christopher gilpin laboratories, diagnostics and drug ... - update on who … · christopher gilpin...
TRANSCRIPT
1 |
Update on WHO TB Diagnostic PoliciesUpdate on WHO TB Diagnostic Policies
Photo: Riccardo Venturi
Christopher Gilpin
Laboratories, Diagnostics and Drug Resistance Unit
WHO Global TB Programme

Outline
� WHO requirements for evaluation of new TB diagnostics
� Xpert MTB/RIF evidence
� Xpert MTB/RIF recommendations
� DST
� Biosafety
� Lineprobe assays
� Upcoming EGMs

Phase 1
Research and Development
Phase 2 Evaluation and Demonstration
Phase 3
WHO evidence assessment
GRADE
Phase 4 Phased uptake and
collection of evidence for
scale-up
Phase 5 Scale-up and policy refinement
Evidence required for WHO review of
diagnostics

• Upstream research and development to define and validate a prototype
• Laboratory validation under international standards, design-locked product
• WHO interact with developers to discuss end-user requirements
Phase 1: Research and Development
• Controlled trials at 3-5 trial sites in high-burden TB and HIV countries
• Product registration with global and/or national regulatory authorities
• Specifications, performance validated in field trials in 5-10 sites of intended use
Phase 2: Evaluation and Demonstration
• New technologies/new indications for use: Dossier with Phase 1 and 2 data
• Generic technologies: ISO13:485 standards; equivalence shown in 2-3 SRLs
• WHO is not a regulatory authority
• WHO does not recommend technologies for individual country use
Phase 3: WHO evidence assessment using GRADE
• Implementation in routine TB services in high-burden TB and HIV countries
• Systematic evaluation: algorithms, workload, operational issues, CE
• Lessons learnt by early implementers used for country adaptation
Phase 4: Phased uptake & evidence for scale-up
• Scale-up, with subsequent data to inform and refine WHO policy guidance
Phase 5: Scale-up & policy refinement
� Expert Group Meeting – Veyrier-du-Lac, France
20-21 May 2013
� WHO commissioned three systematic reviews
� Xpert for the diagnosis of pulmonary TB and rifampicin
resistance in adults
� Xpert for the diagnosis of extrapulmonary TB
� Xpert for the diagnosis of TB in children
� Review of affordability and cost-effectiveness of Xpert
Evidence synthesis for utility
of Xpert MTB/RIF assay

Xpert MTB/RIF for the diagnosis of pulmonary TB in adults
Pooled sensitivity = 88% (84, 92)
Pooled specificity = 99% (98, 99)
27 studies,
9558 participants

Pooled sensitivity = 95% (90, 97)
Pooled specificity = 98% (97, 99)
Xpert MTB/RIF for the detection of rifampicin resistance
24 studies,
2414 specimens
555 rifampicin resistant
specimens

Xpert MTB/RIF for the diagnosis of pulmonary
TB and rifampicin resistance in adults
• Xpert MTB/RIF should be used rather than conventional microscopy, culture
and DST as the initial diagnostic test in adults suspected of having MDR-
TB or HIV-associated TB (strong recommendation, high-quality evidence).
• Xpert MTB/RIF may be used rather than conventional microscopy and
culture as the initial diagnostic test in all adults suspected of having TB
(conditional recommendation acknowledging resource implications, high-
quality evidence) (NEW)
• Xpert MTB/RIF may be used as a follow-on test to microscopy in adults
suspected of having TB but who are not at risk of MDR-TB or HIV
associated TB, especially in further testing of smear-negative specimens
(conditional recommendation acknowledging resource implications, high-
quality evidence).
WHO Policy Recommendations

Xpert MTB/RIF for the diagnosis of pulmonary TB and
rifampicin resistance in adults
• These recommendations apply to the use of Xpert MTB/RIF in processed and unprocessed
sputum specimens;
• These recommendations also apply to gastric lavage and aspirates from adults and children
based on the generalization of data from children;
• These recommendations support the use of a single sputum specimen for diagnostic testing,
acknowledging that processing multiple specimens increase the sensitivity of Xpert MTB/RIF
but has resource implications;
• Conventional microscopy and culture remains essential for monitoring of therapy and for
performing DST other than rifampicin (including for isoniazid and second-line anti-TB drugs);
• Expanding the scope of Xpert MTB/RIF use and its placement in diagnostic algorithms will
have significant operational implementation implications and should be phased in within the
context of TB national strategic plans;
• Emerging data show that Xpert MTB/RIF detects some rifampicin-resistant strains that are
susceptible on phenotypic DST. Sequencing of these discordant results usually resolves in
favour of Xpert MTB/RIF, and patients missed by phenotypic DST have poor treatment
outcomes on first-line treatment.
Remarks: To be read in conjunction with the policy recommendations

