class aminoglycosides 2
TRANSCRIPT

CLASS AMINOGLYCOSIDES
Dr. RAGHU PRASADA M SMBBS,MDASSISTANT PROFESSOR DEPT. OF PHARMACOLOGYSSIMS & RC.

INTRODUCTION
Group of antibiotics used in the treatment of bacteria infections aerobic G-ve
Consists of 2 or more amino sugars and a hexose nucleus
Serious toxicity is a limiting factor for their application
Streptomycin was the first to be discovered in 1943 by Schatz, Bugie and Waksman
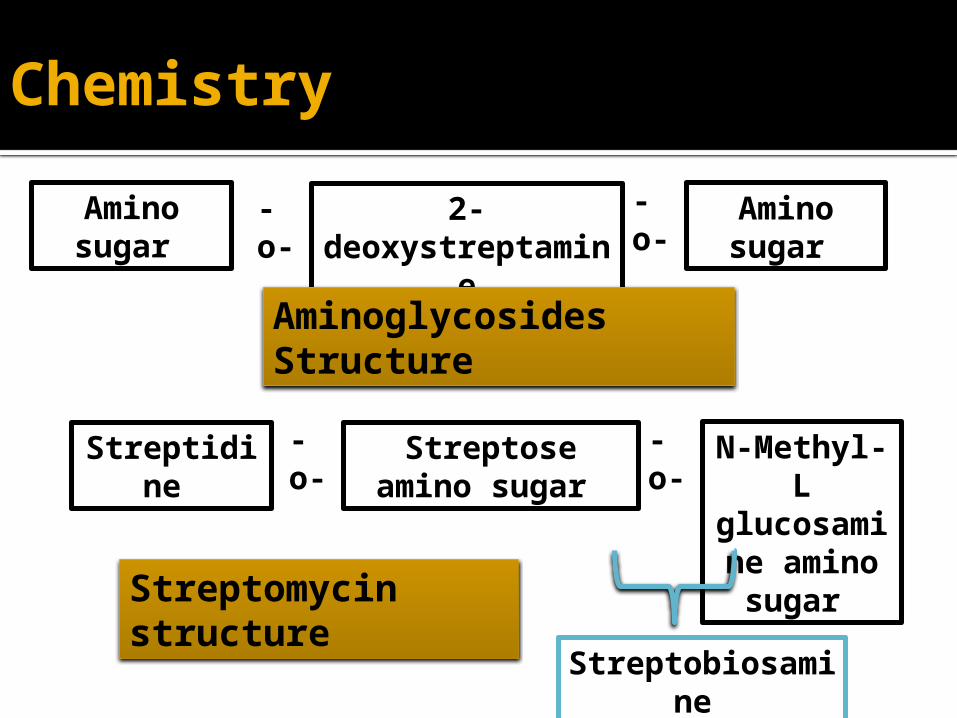
Amino sugar
2-deoxystreptami
ne
Amino sugar
-o-
-o-
Aminoglycosides Structure
Streptidine
Streptose amino sugar
N-Methyl-L
glucosamine amino
sugar
-o-
-o-
Streptobiosamine
Streptomycin structure
Chemistry

Aminoglycoside(AGL)
StretomycesSuffix -mycin
Streptomycin Paromomycin
Neomycin Tobramycin
MicromonosporaSuffix -micin
Gentamicin Amikacin
Netilmicin

Systemic Streptomycin Gentamicin Kanamycin Amikacin Sisomicin Tobramycin Netilimicin Parmomycin Soframycin Spectinomycin
Topical Neomycin Framycetin
Aminoglycosides

Properties
All are sulfate salts which are highly soluble in water and solutions are stable for monthsThey ionize in solution, not absorbed orally, distribute only extracellularly and do not penetrate in brain and CSFAll are excreted unchanged in urineAll are bactericidal and more active at alkaline pHAct by interfering bacterial protein synthesisActive against aerobic gm –ve bacteria, but spectrum differsPartial cross resistance, organisms resistant to one amino glycoside may still respond to anotherNarrow margin of safetyAll exhibit ototoxity and nephrotoxicity.

