chronic disease is an environmental issue
TRANSCRIPT

Chronic Disease is an Environmental Issue
Isadora Guggenheim, FNP, ND, RN, MS, CNS
1

How Does Ozone Work?
• Ozone has no receptors; its pharmacological mechanism of action is indirect, through its mediators
• The response is dependent on the activation of nuclear transduction mechanisms signals (Nrf2: Nuclear factor (erythroid-derived 2)-like 2) and protein synthesis, e.g. SOD (superoxide dismutase), CAT (catalase), HO1 (hemeoxygenase 1), etc.)
• Ozone therapeutic indications are based on the knowledge that low physiological dose of ozone may play important roles within the cell. Ozone does NOT work through free radical mechanisms
• While ozone itself lasts only microseconds in the blood, the reaction of ozone and blood lipids leads to the production of more stable and still highly reactive oxygen species (such as peroxides), which would react similarly and perhaps mimic the pro-oxidant mechanism of immune system defense
• It does work through the generation of many species of lipid peroxides
Herskowitz, 2017
2
“We are Shaped by Adversity”
• “I have come to the frightening conclusion that I am the
decisive element. It is my personal approach that creates the
climate. It is my daily mood that makes the weather....In all
situations, it is my response that decides whether a crisis is
escalated or de-escalated, and a person is humanized or is
dehumanized.” Johann Wolfgang von Goethe
3

OZONEAs soon as it is dissolved in plasma, or in water present on the skin
surface or in the interstitial fluids, it reacts instantaneously with severalsubstrates (soluble antioxidants, albumin, unsaturated fatty acids)
ErythrocytesImproved O2 delivery
ROSEarly phase
PlateletsRelease of autacoidsand growth factors
Bone marrowMay activate differentiation at theerythropoietic level, favouring the
formation of ¨supergiftederythrocytes¨, with improved
biochemical characteristics, activationof metaloproteinases (MP-9)
that favour the release of stem cells
LeukocytesImmune activation
EndotheliumModulation of NO
LOPLate phase
LOP reach in traceamounts to all organs
and can representmessengers
triggering multiformbiological activities
Other organsUpregulation of
oxidativestress proteins and
antioxidant enzymes (4-
hidroxialkenals, byinduction of glutamate
cysteine ligase expression,
produce an increase ofintracellular GSH)
From Dr. Silvia Menendez’ Ozone Masters Course February 2018
4
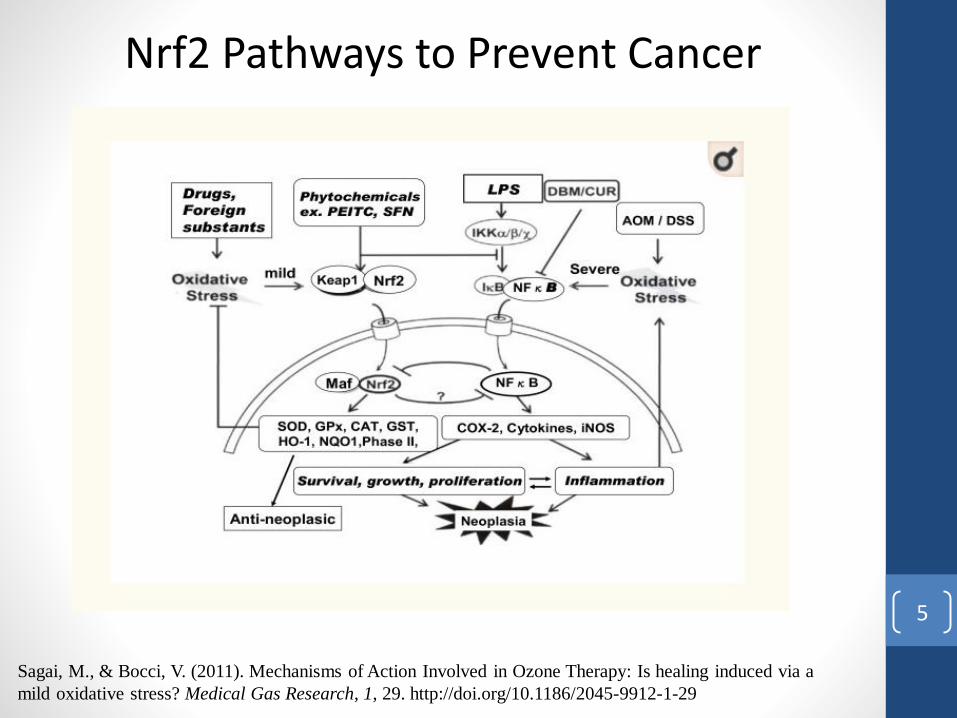
Sagai, M., & Bocci, V. (2011). Mechanisms of Action Involved in Ozone Therapy: Is healing induced via a
mild oxidative stress? Medical Gas Research, 1, 29. http://doi.org/10.1186/2045-9912-1-29
Nrf2 Pathways to Prevent Cancer
5

Biological Responses to Ozone
Therapy• Improves blood circulation and oxygen delivery
• Enhances general metabolism by improving oxygen delivery
• Upregulates cellular antioxidant enzymes and decreases free
radical production
• Activates the immune system and enhances the release of growth
factors, controls viral replication, kills microbes and kills cancer
cells
• Stimulates the neuroendocrine system
• Activates neuroprotective systems
• Helps to liberate heavy metals from tissue storage
• Protects inner mitochondrial membrane and entire electron
transport chain
• Maximal oxygen utilization means better fat burning
• Regulates NAD to NADH -700 to 1
• Oxygen delivery to all tissues
Herskowitz, 2017
6

Biological Responses to Ozone
Therapy Cont’d• Increasing the levels of direct antioxidants, such as GSH, CO, and
bilirubin.
• Stimulating GSH regeneration via glutathione and thioredoxin reductase.
• Increasing the levels of enzymes that detoxify oxidants and electrophils (i.e. catalase, SOD, GPx, GSTr, NADPH-quinone oxidoreductase (NQO1), HO-1, HSP70, etc).
• Increasing the levels of phase II enzymes.
• Inhibiting cytokine-mediated inflammation via the induction of leukotriene B4 reductase.
• Reducing iron overload, and subsequent oxidative stress induced via elevated ferritin.
• Recognizing, repairing, and removing damaged proteins.
• Protection from apoptosis induced via oxidative stress*.
• Increasing DNA repair activity*.
Sagai, M., & Bocci, V. (2011). Mechanisms of Action Involved in Ozone Therapy: Is healing induced via a mild oxidative stress? Medical Gas Research, 1, 29. http://doi.org/10.1186/2045-9912-1-29
7

OZONE BIOLOGICAL EFFECTS
OZONE
Maintains the cellularredox balance
Increases Oxygen Metabolism
Metabolic Regulator
Immunologic Modulator
Maintains the cellularredox balance
Germicidal Power
From Dr. Silvia Menendez’ Ozone Masters Course February 2018
8

Nrf2-nuclear factor-erythroid 2-related factor-2
Pharmacological effects of medical ozone
via ozone-produced peroxides (short-chain-
hydroxy-hydroperoxide with its low
tendency to radical reactions). The three
effects: (1) improved oxygen release by the
red blood cells (RBCs); (2)
Immunomodulation through activation of
the white blood cells (WBCs); and, (3)
Regulation of Cellular redox.
Renate et al, OS & Eng, 2012
“Ozone Peroxide” and its second
messenger. Cysteine residue and
glutathione oxidation processes induce
the cytokines – or anti-oxidant regulation
via NFkB or Nrf2, respectively. NrF2,
this important cytoprotective nuclear
transcription factor can suppress NFkB-
activation (Li W et al, Biochem
Pharmacol. 2008)
From Dr. Silvia Menendez’ Ozone Masters Course February 2018
9

Mild/Moderate Oxidative Stress
Antioxidant Response Elements
(ARE)SOD, GPx,
GSTr, CAT,
HO-1, NQO-1,
HSP
Activates hypoxia
inducible factor –
1 & (HIF-1a)
Initiates mild
immune
responses
Nuclear Factor
of Activated T-
cells (NFAT)
Activated
protein-1 (AP-1)
Activates Nrf2
(nuclear factor-
erythroid 2-
releated factor
2)
• Increases the levels of direct antioxidants, such as GSH
• Stimulates GSH regeneration via glutathione and thioredoxin reductase
• Increases the levels of enzymes that detoxify oxidants (i.e., catalase, SOD, GPx,
GSTr, NADH-quinone, oxidoreductase, (NQO1),HO-1, HSP70, etc)
• Increases the levels of phase II enzymes
• Inhibits cytokine-mediated inflammation
• Reduces iron overload, and subsequent oxidative stress induced via elevated ferritin
• Protects from apoptosis induced via oxidative stress
• Increases DNA repair activity
Biological responses induced via the activation
of Nrf2/ARE with mild/moderate oxidative stress
Herskowitz, 2017
10

From Dr. Silvia Menendez’ Ozone Masters Course February 2018
11

From Dr. Silvia Menendez’ Ozone Masters Course February 2018
12

ROS and Neurodegeneration
Sagai, M., & Bocci, V. (2011). Mechanisms of Action Involved in Ozone Therapy: Is healing induced via a
mild oxidative stress? Medical Gas Research, 1, 29. http://doi.org/10.1186/2045-9912-1-29
13

