chronic pain management in today’s workforce · 1 chronic pain management in today’s workforce...
TRANSCRIPT

1
Chronic Pain Management Chronic Pain Management in Today’s Workforcein Today’s Workforce
Face to Face Disability Management ConferenceMay 25, 2011
Toronto, Canada
Catriona Buist, Psy.D.Clinical Director
Progressive Rehabilitation AssociatesPortland, OR
ObjectivesObjectives
Explain factors that can complicate chronic Explain factors that can complicate chronic painpain
Learn how to identify red flags and prevent Learn how to identify red flags and prevent disability from chronic paindisability from chronic pain
Explore outcomes from evidence based Explore outcomes from evidence based txtx

2
Definition of PainDefinition of Pain
Pain:Pain: an unpleasant sensory and an unpleasant sensory and emotional emotional experience associated with experience associated with actual or potential tissue damage actual or potential tissue damage (International Association for the Study of Pain)(International Association for the Study of Pain)
Acute Pain < 3 monthsAcute Pain < 3 monthsChronic Pain > 3 monthsChronic Pain > 3 months
A Common ProblemA Common ProblemPrevalence of chronic pain in the general Prevalence of chronic pain in the general population has been estimated at about 30%, population has been estimated at about 30%, at least 50 MM Americansat least 50 MM Americans..
One in eight workers loses One in eight workers loses 5 hours per week5 hours per week of of productive time (excluding missed days) from painproductive time (excluding missed days) from pain–– Combining reduced productivity while at work Combining reduced productivity while at work
and lost work days equates to and lost work days equates to $61.2 billion$61.2 billion in in estimated lost productivity for the estimated lost productivity for the year 2001year 2001--2002. 2002.
Associated with major coAssociated with major co--morbid psychiatric morbid psychiatric disorders and emotional sufferingdisorders and emotional suffering
44
Gatchel, R. J., et al, The Biopsychosocial Approach to Chronic Pain:Scientific Advances and Future Directions. Psychological Bulletin, Vol 133, No 4, 581-624, 2007Stewart w et.al. Lost Productive time and costs due to common paStewart w et.al. Lost Productive time and costs due to common pain conditions in the US work force. in conditions in the US work force. JAMA 2003: 290(18)2443JAMA 2003: 290(18)2443

3
Opioids and Workers Comp OutcomesOpioids and Workers Comp OutcomesUsually not recommended, but widely prescribedUsually not recommended, but widely prescribed
“Those who received more than 450 mg MEA were, on “Those who received more than 450 mg MEA were, on average, average, disabled 69 days longerdisabled 69 days longer than those who received no than those who received no early opioids…” early opioids…” (Webster et al, (Webster et al, SpineSpine 2007)2007)
“For the small group of workers with compensable back “For the small group of workers with compensable back injuries who receive opioids longerinjuries who receive opioids longer--term only a minority term only a minority shows clinically important improvement in pain and function. shows clinically important improvement in pain and function. The amount of prescribed opioid received early after injury The amount of prescribed opioid received early after injury strongly predicts longstrongly predicts long--term use.”term use.” (Franklin et al, (Franklin et al, Clin J PainClin J Pain 2009)2009)
“Average claim costs of workers receiving seven or more “Average claim costs of workers receiving seven or more opioid prescriptions were three times more expensive than opioid prescriptions were three times more expensive than those of workers who receive zero or one opioid prescription, those of workers who receive zero or one opioid prescription, and and these workers were 2.7 times more likely to be off work these workers were 2.7 times more likely to be off work and had 4.7 times as many days off work.and had 4.7 times as many days off work.” ” (Swedlow et al (Swedlow et al CWCI CWCI Special ReportSpecial Report 2008)2008)55
Oregon had a Oregon had a 1,250% increase in methadone poisoning1,250% increase in methadone poisoningdeaths from 1999deaths from 1999--2004 (5 to 68 people)2004 (5 to 68 people)
www.usdoj.gov/ndic/pubs25/25930/index.htmwww.usdoj.gov/ndic/pubs25/25930/index.htm

