ckd cheung june07
DESCRIPTION
hhjjTRANSCRIPT
Chronic Kidney Disease Chronic Kidney Disease (CKD) and Diabetes(CKD) and Diabetes
June 20, 2007June 20, 2007
Alfred K. Cheung, M.D.Alfred K. Cheung, M.D.
University of UtahUniversity of Utah

AcknowledgementAcknowledgement
National Kidney FoundationNational Kidney FoundationK/DOQIK/DOQI

Current Terminology
• Kidney, not Renal (or Reno)
• CKD, not CRF
• DKD (= diabetic nephropathy)
• AKI, not ARF
• Still ESRD (End Stage Renal Disease)
• Still RRT (Renal Replacement Therapy)
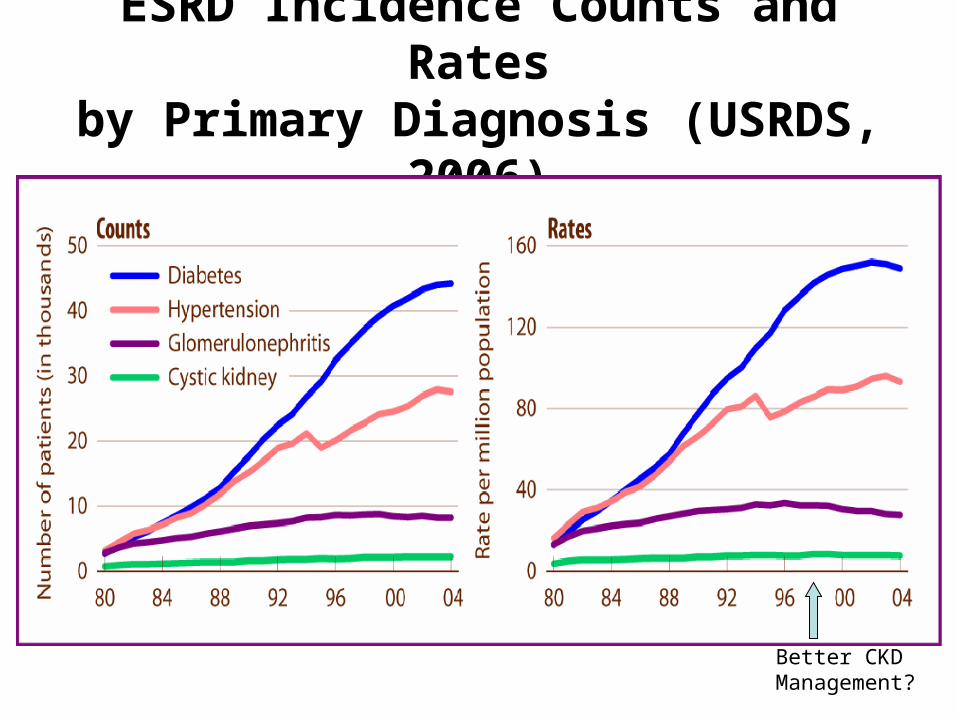
ESRD Incidence Counts and Ratesby Primary Diagnosis (USRDS, 2006)
Better CKD Management?
