chocolate toxicity in animals by dr.amandeep
TRANSCRIPT

Chocolate Toxicity In Pets
Dr.Amandeep Department Of Veterinary MedicineL2013V40M GADVASU
INTRODUCTION
• Theobromine poisoning
• Overdose reaction to the alkaloid theobromine, found
in chocolate , beverages & some other foods
• LD50 of caffeine and theobromine are 100-200 mg/kg
• It may result in potentially life-threatening cardiac
arrhythmias and CNS dysfunction.
INTRODUCTION
• Cocoa beans contain about 1.2% theobromine by
weight
• Processed chocolate, in general has smaller amounts
• Contributing factors include indiscriminate eating
habits & readily available sources of chocolate
• Deaths have also been reported in livestock fed cocoa
by-products

Dogs v/s Cats v/s Humans
• Serious poisoning happens more frequently in
domestic animals, which metabolize theobromine
much more slowly than humans
• If large numbers of filled chocolate candies are
consumed, another serious danger is posed by the fat
and sugar in the fillings, which can sometimes trigger
life-threatening PANCREATITIS several days later
Dogs v/s Cats v/s Humans
• Toxic dose for cats is even lower than for dogs
• But cats are less prone to eating chocolate since they
are unable to taste sweetness
• Half-lives of theobromine and caffeine in dogs are 17.5
hr and 4.5 hr respectively.
In Dogs
• Mild signs like vomition, diarrhea, polydipsia at 20
mg/kg
• Cardiotoxic effects at 40-50 mg/kg
• Seizures at >=60mg/kg
• One ounce of milk chocolate per pound of body weight
is a potentially lethal dose

Pathogenesis
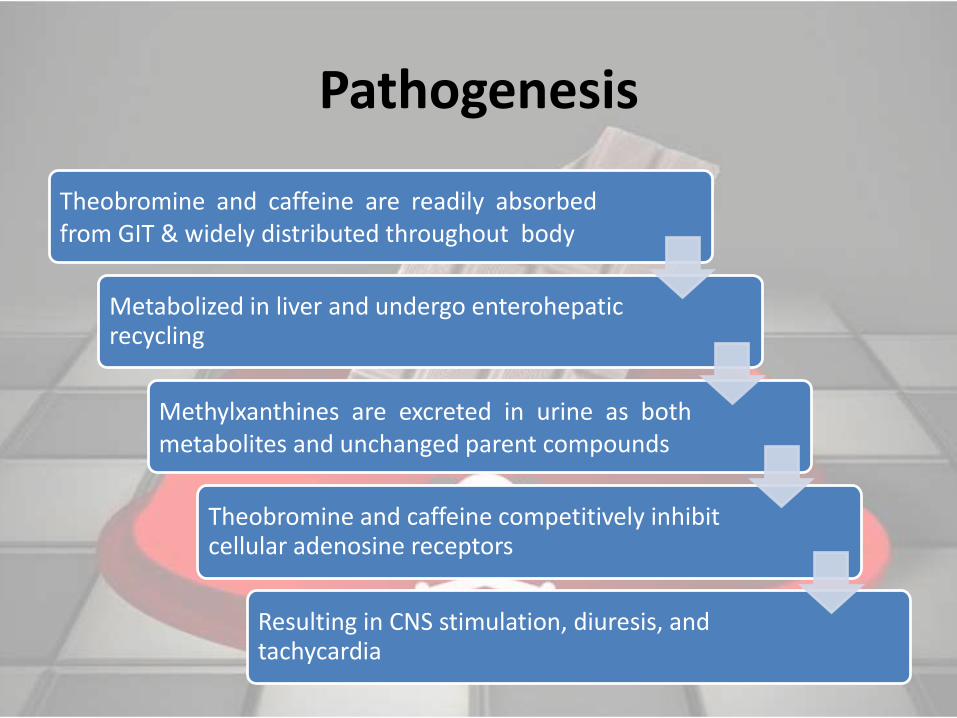
Theobromine and caffeine are readily absorbedfrom GIT & widely distributed throughout body
Metabolized in liver and undergo enterohepaticrecycling
Methylxanthines are excreted in urine as bothmetabolites and unchanged parent compounds
Theobromine and caffeine competitively inhibit cellular adenosine receptors
Resulting in CNS stimulation, diuresis, and tachycardia
Pathogenesis (EFFECT ON MUSCLES)
• Methylxanthines also increase intracellular calcium
levels by increasing cellular calcium entry
• And inhibiting intracellular sequestration of calcium by
the sarcoplasmic reticulum of striated muscle
• Net effect is increased strength and contractility of
skeletal and cardiac muscle
Pathogenesis
• Methylxanthines may also compete for benzodiazepine
receptors within CNS and inhibit phosphodiesterase,
resulting in increased cyclic AMP levels
• Methylxanthines may also increase circulating levels of
epinephrine and norepinephrine