The Herrmann Machine
(n.d.). Retrieved from https://www.h-a-b.de/en/products/ozone/
Ozone Treatments with the Herrmann:
https://www.youtube.com/watch?v=um8JVHb74yU
https://www.youtube.com/watch?v=kjpR7DV8AxI
https://www.youtube.com/watch?v=a4pRTB5DVZc
14
Conclusions and Perspectives
• The application of ozone in medicine represents one of the most intriguing adventures in research. First of all because ozone is too well known as a toxic gas in the troposphere and secondly, in spite of courageous pioneers like Payr, Fisch, Wolff and Auborg, ozone stalled in an empirical phase for almost three decades and it was heavily damaged by the improper use of direct IV infusion by so-called doctors in desperate HIV-AIDS patients. This dangerous and useless application, associated with other deplorable episodes, led the FDA to prohibit the use of ozone in medicine. Today, the basic mechanisms of action of ozone in blood, documenting the existence of a therapeutic window and establishing a framework for understanding and recommending ozone therapy in some diseases have been clarified and we can start to see a faint light at the end of the tunnel. However, owing to the lack of sponsors and funding, the clinical work, fundamental for demonstrating the validity of ozone therapy, proceeds at a snail pace. Furthermore, the urgent need of treating too many patients in poor countries has stimulated the use of “cheap and quick” procedures that hinder progress. Clinical scientists for either prejudice, or lack of knowledge, or exclusive interest in pharmaceutical drugs disregard, if not object, ozone therapy that remains in the hands of practitioners who cannot deliver reliable scientific reports. Thus, optimistically let us say that we are at the end of the beginning but our enthusiasm remains high and we will continue our efforts for allowing the acceptance of ozone therapy as an efficacious approach to be included among the armamentarium of orthodox medicine. (Bocci et al. 2011)
15

Conclusions and Perspectives
• Our comparative study showed air plasma and ozone to have
very high bactericidal potency, both producing nearly 99.99%
efficacy. Moreover, both air plasma and ozone inactivated
different bacterial strains P. aeruginosa and S. aureus to the
same extent. (Lunov et al. 2014)
16

I.V. Ozone with German
Biologics Homotoxicology
“Anti-homotoxic medicine is an indication-oriented approach.
Homotoxic remedies are mixtures of substances of low to middle
potencies. This practice was scientifically supported by Rudolph
Arndt and Hugo Schulz through a quantitative differentiation of
the medicinal effect on Biosystems. It is known as the Arndt-
Schulz Principle. It states:”
• Weak stimuli stimulate the life functions (retro-action of
homeopathic preparations)
• Moderately strong stimuli accelerate them
• Strong stimuli act as inhibitors
• The strongest stimuli suspend the life functions
Biotherapeutic index: Ordinatio antihomotoxica et materia medica (5th ed.) 2000
17

I.V. Ozone with German
Biologics “Dr. Hans-Henrich Reckeweg formulated Homotoxicology in
1952 to provide a holistic perspective on the synthesis of medical
science.”
“According to Homotoxicology all of those processes,
syndromes, and manifestations which we designate as diseases,
are the expression thereof that the body is combatting poisons
and that it wants to neutralize and excrete these poisons. The
body either wins or loses the fight thereby. Those processes,
which we designate as diseases, are always biological, that is
natural teleological processes, which serve poison defense and
detoxification.”
Anti-homotoxic medicine is the connecting link between
allopathic medicine and homeopathy.
Biotherapeutic index: Ordinatio antihomotoxica et materia medica (5th ed.). 2000
18

I.V. Ozone with German Biologics • Homotoxins are chemical, biochemical and non-material influences on the
physical/psyche which can cause ill health in humans. Homotoxins can come from the exterior (exogenic) or originate in the body (endogenic).
• Homotoxons are chemical reaction products from compounds of homotoxins with each other or with other substances (products of metabolism) which neutralize the poisonous property of the homotoxins. Liver cells work to neutralize homotoxins and metabolic waste in an effort to detoxify the organism.
• Retoxins are homotoxins with endogenic substances which cannot be eliminated via excretion or irritation and are designated as “residual poisons” or retoxins. One example in the non-enzymatic glucosilization of tissues and cell surfaces in glucose excess or latent diabetes mellitus.
• Homotoxicosis is a non-physiological condition which arises after the reaction of a homotoxins on cells or in tissues. Homotoxicosis presents after humoral or cellular appearance and is followed by morphological changes on the tissues. Homotoxicosis is triggered by a homotoxin and this leads to defensive measures of the organism whose goal is to eliminate the homotoxins and restore the physiological homeostasis when possible.
• Ground Regulation System is composed of the ground substance plus cellular, humoral and nervous components. Ground substance or extracellular matrix is formed of highly polymerized sugars (proteoglycans and glycosaminoglycans) plus structural and meshing glycoproteins.
Biotherapeutic index: Ordinatio antihomotoxica et materia medica (5th ed.). 2000
19

Biotherapeutic index: Ordinatio antihomotoxica et materia medica (5th ed.). 2000
20

Phase Theory• Humoral Phases
1. Excretion Phase – This phase contains manifestations of increased physiological excretion mechanisms.
2. Reaction Phase – Illnesses of the phase are marked by an exudative inflammation, which enables an
accelerated excretion of toxins from the body.
• The Matrix Phases
1. Deposition Phase – In this phase the excretion mechanisms of the body are overworked and toxins are
deposited in the matrix. This phase often progresses with few symptoms.
2. Impregnation Phase – Diseases in this phase are characterized by the presence of toxins which become a
part of the connective tissue and the matrix, along with changes in the structural components as well as
their functions. The typically increasingly severe symptoms and signs of this phase demonstrate damage
of the organ cells.
• The Cellular Phases
1. Degeneration Phase – During this phase, courses of disease cause serious damage, and destruction of larger
cell groups of an organ takes place
2. Dedifferentiation (neoplasm) Phase – Diseases of this phase are characterized by the development of
undifferentiated, non-specialized cell forms. Malignant diseases stand at the end of this phase.
• Biological Division
1. The boundary between the deposition and impregnation phases, demarcates the pure deposition in the
matrix from the integration of toxins into its structural components. Spontaneous endogenic excretion of
the homotoxins is impeded.
• Vicariation
1. Refers to the transition of the indication signs of an illness within one phase to another organ system, or the
change of the fundamental symptoms and signs into another phase, with or without a change of the organ
system
1. Progressive vicariation: Progressive vicariation refers to an aggravation of the total symptoms and signs of
illness.
2. Regressive vicariation: Regressive vicariation refers to an improvement of the total symptoms and signs of
an illness.
Biotherapeutic index: Ordinatio antihomotoxica et materia medica (5th ed.). 2000
21

The Principles of Action of Anti-
Homotoxic Medicine• The immune system has memory and regulation systems. The
deposition phase and impregnation phase is characterized by
chronic inflammation and auto-aggression. The humoral area
(via immunoglobulins from B-lymphocytes) and the cellular
area (T-cells, granulocytes, macrophages) still counterbalance
each other in this case. A regressive vicariation is still possible
in these matrix phases.
• This is the greatest opportunity for anti-homotoxic medicine.
• Low dose antigen reactions from D1 to D12 create the
bystander effect. Higher potencies, trace elements and
intermediary catalysts stimulates ground regulation.
Biotherapeutic index: Ordinatio antihomotoxica et materia medica (5th ed.). 2000
22

The Ground Regulation
Every organism requires energy to maintain its vital functions and must be continuously fed by the metabolism. Disorders of energy metabolism impair the energy supply which is controlled by the endogenic regulation. An energetically open system needs suitable energy and unsuitable energy must be evacuated. All reactions of the organism proceed at relatively low temperatures and must be accelerated by catalysts. The prerequisite for an effective catalyst is a suitable substrate between and in the cells. Extracellular is located in front of the cells. Cells can only react as they have been informed via the extracellular space. The dynamic structure of the extracellular space and its ground regulation forms in all cells and cell groups. This has a decisive impact on the effectiveness of extracellular and intracellular catalysts. This creates a molecular sieve of matrix components like highly polymerized PG/GAGs, structural proteins (collagen, elastin) and meshing glycoproteins (fibronectin). The ground substance is connected to the endocrine system via the capillary system and via the axons to the central nervous system. The fibroblast is the metabolically active centers.
Biotherapeutic index: Ordinatio antihomotoxica et materia medica (5th ed.). 2000
23

The Ground Regulation
• The connection to the central nervous system is conducted via the autonomic nerve fibers that end in the matrix. The connection to the system of endocrine glands, (pituitary, thyroid, suprarenal glands) are conducted via the capillary system which permeates the matrix. Both systems are connected to each other in the brainstem. The matrix is regulated on site and also under the influence of superimposed control areas. The regulation center in the matrix is the fibroblast corresponding to the glial cell in the central nervous system. It reacts to all incoming information (hormones, neural substances, metabolites, catabolites, pH value changes, etc. ) with a synthesis of bad information (alternative facts). Every surplus or deficit can lead in certain circumstance to detrimental consequences for the total system depending on individually on a circulus vitiosus or viscous circle.
• Connective properties of the PG/GAGs are sieve-like and the matrix can develop latent tissue acidity, increase of free radicals and activation of the proteolytic system turning into a pro-inflammatory situation which can cause damage to all humoral and cellular elements thus progressing to chronic disease states and malignant processes.
Biotherapeutic index: Ordinatio antihomotoxica et materia medica (5th ed.). 2000
24
Homeopathy Hoax or Real?
RESULTS:
• The homeopathy RCT literature grew by 309 records in the 18 years that immediately followed Haidvogl's article, with more than a doubling of the proportion that investigated individualized homeopathy. Discounting one prior publication, the entire systematic review literature on homeopathy RCTs post-dates 1994. A total of 36 condition-specific systematic reviews have been identified in the peer-reviewed literature: 16 of them reported positive, or tentatively positive, conclusions about homeopathy's clinical effectiveness; the other 20 were negative or non-conclusive. Reviews typically have been restricted in the strength of their conclusions by the low quality of the original RCT evidence. Three comprehensive systematic reviews concluded, cautiously, that homeopathy may differ from placebo; a fourth such review reached negative conclusions. A recent high-quality meta-analysis concluded that medicines prescribed in individualized homeopathic treatment may have small, specific, effects.
CONCLUSIONS:
• Despite important growth in research activity since 1994, concerns about study quality limit the interpretation of available RCT data. The question whether homeopathic intervention differs from placebo awaits decisive answer.
Homeopathy. 2015 Oct;104(4):328-32. doi: 10.1016/j.homp.2015.05.003.
25

