic tumours
• Pilocytic astrocytoma
Pilomyxoid astrocytoma
• Subependymal giant cell astrocytoma
• Pleomorphic xanthoastrocytoma
• Diffuse astrocytoma
• Anaplastic astrocytoma
• Glioblastoma
Giant cell glioblastoma
• Gliosarcoma
• Gliomatosis cerebri

Oligodendroglial tumours:
• Oligodendroglioma• Anaplastic oligodendroglioma
Oligoastrocytic tumours
• Oligoastrocytoma• Anaplastic oligoastrocytoma
Ependymal tumours
• Subependymoma• Myxopapillary ependymoma Ependymoma• Anaplastic ependymoma
Choroid plexus tumours
• Choroid plexus papilloma • Atypical choroid plexus papilloma• Choroid plexus carcinoma
Other neuroepithelial tumours
• Astroblastoma• Chordoid glioma of the third ventricle• Angiocentric glioma
Neuronal and mixed neuronal-glial tumours
• Dysplastic gangliocytoma of cerebellum (Lhermitte-Duclos) Desmoplastic infantile astrocytoma/ganglioglioma
• Dysembryoplastic neuroepithelial tumour• Gangliocytoma• Ganglioglioma• Anaplastic ganglioglioma• Central neurocytoma• Extraventricular neurocytoma• Cerebellar liponeurocytoma• papillary glioneuronal tumour• Rosette-forming glioneuronal tumour of the fourth ventricle Paraganglioma
Embryonal tumours
• Medulloblastoma Medulloblastoma with extensive nodularity Anaplastic medulloblastoma• CNS Primitive neuroectodermal tumour• CNS Neuroblastoma• Atypical teratoid/rhabdoid tumour
Tumours of cranial and paraspinal nerves
• Schwannoma• Neurofibroma• Perineurioma• Malignant peripheral nerve sheath tumour (MPNST)

Tumours of the meninges
• Tumours of meningothelial cells
Meningioma Atypical meningioma Anaplastic meningioma
Mesenchymal tumours
• Lipoma ( • Angiolipoma (• Hibernoma• Liposarcoma• Solitary fibrous tumour• Fibrosarcoma• Malignant fibrous histiocytoma• Leiomyoma• Leiomyosarcoma• Rhabdomyoma• Rhabdomyosarcoma• Chondroma• Chondrosarcoma• Osteoma• Osteosarcoma • Osteochondroma• Haemangioma• Epithelioid hemangioendothelioma• Haemangiopericytoma
• Anaplastic haemangiopericytoma
• Angiosarcoma• Kaposi Sarcoma • Ewing Sarcoma - PNET

Tumors of the haematopoietic system
Malignant Lymphomas PlasmocytomaGranulocytic sarcoma
Germ cell tumours
GerminomaEmbryonal carcinoma Yolk sac tumourChoriocarcinomaTeratomaMixed germ cell tumours
Tumours of the sellar region
CraniopharyngiomaGranular cell tumourPituicytomaSpindle cell oncocytoma of the adenohypophysis
Metastatic Tumours
Tumors that originate outside CNS and spread secondarily to CNS via Hematogenous route or by direct invasion from adjacent tissues. Most common primary tumour site
1. Lung2. Breast3. Melanoma4. Renal5. Colorectal
MANAGEMENT OF LOW GRADE GLIOMA
• A glioma is a primary brain tumor that originates from the supportive cells of the brain, called glial cells.
• Glial cells are the most common cellular component of the brain
• Three types of glial cells are there, from which gliomas arise.
• They are –astrocytes: astrocytoma
oligodendrocytes: oligodendroglioma
ependymal cells: ependymoma
GRADATION
• There are various gradation systems introduced for these tumors
• kernohan et al. (abandoned due to little reproducibility of prognostic significance among 4 grades)
• Ringertz et.al ( due to intraobserver variability abandoned later)
• More useful approach is by Daumas -Duport et al.
4 factors taken into consideration -1. nuclear pleomorphism
2.mitoses
3. endothelial proliferation
4.necrosis
WHO Grading :
WHO grade I – low proliferative potential. Possible cure with surgery alone
WHO grade II – infiltrating, but low in mitotic activity. Can recur and progress to other grades
WHO grade III – Histologic evidence of malignancy (mitotic activity), infiltrative, anaplastic
WHO grade IV – mitotically active, necrosis, rapid pre and post-surgical progression

Central Nervous System Glial Tumors (who glial tumor classification)
• Astrocytic tumors• Diffusely infiltrating astrocytomas• Diffuse astrocytoma• Anaplastic astrocytoma• Pleomorphic astrocytoma• Glioblastoma• Giant cell glioblastoma• Gliosarcoma• Pilocytic astrocytoma• Pleomorphic xanthoastrocytoma
• Oligodendroglial tumors and mixed gliomas
• Oligodendroglioma• Anaplastic oligodendroglioma• Oligoastrocytoma• Anaplastic oligoastrocytoma
• Ependymal tumors• Ependymoma• Anaplastic ependymoma• Myxopapillary ependymoma• Subependymoma• Choroid plexus tumors • Neuroepithelial tumors of uncertain origin• Astroblastoma• Chordoid glioma of the third ventricle• Gliomatosis cerebri

Low grade glioma are-
astrocytoma ( grade 1) pilocytic Subependymal giant cell astrocytoma pleomorphic xanthoastrocytoma Desmoplastic cerebral astrocytoma of infancy
diffuse astrocytoma
gemistocytic
Protoplasmic
fibrillary
oligoastrocytoma, and oligodendroglioma (WHO II)
Ependymoma grade ii

