circulatory systemcourses.washington.edu/conj/handouts/01-outline 1.docx · web viewraynaud’s...
TRANSCRIPT
CIRCULATORY SYSTEMSpring, 2019
OBJECTIVES:
Review the path of blood through the chambers of the heart and through the systemic circulation and the pulmonary circulation.
Review the structure of the heart, with special emphasis on the thickness of the walls, the valves, and the major vessels connected to the heart. The lab will help a lot here.
Trace the sequence of events in the cardiac cycle, paying special attention to the diagrams. When do the valves open and close? How does this divide the cardiac cycle into its phases?
Discuss the first and second heart sounds. What causes them and when do they occur relative to systole and diastole? What is a split heart sound? What, in general are third and fourth heart sounds due to?
Describe laminar flow and turbulent flow. What causes murmurs, and, for each valve, when does the murmur for stenosis or insufficiency occur?
What are some conditions that damage valves? Describe in detail how the cardiac action potential coordinates the beating of the heart. What is its
normal sequence over the heart? What are the structures formed from specialized cardiac muscle fibers and what are their roles? Why are cardiac action potentials so long? How do the action potentials differ in the SA node and in regular ventricular muscle fibers? What is the pacemaker potential? What happens if the SA node no longer paces the heart?
What are the major arrhythmias and what affect do these have on typical patients? Discuss electrocardiograms to the extent we do in class and be able to identify those on the course web site. Discuss, to the extent we do in class, the pharmacology of anti-arrhythmic drugs and the use of electronic pacemakers.
About how large is the cardiac output? What is the most important factor regulating the heart rate? Through what mechanism do the neurotransmitters open the ion channels? What factors influence the stroke volume? Especially be sure to understand the Frank-Starling mechanism, and the role it plays in the tilt table experiment.
Discuss the structure of arterial walls. Then discuss how atherosclerosis develops. What circumstances lead to a myocardial infarction, stroke, and claudication? Describe the changes that occur with systolic heart failure and diastolic heart failure. How does the
Law of Laplace make matters worse? Discuss the resulting abnormal hypertrophy of the myocardium. How does the regulation become abnormal? Especially be sure to understand the sequence through which angiotensin II is formed? What is meant by congestive heart failure? What drugs are used to treat congestive heart failure.
Define pressure, flow, and resistance. How are these three variables interrelated? What is the role of the elastic arteries (besides conducting blood)? What is meant by the compliance of a
vessel? How does this change in the aorta with age? What factors determines the mean arterial pressure and the pulse pressure? Briefly compare pressures in the pulmonary circulation with the systemic circulation. What is the structure of arterioles? How are arterioles regulated? Discuss the structure veins, especially with respect to the arteries. What is the advantage of the high
compliance of the venous system? What are the sensors, integrator and effectors in the carotid baroreceptor reflex? When is this reflex
important? Note also the importance of blood volume in longer term regulation. Discuss systemic arterial hypertension. What is meant by essential hypertension and secondary
hypertension? What are the current values used to diagnose hypertension? (see webpage)
Discuss the structure of capillaries. What substances can freely diffuse across capillary walls? Discuss the role of blood proteins in determining fluid balance across capillary walls. What factors can cause edema?
Describe how the cardiovascular system adjusts for standing, and be able to explain typical results with the tilt table used in lab. In other words, why does the pulse pressure change, what does this indicate about the disturbance to the mean arterial pressure, and what is the response of the carotid baroreceptor reflex? Discuss the causes the hypotension brought up on the webpage.
With exercise, why does blood flow increase to the muscles? What factors tend to improve with training for endurance exercise? (more on this last point at the end of the respiratory system)
Be familiar with the disorders described in lecture and at the end of this handout.
A. Review: Organization of the Circulatory System

B. Review: Structure of Heart1. chambers: shape and wall thickness
2. vena cava (2), coronary sinus, pulmonary trunkpulmonary veins (4), aorta
3. valves
4. echocardiograms
aortic and pulmonary valves AV valves (mitral and tricuspid)

C. Valve Disorders and Heart Sounds 1. opening and closing of valves
cardiac cycle plot, as shown to right
normal heart sounds: S1, S2
times of systole and diastole
2. phases of cardiac cycle
systole:isovolumetric contraction
rapid ejection
reduced ejection
diastole:
isovolumetric relaxation
rapid passive filling
reduced passive filling
atrial contraction

3. abnormal sounds
split sounds
S3, S4
laminar and turbulent flow
murmurs
stenosis
insufficiency (regurgitation)
4. causes of stenosis and insufficiency
senile aortic stenosis
bicuspid aortic valve
rheumatic heart disease
infective endocarditis
5. artificial valves