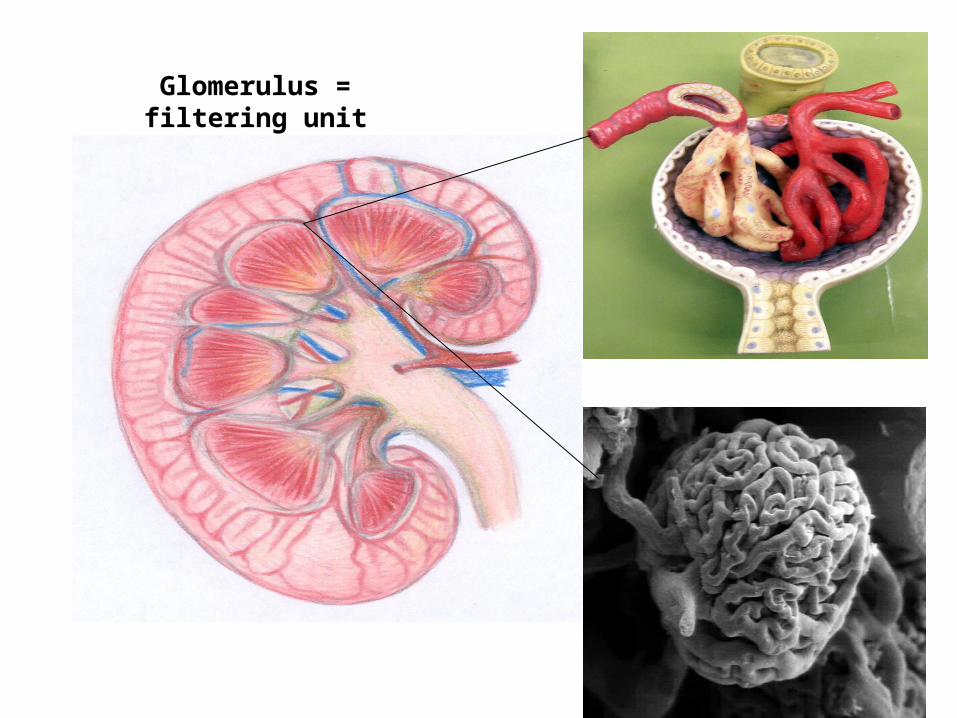
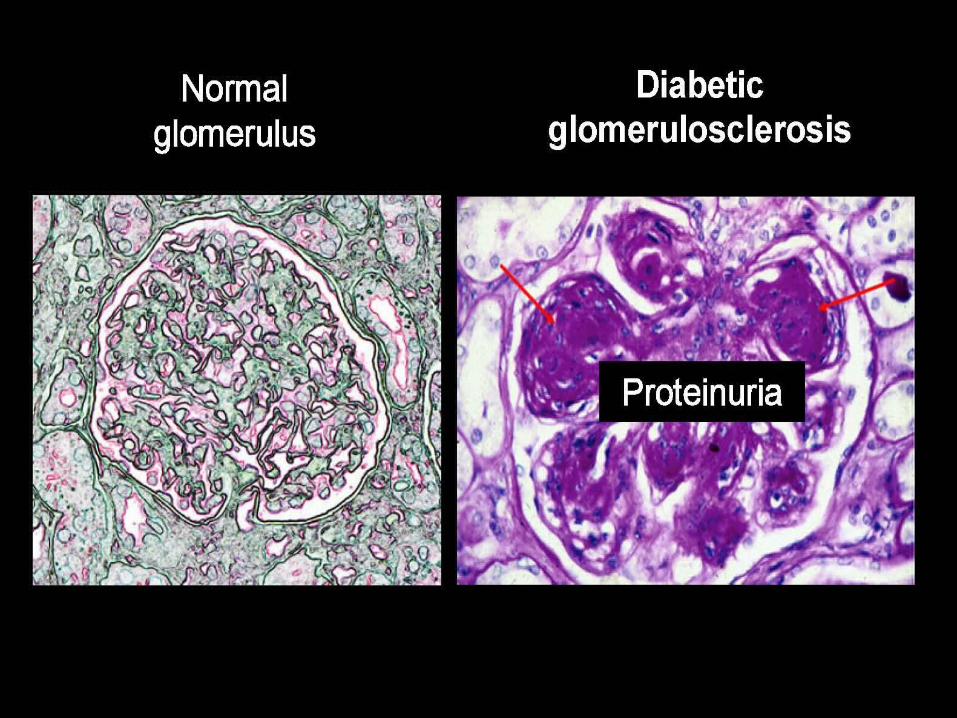
Glomerulus = filtering unit
Importance of Diabetic Kidney Disease
• Kidney disease as diabetic complication:– 30% of Type 1 Diabetes– 40% of Type 2 Diabetes
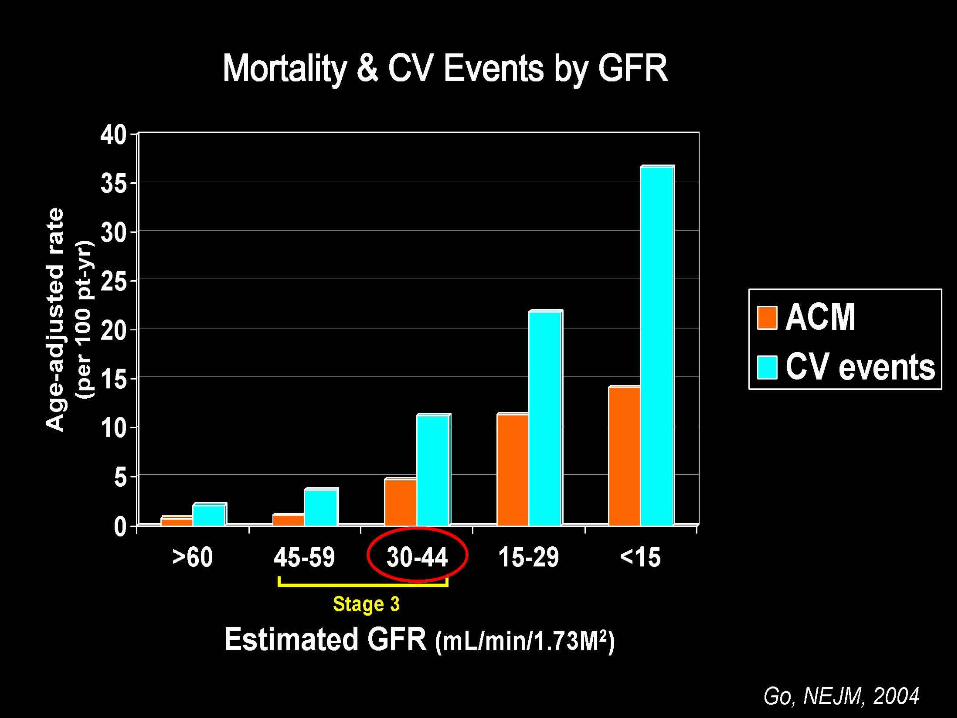
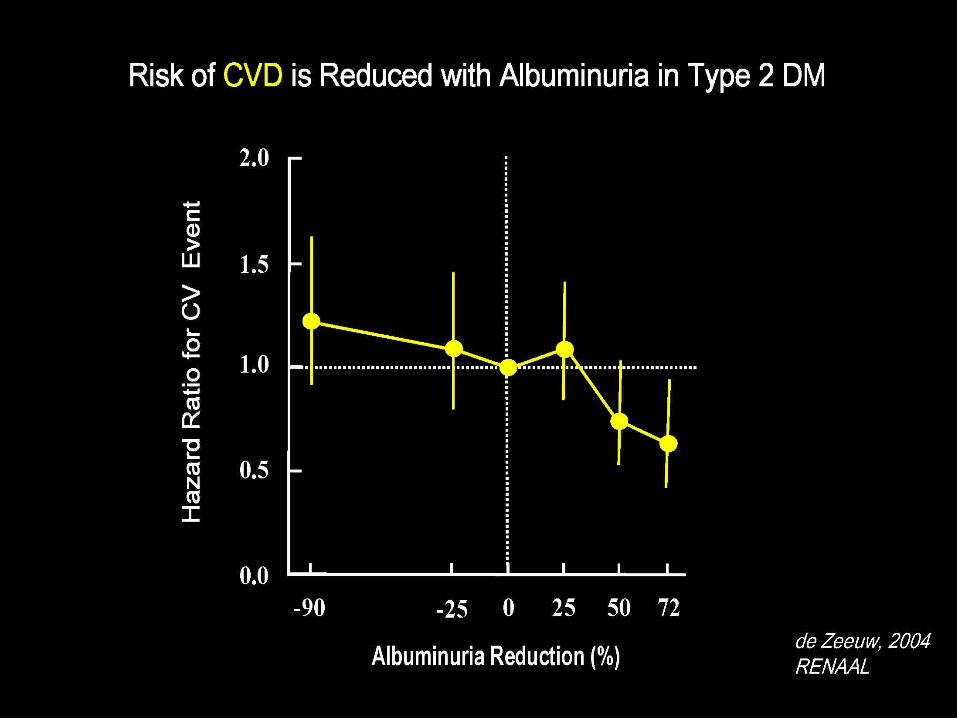
• CKD amplifies CVD risk of diabetes
Diabetic Kidney Disease Screening
• WHEN– Type 1: after 5 years, then annually– Type 2: at diagnosis, then annually
