chronic pain management: current practices and where we should be heading
DESCRIPTION
Chronic Pain Management: current practices and where we should be heading. Assoc. Professor Michael Nicholas, PhD Pain Management Research Institute University of Sydney at Royal North Shore Hospital. Topics to be covered. - PowerPoint PPT PresentationTRANSCRIPT

Chronic Pain Management: current practices and where
we should be heading
Assoc. Professor Michael Nicholas, PhD
Pain Management Research Institute
University of Sydney at Royal North Shore Hospital

Topics to be covered
• Improving rehabilitation outcomes through an integrated management approach
• Pain/chronic pain management process, especially for those with mental health conditions such as depression, anxiety and PTSD
• Management of psychosocial elements in the rehabilitation of clients, especially for those with chronic pain
• The management of 'younger clients' who are having to deal with chronic pain while attempting to maintain their general functioning and productive lives

Time-based classification of pain
• Acute: short-term; usually due to nociception (tissue damage); resolves with healing.
• In back pain, Acute = < 4 wks
Sub-acute = 4-12 weeks
Chronic = > 12 weeks
• Chronic pain: pain lasting > 3-6 months
• Persisting pain (NHMRC: acute pain guidelines)

How common is the problem of chronic pain?
• Blyth et al. (2001) Pain, 89, 127-134.
• 17,000 interviewed (across NSW)
• Chronic pain (>3/12) prevalence (NSW):– 17.1% Males– 20.1% Females
• Interference in activities reported by ~ 60%

Persistent pain by age and sexNSW 1997 Health Survey (Blyth et al., 2001)
11.6
13.8
11.9
13
16.8
15.9
23.9
27.3
29.1
28.3
29.3
27.8
26.4
30.5
17.1
8.2
11.6
10.9
14.1
16.9
18.5
19.7
19.3
25.8
23.1
26.4
20.3
21.3
20.1
18.6
0 5 10 15 20 25 30 35
All
20-24
30-34
40-45
50-54
60-64
70-74
80+
males
females

Despite all the advances in medical technology….
• Complete relief of symptoms (pain) often an unrealistic goal once pain becomes chronic
• More realistic to seek ways to limit disability despite pain• That is, manage pain to limit its impact
Goucke CR. The management of persistent pain. Med J Aust 2003; 178(9): 444-447. Loeser JD. Mitigating the dangers of pursuing cure. In: Cohen MJM, Campbell JN, eds. Pain Treatment Centers at a Crossroads: A Practical and Conceptual
Reappraisal. Seattle, IASP Press, 1996:101-108.
“Traditional” Biological model of pain
PainInjury
(Nociception
or neuropathy)
Impact on activity, mood

Treatment implications?
Pain-freeNociceptionor neuropathy
Normal activity & mood restored
(e.g. Bogduk N. Management of chronic low back pain. Med J Aust 2004; 180 (2): 79-83)

This model works…
• (Usually) in acute pain states• (Usually) in some chronic pain cases with orthopaedic
procedures (eg. hip replacements)• But not always: Compensation status is associated
with poor outcome after surgery (Meta-analysis by Harris et al.. JAMA, April 6, 2005; 293: 1644-52).
• Gabbe et al (MJA, 2007): MVA victims with compensation claims in Victoria had worse health outcomes than those without compensation claims.
• (Temporarily) in selected (~ 5%) chronic cervical and low back pain cases (with radiofrequency lesions)
• But for the rest of those with chronic pain? - On average: 30% reduction in pain. (SeeTurk, Clin J Pain 2002).

What this means
• Outcome of treatment is influenced by the context in which it occurs
• Most people who develop chronic pain will have to learn to live with it
• But pain is rarely only presenting problem

PAIN PERSISTING
PHYSICALDETERIORATION(eg. muscle wasting, joint stiffness)
FEELINGS OF DEPRESSION,HELPLESSNESS,IRRITABILITY
SIDE EFFECTS(eg. stomach problems lethargy, constipation)
© M K Nicholas PhDPain Management & Research CentreRoyal North Shore HospitalSt Leonards NSW 2065AUSTRALIA
EXCESSIVESUFFERING & DISABILITY
Chronic pain often accompanied by other problems that interact
Influence of workplace, home, treatment providers
A BIOPSYCHOSOCIAL PERSPECTIVE
REDUCEDACTIVITY
UNHELPFULBELIEFS &THOUGHTS
REPEATEDTREATMENTFAILURES
LONG-TERMUSE OF ANALGESIC,SEDATIVE DRUGS
LOSS OF JOB, FINANCIALDIFFICULTIES, FAMILYSTRESS