Clinical presentations
• 1.increased ICP
• 2.endocrinological dysfunction
• 3.physiologic deficits due to location causes of varied presentations
• 4.higher order neurocognitive deficits.
• Slow growing tumors can grow upto a big size without producing symptoms, whereas aggressive one may produce headache in early stage.
• Early morning headaches (due to recumbency and hyper ventilation)
• Seizures
• Personality changes, mood fluctuations and depression

Location specific symptomsFrontal tumors Temporal tumors Parietal tumors • Occpital tumors
• Personalitychange
• Abulia• Loss of initiative• b/l gliomas can
cause memory loss, labile mood & urinary incontinence
• Auditory hallucinations
• SuperiorHomonymous quadrantopia
• impaired perception of verbal commands
• Homonymous inf. Quadrantopia
• Hemianaesthesia• Alexia dysgraphia
apraxia
Visual aberration perceptual
disruption of color size and location
• b/l tumors cause cortical blindness

Spinal cord tumorsSite presentation
Foramen magnum 11th and 12th cranial nerve palsies; ipsilateral arm weakness early; cerebellar ataxia; neck pain
Cervical Ipsilateral arm weakness with leg and opposite arm in time; wasting and fibrillation of ipsilateral neck, shoulder girdle, and arm; decreased pain and temperature sensation in upper cervical regions early; pain in cervical distribution
Thoracic Weakness of abdominal muscles; sparing of arms; unilateral root pains; sensory level with ipsilateral changes early and bilateral with time
Lumbosacral Root pain in groin region or sciatic distribution, or both; weakened proximal pelvic muscles; impotence; bladder paralysis; decreased knee jerk and brisk ankle jerks
Cauda equina Unilateral pain in back and leg becoming bilateral when the tumor is quite large; bladder and bowel paralysis
• Classic corpus callosum disconnection syndromes: though rare but can occur in case of infiltrative glioma.
• Anterior involvement: failure of left hand to carry out spoken commands
• Posterior involvement : Inability to read and name colors
Cranial nerve involvement : vi and vii nv. Palsy in case of pontine glioma
ix, x, xii nv. deficits in case of medulla involvement
which has a fulminant course due to involvement of cardiorespiratory centres.
• haemorrahge into a tumor can rise to catastrophic effect as seen in
oligodendroglioma and GBM.
Most of the low grade gliomas present with seizure. Seizures areassociated with a better survival, whereas the presence of functional deficits predicts a poorer outcome.

investigations• Mostly radiological diagnosis are made.
• MRI with gadolinium contrast is imaging modality of choice.
• Low grade gliomas show increased signal on T2 / FLAIR.
Contrast-enhanced MRI provides an improved ability to discern tumors from other pathologic entities, one tumor type from another, and putatively higher-grade from lower-grade malignancies.
• Most low-grade gliomas (except pilocytic astrocytomas and pleomorphic xanthoastrocytoma) do not enhance.
• T1-weighted sagittal images, • gadolinium(Gd)-enhanced and unenhanced T1 axial images,
• T2-weighted axial images
CT is generally reserved
• for those unable (implanted pacemaker, metal fragment,
paramagnetic surgical clips)
or
• unwilling (because of claustrophobia) to undergo MRI.
• Neoplasms having high risk for leptomeningeal seeding should undergo MRI pre operatively, as after surgery arachnoiditis /blood products may mimic seeding.
• Delayed spinal MRI (more than 3 weeks after surgery) combined with an increased dose of gadolinium is a sensitive imaging study for leptomeningeal disease
Neuraxial imaging

• examination of CSF is helpful in assessing for tumor dissemination through the CSF pathways. It is best done before surgery or more than 3 weeks after surgery, as long as there is no uncontrolled
raised intracranial pressure
Typically, medulloblastoma, ependymoma, choroid plexus carcinoma, lymphoma, and some embryonal pineal and suprasellar region tumors have a high enough likelihood of spreading to justify CSF examinations to look for malignant cells (cytology) and specific markers, such as human chorionic gonadotropin- and alpha fetoprotein.
Possible findings : 1. CSF pressure above 150 mm H2O at the lumbar level in a laterally positioned patient,
2.elevated protein, typically greater than 40 mg/dL,3. reduced glucose (below 50mg/ml)4. tumor cells by cytologic examination.

Low grade Astrocytoma.
Tumors included:• Pilocytic astrocytoma
• Pilocytic xanthoastrocytoma
• SEGA
• Diffuse astrocytomas (WHO grade II),
• Location wise:
Cerebellar astrocytomas (15% to 20%)
Hemispheric astrocytomas (10% to 15%)
Midline supratentorial tumors, including the corpus callosum, lateral and third ventricles, and the hypothalamus and thalamus (10% to 15% of all CNS tumors),
Optic pathway tumors (approximately 5% of all CNS tumors),
Brainstem LGA (brainstem tumors account for 10% to 15% of all CNS tumors; 20% to 30% of these are LGA),
LGA of the spinal cord (spinal cord tumors account for 3% to 6% of all CNS tumors; approximately 60% of these are LGA).

Pilocytic astrocytoma
• Imaging:
• T2WI: Solid portions hyperintense to gray matter, Cyst contents hyper intense to CSF
• Cystic cerebellar mass with enhancing mural nodule
• Frequently causes obstructive hydrocephalus (May be a greater clinical management problem than tumor itself or in children)
• Cerebellum is the most common location
• Association with NF 1(classical is bilat. Optic glioma
• Microscopy
• Rosenthal fibers = electron dense GFAP staining cytoplasmic inclusions
• Loose-textured multipolar cells with microcysts, eosinophilic granular bodies.
Peak incidence: 5-15 yrs of age5-10% of all gliomasMost common primary brain tumor in children

axial T1 C+ MR shows a largecystic/solid mass in the righthemisphere, with heterogeneous enhancementof the solid components andlittle surrounding vasogenicedema.

