clarion interprofessional case competition€¦ · transplant confusion at southview hospital page...
TRANSCRIPT

CLARION Interprofessional Case Competition, Spring 2007
Transplant Confusion at Southview Hospital Page 1 of 21 This case study was prepared for the CLARION Interprofessional Case Competition. It was developed as the basis for discussion in the Case Competition. Information in this case is fabricated/fictitious. Any resemblance to any healthcare provider is purely coincidental. No part of this publication may be reproduced, stored in a retrieval system, used in a spreadsheet, or transmitted in any form or by any means-electronic, mechanical, photocopying, recording, or otherwise without the permission of the University of Minnesota.
© 2007 University of Minnesota Board of Regents. The University of Minnesota is an equal-opportunity employer and educator. This document is available in alternate formats. For information, contact Barbara Blalock 612-626-7379.
CLARION INTERPROFESSIONAL CASE COMPETITION
CLARION An Interprofessional Student Committee of the
Center for Health Interprofessional Programs (CHIP) UNIVERSITY OF MINNESOTA
Transplant Confusion at Southview Hospital
The details contained in this case were written as a team by (listed alphabetically)
Karin Alaniz, Ph.D., R.N.
Senior Teaching Specialist School of Nursing
University of Minnesota
Karyn Baum, M.D., M.S. Ed. Associate Professor of Medicine
Special Assistant to the Dean School of Medicine
University of Minnesota
Sandra Potthoff, Ph.D. Associate Professor and MHA Program Director
Division of Health Services Research and Policy
School of Public Health University of Minnesota
William Riley, Ph.D. Associate Dean
School of Public Health University of Minnesota
Don Uden, Pharm.D. Professor
Pharmaceutical Care and Health Systems Associate Dean for Student Services
College of Pharmacy University of Minnesota
Edited by Rebecca Lentz, Director of Communications, University of Minnesota College of Pharmacy

CLARION Interprofessional Case Competition, Spring 2007
Transplant Confusion at Southview Hospital Page 2 of 21 This case study was prepared for the CLARION Interprofessional Case Competition. It was developed as the basis for discussion in the Case Competition. Information in this case is fabricated/fictitious. Any resemblance to any healthcare provider is purely coincidental. No part of this publication may be reproduced, stored in a retrieval system, used in a spreadsheet, or transmitted in any form or by any means-electronic, mechanical, photocopying, recording, or otherwise without the permission of the University of Minnesota.
© 2007 University of Minnesota Board of Regents. The University of Minnesota is an equal-opportunity employer and educator. This document is available in alternate formats. For information, contact Barbara Blalock 612-626-7379.
Case Study Assignment In Crossing the Quality Chasm, the Institute of Medicine proposed that health care in the 21st
Century must be “delivered by systems that are carefully and consciously designed to provide
care that is safe, effective, patient-centered, timely, efficient and equitable. Such systems must be
designed to serve the needs of patients and to ensure that they are fully informed, retain control
and participate in care delivery whenever possible and receive care that is respectful of their
values and preferences. Such systems must facilitate the application of scientific knowledge to
practice and provide clinicians with the tools and supports necessary to deliver evidence-based
care consistently and safely.”
Clinicians at Southview Hospital faced a challenge developing a care plan when John Benson, a
53-year-old man with a history of alcohol abuse, arrived at the hospital’s emergency department.
Cases such as Mr. Benson’s present challenges to developing systems and processes that fulfill
the aims defined in Crossing the Quality Chasm.
The CEO of Southview Hospital asked your interprofessional team to study Mr. Benson’s
sentinel event, understand the sequence of events that lead to this situation and how and why
they occurred. He’s asked you to develop a set of recommendations and an action plan to prevent
the errors from recurring. You must include a cost analysis of your recommendations. Your
recommendations should demonstrate an understanding of the clinical decision-making
challenges facing care providers in cases such as this. Your team should ensure your analysis,
findings and recommendations focus on systems and processes that need to be improved,
changed or eliminated. Your recommendation should also focus on new systems and processes
that should be adopted and not place blame on individuals. You will present your findings,
conclusions and recommendations to the Quality Committee of the Board of Southview Hospital.

CLARION Interprofessional Case Competition, Spring 2007
Transplant Confusion at Southview Hospital Page 3 of 21 This case study was prepared for the CLARION Interprofessional Case Competition. It was developed as the basis for discussion in the Case Competition. Information in this case is fabricated/fictitious. Any resemblance to any healthcare provider is purely coincidental. No part of this publication may be reproduced, stored in a retrieval system, used in a spreadsheet, or transmitted in any form or by any means-electronic, mechanical, photocopying, recording, or otherwise without the permission of the University of Minnesota.
© 2007 University of Minnesota Board of Regents. The University of Minnesota is an equal-opportunity employer and educator. This document is available in alternate formats. For information, contact Barbara Blalock 612-626-7379.
Background
Southview Hospital
Southview Hospital, located in Tampa, Fla., is a 525-bed facility that has seven primary care
clinics located throughout the greater Tampa-St. Petersburg area. It is a not-for-profit hospital
and is not part of any other healthcare system. Approximately 30 percent of patient rooms are
private. The rest have two patient beds per room.
The mission of Southview Hospital is to improve, in a manner that exceeds expectations of
patients and visitors, the health and quality of life for the people it serves. Its values include:
• Respect for the inherent dignity of patients and their families
• Collaboration with patients, families and providers to achieve common goals
• Integrity to ensure all decisions and care are provided with the highest ethical practices
and
• Service excellence in all aspects of care.
Southview Hospital is known for its stroke and heart care. A national news magazine named
Southview one of the top 100 hospitals in the country for cardiovascular care. All clinics have
computerized outpatient medical records. Although physicians in the hospital cannot access
clinic records, all laboratory results are available to physicians in the clinics and hospital
regardless of where the labs were drawn. Approximately 60 percent of Southview Hospital
patients were never seen at one of its clinics.
It was a typical day at the hospital when John Benson, a regular patient in one of the Southview
Hospital clinics, arrived at the emergency department.