Aminoglycosides exhibit concentration dependent killingincreased conc. Can kill more bacteria at rapid rateThey also possess significant Post-antibiotic effect continue to suppress bacterial growth several hours after fall in MIC(Minimum Inhibitary Concentration)Single daily dosing at least as effective as and no more toxic than multiple dosing renal cortical uptake is a capacity dependent saturable processenhanced bactericidal activity
Post antibiotic effect

Mechanism of Action
The aminoglycosides are bactericidal antibioticsTransport of amino glycoside through the bacterial cell wall and cytoplasmic membrane Binding to ribosome resulting in inhibition of protein synthesis act on bacterial 30s ribosomes and distort the messenger ribonucleic acid translation of genetic code prevent the formation of normal complex required to initiate protein synthesis.Different aminoglycosides cause misreading at different levels depending on their selective affinity for specific ribosomal proteins.They also combines anionic membrane groups and damage the bacterial cell membranes (proteins, amino acids leak out) and also block energy production of Kreb’s cycle.

aa
A50S
30S
mRNA
template
Transferase site
P
Nascent polypeptide chain
Mechanism of action of Aminoglycosides
AG’s

50S
5’
5’
3’
5’ 3’AUG
5’ 3’AUG
30S
3’AUG
X
Blocks initiation
Premature termination
Wrong amino acid is incorporated
+ aminoglycosidemRNA translation
AminoglycosidesCauses misreading and premature termination of protein synthesis
Mature protein
Growing polypeptide

Aminoglycoside-bactericidal

30S: Aminoglycosides30S: Tetracyclines50S: Chloramphenicol, 50S: Macrolides, Lincosamides,50S: Linezolide, Streptogramins
RifampicinPolymyxinsβ-lactams, Glycopeptides
Mechanism of different antibiotics

May be plasmid mediated inactivation by microbial enzymes or
Failure of drug penetration mutation of porin channel
Synthesis of metabolizing enzymesAcetyl transferaseacetylationPhosphotransferase phosphorylationAdenyltransferase adenylation
Mutation may alter ribosomal binding site for the aminoglycosidesprevent binding to 30S
• Cross resistance is observed.
Resistance

Pharmacokinetics
Polar agents with poor oral bioavailability highly polar basic drugs with poor membrane permiabilityUsual routes: IM or I.VCmax achieved within 30-90 of IMT1/2—2-3hrsRenal insufficiency 24-48hrsAbsorption increases in inflammationNo significant amount in breast milkPlasma protein binding is minimalVd approximates 25% of lean body weight

Pharmacokinetics
Penetration of CNS: 10-25% of plasma levelDo not reach CSF, Intra-occular fluidAccumulates in the perilymph and endolymph as well as renal cortexVd increases in – leukaemia Elimination is by glomerular filtrationBoth haemo- and peritoneal dialysis remove aminoglycosides

Antibacterial spectrum
• Aerobic G-ve bacteria ( Citrobacter, Enterobacter, E. coli, proteus, shigella, proteus, Pseudomonas, Enterococci and Staph aureus )
• Streptomycin and kanamicin are active against mycobacterium tuberculosis while amikacin, gentamicin and tobramycin are active against S. faecalis and P. aeruginosa.
• They are not effective against G+ve bacilli, G-ve cocci and anaerobes

Therapeutic drug monitoring
Necessary in: Patients with life threatening infections Renal impairment 24 hours into new regimen Neonates Samples usually taken just before and 30 minutes
after a dose

STREPTOMYCIN
• It is older antibiotics and obtained by Streptomyces griseus, used in past but now used for treatment of TB.
• The antibacterium spectrum is relatively narrow.• Sensitive to H.ducrey, Brucella, F.tularensis, Nocardia, M.
tuberculosis, E. coli, Klebsiella, enterococci, Shigella
• Resistance-Many organisms develop rapid resistance. E. coli, S.aureus. S.pneumoniae are resistant
• Partial or unidirectional cross resistance occur.• Usual dosage: 15-25 mg per Kg body wt IM

Uses
TuberculosisSubacute bacterial endocarditisPlagueTularemiaUrinary tract infections, peritonitis, septicemias

GENTAMICIN
It was obtained from Micromonospora purpurea in1964 and has become most common antibiotic in acute infectionsPlasma half life 2-4 hours after i.m. injections same as StreptomicinIt is more potentIt has boarder spectrum of action and effective against P. aeruginosa and most strains of Proteus, E.coli, Klebsiella, enterobactor, SerratiaIt is not effective against M.tuberculosis, Str.pyogenes, St. Pneumoniae, and some St. AureusIt is more nephrotoxic.