Pain - current view
• Pain is an end-product of many interacting processes
in the nervous system (including the brain). • The relationship between injury and pain is quite
variable. • Knowledge of cause of pain is not sufficient to tell us
how much pain a person will have or its impact. • Diagnosis (eg. “Lumbar Discogenic Pain”) is a poor
guide to prediction of disability (Caragee et al, Spine Journal, 2005)

Implications for injury management

Common Mental Health Complications: Depression, Anxiety, Substance abuse and PTSD
• Polatin et al. (1993) reported that 59% of one sample of chronic pain patients demonstrated current symptoms for at least one psychiatric diagnosis, mainly major depression, substance abuse and anxiety disorders
• Individuals with chronic neck or back pain are almost three times more likely to have PTSD than those with no pain (Demyttenaere et al., 2007)
• The US National Comorbidity Study (using DSM-IV criteria), the 12-month prevalence of PTSD in individuals reporting chronic spinal pain was 7.3% (Von Korff et al., 2005).
• Beckham et al (1997) reported that 80% of a sample of 129 Vietnam Veterans presenting with PTSD reported chronic pain

Evidence for impact of Mental disorders in people with chronic pain
• Depression: Lower chance of RTW (Dionne, 2005; Pincus et al., 2002; Sullivan & Stanish 2003; Vowles et al. 2004; Rezai & Cote 2005; Sullivan et al. 2005)
• PTSD: Increased risk for prolonged disability following whiplash injury (Sterling et al., 2003; 2005)
• PTSD: (especially reexperiencing symptoms) in Vietnam Veterans associated with higher levels of pain and pain-related disability (Beckham et al. (1997) and Asmundson et al. (2004)
• Substance abuse disorder : Lower chance of RTW; less likely to have good rehabilitation outcomes; more likely to have re-injury. (Burton et al (1997); Evans et al., (2001)

Consequences of co-morbidity
• Chronic pain patients who have a co-morbid mental disorder have a more impaired quality of life than those without comorbidity (eg. Bair et al., 2003).
Treatment outcomes compromised
• Treatment outcomes can be compromised when both pain and a mental disorder are present but only one of them is targeted for treatment.
• Higher levels of depression have been shown to be predictive of poorer treatment outcomes for chronic pain patients (eg. Cherkin et al., 1996), as well as higher health care costs over time (Engel et al., 1996).

Opportunity
• Improving our understanding of how chronic pain and mental disorders relate to each other offers the prospect of much greater joint treatment effects than we may obtain from just improving treatments for either alone (eg. Haythornthwaite, Neurology, 2006).

Intervening in psychosocial aspects before chronicity sets in (controlled studies from 2000)
Study Intervention & Outcomes (bold) Comment
Van den Hout et al. 2003
Graded activities (behavioural principles) + problem-solving training > Graded activities + education
(on longer-term work status)
Åsenlöf et al.., 2005 Individually-tailored cbt + exercises > exercises (on disability, pain fear of movement)
Linton & Andersson, 2000
6 x 2-hr grp sessions with Clin. Psychologist + Rehab > Information + Rehab (on lost time from work)
Marhold et al., 2001 Same treatment as above > for sub-acute lbp than chronic lbp. (RTW outcome)
Linton et al., 2005 CBT grp = CBT + exercise grp >> minimal tmt grp (examination, reassurance, advice on activities).
(lost time)
Verbeek et al., 2002 Many similarities in content of control grp and treatment grp. No difference between grps on disability & RTW outcome (both improved).
Low distress in both groups
Jelema et al., 2005 Psychosocial intervention = standard care (both by GP only) (on disability) Low level of psychosocial risk factors at baseline
Hlobil et al., 2005 Graded activity grp > usual care. (GPs consistency with program encouraged): Earlier RTW
Hay et al., 2005 CBT (pain management) and manual therapy (+ home exercise) achieved similar results (disability) Average distress low initially so difficult to show much change.
Sullivan et al., 2006 Psychosocial risk factors reduced in both groups (Physio + CBT vs Physio only), but catastrophizing reduced more in combined group. Combined group had better RTW 4-wks after end of treatment.
Loisel et al., 2002 All interventions achieved gains, but comprehensive ‘Sherbrooke’ model (combined occupational and clinical interventions) had fewer days on benefits. (RTW)
Gatchel, et al . 2003 ‘high risk’ acute patients in functional restoration group (CBT approach) >a treatment-as-usual group.
(on indices of disability; work, healthcare utilization, medication use and self-reported pain).
Kant et al. 2008 Physician intervention that targeted identified specific individual concerns + problem-focused counselling when needed) > standard care (on RTW outcomes)
Damush et al., 2003 Brief group program, with telephone follow-up, aimed at increased function, health status > usual care