CLARION Interprofessional Case Competition, Spring 2007
Transplant Confusion at Southview Hospital Page 4 of 21 This case study was prepared for the CLARION Interprofessional Case Competition. It was developed as the basis for discussion in the Case Competition. Information in this case is fabricated/fictitious. Any resemblance to any healthcare provider is purely coincidental. No part of this publication may be reproduced, stored in a retrieval system, used in a spreadsheet, or transmitted in any form or by any means-electronic, mechanical, photocopying, recording, or otherwise without the permission of the University of Minnesota.
© 2007 University of Minnesota Board of Regents. The University of Minnesota is an equal-opportunity employer and educator. This document is available in alternate formats. For information, contact Barbara Blalock 612-626-7379.
Sentinel Event
Day One John Benson, a 53-year-old man with a long history of alcohol abuse, came to the emergency
department (ED) at Southview Hospital because of his wife’s insistence. He had not been eating
well for a week. For the last 24 hours, he had become very short of breath. Upon arrival, Mr.
Benson’s pulse was 184, and he was sweating profusely. The triage nurse Jamie Miller RN took
him directly back to see the ED physician and obtained an electrocardiogram (ECG).
The ECG showed that Mr. Benson had supraventricular tachycardia. The ED physician Sue
Wood, MD, ordered intravenous (IV) adenosine. Once Jamie Miller RN administered the
adenosine, Mr. Benson’s rhythm returned to a normal sinus rhythm. Within minutes of Mr.
Benson having a normal heart rhythm, his lab work was returned. Lab work, which was draw
upon Mr. Benson’s arrival in the ED, showed he was in renal failure with a serum creatinine of
4.2 mg/dL. During a visit to the clinics four months earlier, the serum creatinine level was
1.3 mg/dL. His liver function had also worsened. Upon admission to the ED, his total bilirubin
was 22.1 mg/dL, albumin of 2.2 g/dL, ALT of 40 U/L and AST of 53 U/L and troponin was
<0.6. He denied any chest pain.
After discussing Mr. Benson’s case with the on-call gastroenterologist, Sue Wood, MD admitted
Mr. Benson for acute renal failure and an expedited liver transplant workup. Sue Wood, MD told
Mr. Benson’s wife that Mr. Benson would be admitted and recommended Mrs. Benson return

CLARION Interprofessional Case Competition, Spring 2007
Transplant Confusion at Southview Hospital Page 5 of 21 This case study was prepared for the CLARION Interprofessional Case Competition. It was developed as the basis for discussion in the Case Competition. Information in this case is fabricated/fictitious. Any resemblance to any healthcare provider is purely coincidental. No part of this publication may be reproduced, stored in a retrieval system, used in a spreadsheet, or transmitted in any form or by any means-electronic, mechanical, photocopying, recording, or otherwise without the permission of the University of Minnesota.
© 2007 University of Minnesota Board of Regents. The University of Minnesota is an equal-opportunity employer and educator. This document is available in alternate formats. For information, contact Barbara Blalock 612-626-7379.
home and get some rest. It was 10 p.m., nearly four hours after the Bensons arrived at the
emergency department.
Upon arrival to his shared room on the medical/surgical unit, Mr. Benson met Kathy Swanson,
RN, who was assigned to care for him during the night shift. Kathy Swanson, RN tried to get a
history from Mr. Benson but found him to be quite confused. Jamie Miller RN, briefly
mentioned Mr. Benson was an alcoholic, so Kathy Swanson, RN worried he might be going into
withdrawal. She quickly checked his vital signs and found he had a respiration rate of 24 breaths
per minute, a heart rate of 110 beats per minute, a temperature of 98.4 degrees F and a blood
pressure of 94/54 mmHg. He was slightly hypoxic with a room air saturation of 88 percent,
although it increased to 97 percent as soon as she administered two liters of oxygen/minute via
nasal cannula. Kathy Swanson, RN was unable to obtain most of Mr. Benson’s history due to his
confusion. She called the hospitalist Alex Mechamber, MD, and informed him the patient had
arrived on the floor.
About 30 minutes later, Alex Mechamber, MD arrived to see Mr. Benson. Alex Mechamber, MD
observed Mr. Benson was confused, slightly hypoxic and noticeably jaundiced. His exam
revealed multiple stigmata of chronic liver disease including lower extremity edema, fluid in the
abdomen (ascites) and jaundice. After confirming the labs and reviewing the chest x-ray
(normal) on the electronic medical record (EMR), Alex Mechamber, MD wrote admission orders
that included renal and GI consults for the next morning. He also consulted Lucas Pratt, PharmD,
a clinical pharmacist to start Mr. Benson on the alcohol withdrawal protocol and ordered an
indwelling foley catheter be placed to better monitor the patient’s urine output.
CLARION Interprofessional Case Competition, Spring 2007
Transplant Confusion at Southview Hospital Page 6 of 21 This case study was prepared for the CLARION Interprofessional Case Competition. It was developed as the basis for discussion in the Case Competition. Information in this case is fabricated/fictitious. Any resemblance to any healthcare provider is purely coincidental. No part of this publication may be reproduced, stored in a retrieval system, used in a spreadsheet, or transmitted in any form or by any means-electronic, mechanical, photocopying, recording, or otherwise without the permission of the University of Minnesota.
© 2007 University of Minnesota Board of Regents. The University of Minnesota is an equal-opportunity employer and educator. This document is available in alternate formats. For information, contact Barbara Blalock 612-626-7379.
Although the hospital’s EMR was partially implemented last year, it is used mainly for lab
results and dictations. Physicians still hand write orders, which are then entered in the hospital’s
computer system by the health unit coordinator. Full implementation of the EMR is not
scheduled for another eight months. Alex Mechamber, MD handed the written orders to the
health unit coordinator, who entered the orders (“took them off”) and made a note on the original
page. She missed the foley catheter order in the long list of orders. Subsequently that order was
never entered in the system.
Alex Mechamber, MD was concerned that Mr. Benson could have spontaneous bacterial
peritonitis. He decided to perform a diagnostic paracentesis and removed for analysis and culture
a small amount of fluid from Mr. Benson’s abdomen. Because of Mr. Benson’s confusion, Alex
Mechamber, MD obtained consent for the procedure during a phone conversation with Mrs.
Benson. The paracentesis was performed, and the aspirated fluid obtained confirmed his
suspicion that Mr. Benson had bacterial peritonitis. Mr. Benson was started on ciprofloxacin.
Kathy Swanson, RN checked on Mr. Benson again. He still seemed agitated and was slightly
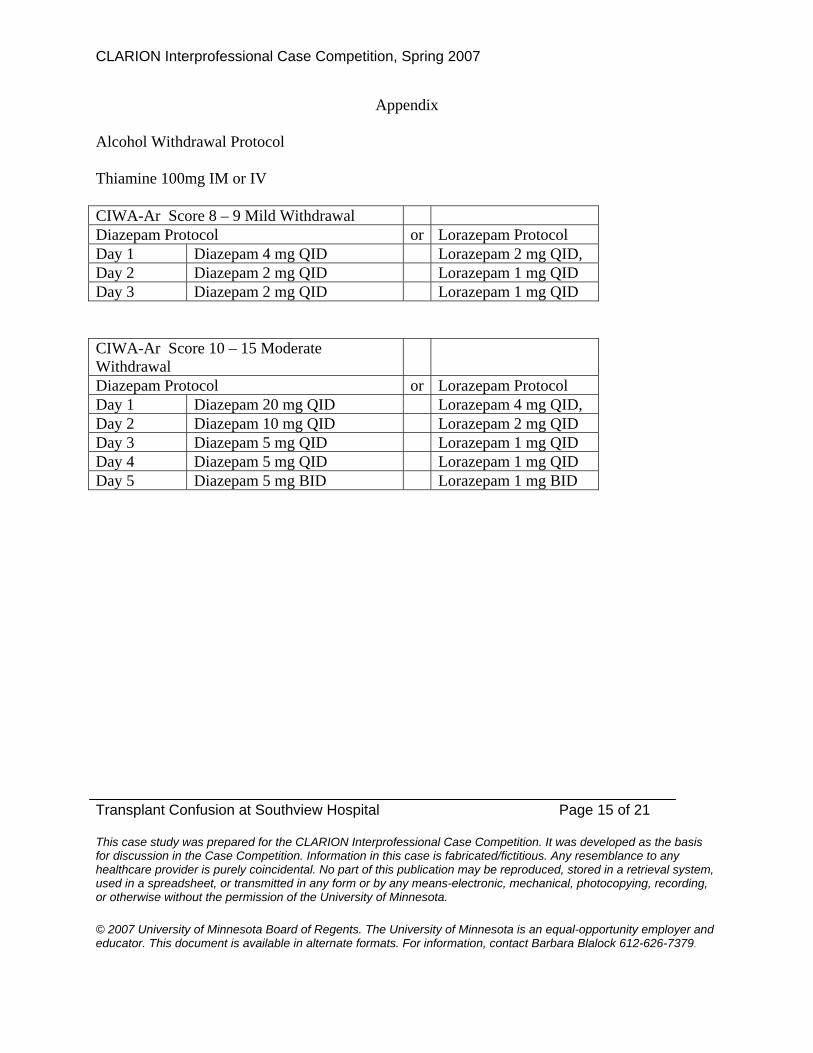
tachycardic at 116 beats per minute. According to the alcohol withdrawal protocol, Lucas Pratt,
PharmD determined Mr. Benson’s Clinical Institute Withdrawal Assessment (CIWA-Ar) score
was 12 points (Appendix). Following protocol, Lucas Pratt, PharmD ordered 20 mg of diazepam
(orally) and thiamine 100 mg intravenously. Mr. Benson eventually calmed down but had
restless sleep throughout the night.

