chronic lateral knee pain and ehlers … place delange... · muscles crossing the knee joint. ......
TRANSCRIPT

Running head: CHRONIC LATERAL KNEE PAIN AND EHLERS-DANLOS 1
The Effects of Massage Therapy on Chronic Lateral
Knee Pain in a Patient with Ehlers-Danlos Syndrome:
A Case Study
Natalie A. Delange
Tel. (250) 303-0218 email. [email protected]
Address. 8869 Driftwood Road, Black Creek, BC. V9J1A9
West Coast College of Massage Therapy - Victoria
CHRONIC LATERAL KNEE PAIN AND EHLERS-DANLOS 2
Acknowledgements
I would like to express my sincere gratitude to the case study subject for his
participation in this project. Volunteering his time to this study has enabled me to
learn and grow as a therapist. The staff, administration and fellow students at
WCCMT Victoria gave insight and shared their knowledge through my studies
for which I’m very appreciative.
Conflict of Interest and Consent
Therapist and patient were acquainted through a mutual friend prior to this study.
In accordance with the College of Massage Therapists of British Columbia’s code
of ethics, proper measures were taken to ensure that this relationship did not affect
or influence the therapist’s clinical treatment of this patient. Informed consent was
obtained from the patient prior to and throughout this study. All identifiable
information has been removed from this study to protect the privacy of the
patient.

CHRONIC LATERAL KNEE PAIN AND EHLERS-DANLOS 3
Abstract
This case study explored the effect of massage therapy on chronic knee pain in an
Ehlers-Danlos Syndrome (EDS) patient. The patient was a 25-year-old male with
a history of chronic pain and “clicking” of the left knee during standing flexion. A
sequence of ten treatments was administered over eight weeks. The lower
extremity was assessed through various orthopedic testing, including hip range of
motion with a goniometer. A variety of general Swedish massage (GSM)
techniques were used throughout this study. Trigger point pressure release
(TPPR), muscle stimulation, myofascial holds and contract-relax stretches were
also included. For homecare, exercises were given to stretch and strengthen the
muscles crossing the knee joint. Lastly, various changes to activities of daily
living (ADLs) were recommended. The effectiveness of the treatments was
measured using a 0-to-10 patient pain scale, orthopedic testing, and knee girth
measurements. The goals of this study were to alleviate lateral knee pain, reduce
lateral patellar pull and increase joint awareness. The results of this study show
that massage therapy proved to be beneficial for this particular patient. Chronic
lateral knee pain was eliminated, tension in the vastus lateralis muscle was
decreased allowing for proper patellar alignment at rest and patient awareness in
joint proprioception was increased. These findings support the use of massage
therapy as a means to alleviate pain and discomfort associated with EDS.
Key words: Ehlers-Danlos Syndrome, Patellar tracking, Massage Therapy

CHRONIC LATERAL KNEE PAIN AND EHLERS-DANLOS 4
Table of Contents
Title Page………………….………………………………………………1
Acknowledgements and Conflict of interest……………...……………….2
Abstract……………………….…………………………………………...3
Table of Contents……………….…………………………………………4
Introduction…………………….………………………………………….5
Methods……………………….…………………………………………..9
Results………………………………….………………………………...18
Discussion/Conclusion………………………………………..………….20
References…………………………………….………………………….23
Appendix A: Progression Photos……………………….………………..28
Appendix B: Letter From The Patient…………………………………...30
Appendix C: Patient Consent Form……………..…………………...…..31

CHRONIC LATERAL KNEE PAIN AND EHLERS-DANLOS 5
Introduction
Ehlers-Danlos Syndrome (EDS) refers to a group of inherited disorders caused by
a genetic mutation in collagen that disrupts the synthesis of connective tissues
(Childs, 2010). The variation of these genes appears to be one of the main reasons
that EDS has such a vast impact on the body’s supporting structures and their
functional ability. This inherited syndrome occurs from 1 in 5,000 to 1 in 10,000
depending on which type of EDS is present (Rombaut, Malfait, Cools,
De Paepe & Calders, 2010). There are 6 main subtypes of the 13 recognized types
of EDS (The Ehlers-Danlos Society, 2017). Research by Malfait and De Paepe
(2014) states that the three most common subtypes of EDS are hypermobility,
classic, and vascular types while kyphoscoliosis, arthrochalasis, and
dermatosparaxis are infrequent. This syndrome presents with a multitude of
clinical manifestations including joint hypermobility, velvety hyperextensible
skin, musculoskeletal pain, easy bruising, and generalized weakness and fragility
of the soft connective tissues (Malfait & De Paepe 2014). Massage cannot
“reprogram defective genes,” however, it could potentially help relieve pain
associated with the hypertonia that is caused by the increased muscular effort
required to support unsteady joints (Werner, 2008).
Massage therapy has yet to be fully researched as a treatment to alleviate pain
associated with EDS, however there are a few alternative options available. A

