chloride nephrosis. - semantic scholar · chloride retention in experimental hydro-nephrosis. by...
TRANSCRIPT
CHLORIDE RETENTION IN EXPERIMENTAL HYDRO-NEPHROSIS.
BY NORMAN M. KEITH, M.D., AND D. SCHUYLER PULFORD, JR., M.D.
(From the Department of Urology of the Johns Hopkins Hospital, Baltimore, Md., andthe Division of Medicine of Mayo Clinic, Rochester, Minn.)
(Received for publication, August 10, 1922.)
In a previous paper (Keith and Pulford) we described a methodfor producing experimental hydronephrosis, which permitted thestudy of renal function in this condition for periods varying fromweeks to months. The method used was the partial obstruction ofboth ureters near the ureteropelvic juncture. After a thoroughfunctional study of hydronephrosis thus produced, further experi-ments were carried out to ascertain how quickly normal functioncould be restored after ureteral obstruction was removed. It wasfound that if the obstruction was removed within a week, renalfunction was rapidly reestablished, but ureteral obstruction of longerduration often led to permanent damage to the kidney. This methodof production of a lesion in the kidney with the later withdrawal ofthe original cause offered unusual opportunities for observing theexcretory function of the kidney during the acute and later reparativestage of a pathologic process. In our previous work the excretionof nitrogenous bodies, particularly urea, andphenolsulfonephthaleinwas emphasized, whereas at present we are reporting observationson the excretion of chlorides. We have noted in hydronephrosisthat the regulating mechanism concerned in excretion of chloridediffers in several respects from that controlling the elimination ofurea and phenolsulfonephthalein. This finding is in agreementwith the results obtained by Widal and Javal, and McLean in othertypes of renal lesions. In the present study it will be shown that thewater and chloride. intake must be carefully controlled. Further,it was found that when both urea and chlorides are retained they donot accumulate quantitatively in the same degree in the blood plasma.
175
CHLORIDE RETENTION IN HYDRONEPHROSIS
Methods.
Female dogs were used exclusively because of the ease of catheteri-zation. Between experiments they were given a diet of 200 gm. ofground beef and 300 cc. of water each day. Each dog was subjectedto several control tests before being selected for use. The urine wasshown by the routine tests to be free from albumin, casts, and eryth-rocytes. The excretion of phenolsulfonephthalein and the contentof urea in the blood were found to be normal before an experi-ment was started. The dogs were kept in metabolism cages and inthe short experiments they were allowed no food. In the first fewexperiments, when measured amounts of water were given by mouthas a medium for salt administration, vomiting often occurred and theresults were not completely satisfactory. In the later experimentsneither food nor water was allowed by mouth and sodium chloridewas given subcutaneously, daily, in a concentration of about 1 percent; that is, approximately 2 gm. to 200 cc. of water, the exactpercentage being determined quantitatively in each lot of solutionused. Hydronephrosis was produced by applying rubber bandsaround both ureters (Keith and Pulford).' The determinationsused in the test of kidney function were: phenolsulfonephthaleinexcretion by the test of Rowntree and Geraghty, urea of the urineand the whole blood by Marshall's method (1913, a, b), chlorides ofthe urine by Arnold's modification of Volhardt's method (the inter-fering substances that might be present in urine of dogs could scarcelyaffect the comparative nature of the results), and chlorides of theblood plasma by the method of McLean and Van Slyke. Duplicatedeterminations were always made.
There is considerable variation in the total amount of urine excretedby a fasting animal under constant fluid intake by mouth. In orderthat the urine output might be more constant, and that more accuratestudies on chloride retention might be possible, a 1 per cent sodiumchloride solution was given subcutaneously as noted above. The dailyvariations in the amount of urine were thereby minimized. Sincethe urea content of whole blood and plasma differ so slightly, wehave considered them here as identical.
All operations were performed under ether anesthesia.
176
NORMAN M. KEITH AND D. SCHUYLER PULFORD, JR. 177
Observations on Control Animals.