CLARION Interprofessional Case Competition, Spring 2007
Transplant Confusion at Southview Hospital Page 7 of 21 This case study was prepared for the CLARION Interprofessional Case Competition. It was developed as the basis for discussion in the Case Competition. Information in this case is fabricated/fictitious. Any resemblance to any healthcare provider is purely coincidental. No part of this publication may be reproduced, stored in a retrieval system, used in a spreadsheet, or transmitted in any form or by any means-electronic, mechanical, photocopying, recording, or otherwise without the permission of the University of Minnesota.
© 2007 University of Minnesota Board of Regents. The University of Minnesota is an equal-opportunity employer and educator. This document is available in alternate formats. For information, contact Barbara Blalock 612-626-7379.
Day Two
The next day, Alex Mechamber, MD signed out his patients, including Mr. Benson, to the
hospitalist for the day, Nancy Husby, MD. At about the same time, Kathy Swanson, RN let her
charge nurse know about Mr. Benson so the information could be shared with his day nurse John
Rhee, LPN. Both Alex Mechamber, MD and Kathy Swanson, RN mentioned Mr. Benson’s
confusion, possible alcohol withdrawal and renal failure. That morning Lucas Pratt, PharmD
ordered diazepam 20 mg PO four times daily.
Nancy Husby, MD reviewed Mr. Benson’s labs and vitals. Mr. Benson’s morning labs showed
that his renal failure was worsening: His serum creatinine was 4.7 mg/dL, and his potassium had
increased to 5.4 mmol/L. His liver function tests and vital signs were essentially unchanged. She
could not find any notation about his urine output and spoke with John Rhee, LPN. John Rhee,
LPN said he had not been able to follow Mr. Benson’s urine output because of Mr. Benson’s
incontinence several times during since admission. Nancy Husby MD asked John Rhee, LPN
about the foley catheter order noted in the handwritten orders. John Rhee, LPN said he didn’t see
that order in the EMR but promised to place a catheter as soon as possible.
Mrs. Benson arrived at the hospital around 10 a.m. She was met in the room by the
gastrointestinal physician. When asked about Mr. Benson’s drinking history, Mrs. Benson
admitted that his last drink was three weeks ago. Mr. Benson drank at least a quart of vodka a
day and quit only when he became nauseated. He went through alcohol treatment three times but
always began drinking within a month of completing treatment.
CLARION Interprofessional Case Competition, Spring 2007
Transplant Confusion at Southview Hospital Page 8 of 21 This case study was prepared for the CLARION Interprofessional Case Competition. It was developed as the basis for discussion in the Case Competition. Information in this case is fabricated/fictitious. Any resemblance to any healthcare provider is purely coincidental. No part of this publication may be reproduced, stored in a retrieval system, used in a spreadsheet, or transmitted in any form or by any means-electronic, mechanical, photocopying, recording, or otherwise without the permission of the University of Minnesota.
© 2007 University of Minnesota Board of Regents. The University of Minnesota is an equal-opportunity employer and educator. This document is available in alternate formats. For information, contact Barbara Blalock 612-626-7379.
Early that afternoon, the gastrointestinal and renal physicians left their handwritten
recommendations on the chart. The gastrointestinal physician wrote “the patient is not a
transplant candidate given his recent drinking.” The renal physician noted the worsening renal
failure but stated he didn’t believe Mr. Benson had any indications to begin dialysis that day. The
renal physician noted Mr. Benson may require dialysis in the next few days.
After hearing Mr. Benson fall, John Rhee, LPN found Mr. Benson on the floor in his room
around 8 p.m.. Although confused, Mr. Benson stated he woke up and felt as if he needed to
urinate. He was trying to get to the bathroom when he fell. Two nurses helped him back to bed.
A bed alarm was ordered and placed. He had no obvious injuries, but Mr. Benson’s nurse that
night notified Mrs. Benson and the hospitalist on-call that Mr. Benson had fallen.
Day Three
Mr. Benson’s course during the day was unchanged. He remained confused, agitated and
produced only 200 mL of urine that day. Lucas Pratt, PharmD ordered diazepam 10 mg PO four
times daily.
Day Four
In this morning, Mr. Benson remained confused and again tried to get out of bed and go to the
bathroom. He nearly fell but was caught at the last minute by his roommate. Mr. Benson’s nurse
spoke with the charge nurse, and they requested an attendant. Lucas Pratt, PharmD ordered
diazepam 5 mg PO four times daily.
CLARION Interprofessional Case Competition, Spring 2007
Transplant Confusion at Southview Hospital Page 9 of 21 This case study was prepared for the CLARION Interprofessional Case Competition. It was developed as the basis for discussion in the Case Competition. Information in this case is fabricated/fictitious. Any resemblance to any healthcare provider is purely coincidental. No part of this publication may be reproduced, stored in a retrieval system, used in a spreadsheet, or transmitted in any form or by any means-electronic, mechanical, photocopying, recording, or otherwise without the permission of the University of Minnesota.
© 2007 University of Minnesota Board of Regents. The University of Minnesota is an equal-opportunity employer and educator. This document is available in alternate formats. For information, contact Barbara Blalock 612-626-7379.
When John Rhee, LPN took Mr. Benson’s vitals at 7 a.m., he found Mr. Benson’s blood pressure
was 80/47 mm/Hg. There was 50 mL of urine in the foley catheter bag, which had not been
emptied in eight hours. John Rhee, LPN paged Grant Anderson, MD who was the hospitalist of
the day. Grant Anderson, MD ordered a 500 mL normal saline fluid flush and said he would
return to assess the patient within 30 minutes.
When Grant Anderson, MD returned, he noted Mr. Benson was quite confused, was pulling at
his lines and had diffuse wheezes on examination. Mr. Benson’s abdomen was tense and
distended. Grant Anderson, MD felt Mr. Benson needed a large volume paracentesis and
arranged for the test.
The scheduling nurse in interventional radiology asked about Mr. Benson’s platelet count and
international normalized ratio (INR), which tests his ability to clot after a procedure. Although
his platelet count was normal, Mr. Benson’s INR was elevated at 2.7. The nurse asked Grant
Anderson, MD to correct Mr. Benson’s INR with fresh frozen plasma (FFP) prior to the
procedure. That correction was made. During the procedure, four liters of fluid were removed.
Mr. Benson received intravenous (IV) albumin during the procedure.
Day Five
By day five, Mr. Benson’s serum creatinine had climbed to 6.9 mg/dl, and he required
kayexelate daily to treat his elevated potassium. His BUN had slowly risen from 40 mg/dL on
admission to 81 mg/dL. Mr. Benson remained quite confused despite receiving lactulose and
rifaximin for hepatic encephalopathy, antibiotics for spontaneous bacterial peritonitis and