CHRONIC LATERAL KNEE PAIN AND EHLERS-DANLOS 6
systematic review of pain control methods in patients with EDS was conducted in
2015: The pain solutions perceived as the most beneficial were opioids, surgical
interventions, splints and braces, avoidance of potentially dangerous activities,
heat therapy, as well as massage therapy; opioids were identified to be the
treatment of most success for pain management (Arthur, Caldwell, Forehand &
Keith, 2015).
Patients with EDS can use opioids to control pain, but unwanted complications
and side affects may occur. Symptoms of constipation, drowsiness, and apathy
have been reported, and abuse of medications has also been found to occur
(Prokop, Adamczyk & Krajnik, 2010). The risks and inconvenience
accompanying medications are weighed against the positive results of patients
being able to function with limited pain. Prokop, Adamczyk & Krajnik (2010)
state that opioids should be the patient’s last resource after other methods have
failed.
Another option includes the use of local anesthetic trigger points to help with
chronic myofascial pain with EDS patients. In a 2016 study, a numbing serum
was injected into trigger points of a patient with EDS and paired with hot
hydrotherapy, deep tissue massage, stretches, and use of oral non-steroidal anti-
inflammatory drugs (NSAIDS) (Tewari, Madabushi, Agarwal, Gautam & Khuba,
2017). This study showed 60-80% pain relief within the first week. This method,

CHRONIC LATERAL KNEE PAIN AND EHLERS-DANLOS 7
however, is very invasive. Comparable results were shown in a less invasive
manual trigger point pressure release technique used by massage therapists (Hains
& Hains, 2010).
Physiotherapy is another field that uses manual therapies, which are used to help
mediate pain in EDS patients. Physiotherapy can provide the patient with physical
rehabilitation techniques for unsteady, hypermobile joints and their associated
pain. Physiotherapy uses non-invasive, self-motivated methods, and can be
considered the most successful traditional strategy when dealing with pain
(Keer & Simmonds, 2011). However, while physiotherapy has been shown to
increase proprioception and strengthen unstable joints, EDS patients have
reported the use of physiotherapy alone is not enough (Tewari et al., 2017).
The patient chosen for this study was a healthy 25-year-old male with EDS
suffering from chronic left knee pain. The exact type of EDS the patient has was
undetermined, however, he presented with hyperextensible skin (Figure 1) and
unstable joints of the lower extremity. Skin abnormalities are common in most
EDS subtypes and can include fragility, hyperextensibility, bruising, cigarette
paper appearance, and atrophic scaring (Hauser & Phillips, 2011). Hauser and
Phillips (2011) claim that other than skin abnormalities, the most recurrent
complaints are musculoskeletal pain. The patient’s major complaint was muscle
and knee pains as well as joint instability of the left lower extremity. At rest, the

CHRONIC LATERAL KNEE PAIN AND EHLERS-DANLOS 8
patient’s left patella faced laterally. A weak vastus medialis muscle can have this
affect on the patella (Sakai, Luo, Rand, An, 2000). Myofascial contractures may
develop in the imbalanced muscles supporting unstable joints, which can lead to
pain and discomfort (Tewari et al., 2017). Prior to this study the patient had no
exposure to massage therapy and had yet to find a way to control his pain.
An appropriate non-invasive therapy has yet to be found as a solution for
managing pain experienced by EDS patients. It seems health care providers need
to gain more experience treating the syndrome to be able to provide appropriate
and practicable therapy. The primary goal of this case study was to determine if a
course of massage therapy treatments could alleviate lateral knee pain, reduce
lateral patellar pull at rest, and increase joint awareness and proprioception for a
patient with Ehlers-Danlos Syndrome.
Figure 1: Patient’s knee
presentation