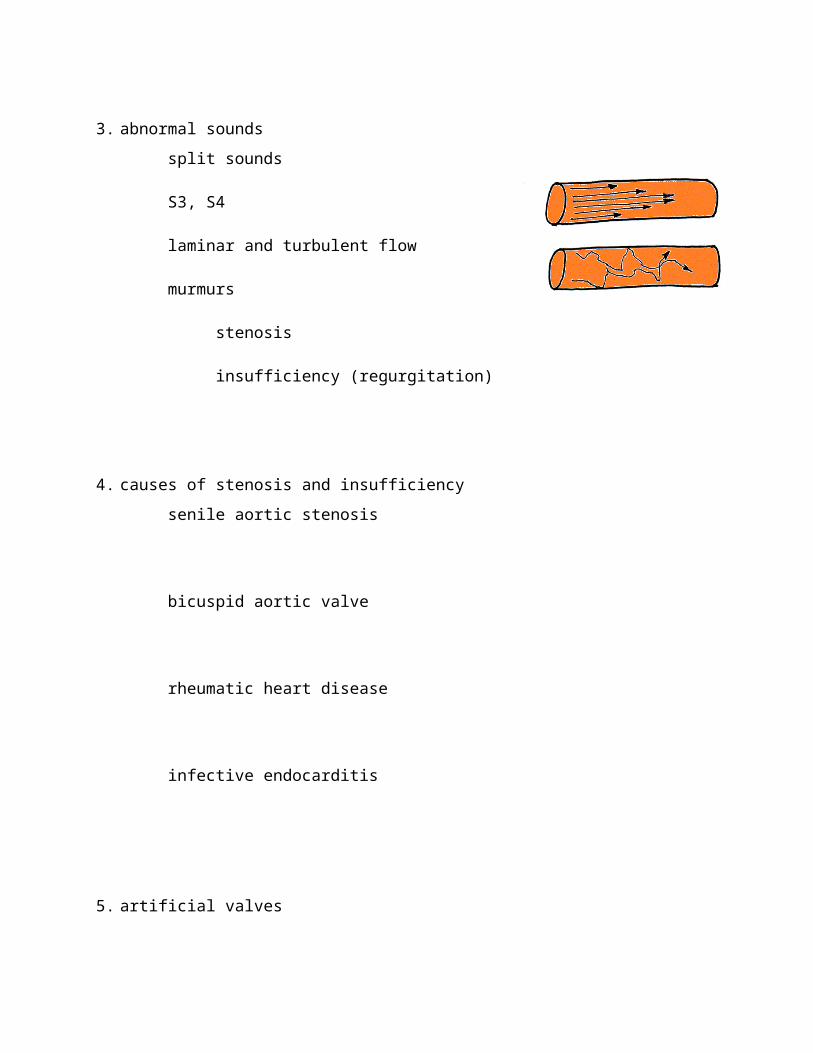
D. Arrhythmias1. normal path of action potential over heart
2. specialized cardiac fibers
SA node
AV node
AV bundle (bundle of His)
right and left bundle branches
Purkinje fibers
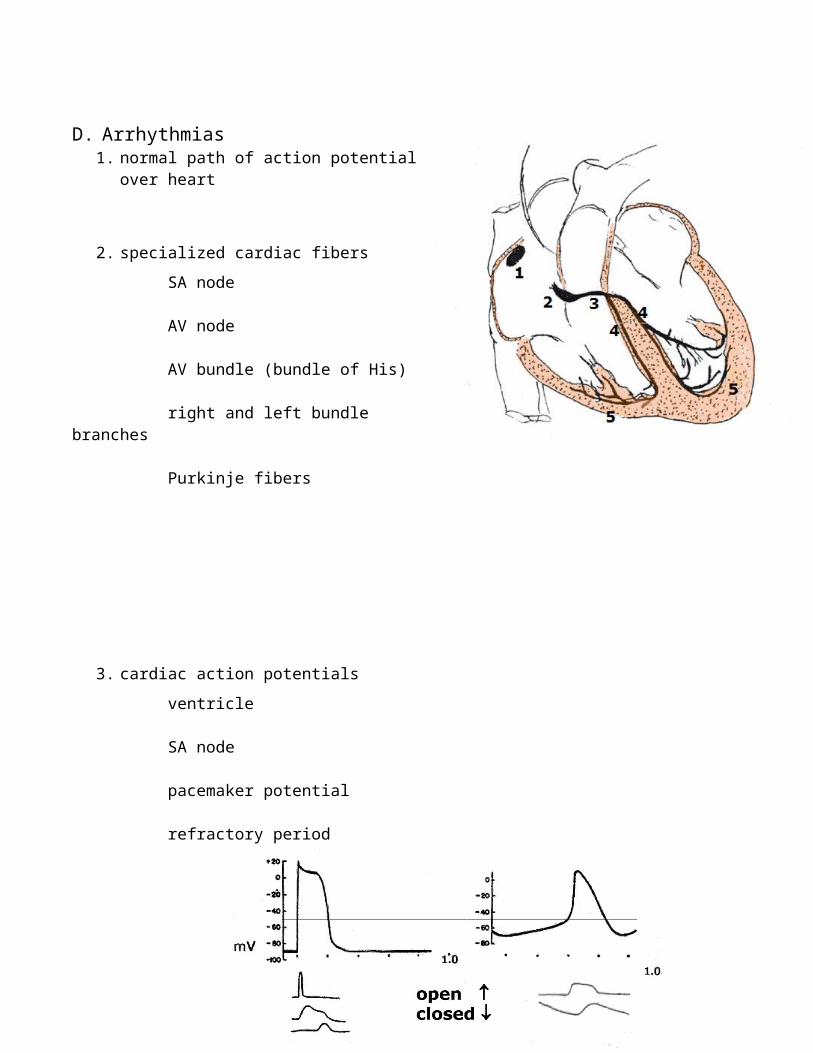
3. cardiac action potentials
ventricle
SA node
pacemaker potential
refractory period

