chest pain
DESCRIPTION
Chest PainTRANSCRIPT

CHEST PAIN SCENARIO 3GROUP 10
AinLatifahRafikaNunungAishahAmalinaMiqdadHarry
AndhikaFadliNovaRina
SCENARIOA collapse 60 years old bus driver was brought into casualty complaining of severesustained crushing pain in a band across the chest spreading into arms Previously he had been wellthough he smoked 10 cigarettes a day On examination he was pale with coldsweaty skin His pulse was weakwith occasional extrasystole(ventricular ectopic beats) His arterial blood pressure was 9075 mmHg Heart sound were normal An ECG revealed large Q wave and ST segment elevation He was admitted with a provisional diagnosis of myocardial infarction due to coronary artery thrombosis Plasma analysis showed raised cardiac enzymes( lactic dehydrogenasecreatine phosphokinaseaspartate aminotransferase) He was given O2 and morphine A streptokinase infusion was set up to lyse the coronary thrombus and he was also started on regularlow dose aspirin
KEYWORD
bull Collapsebull Severe sustained crushing pain in band across chest
spreading into armbull Previously been wellbull Palecold sweaty skinbull Pulse weak with occasional extrasystolebull Artery BP 9075bull Large Q wave ST elevationbull Plasma analysis raised cardiac enzymes
QUESTIONbull 1) Why the patient suffered a crushing pain that spread to
the armbull 2) Why occasional extrasystole occur (pathomechanism)bull 3) What is the relationship between smoking and occasional
extrasystolebull 4) Indication for large Q wave and ST elevation What are
the relationship of these findings with chest pain bull 5) Indication for increasing cardiac enzymesbull 6) What are the relationship between myocardial infarction
with the symptoms (why he is having weak pulse)
DIFFERENTIAL DIAGNOSISSIGN AND SYMPTOM
STEMI CAD
Crushing pain at chest spreading to arm yes yes
Occasional extrasystol yes no
Large Q wave and ST elevasi yes no
Hypotension yes yes
Provisional diagnosis MI due to coroner arteri trombosis
yes yes
Enzim CKCKMB LDH increase yes no
httpwwwemedicinehealthcomcogestive_heart_failure
INTRODUCTIONbull STEMI ST segment elevation myocardial infarctionldquo is a type of
heart attack This is determined by an ECG test
bull Myocardial infarctions (heart attacks) occur when a coronay artery suddenly becomes at least partially blocked by a blood clot causing at least some of the heart muscle being supplied by that artery to become infarcted (that is to die) Heart attacks are divided into two types according to their severity
bull A STEMI is the more severe type
httpheartdiseaseaboutcom STEMI - ST Segment Elevation Myocardial Infarction By Richard N Fogoros MD
BASIC SCIENCE
EKG
Normal heart
Myocardial InfarctionTwo to three days after an MI the myocytes show that they are irreversibly damaged Theyve lost their nuclei PMNs
(polymorphonuclear leukocytes) are the first inflammatory cells on the scene They will begin to clear away the necrotic tissue Later the macrophages will finish the job These dying myocytes will eventually be replaced with scar tissue
httpwwwkumceduinstructionmedicineanatomyhistowebpathpath01htm
httpwwwgooglecomimgreshl=enampgl=idampbiw=1366ampbih=624amptbm=ischamptbnid=KajG2QEK1-M4mMampimgrefurl=httpwwwmedicinenetcomheart_attack_pathology_photo_essaypage3htmampdocid=CZHmHLYLNv9ueMampimgurl=httpimagesmedicinenetcomimagesillustrationsmyocardial_infarction_1jpgampw=400amph=308ampei=8_KDUK3PH8nlrAeTzYHwBwampzoom=1ampiact=hcampvpx=398ampvpy=128ampdur=3820amphovh=197amphovw=256amptx=206ampty=150ampsig=116867615274730240580amppage=2amptbnh=151amptbnw=196ampstart=21ampndsp=27ampved=1t429r23s20i206
PATHOPHYSIOLOGY OF
ST-ELEVATION MYOCARDIAL
INFARCTION (STEMI)
myocardial infarction
A myocardial infarction is defined as
Elevated blood levels of cardiac enzymes
(CKMB or Troponin T)
One of the following criteria are met
The patient has typical
complaints
The ECG shows ST elevation or
depression
pathological Q waves develop
on the ECG
bull PATHOPHYSIOLOGY MIA prolonged imbalance between myocardial oxygen supply and demand leads to the death of myocardial tissue Coronary
atherosclerosis is an essential part of the process in most patients
Ischemic heart disease seems to progress through stages of fatty-streak deposition in coronary arteries to development of
fibro-fatty plaque which then increases in size until it causes luminal obstruction
leading to exertional angina
any stages in this process the atherosclerotic lesion may erode
ulcerate fissure or rupture thereby exposing subendothelial
vessel wall substances to the circulating blood
Procoagulant factors (such as tissue factor) reside within the plaque itself
and in the absence of counterbalancing antithrombotic factor (eg heparin tissue-factor-
inhibitor) and fibrinolytic activities (tissues plasminogen activator [t-PA]
and single-chain urokinase-type plasminogen activator) within the endothelial cells of the coronary
artery can cause thrombosis Recent work suggests that inflammation may play a pivotal role in
the genesis of plaque rupture Total thrombotic occlusion occurs most commonly in proximal coronary
arteries its presence has been documented during the first 4 hours
after infarction in more than 85 of the patients with ST segment elevation
(Crawford MH (2009))
This potent procoagulant stimulus results in thrombus development in
this region In general acute MI occurs when this thrombosis
propagates and occludes flow within the artery resulting in ischemia of
cardiomyocytes distal to the obstruction
The ECG leads in which pathologic Q waves appear reflect the anatomical site of an infarction
TABLE 1 Localization of Myocardial Infarction Anatomical Site Leads with Abnormal ECG
Complexes Coronary Artery Most Often
Responsible Inferior IIIIIaVF RCA
Anteroseptal V1-V2 LAD Anteroapical V3-V4 LAD(distal) Anterolateral V5-V6 I aVL CFX
Posterior V1-V2 (tall R wave not Q wave) RCA
The electrocardiographic differences between these types of MI are summarized as follow
Type of Infarction Pathologic Q waves Acute ST segment Deviation
Q-wave MI Yes ST elevation Non-Q-wave MI No ST depression (and or T
wave inversion)
Angina pectoris- Neck- Shoulder- Arms
ischemic myocardial cells release mediator such as adenosine and
lactate from into local nerve endings
discomfort often refer to other region of the C7 through
dermatome
provocative substances continue to accumulate and active afferent
nerve for longer period
ischemic in acute MI persist and proceed to necrosis
HYPOTENSION
May trigger a dramatic sympathetic nervous system response
Systemic sign of subsequent catecholamine release include diaphoresis (sweating) tachycardia and cool
and clammy skin
cause of vasoconstriction
Systolic Dysfunction
Decrease lungs compliance and stimulates juxtacappilary
receptors
Left ventricle contractility can be
reduced
J receptors effects a reflex that results in rapid shallow
breathing and evokes the subjective feeling of dyspnea
Increase in LV pressure compounded by the ischemia
induced stiffness of the chamber (diastolic dysfunction) is conveyed to the left atrium and pulmonary
veins
Decreasing the stroke volume and causing the diastolic
volume and pressure within the LV to rise
Ischemia affects large amount of myocardium
SERUM MARKER OF INFARCTION
Detection of cardiac-specific troponins and creatine kinase MB isoenzyme
Intracellular macromolecules leak into the cardiac interstitium and ultimately into the bloodstream
Necrosis of myocardial tissue Cause by disruption of the sarcolemma
MYOCARDIAL INFARTION
TYPICAL SYMPTOM- Crushing chest pain
more severe and wider than usual angina
SERUM BIOMARKSCreatine kinaseTroponin
ECG initial finding- St elevation- Q Wave
STEMI
Left Ventricular Function Systolic Function
Upon interruption of antegrade flow in an epicardial coronary artery the zone of myocardium supplied by that vessel immediately loses its ability to shorten and perform contractile work Four abnormal contraction patterns develop in sequence (1) dyssynchrony that is dissociation in the time course of contraction of adjacent segments(2) hypokinesis reduction in the extent of shortening (3) akinesis cessation of shortening and (4) dyskinesis paradoxical expansion and systolic bulging
Hyperkinesis of the remaining normal myocardium initially accompanies dysfunction of the infarcting segment The early hyperkinesis of the noninfarcted zones likely results from acute compensations including increased activity of the sympathetic nervous system and the Frank-Starling mechanism A portion of this compensatory hyperkinesis is ineffective work because contraction of the noninfarcted segments of myocardium hellip
Ventricular Remodelingbull As a consequence of STEMI the changes in left ventricular size shape and
thickness involving both the infarcted and the noninfarcted segments of the ventricle described earlier occur and are collectively referred to as ventricular remodeling which can in turn influence ventricular function and prognosis
bull A combination of changes in left ventricular dilation and hypertrophy of residual noninfarcted myocardium causes remodeling
bull After the size of infarction the two most important factors driving the process of left ventricular dilation are ventricular loading conditions and infarct artery patency
bull Elevated ventricular pressure contributes to increased wall stress and the risk of infarct expansion and a patent infarct artery accelerates myocardial scar formation and increases tissue turgor in the infarct zone reducing the risk of infarct expansion and ventricular dilation
Antman EM Morrow DA McCabe CH et al Enoxaparin versus unfractionated heparin with fibrinolysis for ST-elevation myocardial infarction N Engl J Med 2006 3541477
referencesSLIDE 2 Alpert JS Thygesen K Antman E and Bassand JP Myocardial infarction redefined--a consensus document of The Joint European Society of CardiologyAmerican College of Cardiology Committee for the redefinition of myocardial infarction J Am Coll Cardiol 2000 Sep 36(3) 959-69 pmid10987628bull Book of Pathophysiology of Heart Disease fourth edition editor Leonard SLilly page 179-
184bull ILMU PENYAKIT DALAM Jilid II Edisi V Editor Aru WSudoyo Bambang Setiyohadi
Idrus Alwi page1741-1744
ST elevation MI
ST segment elevation type of acute myocardial infarction require at least 1 mm (01 mV) of ST segment elevation in the limb leads and at least 2 mm elevation in the precordial leads
The clinician must therefore be well versed in recognizing the so-called ECG mimics of acute myocardial infarction which include
These elevations must be present in anatomically contiguous leads (I aVL V5 V6 correspond to the lateral wall V1-V2 correspond to the septal wall V3-V4 correspond to the anterior wall II III aVF correspond to the inferior wall)
left ventricular hypertrophy
left bundle branch block
hyperkalemia
early repolarization
ventricular aneurysm
12-lead electrocardiogram showing ST-segment elevation (orange) in I aVL and V1-V5 with reciprocal changes (blue) in the inferior leads indicative of an anterior wall myocardial infarction
An acute STEMI involving the inferior and right ventricular wall Reciprocal changes are seen in the anterior leads
PATHOLOGIC OF Q-WAVEPathologic Q waves
Any Q-wave in leads V2ndashV3 ge 002 s or QS complex in leads V2 and V3
Q-wave ge 003 s and gt 01 mV deep or QS complex in leads I II aVL aVF or V4ndashV6 in
any two leads of a contiguous lead grouping (I aVLV6 V4ndashV6 II III and aVF)
result of absence of electrical activity