Pleomorphic xanthoastrocytoma
• Imaging:Supratentorial cortical mass
with adjacent enhancing dural "tail"Temporal lobe most
common Parietal> occipital> frontal
lobes
• Microscopy:Fibrillary and giant
multinucleated astrocytes Large xanthomatous (lipid-
containing) cells are GFAP positiveSome positive for
synaptophysin, neurofilament proteins, S-100 proteinCD34 antigen may help
differentiate PXA from other tumors
• Superficial, circumscribed astrocytic tumor noted for cellular pleomorphism and xanthomatous change.
• < 1% of all astrocytoma• Presents within typically first three decades• 2/3 tumors presents within < 18 years

Axial T1 C+ MR shows a cystic masswith a markedly enhancingmural nodule, typical of PXA.These cortically basedmasses are most common inthe temporal lobes
Subependymal giant cell astrocytoma
• Imaging:
well lobulated with strong enhancement mass presented almost always in lateral ventricular wall near foramen of munro. (Almost always)
Asoociated findings like cortical tuber
• Microscopy:
• Giant pyramidal ganglioidastrocytes & Perivascular pseudopalisading
• Often +ve for GFAPand s 100
Most common CNS neoplasm in tuberous sclerosis SGCA typically occurs during the first two decades Mean age of presentation is 11 years
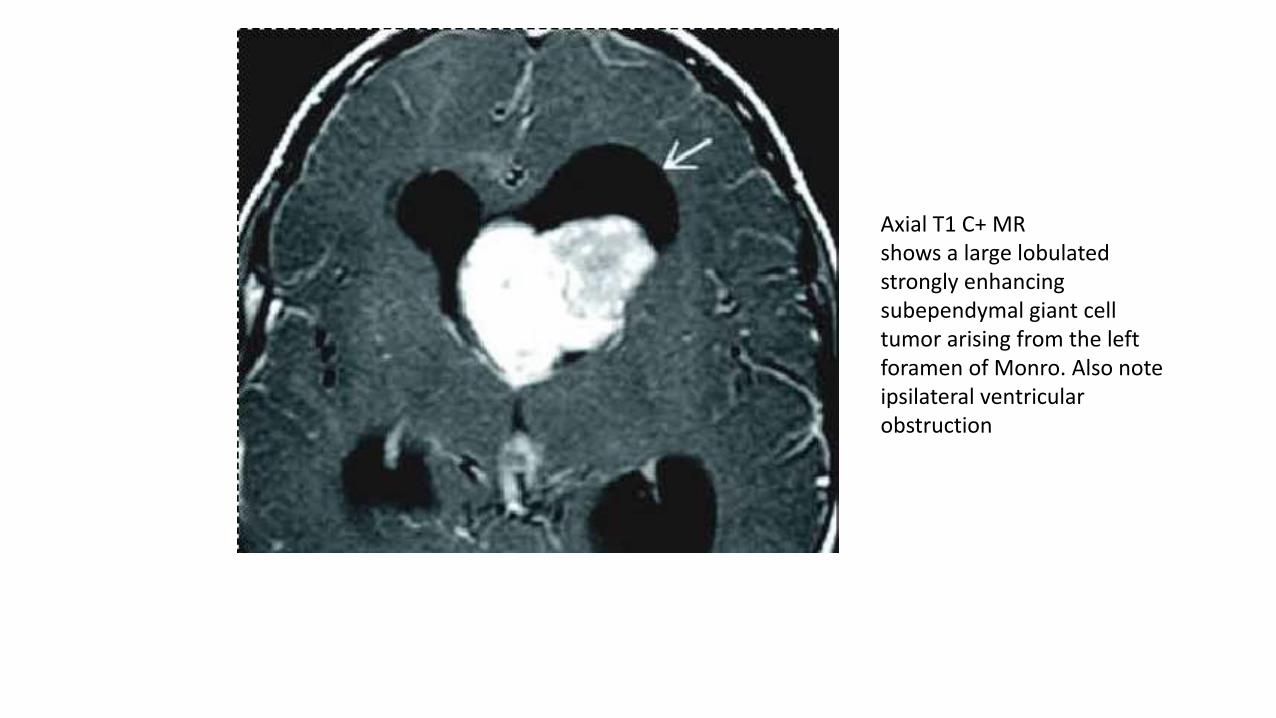
Axial T1 C+ MRshows a large lobulatedstrongly enhancingsubependymal giant celltumor arising from the leftforamen of Monro. Also noteipsilateral ventricularobstruction

Diffuse astrocytoma, grade ii
• Imaging:
Focal or diffuse nonenhancing white matter mass, white matter and gray matter interface
Usually found in Cerebral hemispheres, around 2/3 of incidence is supratentorial
May appear circumscribed on imaging
• Microscopy:
Moderately increased cellularity
Occasional nuclear atypia
Mitotic activity generally absent or very rare
No microvascularproliferation or necrosis
2nd most common astrocytoma of childhood increased tendency for malignant progression or degeneration into anaplastic astrocytoma
or higher grade astrocytoma Three types: 1. gemistocytic
2. fibrillary3.protoplasmic

Axial T2WI MR shows-a diffuse hyperintense whitematter frontal lobe mass withcentral hyperintensity,suggesting cystic change.Note infiltrative margins andcortical involvement.