4. electrocardiogram (see webpage and lab work)
basis of lead II waveform
5. arrhythmias (see Disorders and website for arrhythmias and abnormal electrocardiograms)
first degree AV block
second degree AV block
third degree AV block
premature atrial contraction
premature ventricular contraction
sinus bradycardia
supraventricular tachycardia
ventricular tachycardia
atrial fibrillation
ventricular fibrillation
lethal arrhythmias
pharmacology
E. Regulation of the Heart; Cardiac Output1. heart rate
parasympathetic innervation
sympathetic innervations and epinephrine
2. stroke volume
sympathetic innervation and epinephrine
increased blood in central veins; central venous pressure; end-diastolic volume Frank-Starling mechanism“venous return”
dilation or constriction of arterioles; aortic pressure afterload
F. Atherosclerosis 1. structure of arterial wall
2. sequence in atherosclerosis
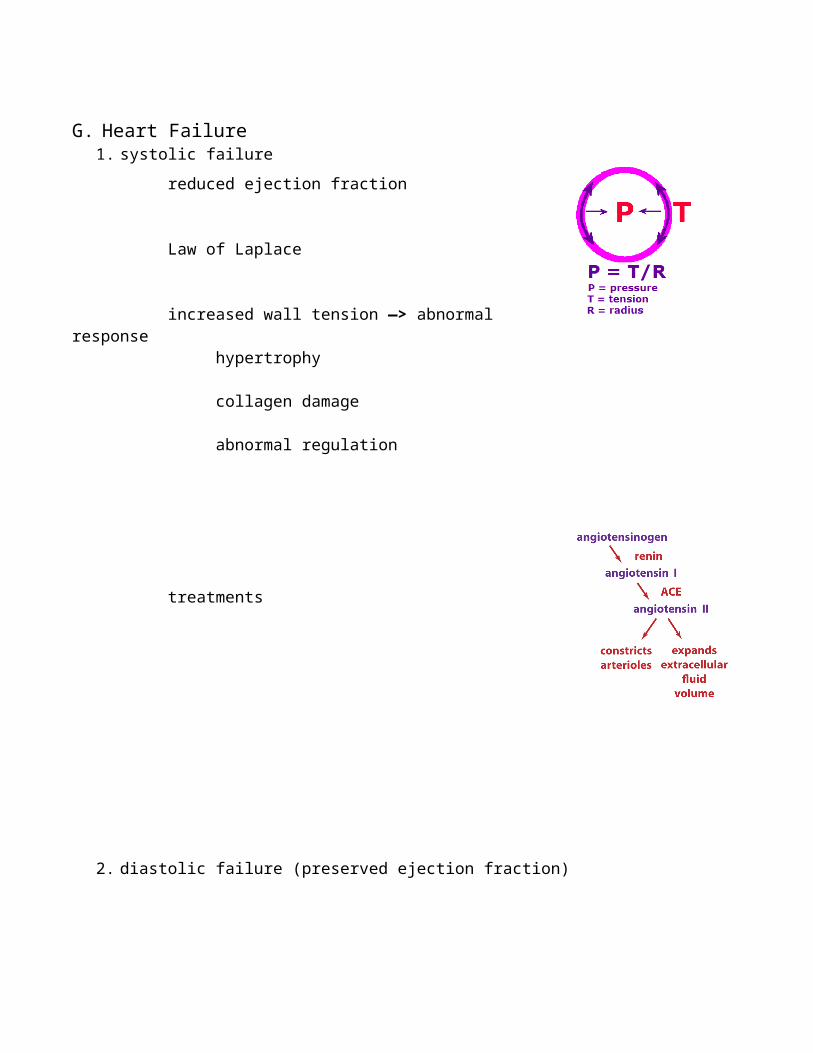
G. Heart Failure1. systolic failure
reduced ejection fraction
Law of Laplace
increased wall tension —> abnormal responsehypertrophy
collagen damage
abnormal regulation
treatments
2. diastolic failure (preserved ejection fraction)