previous myocardial infarction
The evolution of an infarct on the ECG ST elevation Q wave formation T wave inversion
normalisation with a persistent Q wave
PATHOMECANISM CHEST PAINhttpemedicinemedscapecomarticle150215-overview2
ProfDrPeter Kabo Bagaimana Menggunakan Obat-obat kardiovasculer secara Rasional
AtherosclerosisProduce endothelial derived constricting
factor (EDCF)
Increase tonus artery
coronary
Ischemic myocard
Aerobic glycolysis turn
to anerobic glycolysis
Production of adenosin
Diffuse to extracellular
space
Stimulate A1 receptor in cardiac
afferent nerve ending
Bind with somatic cervico
thoracalis nerve at
ascending pathway in
medulla spinalis
Chest pain
SMOKING KILLS
These effects could potentially trigger
symptoms of ischemia in such smokers
One might also expect that the hemodynamic effects of nicotine would contribute to endothelial damage and accelerate the progression of atherosclerosis
Lipolyis - increased levels of circulating free fatty acids
and glycerol in the blood and the resulting increase in fat
metabolism drives a demand for more oxygen leading to
increased coronary blood flow and myocardial oxygen
uptake
addition to its cardiovascular effects such as elevated heart
rate blood pressure and cardiac output
nicotine has metabolic effects in particular increased lipolysis
Nicotine is a sympathomimetic chemical that promotes the release of catecholamines and other
neurotransmitters
SIGNS AND SYMPTOMS
bullChest pain (pressuretightnessheaviness and might radiate to neck arm)
bullIngestion heartburnbullNausea VomitingbullSweatingbullWeaknessbullDizziness
httpwwwcardiosmartorgManageConditionDefaultaspxid=904 httpwwwncbinlmnihgovpmcarticlesPMC2233977
ADDITIONAL EXAMINATION1 Physical examination
Gen appearance Distress Levine signbullHeart rate pulse respirrate variablebullBlood pressure variablebullLow-grade feverbullExamination of jugular venous pulsationsbullPulmonary CracklesbullS4 gallop due to reduced LV compliancebullS3 gallop if LV dysfunction presentbullMurmurs Pericardial friction rubs
2 ECG
The key to rapid diagnosis and risk stratification for the patient with chest painbullTo be obtained within 10 minutes of arrival to Emergency DepartmentbullFor STEMI 1048774ST-segment elevation gt1mm in 2+ contiguous leads OR new left bundle branch block (LBBB)bullLocation of InfarctLeadsInferior MI II III aVFAnterior MI V2-V4Lateral MI I aVL V5-V6
3 Lab studies
Cardiac Biomarkers CK CK-MB cTnbullSerum ChemistriesbullRenal FunctionbullCoagulation StudiesbullComplete Blood Count
TREATMENTAspirin
bullRapidly blocks formation of thromboxaneA2 in platelets by cyclooxygenase inhibitionbull162-325mg chewed (promotes buccalabsorption)bullISIS-2ndash23 reduction in mortality largely additive to the reduction in mortality from streptokinaseOther Adjuvant TherapiesAnalgesicsbullNitratesbullBeta-blockersbullAce InhibitorsbullOxygenbullHeparinbullIV Glycoprotein IIbIIIaInhibitorsbullClopidogrelbullStatins
Thrombolytic TherapybullCommon AgentsbullTNK-tPA30-50mg IV bolusbullReteplase10U x 2 (each over 2 minutes) IVbullAlteplaseup to 100mg in 90mins (based on weight)
bullContraindicationsndashAbsolute Prior intracranial hemorrhage known cerebral vascular lesion malignant intracranial neoplasm ischemic stroke within 3 months suspected aortic dissection active bleeding recent closed head injury or facial trauma within 3monthsndashRelative History of chronic severe HTN severeuncontrolled HTN at presentation (gt180110) history of ischemic stroke gt3 months traumaticprolonged CPR recent internal bleeding (2-4 weeks) pregnancy active peptic ulcer current anticoagulation
Primary PCI
bullPCI = Percutaneous Coronary Intervention
bullPTCA = Percutaneous Transluminal Coronary Angioplasty
bullPOBA = Plain Old Balloon Angioplasty
PROGNOSIS
bullDischarge usually 5 days after admissionbullSmoking CessationbullShort and Long-term survival depend upon resting LV function residual ischemic myocardium and susceptibility to ventricular arrhythmias
THE END
- CHEST PAIN SCENARIO 3 GROUP 10
- SCENARIO
- KEYWORD
- QUESTION
- DIFFERENTIAL DIAGNOSIS
- INTRODUCTION
- BASIC SCIENCE
- EKG
- Normal heart
- Myocardial Infarction Two to three days after an MI the myocyt
- Slide 11
- PATHOPHYSIOLOGY OF ST-ELEVATION MYOCARDIAL INFARCTION (STEMI)
- myocardial infarction
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- HYPOTENSION May trigger a dramatic sympathetic nervous system
- Slide 19
- Slide 21
- Left Ventricular Function Systolic Function
- Ventricular Remodeling
- references
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- PATHOLOGIC OF Q-WAVE
- PATHOMECANISM CHEST PAIN
- Slide 31
- SMOKING kills
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- ThE eND
-

SCENARIOA collapse 60 years old bus driver was brought into casualty complaining of severesustained crushing pain in a band across the chest spreading into arms Previously he had been wellthough he smoked 10 cigarettes a day On examination he was pale with coldsweaty skin His pulse was weakwith occasional extrasystole(ventricular ectopic beats) His arterial blood pressure was 9075 mmHg Heart sound were normal An ECG revealed large Q wave and ST segment elevation He was admitted with a provisional diagnosis of myocardial infarction due to coronary artery thrombosis Plasma analysis showed raised cardiac enzymes( lactic dehydrogenasecreatine phosphokinaseaspartate aminotransferase) He was given O2 and morphine A streptokinase infusion was set up to lyse the coronary thrombus and he was also started on regularlow dose aspirin
KEYWORD
bull Collapsebull Severe sustained crushing pain in band across chest
spreading into armbull Previously been wellbull Palecold sweaty skinbull Pulse weak with occasional extrasystolebull Artery BP 9075bull Large Q wave ST elevationbull Plasma analysis raised cardiac enzymes
QUESTIONbull 1) Why the patient suffered a crushing pain that spread to
the armbull 2) Why occasional extrasystole occur (pathomechanism)bull 3) What is the relationship between smoking and occasional
extrasystolebull 4) Indication for large Q wave and ST elevation What are
the relationship of these findings with chest pain bull 5) Indication for increasing cardiac enzymesbull 6) What are the relationship between myocardial infarction
with the symptoms (why he is having weak pulse)
DIFFERENTIAL DIAGNOSISSIGN AND SYMPTOM
STEMI CAD
Crushing pain at chest spreading to arm yes yes
Occasional extrasystol yes no
Large Q wave and ST elevasi yes no
Hypotension yes yes
Provisional diagnosis MI due to coroner arteri trombosis
yes yes
Enzim CKCKMB LDH increase yes no
httpwwwemedicinehealthcomcogestive_heart_failure
INTRODUCTIONbull STEMI ST segment elevation myocardial infarctionldquo is a type of
heart attack This is determined by an ECG test
bull Myocardial infarctions (heart attacks) occur when a coronay artery suddenly becomes at least partially blocked by a blood clot causing at least some of the heart muscle being supplied by that artery to become infarcted (that is to die) Heart attacks are divided into two types according to their severity
bull A STEMI is the more severe type
httpheartdiseaseaboutcom STEMI - ST Segment Elevation Myocardial Infarction By Richard N Fogoros MD
BASIC SCIENCE
EKG
Normal heart
Myocardial InfarctionTwo to three days after an MI the myocytes show that they are irreversibly damaged Theyve lost their nuclei PMNs
(polymorphonuclear leukocytes) are the first inflammatory cells on the scene They will begin to clear away the necrotic tissue Later the macrophages will finish the job These dying myocytes will eventually be replaced with scar tissue
httpwwwkumceduinstructionmedicineanatomyhistowebpathpath01htm
httpwwwgooglecomimgreshl=enampgl=idampbiw=1366ampbih=624amptbm=ischamptbnid=KajG2QEK1-M4mMampimgrefurl=httpwwwmedicinenetcomheart_attack_pathology_photo_essaypage3htmampdocid=CZHmHLYLNv9ueMampimgurl=httpimagesmedicinenetcomimagesillustrationsmyocardial_infarction_1jpgampw=400amph=308ampei=8_KDUK3PH8nlrAeTzYHwBwampzoom=1ampiact=hcampvpx=398ampvpy=128ampdur=3820amphovh=197amphovw=256amptx=206ampty=150ampsig=116867615274730240580amppage=2amptbnh=151amptbnw=196ampstart=21ampndsp=27ampved=1t429r23s20i206
PATHOPHYSIOLOGY OF
ST-ELEVATION MYOCARDIAL
INFARCTION (STEMI)
myocardial infarction
A myocardial infarction is defined as
Elevated blood levels of cardiac enzymes
(CKMB or Troponin T)
One of the following criteria are met
The patient has typical
complaints
The ECG shows ST elevation or
depression
pathological Q waves develop
on the ECG
bull PATHOPHYSIOLOGY MIA prolonged imbalance between myocardial oxygen supply and demand leads to the death of myocardial tissue Coronary
atherosclerosis is an essential part of the process in most patients
Ischemic heart disease seems to progress through stages of fatty-streak deposition in coronary arteries to development of
fibro-fatty plaque which then increases in size until it causes luminal obstruction
leading to exertional angina
any stages in this process the atherosclerotic lesion may erode
ulcerate fissure or rupture thereby exposing subendothelial
vessel wall substances to the circulating blood
Procoagulant factors (such as tissue factor) reside within the plaque itself
and in the absence of counterbalancing antithrombotic factor (eg heparin tissue-factor-
inhibitor) and fibrinolytic activities (tissues plasminogen activator [t-PA]
and single-chain urokinase-type plasminogen activator) within the endothelial cells of the coronary
artery can cause thrombosis Recent work suggests that inflammation may play a pivotal role in
the genesis of plaque rupture Total thrombotic occlusion occurs most commonly in proximal coronary
arteries its presence has been documented during the first 4 hours
after infarction in more than 85 of the patients with ST segment elevation
(Crawford MH (2009))
This potent procoagulant stimulus results in thrombus development in
this region In general acute MI occurs when this thrombosis
propagates and occludes flow within the artery resulting in ischemia of
cardiomyocytes distal to the obstruction
The ECG leads in which pathologic Q waves appear reflect the anatomical site of an infarction
TABLE 1 Localization of Myocardial Infarction Anatomical Site Leads with Abnormal ECG
Complexes Coronary Artery Most Often
Responsible Inferior IIIIIaVF RCA
Anteroseptal V1-V2 LAD Anteroapical V3-V4 LAD(distal) Anterolateral V5-V6 I aVL CFX
Posterior V1-V2 (tall R wave not Q wave) RCA
The electrocardiographic differences between these types of MI are summarized as follow
Type of Infarction Pathologic Q waves Acute ST segment Deviation
Q-wave MI Yes ST elevation Non-Q-wave MI No ST depression (and or T
wave inversion)
Angina pectoris- Neck- Shoulder- Arms
ischemic myocardial cells release mediator such as adenosine and
lactate from into local nerve endings
discomfort often refer to other region of the C7 through
dermatome
provocative substances continue to accumulate and active afferent
nerve for longer period
ischemic in acute MI persist and proceed to necrosis
HYPOTENSION
May trigger a dramatic sympathetic nervous system response
Systemic sign of subsequent catecholamine release include diaphoresis (sweating) tachycardia and cool
and clammy skin
cause of vasoconstriction
Systolic Dysfunction
Decrease lungs compliance and stimulates juxtacappilary
receptors
Left ventricle contractility can be
reduced
J receptors effects a reflex that results in rapid shallow