CHRONIC LATERAL KNEE PAIN AND EHLERS-DANLOS 9
Methods
Patient profile
The patient was a 25-year-old male presenting with chronic left knee pain for the
last two years. He had been working as a carpenter, so his job was extremely
physical, requiring a lot of heavy lifting and long standing squats. At the age of
14, he was diagnosed with EDS and has suffered from many injuries with extreme
outcomes for the past twelve years. The patient has no familial history of EDS
that he is aware of. At least twice a year he experiences an injury that requires
medical attention. These injuries are usually from trauma to a bony prominence
leading to excess fluid that exceeds the skins capacity, requiring surgical
drainage. He has no history of dislocations or breaks; however, he has suffered
from chronic muscle and joint pain his whole life. Pain medications tried were
acetaminophen and ibuprofen, but did not provide relief for the patient. Other than
emergency visits to the doctor, the patient has never sought out medical attention
or alternative therapy for his condition. The client’s goals and desired outcomes
were to find a non-invasive way to alleviate his chronic pain.
Assessment
The baseline for the subject’s assessment was established during the initial intake
of the first treatment. Beighton score testing, a method used to diagnose
hypermobility associated with EDS, was performed during the first assessment

CHRONIC LATERAL KNEE PAIN AND EHLERS-DANLOS 10
(The Ehlers-Danlos Society, 2017). The following subjective and objective
measures were used to evaluate the treatments’ effectiveness: (1) The patient was
asked to evaluate his progress in terms of pain and subjective disability
(Figure 2); and (2) The examiner used active range of motion, manual muscle
tests, special orthopedic tests, knee girth measurements, and active modalities to
assess knee function (Table 1, 2, and 3). The muscles crossing the knee joint were
the focus of the study based on the research of lateral knee pain referral as well as
the stabilizing muscles of the knee (Rattray & Ludwig, 2000).
Girth measurement was taken by using a tape measure at the supracondylar ridge,
mid patella, and tibial tuberosity bilaterally pre and post treatment to assess knee
effusion. These measurements were taken every treatment to assess knee effusion
and joint irritation.
Pictures were taken of the patient’s knee alignment, active squatting, and sensory
changes during treatments one, five, and ten. These pictures were taken as a
means of visual measurement of the patient’s progress of positioning throughout
the duration of the study (Appendix A).

CHRONIC LATERAL KNEE PAIN AND EHLERS-DANLOS 11
Orthopedic Tests Treatments
Beighton Score Testing 1
Stork 1,8,9
Trendelenburg All
Gillet’s All
Adductor Contractor All
Hamstring 90-90 All
Thomas All
Ober’s All
Apley’s Distraction 1
Apley’s Compression 1, 9
Table 1: Schedule of Orthopedic Testing (Magee, 2014).
Range Of Motion Treatments
Hip ROM 1,2,3,5,6,7,8,9,10
Knee ROM 1, 10
Table 2: Schedule of Range of Motion Measurements
Manual Muscle Tests Treatments
Gluteus Maximus 1,5,6,9,10
Gluteus Medius 1,7,10
Gluteus Minimus 1,7
Piriformis 1
Adductor Group 1,2,3,10
Beceps Femoris 1,6
Vastus Lateralis 1,5
Vastus Medialis Oblique 1,2,3,5,6,7,9,10
Gastrocnemius 1
Table 3: Schedule of Manual Muscle Tests (Kendall, F., McCreary, E., Provance,
P., Rodgers, M., & Romani, W., 2005)

CHRONIC LATERAL KNEE PAIN AND EHLERS-DANLOS 12
Figure 2: Left Lateral Knee Pain Presentation Pre and Post Treatment.
Treatment Plan
This study focused on reducing chronic lateral knee pain, stabilizing the left knee
joint, and reducing lateral pull on the patella at rest. The patient was treated in the
student clinic at the West Coast College of Massage Therapy, Victoria, BC. Each
appointment was 70 minutes in length, which included 10 minutes at the
beginning for interview and assessment, 10 minutes at the end for reassessment
and homecare instructions, and a total of 50 minutes for hands-on treatment. The
Sharp Sharp
Ache
Ache
Tight
Dull
Dull Ache
0
1
2
3
4
5
6
7
8
9
1 2 3 4 5 6 7 8 9 10
Pa
in
Treatment
Pre Treatment
Post Treatment
CHRONIC LATERAL KNEE PAIN AND EHLERS-DANLOS 13
patient received 10 treatments over the course of 8 weeks. Each treatment focused
on the chronic lateral knee pain and vastus lateralis muscle hypertonicity,
however, modifications were made in various treatments to accommodate for
variations in patient’s presenting symptoms (Table 4). During the first half of the
study, treatments were once a week; in the second half, the treatment frequency
was increased to twice a week, as the therapist judged that this could potentially
improve outcomes.
Rattray (2000) explains that general Swedish massage (GSM) has various effects
on the musculoskeletal system, which include increased circulation, improved
lymphatic and venous return, as well as decreased pain perception and
sympathetic nervous system firing. Hypertonic muscles have the ability to restrict
blood flow to the musculature and, therefore, create a domino effect on joints and
circulatory structures around the effected muscle (Stewart, 2014). Based on this,
the therapist chose GSM to improve circulation and decrease the pain and
restrictions caused by the hypertonicity of the patient’s muscles.
Myofascial contractures may develop in the muscles supporting hypermobile
joints causing myofascial pain (Tewari et al., 2017). Shah and Bhalara (2012)
state that fascial restrictions may form due to inflammation, tissue injury, postural
stress, or lack of active range of motion. The two main techniques used to release
fascial adhesions are direct trigger point pressure release and prolonged fascial