Xpert MTB/RIF for the diagnosis of extrapulmonary TB and rifampicin
resistance in adults and children
0% 20% 40% 60% 80% 100%
Pleural fluid
Lymph node
Cerebospinal fluid
Gastric fluid
Tissue
Sensitivity
(A) Sensitivity by sample type
Composite reference standard
0% 20% 40% 60% 80% 100%
Pleural fluid
Lymph node
Cerebospinal…
Gastric fluid
Tissue
Sensitivity
(B) Specificity by sample type
Composite reference standard Culture reference standard
• Mostly consecutive sampling
• Mostly cross-sectional
• Concerns about imperfect reference
standard
• Concerns about setting
• Concerns about sample processing
15 published and 7 unpublished studies, 5922 samples

Xpert MTB/RIF for the diagnosis of extrapulmonary TB
and rifampicin resistance in adults and children
• Xpert MTB/RIF should be used in preference to conventional microscopy and culture as the initial diagnostic test in testing cerebrospinal fluid specimens from patients suspected of having TB meningitis (strong recommendation given the urgency of rapid diagnosis, very low quality of evidence).
• Xpert MTB/RIF may be used as a replacement test for usual practice (including conventional microscopy, culture, and/or histopathology) for testing of specific non-respiratory specimens (lymph nodes and other tissues) from patients suspected of having extrapulmonary TB (conditional recommendation, very low quality of evidence).
WHO Policy Recommendations (NEW)

Xpert MTB/RIF for the diagnosis of extrapulmonary TB
and rifampicin resistance in adults and children
• Individuals suspected of having extrapulmonary TB but with a single Xpert MTB/RIF -negative result should undergo further diagnostic testing, and those with high clinical suspicion for TB (especially children) should be treated even if an Xpert MTB/RIF result is negative or if the test is not available;
• For CSF specimens, Xpert MTB/RIF should be preferentially used instead of culture if the sample volume is low or additional specimens cannot be obtained, in order to reach quick diagnosis. If sufficient volume of material is available, concentration methods should be used to increase yield;
• Pleural fluid is a suboptimal sample for the bacterial confirmation of pleural TB regardless of the method used. A pleural biopsy is the preferred sample. The sensitivity of Xpert MTB/RIF in pleural fluid is very low. Nevertheless, any individual with a positive result from pleural fluid tested by Xpert MTB/RIF should be treated for pleural TB; while those with a negative Xpert MTB/RIF result should have other tests;
• Conventional microscopy and culture are essential for monitoring of therapy and for performing DST for anti-TB agents other than rifampicin (including for isoniazid second-line anti-TB agents);
• Emerging data show that Xpert MTB/RIF detects some rifampicin-resistant strains that are susceptible on phenotypic DST. Sequencing of these discordant results usually resolves in favour of Xpert MTB/RIF, and patients missed by phenotypic DST have poor treatment outcomes on first-line treatment.
• These recommendations do not apply to stool, urine or blood, given the lack of data on the utility of Xpert MTB/RIF for these specimens
Remarks: To be read in conjunction with the policy recommendations

13 studies,
2603 participants
Xpert MTB/RIF for the diagnosis of pulmonary TB in
children
•Patient selection: inpatients in
higher level care facilities = high
concern regarding applicability
•Imperfect reference standard
culture = unclear risk of bias (not for
RIF resistance)
Pooled sensitivity (95%CrI) Pooled specificity (95% CrI)
ES/IS 66% (52, 77) 98% (96, 99)
GLA 66% (51, 81) 98 % (96, 99)
Xpert for the diagnosis of pulmonary TB and rifampicin
resistance in children
• Xpert MTB/RIF should be used rather than conventional microscopy, culture and
DST as the initial diagnostic test in children suspected of having MDR-TB or HIV-
associated TB (strong recommendation, very low-quality evidence).
• Xpert MTB/RIF may be used rather than conventional microscopy and culture as
the initial diagnostic test in all children suspected of having TB (conditional
recommendation acknowledging resource implications, very low-quality evidence).
WHO Policy Recommendations (NEW)