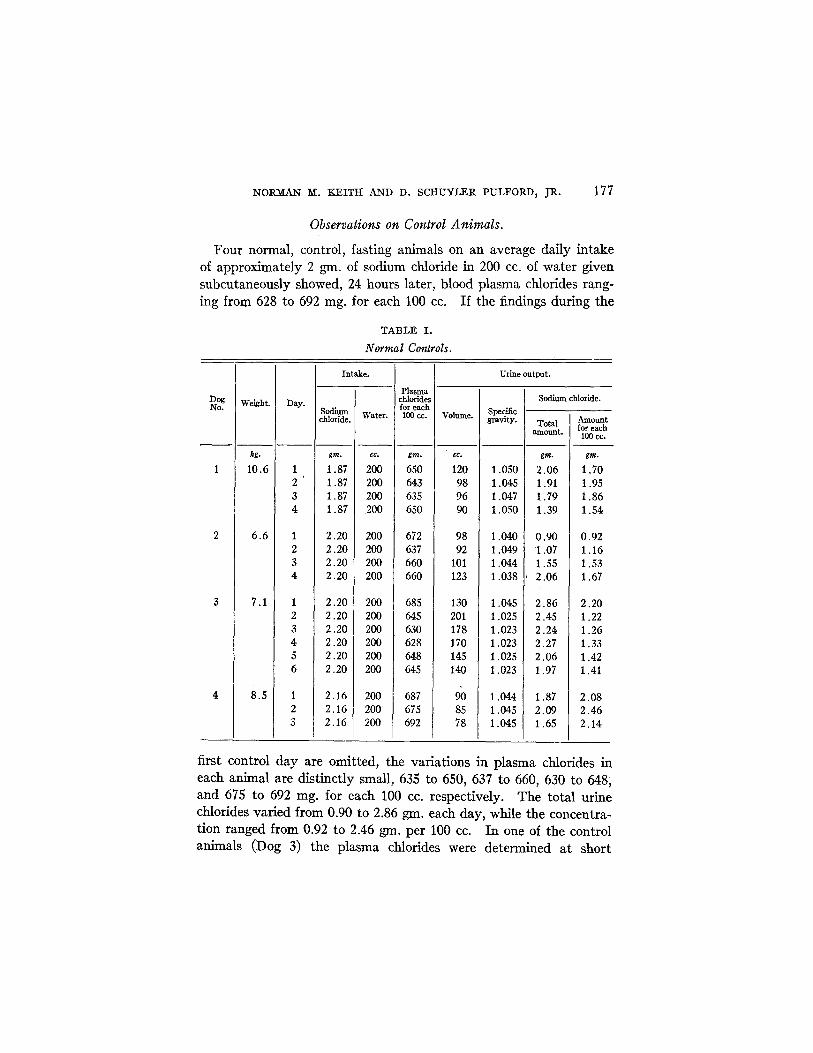
Four normal, control, fasting animals on an average daily intakeof approximately 2 gm. of sodium chloride in 200 cc. of water givensubcutaneously showed, 24 hours later, blood plasma chlorides rang-ing from 628 to 692 mg. for each 100 cc. If the findings during the
TABLE I.
Normal Controls.
DogNo.
1
2
3
4
Weight.
kg.
10.6
6.6
7.1
8.5
Day.
1234
1234
123456
123
Intake.
Sodiumchloride.
gm.
1.871.871.871.87
2.202.202.202.20
2.202.202.202.202.202.20
2.162.162.16
Water.
cc.
200200200200
200200200200
200200200200200200
200200200
Plasmachloridesfor each
100 cc.
gm.
650643635650
672637660660
685645630628648645
687675692
Urine output.
Volume.
cc.
120989690
9892
101123
130201178170145140
908578
Specificgravity.
1.0501.0451.0471.050
1.0401.0491.0441.038
1.0451.0251.0231.0231.0251.023
1.0441.0451.045
Sodium chloride.
Totalamount.
gm.
2.061.911.791.39
0.901.071.552.06
2.862.452.242.272.061.97
1.872.091.65
Amountfor each
100 cc.
gm.
1.701.951.861.54
0.921.161.531.67
2.201.221.261.331.421.41
2.082.462.14
first control day are omitted, the variations in plasma chlorides ineach animal are distinctly small, 635 to 650, 637 to 660, 630 to 648,and 675 to 692 mg. for each 100 cc. respectively. The total urinechlorides varied from 0.90 to 2.86 gm. each day, while the concentra-tion ranged from 0.92 to 2.46 gm. per 100 cc. In one of the controlanimals (Dog 3) the plasma chlorides were determined at short
= - -
- � �
--- -
178 CHLORIDE RETENTION IN HYDRONEPHROSIS
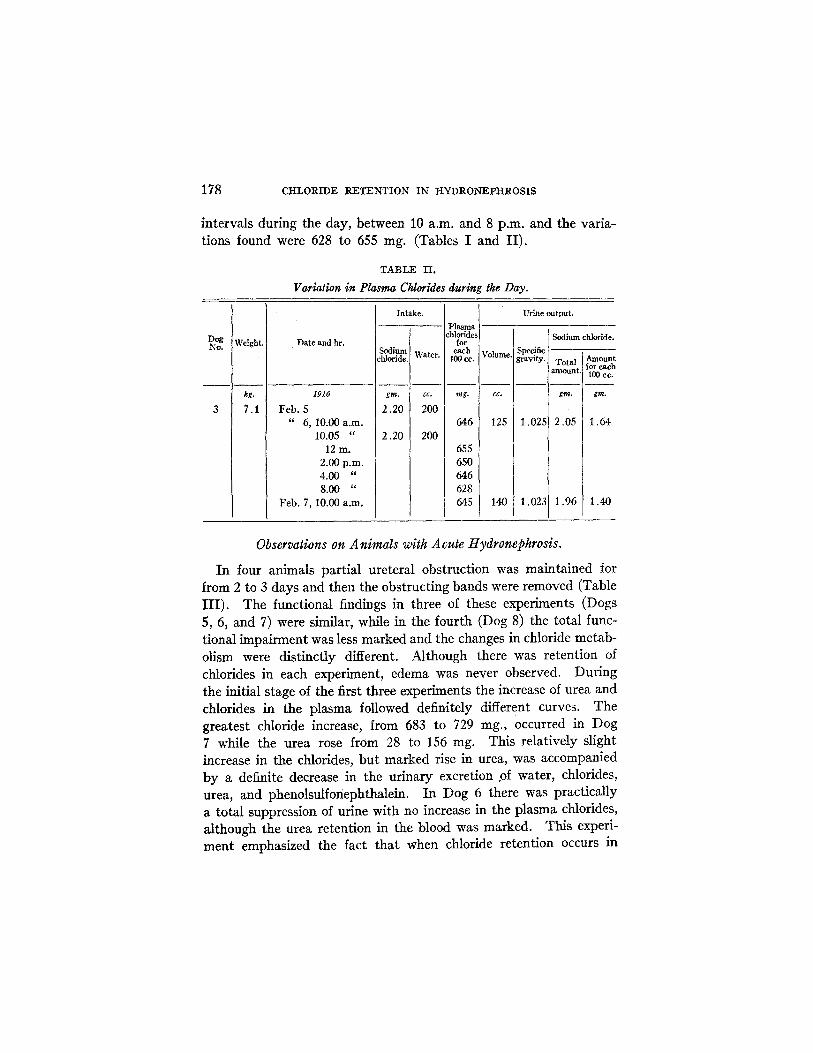
intervals during the day, between 10 a.m. and 8 p.m. and the varia-tions found were 628 to 655 mg. (Tables I and II).