• HOW– Albumin-to-Creatinine ratio in random urine
• Microalbuminuria = 30-300 mg/g• Macroproteinuria
– Estimate GFR (eGFR) from serum creatinine using formulas
– Retinopathy: useful clue
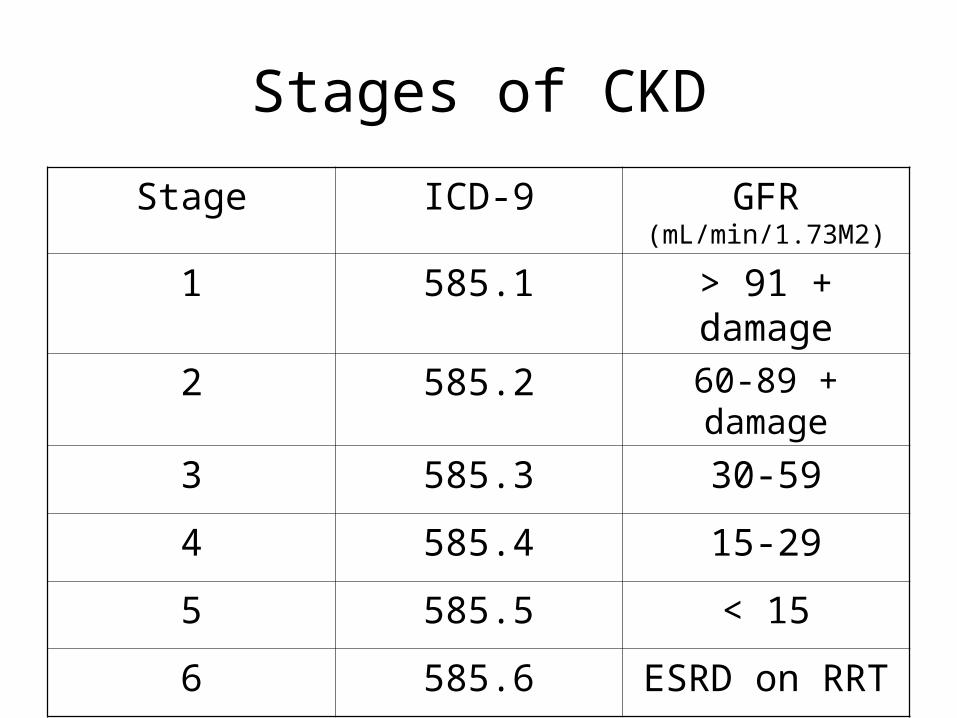
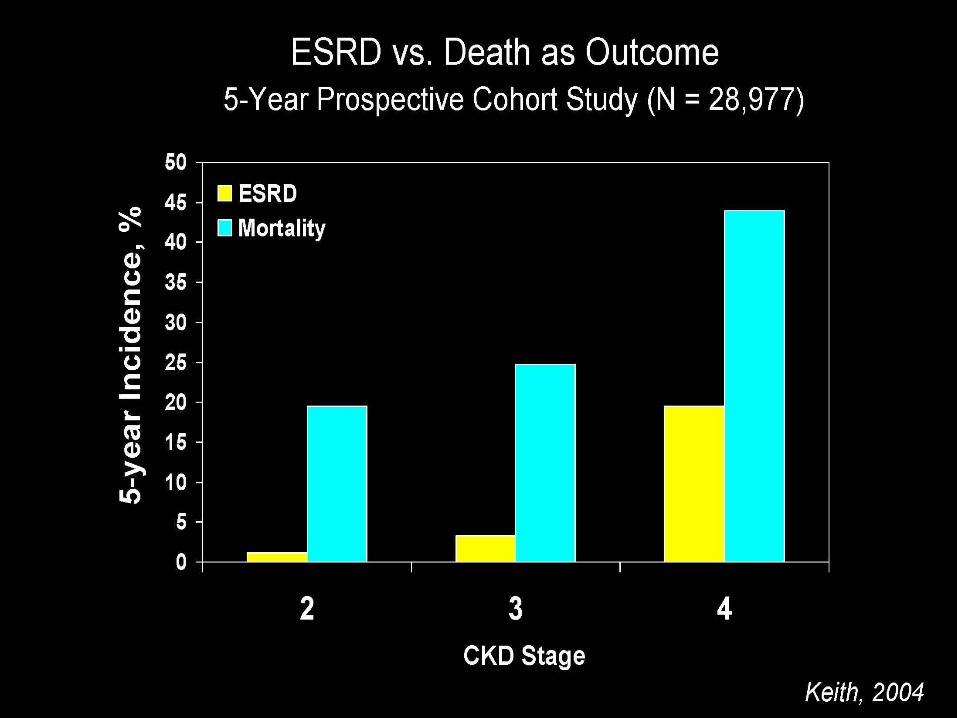
Stages of CKD
Stage ICD-9 GFR (mL/min/1.73M2)
1 585.1 > 91 + damage
2 585.2 60-89 + damage
3 585.3 30-59
4 585.4 15-29
5 585.5 < 15
6 585.6 ESRD on RRT

Action Plan in the Clinic