H. Hypertension1. pressure, flow and resistance
2. role of elastic arteries
3. compliance; effect of age
4. structure of arterioles
5. control of arteriolesautonomic nerves
paracrines
hormones
local chemical factors
K+, CO2, osmolarity, etc
6. Veinsstructure
sympathetic innervation

7. mean arterial pressure
8. pulse pressure
9. normal regulation of mean arterial pressurecardiac output and total peripheral resistance
carotid baroreceptor reflex
hormones

10. hypertension
secondary
essential hypertension
11. treatments
I. SYNCOPE

J. Capillaries1. structure
2. permeability
3. fluid balance across capillary wall osmotic effect of blood proteins capillary pressure
4. edema
K. Standing, Walking

L. Exercise (Check out chart below, although this is mainly covered in respiration.)
College Students World Class
AthletesControl Bedrest Training
VO2max (l/min) 3.3 2.4 3.9 5.3Maximum Ventilation (l/min) 191 201 197 219Arterial O2 (ml O2/100 ml blood) 21.9 20.5 20.8 22.4Art.-Ven. O2 Diff. (ml O2/100 ml blood) 16.2 16.5 17.1 18.0Maximum Cardiac Output(l/min) 20.0 14.8 22.8 30.4Maximum Heart Rate (beats/min) 192 197 190 182Stroke Volume (ml) 104 74 120 167
DISORDERS AND TERMINOLOGYBe sure to see the webpages, because they also cover a number of the following disorders.
Valve ProblemsSplit Heart Sounds. Some types of difficulties alter the timing of the closing of the valves. For example, if the aortic and pulmonary valves do not close synchronously, the second heart sound is said to be split. Instead of the usual "lub--dup", the heart produces "lub--dadup". The first heart sound may also be split. Split heart sounds arise if the two ventricles are not activated simultaneously, if one ventricle is abnormally enlarged (hypertrophy), or if ejection of the blood from one ventricle is hampered. A small amount of splitting of the second sound often occurs normally during inspiration due to changes at that time in pulmonary blood vessels.
Murmurs. Normally, little or no noise arises due to the movement of the blood through the heart and blood vessels, because the blood flows in an orderly pattern termed laminar. However, if blood is forced rapidly through abnormal, narrow channels or openings, the flow changes into an erratic pattern termed turbulent. This type of flow is noisy, and sounds arising in this way in the heart are called murmurs.
One possible cause of a murmur is an insufficient valve that does not completely seal on closing, allowing the blood to regurgitate (squirt backward) through the valve. Inevitably, the backward flow is turbulent and produces a murmur. Atrioventricular insufficiency occurs while the ventricles contract, between the first and second heart sounds. Aortic or pulmonary insufficiency, on the other hand, occurs after the second heart sound, while the ventricles are relaxed.
Murmurs also result from valves that are not able to open fully, creating a stenosis (narrowed channel). For example, in senile aortic stenosis in the elderly damage to the endothelium and connective tissue results in fibrosis and calcification of the valve leaflets. In younger people, a congenital bicuspid aortic valve leads to similar stenosis.