TABLE II.
Variation in Plasma Chlorides during the Day.
Weight.
kg.
7.1
Date and hr.
1916
Feb. 5" 6, 10.00 a.m.
10.05 "12 m.
2.00 p.m.4.00 "8.00 "
Feb. 7, 10.00 a.m.
Intake.
Sodiumchloride.
gm.
2.20
2.20
Water.
cc.
200
200
Plasmachlorides
foreach
100 cc.
mg.
646
655650646628645
Urine output.
Volume.
cc.
125
140
Specificgravity.
1.025
1.023
Sodium chloride.
Totalamount.
gm.
2.05
1.96
Amountfor each100 cc.
gm.
1.64
1.40
Observations on Animals with Acute Hydronephrosis.
In four animals partial ureteral obstruction was maintained forfrom 2 to 3 days and then the obstructing bands were removed (TableIII). The functional findings in three of these experiments (Dogs5, 6, and 7) were similar, while in the fourth (Dog 8) the total func-tional impairment was less marked and the changes in chloride metab-olism were distinctly different. Although there was retention ofchlorides in each experiment, edema was never observed. Duringthe initial stage of the first three experiments the increase of urea andchlorides in the plasma followed definitely different curves. Thegreatest chloride increase, from 683 to 729 mg., occurred in Dog7 while the urea rose from 28 to 156 mg. This relatively slightincrease in the chlorides, but marked rise in urea, was accompaniedby a definite decrease in the urinary excretion pf water, chlorides,urea, and phenolsulfonephthalein. In Dog 6 there was practicallya total suppression of urine with no increase in the plasma chlorides,although the urea retention in the blood was marked. This experi-ment emphasized the fact that when chloride retention occurs in
DogNo.
3
:
-------------- .
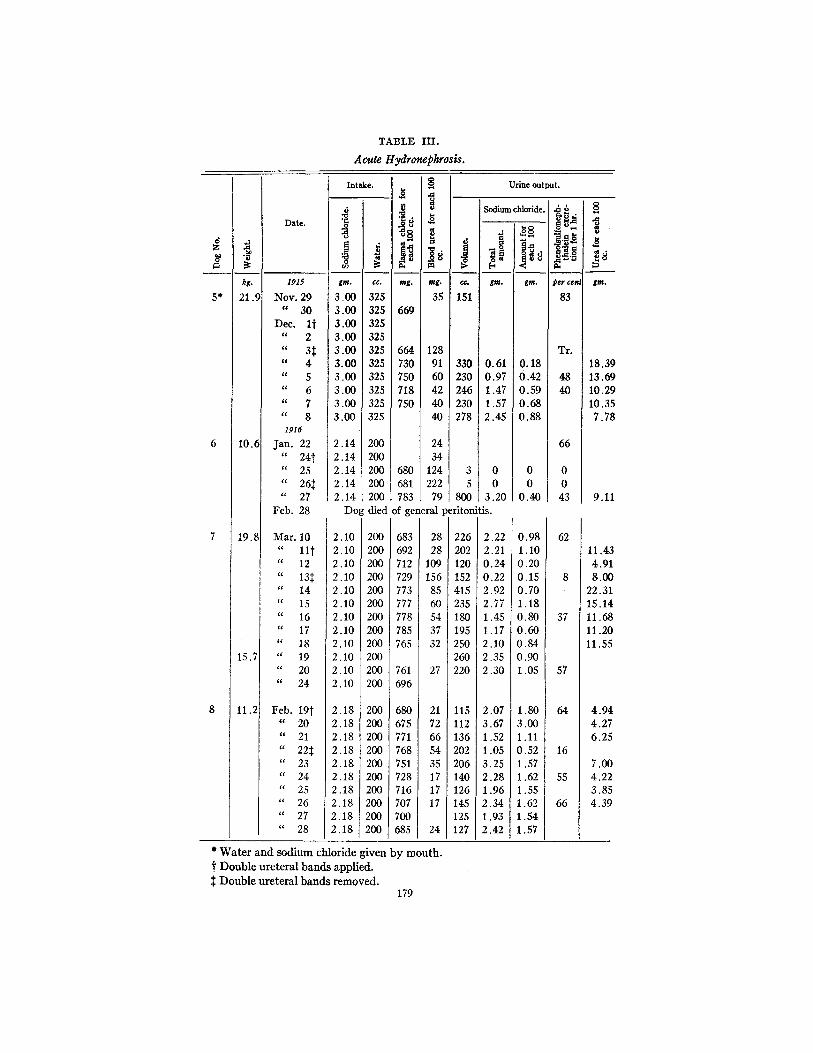
TABLE III.