4
Guidelines on OpioidsGuidelines on Opioids
““Given the uncertainty regarding the balance Given the uncertainty regarding the balance between benefit and risk when opioids are used in between benefit and risk when opioids are used in the management of chronic nonthe management of chronic non--malignant pain, malignant pain, and, in particular, in association with their use for and, in particular, in association with their use for chronic musculoskeletal pain, the use of opioids chronic musculoskeletal pain, the use of opioids during the subduring the sub--acute and chronic phases of an acute and chronic phases of an injury, especially in the absence of an objectively injury, especially in the absence of an objectively identifiable pain generator, cannot be identifiable pain generator, cannot be recommended.recommended.””
Genovese, Harris, Korevaar 2007
ACOEM Guidelines, 2nd ed.77
Nationwide spine fusion numbers & charges Nationwide spine fusion numbers & charges (source: HCUPnet, AHRQ)(source: HCUPnet, AHRQ)
No. of Spine fusions
0
50,000
100,000
150,000
200,000
250,000
300,000
350,000
400,000
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
(All spinal levels, all indications, all techniques)Deyo

5
Obstacles to Chronic Pain ManagementObstacles to Chronic Pain Management
Failure to diagnose the anatomic source of painFailure to diagnose the anatomic source of pain
Failure to search for and address psychosocial Failure to search for and address psychosocial risk factorsrisk factors
Competing philosophiesCompeting philosophies–– Interdisciplinary vs. InterventionalInterdisciplinary vs. Interventional
Lack of understanding and willingness of injured Lack of understanding and willingness of injured worker, attorney and/or treating provider to worker, attorney and/or treating provider to consider interdisciplinary treatmentconsider interdisciplinary treatment
Chronic Pain Defined by the Chronic Pain Defined by the Pain Management Task Force Pain Management Task Force (May 2010)(May 2010)
Office of The Army Surgeon GeneralOffice of The Army Surgeon General
““Chronic pain continues beyond the normal time Chronic pain continues beyond the normal time expected for healing and is associated with the expected for healing and is associated with the onset of onset of pathophysiologic changes in the central pathophysiologic changes in the central nervous system that may adversely affect an nervous system that may adversely affect an individual’s emotional and physical wellindividual’s emotional and physical well--being, being, cognition, level of function, and quality of life.cognition, level of function, and quality of life.Chronic pain serves no apparent useful purpose Chronic pain serves no apparent useful purpose for the individual and may be diagnostically and for the individual and may be diagnostically and therapeutically approached as a therapeutically approached as a chronic disease chronic disease process.”process.”

6
How Does Chronic Pain
Develop?
The Fear-Avoidance Cycle
www.lower-back-pain-toolkit.com
Central Sensitization
www.lower-back-pain-toolkit.com
7
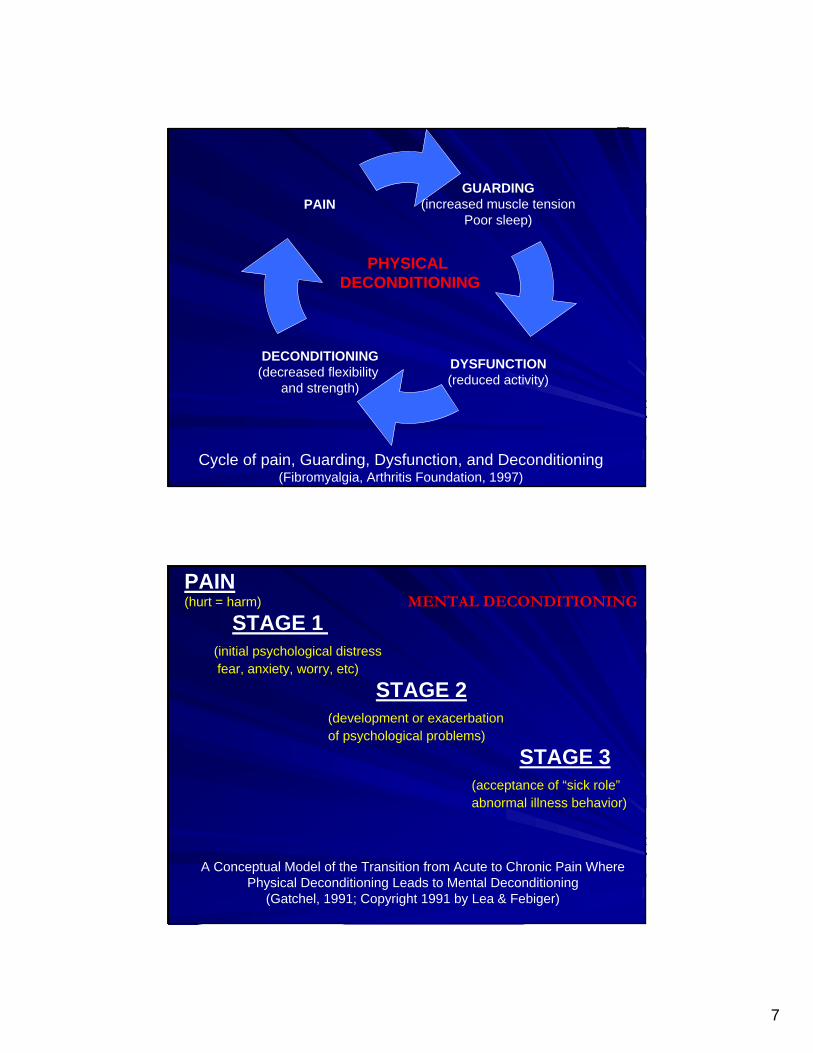
GUARDING(increased muscle tension
Poor sleep)
DYSFUNCTION(reduced activity)
PAIN
DECONDITIONING(decreased flexibility
and strength)
Cycle of pain, Guarding, Dysfunction, and Deconditioning(Fibromyalgia, Arthritis Foundation, 1997)
PHYSICAL DECONDITIONING
PAIN(hurt = harm)
STAGE 1(initial psychological distressfear, anxiety, worry, etc)
STAGE 2(development or exacerbation of psychological problems)
STAGE 3(acceptance of “sick role” abnormal illness behavior)
A Conceptual Model of the Transition from Acute to Chronic Pain Where Physical Deconditioning Leads to Mental Deconditioning
(Gatchel, 1991; Copyright 1991 by Lea & Febiger)
MENTAL DECONDITIONING