Also, murmurs can also arise congenitally as the heart develops. For example, sometimes openings remain between the right and left ventricles, the right and left atria, or the pulmonary artery and aorta.
Rheumatic Heart Disease. Rheumatic heart disease is a complication that can develop following an acute infection by certain strains of streptococcus ("strep throat"). Some months after the acute infection clears up, severe scarring of valves in the heart can occur. Apparently, antibodies against the streptococcus bacteria cross-react with molecules in the heart. Mitral valve stenosis is the most common result. The inflamed cusps thicken, fuse at the edges and calcify. Today, this is mainly a problem in the developing world, although occasionally cases occur in this country.
Endocarditis. Bacterial endocarditis occurs when bacteria infect a valve in the heart. For example, an intravenous drug user may inject a skin bacterium, such as Staphlococcus aureus, along with the drug. Or similarly, bacteria may enter the blood via an intravenous catheter in a hospital. The valve cusps seem to be a natural place for the bacteria to colonize. The cusps become inflamed, with bacteria, platelets and fibrin accumulating. Congestive heart failure then develops if the valve is seriously damaged.
ArryhthmiasAny disturbance in the normal rhythm of the heartbeat is called an arryhthmia. (See webpage for ECGs.)
AV block. An AV block occurs when the action potential is delayed or stops at the AV node. There are three degrees of AV block. In first degree AV block, the PR interval is prolonged (>0.2 sec). This can occur in a normal, healthy individual, who typically is a well-trained individual with lots of “vagal tone”, or it may reflect underlying heart disease. In second degree AV block, some action potentials pass while others stop completely. For example, perhaps every second or every third action potential stops. Again this can occur normally or reflect underlying heart disease. In third degree AV block, every action potentials is blocked. But the heart nonetheless continue to pump blood because bundle branch or Purkinje fibers initiate a slow ventricular beat (about 30/min). Of course, it is out of synchrony with the atrial beat. The tendency of the AV node to block actually can be useful. If an atrial action potential arrives abnormally soon after another, the second action potential will be blocked, thereby allowing the ventricle time to fill before contracting. Thus, some substantial disturbances in atrial rhythm can be tolerated without seriously impairing ventricular pumping.
Premature Contractions. Premature contractions occur if an ectopic focus generates an occasional extra beat. There are two possibilities, premature atrial contractions (PAC, APB) and premature ventricular contractions (PVC, VPB). It is possible to determine whether the premature contraction is atrial or ventricular by listening with a stethoscope. If the extra action potential originates in an atrium, it will conduct to the SA node and reset its rhythm. On the other hand, if the ectopic focus is in a ventricle, the action potential will conduct over the ventricles, but not up into atria and SA node. Consequently, the ongoing atrial rhythm is not disturbed. Immediately following the ventricular premature contraction, however, one of the regular beats of the heart is skipped. This is because at that time the action potential from the atria falls in the refractory period of the action potential causing the premature contraction. Premature atrial contractions and premature ventricular contractions are not uncommon in young, healthy people. But premature contractions, of course, can also arise due to damage to heart muscle fibers.
Bundle Branch Block. If a bundle branch stops conducting action potentials, perhaps due to a myocardial infarction, the ventricles beat asynchronously. This is because the action potential conducts

first into one ventricle and then from there into the second ventricle. As a consequence, the QRS complex is misshapen and prolonged, and the heart sounds substantially split.
Sinus Bradycardia. Bradycardia is often defined as a heart rate less than 60/minute. Of course, this can occur in a healthy person who is in good condition. Excellent endurance athletes can have a heart rate in the thirties when first awakening in the morning. Pathological sinus bradycardia begins to create symptoms as the heart rate drops below about 50/minute. The patient is likely to be at least 50 and probably has cardiovascular disease of some sort. The most common case is sick sinus syndrome, in which degeneration in the SA node is responsible for the slow heart rate. Symptoms include syncope, dizziness, exercise intolerance and similar symptoms associated with inadequate blood flow to the brain and body. Various drugs can also cause bradycardia (such as digoxin, Ca++ channel blockers, and various others). Some disorders, such as hypothyroidism and anorexia, can also have this as a symptom.
Supraventricular Tachycardia. A number of circumstances can cause the AV node or the atrial tissue above it to generate action potentials very rapidly in a condition called supraventricular tachycardia. One cause is re-entry, which involves a pathway that carries the action potential in a circle back to previously activated muscles fibers. The result is many closely spaced action potentials. The rapid beating of the heart usually occurs in sudden bouts, not uncommonly in otherwise healthy, young individuals. This type is often called paroxymal supraventricular tachycardia since the onset to a fast heart rate is sudden. Excessive caffiene, smoking or alcohol increase the risk.
But in Wolff-Parkinson-White syndrome supraventricular tachycardia arises from an anatomically abnormal accessory pathway in which some cardiac muscle interconnects an atrium with the underlying ventricular tissue. This allows an action potential to re-enter the atrium. Ablation of the abnormal pathway with a catheter using radio frequency waves in the usual solution.
Ventricular Tachycardia. If an ectopic focus in a ventricle is serious, it can generate continuous, repetitive action potentials, causing the ventricles to beat rapidly. This is termed ventricular tachycardia. Because the ventricles are activated in an abnormal pattern, the heart sounds are usually substantially split. A heart beating out of control in this way is a dangerous condition because it can lapse into ventricular fibrillation.
Atrial Fibrillation. In fibrillation the action potential no longer spreads over the heart and then dies out, but conducts in multiple, never-ending patterns over the heart. Sometimes this is referred to as a "circus" movement, because the action potential follows circular pathways that return it to previously activated muscle fibers again and again. Fibrillating heart muscle tissue does not contract in a periodic, pumping mode, but in a chaotic, continuous fashion. When the fibrillation is in the atria, the ventricles continue to pump blood, because atrial action potentials arrive randomly at the AV node, travel through the AV node and cause ventricular contractions. The condition is disconcerting to hear with a stethoscope because the heart beats at nearly random intervals. Blood nonetheless may be pumped reasonably well, because the atria are not necessary for the filling of the ventricles, and the random ventricular contractions usually pump enough blood. Atrial fibrillation is most common in the elderly, where it has more effect on the pumping of the ventricles. This is because the ventricles are stiffer and thus rely more on atrial contraction for filling. But the biggest problem is the tendency of stagnant blood in the fibrillating atria to clot. Should the clot break free, it likely would precipitate a stroke.
Ventricular Fibrillation. Ventricular fibrillation is immediately life threatening, since no blood is pumped into the arteries. The ventricles are in a state of continuous, twitching contracture; they do not alternately fill and eject blood. The typical treatment in such an emergency is to massively shock the