CHRONIC LATERAL KNEE PAIN AND EHLERS-DANLOS 14
holds (Paolini, 2009). As defined by Rattray, “a trigger point (TrP) is a
hyperirritable spot, usually within a taught band of skeletal muscle or it’s fascia”
(Rattray & Ludwig, 2000). Myofascial pain is a common presentation of pain
with EDS patients (Castori et al., 2012) and TrP in the vastus lateralis muscle can
refer pain into the lateral thigh and knee (Rattray & Ludwig, 2000), therefore,
MFR was chosen as an appropriate technique to use during treatments.
Contract-relax stretching was chosen to further assist in relaxing the hypertonic
muscles attaching around the knee joint. A thermaphore (deep moist heating pad)
was used to warm the muscles before being stretched (Rattray & Ludwig, 2000).
Tapotement is one of the most useful stimulatory strokes in massage (Rattray &
Ludwig, 2000). Rattray and Ludwig (2000) state that tapotement for less then
three minutes helps stimulate fatigued muscles by increasing sympathetic nervous
system firing. To strengthen the fatigued and hypotoned muscles around unstable
joints, the therapist used a fingertip tapotement technique while the patient
actively engaged the muscle.
Treatment Details
Treatments one to five were designed to be exactly the same, with modifications
depending on daily presentation of the patient (Table 4). Each treatment focused
on relieving the myofascial adhesions of the vastus lateralis muscle in addition to

CHRONIC LATERAL KNEE PAIN AND EHLERS-DANLOS 15
stimulating the fatigued vastus medialis oblique muscle in order to reduce lateral
patellar displacement. The patient was positioned in prone for 20 minutes; a
thermaphore placed under the anterior thighs for the first 5 minutes to warm the
quadriceps muscles, and then GSM was applied to the whole posterior leg by
techniques including effleurage, palmer stroking, picking up, wringing, and
knuckle kneading (Rattray & Ludwig, 2000). Muscle stripping was applied to the
hamstring muscles and the gastrocnemius muscle. Attachment release was applied
to the vastus lateralis and vastus medialis muscles along the linea aspera. A
contract relax stretch was performed on the quadriceps once they had been
warmed up by the thermaphore. Stimulation was then done to the gluteus
maximus muscle by rapid fingertip tapotement while the patient actively extended
his hip up and down for one minute. This stimulatory technique was used to
encourage proper muscle firing with hip extension. Treatment was bilateral,
however, less time was spent on the unaffected leg. The patient was positioned in
the supine position for 30 minutes. GSM including longitudinal stroking, picking
up, wringing and knuckle kneading was administered to the anterior thigh. Focus
was given to the lateral thigh muscles of the left leg. Muscle stripping along the
vastus lateralis muscle and iliotibial band C-bending was administered.
C-Bending is used to target golgi tendon organs, proprioception nerve receptors
near musculotendonous junctions, as a means to ease spasm and tone of a muscle
(Rattray & Ludwig, 2000). Trigger point therapy was conducted to the vastus

CHRONIC LATERAL KNEE PAIN AND EHLERS-DANLOS 16
lateralis and vastus medialis an inch above the insertion point at the patella. The
therapist first palpated the trigger point, pressed down toward the belly of the
muscle until the patient reached a seven on the pain scale, and then held the
compression until the pain subsided to a one or zero. Therapist repeated TPPR
three times on each muscle followed by active ROM by the patient to restore
motion and muscle length (Rattray & Ludwig, 2000). Finally, stimulation to the
vastus medialis oblique muscle was done for one minute as the patient actively
extended the knee. The goal of this modality was to encourage proper muscle
firing with knee extension and increase tonicity of the vastus medialis oblique
muscle.
Treatments 5-10 were identical to the first five treatments; however, instead of
trigger point therapy a fascial hold was done. The trigger points that were
palpable in the first half of treatments became impalpable, yet the fascial
restrictions were still present. Three fascial holds were conducted by grasping the
thigh and applying a superior glide with hands on either side and held for one
minute. The fascial holds were the last technique used in each of the last five
treatments.