Xpert MTB/RIF for the diagnosis of pulmonary TB and
rifampicin resistance in children
• These recommendations apply to the use of Xpert MTB/RIF in processed and unprocessed sputum specimens;
• These recommendations also apply to gastric lavage and aspirates;
• Children suspected of having pulmonary TB but with a single Xpert MTB/RIF -negative result should undergo further diagnostic testing, and a child with high clinical suspicion for TB should be treated even if an Xpert MTB/RIF result is negative or if the test is not available.
Remarks to be read in conjunction with the policy recommendations

WHO Guidance Documents on Xpert MTB/RIF
http://www.who.int/tb/laboratory/xpert_launchupdate/en/
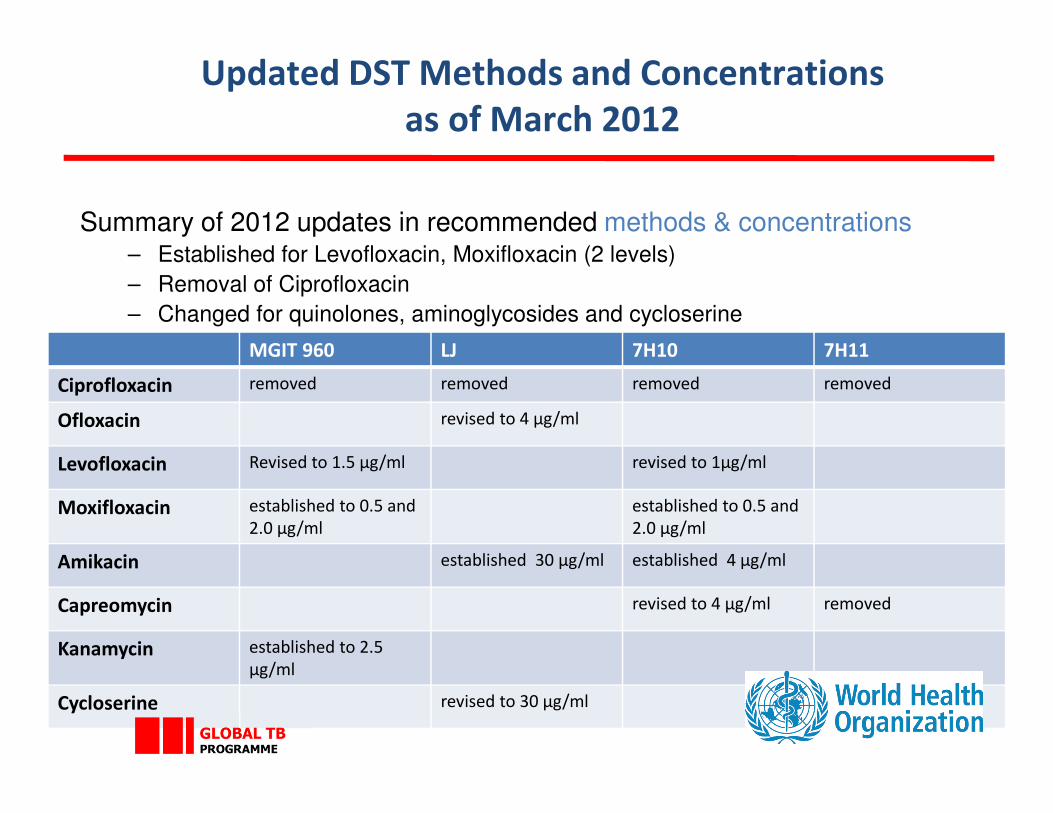
Updated DST Methods and Concentrations
as of March 2012
Summary of 2012 updates in recommended methods & concentrations– Established for Levofloxacin, Moxifloxacin (2 levels)
– Removal of Ciprofloxacin
– Changed for quinolones, aminoglycosides and cycloserine
MGIT 960 LJ 7H10 7H11
Ciprofloxacin removed removed removed removed
Ofloxacin revised to 4 μg/ml
Levofloxacin Revised to 1.5 μg/ml revised to 1μg/ml
Moxifloxacin established to 0.5 and
2.0 μg/ml
established to 0.5 and
2.0 μg/ml
Amikacin established 30 μg/ml established 4 μg/ml
Capreomycin revised to 4 μg/ml removed
Kanamycin established to 2.5
μg/ml
Cycloserine revised to 30 μg/ml