heart, depolarizing all of the muscle fibers. Hopefully, this wipes the slate clean, allowing action potentials to arise and flow over the heart in the normal fashion.
Anti-Arrhythmic Drugs. Drugs often can be helpful in reducing the excitability of the heart in arrhythmias, although modifying the cardiac action potential carries with it the risk of serious adverse effects. Lidocaine is an example of Na+ channel blocker used for arrhythmias. (Lidocaine is also used as a local anesthetic. The drug works by reducing the number of functional Na+ channels by slowing their recovery from an inexcitable configuration. If more action potentials occur, more Na+ channels enter and linger in the inexcitable form.) Verapamil, by contrast, is an example of a drug that reduces arrhythmias by blocking Ca++ channels. Adenosine, which opens a K+ channel, is another drug used for paroxymal supraventricular tachycardia. (Adenosine is a physiological regulatory molecule and is blocked by caffiene.) Beta-adrenergic blockers are used when reducing sympathetic effects is helpful, such as some cases of paroxymal supraventricular tachycardia.
Heart FailureSystolic Heart Failure. As a heart begins failing, whether from a myocardial infarction or any other cause, changes appear both in the heart and in regulatory processes. Due to the damage, the ejection fraction decreases and the central venous pressure rises, producing congestive heart failure. The heart dilates as it struggles to eject blood, an effect accentuated by the Law of Laplace.
But because heart muscle is weak, it cannot respond to the stretch with an increased contraction. Subsequently, the stretch and abnormal load on the heart stimulates abnormal hypertrophy of the muscle fibers and connective tissue damage. (see webpage for more details). The weak contractions also lead to abnormal regulation, since mechanisms that stimulate the heart and support the arterial pressure tend to be continually activated. Notably, there is a sustained increase in sympathetic activity, plasma renin and plasma vasopressin.
In normal circumstances, these factors help the body accommodate for the low cardiac output. But with a chronic failing heart, they further increase the load on the weak heart.
Diastolic Heart Failure. In diastolic heart failure, the ejection fraction remains normal, but the compliance of the heart wall decreases. The heart does not relax normally and, in contrast to systolic heart failure, the end-diastolic volume decreases. It is difficult for the stroke volume to increase and the patients have a reduced exercise tolerance. Extracellular fluid volume expands here as it does in systolic heart failure.
Digoxin (optional). Digoxin, which is found in foxglove, binds to the Na+/K+ active transporter and blocks its transport. If digoxin (or other cardiac glycosides) are ingested in sufficient quantities, the widespread blocking of active transport of course is fatal. In smaller amounts, however, digoxin increases the force with which heart muscle contracts and often is used effectively as a drug to stimulate failing hearts.