When pain has become chronic?
• Is it too late?

Pain management plan for chronic pain may need to be adjusted for severity/complexity of
case
• ‘Dose-response’ relationship for CBT pain management programs and chronic pain
• Basic message: More distressed/disabled cases need more extensive treatment
• Evidence:Guzman et al., BMJ 2002: systematic reviewWilliams et al. Pain 1999: RCTMarhold and Linton, Pain 2001: RCTHaldorsen et al., Pain 2002: RCT
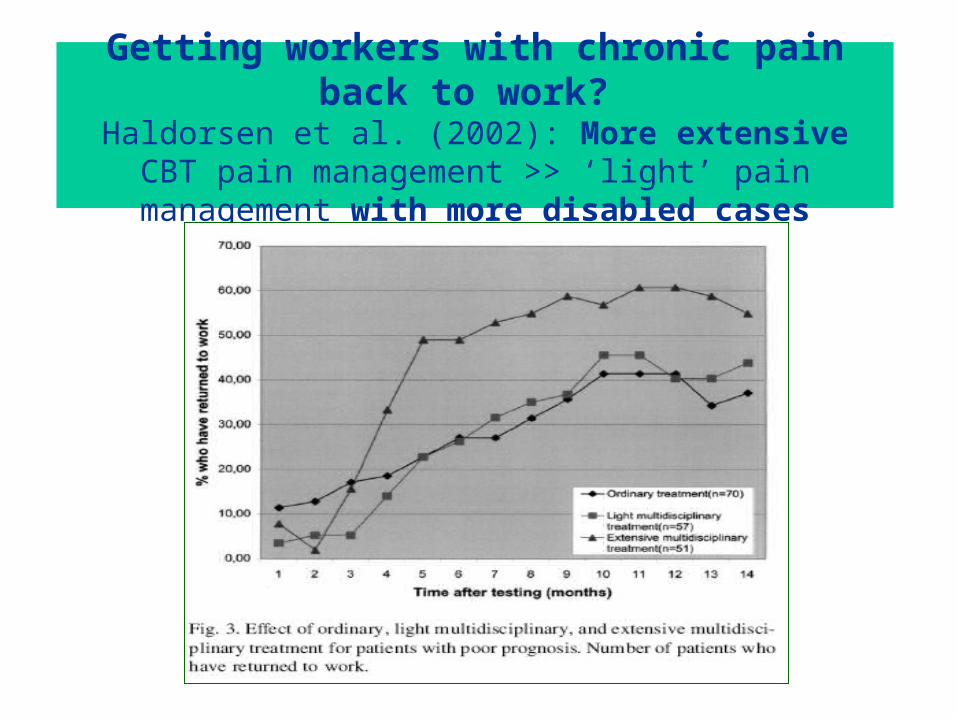
Getting workers with chronic pain back to work? Haldorsen et al. (2002): More extensive CBT pain
management >> ‘light’ pain management with more disabled cases

Implications
• When psychosocial risk/prognostic factors low, usual care is sufficient (Usual care seems effective in “uncomplicated cases of LBP” – Jallema et al. Pain 2006)
• When psychosocial risk/prognostic factors high, interventions targeting these aspects often more effective than usual care