Acute Hydronephrosis.
Intake.
gm. cc. mg. mg.
3.00 325 353.00 325 6693.00 3253.00 3253.00 325 664 1283.00 325 730 913.00 325 750 603.00 325 718 423.00 325 750 403.00 325 40
2.14 200 242.14 200 342.14 200 680 1242.14 200 681 2222.14 200 783 79
Feb. 28 Do
Mar. 10" lit
" 12
" 131;" 14" 15" 16" 17" 18" 19" 20" 24
Feb. 19t" 20
" 21" 22
" 23" 24" 25" 26" 27" 28
2.102.102.102.102.102.102.102.102.102.102.102.10
2.182.182.182.182.182.182.182.182.182.18
g died of general I
683692712729773777778785765
761696
680675771768751728716707700685
200200200200200200200200200200200200
200200200200200200200200200200
2828
109156
8560543732
27
2172665435171717
24
* Water and sodium chloride given by mouth.t Double ureteral bands applied.T Double ureteral bands removed.
179
Urine output.
0
Cc.
151
330230246230278
35
800
Sodium chloride.
-a
gtm.
0.610.971.471.572.45
00
3.20eritonitis.
226202120152415235180195250260220
115112136202206140126145125127
2.222.210.240.222.922.771.451.172.102.352.30
2.073.671.521.053.252.281.962.341.932.42
-8
O30
gm.
0.180.420.590.680.88
00
0.40
0.981.100.200.150.701.180.800.600.840.901.05
1.803.001.110.521.571.621.551.621.541.57
Date.
1915
Nov. 29" 30
Dec. It" 2
" 3t" 4
"C 5
" 6
" 7
" 8
1916
Jan. 22" 24t" 25
" 26t"' 27
z
5*
6
7
8
kg.
21.5
10.6
19.8
15.7
11.2
.I
t8
.R
Per cete
83
Tr.
4840
66
00
43
62
8
37
57
64
16
55
66
8
0
gom.
18.3913.6910.2910.357.78
9.11
11.434.918.00
22.3115.1411.6811.2011.55
4.944.276.25
7.004.223.854.39
_
A- . -AA .... .. /.
I.- j .- .- -
CHLORIDE RETENTION IN HYDRONEPHROSIS
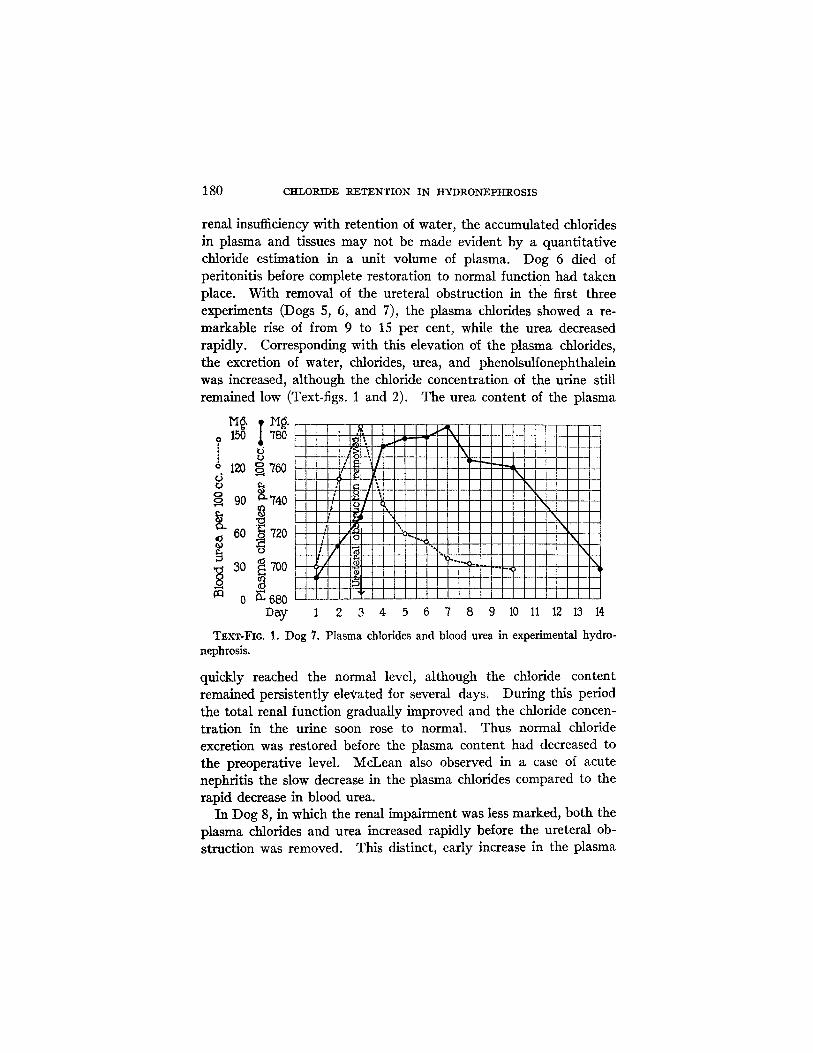