Homeopathy Adverse Health Affects• Homeopathy has the potential to harm patients and consumers in both
direct and indirect ways. Clinicians should be aware of its risks and
advise their patients accordingly. (Posadzki et al. 2012)
• An audit of the Bristol Homeopathic Hospital among 116 patients
reported that 11% of them experienced AEs, including headaches,
lethargy or vomiting. This percentage figure is difficult to interpret as
the authors categorize diarrhea, eczema, gastrointestinal upset, hair
loss, infections, nausea, migraines, pains, rash, skin irritation, tension
headaches, tiredness/fatigue as ‘homeopathic aggravations’, new
symptoms and/or return of old symptoms. Our own review of the
evidence for or against the existence of homeopathic aggravations
included 24 placebo‐controlled trials reporting aggravations, and we
came to the conclusion that ‘this systematic review does not provide
clear evidence that homeopathic aggravations exist’ (Posadzki et al.
2012)
26

Homeopathy Misreported• Detailed examination of the 37 original articles cited by Posadzki and colleagues has uncovered
numerous striking errors. As there are too many to mention in this comment, we draw your attention to just some examples of our key concerns below.
• In reporting on four cases of AEs published by Ibsen et al., Posadzki and colleagues categorize these as ‘likely’ to have been caused by homeopathy. However, there is actually no reference made to homeopathy whatsoever in the Ibsen article. The word ‘homeopathy’ only appeared in the English abstract as an incorrect translation of the term ‘alternative treatment’.
• Of even greater concern is the reporting of a case report by Geukens of cure by homeopathy, which has been reported by Posadzki et al. as a case of homeopathy causing ‘heart disease and bladder cancer’. In actual fact, the patient was cured from his initial symptoms of vertigo and heart disease using homeopathic medicines; he then presented 7 years later with cancer of the bladder. It is difficult to see how the causality of the cancer could be attributed to the successful treatment of the heart‐condition. The cancer was subsequently treated using conventional treatment, the side‐effects of which were successfully dealt with using homeopathy. The patient recovered, with no further complaint. How does one end up with causality ‘Almost certain’ for homeopathy in a clear case were homeopathy was instrumental in providing cure? (Posadzki et al. 2012)
Differentiating between ordinary standards of homeopathic care and clinical negligence:
• When assessing the safety of a medical intervention it is usual to differentiate between non‐preventable AEs and those which are preventable with ordinary standards of care i.e. cases of clinical negligence. Posadzki et al. have failed to make any such distinction. The four deaths they report as being caused by homeopathy involve either mis-prescribing of poisonous substances or failure to refer the patient for essential conventional medical treatment. As these cases contravene what is considered standard homeopathic care, they should be classified as cases of clinical negligence. (Posadzki et al. 2012) 27

Inaccuracies
• The authors have also shown a lack of consistency in their decision‐making
processes regarding inclusion/exclusion of data. For example, 1070 of the
1159 cases identified by Posadzki et al. come from a single article reporting
calls to a toxicological information center. These comprised calls for
information (e.g. following inadvertent ingestion of a homeopathic remedy)
some of which lead to actual AE cases with a maximum severity of ‘minor’
or ‘mild’. As the article by Zuzak et al. presented 2143 similar cases, it is
unclear why these were omitted. (Tournier et al. 2013)
• Sadly the quality of this review by Posadzki et al. falls short of this standard
by such a large margin, that at best the authors’ results are unreliable, and at
worst we must consider whether the degree of inaccuracy is such that
retraction of this article becomes necessary to preserve the quality of the
peer‐reviewed literature. (Tournier et al. 2013)
28

Adverse Health Effects of
Aluminum • Induced formation of oxygen radicals – oxidative damage
• Impaired bone mineralization – Osteomalacia
• Delayed neurological development – Encephalopathy/ Dementia/ Alzheimer’s
• Reduces erythrocyte lifespan and interferes with hemoglobin synthesis – microcytic hypochromic anemia
• Contact allergy
• Adverse reactions to vaccines with Al adjuvants
• Pneumoconiosis after long-term inhalation – (potroom asthma)
• Can effect neurologic, hematopoietic, skeletal, respiratory, gastrointestinal and immunologic systems
• Increased risk of lung and bladder cancer
(Willhite 2014)29

Mechanisms of Action -
Aluminum Air - Water – Food
Low Daily Doses – Systemic Intoxication
• “Mitochondrial metabolism is the main site of the toxicological action of Al due to interference with “Fe-dependent redox sensitive enzymes in the tricarboxylic acid (TCA) cycle and oxidative phosphorylation”
• “Cellular metabolic shift from oxidative ATP production to anaerobic glycolysis –resulting in increased α-ketoglutarate and succinate and reduced L-carnitine”
• “Depletion of mitochondrial iron, H2O2, O2 and OH”
• “Reduced fatty acid β – Oxidation, Increased peroxidation”
• “Al +3 binds with phospholipids in cell membrane altering membrane fluid dynamics through peroxidation”
• “Stress in endoplasmic reticulum leading to cytochrome c release from mitochondria and activation of apoptotic demise”
• “Genomic Effect increased p53 followed by Bax translocation leading to DNA fragmentation at the lowest Al +3 Concentration”
• “Decreases antioxidant enzyme – G-6-PDH, SOD and catalase”
(Willhite 2014)
30
Adverse Health Effects of Manganese and CopperManganese:• Neurotoxicity – Brain is main target of Mn intoxication
• Tends to accumulate in the liver, pancreas, bone, kidney and brain
• MOA - oxidative stress, mitochondrial dysfunction, protein misfolding, endoplasmic reticulum stress, autophagy dysregulation, apoptosis and disruption of other metal homeostasis
• Link to Parkinson’s
• Interferes with absorption of dietary iron
• Impairs activity of copper metallo-enzymes
• Impaired thiamin B1 metabolism
(Willhite 2014)
Copper:• Neurotoxicity
• “Cu-induced oxidative damage has been implicated in disorders associated with abnormal Cu metabolism and neurodegenerative changes.” (Gaetke, 2003)
• Associated with Wilson’s disease, liver dysfunction, tremors, involuntary movements, muscle stiffness, muscle spasms, myopathy, gait abnormalities, mood disorders, memory deterioration
• Associated with Alzheimer’s and Parkinson’s
(Gaetke 2003)
31

Elevated Aluminum, Manganese
and Copper - Case I: J.E. • 42 y.o. female PTC with 10 year hx of Lyme dz and co-infections. 10
years ago, pt. complained of hot flashes, rashes, clumsiness, loss of balance, vision changes, optic neuritis, gained 70 pounds and went from fully functional 3 time Emmy winner to barely being able to get out of bed.
• Previous labs revealed the following: June 2017
• Platelet count 557 x 10 RR: 144-400
• CRP 1.3 RR: <0.5
• ESR 56 RR: <26
• Ferritin 6 RR: 10-291, Iron, %Sat. 6% RR:20-55%, TIBC 531 RR: 228-428
• Histone Ab IgG 1.0 units RR: 0.0-0.9
• Q Fever Ab+, Lyme Ab+ C6 with bands 18 & 4, Bartonella Ab+, Ehrlichiosis Ab+, Babesia Ab+, Pneumococcal Ab+ and low for Type 4,5,8,9,12,14,19,22,26,34,43,51,54,68,70
• Immunoglobuline G 548RR: 700-1600 Subclass 1 204 RR: 422-1292 32

Elevated Aluminum, Manganese and Copper Cont’d. • Imaging: Stable fatty infiltration of liver, small to moderate size hiatal hernia, CT
of chest – small patch of faint ground glass density and nodularity in the medial segment of the right middle lobe, focal bronchial thickening, possibility of distal bronchial or bronchiolar plugging
• Brain Imaging: Moderate nonspecific white matter signal abnormality involving the periventricular white matter and subcortical white matter DDX: Demyelinating disease and microvascular disease.
• Following contrast: punctate area of enhancement in the right interior basal ganglia in pencaudate location measuring 3mm on axial image.
• PTC with sxs: Fatigue, muscle weakness, H/A (migraine), blurry vision, SOB, asthma, heart palpitations, heartburn/reflux, low grade nausea, abdominal pain, PMS, no libido, joint pain/stiffness, pustular psoriasis on hands and feet with weeping and seeping, restless leg, chronic iron deficiency anemia, numbness/tingling, brain fog, memory issues, balance issues, vertigo, depression/anxiety, excessive stress, hot/cold intolerance, hypothyroid, excessive sweating, pre-diabetes, MCS
• PE: confirmed above, noted continuous eye flutters with Pulse Ox: 94, Ht: 5.1 Wt: 196
• Current Meds: Synthyroid, Pulmicort, Xanax ER/Regular, Celexa, Trinessa (BC), Trofranil, Multivitamin, Vitamin C, Pro Air Albuterol Rescue Inhaler, Prevacid, Zantac, Gaviscon (Ask me for dosages)
33