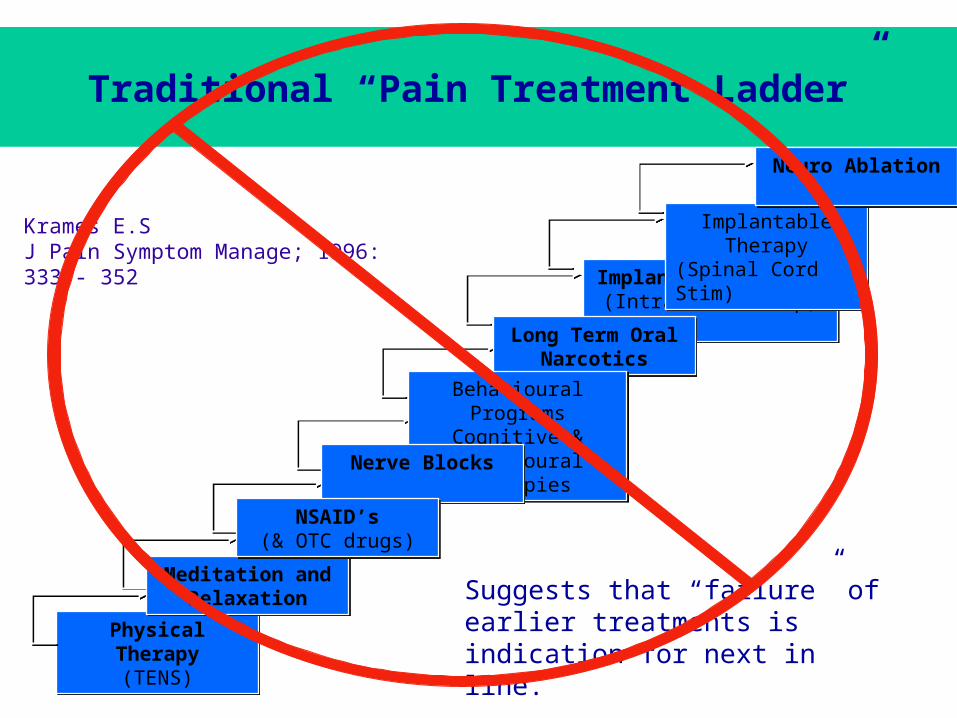
Traditional “Pain Treatment Ladder”
Physical Therapy(TENS)
Physical Therapy(TENS)
Implantable Therapy(Intrathecal Pump)
Implantable Therapy(Intrathecal Pump)
Implantable Therapy(Spinal Cord Stimulator)Implantable Therapy
(Spinal Cord Stimulator)
Long Term Oral Narcotics
Long Term Oral Narcotics
Meditation and Relaxation
Meditation and Relaxation
Behavioural ProgramsCognitive & Behavioural
Therapies
Behavioural ProgramsCognitive & Behavioural
Therapies
Nerve BlocksNerve Blocks
Neuro AblationNeuro Ablation
NSAID’s(& over the counter drugs)
NSAID’s(& over the counter drugs)
Krames E.SJ Pain Symptom Manage; 1996: 333 - 352
Basic rule: “failure” of earlier treatments leads to consideration of next in ladder
Traditional “Pain Treatment Ladder”
Physical Therapy(TENS)
Physical Therapy(TENS)
Implantable Therapy(Intrathecal Pump)
Implantable Therapy(Intrathecal Pump)
Implantable Therapy(Spinal Cord Stim)Implantable Therapy
(Spinal Cord Stim)
Long Term Oral Narcotics
Long Term Oral Narcotics
Meditation and Relaxation
Meditation and Relaxation
Behavioural ProgramsCognitive &
Behavioural Therapies
Behavioural ProgramsCognitive &
Behavioural TherapiesNerve BlocksNerve Blocks
Neuro AblationNeuro Ablation
NSAID’s(& OTC drugs)
NSAID’s(& OTC drugs)
Krames E.SJ Pain Symptom Manage; 1996: 333 - 352
Suggests that “failure” of earlier treatments is indication for next in line.
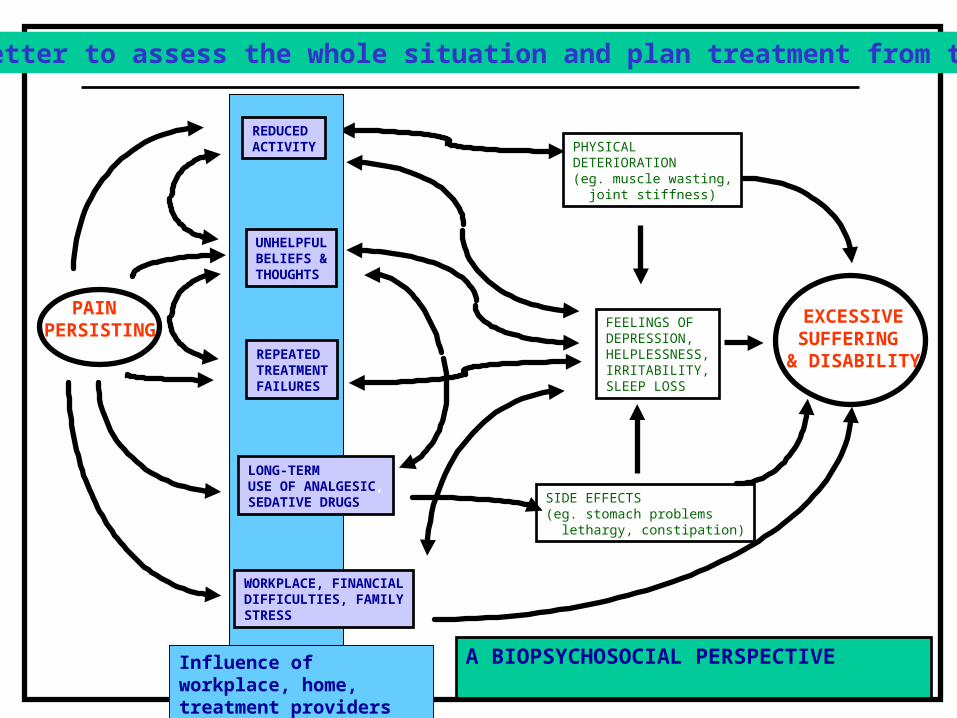
PAIN PERSISTING
PHYSICALDETERIORATION(eg. muscle wasting, joint stiffness)
FEELINGS OF DEPRESSION,HELPLESSNESS,IRRITABILITY,SLEEP LOSS
SIDE EFFECTS(eg. stomach problems lethargy, constipation)
© M K Nicholas PhDPain Management & Research CentreRoyal North Shore HospitalSt Leonards NSW 2065AUSTRALIA
EXCESSIVESUFFERING & DISABILITY
Better to assess the whole situation and plan treatment from there
A BIOPSYCHOSOCIAL PERSPECTIVEInfluence of workplace, home, treatment providers
WORKPLACE, FINANCIALDIFFICULTIES, FAMILYSTRESS
LONG-TERMUSE OF ANALGESIC,SEDATIVE DRUGS
REPEATEDTREATMENTFAILURES
UNHELPFULBELIEFS &THOUGHTS
REDUCEDACTIVITY