• Determine AKI vs. CKD?• Estimate GFR and rate of decline• Identify kidney disease requiring specific Rx• Slow progression of CKD• Review medications• Identify + treat systemic complications• Prepare for replacement therapy
Depending on CKD Stage
Formulas for Estimating GFR
• Cockcroft-Gault• MDRD (Modification of Diet in Renal Disease Study)
– GFR calculator (www.kidney.org)
• GFR depends on:– Serum creatinine– Age– Gender– Race
Interventions to Slow CKD Progression
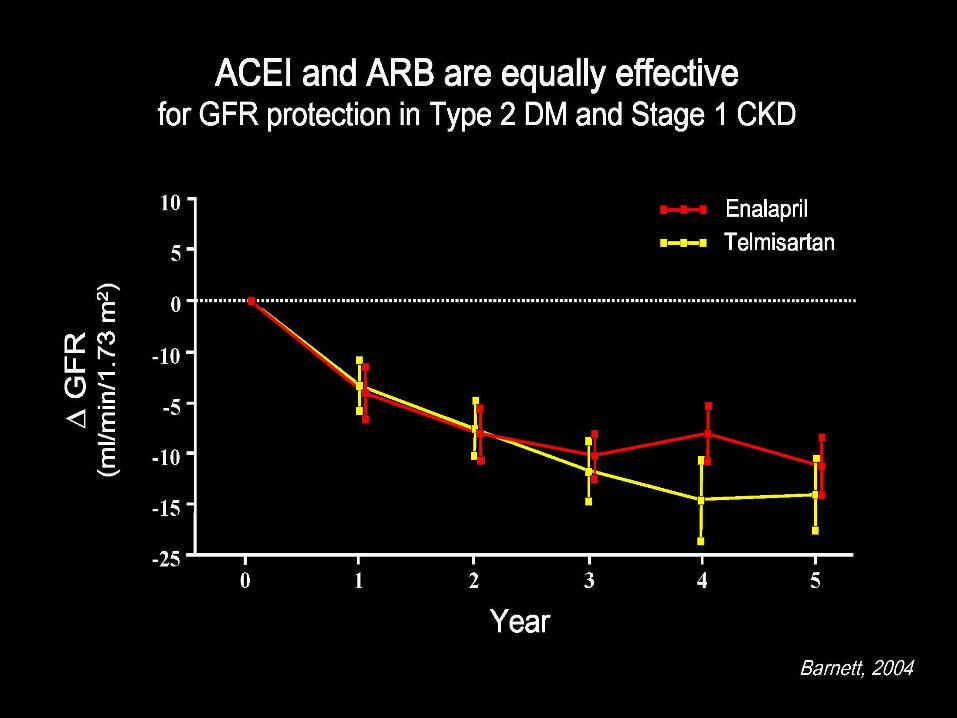
• Strong evidence– Blood pressure control– ACEI / ARB– Glucose control in DM
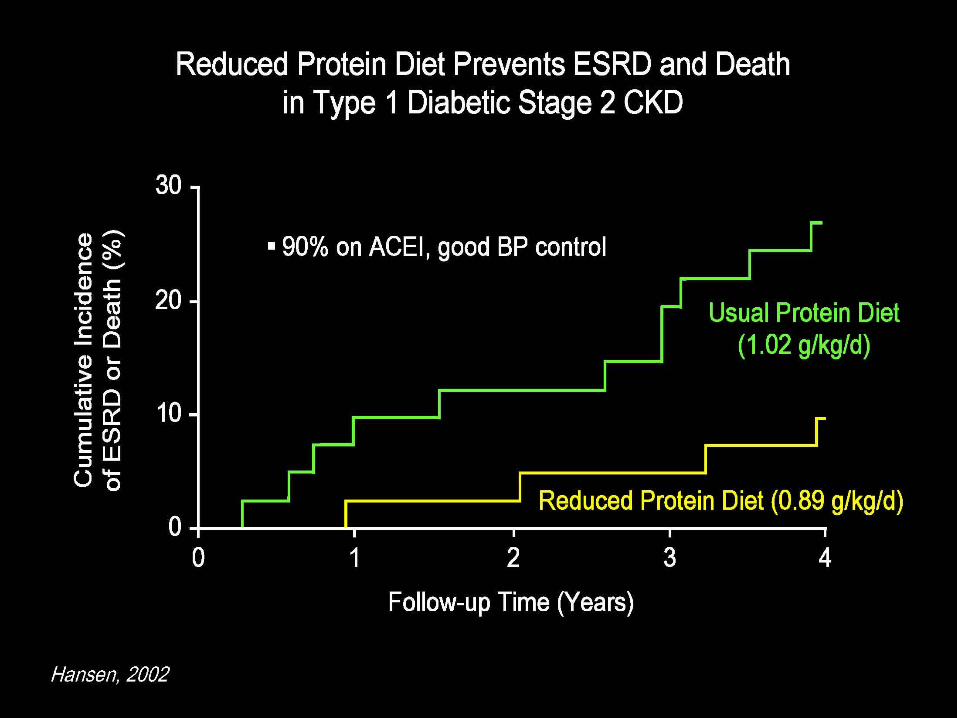
• Weaker evidence– Protein restriction– Lowering LDL cholesterol
Management of Albuminuria in Normotensive Diabetic
• Normotensive DM patients with macroalbuminuria should be treated with ACEI / ARB
• Treatment with an ACE inhibitor or an ARB should be considered in normotensive persons with diabetes and microalbuminuria