Methylxanthines have following modes of action
• Antagonism of Adenosine Receptors: this antagonism results
in stimulation of the central nervous system and an increase in
heart rate and also diureses
• Inhibition of Cyclic Nucleotide phosphodiesterase:
consequently there is an increase in cyclic AMP, which in turn
leads to greater catecholamine release and their effect
• Modulation of Intracellular Calcium Concentrations:Ventricular
fibrillation, and other cardiac dysrhythmias are most frequently
the ultimate cause of death

Clinical Signs• Within 6-12 hours
• Initially
Nausea & Polydipsia
Vomiting & Diarrhea
Abdominal distension
Restlessness & increased Urination
• Progress to hyperactivity, polyuria, ataxia, tremors &
seizures
Clinical Signs
• Tachycardia, premature ventricular contractions,
tachypnea, cyanosis, hypertension, hyperthermia,
bradycardia, hypotension or coma
• In later course hypokalemia, due to cardiac dysfunction
• Eventually death due to cardiac arrhythmias,
hyperthermia or respiratory failure
Lesions
• No specific lesions
• May be found in animals succumbing to chocolatetoxicosis
• Hyperemia, hemorrhages or congestion of multipleorgans
• Severe arrhythmias may result in pulmonary edema orcongestion
• Chocolate or cocoa bean hulls be present in the GI tract

Diagnosis Diagnosis
• Amphetamine toxicosis
• Cocaine toxicosis
• Ingestion of antihistamines and antidepressants
• Other CNS stimulants
Treatment
• Dogs presenting with clinical signs
• Inital stabilisation of Cardiorespiratory System:
– Tachycardia: beta-blockers, eg orally administered metoprolol @ 0.2-0.4 mg per kg slow I/V every 8 hours
– Premature Ventricluar Contractions: lidocaine; iv bolus of 1-2mg/kg I/V followed by 25-80 mg/kg/min infusion administered slowly,
– Bradycardia: Atropine at dose of 0.01mg to 0.02mg per kg
Treatment
• Treatment of seizures and hyperactivity
– IV Diazepam at a dose of 0.5 to 2 mg/kg
– Alternative to diazepam is barbiturates
– Treating the seizures and hyperactivity should help
restore normal body temperature
– If animal still hyperthermic then this should be
treated directly

Treatment
• Correction of acid/base and electrolyte inbalances
• Insertion of urinary catheter
– Helps prevent further absorption of theobromine
and caffeine across bladder wall as methyxanthines
can be reabsorbed across urinary bladder wall
Treatment
Dogs with a known history of recent chocolate ingestion but who have not yet developed clinical signs
• Administration of apomorphine (0.03mg/kg IV) or
hydrogen peroxide (1-5 ml/kg po) - to induce emesis
• Activated charcoal (1-4g/kg,po) in order to minimise
further absorption of methylxanthines
Prognosis
• Clinical signs can persist upto 72 hours
• If treated correctly and early enough with in 5min
consult the prognosis is good and a complete recovery
can be expected
• For animals presenting with seizures and arrhythmias
the prognosis is guarded.


Thanks