Combining medical and psychological interventions for chronic pain
• Haythornthwaite (2005) Clinical trials studying pharmacotherapy and psychological treatments alone and together. Neurology 2005; 65(suppl 4): S20-S31.
• Holroyd et al. (1995; 2001): Treatment of headaches – combination of medication & cbt
• Kishino et al. (2000) Psychological intervention plus exercise for post-surgical pain
• Leibing et al. (1999); Sharpe et al. (2001): rheumatoid arthritis patients: combined rheumatology treatment & cbt more effective

Could we learn from other fields that deal with chronic illnesses/diseases?
• “Medical care for chronic illness is rarely effective in the absence of adequate self-care (by patient)”.
Von Korff et al. (1997) Ann Int Med, 127, 1097-1102

Workplace-based interventions
Workplace-based Return-to-work Interventions: A Systematic Review of
the Quantitative Literature
Franche et al. J. Occupational Rehabilitation 2005; 15 (4)

Key findings (Franche et al. 2005)
Workplace intervention strategies Strength of Evidence
(less) Work loss• Early contact with the worker by
the workplace Moderate
• Work accommodation offer Strong
• Contact between healthcare provider Strongand the workplace
• RTW coordination Moderate
• Super-numerary replacements Insufficient

Some conclusions
• Chronic pain is common (1 in 5 people)• It is a risk factor for disability• The presence of mental disorders increases risk of
disability in those with chronic pain• Curative treatment is unlikely (no magic bullet)• Interventions need to be targeted against identified
risk factors (bio – psycho – social) • Challenge: Collaborative approach offers best chance
of success• All stakeholders must play active, informed roles