renal insufficiency with retention of water, the accumulated chloridesin plasma and tissues may not be made evident by a quantitativechloride estimation in a unit volume of plasma. Dog 6 died ofperitonitis before complete restoration to normal function had takenplace. With removal of the ureteral obstruction in the first threeexperiments (Dogs 5, 6, and 7), the plasma chlorides showed a re-markable rise of from 9 to 15 per cent, while the urea decreasedrapidly. Corresponding with this elevation of the plasma chlorides,the excretion of water, chlorides, urea, and phenolsulfonephthaleinwas increased, although the chloride concentration of the urine stillremained low (Text-figs. 1 and 2). The urea content of the plasma
M g.o 150 780
U° 120 ` 760U V.
A 90 740
g 60 720
30 700
'n ;fiDay 1 2 3 4 5 6 7 8 9 10 11 12 13 14
TExT-FIG. 1. Dog 7. Plasma chlorides and blood urea in experimental hydro-nephrosis.
quickly reached the normal level, although the chloride contentremained persistently elevated for several days. During this periodthe total renal function gradually improved and the chloride concen-tration in the urine soon rose to normal. Thus normal chlorideexcretion was restored before the plasma content had decreased tothe preoperative level. McLean also observed in a case of acutenephritis the slow decrease in the plasma chlorides compared to therapid decrease in blood urea.
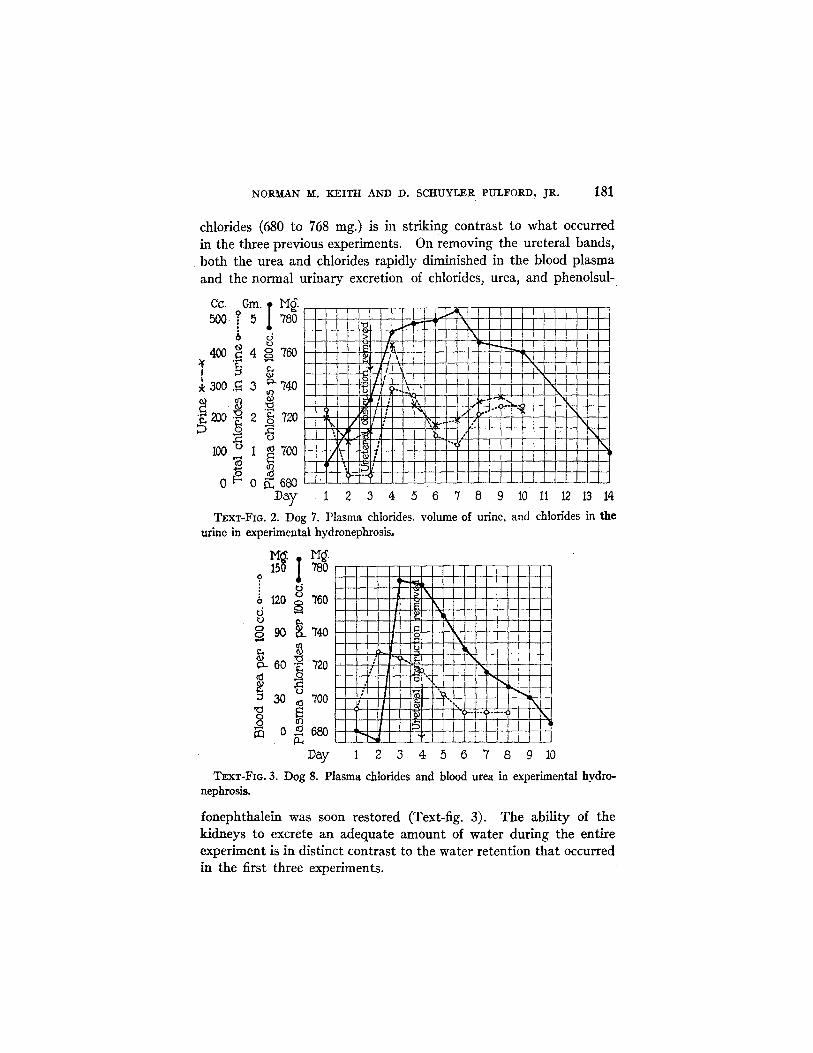
In Dog 8, in which the renal impairment was less marked, both theplasma chlorides and urea increased rapidly before the ureteral ob-struction was removed. This distinct, early increase in the plasma
-Li
180
NORMAN M. KEITH AND D. SCHUYLER PULFORD, JR.