breathing and evokes the subjective feeling of dyspnea
Increase in LV pressure compounded by the ischemia
induced stiffness of the chamber (diastolic dysfunction) is conveyed to the left atrium and pulmonary
veins
Decreasing the stroke volume and causing the diastolic
volume and pressure within the LV to rise
Ischemia affects large amount of myocardium
SERUM MARKER OF INFARCTION
Detection of cardiac-specific troponins and creatine kinase MB isoenzyme
Intracellular macromolecules leak into the cardiac interstitium and ultimately into the bloodstream
Necrosis of myocardial tissue Cause by disruption of the sarcolemma
MYOCARDIAL INFARTION
TYPICAL SYMPTOM- Crushing chest pain
more severe and wider than usual angina
SERUM BIOMARKSCreatine kinaseTroponin
ECG initial finding- St elevation- Q Wave
STEMI
Left Ventricular Function Systolic Function
Upon interruption of antegrade flow in an epicardial coronary artery the zone of myocardium supplied by that vessel immediately loses its ability to shorten and perform contractile work Four abnormal contraction patterns develop in sequence (1) dyssynchrony that is dissociation in the time course of contraction of adjacent segments(2) hypokinesis reduction in the extent of shortening (3) akinesis cessation of shortening and (4) dyskinesis paradoxical expansion and systolic bulging
Hyperkinesis of the remaining normal myocardium initially accompanies dysfunction of the infarcting segment The early hyperkinesis of the noninfarcted zones likely results from acute compensations including increased activity of the sympathetic nervous system and the Frank-Starling mechanism A portion of this compensatory hyperkinesis is ineffective work because contraction of the noninfarcted segments of myocardium hellip
Ventricular Remodelingbull As a consequence of STEMI the changes in left ventricular size shape and
thickness involving both the infarcted and the noninfarcted segments of the ventricle described earlier occur and are collectively referred to as ventricular remodeling which can in turn influence ventricular function and prognosis
bull A combination of changes in left ventricular dilation and hypertrophy of residual noninfarcted myocardium causes remodeling
bull After the size of infarction the two most important factors driving the process of left ventricular dilation are ventricular loading conditions and infarct artery patency
bull Elevated ventricular pressure contributes to increased wall stress and the risk of infarct expansion and a patent infarct artery accelerates myocardial scar formation and increases tissue turgor in the infarct zone reducing the risk of infarct expansion and ventricular dilation
Antman EM Morrow DA McCabe CH et al Enoxaparin versus unfractionated heparin with fibrinolysis for ST-elevation myocardial infarction N Engl J Med 2006 3541477
referencesSLIDE 2 Alpert JS Thygesen K Antman E and Bassand JP Myocardial infarction redefined--a consensus document of The Joint European Society of CardiologyAmerican College of Cardiology Committee for the redefinition of myocardial infarction J Am Coll Cardiol 2000 Sep 36(3) 959-69 pmid10987628bull Book of Pathophysiology of Heart Disease fourth edition editor Leonard SLilly page 179-
184bull ILMU PENYAKIT DALAM Jilid II Edisi V Editor Aru WSudoyo Bambang Setiyohadi
Idrus Alwi page1741-1744
ST elevation MI
ST segment elevation type of acute myocardial infarction require at least 1 mm (01 mV) of ST segment elevation in the limb leads and at least 2 mm elevation in the precordial leads
The clinician must therefore be well versed in recognizing the so-called ECG mimics of acute myocardial infarction which include
These elevations must be present in anatomically contiguous leads (I aVL V5 V6 correspond to the lateral wall V1-V2 correspond to the septal wall V3-V4 correspond to the anterior wall II III aVF correspond to the inferior wall)
left ventricular hypertrophy
left bundle branch block
hyperkalemia
early repolarization
ventricular aneurysm
12-lead electrocardiogram showing ST-segment elevation (orange) in I aVL and V1-V5 with reciprocal changes (blue) in the inferior leads indicative of an anterior wall myocardial infarction
An acute STEMI involving the inferior and right ventricular wall Reciprocal changes are seen in the anterior leads
PATHOLOGIC OF Q-WAVEPathologic Q waves
Any Q-wave in leads V2ndashV3 ge 002 s or QS complex in leads V2 and V3
Q-wave ge 003 s and gt 01 mV deep or QS complex in leads I II aVL aVF or V4ndashV6 in
any two leads of a contiguous lead grouping (I aVLV6 V4ndashV6 II III and aVF)
result of absence of electrical activity
previous myocardial infarction
The evolution of an infarct on the ECG ST elevation Q wave formation T wave inversion
normalisation with a persistent Q wave
PATHOMECANISM CHEST PAINhttpemedicinemedscapecomarticle150215-overview2
ProfDrPeter Kabo Bagaimana Menggunakan Obat-obat kardiovasculer secara Rasional
AtherosclerosisProduce endothelial derived constricting
factor (EDCF)
Increase tonus artery
coronary
Ischemic myocard
Aerobic glycolysis turn
to anerobic glycolysis
Production of adenosin
Diffuse to extracellular
space
Stimulate A1 receptor in cardiac
afferent nerve ending
Bind with somatic cervico
thoracalis nerve at
ascending pathway in
medulla spinalis
Chest pain
SMOKING KILLS
These effects could potentially trigger
symptoms of ischemia in such smokers
One might also expect that the hemodynamic effects of nicotine would contribute to endothelial damage and accelerate the progression of atherosclerosis
Lipolyis - increased levels of circulating free fatty acids
and glycerol in the blood and the resulting increase in fat
metabolism drives a demand for more oxygen leading to
increased coronary blood flow and myocardial oxygen
uptake
addition to its cardiovascular effects such as elevated heart
rate blood pressure and cardiac output
nicotine has metabolic effects in particular increased lipolysis
Nicotine is a sympathomimetic chemical that promotes the release of catecholamines and other
neurotransmitters
SIGNS AND SYMPTOMS
bullChest pain (pressuretightnessheaviness and might radiate to neck arm)
bullIngestion heartburnbullNausea VomitingbullSweatingbullWeaknessbullDizziness
httpwwwcardiosmartorgManageConditionDefaultaspxid=904 httpwwwncbinlmnihgovpmcarticlesPMC2233977
ADDITIONAL EXAMINATION1 Physical examination
Gen appearance Distress Levine signbullHeart rate pulse respirrate variablebullBlood pressure variablebullLow-grade feverbullExamination of jugular venous pulsationsbullPulmonary CracklesbullS4 gallop due to reduced LV compliancebullS3 gallop if LV dysfunction presentbullMurmurs Pericardial friction rubs
2 ECG
The key to rapid diagnosis and risk stratification for the patient with chest painbullTo be obtained within 10 minutes of arrival to Emergency DepartmentbullFor STEMI 1048774ST-segment elevation gt1mm in 2+ contiguous leads OR new left bundle branch block (LBBB)bullLocation of InfarctLeadsInferior MI II III aVFAnterior MI V2-V4Lateral MI I aVL V5-V6
3 Lab studies
Cardiac Biomarkers CK CK-MB cTnbullSerum ChemistriesbullRenal FunctionbullCoagulation StudiesbullComplete Blood Count
TREATMENTAspirin
bullRapidly blocks formation of thromboxaneA2 in platelets by cyclooxygenase inhibitionbull162-325mg chewed (promotes buccalabsorption)bullISIS-2ndash23 reduction in mortality largely additive to the reduction in mortality from streptokinaseOther Adjuvant TherapiesAnalgesicsbullNitratesbullBeta-blockersbullAce InhibitorsbullOxygenbullHeparinbullIV Glycoprotein IIbIIIaInhibitorsbullClopidogrelbullStatins
Thrombolytic TherapybullCommon AgentsbullTNK-tPA30-50mg IV bolusbullReteplase10U x 2 (each over 2 minutes) IVbullAlteplaseup to 100mg in 90mins (based on weight)
bullContraindicationsndashAbsolute Prior intracranial hemorrhage known cerebral vascular lesion malignant intracranial neoplasm ischemic stroke within 3 months suspected aortic dissection active bleeding recent closed head injury or facial trauma within 3monthsndashRelative History of chronic severe HTN severeuncontrolled HTN at presentation (gt180110) history of ischemic stroke gt3 months traumaticprolonged CPR recent internal bleeding (2-4 weeks) pregnancy active peptic ulcer current anticoagulation
Primary PCI
bullPCI = Percutaneous Coronary Intervention
bullPTCA = Percutaneous Transluminal Coronary Angioplasty
bullPOBA = Plain Old Balloon Angioplasty
PROGNOSIS
bullDischarge usually 5 days after admissionbullSmoking CessationbullShort and Long-term survival depend upon resting LV function residual ischemic myocardium and susceptibility to ventricular arrhythmias
THE END
- CHEST PAIN SCENARIO 3 GROUP 10
- SCENARIO
- KEYWORD
- QUESTION
- DIFFERENTIAL DIAGNOSIS
- INTRODUCTION
- BASIC SCIENCE
- EKG
- Normal heart
- Myocardial Infarction Two to three days after an MI the myocyt
- Slide 11
- PATHOPHYSIOLOGY OF ST-ELEVATION MYOCARDIAL INFARCTION (STEMI)
- myocardial infarction
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- HYPOTENSION May trigger a dramatic sympathetic nervous system
- Slide 19
- Slide 21
- Left Ventricular Function Systolic Function
- Ventricular Remodeling
- references
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- PATHOLOGIC OF Q-WAVE
- PATHOMECANISM CHEST PAIN
- Slide 31
- SMOKING kills
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- ThE eND
-

KEYWORD
bull Collapsebull Severe sustained crushing pain in band across chest
spreading into armbull Previously been wellbull Palecold sweaty skinbull Pulse weak with occasional extrasystolebull Artery BP 9075bull Large Q wave ST elevationbull Plasma analysis raised cardiac enzymes
QUESTIONbull 1) Why the patient suffered a crushing pain that spread to
the armbull 2) Why occasional extrasystole occur (pathomechanism)bull 3) What is the relationship between smoking and occasional
extrasystolebull 4) Indication for large Q wave and ST elevation What are
the relationship of these findings with chest pain bull 5) Indication for increasing cardiac enzymesbull 6) What are the relationship between myocardial infarction
with the symptoms (why he is having weak pulse)
DIFFERENTIAL DIAGNOSISSIGN AND SYMPTOM
STEMI CAD
Crushing pain at chest spreading to arm yes yes
Occasional extrasystol yes no
Large Q wave and ST elevasi yes no
Hypotension yes yes
Provisional diagnosis MI due to coroner arteri trombosis
yes yes
Enzim CKCKMB LDH increase yes no
httpwwwemedicinehealthcomcogestive_heart_failure
INTRODUCTIONbull STEMI ST segment elevation myocardial infarctionldquo is a type of
heart attack This is determined by an ECG test
bull Myocardial infarctions (heart attacks) occur when a coronay artery suddenly becomes at least partially blocked by a blood clot causing at least some of the heart muscle being supplied by that artery to become infarcted (that is to die) Heart attacks are divided into two types according to their severity
bull A STEMI is the more severe type
httpheartdiseaseaboutcom STEMI - ST Segment Elevation Myocardial Infarction By Richard N Fogoros MD
BASIC SCIENCE
EKG
Normal heart
Myocardial InfarctionTwo to three days after an MI the myocytes show that they are irreversibly damaged Theyve lost their nuclei PMNs
(polymorphonuclear leukocytes) are the first inflammatory cells on the scene They will begin to clear away the necrotic tissue Later the macrophages will finish the job These dying myocytes will eventually be replaced with scar tissue
httpwwwkumceduinstructionmedicineanatomyhistowebpathpath01htm