AKI Superimposed on CKD
• Dehydration
• BP too low
• Obstruction
• Contract dye
• Drugs– Nephrotoxic or allergic or hemodynamic– NSAID (including Cox-2 inhibitors)– ACEI / ARB
Systemic Complications of CKD
• Hypertension
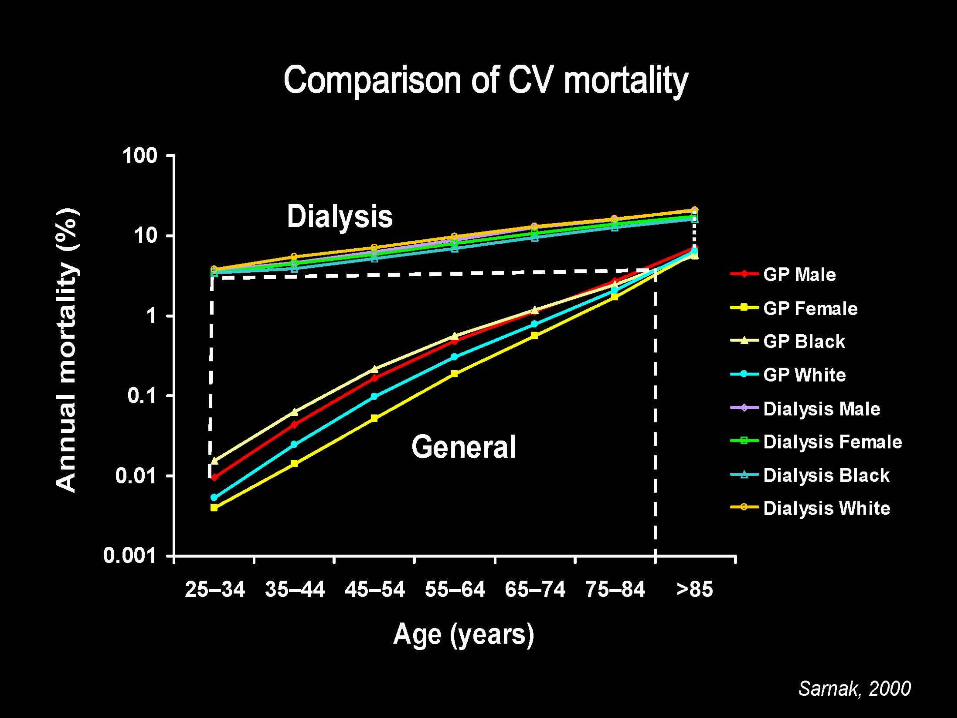
• Cardiovascular disease
• Anemia
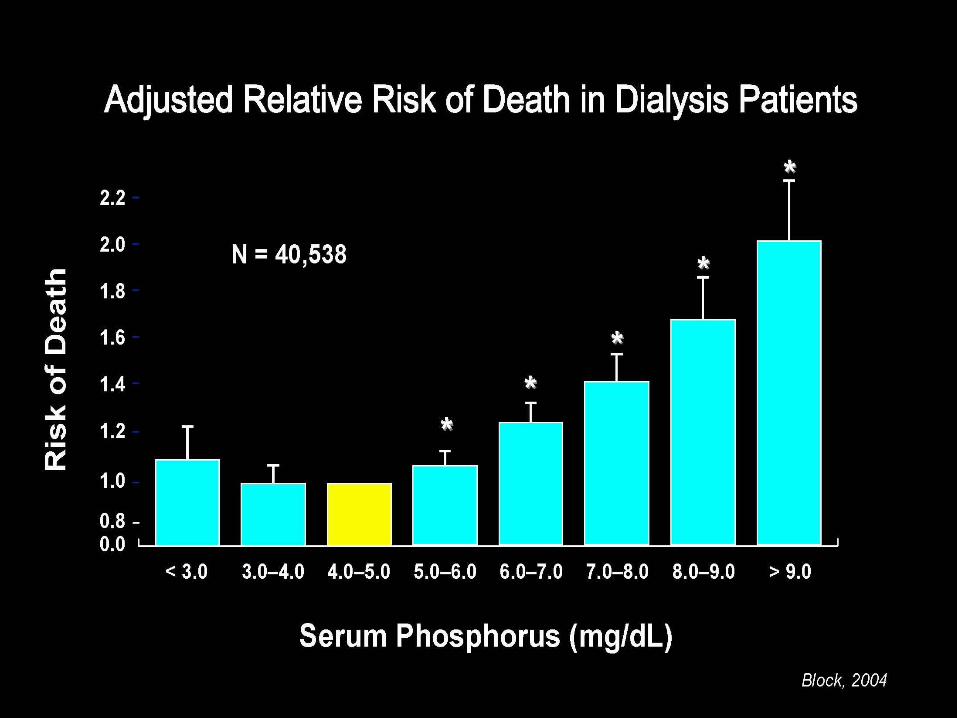
• Calcium-phosphorus-parathyroid
American Heart Association
• Patients with CKD– Should be considered as highest-risk group