CHRONIC LATERAL KNEE PAIN AND EHLERS-DANLOS 17
Treatment # Modification Reasoning
2 Contract relax applied to
hamstrings before treatment
Patient presented with a
posterior hip rotation in the
assessment and the therapist
used a contract relax technique
to help adjust the hip angle.
3 No stimulation to VMO Patient had a constant ache in
his left knee during the
treatment and therapist did not
want to aggravate it.
5, 6, 7 Contract relax to hamstring
muscles in supine
Patient presented with very
hypertoned hamstring muscles.
9 No thermaphore used in prone Swelling present in the left
knee.
Table 4: Treatment Modifications
Home care:
Patient was given homecare after each treatment. The focus of homecare was
stretching, strengthening, and patient awareness and education on biomechanics
of proper squatting techniques. Stretching exercises addressed the hypertoned
muscles of the lower extremity. Strengthening exercises of vastus medialis
oblique muscle and gluteal muscles were used to increase stability of the knee and
hip joint.

CHRONIC LATERAL KNEE PAIN AND EHLERS-DANLOS 18
Results
Throughout the course of this case study the patient continued to make positive
gains. To start, patient awareness increased rapidly throughout the study. Partway
through the study, the patient reported “I am continuously thinking about how I
am squatting and the forces on my knee.” Additionally, lateral thigh tension was
reduced significantly when measured with Ober’s orthopedic testing protocol,
progressing from positive to negative throughout the study (Table 5); this
improvement was also evident in the pictures (Appendix A), which showcase the
patella shifting from lateral to a more neutral position by the end of the study. By
evaluating lateral knee pain in every treatment using Rattray’s (2000) pain scale, a
decrease was apparent from the initial treatment to the final treatment. The
patient’s pain started at an eight out of ten at the beginning and progressed to a
zero out of ten in the last couple of treatments where pain was non existent
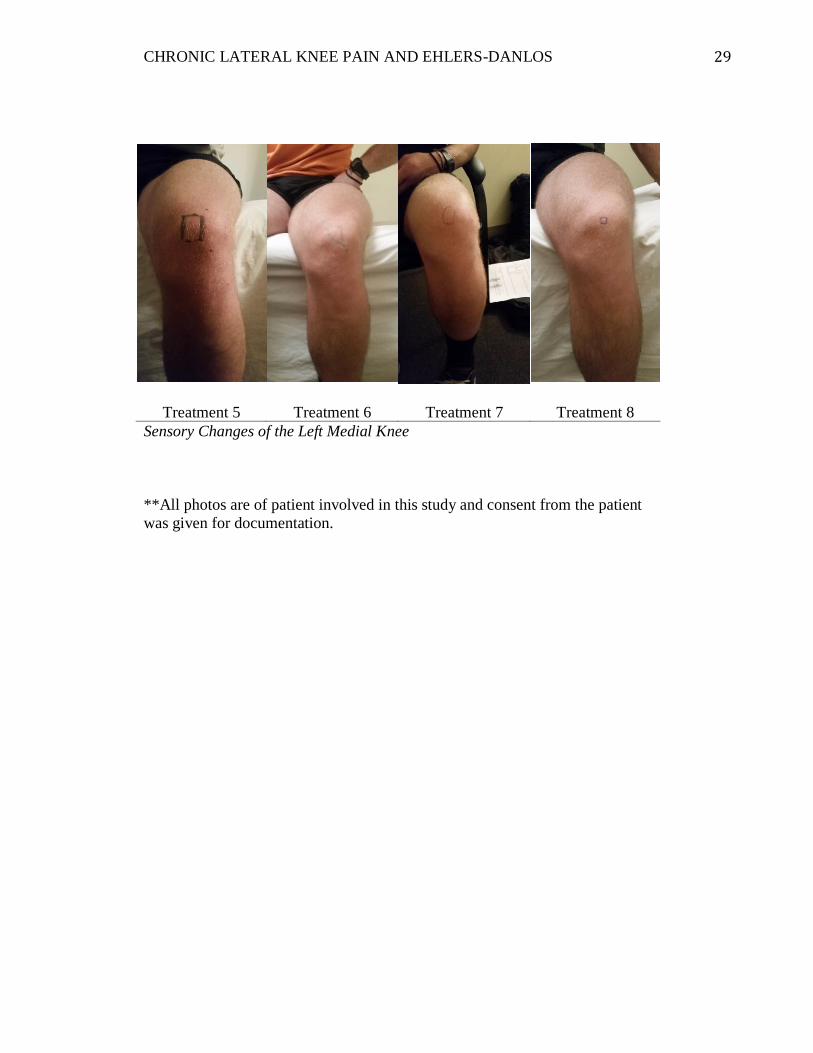
(Figure 2). During the intake of the fifth treatment the patient reported a “numb”
sensation in his left medial knee. The “numbness” gradually diminished as
treatments progressed (Appendix A). By the end of the study all measures of
effectiveness showed improved results.