CLARION Interprofessional Case Competition, Spring 2007
Transplant Confusion at Southview Hospital Page 10 of 21 This case study was prepared for the CLARION Interprofessional Case Competition. It was developed as the basis for discussion in the Case Competition. Information in this case is fabricated/fictitious. Any resemblance to any healthcare provider is purely coincidental. No part of this publication may be reproduced, stored in a retrieval system, used in a spreadsheet, or transmitted in any form or by any means-electronic, mechanical, photocopying, recording, or otherwise without the permission of the University of Minnesota.
© 2007 University of Minnesota Board of Regents. The University of Minnesota is an equal-opportunity employer and educator. This document is available in alternate formats. For information, contact Barbara Blalock 612-626-7379.
diazepam for possible alcohol withdrawal. Lucas Pratt, PharmD ordered diazepam 5 mg PO two
times daily.
Back from her day off, Nancy Husby, MD visited Mr. Benson during her morning rounds. Mrs.
Benson asked when her husband would be placed on the transplant list. Surprised by the request,
Nancy Husby, MD reviewed Mr. Benson’s chart and confirmed there were two notes from the
gastroenterologist physician stating that Mr. Benson wasn’t a transplant candidate because of
recent drinking and an extremely poor three-month prognosis. Nancy Husby, MD explained this
to Mrs. Benson, who became quite upset she was not informed earlier. Mrs. Benson said she felt
that the hospital had “mislead her and her husband” since they were told Mr. Benson was being
admitted for an expedited transplant workup.
About 3 p.m., Mr. Benson was still confused, and he pulled out his intravenous line despite the
presence of an attendant in the room. Due to Mr. Benson’s coagulopathy, he bled quite
profusely. His nurse finally controlled the bleeding within 30 minutes by placing pressure where
the intravenous line had been.
Day Six
Kathy Swanson, RN was Mr. Benson’s night nurse. Just after midnight, she found him to be very
short of breath. His respiration was 32 breaths per minute, and his oxygen saturation was 92
percent on two liters of oxygen/minute. Kathy Swanson, RN called the overnight hospitalist
David Cramer, MD, who promptly saw Mr. Benson.