for CVD– Should be treated as such
Sarnak, Circ, 2004
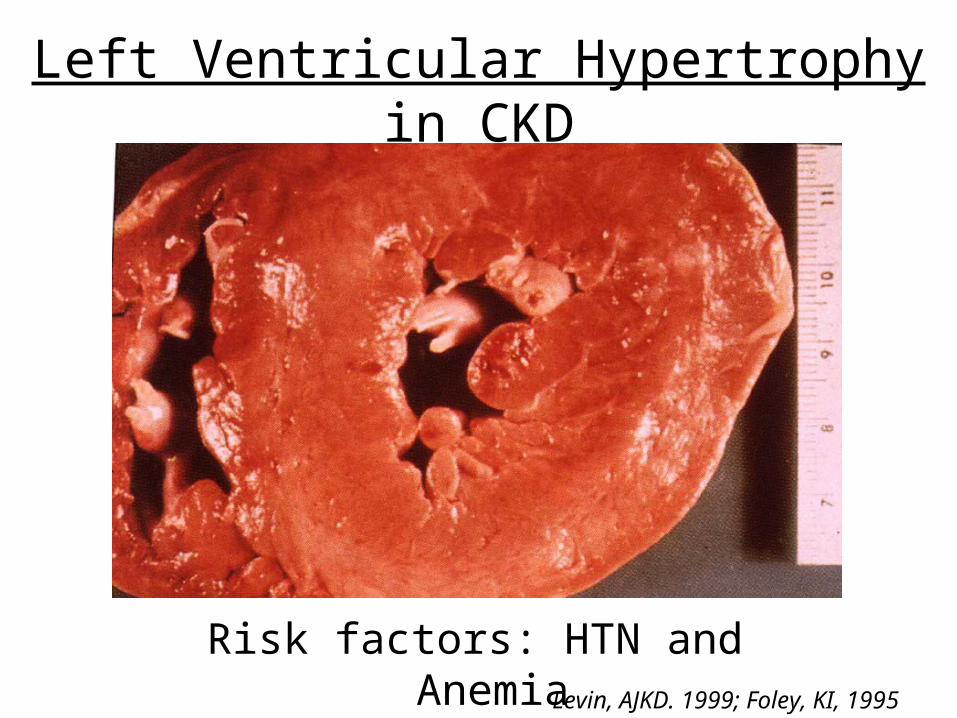
Left Ventricular Hypertrophy in CKD
Risk factors: HTN and AnemiaLevin, AJKD. 1999; Foley, KI, 1995
Erythropoietin Stimulating Agent in CKD
• Administration (SQ q 1-4 wk)– Epoietin-α (start 75-150 units/kg)– Darbepoetin (start 0.45 μg/kg)
• Target Hgb (11-12 g/dL)
• Adverse effects– Iron deficiency (may need IV iron)– Hypertension

What is Renal Diet?