Elevated Aluminum, Manganese and Copper Cont’d. • Assessment: Persistent Lyme/ Co-Infections, Chronic Asthma,
GERD, Fatty Liver, Oxygen Deficiency, Generalized Pain,
Cognitive Impairment, Leaky Gut, Immune Suppression,
Seasonal Allergies, Hypothyroid, Iron Deficiency Anemia,
Metabolic Syndrome, Constipation
• Plan: Clean up Diet, Rebuild immune system with gut repair
protocol, Low dose low Gamma I.V. Ozone with added Rx
Homeopathics, Lab Testing, Advance to Ozone Chelation
(Level 5)
34

Elevated Aluminum, Manganese
& Copper in Serum– Case I: J.E.• Empire City Labs– Significant Findings – November 2017
• CBC w Diff
• WBC 11.9 RR:4.0-11.0, RDWCV 15.8 RR: 11.0-15.0, NE# 7.58 RR: 1.40-6.51, IG# 0.04 RR: 0.00-0.03
• %CD8 -/ CD57+ Lymphs 1.9 RR: 2.0-17.0
• Alkaline Phosphatase, ALP 134 RR: 45-129
• Cardiac IQ
• Cholesterol 213 RR: <200, Triglycerides 190 RR: <150, LDL Direct Cholesterol 149.9 RR:<130, LP(a) 139.71 RR: <30, LDL Pattern B
• CRP, High Sensitivity 22.67 RR: <3
• Hemoglobin A1C 6.1 RR: 4.2-5.6
• Pregnenolone <5 RR: 22-237, SHBG 245.5 RR: 18.0-144.0, Dihydrotestosterone <5 RR: 5-46, ACTH, Plasma <5 RR: 6-50
• IGF - 1 86 RR: 101-267
• TNF- Alpha, Highly Sensitive 0.29 RR: 0.56-1.40
• Complement C-3 245 RR: 90-170, Complement C-4 51 RR: 12-36, C3A Level 3115 RR: 0-780
• HH6 1:10 Past Infection, M. Pneumonia 1.11 Past Infection
• Vascular Endothelial GF 511 RR: 31-86
• Food Allergies IgE: Class I RR: 0-10 – Cheese Mold 0.11, Egg White 0.33, Corn 0.14, Milk 0.24, Sesame Seed 0.18
• Aluminum Serum 7 RR: <7, Copper 247 RR: 70- 175, Manganese 1.5 RR: <1.2
• Vitamin C <0.1 RR:0.2-1.535
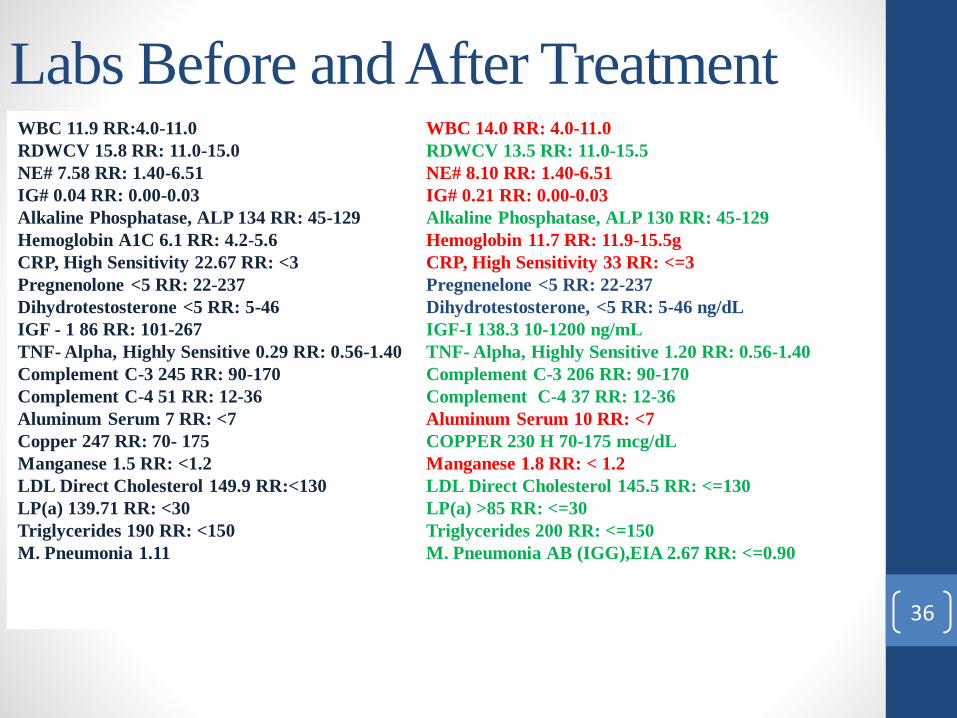
Labs Before and After Treatment WBC 11.9 RR:4.0-11.0
RDWCV 15.8 RR: 11.0-15.0
NE# 7.58 RR: 1.40-6.51
IG# 0.04 RR: 0.00-0.03
Alkaline Phosphatase, ALP 134 RR: 45-129
Hemoglobin A1C 6.1 RR: 4.2-5.6
CRP, High Sensitivity 22.67 RR: <3
Pregnenolone <5 RR: 22-237
Dihydrotestosterone <5 RR: 5-46
IGF - 1 86 RR: 101-267
TNF- Alpha, Highly Sensitive 0.29 RR: 0.56-1.40
Complement C-3 245 RR: 90-170
Complement C-4 51 RR: 12-36
Aluminum Serum 7 RR: <7
Copper 247 RR: 70- 175
Manganese 1.5 RR: <1.2
LDL Direct Cholesterol 149.9 RR:<130
LP(a) 139.71 RR: <30
Triglycerides 190 RR: <150
M. Pneumonia 1.11
WBC 14.0 RR: 4.0-11.0
RDWCV 13.5 RR: 11.0-15.5
NE# 8.10 RR: 1.40-6.51
IG# 0.21 RR: 0.00-0.03
Alkaline Phosphatase, ALP 130 RR: 45-129
Hemoglobin 11.7 RR: 11.9-15.5g
CRP, High Sensitivity 33 RR: <=3
Pregnenelone <5 RR: 22-237
Dihydrotestosterone, <5 RR: 5-46 ng/dL
IGF-I 138.3 10-1200 ng/mL
TNF- Alpha, Highly Sensitive 1.20 RR: 0.56-1.40
Complement C-3 206 RR: 90-170
Complement C-4 37 RR: 12-36
Aluminum Serum 10 RR: <7
COPPER 230 H 70-175 mcg/dL
Manganese 1.8 RR: < 1.2
LDL Direct Cholesterol 145.5 RR: <=130
LP(a) >85 RR: <=30
Triglycerides 200 RR: <=150
M. Pneumonia AB (IGG),EIA 2.67 RR: <=0.90
36

37
38

39
Carduus marianus
40

Taraxacum officinale
41

Cyclamen europaeum
42
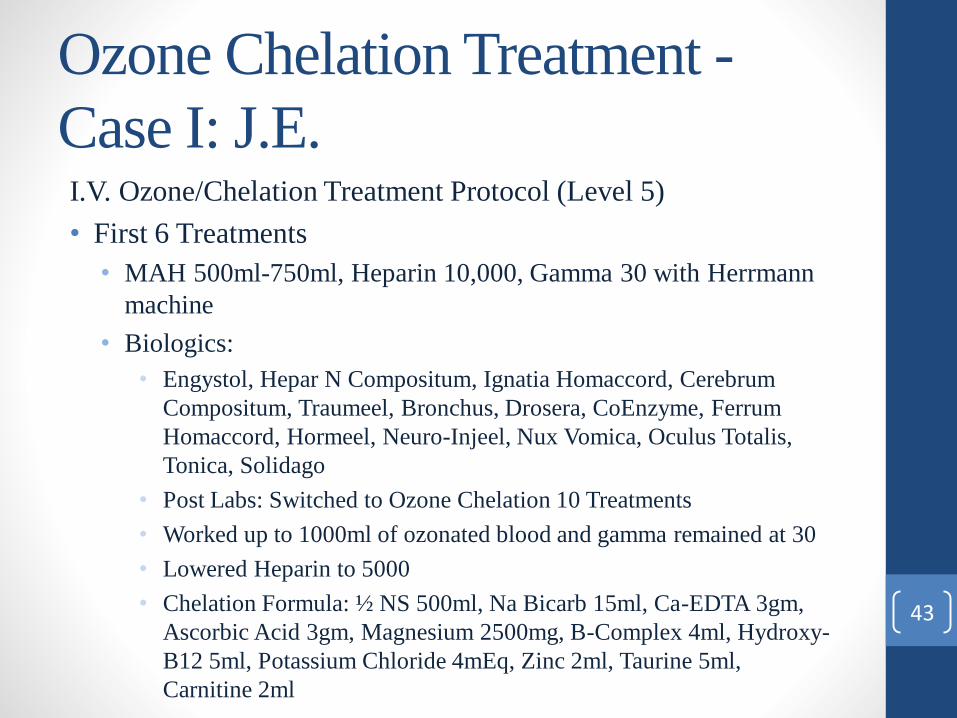
Ozone Chelation Treatment -
Case I: J.E.I.V. Ozone/Chelation Treatment Protocol (Level 5)
• First 6 Treatments
• MAH 500ml-750ml, Heparin 10,000, Gamma 30 with Herrmann
machine
• Biologics:
• Engystol, Hepar N Compositum, Ignatia Homaccord, Cerebrum
Compositum, Traumeel, Bronchus, Drosera, CoEnzyme, Ferrum
Homaccord, Hormeel, Neuro-Injeel, Nux Vomica, Oculus Totalis,
Tonica, Solidago
• Post Labs: Switched to Ozone Chelation 10 Treatments
• Worked up to 1000ml of ozonated blood and gamma remained at 30
• Lowered Heparin to 5000
• Chelation Formula: ½ NS 500ml, Na Bicarb 15ml, Ca-EDTA 3gm,
Ascorbic Acid 3gm, Magnesium 2500mg, B-Complex 4ml, Hydroxy-
B12 5ml, Potassium Chloride 4mEq, Zinc 2ml, Taurine 5ml,
Carnitine 2ml
43
Patient Improvements –
Case I: J.E• Energy , sleep, skin, cognition, digestion, mood, feeling more
in control, more stamina
• Even though this is a documented clinical failure the patient
did receive benefits from ozone chelation
44