The action of digoxin on the contraction of the heart is indirect. Following the partial blocking of active transport, the concentration of Na+ inside the heart muscle cells increases somewhat. This in turn decreases the movement of Ca++ out of the cell by the cotransporter that exchanges Ca++ for Na+. This is because the Na+ concentration gradient supplies the energy for this cotransporter. Recall the energetics of cotransport. The movement of one substance down its concentration gradient can serve as a source of energy for transferring the other substance across the membrane. As the action of digitalis reduces the Na+ gradient, less Ca++ is transferred out of the cell. The resulting increase in Ca++ inside the cell increases the heart's contraction.
AtherosclerosisThe most common factor leading to blockage of the coronary arteries is atherosclerosis, a leading cause of death in Western, developed countries. The initial causes of atherosclerosis are still not well-understood. Apparently, the process begins with damage to the endothelium lining the arterial walls. Atherosclerosis can then be viewed as a subsequent, nonadaptive response of the blood vessel to the damage. Increasingly, atherosclerosis is being viewed as a disorder of chronic inflammation.
As atherosclerosis develops, monocytes and platelets adhere to the site of damage, with the monocytes migrating through the endothelium and becoming macrophages. Low density lipoprotein, the type that supplies cholesterol to cells, also moves through the endothelium. The macrophages take up the lipoprotein, becoming foam cells. The lipoprotein is especially likely to be taken up if it has been oxidized by oxygen free radicals. At this point, the wall of the artery is at the fatty streak stage.
The macrophages, platelets and epithelial cells release growth factors that stimulate the growth of nearby smooth muscle cells and fibroblasts. Smooth muscle cells migrate from the media into the intima. Some of these deposit additional connective tissue, and as the abnormal region grows it becomes a fibrous plaque.
The central region tends to become necrotic, with the degenerating cells releasing cholesterol crystals. As the plaque grows, it slowly begins to occlude the artery. Surprisingly, about three-quarters of the cross sectional area of the coronary artery must be blocked before symptoms begin to appear. With time the plaques tend to become calcified.
The stability of different plagues can vary, depending apparently on the thickness of the fibrous cap overlying the main portion of the plaque. If the cap is thin and ruptures, molecules, such as the extracellular lipids, are exposed that strongly promote clotting. A myocardial infarction results when the clot breaks free and clogs the artery.
Atherosclerosis does not tend to occur uniformly in the arteries, but is much more likely at certain spots in the aorta and its major branches.
Risk Factors in Atherosclerosis. As anyone who reads the popular press is aware, there are many divergent, yet still authoritative, opinions about the causes of atherosclerosis. Definite, major risk factors include hypertension, cigarette smoking, obesity, and diabetes mellitus. Moreover, high levels of cholesterol in the blood correlate with a more rapid progression of atherosclerosis. Most cholesterol in the blood is found in the low density lipoprotein fraction, and it is this cholesterol that accumulates in atherosclerosis. By contrast, cholesterol is removed from tissues via high density lipoprotein, and increased levels of this lipoprotein correlate with a reduced incidence of atherosclerosis. Last quarter

you studied the HMG CoA reductase inhibitors (statins), which block the synthesis of cholesterol in the liver. These are some of the most potent and widely used of the cholesterol lowering drugs.
Ischemic Heart Disease. Lack of adequate flow of blood to the heart, typically due to atherosclerosis, is termed ischemic heart disease. One usual consequence of ischemic heart disease is angina pectoris. With exercise, emotional stress or other conditions placing demands on the heart, not enough blood flows to portions of the heart, and pain described as "burning" or "a tightness" is felt in the chest and radiating up the left arm. With rest, the pain subsides. Note that this is an example of referred pain.
Myocardial Infarction. An area of necrosis due to sudden blockage of flow in a coronary artery is termed a myocardial infarction or, more popularly, a "heart attack". Atherosclerosis again is the usual cause. The formation of a clot on the roughened inside surface of the arteries is involved in most cases.
Claudication. Many patients who have arteries in the legs narrowed by atherosclerosis have the symptoms of claudication. This condition is defined by pain occurring in the legs upon walking. The usual location of the pain is in the calves and it does not disappear with continued walking. Resting, on the other hand, does relieve the pain. Usually the condition limits the patient’s daily activities and quality of life. Only five percent undergo amputation within five years. Claudication is treated with exercise therapy, smoking cessation, antiplatelet agents, and control of hyperlipidemia, diabetes and hypertension.
HypertensionAbout 20% of the population have hypertension, the condition in which the arterial pressure is higher than the normal range. (See website for specific values.) Over 90% of these cases are classified as essential hypertension, an admittedly ambiguous term. It implies that the hypertension is not a secondary result of some other identifiable disease process, but instead originates in the mechanisms regulating arterial pressure. As with type II diabetes, many people with hypertension are unaware that they have a problem.
Elevated sympathetic effects are usually found in cases of essential hypertension that are classified as either borderline or mild. The result is typically an increased cardiac output, although for some reason not an increased total peripheral resistance. This pattern is most typical of a younger person. By contrast, in moderate to severe cases of essential hypertension, sympathetic effects and the cardiac output are not increased but the total peripheral resistance is. In general, as essential hypertension becomes more established and severe, the cardiac output falls and the total peripheral resistance rises. While these observations are fairly widely accepted, the origins and causes of essential hypertension remain controversial. The kidney is almost surely involved in the process.
Note that the carotid baroreceptor and related reflexes would not be expected to correct for the hypertension. These sensors respond vigorously to short-term changes, but adapt and cease responding when the change is prolonged.
Hypertension that is identified as secondary to another disease process is often related to kidney function. This is a reflection of the interrelationships of the regulation of the cardiovascular system and the kidneys.