oligodendroglima
• Location: Typically involves subcortical white matter and cortex of which majority are supratentorial (85%),
• Most common site is frontal lobe
• peak incidence in 4th to 5th decade.
Imaging:
Flair:• Typically heterogeneous, hyperintense• o May appear well circumscribed but
infiltrative
T2* GRE: calcification seen as areas of "blooming” which is avery good diagnostic clue.
Microscopy:
Moderately cellular tumors with occasional mitoses
Rounded, homogeneous nuclei and clear cytoplasm
"Fried egg" and "honeycomb" patterns.
Immunohistochemistry: Oligl+, GFA
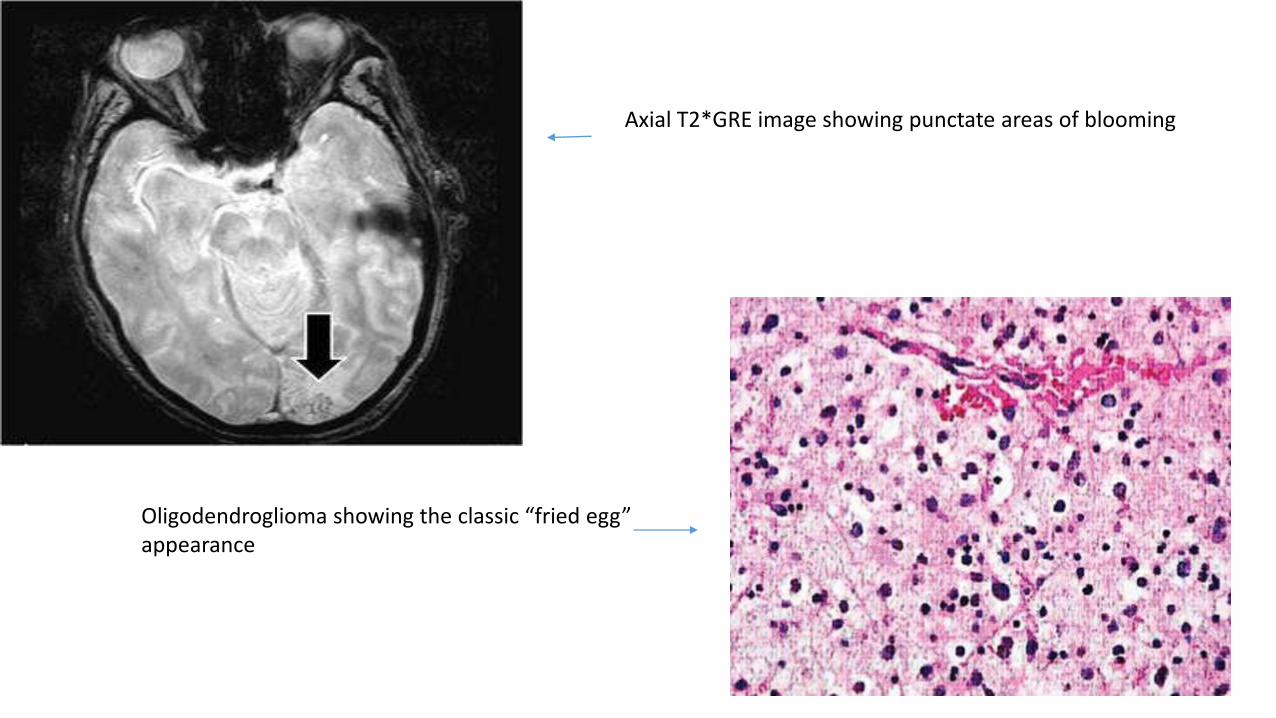
Axial T2*GRE image showing punctate areas of blooming
Oligodendroglioma showing the classic “fried egg” appearance
Treatment of low grade astrocytoma
Surgery is the mainstay of treatment:
goals of surgery :
• Establish a tissue diagnosis.
• removal of as much tumor as possible without increasing the neurologic deficit.
• Removal of an epileptogenic focus if present.
Medical management: Anti convulsants( may be given prophylactically) Steroid (dexamethasone) to decrease the vasogenic oedema CSF deversion procedure e.g: ventricloperitoneal shunt
Definitive management:

Surgery is the mainstay of treatment.
Complete resection incomplete resection surgically nonresectable
complete resection is achieved in approximately 80% of cerebral, cerebellar, and spinal-cord tumors and 40% of diencephalic tumors.In case of smaller tumors & non eloquent part of brain, usually tumors are completely resectable. They produce very satisfactory result with long-term disease-free and overall survival rates of 80% to 100%. Though there is doubt regarding In survival difference in either type, but postoperative adjuvant therapy is clearly not indicated.
For children who undergo less than complete resection, the progression-free survival rate after surgery alone is not as good as complete resection.Here comes the question of adjuvant therapy.
Pediatric oncology group study:
In case of subtotal resection (defined as <1.5 cm residual tumor) observed without any adjavanttherapy.
5 year progression free survival is 64 %
Majority of the patient may be salvaged by second look surgery
Overall survival is 95% in pog study
Consequently, the usual recommendation following subtotal resection will be
close follow-up.
Trial RTOG 9802
• 111 patients• Evaluation of recurrence risk in neurosurgeon defined GTR • Shows that postoperative residual tumor is an imp. Variable of
recurrence.
• 5 year recurrence rate is 26% vs. 68 % for patients with <1 cm residual lesion &1 to 2 cm residual tumors & 89% with a residual tumor of more than 2 cm.
Residual tumor of 1 cm or more according to MR imaging is found to be predictive of a poorer PFS

Role of radiotherapy as adjuvant therapy
• Patient selection for and the timing and dose of postoperative irradiation are controversial issues.
• Major concerns are:
No improvement of overall survival
Though progressive disease free survival is appreciated
Incidence is high among Young age population
neurocognitive decline , dementia , behavioural changes, vasculopathy, development of 2nd malignancy are very high in postRT young patient as RT causes disruption of myelination and cortical atrophy.
Gradual decline of IQ over time.

Three phase iii trials
RT improved median PFS (5.3 year vs. 3.4 year)(p<.001) but not overall survival.