8
Recognizing Chronic PainRecognizing Chronic PainChronic pain behaviors can be seen in some Chronic pain behaviors can be seen in some claims as early as 2 weeks postclaims as early as 2 weeks post--injuryinjury
Most cases with duration of disability >3 mos for Most cases with duration of disability >3 mos for soft tissue injury show chronic pain behaviorssoft tissue injury show chronic pain behaviors
50% of patients with > 3 mos disability will not 50% of patients with > 3 mos disability will not RTW at 12 mos (industry data)RTW at 12 mos (industry data)
PainPain is the primary problem which continues to is the primary problem which continues to interfere with all aspects of the injured or disabled interfere with all aspects of the injured or disabled employee’s life, including RTW and ADL’semployee’s life, including RTW and ADL’s
1515
The The fear fear of pain of pain is more disabling is more disabling
than the pain than the pain itself.itself.
(Waddell)(Waddell)

9
September 2010 © 2010 Help Pain Medical Network, Inc. All rights reserved. 17
Pain Related ImpairmentPain Related Impairment
Do FearDo Fear--Avoidance Beliefs Play a Role on the Association Between Low BacAvoidance Beliefs Play a Role on the Association Between Low Back Pain and k Pain and Sickness Absence? A Prospective Cohort Study Among Female HealthSickness Absence? A Prospective Cohort Study Among Female Health Care WorkersCare WorkersJensen, JetteNygaard; Karpatschof, Benny; Labriola, Merete; AlbeJensen, JetteNygaard; Karpatschof, Benny; Labriola, Merete; Albertsen, Karen. Journal of Occupational and rtsen, Karen. Journal of Occupational and Environmental Medicine. 52(1):85Environmental Medicine. 52(1):85––90, January 2010.90, January 2010.
High “fear-avoidance” beliefs result in higher absence days from work3
Nu
mbe
r of
Sic
knes
s A
bse
nce
Day
s
17
28
24
53
0
10
20
30
40
50
60
Low-Moderate LBP High LBP
Low-Moderate Fear-Avoidance Beliefs
High Fear-AvoidanceBeliefs
Predictors of Persistent Disabling LBPPredictors of Persistent Disabling LBP
Maladaptive pain coping behaviorsMaladaptive pain coping behaviors–– Fear avoidanceFear avoidance (avoiding movement, activities)(avoiding movement, activities)–– CatastrophizingCatastrophizing (excessive negative thoughts)(excessive negative thoughts)Nonorganic signs Nonorganic signs (somatic focus)(somatic focus)
Functional impairmentFunctional impairmentLow general health statusLow general health statusPresence of psychiatric coPresence of psychiatric co--morbiditiesmorbidities
Chou, R., & Shekelle, P. Will This Patient Develop Persistent DisablingLow Back Pain? JAMA. April 7, 2010; Vol 303, No. 13, 1295-1302