httpwwwgooglecomimgreshl=enampgl=idampbiw=1366ampbih=624amptbm=ischamptbnid=KajG2QEK1-M4mMampimgrefurl=httpwwwmedicinenetcomheart_attack_pathology_photo_essaypage3htmampdocid=CZHmHLYLNv9ueMampimgurl=httpimagesmedicinenetcomimagesillustrationsmyocardial_infarction_1jpgampw=400amph=308ampei=8_KDUK3PH8nlrAeTzYHwBwampzoom=1ampiact=hcampvpx=398ampvpy=128ampdur=3820amphovh=197amphovw=256amptx=206ampty=150ampsig=116867615274730240580amppage=2amptbnh=151amptbnw=196ampstart=21ampndsp=27ampved=1t429r23s20i206
PATHOPHYSIOLOGY OF
ST-ELEVATION MYOCARDIAL
INFARCTION (STEMI)
myocardial infarction
A myocardial infarction is defined as
Elevated blood levels of cardiac enzymes
(CKMB or Troponin T)
One of the following criteria are met
The patient has typical
complaints
The ECG shows ST elevation or
depression
pathological Q waves develop
on the ECG
bull PATHOPHYSIOLOGY MIA prolonged imbalance between myocardial oxygen supply and demand leads to the death of myocardial tissue Coronary
atherosclerosis is an essential part of the process in most patients
Ischemic heart disease seems to progress through stages of fatty-streak deposition in coronary arteries to development of
fibro-fatty plaque which then increases in size until it causes luminal obstruction
leading to exertional angina
any stages in this process the atherosclerotic lesion may erode
ulcerate fissure or rupture thereby exposing subendothelial
vessel wall substances to the circulating blood
Procoagulant factors (such as tissue factor) reside within the plaque itself
and in the absence of counterbalancing antithrombotic factor (eg heparin tissue-factor-
inhibitor) and fibrinolytic activities (tissues plasminogen activator [t-PA]
and single-chain urokinase-type plasminogen activator) within the endothelial cells of the coronary
artery can cause thrombosis Recent work suggests that inflammation may play a pivotal role in
the genesis of plaque rupture Total thrombotic occlusion occurs most commonly in proximal coronary
arteries its presence has been documented during the first 4 hours
after infarction in more than 85 of the patients with ST segment elevation
(Crawford MH (2009))
This potent procoagulant stimulus results in thrombus development in
this region In general acute MI occurs when this thrombosis
propagates and occludes flow within the artery resulting in ischemia of
cardiomyocytes distal to the obstruction
The ECG leads in which pathologic Q waves appear reflect the anatomical site of an infarction
TABLE 1 Localization of Myocardial Infarction Anatomical Site Leads with Abnormal ECG
Complexes Coronary Artery Most Often
Responsible Inferior IIIIIaVF RCA
Anteroseptal V1-V2 LAD Anteroapical V3-V4 LAD(distal) Anterolateral V5-V6 I aVL CFX
Posterior V1-V2 (tall R wave not Q wave) RCA
The electrocardiographic differences between these types of MI are summarized as follow
Type of Infarction Pathologic Q waves Acute ST segment Deviation
Q-wave MI Yes ST elevation Non-Q-wave MI No ST depression (and or T
wave inversion)
Angina pectoris- Neck- Shoulder- Arms
ischemic myocardial cells release mediator such as adenosine and
lactate from into local nerve endings
discomfort often refer to other region of the C7 through
dermatome
provocative substances continue to accumulate and active afferent
nerve for longer period
ischemic in acute MI persist and proceed to necrosis
HYPOTENSION
May trigger a dramatic sympathetic nervous system response
Systemic sign of subsequent catecholamine release include diaphoresis (sweating) tachycardia and cool
and clammy skin
cause of vasoconstriction
Systolic Dysfunction
Decrease lungs compliance and stimulates juxtacappilary
receptors
Left ventricle contractility can be
reduced
J receptors effects a reflex that results in rapid shallow
breathing and evokes the subjective feeling of dyspnea
Increase in LV pressure compounded by the ischemia
induced stiffness of the chamber (diastolic dysfunction) is conveyed to the left atrium and pulmonary
veins
Decreasing the stroke volume and causing the diastolic
volume and pressure within the LV to rise
Ischemia affects large amount of myocardium
SERUM MARKER OF INFARCTION
Detection of cardiac-specific troponins and creatine kinase MB isoenzyme
Intracellular macromolecules leak into the cardiac interstitium and ultimately into the bloodstream
Necrosis of myocardial tissue Cause by disruption of the sarcolemma
MYOCARDIAL INFARTION
TYPICAL SYMPTOM- Crushing chest pain
more severe and wider than usual angina
SERUM BIOMARKSCreatine kinaseTroponin
ECG initial finding- St elevation- Q Wave
STEMI
Left Ventricular Function Systolic Function
Upon interruption of antegrade flow in an epicardial coronary artery the zone of myocardium supplied by that vessel immediately loses its ability to shorten and perform contractile work Four abnormal contraction patterns develop in sequence (1) dyssynchrony that is dissociation in the time course of contraction of adjacent segments(2) hypokinesis reduction in the extent of shortening (3) akinesis cessation of shortening and (4) dyskinesis paradoxical expansion and systolic bulging
Hyperkinesis of the remaining normal myocardium initially accompanies dysfunction of the infarcting segment The early hyperkinesis of the noninfarcted zones likely results from acute compensations including increased activity of the sympathetic nervous system and the Frank-Starling mechanism A portion of this compensatory hyperkinesis is ineffective work because contraction of the noninfarcted segments of myocardium hellip
Ventricular Remodelingbull As a consequence of STEMI the changes in left ventricular size shape and
thickness involving both the infarcted and the noninfarcted segments of the ventricle described earlier occur and are collectively referred to as ventricular remodeling which can in turn influence ventricular function and prognosis
bull A combination of changes in left ventricular dilation and hypertrophy of residual noninfarcted myocardium causes remodeling
bull After the size of infarction the two most important factors driving the process of left ventricular dilation are ventricular loading conditions and infarct artery patency
bull Elevated ventricular pressure contributes to increased wall stress and the risk of infarct expansion and a patent infarct artery accelerates myocardial scar formation and increases tissue turgor in the infarct zone reducing the risk of infarct expansion and ventricular dilation
Antman EM Morrow DA McCabe CH et al Enoxaparin versus unfractionated heparin with fibrinolysis for ST-elevation myocardial infarction N Engl J Med 2006 3541477
referencesSLIDE 2 Alpert JS Thygesen K Antman E and Bassand JP Myocardial infarction redefined--a consensus document of The Joint European Society of CardiologyAmerican College of Cardiology Committee for the redefinition of myocardial infarction J Am Coll Cardiol 2000 Sep 36(3) 959-69 pmid10987628bull Book of Pathophysiology of Heart Disease fourth edition editor Leonard SLilly page 179-
184bull ILMU PENYAKIT DALAM Jilid II Edisi V Editor Aru WSudoyo Bambang Setiyohadi
Idrus Alwi page1741-1744
ST elevation MI
ST segment elevation type of acute myocardial infarction require at least 1 mm (01 mV) of ST segment elevation in the limb leads and at least 2 mm elevation in the precordial leads
The clinician must therefore be well versed in recognizing the so-called ECG mimics of acute myocardial infarction which include
These elevations must be present in anatomically contiguous leads (I aVL V5 V6 correspond to the lateral wall V1-V2 correspond to the septal wall V3-V4 correspond to the anterior wall II III aVF correspond to the inferior wall)
left ventricular hypertrophy
left bundle branch block
hyperkalemia
early repolarization
ventricular aneurysm
12-lead electrocardiogram showing ST-segment elevation (orange) in I aVL and V1-V5 with reciprocal changes (blue) in the inferior leads indicative of an anterior wall myocardial infarction
An acute STEMI involving the inferior and right ventricular wall Reciprocal changes are seen in the anterior leads
PATHOLOGIC OF Q-WAVEPathologic Q waves
Any Q-wave in leads V2ndashV3 ge 002 s or QS complex in leads V2 and V3
Q-wave ge 003 s and gt 01 mV deep or QS complex in leads I II aVL aVF or V4ndashV6 in
any two leads of a contiguous lead grouping (I aVLV6 V4ndashV6 II III and aVF)
result of absence of electrical activity
previous myocardial infarction
The evolution of an infarct on the ECG ST elevation Q wave formation T wave inversion
normalisation with a persistent Q wave
PATHOMECANISM CHEST PAINhttpemedicinemedscapecomarticle150215-overview2
ProfDrPeter Kabo Bagaimana Menggunakan Obat-obat kardiovasculer secara Rasional
AtherosclerosisProduce endothelial derived constricting
factor (EDCF)
Increase tonus artery
coronary
Ischemic myocard
Aerobic glycolysis turn
to anerobic glycolysis
Production of adenosin
Diffuse to extracellular
space
Stimulate A1 receptor in cardiac
afferent nerve ending
Bind with somatic cervico
thoracalis nerve at
ascending pathway in
medulla spinalis
Chest pain
SMOKING KILLS
These effects could potentially trigger
symptoms of ischemia in such smokers
One might also expect that the hemodynamic effects of nicotine would contribute to endothelial damage and accelerate the progression of atherosclerosis
Lipolyis - increased levels of circulating free fatty acids
and glycerol in the blood and the resulting increase in fat
metabolism drives a demand for more oxygen leading to
increased coronary blood flow and myocardial oxygen
uptake
addition to its cardiovascular effects such as elevated heart
rate blood pressure and cardiac output
nicotine has metabolic effects in particular increased lipolysis
Nicotine is a sympathomimetic chemical that promotes the release of catecholamines and other
neurotransmitters
SIGNS AND SYMPTOMS
bullChest pain (pressuretightnessheaviness and might radiate to neck arm)
bullIngestion heartburnbullNausea VomitingbullSweatingbullWeaknessbullDizziness
httpwwwcardiosmartorgManageConditionDefaultaspxid=904 httpwwwncbinlmnihgovpmcarticlesPMC2233977
ADDITIONAL EXAMINATION1 Physical examination
Gen appearance Distress Levine signbullHeart rate pulse respirrate variablebullBlood pressure variablebullLow-grade feverbullExamination of jugular venous pulsationsbullPulmonary CracklesbullS4 gallop due to reduced LV compliancebullS3 gallop if LV dysfunction presentbullMurmurs Pericardial friction rubs
2 ECG
The key to rapid diagnosis and risk stratification for the patient with chest painbullTo be obtained within 10 minutes of arrival to Emergency DepartmentbullFor STEMI 1048774ST-segment elevation gt1mm in 2+ contiguous leads OR new left bundle branch block (LBBB)bullLocation of InfarctLeadsInferior MI II III aVFAnterior MI V2-V4Lateral MI I aVL V5-V6
3 Lab studies
Cardiac Biomarkers CK CK-MB cTnbullSerum ChemistriesbullRenal FunctionbullCoagulation StudiesbullComplete Blood Count
TREATMENTAspirin
bullRapidly blocks formation of thromboxaneA2 in platelets by cyclooxygenase inhibitionbull162-325mg chewed (promotes buccalabsorption)bullISIS-2ndash23 reduction in mortality largely additive to the reduction in mortality from streptokinaseOther Adjuvant TherapiesAnalgesicsbullNitratesbullBeta-blockersbullAce InhibitorsbullOxygenbullHeparinbullIV Glycoprotein IIbIIIaInhibitorsbullClopidogrelbullStatins
Thrombolytic TherapybullCommon AgentsbullTNK-tPA30-50mg IV bolusbullReteplase10U x 2 (each over 2 minutes) IVbullAlteplaseup to 100mg in 90mins (based on weight)