chlorides (680 to 768 mg.) is in striking contrast to what occurredin the three previous experiments. On removing the ureteral bands,both the urea and chlorides rapidly diminished in the blood plasmaand the normal urinary excretion of chlorides, urea, and phenolsul-
cc. Gm. M.500.? 5 780
6 d
400 i 4 o 760
* 300 . 3 740
200 2 720
100 1 1" 700,o 0 0 68ay
..... I I
r IFS'>F 1 2 3 4 5 6 7 8 9
TEXT-FIG. 2. Dog 7. Plasma chlorides, volume of urine,urine in experimental hydronephrosis.
M. .150 1 780
06 120 760o
° 90 740Calo 0v 60 ' 720
j 30 5 700o E
q o 0 680
Day
10 11 12 13 14
and chlorides in the
1 2 3 4 5 6 7 8 9 10
TEXT-FIG. 3. Dog 8. Plasma chlorides and blood urea in experimental hydro-nephrosis.
fonephthalein was soon restored (Text-fig. 3). The ability of thekidneys to excrete an adequate amount of water during the entireexperiment is in distinct contrast to the water retention that occurredin the first three experiments.
181
CHLORIDE RETENTION IN HYDRONEPHROSIS
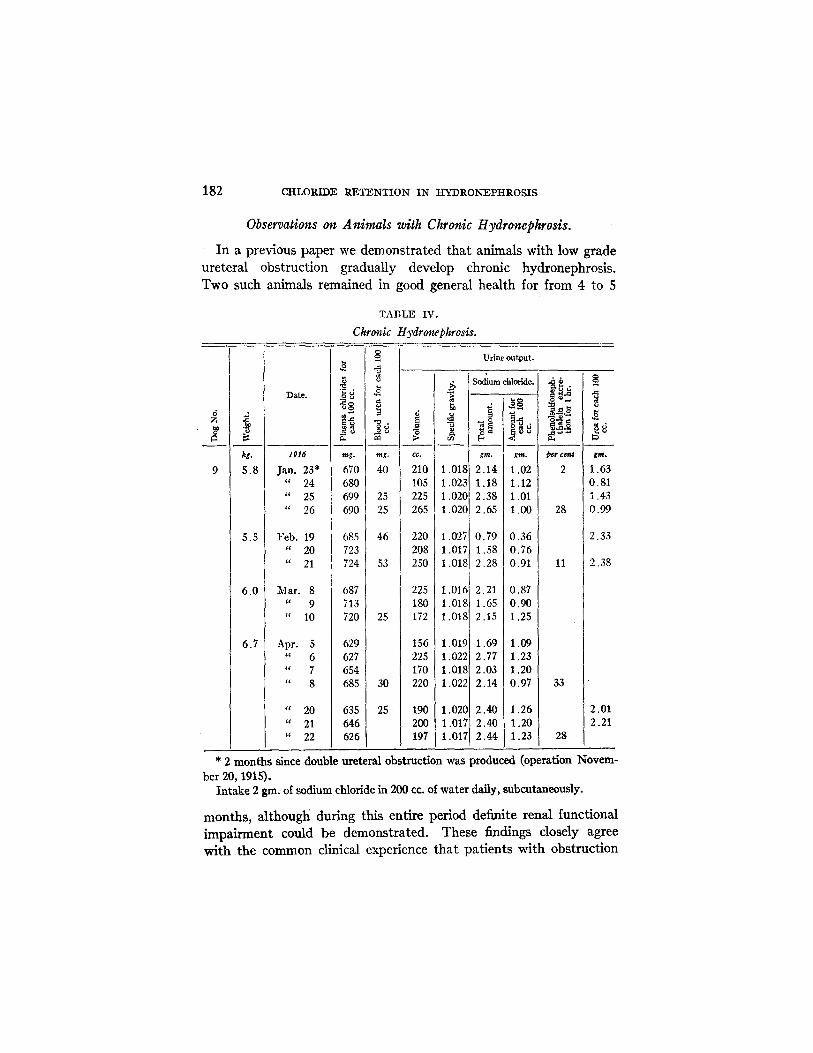
Observations on Animals with Chronic Hydronephrosis.
In a previous paper we demonstrated that animals with low gradeureteral obstruction gradually develop chronic hydronephrosis.Two such animals remained in good general health for from 4 to 5
kg.
5.8
5.5
6.0
6.7
Date.
1916
Jan. 23*" 24
" 25
" 26
Feb. 19" 20
" 21
Mar. 8" 9
" 10
Apr. 5678
" 20" 21" 22
TABLE IV.
Chronic Hydronephrosis.
ig.
mg.
670680699690
685723724
687713720
629627654685
635646626
ng.
40
25
25
ing.
40
2525
46
53
25
30
25
Urine output.
CC.