EORTC 22845 (Karim et al. 2002; van den Bent et al. 2005) –phase III: 311 patients
(WHO 1–2, 51% astro., 14% oligo., 13%mixed oligo-astro) treated with surgery (42% GTR,
19% STR,
35% biopsy) randomized to observation vs. post-op RT to 54 Gy.
RT improved median PFS (5.3 year vs. 3.4 year), 5-year PFS (55 vs. 35 %), but not OS (68 vs.
66%). Sixty-five percent of patients in the observation arm received salvage RT.
• No difference in rate of malignant transformation (66–72%).
• No survival benefit, but RT delays time to relapse by ~2 years
EORTC 22844 (Karim et al. 1996) – phase III: 343 patients (WHO 1–2, astro., oligo. and mixed) treated with surgery
(25% GTR, 30% STR, 40% biopsy) randomized to post-op RT 45 Gy vs. 59.4 Gy radiation therapy using multiple
localized treatment fields.
Initial analysis failed to demonstrate a difference in survival rates between the two doses. The 5-year OS was 58% with 45
Gy and 59% with 59.4 Gy.
Five-year OS oligo vs. astro = 75 vs. 55%,
<40 year vs. >40 year = 80 vs. 60%.
Age <40 year, oligo histology, low T-stage, GTR, and good neurologic status are important prognostic factors

INT/NCCTG (Shaw et al. 2002) – phase III: 203 patients (WHO 1–2, astro, oligo, mixed)
treated with surgery (14% GTR, 35% STR, 51% Bx) randomized to post-op RT 50.4 Gy vs.
64.8 Gy. also using multiple localized treatment fields.
Initial analysis also failed to demonstrate a difference in survival rates between the two doses.
The 5-year OS was 73% with 50.4 Gy and 68% with 64.8 Gy.
Best survival in patients <40 year, tumor <5 cm, oligo histology and GTR.
Pattern of failure: 92% in field, 3% within 2 cm of RT field.
INDICATION OF ADJUVANT RT
Dose of ADJ. RT:
• Consequently, low-dose radiotherapy, 50.4 Gy-54 Gyin 1.8 Gy-2Gy per fractions, has become an accepted practice for patients with low-grade gliomas.
1.Tumor progression
2.Compromise neurologic function
3.Unresectable (NOT SUITABLE FOR 2ND LOOK SURGERY)
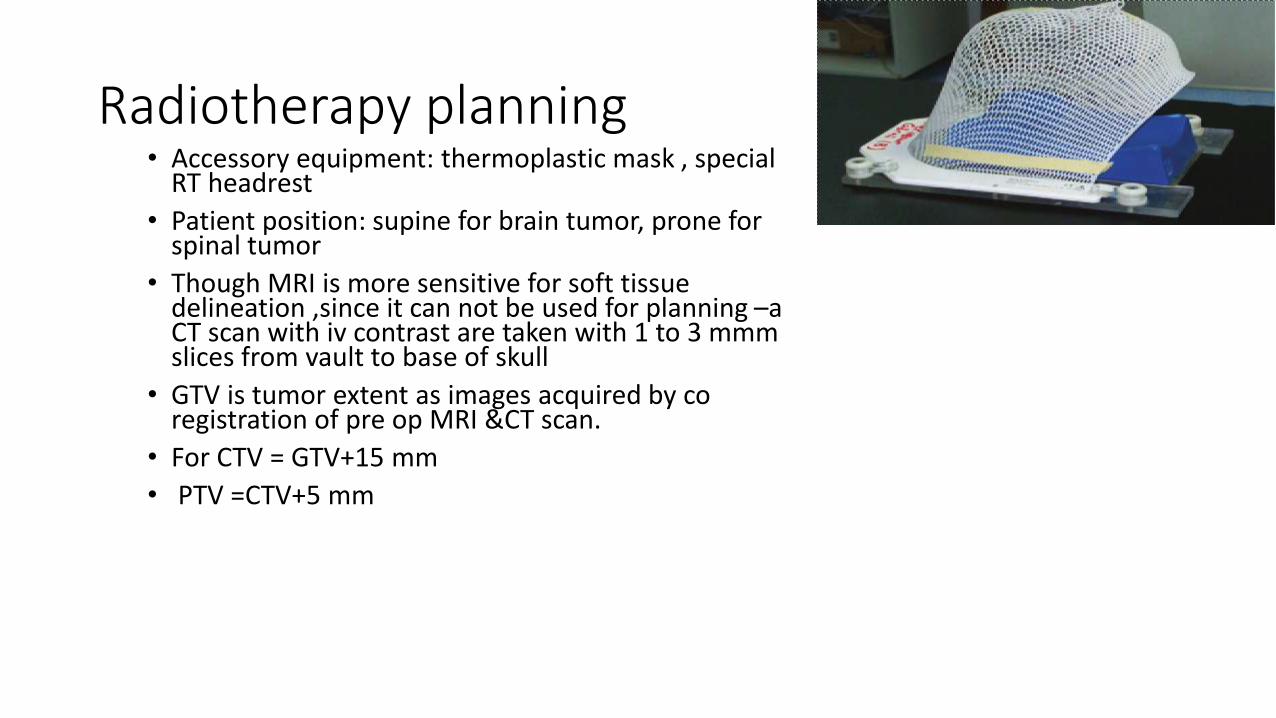
Radiotherapy planning• Accessory equipment: thermoplastic mask , special
RT headrest
• Patient position: supine for brain tumor, prone for spinal tumor
• Though MRI is more sensitive for soft tissue delineation ,since it can not be used for planning –a CT scan with iv contrast are taken with 1 to 3 mmm slices from vault to base of skull
• GTV is tumor extent as images acquired by co registration of pre op MRI &CT scan.
• For CTV = GTV+15 mm
• PTV =CTV+5 mm
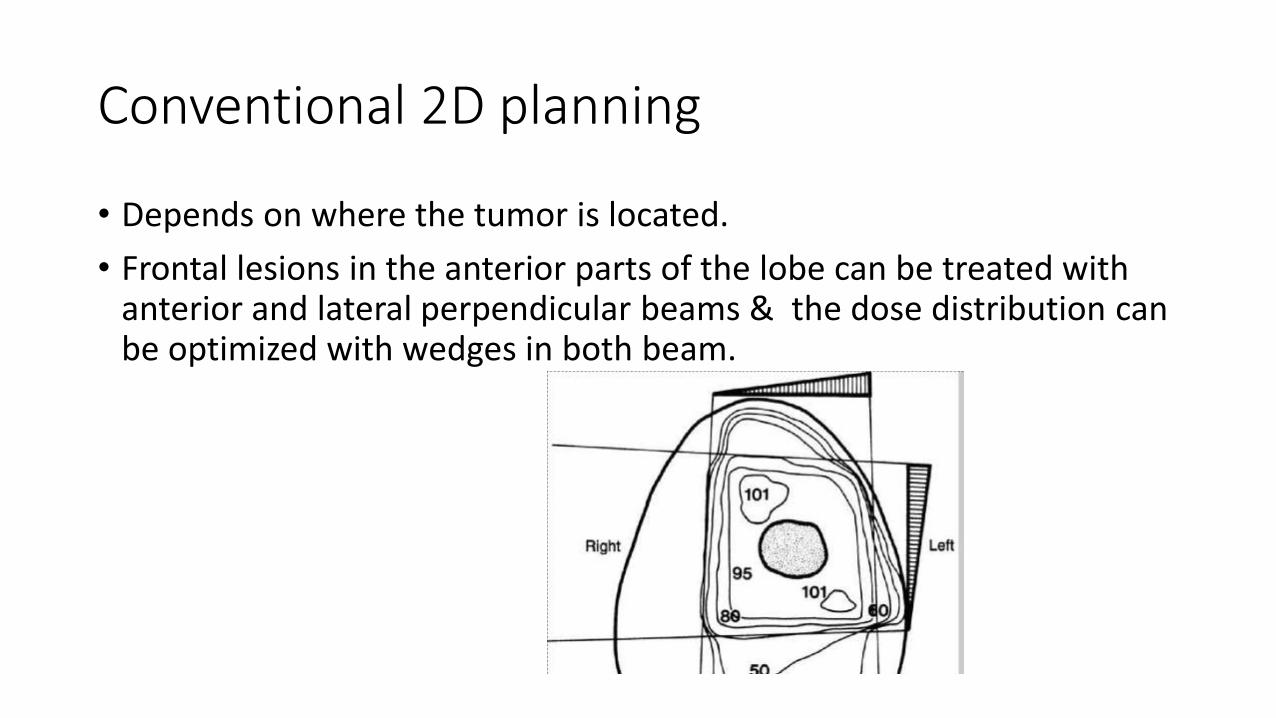
Conventional 2D planning
• Depends on where the tumor is located.
• Frontal lesions in the anterior parts of the lobe can be treated with anterior and lateral perpendicular beams & the dose distribution can be optimized with wedges in both beam.