CHRONIC LATERAL KNEE PAIN AND EHLERS-DANLOS 19
Orthopedic Test Treatment # Pre Treatment Post Treatment
Beighton Score 1 4/9 ---
Stork Test
1 (+) Bilaterally (+) Bilaterally
8 (-) Bilaterally (-) Bilaterally
9 (+) Left (-) Bilaterally
10 (-) Bilaterally (-) Bilaterally
Trendelenburg
Test
1 (+) Bilaterally (+) Bilaterally
2-10 (-) Bilaterally (-) Bilaterally
Gillet’s Test
1 (+) Left (-) Bilaterally
2 (+) Right (-) Bilaterally
3-10 (-) Bilaterally (-) Bilaterally
Adductor
Contracture Test
1 (+) Bilaterally (+) Bilaterally
2 (+) Bilaterally (+) Bilaterally
3 (+) Left (-) Bilaterally
4-10 (-) Bilaterally (-) Bilaterally
Thomas Test
1 (+) Bilaterally (+) Bilaterally
2 (+) Bilaterally (-) Bilaterally
3 (-) Bilaterally (-) Bilaterally
4 (+) Right (-) Bilaterally
5-10 (-) Bilaterally (-) Bilaterally
Ober’s Test
1 (+) Left (+) Left
2 (+) Left (-) Bilaterally
3 (+) Right (-) Bilaterally
4 (+) Left (-) Bilaterally
5-10 (-) Bilaterally (-) Bilaterally
Eli’s Test
2,3,4 (+) Bilaterally (+) Bilaterally
5 (-) Bilaterally (-) Bilaterally
6 (+) Left (-) Bilaterally
7-10 (-) Bilaterally (-) Bilaterally
Apley’s
Compression Test
1 (+) Left (-) Bilaterally
9 (+) Left (-) Bilaterally
Table 5: Orthopedic Test Results Pre & Post Treatment
CHRONIC LATERAL KNEE PAIN AND EHLERS-DANLOS 20
Discussion/ Conclusion
Musculoskeletal and joint pain is a common issue within the average population
and the EDS community. There are many treatments that attempt to alleviate the
discomfort associated with joint pain. There are no studies, to the therapist’s
knowledge, that specifically document the effects of massage therapy on the EDS
population.
This case study explored the effect of massage therapy on chronic knee pain in an
EDS patient. This patient was able to experience the benefit of massage for the
first time. He communicated throughout the study the positive impact the sessions
had on his knee and how much relief it had brought to his body. He expressed his
gratitude for being chosen for this study as he had finally found a way to relieve
his pain (Appendix B). Apart from finding pain relief, the study taught him a great
deal about himself and how his daily movements relate to his overall health.
The primary goal of this case study was to determine if a course of massage
therapy treatments could alleviate lateral knee pain, reduce lateral patellar pull at
rest, and increase joint awareness and proprioception. The treatment outcomes in
this study were extremely positive. A quote from one of the treatments, “I feel
like I have a new knee,” showcases this positive outcome. The stability in the
knee joint was improved through dedication to homecare. Trendelenberg and
Stork orthopedic tests began to show negative by the middle of the study and