10
Risk Factors that Predict Risk Factors that Predict LongLong--Term DisabilityTerm Disability
Maladaptive attitudes and beliefsMaladaptive attitudes and beliefsLack of social supportLack of social supportHeightened emotional reactivityHeightened emotional reactivityJob dissatisfactionJob dissatisfactionSubstance abuseSubstance abuseCompensation statusCompensation statusPrevalence of pain behaviors (Turk, 1997)Prevalence of pain behaviors (Turk, 1997)Psychiatric diagnosis (Gatchel & Epker, 1999)Psychiatric diagnosis (Gatchel & Epker, 1999)
Sick role solidifies; loss of hope for health recovery; Sick role solidifies; loss of hope for health recovery; generalized incompetent coping, frequently irreversible.generalized incompetent coping, frequently irreversible.
Learned Learned helplessnesshelplessness
Stage 5Stage 5
Lack of systematized documentation to support proof of Lack of systematized documentation to support proof of disability & the adversary system further foster attitudes of disability & the adversary system further foster attitudes of passivity, exaggerated illness behavior, & possibly passivity, exaggerated illness behavior, & possibly malingering.malingering.
Legal interventionLegal interventionStage 4Stage 4
Confusion, anger & hostility; increasing dependency & Confusion, anger & hostility; increasing dependency & idleness; economic preoccupation & difficulty; decline in idleness; economic preoccupation & difficulty; decline in competence for gainful employment.competence for gainful employment.
Stabilization of Stabilization of chronicitychronicity
Stage 3Stage 3
Following recovery from the injury, pt fails to return to normalFollowing recovery from the injury, pt fails to return to normalsocial roles & productivity. Repeated medical interventions social roles & productivity. Repeated medical interventions may be performed, leading to possible iatrogenic may be performed, leading to possible iatrogenic complications, chronicity, & learned pain behaviorcomplications, chronicity, & learned pain behavior
Medical interventionMedical interventionStage 2Stage 2
Relationships among the nature of the accident, the severity of Relationships among the nature of the accident, the severity of the injury, & the claimed inability to work are often weak.the injury, & the claimed inability to work are often weak.
The accidentThe accidentStage 1Stage 1
Demanding work, job dissatisfaction, situational stress, poor Demanding work, job dissatisfaction, situational stress, poor general coping skills, social model for disabilitygeneral coping skills, social model for disability
Crisis buildCrisis build--upupPremorbid Premorbid StageStage
Brena SF, Chapman, SL. Pain and litigation. In Wall PD, Melzack R, eds. Textbook of Pain. Edinburgh: Churchill Livingstone; 1989
Stages in the Development of Disability
11
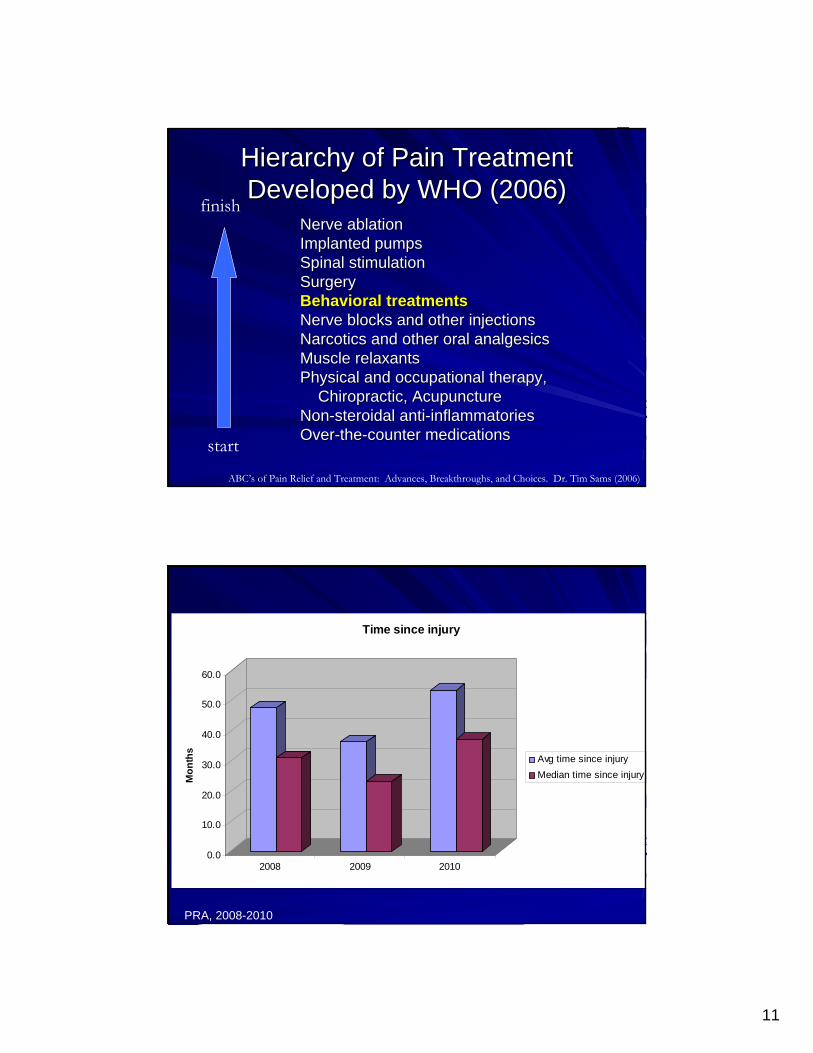
Hierarchy of Pain Treatment Hierarchy of Pain Treatment Developed by WHO (2006)Developed by WHO (2006)
Nerve ablation Nerve ablation Implanted pumpsImplanted pumpsSpinal stimulationSpinal stimulationSurgerySurgeryBehavioral treatmentsBehavioral treatmentsNerve blocks and other injectionsNerve blocks and other injectionsNarcotics and other oral analgesicsNarcotics and other oral analgesicsMuscle relaxantsMuscle relaxantsPhysical and occupational therapy, Physical and occupational therapy,
Chiropractic, AcupunctureChiropractic, AcupunctureNonNon--steroidal antisteroidal anti--inflammatoriesinflammatoriesOverOver--thethe--counter medicationscounter medicationsstart
ABC’s of Pain Relief and Treatment: Advances, Breakthroughs, and Choices. Dr. Tim Sams (2006)
finish
0.0
10.0
20.0
30.0
40.0
50.0
60.0
Mon
ths
2008 2009 2010
Time since injury
Avg time since injuryMedian time since injury
PRA, 2008-2010