Contd..
• Midcerebral tumors crossing the midline are treated with parallel-opposed bilateral portals,
• Posterior parietal or occipital lesions can be treated with posterior and lateral beams (may be wedged for dose homogenization)
• Brainstem lesions are adequately treated with parallel-opposed lateral portals which may be combined with a posterior midline portal that does not irradiate the eyes.
• Unilateral cerebellar lesions can be covered by appropriately wedged posterior and lateral portals.
Role of IMRT• In view of complex tumor structureodd location like temporal region to increase conformalityto better spare the normal tissue, many centres use the IMRT.
Disadvantage:Since on low grade glioma tumor is admixed with normal
tissue, it results in dose heterogeneity.if IMRT is used with a prescription of 54 Gy in 30 fractions, this
will typically result in heterogeneity of 10% or more in the target. This increased heterogeneity results in an increased daily dose per fraction and an increased biologically equivalent dose approaching towards high-dose which increases the risk of radiation necrosis.

Role of chemotherapy
• Low grade glioma are traditionally resistant to chemoterapy.
• Studies are very less in number.
• A national phase iii trial by children cancer group ccg 9952 is testing efficacy for procarbazine and vincristine versus TPCV in unresectable / progressive tumor, but results are yet to come.
• Currently another drug temozolomide is investigated in multiple small studies.
in half the patients there is imaging stability / improvement of symptoms,
but criteria for use of this drug is yet to come.

Contd…• The most significant study is the INT/RTOG 9802 trial : phase III study on
low-grade gliomas. • Principles followed:Low-risk (<40 year + GTR) observed until symptoms.251 high-risk (>40 year or STR or biopsy) patients randomized to RT alone
vs. RT --> PCV ×6 cycles q8 weeks where RT is given as 54 Gy to FLAIR detected GTV + 2 cm margin without any boost.
• Result: Five-year OS was 72 vs. 63% (p = 0.33), 5-year PFS was 63 vs. 46%(p = 0.06) in favour of addition of chemotherapy.
• Inference:This study noted an increase of PFS but not OS with radiotherapy followed by PCV chemotherapy.