CLARION Interprofessional Case Competition, Spring 2007
Transplant Confusion at Southview Hospital Page 11 of 21 This case study was prepared for the CLARION Interprofessional Case Competition. It was developed as the basis for discussion in the Case Competition. Information in this case is fabricated/fictitious. Any resemblance to any healthcare provider is purely coincidental. No part of this publication may be reproduced, stored in a retrieval system, used in a spreadsheet, or transmitted in any form or by any means-electronic, mechanical, photocopying, recording, or otherwise without the permission of the University of Minnesota.
© 2007 University of Minnesota Board of Regents. The University of Minnesota is an equal-opportunity employer and educator. This document is available in alternate formats. For information, contact Barbara Blalock 612-626-7379.
Mr. Benson’s abdomen was tense and tender. He took short, shallow breaths which were limited
by his ascites (fluid in his abdomen). David Cramer, MD performed an emergent bedside
paracentesis after giving Mr. Benson another six units of FFP. David Cramer, MD removed
another four liters of fluid from Mr. Benson’s abdomen. By the end of the procedure, Mr.
Benson seemed to be breathing more easily.
Mr. Benson’s morning labs were returned by 8 a.m. The labs showed his creatinine was up to 7.7
mg/dL, and his blood urea nitrogen (BUN) was 85 mg/dL. He was still quite confused, oriented
to person only and had crackles on his lung exam consistent with fluid overload. The
nephrologist saw Mr. Benson and decided to begin dialysis later that day after a femoral dialysis
line could be placed.
The gastrointestinal physician also saw Mr. Benson again and reaffirmed he was not a transplant
candidate because of his lack of sobriety and his nearly 100 percent three-month mortality.
That afternoon, the nephrologist decided to place a specialized femoral line for dialysis access.
He asked June Carter, RN, Mr. Benson’s shift nurse, to assist him. June Carter, RN was new to
the medicine unit and had never helped place a femoral line. She was afraid to mention this to
the physician. June Carter, RN was also concerned because she had four other patients, one of
whom required frequent pain medications. She told the nephrologist she wasn’t sure the line
should be placed on the unit. He replied he had placed them on other medicine units in other
hospitals.
During the procedure, the nephrologist accidentally cannulated the right femoral artery (instead
of the femoral vein). This led to significant bleeding into the groin area. Despite direct pressure,

CLARION Interprofessional Case Competition, Spring 2007
Transplant Confusion at Southview Hospital Page 12 of 21 This case study was prepared for the CLARION Interprofessional Case Competition. It was developed as the basis for discussion in the Case Competition. Information in this case is fabricated/fictitious. Any resemblance to any healthcare provider is purely coincidental. No part of this publication may be reproduced, stored in a retrieval system, used in a spreadsheet, or transmitted in any form or by any means-electronic, mechanical, photocopying, recording, or otherwise without the permission of the University of Minnesota.
© 2007 University of Minnesota Board of Regents. The University of Minnesota is an equal-opportunity employer and educator. This document is available in alternate formats. For information, contact Barbara Blalock 612-626-7379.
the site continued to bleed heavily. June Carter, RN informed the nephrologist that Mr. Benson’s
morning labs showed an INR of 3.8. The nephrologist ordered six units of fresh frozen plasma
stat. June Carter RN held pressure on the site for another 30 minutes.
While June Carter, RN applied direct pressure to the site, the nephrologist called interventional
radiology to place the dialysis access line. The staff in interventional radiology agreed to do the
procedure as an add-on (i.e,. when they have time). The staff in interventional radiology insisted
the INR be less than 1.4 prior to the procedure. After a total of 10 units of FFP, the INR was 1.3.
Interventional radiology placed dialysis access (Quenton) placed around 10 p.m. Dialysis was
planned for first thing the next morning.
Day Seven
At 5 a.m. Kathy Swanson, RN noticed Mr. Benson was very short of breath, breathing nearly 40
times a minute and using accessory muscles to breathe. She promptly paged Alex Mechamber,
MD, who paged the nephrologists to dialyze Mr. Benson. The dialysis run removed 3.5 liters of
fluid. The nephrologist planned to dialyze Mr. Benson again the next day to remove more fluid.
Day Eight
After his second dialysis run, Mr. Benson was noticeably less confused. He stopped pulling at his
intravenous lines and was able to eat more than a few bites at a time. Mr. Benson was extremely
weak. Physical and occupational therapists began working with him to improve his strength.
During the next three days, Mr. Benson continued to undergo dialysis and have fluid removed

CLARION Interprofessional Case Competition, Spring 2007
Transplant Confusion at Southview Hospital Page 13 of 21 This case study was prepared for the CLARION Interprofessional Case Competition. It was developed as the basis for discussion in the Case Competition. Information in this case is fabricated/fictitious. Any resemblance to any healthcare provider is purely coincidental. No part of this publication may be reproduced, stored in a retrieval system, used in a spreadsheet, or transmitted in any form or by any means-electronic, mechanical, photocopying, recording, or otherwise without the permission of the University of Minnesota.
© 2007 University of Minnesota Board of Regents. The University of Minnesota is an equal-opportunity employer and educator. This document is available in alternate formats. For information, contact Barbara Blalock 612-626-7379.
slowly. He required another paracentesis to remove fluid from his abdomen. He was very weak
and struggled with intermittent nausea.
Day Eleven
June Carter, RN was Mr. Benson’s nurse this day. Mrs. Benson told June Carter, RN she felt
frustrated. Mrs. Benson stated she felt as if the doctors reacted to each new problem but her
husband’s overall care plan and prognosis were unclear.
That afternoon, there was a hastily assembled care conference. Attending the conference were
the Bensons, the care coordinator and Alex Mechamber, MD. June Carter, RN only attended for
a few minutes because of other patient-care duties. The physician conducted the care conference
during which Mr. Benson’s very poor overall prognosis and the inability to offer him a transplant
were discussed. The participants also discussed the code status. Mr. Benson was afraid to
designate himself as do not resuscitate (DNR/DNI) because he worried the “doctors would give
up” on and ignore him. The care plan did not significantly change as a result of the conference.
Day Fourteen
During his dialysis session, Mr. Benson suddenly became acutely short of breath and
hypotensive. Despite administration of intravenous normal saline, Mr. Benson’s blood pressure
remained dangerously low at 76/44 mmHg. He was immediately transferred to the intensive care
unit.