12
Tackling Musculoskeletal Problemsa guide for clinic and workplace identifying obstacles using the psychosocial flags frameworkKendall, Burton, Main, & Watson: TSO Books, 2009 www.tsoshop.co.uk/flags
Flags are about identifying obstacles to being active and working
The important thing is to figure out how these can be overcome or bypassed
Collaborate and coordinate a plan of care for person, workplace, and healtcare
PERSON
WORKPLACE
CONTEXT
www.tsoshop.co.uk/flags
Initial (0-2 weeks) Early (2-12 weeks) Persistent (>12 weeks)

13
ReturnReturnto to
FunctionFunction
Multidisciplinary Functional Assessment
Rehabilitation Team• Physical Therapy
• Occupational Therapy
• Vocational Services
Psychological Assessment
Medical Management of Pain
• Full Musculoskeletal and Biomechanical Assessment
• Nursing
• CBT
• Relaxation Tools
• Biofeedback
• Self Hypnosis
Minimally InvasiveInterventionalPain Management
PRA Programs PRA Programs and Servicesand Services
Provide quick access for assessment and Provide quick access for assessment and txtx of LBPof LBP
Provide activityProvide activity--based coordinated interdisciplinary care based coordinated interdisciplinary care with an emphasis on return to function and meaningful with an emphasis on return to function and meaningful activityactivity
Early identification of obstacles to recovery and Early identification of obstacles to recovery and function function
Supplement rehabilitation plan with evidenceSupplement rehabilitation plan with evidence--based based psychotherapy as neededpsychotherapy as needed
Low Back Pain Program Objectives