bullContraindicationsndashAbsolute Prior intracranial hemorrhage known cerebral vascular lesion malignant intracranial neoplasm ischemic stroke within 3 months suspected aortic dissection active bleeding recent closed head injury or facial trauma within 3monthsndashRelative History of chronic severe HTN severeuncontrolled HTN at presentation (gt180110) history of ischemic stroke gt3 months traumaticprolonged CPR recent internal bleeding (2-4 weeks) pregnancy active peptic ulcer current anticoagulation
Primary PCI
bullPCI = Percutaneous Coronary Intervention
bullPTCA = Percutaneous Transluminal Coronary Angioplasty
bullPOBA = Plain Old Balloon Angioplasty
PROGNOSIS
bullDischarge usually 5 days after admissionbullSmoking CessationbullShort and Long-term survival depend upon resting LV function residual ischemic myocardium and susceptibility to ventricular arrhythmias
THE END
- CHEST PAIN SCENARIO 3 GROUP 10
- SCENARIO
- KEYWORD
- QUESTION
- DIFFERENTIAL DIAGNOSIS
- INTRODUCTION
- BASIC SCIENCE
- EKG
- Normal heart
- Myocardial Infarction Two to three days after an MI the myocyt
- Slide 11
- PATHOPHYSIOLOGY OF ST-ELEVATION MYOCARDIAL INFARCTION (STEMI)
- myocardial infarction
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- HYPOTENSION May trigger a dramatic sympathetic nervous system
- Slide 19
- Slide 21
- Left Ventricular Function Systolic Function
- Ventricular Remodeling
- references
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- PATHOLOGIC OF Q-WAVE
- PATHOMECANISM CHEST PAIN
- Slide 31
- SMOKING kills
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- ThE eND
-

QUESTIONbull 1) Why the patient suffered a crushing pain that spread to
the armbull 2) Why occasional extrasystole occur (pathomechanism)bull 3) What is the relationship between smoking and occasional
extrasystolebull 4) Indication for large Q wave and ST elevation What are
the relationship of these findings with chest pain bull 5) Indication for increasing cardiac enzymesbull 6) What are the relationship between myocardial infarction
with the symptoms (why he is having weak pulse)
DIFFERENTIAL DIAGNOSISSIGN AND SYMPTOM
STEMI CAD
Crushing pain at chest spreading to arm yes yes
Occasional extrasystol yes no
Large Q wave and ST elevasi yes no
Hypotension yes yes
Provisional diagnosis MI due to coroner arteri trombosis
yes yes
Enzim CKCKMB LDH increase yes no
httpwwwemedicinehealthcomcogestive_heart_failure
INTRODUCTIONbull STEMI ST segment elevation myocardial infarctionldquo is a type of
heart attack This is determined by an ECG test
bull Myocardial infarctions (heart attacks) occur when a coronay artery suddenly becomes at least partially blocked by a blood clot causing at least some of the heart muscle being supplied by that artery to become infarcted (that is to die) Heart attacks are divided into two types according to their severity
bull A STEMI is the more severe type
httpheartdiseaseaboutcom STEMI - ST Segment Elevation Myocardial Infarction By Richard N Fogoros MD
BASIC SCIENCE
EKG
Normal heart
Myocardial InfarctionTwo to three days after an MI the myocytes show that they are irreversibly damaged Theyve lost their nuclei PMNs
(polymorphonuclear leukocytes) are the first inflammatory cells on the scene They will begin to clear away the necrotic tissue Later the macrophages will finish the job These dying myocytes will eventually be replaced with scar tissue
httpwwwkumceduinstructionmedicineanatomyhistowebpathpath01htm
httpwwwgooglecomimgreshl=enampgl=idampbiw=1366ampbih=624amptbm=ischamptbnid=KajG2QEK1-M4mMampimgrefurl=httpwwwmedicinenetcomheart_attack_pathology_photo_essaypage3htmampdocid=CZHmHLYLNv9ueMampimgurl=httpimagesmedicinenetcomimagesillustrationsmyocardial_infarction_1jpgampw=400amph=308ampei=8_KDUK3PH8nlrAeTzYHwBwampzoom=1ampiact=hcampvpx=398ampvpy=128ampdur=3820amphovh=197amphovw=256amptx=206ampty=150ampsig=116867615274730240580amppage=2amptbnh=151amptbnw=196ampstart=21ampndsp=27ampved=1t429r23s20i206
PATHOPHYSIOLOGY OF
ST-ELEVATION MYOCARDIAL
INFARCTION (STEMI)
myocardial infarction
A myocardial infarction is defined as
Elevated blood levels of cardiac enzymes
(CKMB or Troponin T)
One of the following criteria are met
The patient has typical
complaints
The ECG shows ST elevation or
depression
pathological Q waves develop
on the ECG
bull PATHOPHYSIOLOGY MIA prolonged imbalance between myocardial oxygen supply and demand leads to the death of myocardial tissue Coronary
atherosclerosis is an essential part of the process in most patients
Ischemic heart disease seems to progress through stages of fatty-streak deposition in coronary arteries to development of
fibro-fatty plaque which then increases in size until it causes luminal obstruction
leading to exertional angina
any stages in this process the atherosclerotic lesion may erode
ulcerate fissure or rupture thereby exposing subendothelial
vessel wall substances to the circulating blood
Procoagulant factors (such as tissue factor) reside within the plaque itself
and in the absence of counterbalancing antithrombotic factor (eg heparin tissue-factor-
inhibitor) and fibrinolytic activities (tissues plasminogen activator [t-PA]
and single-chain urokinase-type plasminogen activator) within the endothelial cells of the coronary
artery can cause thrombosis Recent work suggests that inflammation may play a pivotal role in
the genesis of plaque rupture Total thrombotic occlusion occurs most commonly in proximal coronary
arteries its presence has been documented during the first 4 hours
after infarction in more than 85 of the patients with ST segment elevation
(Crawford MH (2009))
This potent procoagulant stimulus results in thrombus development in
this region In general acute MI occurs when this thrombosis
propagates and occludes flow within the artery resulting in ischemia of
cardiomyocytes distal to the obstruction
The ECG leads in which pathologic Q waves appear reflect the anatomical site of an infarction
TABLE 1 Localization of Myocardial Infarction Anatomical Site Leads with Abnormal ECG
Complexes Coronary Artery Most Often
Responsible Inferior IIIIIaVF RCA
Anteroseptal V1-V2 LAD Anteroapical V3-V4 LAD(distal) Anterolateral V5-V6 I aVL CFX
Posterior V1-V2 (tall R wave not Q wave) RCA
The electrocardiographic differences between these types of MI are summarized as follow
Type of Infarction Pathologic Q waves Acute ST segment Deviation
Q-wave MI Yes ST elevation Non-Q-wave MI No ST depression (and or T
wave inversion)
Angina pectoris- Neck- Shoulder- Arms
ischemic myocardial cells release mediator such as adenosine and
lactate from into local nerve endings
discomfort often refer to other region of the C7 through
dermatome
provocative substances continue to accumulate and active afferent
nerve for longer period
ischemic in acute MI persist and proceed to necrosis
HYPOTENSION
May trigger a dramatic sympathetic nervous system response
Systemic sign of subsequent catecholamine release include diaphoresis (sweating) tachycardia and cool
and clammy skin
cause of vasoconstriction
Systolic Dysfunction
Decrease lungs compliance and stimulates juxtacappilary
receptors
Left ventricle contractility can be
reduced
J receptors effects a reflex that results in rapid shallow
breathing and evokes the subjective feeling of dyspnea
Increase in LV pressure compounded by the ischemia
induced stiffness of the chamber (diastolic dysfunction) is conveyed to the left atrium and pulmonary
veins
Decreasing the stroke volume and causing the diastolic
volume and pressure within the LV to rise
Ischemia affects large amount of myocardium
SERUM MARKER OF INFARCTION
Detection of cardiac-specific troponins and creatine kinase MB isoenzyme
Intracellular macromolecules leak into the cardiac interstitium and ultimately into the bloodstream
Necrosis of myocardial tissue Cause by disruption of the sarcolemma
MYOCARDIAL INFARTION
TYPICAL SYMPTOM- Crushing chest pain
more severe and wider than usual angina
SERUM BIOMARKSCreatine kinaseTroponin
ECG initial finding- St elevation- Q Wave
STEMI
Left Ventricular Function Systolic Function
Upon interruption of antegrade flow in an epicardial coronary artery the zone of myocardium supplied by that vessel immediately loses its ability to shorten and perform contractile work Four abnormal contraction patterns develop in sequence (1) dyssynchrony that is dissociation in the time course of contraction of adjacent segments(2) hypokinesis reduction in the extent of shortening (3) akinesis cessation of shortening and (4) dyskinesis paradoxical expansion and systolic bulging
Hyperkinesis of the remaining normal myocardium initially accompanies dysfunction of the infarcting segment The early hyperkinesis of the noninfarcted zones likely results from acute compensations including increased activity of the sympathetic nervous system and the Frank-Starling mechanism A portion of this compensatory hyperkinesis is ineffective work because contraction of the noninfarcted segments of myocardium hellip
Ventricular Remodelingbull As a consequence of STEMI the changes in left ventricular size shape and
thickness involving both the infarcted and the noninfarcted segments of the ventricle described earlier occur and are collectively referred to as ventricular remodeling which can in turn influence ventricular function and prognosis
bull A combination of changes in left ventricular dilation and hypertrophy of residual noninfarcted myocardium causes remodeling
bull After the size of infarction the two most important factors driving the process of left ventricular dilation are ventricular loading conditions and infarct artery patency
bull Elevated ventricular pressure contributes to increased wall stress and the risk of infarct expansion and a patent infarct artery accelerates myocardial scar formation and increases tissue turgor in the infarct zone reducing the risk of infarct expansion and ventricular dilation
Antman EM Morrow DA McCabe CH et al Enoxaparin versus unfractionated heparin with fibrinolysis for ST-elevation myocardial infarction N Engl J Med 2006 3541477
referencesSLIDE 2 Alpert JS Thygesen K Antman E and Bassand JP Myocardial infarction redefined--a consensus document of The Joint European Society of CardiologyAmerican College of Cardiology Committee for the redefinition of myocardial infarction J Am Coll Cardiol 2000 Sep 36(3) 959-69 pmid10987628bull Book of Pathophysiology of Heart Disease fourth edition editor Leonard SLilly page 179-
184bull ILMU PENYAKIT DALAM Jilid II Edisi V Editor Aru WSudoyo Bambang Setiyohadi
Idrus Alwi page1741-1744
ST elevation MI
ST segment elevation type of acute myocardial infarction require at least 1 mm (01 mV) of ST segment elevation in the limb leads and at least 2 mm elevation in the precordial leads
The clinician must therefore be well versed in recognizing the so-called ECG mimics of acute myocardial infarction which include
These elevations must be present in anatomically contiguous leads (I aVL V5 V6 correspond to the lateral wall V1-V2 correspond to the septal wall V3-V4 correspond to the anterior wall II III aVF correspond to the inferior wall)
left ventricular hypertrophy
left bundle branch block
hyperkalemia
early repolarization
ventricular aneurysm
12-lead electrocardiogram showing ST-segment elevation (orange) in I aVL and V1-V5 with reciprocal changes (blue) in the inferior leads indicative of an anterior wall myocardial infarction
An acute STEMI involving the inferior and right ventricular wall Reciprocal changes are seen in the anterior leads