Aquilegia vulgaris
45
Adverse Health Effects of Lead• Hypertension
• Peripheral Arterial Disease
• Coronary Heart Disease
• Increased risk of stroke
• Left ventricular hypertrophy
• Cardiac Rhythm Alteration –
AFIB
• Cognitive Degeneration
• Renal Disease
• Mood Disorders (Depression
etc.)
• Systemic Inflammation
• Arthritis
• Associated with ADD and
ADHD
• Impaired Dental Health
• Delayed sexual maturation
• Probably Carcinogenic
• Reduced Fertility
• Nervous System Dysfunction
• Linked to ALS
• Violence and Aggression
Flora, 2012
46

Mechanisms of Action - Lead
• Oxidative Stress
• “Ionic mechanism of action for lead mainly arises due to its ability to substitute other bivalent cations like Ca2+, Mg2+, Fe2+ and monovalent cations like Na+ (though bivalent cations are more readily substituted), affecting various fundamental biological processes of the body (Lidsky & Schneider, 2003). Significant effects have been found on various fundamental cellular processes like intra and intercellular signaling, cell adhesion, protein folding and maturation, apoptosis, ionic transportation, enzyme regulation, release of neurotransmitters, etc. (Garza et al., 2006)”
- Flora, 2012
• “Lead, even in picomolar concentration, can replace calcium, thereby affecting key neurotransmitters like protein kinase C, which regulates long term neural excitation and memory storage. It also affects the sodium ion concentration, which is responsible for numerous vital biological activities like generation of action potentials in the excitatory tissues for the purpose of cell to cell communication, uptake of neurotransmitters (choline, dopamine and GABA) and regulation of uptake and retention of calcium by synaptosomes. This interaction between lead and sodium seriously impairs the normal functioning of the aforementioned sodium dependent processes (Bressler et al., 1999).”
- Flora, 2012 47

Elevated Lead in Tissue Storage
–Case II: S.J. • 54 y.o. male PTC with R knee and hip pain, hx of Lyme, chronic gastrointestinal
upset, headaches (migraines, cluster and tension), muscle spasms, histamine dumping syndrome, irritable bowel with mixed diarrhea/constipation, “aging too quickly”, chronic cold sores, chronic cervical pain/subluxation, hx of HSV1 and 2, joint pain, chronic fatigue and unconfirmed low T.
• Started treatment in July 2016 with Prolozone for R knee and R hip, I.V. Meyer’s with Glutathione (1000mg), 10 pass MAH(2000-2500 ozonated blood) Gamma 70 Heparin 10,000u with Herrmann x 1 session per week for 7 weeks. (Level 5)
• Added Biologics: Traumeel, CoEnzyme, Engystol, Cerebrum Compositum, Testis Compositum, Lymphomyosot, Galium, Glandula Thymi, Herpes Nosode, Hepeel, Spascupreel, Spigelon, Chelidonium, Cimicifuga, Vitamin C, Coloncynthis, NuxVomica, Discus Compositum, Neuralgo-Rheum, Medorrhinum, Injeel, AcidumFumaricum, Acidum DL-Malicum, Zeel, Glyoxal, Ubichinon, Colon-Suis, Duodenum-Suis, ATP, Ignatia-Injeel, Graphites, Mucosa Compositum
• Started with Gut Repair Protocol, Liver support, Joint support, Immune support, Natural support for food cravings (Level 5)
• Later added Cardiac support48

Vitex agnus-castus
49

Conium maculatum
50

Damiana
51

Elevated Lead in Tissue Storage
–Case II: S.J. • Empire City Labs– Significant Findings
• NE#% 76.50 RR: 39-71
• LY% 15 RR: 19-53
• Abs. CD8-CD57+ Lymphs 46 RR: 60-360
• LDL Peak Size 216.8 RR:>218
• Homocysteine 16.4 RR: 3.7-13.9
• Cholesterol 161.7 RR:<130
• Pregnenolone 11 RR: 22-237
• Progesterone 0.21 RR: 0.28-1.22
• ACTH
• Plasma <5 RR: 6-50
• TNF-Alpha 2.25 RR 0.56-1.40
• ANA screen 0.9 RR: 0.0-0.7
• C3A Level 1904 RR: 0-780
• EBV IGG 226.0 RR: <18.0
• HSV-1 IGG 31.2 RR: <0.9
• HSV-2 IGG RR: 9.5
• HH 6 AB IGG 1:40 RR:<1.20
• M. Pneum. IGG 3.46 RR:<0.9
• VEGF Vascular Endothelial GF 194 RR: 31-86
• Lead in Serum 1.57 RR: 0-5
• Aluminum 5 RR: <7
• Cadmium 0.52 RR:1.7ug/L or less for non-smokers
• Mercury 0.79 RR: 0-10
• Arsenic 1.00 RR: 0-23
• Copper 91 RR: 70-175
• Vitamin C 0.1 RR: 0.2 – 1.5
• Vitamin D 25-Hydroxy 27.73 RR: 33.0-100.00
• LDL Pattern B
• LDL Small 246 RR: <161
• LDL Medium 331 RR: <200
• HDL Large 4410 RR: >9387
• Omega-3 1.5 RR:>3.2
52

53

54
55

Urine Toxic Metals Provocative
Challenge – Case II: S.J. • EDTA 3000mg
• DMSA 3000mg
• 6 Hour Urine Challenge
• Results:
• Al 48 RR: <25
• Cadmium 1.7 RR: <0.8
• Cesium 21 RR: <9
• Lead 40 RR:<2
• Mercury 2.9 RR: <3
• Nickel 11 RR: <8
• Thallium 0.7 RR: <0.5
• Creatinine 26.5 RR: 35-240 mg/dL56

Ozone Chelation Treatment –
Case II: S.J.Follow up Results: Urine Toxic Metals
• Al 9.3 RR: <25
• Cadmium 0.4 RR: 0.8
• Cesium 7.1 RR: <9
• Lead 5.1 RR: <2
• Mercury : Undetected
• Nickel 4.2 RR: <8
• Thallium 0.1 RR: <0.5
• Creatinine 52.5 RR: 35-240
57
Ozone Chelation Treatment –
Case II: S.J.• Switched to Ozone Chelation post results
• 10 Pass MAH followed by Chelation protocol
• EDTA 3gm as in first case plus Zinc 3ml, Taurine 5ml,
Carnitine 2-3ml x 12 tx: One tx per month as Pt. could not
come weekly due to distance
• Tx #10 Pt. had eye infection
• Used an eye cup to insufflate direct ozone for 1 minute into R eye
• Applied Ozone cream on affected eyelid as well
Level 558

Patient Improvements – Case II:
S.J. • Patient has improved daily function
• Improved gastrointestinal system
• Not as sensitive to foods
• Significant reduction in headaches
• Significant reduction in systemic inflammation
• Feels younger
• Able to do 100 mile bike rides
• No R knee or R hip complaints
• Brain fog cleared/ Cognition improved
• Improved coping mechanisms
• Great Sense of Humor! 59

Arnica montana
60

Calendula officinalis
61

Elevated Aluminum, Mixed Connective Tissue Disease & Oxygen Deficiency – Case III S.P.
• 69 y.o female, PTC with HTN, Scoliosis, Mixed Connective Tissue Disease, Metabolic Syndrome, Raynaud’s, Rosacea, Missing Fat Pad in Left Foot, Poor Methylation and Oxygen Deficiency
• Current Medications: Chlorthalidone 25mg/day, Labetalol 50mg twice/day, Irbesartan 150mg/day
• Started treatment 4/23/2018, MAH blood 650ml, ozone gamma 55, heparin u 5000
• German Biologics: ATP, Glyoxal, Ubichinon
• 3rd – 9th Session: Added Engystol
• Recommended Endoscopy to r/o H. Pylori
• Recommended Ketogenic Diet
• Oral Nutraceuticals: Resveratrol, Alpha-Lipoic Acid, Biotin, Arginine, Alpha-Ketoglutarate, Whey Peptide, Quercetin, L-Glutamic Acid, Betaine HCI, Pepsin, Gentian
• 6/12/2018 – Added Nutraceuticals Cardio Protection, 5-MTHFR, Liver Protection, Andrographis
• Recommended Coronary Calcium Artery Score62