CLARION Interprofessional Case Competition, Spring 2007
Transplant Confusion at Southview Hospital Page 14 of 21 This case study was prepared for the CLARION Interprofessional Case Competition. It was developed as the basis for discussion in the Case Competition. Information in this case is fabricated/fictitious. Any resemblance to any healthcare provider is purely coincidental. No part of this publication may be reproduced, stored in a retrieval system, used in a spreadsheet, or transmitted in any form or by any means-electronic, mechanical, photocopying, recording, or otherwise without the permission of the University of Minnesota.
© 2007 University of Minnesota Board of Regents. The University of Minnesota is an equal-opportunity employer and educator. This document is available in alternate formats. For information, contact Barbara Blalock 612-626-7379.
Upon arrival to the intensive care unit, Mr. Benson’s breathing worsened. He was intubated and
started on prophylactic broad-spectrum antibiotics. He received intravenous medications to
maintain his blood pressure. The medical team called Mrs. Benson and told her about Mr.
Benson’s change in status.
Six hours later, Mr. Benson went into cardiac arrest. Despite all efforts, he could not be revived
and was pronounced dead after 45 minutes of resuscitation efforts.
Mrs. Benson confided to the medical intensive care unit nurse that Mr. Benson would not have
wanted any more invasive procedures. Mrs. Benson said she didn’t know how to tell the
physicians. He wanted to die at home with his family. Mrs. Benson deeply regretted not making
that happen.
CLARION Interprofessional Case Competition, Spring 2007
Transplant Confusion at Southview Hospital Page 15 of 21 This case study was prepared for the CLARION Interprofessional Case Competition. It was developed as the basis for discussion in the Case Competition. Information in this case is fabricated/fictitious. Any resemblance to any healthcare provider is purely coincidental. No part of this publication may be reproduced, stored in a retrieval system, used in a spreadsheet, or transmitted in any form or by any means-electronic, mechanical, photocopying, recording, or otherwise without the permission of the University of Minnesota.
© 2007 University of Minnesota Board of Regents. The University of Minnesota is an equal-opportunity employer and educator. This document is available in alternate formats. For information, contact Barbara Blalock 612-626-7379.
Appendix Alcohol Withdrawal Protocol Thiamine 100mg IM or IV CIWA-Ar Score 8 – 9 Mild Withdrawal Diazepam Protocol or Lorazepam Protocol Day 1 Diazepam 4 mg QID Lorazepam 2 mg QID, Day 2 Diazepam 2 mg QID Lorazepam 1 mg QID Day 3 Diazepam 2 mg QID Lorazepam 1 mg QID CIWA-Ar Score 10 – 15 Moderate Withdrawal
Diazepam Protocol or Lorazepam Protocol Day 1 Diazepam 20 mg QID Lorazepam 4 mg QID, Day 2 Diazepam 10 mg QID Lorazepam 2 mg QID Day 3 Diazepam 5 mg QID Lorazepam 1 mg QID Day 4 Diazepam 5 mg QID Lorazepam 1 mg QID Day 5 Diazepam 5 mg BID Lorazepam 1 mg BID
CLARION Interprofessional Case Competition, Spring 2007
Transplant Confusion at Southview Hospital Page 16 of 21 This case study was prepared for the CLARION Interprofessional Case Competition. It was developed as the basis for discussion in the Case Competition. Information in this case is fabricated/fictitious. Any resemblance to any healthcare provider is purely coincidental. No part of this publication may be reproduced, stored in a retrieval system, used in a spreadsheet, or transmitted in any form or by any means-electronic, mechanical, photocopying, recording, or otherwise without the permission of the University of Minnesota.
© 2007 University of Minnesota Board of Regents. The University of Minnesota is an equal-opportunity employer and educator. This document is available in alternate formats. For information, contact Barbara Blalock 612-626-7379.
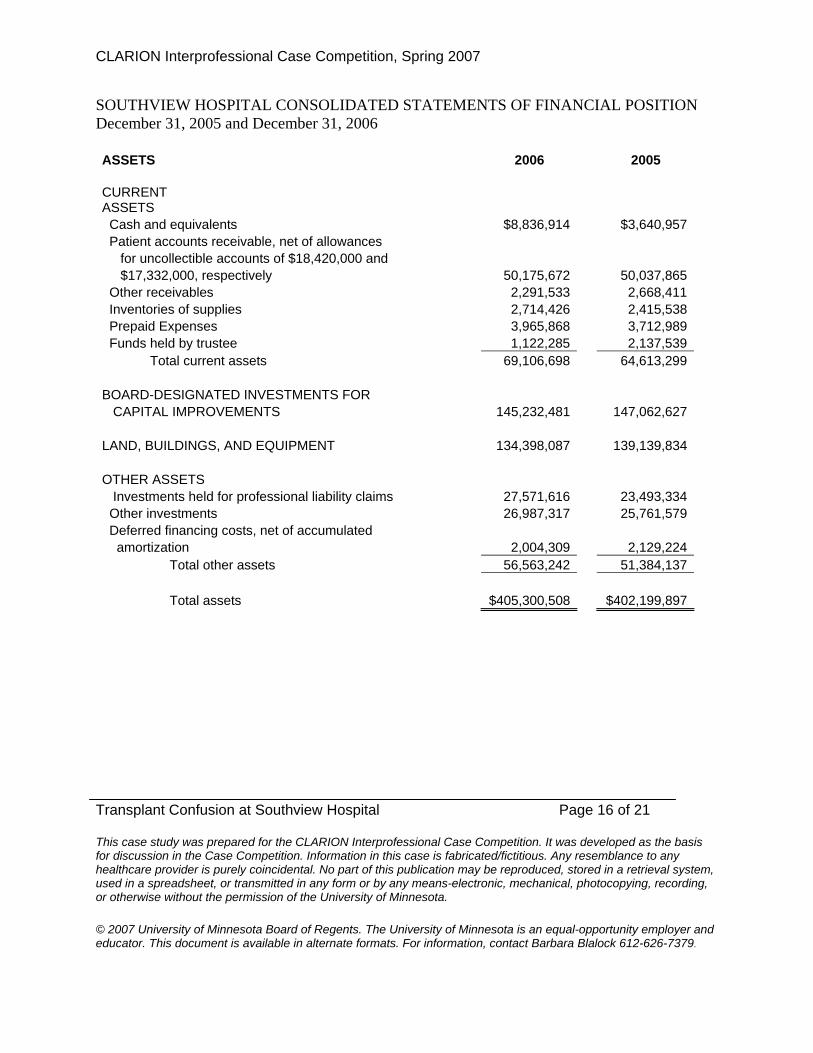
SOUTHVIEW HOSPITAL CONSOLIDATED STATEMENTS OF FINANCIAL POSITION December 31, 2005 and December 31, 2006 ASSETS 2006 2005 CURRENT ASSETS Cash and equivalents $8,836,914 $3,640,957 Patient accounts receivable, net of allowances for uncollectible accounts of $18,420,000 and $17,332,000, respectively 50,175,672 50,037,865 Other receivables 2,291,533 2,668,411 Inventories of supplies 2,714,426 2,415,538 Prepaid Expenses 3,965,868 3,712,989 Funds held by trustee 1,122,285 2,137,539 Total current assets 69,106,698 64,613,299 BOARD-DESIGNATED INVESTMENTS FOR CAPITAL IMPROVEMENTS 145,232,481 147,062,627 LAND, BUILDINGS, AND EQUIPMENT 134,398,087 139,139,834 OTHER ASSETS Investments held for professional liability claims 27,571,616 23,493,334 Other investments 26,987,317 25,761,579 Deferred financing costs, net of accumulated amortization 2,004,309 2,129,224 Total other assets 56,563,242 51,384,137 Total assets $405,300,508 $402,199,897