PATHOLOGIC OF Q-WAVEPathologic Q waves
Any Q-wave in leads V2ndashV3 ge 002 s or QS complex in leads V2 and V3
Q-wave ge 003 s and gt 01 mV deep or QS complex in leads I II aVL aVF or V4ndashV6 in
any two leads of a contiguous lead grouping (I aVLV6 V4ndashV6 II III and aVF)
result of absence of electrical activity
previous myocardial infarction
The evolution of an infarct on the ECG ST elevation Q wave formation T wave inversion
normalisation with a persistent Q wave
PATHOMECANISM CHEST PAINhttpemedicinemedscapecomarticle150215-overview2
ProfDrPeter Kabo Bagaimana Menggunakan Obat-obat kardiovasculer secara Rasional
AtherosclerosisProduce endothelial derived constricting
factor (EDCF)
Increase tonus artery
coronary
Ischemic myocard
Aerobic glycolysis turn
to anerobic glycolysis
Production of adenosin
Diffuse to extracellular
space
Stimulate A1 receptor in cardiac
afferent nerve ending
Bind with somatic cervico
thoracalis nerve at
ascending pathway in
medulla spinalis
Chest pain
SMOKING KILLS
These effects could potentially trigger
symptoms of ischemia in such smokers
One might also expect that the hemodynamic effects of nicotine would contribute to endothelial damage and accelerate the progression of atherosclerosis
Lipolyis - increased levels of circulating free fatty acids
and glycerol in the blood and the resulting increase in fat
metabolism drives a demand for more oxygen leading to
increased coronary blood flow and myocardial oxygen
uptake
addition to its cardiovascular effects such as elevated heart
rate blood pressure and cardiac output
nicotine has metabolic effects in particular increased lipolysis
Nicotine is a sympathomimetic chemical that promotes the release of catecholamines and other
neurotransmitters
SIGNS AND SYMPTOMS
bullChest pain (pressuretightnessheaviness and might radiate to neck arm)
bullIngestion heartburnbullNausea VomitingbullSweatingbullWeaknessbullDizziness
httpwwwcardiosmartorgManageConditionDefaultaspxid=904 httpwwwncbinlmnihgovpmcarticlesPMC2233977
ADDITIONAL EXAMINATION1 Physical examination
Gen appearance Distress Levine signbullHeart rate pulse respirrate variablebullBlood pressure variablebullLow-grade feverbullExamination of jugular venous pulsationsbullPulmonary CracklesbullS4 gallop due to reduced LV compliancebullS3 gallop if LV dysfunction presentbullMurmurs Pericardial friction rubs
2 ECG
The key to rapid diagnosis and risk stratification for the patient with chest painbullTo be obtained within 10 minutes of arrival to Emergency DepartmentbullFor STEMI 1048774ST-segment elevation gt1mm in 2+ contiguous leads OR new left bundle branch block (LBBB)bullLocation of InfarctLeadsInferior MI II III aVFAnterior MI V2-V4Lateral MI I aVL V5-V6
3 Lab studies
Cardiac Biomarkers CK CK-MB cTnbullSerum ChemistriesbullRenal FunctionbullCoagulation StudiesbullComplete Blood Count
TREATMENTAspirin
bullRapidly blocks formation of thromboxaneA2 in platelets by cyclooxygenase inhibitionbull162-325mg chewed (promotes buccalabsorption)bullISIS-2ndash23 reduction in mortality largely additive to the reduction in mortality from streptokinaseOther Adjuvant TherapiesAnalgesicsbullNitratesbullBeta-blockersbullAce InhibitorsbullOxygenbullHeparinbullIV Glycoprotein IIbIIIaInhibitorsbullClopidogrelbullStatins
Thrombolytic TherapybullCommon AgentsbullTNK-tPA30-50mg IV bolusbullReteplase10U x 2 (each over 2 minutes) IVbullAlteplaseup to 100mg in 90mins (based on weight)
bullContraindicationsndashAbsolute Prior intracranial hemorrhage known cerebral vascular lesion malignant intracranial neoplasm ischemic stroke within 3 months suspected aortic dissection active bleeding recent closed head injury or facial trauma within 3monthsndashRelative History of chronic severe HTN severeuncontrolled HTN at presentation (gt180110) history of ischemic stroke gt3 months traumaticprolonged CPR recent internal bleeding (2-4 weeks) pregnancy active peptic ulcer current anticoagulation
Primary PCI
bullPCI = Percutaneous Coronary Intervention
bullPTCA = Percutaneous Transluminal Coronary Angioplasty
bullPOBA = Plain Old Balloon Angioplasty
PROGNOSIS
bullDischarge usually 5 days after admissionbullSmoking CessationbullShort and Long-term survival depend upon resting LV function residual ischemic myocardium and susceptibility to ventricular arrhythmias
THE END
- CHEST PAIN SCENARIO 3 GROUP 10
- SCENARIO
- KEYWORD
- QUESTION
- DIFFERENTIAL DIAGNOSIS
- INTRODUCTION
- BASIC SCIENCE
- EKG
- Normal heart
- Myocardial Infarction Two to three days after an MI the myocyt
- Slide 11
- PATHOPHYSIOLOGY OF ST-ELEVATION MYOCARDIAL INFARCTION (STEMI)
- myocardial infarction
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- HYPOTENSION May trigger a dramatic sympathetic nervous system
- Slide 19
- Slide 21
- Left Ventricular Function Systolic Function
- Ventricular Remodeling
- references
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- PATHOLOGIC OF Q-WAVE
- PATHOMECANISM CHEST PAIN
- Slide 31
- SMOKING kills
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- ThE eND
-

DIFFERENTIAL DIAGNOSISSIGN AND SYMPTOM
STEMI CAD
Crushing pain at chest spreading to arm yes yes
Occasional extrasystol yes no
Large Q wave and ST elevasi yes no
Hypotension yes yes
Provisional diagnosis MI due to coroner arteri trombosis
yes yes
Enzim CKCKMB LDH increase yes no
httpwwwemedicinehealthcomcogestive_heart_failure
INTRODUCTIONbull STEMI ST segment elevation myocardial infarctionldquo is a type of
heart attack This is determined by an ECG test
bull Myocardial infarctions (heart attacks) occur when a coronay artery suddenly becomes at least partially blocked by a blood clot causing at least some of the heart muscle being supplied by that artery to become infarcted (that is to die) Heart attacks are divided into two types according to their severity
bull A STEMI is the more severe type
httpheartdiseaseaboutcom STEMI - ST Segment Elevation Myocardial Infarction By Richard N Fogoros MD
BASIC SCIENCE
EKG
Normal heart
Myocardial InfarctionTwo to three days after an MI the myocytes show that they are irreversibly damaged Theyve lost their nuclei PMNs
(polymorphonuclear leukocytes) are the first inflammatory cells on the scene They will begin to clear away the necrotic tissue Later the macrophages will finish the job These dying myocytes will eventually be replaced with scar tissue
httpwwwkumceduinstructionmedicineanatomyhistowebpathpath01htm
httpwwwgooglecomimgreshl=enampgl=idampbiw=1366ampbih=624amptbm=ischamptbnid=KajG2QEK1-M4mMampimgrefurl=httpwwwmedicinenetcomheart_attack_pathology_photo_essaypage3htmampdocid=CZHmHLYLNv9ueMampimgurl=httpimagesmedicinenetcomimagesillustrationsmyocardial_infarction_1jpgampw=400amph=308ampei=8_KDUK3PH8nlrAeTzYHwBwampzoom=1ampiact=hcampvpx=398ampvpy=128ampdur=3820amphovh=197amphovw=256amptx=206ampty=150ampsig=116867615274730240580amppage=2amptbnh=151amptbnw=196ampstart=21ampndsp=27ampved=1t429r23s20i206
PATHOPHYSIOLOGY OF
ST-ELEVATION MYOCARDIAL
INFARCTION (STEMI)
myocardial infarction
A myocardial infarction is defined as
Elevated blood levels of cardiac enzymes
(CKMB or Troponin T)
One of the following criteria are met
The patient has typical
complaints
The ECG shows ST elevation or
depression
pathological Q waves develop
on the ECG
bull PATHOPHYSIOLOGY MIA prolonged imbalance between myocardial oxygen supply and demand leads to the death of myocardial tissue Coronary
atherosclerosis is an essential part of the process in most patients
Ischemic heart disease seems to progress through stages of fatty-streak deposition in coronary arteries to development of
fibro-fatty plaque which then increases in size until it causes luminal obstruction
leading to exertional angina
any stages in this process the atherosclerotic lesion may erode
ulcerate fissure or rupture thereby exposing subendothelial
vessel wall substances to the circulating blood
Procoagulant factors (such as tissue factor) reside within the plaque itself
and in the absence of counterbalancing antithrombotic factor (eg heparin tissue-factor-
inhibitor) and fibrinolytic activities (tissues plasminogen activator [t-PA]
and single-chain urokinase-type plasminogen activator) within the endothelial cells of the coronary
artery can cause thrombosis Recent work suggests that inflammation may play a pivotal role in
the genesis of plaque rupture Total thrombotic occlusion occurs most commonly in proximal coronary
arteries its presence has been documented during the first 4 hours
after infarction in more than 85 of the patients with ST segment elevation
(Crawford MH (2009))
This potent procoagulant stimulus results in thrombus development in
this region In general acute MI occurs when this thrombosis
propagates and occludes flow within the artery resulting in ischemia of
cardiomyocytes distal to the obstruction
The ECG leads in which pathologic Q waves appear reflect the anatomical site of an infarction
TABLE 1 Localization of Myocardial Infarction Anatomical Site Leads with Abnormal ECG
Complexes Coronary Artery Most Often
Responsible Inferior IIIIIaVF RCA
Anteroseptal V1-V2 LAD Anteroapical V3-V4 LAD(distal) Anterolateral V5-V6 I aVL CFX
Posterior V1-V2 (tall R wave not Q wave) RCA
The electrocardiographic differences between these types of MI are summarized as follow
Type of Infarction Pathologic Q waves Acute ST segment Deviation
Q-wave MI Yes ST elevation Non-Q-wave MI No ST depression (and or T
wave inversion)
Angina pectoris- Neck- Shoulder- Arms
ischemic myocardial cells release mediator such as adenosine and
lactate from into local nerve endings
discomfort often refer to other region of the C7 through
dermatome
provocative substances continue to accumulate and active afferent
nerve for longer period
ischemic in acute MI persist and proceed to necrosis
HYPOTENSION
May trigger a dramatic sympathetic nervous system response
Systemic sign of subsequent catecholamine release include diaphoresis (sweating) tachycardia and cool
and clammy skin
cause of vasoconstriction
Systolic Dysfunction
Decrease lungs compliance and stimulates juxtacappilary
receptors
Left ventricle contractility can be
reduced
J receptors effects a reflex that results in rapid shallow
breathing and evokes the subjective feeling of dyspnea
Increase in LV pressure compounded by the ischemia
induced stiffness of the chamber (diastolic dysfunction) is conveyed to the left atrium and pulmonary
veins
Decreasing the stroke volume and causing the diastolic
volume and pressure within the LV to rise
Ischemia affects large amount of myocardium
SERUM MARKER OF INFARCTION
Detection of cardiac-specific troponins and creatine kinase MB isoenzyme
Intracellular macromolecules leak into the cardiac interstitium and ultimately into the bloodstream
Necrosis of myocardial tissue Cause by disruption of the sarcolemma
MYOCARDIAL INFARTION
TYPICAL SYMPTOM- Crushing chest pain
more severe and wider than usual angina
SERUM BIOMARKSCreatine kinaseTroponin
ECG initial finding- St elevation- Q Wave
STEMI
Left Ventricular Function Systolic Function
Upon interruption of antegrade flow in an epicardial coronary artery the zone of myocardium supplied by that vessel immediately loses its ability to shorten and perform contractile work Four abnormal contraction patterns develop in sequence (1) dyssynchrony that is dissociation in the time course of contraction of adjacent segments(2) hypokinesis reduction in the extent of shortening (3) akinesis cessation of shortening and (4) dyskinesis paradoxical expansion and systolic bulging