• Low sodium
• Low potassium– What about DASH?
• Low phosphorus– Adding glucose and fat targets?
• Should be individualized
Symptoms of Uremia
• None or subtle
• Fatigue, lack of energy
• Anorexia (nausea/vomiting)
• Sleep disturbance
• Impaired cognitive function
• Impotence
When to Start Replacement Therapy
• Phophorus higher than hct• Pale and sallow• Needs a razor blade to scratch the itch• Vomiting day & night• Legs twitching• Hands flapping• Uremic smell you cannot stand
• Too late!!• Should start no later than mildly symptomatic• Usually GFR 7-8 mL/min

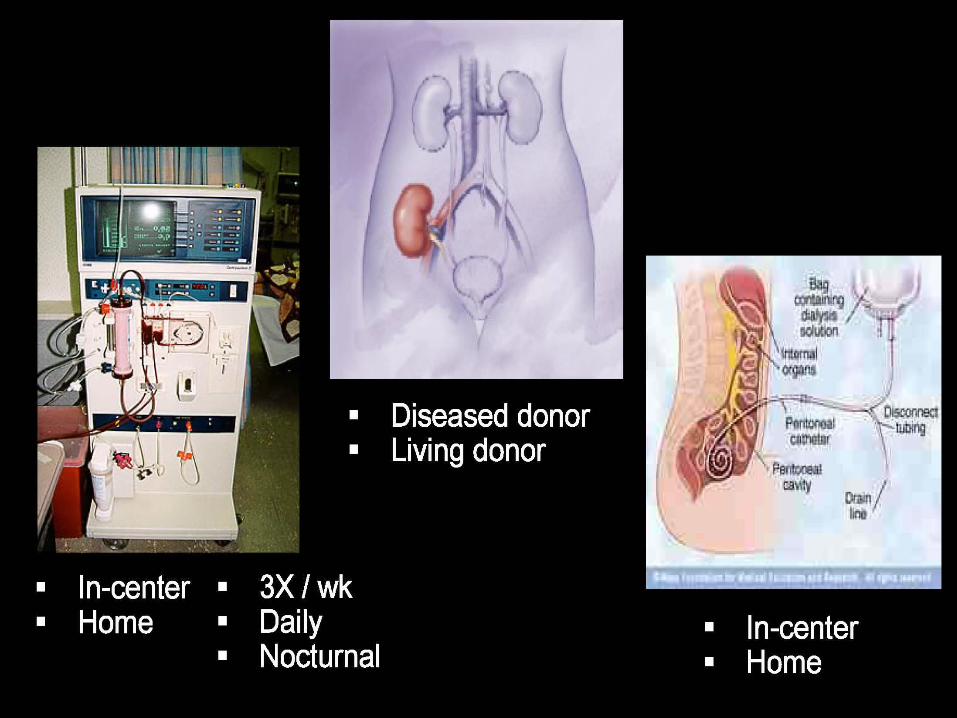
Preparation for RRT
• GFR 20 mL/min (depends on rate of decline)
• Early CKD education (including diet)
• Early nephrology referral for co-management (delineate responsibilities)
• Arm vein preservation