Elevated Aluminum, Mixed Connective Tissue Disease & Oxygen Deficiency – Case III S.P.
• 10th Session – Started Ozone Chelation
• 500ml of half normal saline, NA bicarb 10ml, Ca-EDTA 1gm, Mg Sulfate 2500mg, B Complex 1ml, Dexpanthenol 4ml, Pyridoxine 2ml, Hydroxy – B12 5mg, Potassium Chloride 4 mEq, Zinc 1ml, Carnitine 1ml, Taurine 3ml
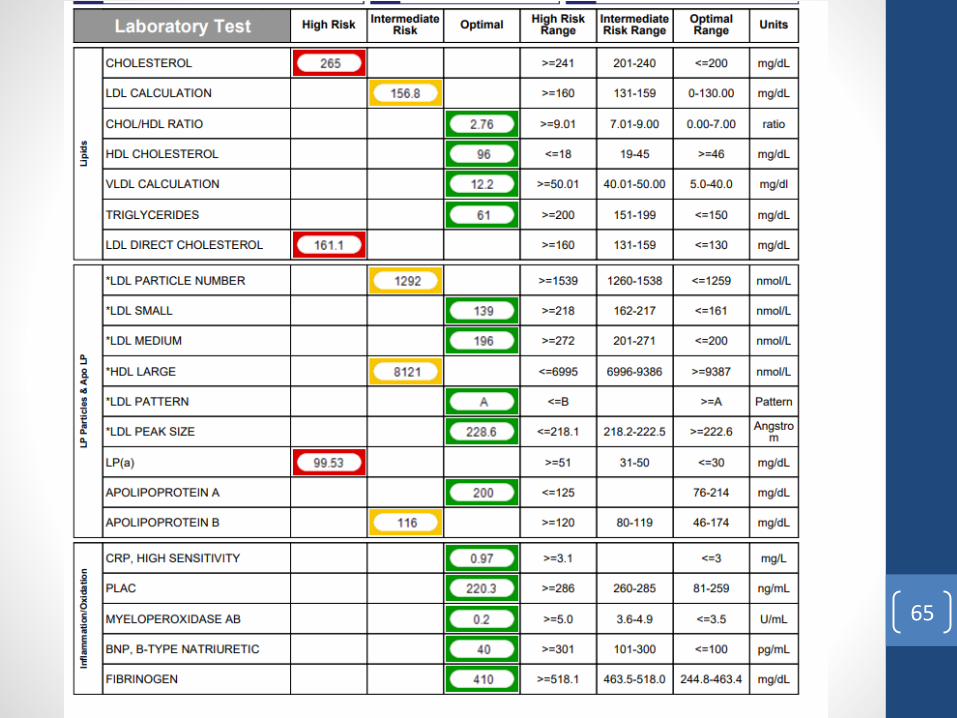
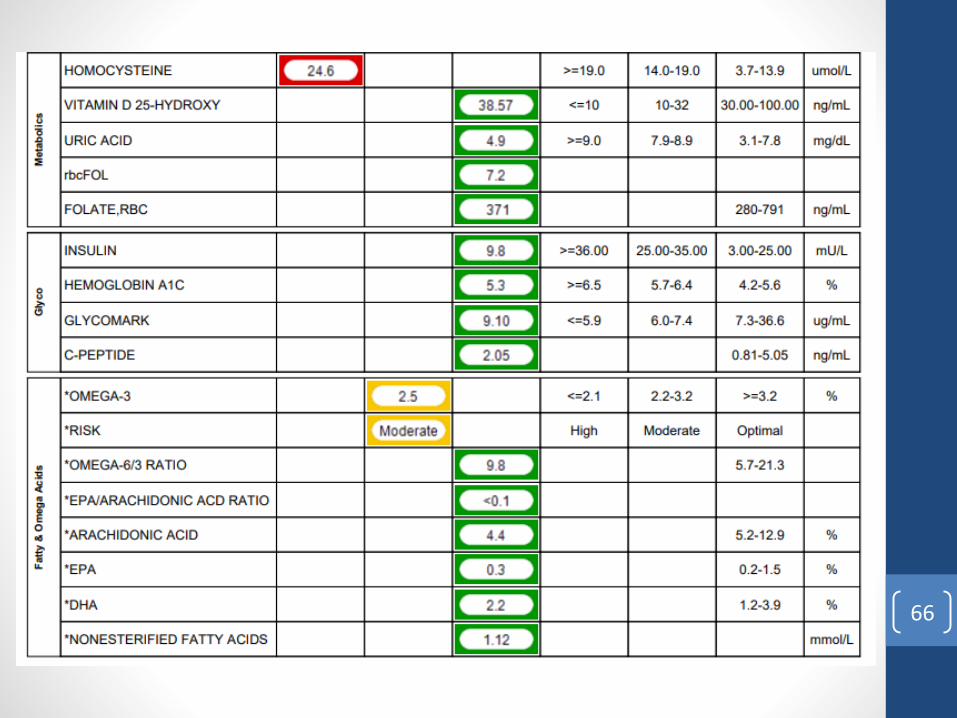
• Empire City Labs – 6/5/2018 – Abnormals
• Blood Type: B+
• ESR 36 H <=30 mm/hr
• ALKALINE PHOSPHATASE, ALP 163 H 45-129 U/L
• MANGANESE,SERUM 1.2 H < 1.2 mcg/L
• HOMOCYSTEINE 24.6 H 3.7-13.9 umol/L
• CHOLESTEROL 265 H <=200 mg/dL
• LDL DIRECT CHOLESTEROL 161.1 H <=130 mg/dL
• LP(a) 99.53 H <=30 mg/dL
• T3 REVERSE, LC/MS/MS 26 H 8-25 ng/dL
• PREGNENOLONE,LC/MS/MS
• SHBG 79 H 14-73 nmol/L
• DIHYDROTESTOSTERON,LCMSMS
• TNF-ALPHA,HIGHLY SENSITIVE 2.42 H 0.56-1.40 pg/mL
• ANA Screen(Symphony) 0.8 H 0-0.7 Ratio63

• EPSTEIN-BARR VIRUS EA(D)IGG 72.0 H <=9.0 U/mL
• EPSTEIN-BARR VIRUS IGG >750.0 H <=18.0 U/mL
• EBV NUCLEAR ANTIGEN,AB(IGG) 360.0 H <=18.0 U/mL
• LYME DISEASE (IGG,IGM) WB
• 41 kDa (IGG) BAND Reactive Nonreactive 39 kDa (IGG) BAND Reactive Nonreactive
• HERPES SIMPLEX VIRUS-1 IGG 58.3 H <=0.9 INDEX
• HERPESVIRUS 6 AB IGG,IFA 1:80 H
• CYTOMEGALOVIR, CMV AB IGG >10 H 0.0-0.6 U/mL
• M.PNEUMONIAE AB (IGG),EIA 2.99 H <=0.90
• VASCULAR ENDOTHELIAL GF 518 H 31-86 pg/mL
• ALUMINUM 17 H < 7 mcg/L
• BIOTIN (VITAMIN B7) >3600.0 H 221.0- 3004.0 pg/mL
64
65
66

67

The Source of Aluminum
68

September 2018 Aluminum in serum zero.69
Case V: P.R.
• 52 y.o male PTC with HPV related condyloma acuminatum
(AIN 1) had surgery to remove warts saw Dr. Robins NYC
four times for DIV 50 gamma 30-45cc
• Supplements: Vitamin C and probiotics
• Patient wanted comprehensive systemic treatment to prevent
recurrence
• Recommended weekly MAH treatment with German Biologic
and Immune Support
70

Treatment - Case V: P.R.
• Patient did 10 Pass MAH gamma 70 first treatment with Thuja
• Treatments 2-16 multi-pass 650ml- 1000ml with Thuja
• Patient cleaned diet, exercises daily, always in good mood and
enjoys his life
• No Recurrence
71

72

Case VI: D.C.
• 60 y.o. female PTC with HSV II (dx 4 y.o.), HPV (LEEP
1991), depression d/t dx, hypothyroidism, adrenal
hypofunction, Transphenoidal Rathke’s Cyst removal 12/09
• Current Meds: Hydrocortisone, Synthroid, Valtrex, Premarin,
Vitamin D, Calcium
• Supplements: Propolis, Cordyceps, Lysine, Flax Seed Oil,
Liposomal Vitamin C, Olive Leaf Extract, Immulox,
Monolaurin, Argentyn 23, CoQ 10, Pekana Desbro
Comprehensive Detox, Methyl Protect, B12, Immunotix
• Family Hx: Father- deceased, heart event 53 y.o., Mother-
deceased, Parkinson’s 87 y.o.
73