Hyperkinesis of the remaining normal myocardium initially accompanies dysfunction of the infarcting segment The early hyperkinesis of the noninfarcted zones likely results from acute compensations including increased activity of the sympathetic nervous system and the Frank-Starling mechanism A portion of this compensatory hyperkinesis is ineffective work because contraction of the noninfarcted segments of myocardium hellip
Ventricular Remodelingbull As a consequence of STEMI the changes in left ventricular size shape and
thickness involving both the infarcted and the noninfarcted segments of the ventricle described earlier occur and are collectively referred to as ventricular remodeling which can in turn influence ventricular function and prognosis
bull A combination of changes in left ventricular dilation and hypertrophy of residual noninfarcted myocardium causes remodeling
bull After the size of infarction the two most important factors driving the process of left ventricular dilation are ventricular loading conditions and infarct artery patency
bull Elevated ventricular pressure contributes to increased wall stress and the risk of infarct expansion and a patent infarct artery accelerates myocardial scar formation and increases tissue turgor in the infarct zone reducing the risk of infarct expansion and ventricular dilation
Antman EM Morrow DA McCabe CH et al Enoxaparin versus unfractionated heparin with fibrinolysis for ST-elevation myocardial infarction N Engl J Med 2006 3541477
referencesSLIDE 2 Alpert JS Thygesen K Antman E and Bassand JP Myocardial infarction redefined--a consensus document of The Joint European Society of CardiologyAmerican College of Cardiology Committee for the redefinition of myocardial infarction J Am Coll Cardiol 2000 Sep 36(3) 959-69 pmid10987628bull Book of Pathophysiology of Heart Disease fourth edition editor Leonard SLilly page 179-
184bull ILMU PENYAKIT DALAM Jilid II Edisi V Editor Aru WSudoyo Bambang Setiyohadi
Idrus Alwi page1741-1744
ST elevation MI
ST segment elevation type of acute myocardial infarction require at least 1 mm (01 mV) of ST segment elevation in the limb leads and at least 2 mm elevation in the precordial leads
The clinician must therefore be well versed in recognizing the so-called ECG mimics of acute myocardial infarction which include
These elevations must be present in anatomically contiguous leads (I aVL V5 V6 correspond to the lateral wall V1-V2 correspond to the septal wall V3-V4 correspond to the anterior wall II III aVF correspond to the inferior wall)
left ventricular hypertrophy
left bundle branch block
hyperkalemia
early repolarization
ventricular aneurysm
12-lead electrocardiogram showing ST-segment elevation (orange) in I aVL and V1-V5 with reciprocal changes (blue) in the inferior leads indicative of an anterior wall myocardial infarction
An acute STEMI involving the inferior and right ventricular wall Reciprocal changes are seen in the anterior leads
PATHOLOGIC OF Q-WAVEPathologic Q waves
Any Q-wave in leads V2ndashV3 ge 002 s or QS complex in leads V2 and V3
Q-wave ge 003 s and gt 01 mV deep or QS complex in leads I II aVL aVF or V4ndashV6 in
any two leads of a contiguous lead grouping (I aVLV6 V4ndashV6 II III and aVF)
result of absence of electrical activity
previous myocardial infarction
The evolution of an infarct on the ECG ST elevation Q wave formation T wave inversion
normalisation with a persistent Q wave
PATHOMECANISM CHEST PAINhttpemedicinemedscapecomarticle150215-overview2
ProfDrPeter Kabo Bagaimana Menggunakan Obat-obat kardiovasculer secara Rasional
AtherosclerosisProduce endothelial derived constricting
factor (EDCF)
Increase tonus artery
coronary
Ischemic myocard
Aerobic glycolysis turn
to anerobic glycolysis
Production of adenosin
Diffuse to extracellular
space
Stimulate A1 receptor in cardiac
afferent nerve ending
Bind with somatic cervico
thoracalis nerve at
ascending pathway in
medulla spinalis
Chest pain
SMOKING KILLS
These effects could potentially trigger
symptoms of ischemia in such smokers
One might also expect that the hemodynamic effects of nicotine would contribute to endothelial damage and accelerate the progression of atherosclerosis
Lipolyis - increased levels of circulating free fatty acids
and glycerol in the blood and the resulting increase in fat
metabolism drives a demand for more oxygen leading to
increased coronary blood flow and myocardial oxygen
uptake
addition to its cardiovascular effects such as elevated heart
rate blood pressure and cardiac output
nicotine has metabolic effects in particular increased lipolysis
Nicotine is a sympathomimetic chemical that promotes the release of catecholamines and other
neurotransmitters
SIGNS AND SYMPTOMS
bullChest pain (pressuretightnessheaviness and might radiate to neck arm)
bullIngestion heartburnbullNausea VomitingbullSweatingbullWeaknessbullDizziness
httpwwwcardiosmartorgManageConditionDefaultaspxid=904 httpwwwncbinlmnihgovpmcarticlesPMC2233977
ADDITIONAL EXAMINATION1 Physical examination
Gen appearance Distress Levine signbullHeart rate pulse respirrate variablebullBlood pressure variablebullLow-grade feverbullExamination of jugular venous pulsationsbullPulmonary CracklesbullS4 gallop due to reduced LV compliancebullS3 gallop if LV dysfunction presentbullMurmurs Pericardial friction rubs
2 ECG
The key to rapid diagnosis and risk stratification for the patient with chest painbullTo be obtained within 10 minutes of arrival to Emergency DepartmentbullFor STEMI 1048774ST-segment elevation gt1mm in 2+ contiguous leads OR new left bundle branch block (LBBB)bullLocation of InfarctLeadsInferior MI II III aVFAnterior MI V2-V4Lateral MI I aVL V5-V6
3 Lab studies
Cardiac Biomarkers CK CK-MB cTnbullSerum ChemistriesbullRenal FunctionbullCoagulation StudiesbullComplete Blood Count
TREATMENTAspirin
bullRapidly blocks formation of thromboxaneA2 in platelets by cyclooxygenase inhibitionbull162-325mg chewed (promotes buccalabsorption)bullISIS-2ndash23 reduction in mortality largely additive to the reduction in mortality from streptokinaseOther Adjuvant TherapiesAnalgesicsbullNitratesbullBeta-blockersbullAce InhibitorsbullOxygenbullHeparinbullIV Glycoprotein IIbIIIaInhibitorsbullClopidogrelbullStatins
Thrombolytic TherapybullCommon AgentsbullTNK-tPA30-50mg IV bolusbullReteplase10U x 2 (each over 2 minutes) IVbullAlteplaseup to 100mg in 90mins (based on weight)
bullContraindicationsndashAbsolute Prior intracranial hemorrhage known cerebral vascular lesion malignant intracranial neoplasm ischemic stroke within 3 months suspected aortic dissection active bleeding recent closed head injury or facial trauma within 3monthsndashRelative History of chronic severe HTN severeuncontrolled HTN at presentation (gt180110) history of ischemic stroke gt3 months traumaticprolonged CPR recent internal bleeding (2-4 weeks) pregnancy active peptic ulcer current anticoagulation
Primary PCI
bullPCI = Percutaneous Coronary Intervention
bullPTCA = Percutaneous Transluminal Coronary Angioplasty
bullPOBA = Plain Old Balloon Angioplasty
PROGNOSIS
bullDischarge usually 5 days after admissionbullSmoking CessationbullShort and Long-term survival depend upon resting LV function residual ischemic myocardium and susceptibility to ventricular arrhythmias
THE END
- CHEST PAIN SCENARIO 3 GROUP 10
- SCENARIO
- KEYWORD
- QUESTION
- DIFFERENTIAL DIAGNOSIS
- INTRODUCTION
- BASIC SCIENCE
- EKG
- Normal heart
- Myocardial Infarction Two to three days after an MI the myocyt
- Slide 11
- PATHOPHYSIOLOGY OF ST-ELEVATION MYOCARDIAL INFARCTION (STEMI)
- myocardial infarction
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- HYPOTENSION May trigger a dramatic sympathetic nervous system
- Slide 19
- Slide 21
- Left Ventricular Function Systolic Function
- Ventricular Remodeling
- references
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- PATHOLOGIC OF Q-WAVE
- PATHOMECANISM CHEST PAIN
- Slide 31
- SMOKING kills
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- ThE eND
-

INTRODUCTIONbull STEMI ST segment elevation myocardial infarctionldquo is a type of
heart attack This is determined by an ECG test
bull Myocardial infarctions (heart attacks) occur when a coronay artery suddenly becomes at least partially blocked by a blood clot causing at least some of the heart muscle being supplied by that artery to become infarcted (that is to die) Heart attacks are divided into two types according to their severity
bull A STEMI is the more severe type
httpheartdiseaseaboutcom STEMI - ST Segment Elevation Myocardial Infarction By Richard N Fogoros MD
BASIC SCIENCE
EKG
Normal heart
Myocardial InfarctionTwo to three days after an MI the myocytes show that they are irreversibly damaged Theyve lost their nuclei PMNs
(polymorphonuclear leukocytes) are the first inflammatory cells on the scene They will begin to clear away the necrotic tissue Later the macrophages will finish the job These dying myocytes will eventually be replaced with scar tissue
httpwwwkumceduinstructionmedicineanatomyhistowebpathpath01htm
httpwwwgooglecomimgreshl=enampgl=idampbiw=1366ampbih=624amptbm=ischamptbnid=KajG2QEK1-M4mMampimgrefurl=httpwwwmedicinenetcomheart_attack_pathology_photo_essaypage3htmampdocid=CZHmHLYLNv9ueMampimgurl=httpimagesmedicinenetcomimagesillustrationsmyocardial_infarction_1jpgampw=400amph=308ampei=8_KDUK3PH8nlrAeTzYHwBwampzoom=1ampiact=hcampvpx=398ampvpy=128ampdur=3820amphovh=197amphovw=256amptx=206ampty=150ampsig=116867615274730240580amppage=2amptbnh=151amptbnw=196ampstart=21ampndsp=27ampved=1t429r23s20i206
PATHOPHYSIOLOGY OF
ST-ELEVATION MYOCARDIAL
INFARCTION (STEMI)
myocardial infarction
A myocardial infarction is defined as
Elevated blood levels of cardiac enzymes
(CKMB or Troponin T)
One of the following criteria are met
The patient has typical
complaints
The ECG shows ST elevation or
depression
pathological Q waves develop
on the ECG
bull PATHOPHYSIOLOGY MIA prolonged imbalance between myocardial oxygen supply and demand leads to the death of myocardial tissue Coronary
atherosclerosis is an essential part of the process in most patients
Ischemic heart disease seems to progress through stages of fatty-streak deposition in coronary arteries to development of
fibro-fatty plaque which then increases in size until it causes luminal obstruction
leading to exertional angina
any stages in this process the atherosclerotic lesion may erode
ulcerate fissure or rupture thereby exposing subendothelial
vessel wall substances to the circulating blood
Procoagulant factors (such as tissue factor) reside within the plaque itself
and in the absence of counterbalancing antithrombotic factor (eg heparin tissue-factor-
inhibitor) and fibrinolytic activities (tissues plasminogen activator [t-PA]
and single-chain urokinase-type plasminogen activator) within the endothelial cells of the coronary
artery can cause thrombosis Recent work suggests that inflammation may play a pivotal role in
the genesis of plaque rupture Total thrombotic occlusion occurs most commonly in proximal coronary
arteries its presence has been documented during the first 4 hours
after infarction in more than 85 of the patients with ST segment elevation
(Crawford MH (2009))
This potent procoagulant stimulus results in thrombus development in
this region In general acute MI occurs when this thrombosis
propagates and occludes flow within the artery resulting in ischemia of
cardiomyocytes distal to the obstruction