CHRONIC LATERAL KNEE PAIN AND EHLERS-DANLOS 21
continued to do so throughout the remainder of the study (Table 5). The negative
results of these orthopedic tests prove stability of the lower extremity improved
throughout the study. Dedication to homecare strengthening exercises of the
vastus medialis oblique muscle and patient education on proper squat techniques
allowed the patient to eventually squat without “clicking” (Appendix A), which
further seems to prove that stability of the knee was increased. Lateral knee pain
diminished throughout the study and by the end was non-existent (Figure 2).
Through negative Thomas and Ober’s orthopedic tests it is clear that lateral thigh
tonicity was decreased which allowed for the patella to rest in a more neutral
position. Progression pictures in Appendix A illustrate the patella gradually
shifting from lateral to a more neutral position by the end of the study.
One deviation from the positive results occurred after treatment 5. The patient
began to feel a “numb and tingling” sensation in the left medial knee. The reason
for this is idiopathic, however, the therapist predicts this was due to the increase
in weight applied during vastus medialis oblique muscle strengthening. Over
exertion of the vastus medialis muscle can lead to hypertrophy of the muscle and
cause irritation of the branch of the femoral nerve that runs through vastus
medialis oblique muscle (Detterline, A., Babb, J., & Noyes, F. R., 2016).
This study contained cost efficient homecare and positive treatment results,
leading to client compliance. Massage therapy showed to be helpful for this

CHRONIC LATERAL KNEE PAIN AND EHLERS-DANLOS 22
specific patient; however, further studies need to be conducted to further
consolidate the affects of massage therapy on chronic musculoskeletal pain
experienced by EDS patients.

CHRONIC LATERAL KNEE PAIN AND EHLERS-DANLOS 23
References
Arthur, K., Caldwell, K., Forehand, S., & Keith, D. (2015). Pain control methods
in use and perceived effectiveness by patients with Ehler-Danlos
syndrome: a descriptive study. Disability and Rehabilitation, 38(11),
1063-1074.
doi: 10.2109/09638288.2015.1092175
Beighton, P., De Paepe, A., Steinmann, B., Tsipouras, P., & Wenstrup, R. J.
(1998). Ehlers danlos syndromes: revised nosology. American Journal of
Medical Genetics, 77(1), 31-7.
Castori, M., Morlino, S., Celletti, C., Celli, M., Morrone, A., Colombi, M.,
Camerota, F., & Grammatico, P. (2012). Management of pain and fatigue
in the joint hypermobility syndrome (aka ehlers-danlos syndrome,
hypermobility type): principles and proposal for a multidisciplinary
approach. American Journal of Medical Genetics Part A, 158(8), 2055-
2070.
doi: 10.1002/ajmg.a.35483
Childs, S. G. (2010). Musculoskeletal manifestations of Ehlers–Danlos
Syndrome. Orthopaedic Nursing, 29(2), 133-139.
doi: 10.1097/NOR.0b013e3181d243f4
CHRONIC LATERAL KNEE PAIN AND EHLERS-DANLOS 24
De Paepe, A., & Malfait, F. (2012). The Ehlers–Danlos syndrome, a disorder with
many faces. Clinical Genetics, 82(1), 1-11.
doi:10.1111/j.1399-0004.2012.01858.x
Detterline, A., Babb, J., & Noyes, F. R. (2016). Medial and anterior knee
anatomy. Noyes' Knee Disorders: Surgery, Rehabilitation, Clinical
Outcomes E-Book, 1.
Hains, G., & Hains, F. (2010). Patellofemoral pain syndrome managed by
ischemic compression to the trigger points located in the peri-patellar and
retro-patellar areas: a randomized clinical trial. Clinical Chiropractic, 13,
201-209.
doi: 10.1016/j.clch.2010.05.001
Hauser, R., & Phillips, H. (2011). Treatment of joint hypermobility syndrome,
including ehlers-danlos syndrome, with hackett-hemwall prolotherapy.
Journal of Prolotherapy, 3(2), 612-629.
Hertling, D., & Kessler, R.M. (2006). Management of common musculoskeletal
disorders: physical therapy principles and methods (4th ed.).
Philadelphia, PA: Lippincott Williams & Wilkins.
CHRONIC LATERAL KNEE PAIN AND EHLERS-DANLOS 25
Keer, R., & Simmonds, J. (2011). Joint protection and physical rehabilitation of
the adult with hypermobility syndrome. Current Opinion in
Rheumatology, 23(2), 131-136.
doi: 10.1097/BOR.0b013e328342d3af
Kendall, F., McCreary, E., Provance, P., Rodgers, M., & Romani, W. (2005).
Muscles testing and function with posture and pain (5th ed.). Philadelphia,
PA: Lippincott Williams & Wilkins.
Kisner, C., & Colby, L. A. (2012). Therapeutic exercise: foundations and
techniques. Fa Davis.
Magee, D. J. (2014). Orthopedic physical assessment (6th ed.). St. Louis:
Saunders Elsevier.
Malfait, F., & De Paepe, A. (2014). Progress in heritable soft connective tissue
diseases. Advances in experimental medicine and biology. (802)129-143.
doi:10.1007/978-94-007-7893-1_9
Paolini, J. (2009). Review of myofascial release as an effective massage
therapy technique. Athletic Therapy Today, 14(5), 30-34.
doi: 10.1123/att.14.5.30