Treatment- Case VI: D.C.
• 10 Sessions: 10 pass MAH 2000-2500ml gamma 70 with German Biologics• Herpes Simplex Nosode
• Injeel
• Neuro-injeel
• Cerebrum Compositum
• Lymphomyosot
• Traumeel
• Galium
• Glandula – Thymi
• Glandula – Thyroidea
• Chelidonium
• Engystol
• Hepeel
• Hepar Suis – Injeel
• Glyoxal Compositum
• Ubichinon Compositum
74
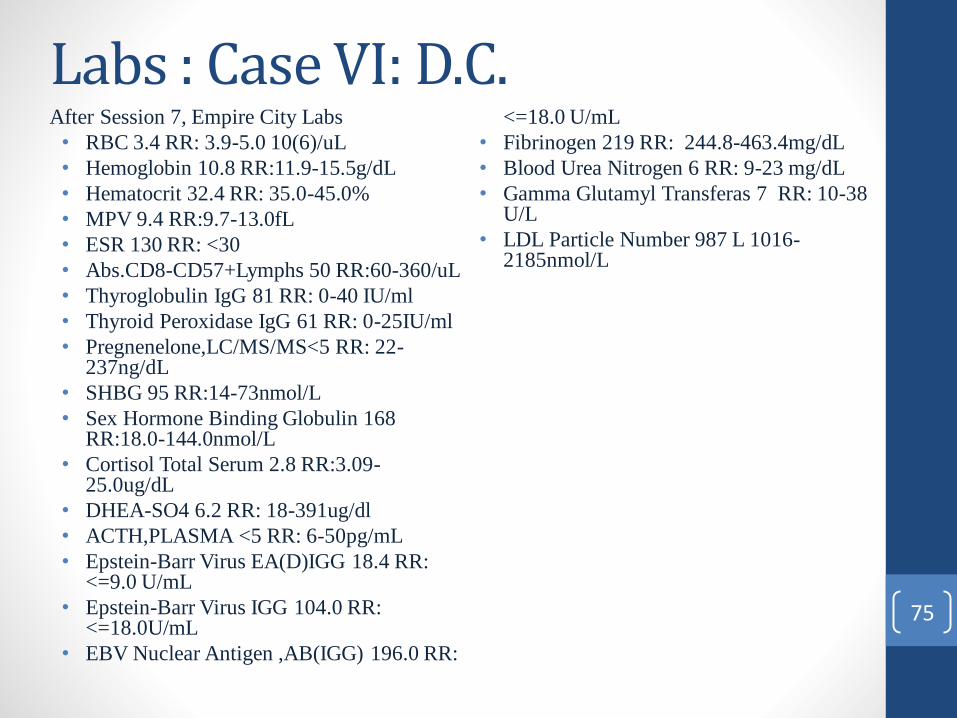
Labs : Case VI: D.C.After Session 7, Empire City Labs
• RBC 3.4 RR: 3.9-5.0 10(6)/uL
• Hemoglobin 10.8 RR:11.9-15.5g/dL
• Hematocrit 32.4 RR: 35.0-45.0%
• MPV 9.4 RR:9.7-13.0fL
• ESR 130 RR: <30
• Abs.CD8-CD57+Lymphs 50 RR:60-360/uL
• Thyroglobulin IgG 81 RR: 0-40 IU/ml
• Thyroid Peroxidase IgG 61 RR: 0-25IU/ml
• Pregnenelone,LC/MS/MS<5 RR: 22-237ng/dL
• SHBG 95 RR:14-73nmol/L
• Sex Hormone Binding Globulin 168 RR:18.0-144.0nmol/L
• Cortisol Total Serum 2.8 RR:3.09-25.0ug/dL
• DHEA-SO4 6.2 RR: 18-391ug/dl
• ACTH,PLASMA <5 RR: 6-50pg/mL
• Epstein-Barr Virus EA(D)IGG 18.4 RR: <=9.0 U/mL
• Epstein-Barr Virus IGG 104.0 RR: <=18.0U/mL
• EBV Nuclear Antigen ,AB(IGG) 196.0 RR:
<=18.0 U/mL
• Fibrinogen 219 RR: 244.8-463.4mg/dL
• Blood Urea Nitrogen 6 RR: 9-23 mg/dL
• Gamma Glutamyl Transferas 7 RR: 10-38 U/L
• LDL Particle Number 987 L 1016-2185nmol/L
75

Labs: Case VI: D.C. Cont’d.
• Epstein-Barr Virus IGG 104.0 RR: <=18.0U/mL
• EBV Nuclear Antigen ,AB(IGG) 196.0 RR: <=18.0 U/mL
• Fibrinogen 219 RR: 244.8-463.4mg/dL
• Blood Urea Nitrogen 6 RR: 9-23 mg/dL
• Gamma Glutamyl Transferas 7 RR: 10-38 U/L
• LDL Particle Number 987 L 1016-2185nmol/L
• HDL LARGE 4048 RR: 5038-17886 nmol/L
• Testosterone Bioavailable 0.4 RR:0.5-8.5 ng/dL
• Dihydrotestosterone,LCMSMS
<5 RR: 5-46ng/dL
• DHEA-SO4 9 RR: 18-391 ug/dl
• IGF-1 71 L 81-225 ng/mL
• Complement C-3 88 RR: 90-170mg/dl
• Herpes Simplex Virus-2 IgG 1.2 RR <=0.9
• Herpes Virus 6 AB IGG,IFA 1:40
• M. Pneumoniae AB (IGG),EIA 3.01 RR: <=0.90
• Vitamin B12 2343 RR: 211-911pg/mLCoenzymeE Q10 2.21 RR: 0.44-1.64mg/L
• RMSF IGG Detected76

77

Passiflora
78

Post Lab Recommendations – Case VI: D.C. • Liver Support
• DHEA
• IG 26 DF
• Pregnenelone
• Adrenal Support
79

Patient Progress- Case VI: D.C
• Will switch to Naturethroid
• Feeling much better, no suicidal ideation, has more energy,
learned BOD breathing dynamic, better color, improved
digestion, no outbreaks, feels stronger
80

Chelidonium
81

Treatment Failures
82

Case III: J.P.• 57 y.o. female massage therapist PTC with stage 2-3 infiltrating
ductal carcinoma poorly differentiated hypoechoic nodule with focal
apocrine features 2.1 cm ER+ PR+ HER- breast cancer. Diagnosed
April 2015. Lumpectomy July 2015. Suggested mastectomy. August
2016 Dx invasive ductal. Patient decided not to do Tamoxifen 1 year
later recurrence tumor behind right nipple and positive lymph nodes.
• Family Hx: Mother – deceased colon cancer 86 y.o., Father –
deceased heart attack 59 y.o, Sister – deceased Colon Cancer 55 y.o,
Brother - deceased Melanoma 39 y.o.
83
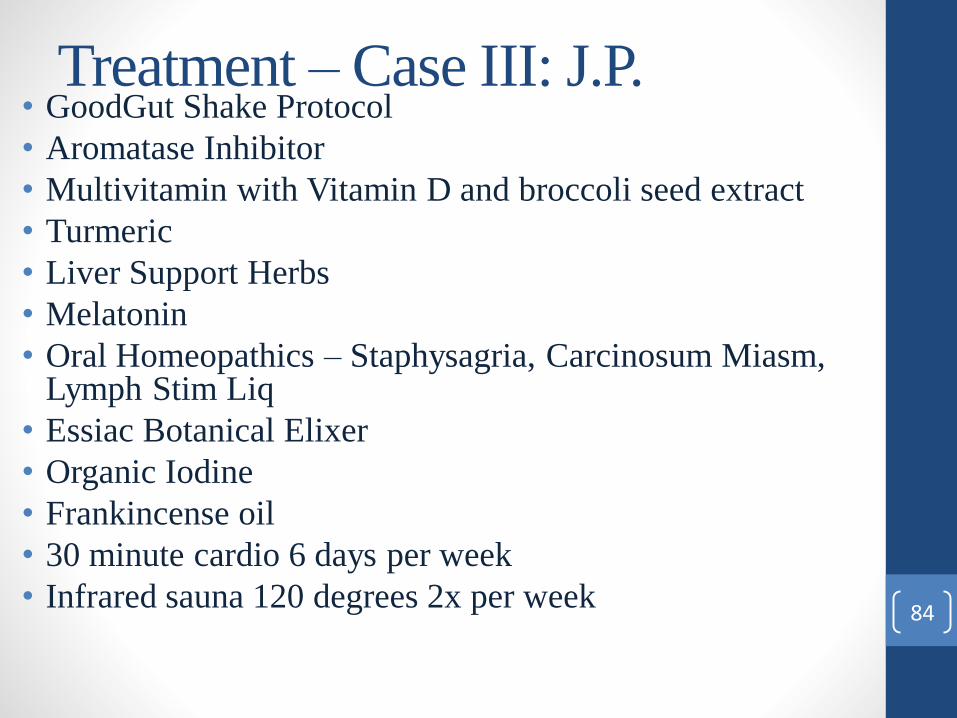
Treatment – Case III: J.P.• GoodGut Shake Protocol
• Aromatase Inhibitor
• Multivitamin with Vitamin D and broccoli seed extract
• Turmeric
• Liver Support Herbs
• Melatonin
• Oral Homeopathics – Staphysagria, Carcinosum Miasm, Lymph Stim Liq
• Essiac Botanical Elixer
• Organic Iodine
• Frankincense oil
• 30 minute cardio 6 days per week
• Infrared sauna 120 degrees 2x per week84

Treatment – Case III: J.P.• 4 – 10 Pass MAH treatments Gamma 70 with German Biologics in 2017
• Tonsilla
• Chelidonium
• Ignatia
• Carcinoma-Coli
• Ubichinon
• Galium
• Hepar comp
• Hormeel
• Lymphomyosot
• Glandula lymphatica
• Selenium
• After 3rd MAH treatment we added in Scorpio Venom for 250 days – 5ml per day
• Patient moved and contracted sinus infection which turned into Pneumonia as evidenced by X-Ray on right lung
• PET Scan revealed metastatic tumors in lymphatic chain – no biopsies, pneumonia treatment –prednisone and Levaquin for 7 days
• Patient switched to cephalosporin because of difficulty breathing
• Came in for a 10 Pass MAH Gamma 70 with added German Biologics • Sinusitis nosode
• Drosera
• Traumeel
• Phosphor
• Grippe
• Funiculus-Umbilicus
85

Treatment – Case III: J.P.
• Two of the treatments injected sodium bicarb 8.4% 3ml and 20
Gamma Ozone 20ml direct into tumor
• Will Redo PET scan in 3 months
• Patient is able to massage 5 patients per day
Patient transcended May 2018.
86