Critical concentrations for first- and second-line
Updated in 2012
• These recommendations apply to the use of Xpert MTB/RIF in processed and unprocessed sputum specimens;
• These recommendations also apply to gastric lavage and aspirates;
Remarks to be read in conjunction with the policy recommendationsDrug groupa Drug
DST
method
available
DST critical concentrations (μg/ml)
Löwenstein-
Jensenb
Middlebrook
7H10b
Middlebrook
7H11b
MGIT960
Group 1
First-line oral anti-TB agents
Isoniazid
Rifampicinc
Ethambutold
Pyrazinamide
Solid, liquid
Solid, liquid
Solid, liquid
Liquid
0.2
40.0
2.0
-
0.2
1.0
5.0
-
0.2
1.0
7.5
-
0.1
1.0
5.0
100.0
Group 2
Injectable anti-TB agents
Streptomycine
Kanamycin
Amikacin
Capreomycin
Solid, liquid
Solid, liquid
Solid, liquid
Solid, liquid
4.0
30.0
30.0
40.0
2.0
5.0
4.0
4.0
2.0
6.0
-
-
1.0
2.5
1.0
2.5
Group 3
Fluoroquinolones
Ofloxacinf
Levofloxacin
Moxifloxacing
Gatifloxacinh
Solid, liquid
Solid, liquid
Solid,liquid
Solid
4.0
-
-
-
2.0
1.0
0.5/2.0
1.0
2.0
-
-
-
2.0
1.5
0.5/2.0
-
Group 4i
Oral bacteriostatic second-line anti-TB
agents
Ethionamide
Prothionamide
Cycloserine
P-aminosalicylic acid
Solid, liquid
Solid, liquid
Solid
Solid, liquid
40.0
40.0
30.0
1.0
5.0
-
-
2.0
10.0
-
-
8.0
5.0
2.5
-
4.0
Group 5i
Anti-TB agents with unclear efficacy (not
recommended by WHO for routine use in
MDR-TB patients)
Clofazimine
Amoxicillin/clavulanate
Clarithromycin
Linezolid
Liquid
None
None
Liquid
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
1.0

Challenges remaining for DST determination
• Neither genotypic nor phenotypic DST are an absolute gold standard.
• Genotypic DST: not all mutations known. Silent mutations, phylogenetic polymorphisms, and mutations of unknown significance are problematic.
• “Borderline” Rifampicin resistance (prevalence, geographic spread);
• Studies to describe molecular mutations for second-line drugs to advance development of molecular/genotypic tests.
• The nuances of each type of test need to be better understood and considered in evaluations of future DST.
• Role of next generation DNA sequencing in determining DST
• Studies that systematically evaluate head-to-head test comparisons using appropriate design and linked to patient outcomes;

WHO TB Laboratory Biosafety Manual
• Available in six languages
• Uses a risk assessment based approach
• Describes the minimal precautions needed for performing different
procedures in the TB laboratory
• Does not refer to different biosafety levels
• Uses the term “TB Containment Laboratory”
English French Spanish Russian Chinese Portuguese

Line probe assays- Update
• Evaluation of two new versions of line probe assays meeting WHO recommended characteristics:
– Nipro NTM+MDRTB Detection kit 2
– Hain Genotype MTBDRplus version 1
– Hain Genotype MTBDRplus version 2
• Non-inferiority study
• Recommended for use in AFB smear positive processed sputum sediments and positive cultures only
• The Genotype MTBDRsl assay cannot be used as a replacement test for conventional phenotypic DST
Upcoming Expert Group Meetings
• Evaluation of urinary LAM –2015
• Evaluation of utility of phenotypic and genotypic
methods (including LPA and DNA sequencing) for
DST –2015

Acknowledgements
Laboratory, Diagnostics and Drug Resistance unit in the
WHO Global TB Programme:
Karin Weyer, Fuad Mirzayev, Wayne van Gemert, Jean
Iragena, Diego Zallocco, Henriikka Huttunen, Denisa
Pohancanikova, Fraser Wares, Ernesto Jaramillo, Dennis
Falzon, Vineet Bhatia, Linh Nguyen, Lynne Harrop