chriscunningham … colorectal! abriefhistoryofrectalcancersurgery 0 20 40 60 80 100 120 1845 1910...
TRANSCRIPT

Oxford Colorectal
New approaches in managing rectal cancer
Chris Cunningham Oxford University Hospitals NHS Founda>on Trust

Oxford Colorectal
Areas of change in rectal cancer
Organ preserva>on in early stage disease
More effec>ve minimally invasive surgery
for advanced disease

Oxford Colorectal

Oxford Colorectal
A brief history of rectal cancer surgery
0
20
40
60
80
100
120
1845 1910 1950 1975 2000 2012
Recurrence
mortality Buess%
1984%
Lisfranc%
1822%
Billroth%
1860%
Kocher,%Kraske%
1874%
Miles%
1908%
Dixon%
1948%
Parks%
1982%
Heald,%Quirke%
1986%
TME%and%preop%RT%
2001%
Lloyd%Davies%
1939%
Bosset%and%Gerard%
2006%
Holms%
2008%
1984%
Miles Lisfranc Lloyd-‐Davies Parks Heald Holm Bilroth
Mortality Local recurrence

Oxford Colorectal
A brief history of rectal cancer surgery
0
20
40
60
80
100
120
1845 1910 1950 1975 2000 2012
Cancer rel death Recurrence
mortality
Stoma Buess%
1984%
Lisfranc%
1822%
Billroth%
1860%
Kocher,%Kraske%
1874%
Miles%
1908%
Dixon%
1948%
Parks%
1982%
Heald,%Quirke%
1986%
TME%and%preop%RT%
2001%
Lloyd%Davies%
1939%
Bosset%and%Gerard%
2006%
Holms%
2008%
1984%
Miles Lisfranc Lloyd-‐Davies Parks Heald Holm Bilroth
Mortality Local recurrence
Death at 5 Years Stoma

Oxford Colorectal
A brief history of rectal cancer surgery
0
20
40
60
80
100
120
1845 1910 1950 1975 2000 2012
Morbidity
Cancer rel death Recurrence
mortality
Stoma Buess%
1984%
Lisfranc%
1822%
Billroth%
1860%
Kocher,%Kraske%
1874%
Miles%
1908%
Dixon%
1948%
Parks%
1982%
Heald,%Quirke%
1986%
TME%and%preop%RT%
2001%
Lloyd%Davies%
1939%
Bosset%and%Gerard%
2006%
Holms%
2008%
1984%
Miles Lisfranc Lloyd-‐Davies Parks Heald Holm Bilroth
Mortality Local recurrence
Death at 5 Years Stoma
Major morbidity

Oxford Colorectal
Radical surgery for T1 cancer Radical surgery
Opera>ve Mortality 2-‐4%
Stoma rate 40%
Major morbidity 30%
Local recurrence
<5%
Death from LR <2.5%
Metasta>c disease 5-‐10%
Overall survival 85-‐90%

Oxford Colorectal
Is there an no alterna>ve to a big opera>on?

Oxford Colorectal
ERC defined as T1 (possibly T2 invasion) Absence of lymph node spread Risk of nodal disease in T1 cancers varies from 3-‐25%
size and depth of invasion lympha>c invasion differen>a>on vascular invasion tumour budding
Cure can be achieved by local excision
Early Rectal Cancer

Oxford Colorectal
Local excision for early rectal cancer

Oxford Colorectal
Transanal endoscopic microsurgery Local excision by TEM offers precise par>al or full thickness excision of the extra-‐peritoneal rectum

Oxford Colorectal
Transanal endoscopic microsurgery
• GA, inpa>ent 1-‐2 days • Complica>on rate 5-‐15% • Good func>onal
recovery 70
72
74
76
78
80
82
84
86
88
90
pre-‐opera>ve 6 weeks 3 month 6 month
VAS

Oxford Colorectal

Oxford Colorectal

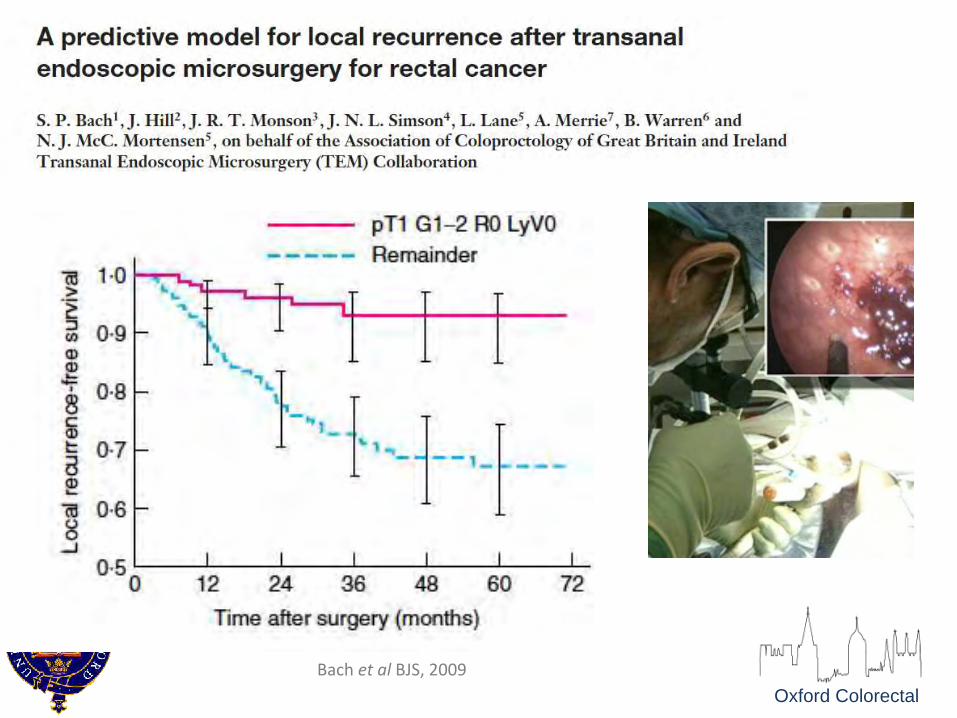
Oxford Colorectal Bach et al BJS, 2009
Oxford Colorectal Bach et al BJS, 2009