Case IV: L.J.
• 96 y.o male patient PTC with Stage 4 Squamous Cell Cancer in
left lateral pharyngeal wall with submandibular Para-
pharyngeal infiltration – Tonsillar Cancer with metastatic
lymphadenopathy within the left submandibular and left
jugulodigastric lymph nodes
• Current Meds- Doxazosin 2mg, Naltrexone 3mg, Testosterone
cream
• Supplements – Vitamin D3, 5K, Betaine HCL, DIM, Sun
Chlorella, Melatonin, Salvestrols, Cyto-Control, Myco-
Control, Coconut oil, Prostabel, Vitamin A 5000iu, Lugol’s
Solution Iodine, ARG Pancreas, Macuguard, 4 Sight, EZ Flo
Tea, Oncoplex ES, Daily Essential Nutrients, Modified Citrus
Pectin 87

Case IV: L.J.
• Significant Findings – Empire City Labs
• Pregnenelone LC/MS/MS 15 RR:22-237ng/dL
• Sex Hormone Binding Globulin 165.4 RR:10.0-57.0nmol/L
• FSH(Follicle Stimulating Hormone) 29.6 RR: 1.4-
18.1mIU/mL
• Cortisol Total Serum 26.5 RR: 3.09-25.0 ug/dL
• IGF-1 83 RR:163-584ng/mL
• Carnitine Total 28 RR:30-70umol/L
• Carnitine Free 22 RR:23-59umol/L
• Homocysteine 16 RR:3.7-13.9umol/L
• Cortisol Free 2nd Void U 189.5 RR: 3.5-87.1 88

89

Case IV: L.J. After Labs
• L-Carnitine 500 mg BID, Pregnenelone 30 mg in AM, Methyl Protect, IG 26DF
• Ketogenic Diet
• 14 Multi-Pass Treatments with Herrmann Machine Gamma 55 500-1000ml and German Biologics
• Tonsilla Compositum
• Sabal Homaccord
• Solidago Compositum
• Heppar Compositum
• Chelidonium
• Lymphomyosot
• Momordica Compositum
• Glyoxal
• CoEnzyme
• Engystol
• Herpes Nosode
• Mucosa Compositum
• ATP
• Occulis Totalis
• Tumor injection x9 sodium bicarb 8.4% 5ml Ozone 20 ml gamma 39
• Patient does C drips with another doctor every week
• “Overall I think L.J. is doing very well. His cancer seems to be reasonably stabile over the last 14 months
and his quality of life is reasonably good. But there is some evidence that the local condition is worse.”
Dr.S
• At this time L.J. manages pain with tramadol, morphine and medical marijuana, he is on hospice and
continues to come weekly for multi-pass treatment
• Patient transcended June 2018.
90

Finnish Sauna Was Recommended in all Three Cases
“In the control group, neither summed stress score (SSS) nor summed
difference score (SDS) of myocardial scintigraphy changed. However, Waon
therapy improved both SSS (16±7 to 9±6, p<0.01) and SDS (7±4 to 3±2,
p<0.01), and the improvement was greater in patients with higher SSS and SDS
scores at the baseline. Waon therapy extended treadmill exercise time (430±185
to 511±192 s, p<0.01) and improved flow-mediated dilation of the brachial
artery (4.1±1.3 to 5.9±1.8%, p<0.05), but tended to decrease the number of
circulating CD34-positive bone marrow-derived cells.” LOE 4
Repeated sauna therapy improves myocardial perfusion in patients with chronically occluded coronary artery-related
ischemia Sobajima, Mitsuo et al. International Journal of Cardiology , Volume 167 , Issue 1 , 237 - 24391

LOE 392

Low Dose Naltrexone • Naltrexone is an FDA-approved drug
• Inhibits Opioid receptors
• Reduces pain
• Targets same receptors that respond to morphine, heroine and
other opioids
• Small doses 0.5 – 4.5mg profoundly affects the immune
system
• LDN attaches to opioid receptors and temporarily blocks
endorphin attachment
• This signals the body to increase endorphin production,
orchestrates the activity of stem cells, macrophages and other
immune cells
Brown N, Panksepp J. Low-dose naltrexone for disease preventionand quality of
life. Med Hypothesis. 209; 72: 333-337
93

Low Dose Naltrexone
• Effective therapy for conditions ranging from autoimmune disorders, allergies, cancer and autism
• Some conditions LDN may help:• ALS
• Alzheimer’s
• Autism
• Celiac Disease
• Crohn’s Disease
• Emphysema
• Endometriosis
• HIV/AIDS
• Lupus
• Inflammatory Bowel Disease
• Multiple Sclerosis
• Psoriasis
• Rheumatoid Arthritis
• Sarcoidosis
• Scleroderma
Brown N, Panksepp J. Low-dose naltrexone for disease preventionand quality of life. Med Hypothesis.
209; 72: 333-337
94
In Conclusion
I strongly encourage environmental medicine providers to incorporate ozone
chelation into clinical practice, as in my opinion and evidenced by clinical cases,
ozone chelation is a safe, effective and time efficient protocol to reduce and
eliminate heavy metal toxicity. Join me in the Ozonosphere!
95

ReferencesBellinger, D. (2011). The Protean Toxicities of Lead: New Chapters in a Familiar Story. International Journal of Environmental Research and Public Health, 8(12), 2593-2628.
doi:10.3390/ijerph8072593
Biotherapeutic index: Ordinatio antihomotoxica et materia medica (5th ed.). (2000). Baden-Baden, Germany: Biologische Heilmittel Heel GmbH.
Bocci et al. Medical Gas Research 2011, 1:6 http://www.medicalgasresearch.com/content/1/1/6
Bocci, V. Is it true that ozone is always toxic? The end of a dogma. ToxicolApplPharmacol216, 493-504 (2006).
Brown N, Panksepp J. Low-dose naltrexone for disease preventionand quality of life. Med Hypothesis. 209; 72: 333-337
Flora, G., Gupta, D., & Tiwari, A. (2012). Toxicity of lead: a review with recent updates. Interdisciplinary Toxicology, 5(2). doi:10.2478/v10102-012-0009-2
Gaetke, L., & Chow, C. (2003). Copper Toxicity, Oxidative Stress, and Antioxidant Nutrients. Elsevier, 189(1-2), 147-173. doi:https://doi.org/10.1016/S0300-483X(03)00159-8
Gregorio Martínez-Sánchez “Ozone as U-ShapedDose ResponsesMoleculesHormentines” Dose Response (Prepress) FormerlyNonlinearilyin Biology, Toxicology, and Medicine.
Copyright © 2010 Universityof Massachusetts. ISSBN: 1559-3258 DOI: 10.2203/doseresponse 10-001.
Homeopathy. 2015 Oct;104(4):328-32. doi: 10.1016/j.homp.2015.05.003.
Herskowitz, A., M.D. (2017, February). Hyperbaric Ozone. Lecture presented at Ozone Masters 2017, Pal Alto, California.
Lunov, Oleg, et al. “Cell Death Induced by Ozone and Various Non-Thermal Plasmas: Therapeutic Perspectives and Limitations.” Nature News, Nature Publishing Group, 20 Nov.
2014, www.nature.com/articles/srep07129
LDNScience – What is LDN Used For? http://www.ldnscience.org/low-dose-naltrexone/what-is-ldn-used-for. Accessed February 23, 2015
Posadzki, P., Alotaibi, A., & Ernst, E. (2012, November 20). Adverse effects of homeopathy: A systematic review of published case reports and case series. Retrieved from
https://onlinelibrary.wiley.com/doi/full/10.1111/ijcp.12026
Repeated sauna therapy improves myocardial perfusion in patients with chronically occluded coronary artery-related ischemia Sobajima, Mitsuo et al. International Journal of
Cardiology , Volume 167 , Issue 1 , 237 - 243
Sagai, M., & Bocci, V. (2011). Mechanisms of Action Involved in Ozone Therapy: Is healing induced via a mild oxidative stress? Medical Gas Research, 1, 29.
http://doi.org/10.1186/2045-9912-1-29
Shallenberger, F. (2011). Principles and applications of ozone therapy: a paractical guideline for physicians. Carson City, Nev.?: Frank Shallenberger.
Tournier, A., Roberts, E. R., & Viksveen, P. (2013, March 24). Adverse effects of homeopathy: A systematic review of published case reports and case series – comment by
Tournier et al. Retrieved from https://onlinelibrary.wiley.com/doi/abs/10.1111/ijcp.12138
Viebahn-Hänsler, R., Fernández, O.S.L. & Fahmy, Z. Ozone in Medicine: The Low-Dose Ozone Concept. Guidelines and Treatment Strategies. Ozone Science & Engineering34,
408-424 (2012).
Viviana, C. & Gabriele, T. Exposure to low ozone concentrations induces cytoskeletal reorganization, mitochondrial activity and nuclear transcription in epithelial human cells. in
EuropenaCooperation of Medical Ozone Societies Congress (Zurich, 2014).
Willhite, C. C., Karyakina, N. A., Yokel, R. A., Yenugadhati, N., Wisniewski, T. M., Arnold, I. M., . . . Krewski, D. (2014). Systematic review of potential health risks posed by
pharmaceutical, occupational and consumer exposures to metallic and nanoscale aluminum, aluminum oxides, aluminum hydroxide and its soluble salts. Critical Reviews in
Toxicology,44(Sup4), 1-80. doi:10.3109/10408444.2014.934439
96