CLARION Interprofessional Case Competition, Spring 2007
Transplant Confusion at Southview Hospital Page 17 of 21 This case study was prepared for the CLARION Interprofessional Case Competition. It was developed as the basis for discussion in the Case Competition. Information in this case is fabricated/fictitious. Any resemblance to any healthcare provider is purely coincidental. No part of this publication may be reproduced, stored in a retrieval system, used in a spreadsheet, or transmitted in any form or by any means-electronic, mechanical, photocopying, recording, or otherwise without the permission of the University of Minnesota.
© 2007 University of Minnesota Board of Regents. The University of Minnesota is an equal-opportunity employer and educator. This document is available in alternate formats. For information, contact Barbara Blalock 612-626-7379.
LIABILITIES AND NET ASSETS CURRENT LIABILITIES Current maturities of long-term debt $3,862,238 $3,641,886 Borrowings on line of credit 2,000,000 Accounts payable 11,696,578 13,889,789 Estimated third-party payor settlements 7,199,771 10,591,479Accrued expenses: Estimated claims payable 520,191 1,150,772 Salaries and benefits 12,986,135 11,027,080 Vacation pay 8,321,616 7,560,003 Interest and other 1,504,379 1,515,879 Total current liabilities 46,090,908 51,376,888 OTHER LIABILITIES Accrued professional liability claims 4,427,490 4,088,861 Pension and benefit obligations 22,312,963 19,243,327 Total other liabilities 26,740,453 23,332,188 LONG-TERM DEBT, less current maturities 97,604,387 101,345,496 Total liabilities 170,435,748 176,054,572 COMMITMENTS AND CONTINGENCIES NET ASSETS 234,864,760 226,145,325 Total liabilities and net assets $405,300,508 $402,199,897

CLARION Interprofessional Case Competition, Spring 2007
Transplant Confusion at Southview Hospital Page 18 of 21 This case study was prepared for the CLARION Interprofessional Case Competition. It was developed as the basis for discussion in the Case Competition. Information in this case is fabricated/fictitious. Any resemblance to any healthcare provider is purely coincidental. No part of this publication may be reproduced, stored in a retrieval system, used in a spreadsheet, or transmitted in any form or by any means-electronic, mechanical, photocopying, recording, or otherwise without the permission of the University of Minnesota.
© 2007 University of Minnesota Board of Regents. The University of Minnesota is an equal-opportunity employer and educator. This document is available in alternate formats. For information, contact Barbara Blalock 612-626-7379.
SOUTHVIEW HOSPITAL CONSOLIDATED STATEMENTS OF ACTIVITIES Years ended December 31, 2005 and December 31, 2006 2006 2005 REVENUE Net patient service revenue $354,294,440 $318,508,773 Other operating revenue 16,870,052 14,137,826
Total Revenue $371,164,492 $332,646,599
EXPENSES Salaries 176,343,489 156,228,717 Supplies 58,782,392 54,889,509 Employee Benefits 37,466,291 32,868,930 Professional Fees 24,459,619 22,245,550 Depreciation and amortization 21,797,301 20,055,496 Provision for bad debts 8,368,923 9,870,023 Building and equipment rental 4,911,794 5,287,088 Maintenance and repairs 6,904,635 5,705,497 Patient service tax 4,916,584 5,234,225 Interest 6,102,318 6,369,142 Utilities 5,034,531 4,436,019 Insurance and other 7,192,612 5,523,785 362,280,489 328,713,981
INCOME FROM OPERATIONS
8,884,003 3,932,618 NONOPERATING GAINS 4,186,480 16,090,648 EXCESS OF REVENUES OVER EXPENSES 13,070,483 20,023,266 RESTRICTED CONTRIBUTIONS, primarily for 434,208 599,672 capital acquisitions NET CHANGE IN UNREALIZED GAIN ON INVESTMENTS (2,139,792) (14,949,455) ADDITIONAL MINIMUM BENEFIT OBLIGATION (2,645,464) INCREASE IN NET ASSETS 8,719,435 5,673,483
CLARION Interprofessional Case Competition, Spring 2007
Transplant Confusion at Southview Hospital Page 19 of 21 This case study was prepared for the CLARION Interprofessional Case Competition. It was developed as the basis for discussion in the Case Competition. Information in this case is fabricated/fictitious. Any resemblance to any healthcare provider is purely coincidental. No part of this publication may be reproduced, stored in a retrieval system, used in a spreadsheet, or transmitted in any form or by any means-electronic, mechanical, photocopying, recording, or otherwise without the permission of the University of Minnesota.
© 2007 University of Minnesota Board of Regents. The University of Minnesota is an equal-opportunity employer and educator. This document is available in alternate formats. For information, contact Barbara Blalock 612-626-7379.
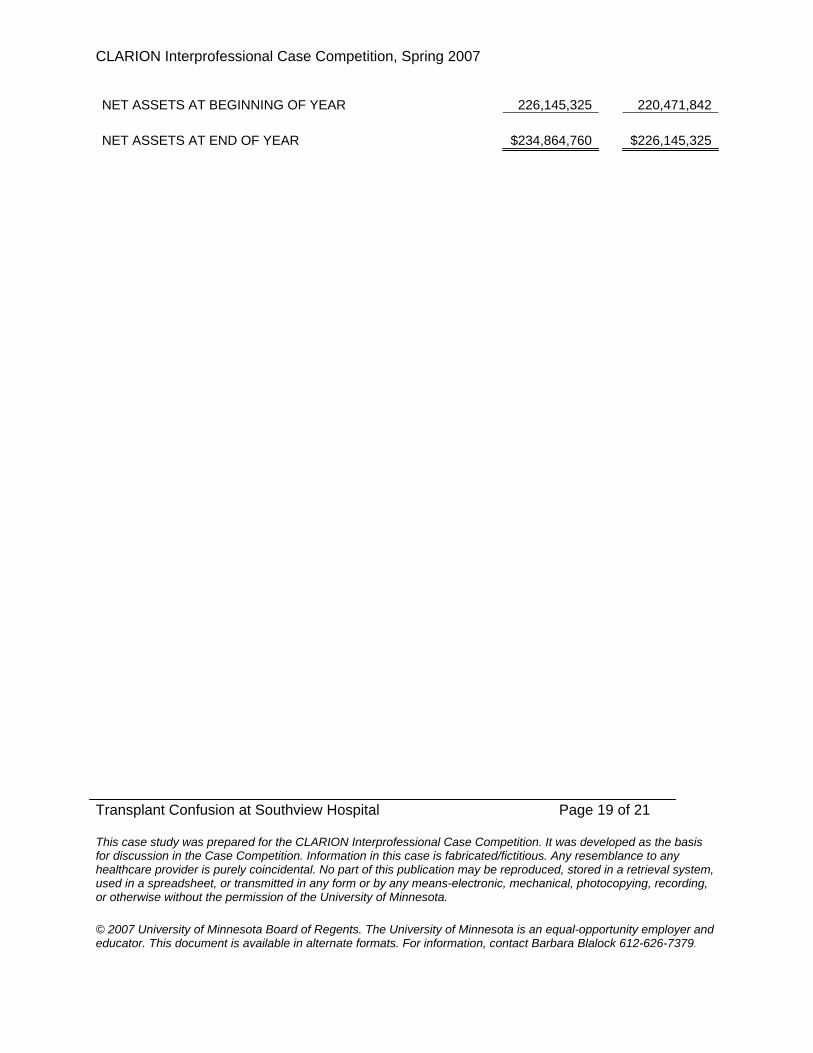
NET ASSETS AT BEGINNING OF YEAR 226,145,325 220,471,842 NET ASSETS AT END OF YEAR $234,864,760 $226,145,325