210105225265
220208250
225180172
156225170220
190200197
i0
1.0181.0231.0201.020
1.0271.0171.018
1.0161.0181.018
1.0191.0221.0181.022
1.0201.0171.017
Sodium chloride.
.0
gm.
2.141.182.382.65
0.791.582.28
2.211.652.15
1.692.772.032.14
2.402.402.44
gm.
1.021.121.011.00
0.360.760.91
0.870.901.25
1.091.231.200.97
1.261.201.23
O.0
pcr cen
2
28
11
33
28
80
t
gm.
1.630.811.430.99
2.33
2.38
2.012.21
* 2 months since double ureteral obstruction was produced (operation Novem-ber 20, 1915).
Intake 2 gingm. of sodium chloride in 200 cc. of water daily, subcutaneously.
months, although during this entire period definite renal functionalimpairment could be demonstrated. These findings closely agreewith the common clinical experience that patients with obstruction
182
9
W- : -
-- -- --

NORMAN M. IEITH AND D. SCHUYLER PULFORD, JR.
in the lower urinary tract may have comparatively good health formonths or years, even with marked pathologic changes in the kidneysand greatly reduced renal function. In one experiment (Dog 9,Table IV) studies in chloride metabolism were carried out on fiveoccasions for periods of from 3 to 4 days. Food was not given, andsodium chloride and water were administered subcutaneously asoutlined. In only two of these periods (February and March)were the total chloride excretion and concentration in the urine defi-nitely reduced, and associated with this decreased chloride outputthe plasma chlorides showed a moderate rise. During the periodsof study in January and April the plasma chloride content and theurinary output and concentration were within normal limits. Thusat the end of this experiment in April, in which renal function hadbeen impaired for 5 months and marked anatomic changes had de-veloped in the kidneys, 2 the chloride metabolism as evidenced by theconcentration in the blood plasma and the total urinary output wasnormal. The concentration of the chlorides in the urine at this timetended to be somewhat low and uniform, but still above the minimalconcentration noted in the series of normal controls under the sameexperimental conditions. It is an interesting fact that this dogexcreted constantly a large volume of urine.
DISCUSSION.
The results obtained in these experiments emphasize the closerelationship between the water and chloride equilibrium in the animalorganism. With a constant moderate intake of water and sodiumchloride, as administered in the control experiments, the chloridecontent of the plasma and the daily renal excretion of water andchlorides remain remarkably constant. This constancy of the chloridebalance under normal conditions was the basis of the work of Ambardand Weill when they introduced their threshold formula for theexcretion of chlorides. When this finely adjusted mechanism isdisturbed by renal injury, as in these experiments by an acute orchronic hydronephrosis, the close interrelationship between the water
2 See Keith, N. M., and Pulford, D. S., Jr., Experimental hydronephrosis.Functional and anatomic changes in the kidney following partial ureteral obstruc-tion, Arch. Int. Med. .1917 xx, 864, Fig. 2.
183
CHLORIDE RETENTION IN HYDRONEPHROSIS
and chloride balance is still evident, but certain distinctly abnormalchanges are brought about. If water and chlorides are equallyretained in the body, the plasma concentration of chlorides will notrise appreciably. This was the case in Dogs 5, 6, and 7 (Table III).Similar results were obtained by Leva in experimental uraniumnephritis. The obvious reason for the rapid increase of the ureacontent of the tissues in spite of the retained water is that urea unlikethe chlorides is being continually produced by the organism in largeamounts. The interesting feature in three of the experiments isthe striking rise in the plasma chloride content following the removalof the ureteral obstruction. This rise is chiefly due to the changesin renal function. The injured kidney has regained the ability toexcrete water and urea readily, but chloride excretion, in contrastto water excretion, lags. The persistent retention of chlorides inthe tissues is then indicated by a high plasma concentration, orthreshold. The subsequent gradual fall in plasma chlorides to thenormal level seems to be directly associated with the recovery of thespecific renal function involved in chloride excretion. The rapidurea excretion after the removal of the ureteral obstruction closelyfollows the output of water. We should expect such a result becauseof the high urea content of the blood and the fact that urea in contrastto the chlorides is a non-threshold substance.
The experiment (Dog 8) furnishes a good example of simple ordry chloride retention. The kidney readily excretes water, but isunable to eliminate an adequate amount of chlorides. The resultingaccumulation of chlorides in the body is indicated by an increasedconcentration in the plasma. Heineke and Meyerstein, Leva, andAustin and Jonas have shown that a similar rise in the blood orplasma chlorides takes place in experimental uranium nephritis whenthe intake of sodium chloride is large, as compared with that of water.Dry chloride retention has also been demonstrated in clinical casesof nephritis by Widal and Lemierre, Ambard and Beaujard, Leva,and others.
When the ureteral obstruction was removed in Dog 8 there was arapid recovery of total renal function including the ability to excretechlorides. The plasma chloride content fell more rapidly than inexperiments on Dogs 5 and 7, but still did not reach the control levelfor several days after the blood urea was normal.
184
NORMAN M. KEITH AND D. SCHUYLER PULFORD, JR.