Role of SRS in recurrent/unresectable tumors
• SRS is usually used
1.in boosting after RT for residual tumor in early post-operative period
2. salvage treatment at the time of recurrence.
3. SRS following pathological diagnosis for tumors located in eloquent areas & unresectable tumors.( but dose reduction is necessary to avoid increased normal tissue dose and thus compromising tumor control.)
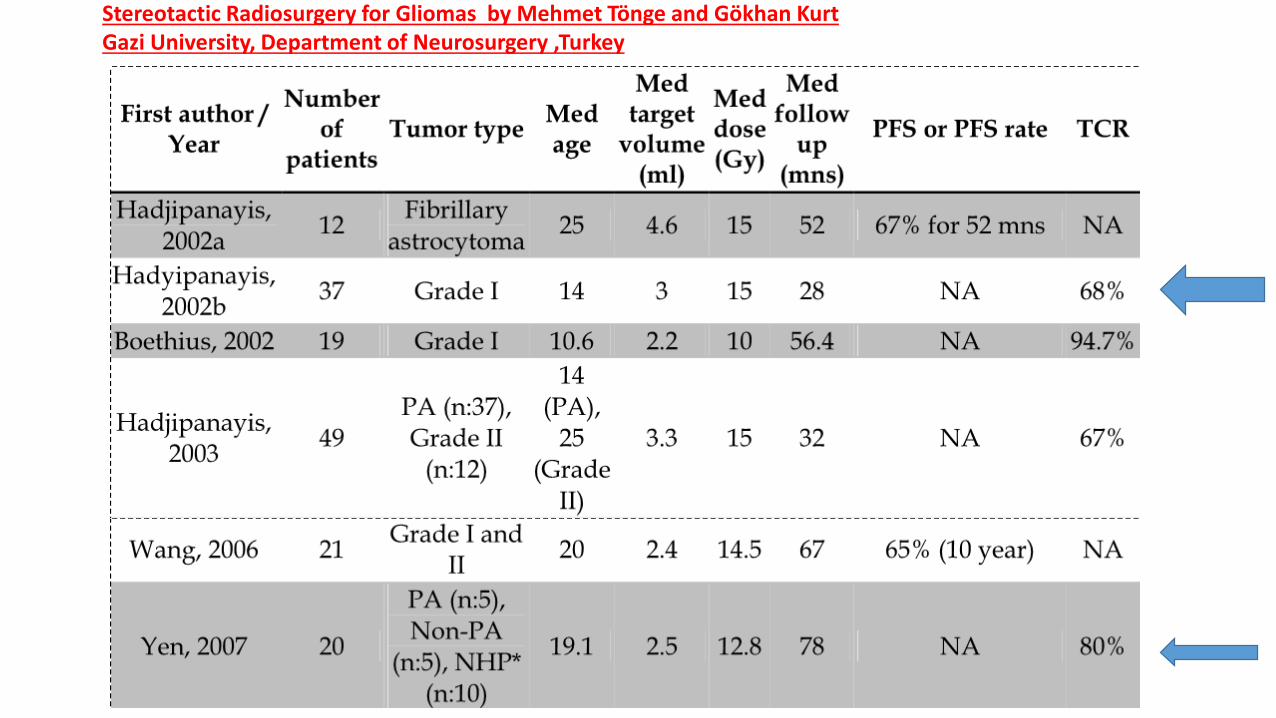
Stereotactic Radiosurgery for Gliomas by Mehmet Tönge and Gökhan Kurt Gazi University, Department of Neurosurgery ,Turkey

TCR for pure solid tumors was 84% in a study including both solid and cystic tumors with overall 68% TCR (Hadjipanayis et al.,)
80% TCR during 78 month follow-up was reported in a series of 20 unresectable focal brainstem gliomaswith gamma knife with mean 12.8 Gy doses (Yen et al., 2007).
Prognostication in using SRS
Yet long term studies are needed to confirm its role.
EPENDYMOMA
• There are three types:
Myxopapillary ependymoma (WHO grade I).
Ependymoma (WHO grade II),
Anaplastic ependymoma (WHO grade III),
Location:
• 2/3rd infra tentorial, (common site--4th ventricle)
• 1/3rd supratentorial, (majority is present in periventricular WM)
Often termed as Soft or "plastic" tumor as it Squeezes out through 4th ventricle foramina into cisterns.

Contd…
• Risk of leptomeningeal seeding is high, but most often seen in anaplastic variety, and ependymoblastome-an agressive tumor.
• Microscopically rosette formation is very characteristics---such as
Perivascular pseudorosettes
True ependymal rosettes (less frequent
Treatment:
modality
surgery It is main modality of treatment, In which completeness of surgery is highle important issue.
In supratentorial tumors , almost 70-90% tumors is completely resectable whrereas in infreyentorial tu,ors complete resection is less frequently possible.
Most commonly residual tumors is left behind in the floor of the ventricle/foramen of luschka.( 2nd look surgery is needed sometimes.)
Post op RT. It is standard of care in children.To avoid or delay it only results in worse disease free survival or overall survival. It only can be considered in -(a) patients with ependymoma of the spinal cord who have
undergone complete resection (b) selected patients with supratentorial ependymoma,
(1.intraventricular tumors & 2. solid and noneloquent areas extraventricular tumors which can be resected with a wider margin ).

Radiotherapy treatment volumes
Local RT:
GTV= tumor bed +any extension of tumor caudally through foramen of magnum+surgical shift.+any residual tuorCTV= GTV +1 cm(some institutions take it as 0.5 cm)
Craniospinal irradiation:it is previously practiced irrespective of situation, but present scenario shows-1.local recurrence is the primary pattern of failure(all failure occurs within 95% isodose.)2.Prophylactic treatment may not prevent spinal metastases.3. Seeding is uncommon in the absence of local failure.Thus for low grade ependymoma CSI is largely abondoned., though some says it may be continued in case of anaplastic vareity?/ infratentorial tumors.thus currently only CSF seeding proven by MRI or CSF study is
candidate for CSI.

Treatment dose:
• Improved tumor control is seen with dose of >45 to 50 GY upto 54 GY.
• patients with neuraxis spread shold receive CSI (40 to 45 GY) with boost to the areas of gross disease and to the primary tumor site upto 54 GY.
• Current standard of treatment in children > 18 months / supra-infratentorial tumors Dose is upto 54 GY.