CHRONIC LATERAL KNEE PAIN AND EHLERS-DANLOS 26
Prokop, A., Adamczyk, A., & Krajnik, M. (2010). Chronic use of opioids in
a patient with ehlers-danlos syndrome- a case report. Advances in
Palliative Medicine, 9(2), 53-59.
Rattray, F., & Ludwig, L. (2000). Clinical massage therapy. Elora,
Ontario: Talus Incorporated.
Rombaut, L., Malfait, F., Cools, A., De Paepe, A., & Calders, P. (2010).
Musculoskeletal complaints, physical activity and health-related quality of
life among patients with the ehlers-danlos syndrome hypermobility type.
Disability and Rehabilitation, 32 (16), 1339-1345.
doi: 10.3109/09638280903514739
Sakai, N., Luo, Z. P., Rand, J. A., & An, K. N. (2000). The influence of weakness
in the vastus medialis oblique muscle on the patellofemoral joint: an in
vitro biomechanical study. Clinical Biomechanics, 15(5), 335-339.
doi: 10.1016/S0268-0033(99)00089-3
Shah, S., & Bhalara, A. (2012). Myofascial release. International Journal
of Health Sciences and Research, 2(2), 69-77.
CHRONIC LATERAL KNEE PAIN AND EHLERS-DANLOS 27
Stewart, T. (2014). About your muscles: what you may not know~and why it
matters. NeuroSoma Muscle Therapy, 1-10.
Retrieved from
http://neurosoma.com/wp-content/uploads/About-Your-Muscles-What-
you-May-Not-Know-Why-it-Matters.pdf
Tewari, S., Madabushi, R., Agarwal, A., Gautam, S. K., & Khuba, S.
(2017). Chronic pain in a patient with ehlers-danlos syndrome
(hypermobility type): the role of myofascial trigger point injections.
Journal of Bodywork and Movement Therapies, 21(1), 194-196.
doi: 10.1016/j.jbmt.2016.06.017
The Ehlers-Danlos Society (2017). EDS/HSD info. Retrieved from
https://ehlers-danlos.com/privacy/
Werner R. (2008). Ehlers-Danlos Syndrome (EDS). Massage Today, 8(10).
Retrieved from
http://www.massagetoday.com/mpacms/mt/article.php?id=13874

CHRONIC LATERAL KNEE PAIN AND EHLERS-DANLOS 28
APPENDIX A: Progression Photos
Treatment 1 Treatment 5 Treatment 10
Left Knee Presentation: one mark made on center of patella and another on the
tibial tuberosity to showcase lateral patellar pull at rest.
Treatment 1 Treatment 5 Treatment 10
Squat Performed Without “Clicking”
CHRONIC LATERAL KNEE PAIN AND EHLERS-DANLOS 29
Treatment 5 Treatment 6 Treatment 7 Treatment 8
Sensory Changes of the Left Medial Knee
**All photos are of patient involved in this study and consent from the patient
was given for documentation.

CHRONIC LATERAL KNEE PAIN AND EHLERS-DANLOS 30
APPENDIX B: Letter From The Patient
“I just wanted to send a very warm thank you for all of our massage therapy
sessions. To be honest I had no idea massage could be of benefit to me until a few
weeks prior to treatments when you reached out to me. As soon as we started it
was clear that this was the right treatment for me. It was relaxing, therapeutic,
and gave instant results! I have found a noticeable change in the way I perform
sports, work, and even carry myself. It wasn’t until I missed on of our sessions
when I realized how much I needed it. My left knee pain was a bizarre pain that I
wrote off to be normal. My knee feels great now and I really appreciate you for
all the help and care you have provided me with through our sessions.”

CHRONIC LATERAL KNEE PAIN AND EHLERS-DANLOS 31
APPENDIX C: Patient Consent Form