In the single experiment on chronic hydronephrosis (Dog 9) it issignificant that the chloride metabolism under these experimentalconditions deviated so little from the normal. The constant increasedexcretion of urine, or polyuria, such a common phenomenon in chronicrenal lesions, appears to be the compensating mechanism whichprevents any marked retention of chlorides, urea, or water. Therenal cells in diffuse chronic nephritis work at a maximal excretoryrate during the entire 24 hours, and thus for a time are able to ridthe body of its accumulated excretory products. Probably, if moresodium chloride had been administered in the same volume of waterduring the foregoing experimental periods, a noticeable chlorideretention would have resulted and caused a rise in the plasma chlorides.
In experiments on Dogs 6 and 7 the plasma chlorides do not showany appreciable increase during the initial period. The explanationfor the failure of the plasma chlorides to rise when there was definitechloride retention would appear to be the dilution by the retainedwater of the tissue chlorides as a whole. This explanation might alsoaccount for the low plasma chloride concentration reported byHeineke and Meyerstein in experimental chromate and uraniumnephritis and also in clinical cases of severe renal insufficiency. Inthe latter, low plasma chlorides have been noted by Lewis and Riversin bichloride poisoning, by Major in chromic acid poisoning, and byKeith and Thomson in acute glomerular nephritis. In all these casesoliguria or anuria was present and the intake of fluids was high.
SUMMARY.
1. In acute experimental hydronephrosis chloride retention occursas well as retention of water, urea, and phenolsulfonephthalein.
2. If both water and chlorides are retained there may be no appre-ciable rise in the plasma chloride content.
3. When chlorides are retained, but not water, the chloride contentof the plasma rises strikingly.
4. After the removal of the ureteral obstruction in acute hydro-nephrosis all renal functions, water, urea, and chloride excretion,may be rapidly restored in equal degree, or the chlorides may beretained temporarily while there is free excretion of water and urea.
5. In chronic hydronephrosis adequate daily excretion of urea'andchlorides may be maintained by a compensatory polyuria.
185
CHLORIDE RETENTION IN YDRONEPHROSIS
6. Chloride retention or an abnormal chloride excretion may occurin certain renal lesions when there is no change in the urea, phenol-sulfonephthalein, or water excretion.
BIBLIOGRAPHY.
Ambard, L., and Beaujard, E., La rtention chlorurhe sche, Senaine md.,1905, xxv, 133.
Ambard, L., and Weill, A., La scretion rnale des chlorures, Sermaine med., 1912,xxxii, 217.
Arnold, C., Kurze Methode zur Bestimmung der Chloride im normalen undpathologischen Harne der Sugethiere und Menschen, in der Milch und inserosen Fliissigkeiten, Arch. ges. Physiol., 1885, xxxv, 541.
Austin, J. H., and Jonas, L., Effects of diet upon the plasma chlorides and chlorideexcretion in the dog, J. Biol. Chem., 1918, xxxiii, 91.
Heineke, A., and Meyerstein, W., Experimentelle Untersuchungen fiber denHydrops bei Nierenkrankheiten, Deutsch. Arch. klin. Med., 1907, xc, 101.
Keith, N. M., and Pulford, D. S., Jr., Experimental hydronephrosis. Functionaland anatomic changes in the kidney following partial ureteral obstruction,Arch. Int. Med., 1917, xx, 853.
Keith, N. M., and Thomson, W. W. D., War nephritis. A clinical, functionaland pathological study, Quart. J. Med., 1917-18, xi, 229.
Leva, J., Organuntersuchungen, sowie experimentelle Studien fiber anhydropischeChlorretention, Z. klin. AMed., 1916, lxxxii, 1.
Lewis, D. S., and Rivers, T. N., Chemical studies on a case of bichloride poisoning,Bull. Johns Hopkins Hosp., 1916, xxvii, 193.
McLean, F. C., The numerical laws governing the rate of excretion of urea andchlorides in man. II. The influence of pathological conditions and ofdrugs on excretion, J. Exp. Med., 1915, xxii, 366.
McLean, F. C., and Van Slyke, D. D., A method for the determination of chloridesin small amounts of body fluids, J. Biol. Chem., 1915, xxi, 361.
Major, R. H., Studies on a case of chromic acid nephritis, Bull. Johns HopkinsHosp., 1922, xxxiii, 56.
Marshall, E. K., Jr., A rapid clinical method for the estimation of urea in urine,J. Bio!. Chem., 1913, a, xiv, 283.
Marshall, E. K., Jr., A new method for the determination of urea in blood, J.Biol. Chem., 1913, b, xv, 487.
Rowntree, L. G., and Geraghty, J. T., The phthalein test. An experimental andclinical study of phenolsulfonephthalein in relation to renal function inhealth and disease, Arch. Inzt. Med., 1912, ix, 284.
Widal, F., and Javal, A., La retention de l'ur6e dans le mal de Bright, comparee a laretention des chlorures, Semaine Emd., 1905, xxv, 313.
Widal, F., and Lemierre, A., Pathogenie de certains cedemes brightiques; actiondu chlorure de sodium inghr, Bull. et mam. Soc. fd. hp. Paris, 1903, xx,series 3, 785.
186