Other DisordersSyncope. Syncope is defined as a sudden loss of consciousness and postural tone, followed by spontaneous recovery. (i.e. “fainting”) This occurs due to a sudden reduction in the flow of blood to the brain. In perhaps a third or more of the cases, the cause of such an episode remains unknown. Beyond this, there are various, quite different causes. Some that we have already discussed include cardiac ischemia or certain arrhythmias, stroke, and transient ischemia attack. Also, seizures can produce similar outward symptoms.
After the “unknown” category, the most common type of syncope is termed vasovagal syncope. This involves neural reflexes regulating the heart and tone in blood vessels. Examples include emotional fainting and various situational causes such as fainting on coughing or defecation. Also, healthy athletes sometimes collapse upon completion of exercise. The website discussed the response expected on the tilt-table in someone with vasovagal syncope.
Another common cause is postural hypotension (orthostatic hypotension). It can be due, for example, to depletion of extracellular fluid volume or autonomic dysfunction. The reason for autonomic dysfunction can be unknown or it can be due to variety of disorders, such as diabetes mellitus, kidney disorders, malnutrition, and exposure to various toxic substances. If the autonomic neuropathy is severe, there may be virtually no sympathetic activation with upright posture.
Aneurysms. Aneurysms are localized dilations of blood vessels. Aneurysms of the aorta are especially common in atherosclerosis. The most common site is the aorta between the renal arteries and the common iliac arteries. Hypertension often contributes to the dilation. The swelling is typically ovoid and parallel to the long axis of the vessel. The interior contains atherosclerotic lesions and typically a clot (thrombus). Also, the lesions usually are calcified, as are the atherosclerotic vessels distal to the aorta. With time, fibrous tissue tends to replace the normal structure of the wall.
Aneurysms of the cerebral arteries are less common, but important because they can lead to dangerous hemorrhaging in the brain. (This accounts for about 5-10% of all "strokes".) The most common are called berry aneurysms because the sac-like dilation resembles a berry attached to a twig. Almost all occur at branch points near the circle of Willis. Causes include congenital malformations, atherosclerosis and hypertension.
In dissecting aneurysms, blood enters the wall of the artery, creating a blood-filled space. Hypertension is usually involved. Surgical intervention is usually imperative.
Raynaud’s Disease. Raynaud’s disease is the spasm of arteries serving the fingers (and sometimes toes) in response to cold temperatures. The most typical patient is a woman between 20 and 40 and living in a cool climate, although it occurs in others. Upon exposure to cold air, the fingers first become white as blood flow is restricted by strong sympathetic vasoconstriction. The color then tends to change to blue as cyanosis occurs due to desaturation of hemoglobin in the small vessels in the skin. Finally, in a third phase the blood vessels dilate as a local response to poor blood flow, and the fingers become red. The patient tends to feel numbness, paresthesia, and pain, the latter especially as the blood flow resumes. Typically, the problems do not become more severe and the patient gets along by wearing mittens or gloves and in general by preventing the sequence from getting started by keeping the hands warm. But in some patients vasodilating drugs are used.
While most cases of Raynaud’s disease do not become severe, the symptoms occasionally can indicate some other, more serious disorder, such as rheumatoid arthritis. In these types of cases, the symptoms may not be bilateral symmetrical and may worsen with time.

Venous Thrombosis. Venous thrombosis (thrombophlebitis) refers to the abnormal formation of a clot in either a deep or superficial vein. A deep thrombosis usually forms in the legs, especially the calves. Numerous factors can be responsible, involving some combination of the following three factors: injury or irritation of the endothelium; excessive tendency of the blood to clot, as may occur in certain cancers; and sluggish flow of blood through the vessel, such as might occur in prolonged bed rest or heart disease. The greatest danger is a pulmonary embolism, which occurs if the clot breaks free and flows through the right heart into the pulmonary circulation. A small clot is usually medically insignificant. But a massive clot is often fatal.
However, even a small clot can cause a stroke if the patient has a patent foramen ovale. The foramen ovale allows blood to flow from the right atrium to the left atrium in the fetus. But the foramen ovale closes following birth, although it remains open or “patent” in surprising fraction of the population. Usually this does not cause symptoms. However, an otherwise insignificant venous clot may not be filtered out by the lungs, but rather passes through the foramen ovale, leading to a stroke .
Varicose Veins. Varicose veins, which are expanded veins, are quite common, especially in the superfical leg veins. Also common are hemorrhoids, which are essentially varicose veins in the anal canal and rectum. Dilation of the veins and failure of their valves go hand-in-hand, each reinforcing the other. Varicose veins also tend to lengthen, giving them a twisted appearance. Factors promoting varicose veins include heredity, a standing occupation, pregnancy, obesity, and increasing age.