14
Clinical Effectiveness & CostClinical Effectiveness & Cost--Effectiveness of Treatment for Effectiveness of Treatment for Patients with Chronic PainPatients with Chronic Pain ((Turk, D Turk, D Clinical Journal of PainClinical Journal of Pain, 2002;18:355, 2002;18:355--365365)
Investigated the clinical and costInvestigated the clinical and cost--effectiveness of effectiveness of various treatment (pharmacological, conservative various treatment (pharmacological, conservative care, surgery, spinal cord stimulation, implantable care, surgery, spinal cord stimulation, implantable drug delivery systems and pain rehabilitation drug delivery systems and pain rehabilitation programs) for patients with chronic pain. programs) for patients with chronic pain.
–– Interdisciplinary pain management programs yield Interdisciplinary pain management programs yield significantly better outcomes than other pain significantly better outcomes than other pain treatment approaches for: treatment approaches for:
return to work, functional activities, closure of return to work, functional activities, closure of disability claims, health care utilization, with disability claims, health care utilization, with substantially fewer iatrogenic consequences substantially fewer iatrogenic consequences and adverse events.and adverse events.
EvidenceEvidence--Based Clinical Practice Guidelines Based Clinical Practice Guidelines from the APS for Low Back Painfrom the APS for Low Back Pain
(Chou, R. & Huffman, L, 2010(Chou, R. & Huffman, L, 2010--2011)2011)
For subacute low back pain, For subacute low back pain, interdisciplinary rehabilitationinterdisciplinary rehabilitation(particularly with a work site visit) was associated with (particularly with a work site visit) was associated with quicker return to work, reduced sick leave, and quicker return to work, reduced sick leave, and moderately improved disability relative to usual care moderately improved disability relative to usual care
(two lower(two lower--quality trials) (level of evidence: fair). quality trials) (level of evidence: fair).
For chronic low back pain, For chronic low back pain, intensive interdisciplinary intensive interdisciplinary rehabilitation with functional restorationrehabilitation with functional restoration is moderately is moderately more effective than usual care or nonmore effective than usual care or non--interdisciplinary interdisciplinary rehabilitation for reducing pain and improving function, rehabilitation for reducing pain and improving function, though effects on workthough effects on work--related outcomes are related outcomes are inconsistent (four trials, two higherinconsistent (four trials, two higher--quality) (level of quality) (level of evidence good). evidence good).
Less intensive (<100 hours) interdisciplinary rehabilitation Less intensive (<100 hours) interdisciplinary rehabilitation was not more effective than usual care or nonwas not more effective than usual care or non--interdisciplinary rehabilitation interdisciplinary rehabilitation
(five trials) (level of evidence: good).(five trials) (level of evidence: good).

15
Designed to help a person become part of the treatment Designed to help a person become part of the treatment team and take an active role in regaining control of his or team and take an active role in regaining control of his or her life in spite of the pain.her life in spite of the pain.
Multiple disciplines working together on a team within one facility working toward the same shared treatment goals with the patient
The programs are focused on the total person and not just The programs are focused on the total person and not just the pain.the pain.
Focus on functional restoration and behavior modificationFocus on functional restoration and behavior modification
1515--20 days (620 days (6--8 hours/day)8 hours/day)Pain Management Programs
by the American Chronic Pain Association
What is an Interdisciplinary Pain Program?
Goals of Interdisciplinary Pain ProgramGoals of Interdisciplinary Pain ProgramINCREASE FUNCTIONINCREASE FUNCTION and activity leveland activity levelReduce painReduce painSimplify medication / reduce opioidsSimplify medication / reduce opioidsGraded physical exerciseGraded physical exerciseReduce emotional distress, such as depression Reduce emotional distress, such as depression and anxiety (CBT)and anxiety (CBT)Increase selfIncrease self--management / coping skillsmanagement / coping skillsIncrease quality of lifeIncrease quality of lifeTeach selfTeach self--regulation of psychophysical arousalregulation of psychophysical arousalDecrease inappropriate health care utilizationDecrease inappropriate health care utilization
Pain Management Programs by the American Chronic Pain Association