Oxford Colorectal
Local excision cures early rectal cancer
• pT1 • Tumour <3cm diameter • Complete excision (R0) • G1/2 • No lympha>c or vascular invasion

Oxford Colorectal
What if the post TEM pathology is unfavourable?
How do we manage these risks of recurrence?
What risk of recurrence is acceptable?

Oxford Colorectal
Assessing risk of recurrence
22mm cancer pT1, sm3, Ly1, R0

Oxford Colorectal
Bach et al BJS, 2009
22mm cancer pT1, sm3, Ly1, R0
Assessing risk of recurrence

Oxford Colorectal
Bach et al BJS, 2009
22mm cancer pT1, sm3, Ly1, R0
Assessing risk of recurrence

Oxford Colorectal
Bach et al BJS, 2009
25 %
22mm cancer pT1, sm3, Ly1, R0
Assessing risk of recurrence

Oxford Colorectal Solomon M, Pager C, Keshava A, Findlay M, Butow P, Salkeld G, et al. What Do Pa>ents Want? Diseases of the Colon & Rectum. 2003;46(10):1351-‐7.

Oxford Colorectal
How can we mi>gate recurrence?
• Offer comple>on radical surgery if poor post LE pathology?
• Close surveillance
• Offer radiotherapy ajer LE

Oxford Colorectal
How can we mi>gate recurrence?
• Offer comple>on radical surgery if poor post LE pathology?
• Close surveillance
• Offer radiotherapy ajer LE

Oxford Colorectal
Diseases of the colon and rectum. 2005; 48: 429-‐37

Oxford Colorectal
“In T1 and T2 tumours excised by TEM and subsequently treated by TME no recurrence was noted… excision biopsy followed by radical reopera>on is reasonable for early tumours” BJS, 2009
TEM then TME TEM then TME
TEM alone TEM alone

Oxford Colorectal
How can we mi>gate recurrence?
• Offer comple>on radical surgery if poor post LE pathology?
• Close surveillance
• Offer radiotherapy ajer LE

Oxford Colorectal
3-‐36 months 42 months
45 months 48 months
MRI surveillance

Oxford Colorectal
3-‐36 months 42 months
45 months 48 months
MRI surveillance

Oxford Colorectal
Final pathology

Oxford Colorectal
How can we mi>gate recurrence?
• Offer comple>on radical surgery if poor post LE pathology?
• Close surveillance
• Offer radiotherapy ajer LE

Oxford Colorectal
Systema>c review and meta-‐analysis of oncological outcome ajer local excision of pT1-‐2 rectal cancer with adjuvant (chemo)radiotherapy
compared to comple>on TME surgery
Borstlap WAA, et al, BJS 2016
Local recurrence according to post TEM treatment
Stage LE then CRT LE then TME
T1 10% 6%
T2 16% 10%

Oxford Colorectal
Systema>c review and meta-‐analysis of oncological outcome ajer local excision of pT1-‐2 rectal cancer with adjuvant (chemo)radiotherapy
compared to comple>on TME surgery
Local recurrence according to post TEM treatment
Stage LE then CRT LE then TME LE alone
T1 10% 6% 15-‐20%
T2 16% 10% 30-‐40%
Borstlap WAA, et al, BJS 2016

Oxford Colorectal
What can be done to extend the use of local excision?
Where is the evidence for
effec>ve use of LE ajer CRT?

Oxford Colorectal Surg Endosc. 2008
DFS 96% 96%

Oxford Colorectal Surg Endosc. 2008
DFS 96% 96%

Oxford Colorectal Surg Endosc. 2008
DFS 96% 96%

Oxford Colorectal

Oxford Colorectal

Oxford Colorectal Bujko K,et al, Radiotherapy and Oncology. 2013.

Oxford Colorectal Bujko K,et al, Radiotherapy and Oncology. 2013.
“…..acceptable local recurrence rate ajer preopera>ve radiotherapy and local excision of small, radiosensi>ve tumours in elderly pa>ents”

Oxford Colorectal
UK TREC Trial: Tes>ng the role for neo-‐adjuvant SCRT

Oxford Colorectal
STARTREC – Study design Phase II/III clinical trial
TME
W&W TEM
Poor/inadequate response
Liole or no residual disease
Good response: residual disease
high risk conversion TME
evalua>on TME
Organ preserva>on
5x5 Gy CRT
cT1-‐3b N0
Radical Surgery Organ preserva>on
week 11-‐13 – central review
week 1-‐5
CCR Not CCR week 16-‐20 – central review

Oxford Colorectal
EMR or TEM treatment of >3cm adenomas
Polypectomy
EMR/ESD
TEM
TME