CLARION Interprofessional Case Competition, Spring 2007
Transplant Confusion at Southview Hospital Page 20 of 21 This case study was prepared for the CLARION Interprofessional Case Competition. It was developed as the basis for discussion in the Case Competition. Information in this case is fabricated/fictitious. Any resemblance to any healthcare provider is purely coincidental. No part of this publication may be reproduced, stored in a retrieval system, used in a spreadsheet, or transmitted in any form or by any means-electronic, mechanical, photocopying, recording, or otherwise without the permission of the University of Minnesota.
© 2007 University of Minnesota Board of Regents. The University of Minnesota is an equal-opportunity employer and educator. This document is available in alternate formats. For information, contact Barbara Blalock 612-626-7379.
SOUTHVIEW HOSPITAL CONSOLIDATED STATEMENTS OF CASH FLOWS Years ended December 31, 2005 and December 31, 2006 2006 2005 CASH FLOWS FROM OPERATING ACTIVITIES: Increase in net assets $8,719,435 $5,673,483 Adjustments to reconcile increase in net assets to net cash provided by operating activities: Depreciation and amortization 21,797,301 20,055,496 Restricted contributions (434,208) (599,672) Additional minimum benefit obligation 2,645,464 Net realized (gains) losses on sales of investments held for professional liability gains (94,809) 18,640 Net realized losses (gains) on sales of board-designated investments 7,357,142 (4,696,175) Net change in unrealized gain on investments 2,139,792 14,949,455 Increase in patient accounts receivable (8,506,730) (23,644,405) Provision for bad debts 8,368,923 9,870,023 Increase (decrease) in pension and benefit obligations 424,172 (243,919) (Decrease) increase in other assets and liabilities, net (4,464,025) 2,225,708 Net cash provided by operating activities 37,952,457 23,608,634 CASH FLOWS FROM INVESTING ACTIVITIES: Purchases of land, buildings, and equipment (15,410,188) (28,252,831) Purchases of investments held for professional liability claims (12,615,452) (20,717,620) Proceeds from sales of investments held for professional liability claims 9,552, 024 21,284,556 Purchases of board-designated investments (230,177,827) (226,044,752) Proceeds from sales of board-designated investments 221,687,488 224,255,835 Increase in other investments (1,667,242) (3,837,803)Decrease (increase) in funds held by trustee 1,015,254 (1,076,061) Net cash used in investing activities (27,615,943) (34,388,676) CASH FLOWS FROM FINANCING ACTIVITIES: Payments on long-term debt (3,574,765) (3,433,013) Proceeds from issuance of long-term debt 12,000,000 Borrowings on line of credit 3,000,000 15,000,000 Payments on line of credit (5,000,000) (13,000,000)

CLARION Interprofessional Case Competition, Spring 2007
Transplant Confusion at Southview Hospital Page 21 of 21 This case study was prepared for the CLARION Interprofessional Case Competition. It was developed as the basis for discussion in the Case Competition. Information in this case is fabricated/fictitious. Any resemblance to any healthcare provider is purely coincidental. No part of this publication may be reproduced, stored in a retrieval system, used in a spreadsheet, or transmitted in any form or by any means-electronic, mechanical, photocopying, recording, or otherwise without the permission of the University of Minnesota.
© 2007 University of Minnesota Board of Regents. The University of Minnesota is an equal-opportunity employer and educator. This document is available in alternate formats. For information, contact Barbara Blalock 612-626-7379.
Restricted contributions 434,208 599,672 Net cash (used in) provided by financing activities (5,140,557) 11,166,659 INCREASE IN CASH AND CASH EQUIVALENTS 5,195,957 386,617 CASH AND CASH EQUIVALENTS AT BEGINNING OF YEAR 3,640,957 3,254,340 CASH AND CASH EQUIVALENTS AT END OF YEAR $8,836,914 $3,640,957