Cranio Spinal Irradiation• CSI –standard of Care• Coverage of entire target volume that includes the
meninges overlying the brain and spine including the extensions along the nerve roots is critical
• Prone/ Supine*• full-body immobilization• using neck extension together with careful selection of the
level for the junction of the brain and spine fields –• it is possible to avoid including the dentition in the exit from the
superior aspect of the spinal field, and thus any damage to developing teeth that may result in stunted tooth growth, impaction, incomplete calcification, delayed development, and caries.
Patient Positioning and Immobilization

• CT simulation is • necessary to ensure adequate coverage of CTV in subfrontal region:Cribriform plate
• invaluable in identifying the lateral aspect of CTV for the spine field that includes the extensions of the meninges along the nerve roots to the lateral aspects of the spinal ganglia.
• The field, which must be wide enough to encompass the intervertebral foramina in the lumbar region, can be blocked laterally in the dorsal region to avoid unnecessary irradiation of the heart and lungs
• In the lumbar region, it is important to avoid an excessively wide field that will result in unnecessary irradiation of the bone marrow and gonads
• Traditionally the lower border of the spine field was placed at the lower border of the second sacral vertebra, but it is well documented that the lower border of the thecal sac can be as high as L5 or as low as S3.
photons in the 6 to 10 MV range provide satisfactory coverage of the PTV.
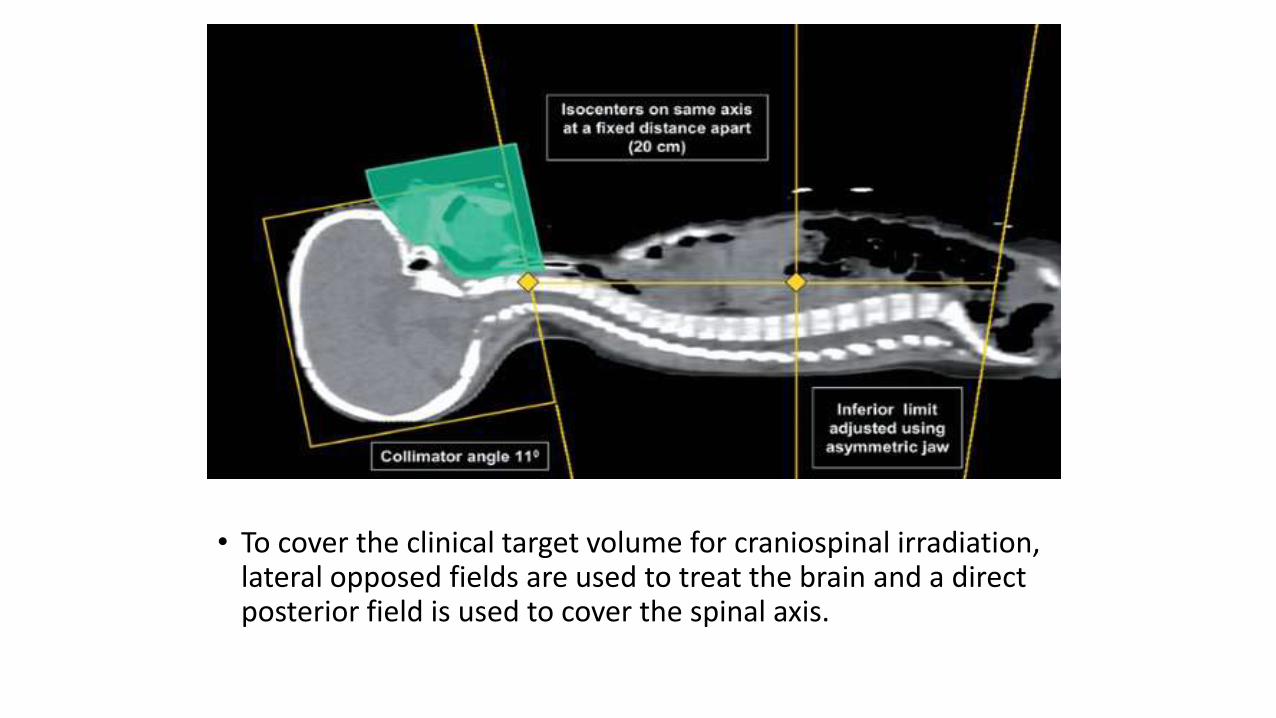
• To cover the clinical target volume for craniospinal irradiation, lateral opposed fields are used to treat the brain and a direct posterior field is used to cover the spinal axis.

Take home massage
According o gradation systems by WHO, pilocytic astrocytoma, ependymomaoligodendroglioma ,oligoastrocytoma are low grade gliomas.
Most low-grade gliomas (except pilocytic astrocytomas and pleomorphic xanthoastrocytoma) do not enhance.
Low grade gliomas show increased signal on T2 / FLAIR.
most common form of presentation is seizure.
Surgery is the mainstay pf treatment. complete resection is achieved in approximately 80% of cerebral, cerebellar, and spinal-cord
tumors and 40% of diencephalic tumors Residual tumor of 1 cm or more according to MR imaging is found to be predictive of a poorer
PFS

In case of ependymoma too surgery is mainstay of treatment.
post op RT is standard of care in children.
CSI has a doubtful role in routine prescription. Definite indication is csf seeding proven by imaging or CSF study Current standard of treatment in children > 18 months / supra-infratentorial tumors Dose is upto 54
GY.
Indications of RT :1.Tumor progression ,2.Compromise neurologic function 3.Unresectable (NOT SUITABLE FOR 2ND LOOK SURGERY
low-dose radiotherapy, 50.4 Gy-54 Gy in 1.8 Gy-2Gy per fractions, has become an accepted practice for patients with low-grade gliomas
Chemotherapy has no proven benefits.