16
Helping Helping Change Change
Unhealthy Unhealthy HabitsHabits
Who is Part of an Interdisciplinary Who is Part of an Interdisciplinary TEAMTEAMPatientPatient
MD: PM&R and Occupational Medicine MD: PM&R and Occupational Medicine
Psychologist Psychologist
Rehabilitation Nurses Rehabilitation Nurses
Physical Therapist / Occupational TherapistPhysical Therapist / Occupational Therapist
Case Management /Social WorkersCase Management /Social Workers
Vocational CounselorsVocational Counselors
Biofeedback TherapistBiofeedback Therapist
CAM CAM –– Acupuncturist, massage therapist, chiropractic, etcAcupuncturist, massage therapist, chiropractic, etc
Nutritionist/dieticiansNutritionist/dieticians
PharmacistsPharmacists
Significant othersSignificant others

17
Physician ServicesPhysician ServicesComprehensive medical mgmtComprehensive medical mgmt
Patient educationPatient education
Formulation of medication treatment planFormulation of medication treatment plan
Communication with the referring physician & CMCommunication with the referring physician & CM
Rating examinations and disability determinationsRating examinations and disability determinations
Job analysis review & recommendationsJob analysis review & recommendations
Medication management Medication management –– Monitoring time contingent medication use & taper Monitoring time contingent medication use & taper
schedules)schedules)
Education on comorbidities Education on comorbidities –– shared emphasis on improving health, shared emphasis on improving health,
wellness, and taking selfwellness, and taking self--responsibilityresponsibility
TENS unit managementTENS unit management
Sleep hygiene and nutrition educationSleep hygiene and nutrition education
Nursing ServicesNursing Services
Sleep Hygiene
TENS

18
Physical TherapyPhysical Therapy
Education on Anatomy & PhysiologyEducation on Anatomy & PhysiologyHome exercise programHome exercise programCardiovascular fitness Cardiovascular fitness StretchingStretchingIncrease flexibilityIncrease flexibilityIncrease strengthIncrease strengthIncrease enduranceIncrease enduranceImprove posture Improve posture
SelfSelf--Management ToolsManagement Tools

19
People don’t hurt if they have something better to do. W. Fordyce, Ph.D.
We don’t stop playing because we grow old, we We don’t stop playing because we grow old, we grow old because we stop playing grow old because we stop playing George Bernard ShawGeorge Bernard Shaw
Occupational TherapyOccupational Therapy
Increase functional tolerances Increase functional tolerances Eliminate excessive guarding behaviorsEliminate excessive guarding behaviorsErgonomic consultationErgonomic consultationBody mechanics Body mechanics SelfSelf--pacingpacingGoal settingGoal settingPlanner usePlanner useADLsADLs

20
The ActivityThe Activity--Rest Cycle in Chronic Pain Rest Cycle in Chronic Pain (Gil, Ross, & Keefe, 1988) in Psychological Approaches to Pain Management: A Practitioner’s
Handbook. Edited by Robert J. Gatchel and Dennis C. Turk (1996)
Ergonomics &
Body Mechanicsfor
Activities of Daily Living

21
Vocational ServicesVocational Services
Provide vocational guidanceProvide vocational guidance
Job Analysis Review & RecommendationsJob Analysis Review & Recommendations
Provide information on Worker’s Comp systemProvide information on Worker’s Comp system
Provide info on labor market/wage & occupations Provide info on labor market/wage & occupations
Communicate with stakeholdersCommunicate with stakeholders
Case ManagementCase Management
Work Hardening/ConditioningWork Hardening/Conditioning
Biofeedback ServicesBiofeedback Services
Stress management through relaxationStress management through relaxation
Diaphragmatic breathingDiaphragmatic breathing
Muscle tension reductionMuscle tension reduction
Heart rate variability Heart rate variability

22
“It’s got to come out, of course, but that doesn’t address the
deeper problem.”
Dealing with Psychosocial IssuesCan Be Challenging
Psychological ServicesPsychological Services
Pain CatastrophizingPain-related Anxiety FearHelplessness
PainPsychological DistressPhysical Disability
Self-efficacyPain Coping StrategiesReadiness to ChangeAcceptance
PainPsychological DistressPhysical Disability
The Journal of Pain 5(4), Keefe, FJ, Rumble, ME, Scipio, CD, Giordano, LA, Perri LCM. Psychological aspects of persistent pain: current state of the science, 195-211.