GENTAMICIN
The dose calculated according to body weight and level of renal function. For an average adult, dose is 3-5 mg/kg/day, i.m. 0.3% eye ear drops.Uses-Inexpensive and reliable efficacyTherapeutic Applications: UTI, Pneumonia (nosocomial), Peritonitis, meningitis and sepsisIts use should be restricted to serious gram negative bacillary infectionsRespiratory infections-it is often combined with penicillin/cephalosporin or another antibiotic in these situationspoor penetration and low pH

GENTAMICIN
Aminoglycoside as single agent our side Urinay Tract is less effectiveTreatment of endocarditis Streptococci, staphylococci, enterococciPlasma levels upto 1-3mcg/ml Topical-infected burns, wounds, skin lessions (with purulent exudatesIntrathecal- meningitis caused by gram negetive b’a

TOBRAMYCIN
Similar antibacterial spectrum with gentamicin Dose-5-6mg/kgTreat infections caused by P.aeruginosa, enterococcus fecalisLower respiratory tract infections by pseudomonas aeruginosa in cystic fibrosis 300mg/5ml inhalational solution is administeredNeprotoxicity is less than gentamicin

AMIKACIN
Less toxic semisynthetic derivative of kanamycinResistant to enzymes that inactivate gentamicin and tobramcyin Widest spectrum of activity Uses: Same as gentamicinReserve drug for hospital acquired Gm-ve bacillary infections Multidrug resistant TB resistant to streptomycin, along with other drugs Dose : 15mg/kg/day in 1-3 doses

• Identical to gentamicin • More potent on pseudomonas and -hemolytic
streptococci • Used interchangeably with gentamicin
SISOMYCIN

NETILMICIN
Resistant to many enzyme that inactivate gentamicin and tobramycin additional ethyl group protects from enzymatic degradationLowest toxicity among aminoglycosidesSemisynthetic derivative of sisomicin More active against klebsiella, enterobacter & staphylococci Less active against pseudomonas aeruginosa Doses and pharmacokinetics similar to gentamicin Uses-Septicemia, Lower respiratory tract infection Urinary tract infection, peritonitis and endometritis

wide spectrum active against Gm-ve bacilli and some gm+ve cocci
Pseudomonas and strep.pyogenes not sensitive Topically used in skin, eye and external ear infections
combined with bacitracin or polymyxin-B to widen antibacterial spectrum and to prevent emergence of resistant strains
Solutions 1-5mg/ml used on infected surfaces, injected into joints, pleural cavity, tissue spaces, abscess cavities
NEOMYCIN AND KANAMYCIN

NEOMYCIN AND KANAMYCIN
Preparation of bowel before surgery 1 gm TDS + erlythromycin base aerobic flora
Hepatic encephalopathy- 1g/6th hrlyused to suppress coliform flora, with decreased protein intake, + lactulose decrease ammonia production
Bladder irrigation along with polymyxin B

PARAMOMYCIN
Properties similar to neomycin Effective against visceral leishmainiasis by parentral routeUses – Intestinal infectionsTreatment of hepatic encephalopathy Treatment of amoebiasis

Very similar to neomycin Too toxic for systemic administration Used topically on skin, eye ear
FRAMYCETIN

Adverse effects
Ototoxicity: Vestibular and cochlear part affected. concentrated in labyrinthine fluid. greater when plasma concentration of drug is high. Vestibular/cochlear sensory cells get destructive changes
Nephrotoxicity-It is more in elderly and in those with preexisting kidney disease. Damage is reversible if drug is discontinued.It has been suggested that aminoglycosides interfere with production of prostaglandins in kidney and so there is reduced GFR.
Adverse effects
Neuromuscular blockade: All aminoglycosides reduce Ach release from motor nerve ending, they have curare like action and cause neuromuscular blockade that can cause paralysis and fatal respiratory arrest.They may cause apnea on iv injection, the blockade if severe can be effectively treated by neostigmine.Neurotoxic effects – Optic neuritis, peripheral neuritis, Others: Angioedema, skin rash, blood dyscrasia, eosinophilia, fever, stomatitis, anaphylaxis
Contraindication
PregnancyMyasthenia gravis Renal impairmentParkinson’s diseaseEar drops are contraindicated . Hearing defect, deafness, tinnitus appears, on stopping drug tinnitus disappers.

DRUG INTERACTIONS
Antipseudomonal penicillins inactivate aminoglycosides.Ethacrynic acid loop diuretics.Nephrotoxic agents.Neuromuscular blocking agents.
ACh ACh
ACh
ACh
AChACh
ACh
Ac + Ch
cholineacetyltransferase
high affinityuptake
vesicle
receptorACh esterase
ACh
tdh
AcetylCoA + Ch
TDH 7/9
0
SPECTINOMYCIN
Aminocyclitol antibiotic Lacks amino sugars and glycoside bonds Drug resistant gonorrhoea and penicillin-allergic
patients Given by IM route 40mg/kg Nephrotoxicity and anemia can occur

THANK YOUDownload slides from
Authorstream/presentations/raghuprasada
Slideshare/presentations/raghuprasada
Youtube/raghuprasada