23
What Indicates Progress in Treatment?What Indicates Progress in Treatment?
“When successful rehabilitation occurs, there is an “When successful rehabilitation occurs, there is an important cognitive shift from beliefs about important cognitive shift from beliefs about
helplessness and passivity to resourcefulness and helplessness and passivity to resourcefulness and ability to function regardless of pain.”ability to function regardless of pain.”
Jensen, Romano, Turner, 1999; Tota-Faucette, Gil, Williams, 1993; Williams & Thorn, 1989
Outcomes PRA Pain Program 2010Outcomes PRA Pain Program 2010
48% Decreased pain48% Decreased pain98% increased lifting tolerance 98% increased lifting tolerance 89% increased endurance 89% increased endurance 80% decreased depression (BDI80% decreased depression (BDI--II)II)70% increased self70% increased self--confidence in ability to cope confidence in ability to cope with pain (PSEQ)with pain (PSEQ)Of those who entered program on opioids 70% Of those who entered program on opioids 70% reduced their dosereduced their doseAverage dose reduction 70%Average dose reduction 70%96% recommended medically stationary (MMI) 96% recommended medically stationary (MMI) and recommended RTW full time with restrictionsand recommended RTW full time with restrictions

24
Comprehensive Pain Management Comprehensive Pain Management Programs Selected For Individuals Who…Programs Selected For Individuals Who…
Previously failed less intense interventionPreviously failed less intense interventionHave higher rates of opioid use (dose escalation)Have higher rates of opioid use (dose escalation)Activities limited due to fear of pain Activities limited due to fear of pain Have problems with vocational functioningHave problems with vocational functioningExperience high levels of emotional distressExperience high levels of emotional distressAre disability convictedAre disability convictedAre passive about tx & put life on hold waiting for fixAre passive about tx & put life on hold waiting for fixFeel hopeless and helplessFeel hopeless and helplessMultiple therapies with no improvement in functionMultiple therapies with no improvement in function
ResourcesResourcesThe Canadian Pain SocietyThe Canadian Pain Societyhttp://www.canadianpainsociety.ca/en/links.htmlhttp://www.canadianpainsociety.ca/en/links.html
www.Chronicpainnetwork.comwww.Chronicpainnetwork.com
http://painconsortium.nih.govhttp://painconsortium.nih.gov
Chronic Pain Association of Canada Chronic Pain Association of Canada http://www.chronicpaincanada.com/http://www.chronicpaincanada.com/
Western Pain SocietyWestern Pain Society–– 541541--345345--7300 7300 –– [email protected]@painsociety.com–– www.ampainsoc.org/societies/wpswww.ampainsoc.org/societies/wps/ /
American Pain SocietyAmerican Pain Society–– http://www.ampainsoc.org/http://www.ampainsoc.org/
Caresalliance.orgCaresalliance.org (painkiller safety tips, warning signs and other (painkiller safety tips, warning signs and other educational resources for patients)educational resources for patients)

25
Evidence Based Guidelines Evidence Based Guidelines American College of Occupational and American College of Occupational and Environmental Medicine (ACOEM)Environmental Medicine (ACOEM)Institute of Medicine (IOM)Institute of Medicine (IOM)American Medical Association (AMA)American Medical Association (AMA)Agency for Healthcare Research and Quality Agency for Healthcare Research and Quality (AHRQ)(AHRQ)American Pain Society (APS)American Pain Society (APS)American Society of Interventional Pain American Society of Interventional Pain Physicians (ASIPP)Physicians (ASIPP)Institute of Clinical System Improvement (ICSI)Institute of Clinical System Improvement (ICSI)North American Spine Society (NASS)North American Spine Society (NASS)

26
Being told that you have to learn to Being told that you have to learn to live with pain should not be the end live with pain should not be the end
of the road of the road –– It should be the It should be the beginning…Healing is truly a journey beginning…Healing is truly a journey
Jon Jon KabatKabat--ZinnZinn, Full , Full CatastopheCatastophe LivingLiving
CatrionaCatriona BuistBuist, , Psy.DPsy.D, Clinical Director , Clinical Director
Progressive Rehabilitation Associates Intensive InterdisciplinarProgressive Rehabilitation Associates Intensive Interdisciplinary Pain Programy Pain Program
“Dedicated to providing medical rehabilitation in a caring envir“Dedicated to providing medical rehabilitation in a caring environment to restore onment to restore function and quality of life.” function and quality of life.”