The ECG leads in which pathologic Q waves appear reflect the anatomical site of an infarction
TABLE 1 Localization of Myocardial Infarction Anatomical Site Leads with Abnormal ECG
Complexes Coronary Artery Most Often
Responsible Inferior IIIIIaVF RCA
Anteroseptal V1-V2 LAD Anteroapical V3-V4 LAD(distal) Anterolateral V5-V6 I aVL CFX
Posterior V1-V2 (tall R wave not Q wave) RCA
The electrocardiographic differences between these types of MI are summarized as follow
Type of Infarction Pathologic Q waves Acute ST segment Deviation
Q-wave MI Yes ST elevation Non-Q-wave MI No ST depression (and or T
wave inversion)
Angina pectoris- Neck- Shoulder- Arms
ischemic myocardial cells release mediator such as adenosine and
lactate from into local nerve endings
discomfort often refer to other region of the C7 through
dermatome
provocative substances continue to accumulate and active afferent
nerve for longer period
ischemic in acute MI persist and proceed to necrosis
HYPOTENSION
May trigger a dramatic sympathetic nervous system response
Systemic sign of subsequent catecholamine release include diaphoresis (sweating) tachycardia and cool
and clammy skin
cause of vasoconstriction
Systolic Dysfunction
Decrease lungs compliance and stimulates juxtacappilary
receptors
Left ventricle contractility can be
reduced
J receptors effects a reflex that results in rapid shallow
breathing and evokes the subjective feeling of dyspnea
Increase in LV pressure compounded by the ischemia
induced stiffness of the chamber (diastolic dysfunction) is conveyed to the left atrium and pulmonary
veins
Decreasing the stroke volume and causing the diastolic
volume and pressure within the LV to rise
Ischemia affects large amount of myocardium
SERUM MARKER OF INFARCTION
Detection of cardiac-specific troponins and creatine kinase MB isoenzyme
Intracellular macromolecules leak into the cardiac interstitium and ultimately into the bloodstream
Necrosis of myocardial tissue Cause by disruption of the sarcolemma
MYOCARDIAL INFARTION
TYPICAL SYMPTOM- Crushing chest pain
more severe and wider than usual angina
SERUM BIOMARKSCreatine kinaseTroponin
ECG initial finding- St elevation- Q Wave
STEMI
Left Ventricular Function Systolic Function
Upon interruption of antegrade flow in an epicardial coronary artery the zone of myocardium supplied by that vessel immediately loses its ability to shorten and perform contractile work Four abnormal contraction patterns develop in sequence (1) dyssynchrony that is dissociation in the time course of contraction of adjacent segments(2) hypokinesis reduction in the extent of shortening (3) akinesis cessation of shortening and (4) dyskinesis paradoxical expansion and systolic bulging
Hyperkinesis of the remaining normal myocardium initially accompanies dysfunction of the infarcting segment The early hyperkinesis of the noninfarcted zones likely results from acute compensations including increased activity of the sympathetic nervous system and the Frank-Starling mechanism A portion of this compensatory hyperkinesis is ineffective work because contraction of the noninfarcted segments of myocardium hellip
Ventricular Remodelingbull As a consequence of STEMI the changes in left ventricular size shape and
thickness involving both the infarcted and the noninfarcted segments of the ventricle described earlier occur and are collectively referred to as ventricular remodeling which can in turn influence ventricular function and prognosis
bull A combination of changes in left ventricular dilation and hypertrophy of residual noninfarcted myocardium causes remodeling
bull After the size of infarction the two most important factors driving the process of left ventricular dilation are ventricular loading conditions and infarct artery patency
bull Elevated ventricular pressure contributes to increased wall stress and the risk of infarct expansion and a patent infarct artery accelerates myocardial scar formation and increases tissue turgor in the infarct zone reducing the risk of infarct expansion and ventricular dilation
Antman EM Morrow DA McCabe CH et al Enoxaparin versus unfractionated heparin with fibrinolysis for ST-elevation myocardial infarction N Engl J Med 2006 3541477
referencesSLIDE 2 Alpert JS Thygesen K Antman E and Bassand JP Myocardial infarction redefined--a consensus document of The Joint European Society of CardiologyAmerican College of Cardiology Committee for the redefinition of myocardial infarction J Am Coll Cardiol 2000 Sep 36(3) 959-69 pmid10987628bull Book of Pathophysiology of Heart Disease fourth edition editor Leonard SLilly page 179-
184bull ILMU PENYAKIT DALAM Jilid II Edisi V Editor Aru WSudoyo Bambang Setiyohadi
Idrus Alwi page1741-1744
ST elevation MI
ST segment elevation type of acute myocardial infarction require at least 1 mm (01 mV) of ST segment elevation in the limb leads and at least 2 mm elevation in the precordial leads
The clinician must therefore be well versed in recognizing the so-called ECG mimics of acute myocardial infarction which include
These elevations must be present in anatomically contiguous leads (I aVL V5 V6 correspond to the lateral wall V1-V2 correspond to the septal wall V3-V4 correspond to the anterior wall II III aVF correspond to the inferior wall)
left ventricular hypertrophy
left bundle branch block
hyperkalemia
early repolarization
ventricular aneurysm
12-lead electrocardiogram showing ST-segment elevation (orange) in I aVL and V1-V5 with reciprocal changes (blue) in the inferior leads indicative of an anterior wall myocardial infarction
An acute STEMI involving the inferior and right ventricular wall Reciprocal changes are seen in the anterior leads
PATHOLOGIC OF Q-WAVEPathologic Q waves
Any Q-wave in leads V2ndashV3 ge 002 s or QS complex in leads V2 and V3
Q-wave ge 003 s and gt 01 mV deep or QS complex in leads I II aVL aVF or V4ndashV6 in
any two leads of a contiguous lead grouping (I aVLV6 V4ndashV6 II III and aVF)
result of absence of electrical activity
previous myocardial infarction
The evolution of an infarct on the ECG ST elevation Q wave formation T wave inversion
normalisation with a persistent Q wave
PATHOMECANISM CHEST PAINhttpemedicinemedscapecomarticle150215-overview2
ProfDrPeter Kabo Bagaimana Menggunakan Obat-obat kardiovasculer secara Rasional
AtherosclerosisProduce endothelial derived constricting
factor (EDCF)
Increase tonus artery
coronary
Ischemic myocard
Aerobic glycolysis turn
to anerobic glycolysis
Production of adenosin
Diffuse to extracellular
space
Stimulate A1 receptor in cardiac
afferent nerve ending
Bind with somatic cervico
thoracalis nerve at
ascending pathway in
medulla spinalis
Chest pain
SMOKING KILLS
These effects could potentially trigger
symptoms of ischemia in such smokers
One might also expect that the hemodynamic effects of nicotine would contribute to endothelial damage and accelerate the progression of atherosclerosis
Lipolyis - increased levels of circulating free fatty acids
and glycerol in the blood and the resulting increase in fat
metabolism drives a demand for more oxygen leading to
increased coronary blood flow and myocardial oxygen
uptake
addition to its cardiovascular effects such as elevated heart
rate blood pressure and cardiac output
nicotine has metabolic effects in particular increased lipolysis
Nicotine is a sympathomimetic chemical that promotes the release of catecholamines and other
neurotransmitters
SIGNS AND SYMPTOMS
bullChest pain (pressuretightnessheaviness and might radiate to neck arm)
bullIngestion heartburnbullNausea VomitingbullSweatingbullWeaknessbullDizziness
httpwwwcardiosmartorgManageConditionDefaultaspxid=904 httpwwwncbinlmnihgovpmcarticlesPMC2233977
ADDITIONAL EXAMINATION1 Physical examination
Gen appearance Distress Levine signbullHeart rate pulse respirrate variablebullBlood pressure variablebullLow-grade feverbullExamination of jugular venous pulsationsbullPulmonary CracklesbullS4 gallop due to reduced LV compliancebullS3 gallop if LV dysfunction presentbullMurmurs Pericardial friction rubs
2 ECG
The key to rapid diagnosis and risk stratification for the patient with chest painbullTo be obtained within 10 minutes of arrival to Emergency DepartmentbullFor STEMI 1048774ST-segment elevation gt1mm in 2+ contiguous leads OR new left bundle branch block (LBBB)bullLocation of InfarctLeadsInferior MI II III aVFAnterior MI V2-V4Lateral MI I aVL V5-V6
3 Lab studies
Cardiac Biomarkers CK CK-MB cTnbullSerum ChemistriesbullRenal FunctionbullCoagulation StudiesbullComplete Blood Count
TREATMENTAspirin
bullRapidly blocks formation of thromboxaneA2 in platelets by cyclooxygenase inhibitionbull162-325mg chewed (promotes buccalabsorption)bullISIS-2ndash23 reduction in mortality largely additive to the reduction in mortality from streptokinaseOther Adjuvant TherapiesAnalgesicsbullNitratesbullBeta-blockersbullAce InhibitorsbullOxygenbullHeparinbullIV Glycoprotein IIbIIIaInhibitorsbullClopidogrelbullStatins
Thrombolytic TherapybullCommon AgentsbullTNK-tPA30-50mg IV bolusbullReteplase10U x 2 (each over 2 minutes) IVbullAlteplaseup to 100mg in 90mins (based on weight)
bullContraindicationsndashAbsolute Prior intracranial hemorrhage known cerebral vascular lesion malignant intracranial neoplasm ischemic stroke within 3 months suspected aortic dissection active bleeding recent closed head injury or facial trauma within 3monthsndashRelative History of chronic severe HTN severeuncontrolled HTN at presentation (gt180110) history of ischemic stroke gt3 months traumaticprolonged CPR recent internal bleeding (2-4 weeks) pregnancy active peptic ulcer current anticoagulation
Primary PCI
bullPCI = Percutaneous Coronary Intervention
bullPTCA = Percutaneous Transluminal Coronary Angioplasty
bullPOBA = Plain Old Balloon Angioplasty
PROGNOSIS
bullDischarge usually 5 days after admissionbullSmoking CessationbullShort and Long-term survival depend upon resting LV function residual ischemic myocardium and susceptibility to ventricular arrhythmias
THE END
- CHEST PAIN SCENARIO 3 GROUP 10
- SCENARIO
- KEYWORD
- QUESTION
- DIFFERENTIAL DIAGNOSIS
- INTRODUCTION
- BASIC SCIENCE
- EKG
- Normal heart
- Myocardial Infarction Two to three days after an MI the myocyt
- Slide 11
- PATHOPHYSIOLOGY OF ST-ELEVATION MYOCARDIAL INFARCTION (STEMI)
- myocardial infarction
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- HYPOTENSION May trigger a dramatic sympathetic nervous system
- Slide 19
- Slide 21
- Left Ventricular Function Systolic Function
- Ventricular Remodeling
- references
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- PATHOLOGIC OF Q-WAVE
- PATHOMECANISM CHEST PAIN
- Slide 31
- SMOKING kills
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- ThE eND
-

BASIC SCIENCE
EKG
Normal heart
Myocardial InfarctionTwo to three days after an MI the myocytes show that they are irreversibly damaged Theyve lost their nuclei PMNs
(polymorphonuclear leukocytes) are the first inflammatory cells on the scene They will begin to clear away the necrotic tissue Later the macrophages will finish the job These dying myocytes will eventually be replaced with scar tissue
httpwwwkumceduinstructionmedicineanatomyhistowebpathpath01htm
httpwwwgooglecomimgreshl=enampgl=idampbiw=1366ampbih=624amptbm=ischamptbnid=KajG2QEK1-M4mMampimgrefurl=httpwwwmedicinenetcomheart_attack_pathology_photo_essaypage3htmampdocid=CZHmHLYLNv9ueMampimgurl=httpimagesmedicinenetcomimagesillustrationsmyocardial_infarction_1jpgampw=400amph=308ampei=8_KDUK3PH8nlrAeTzYHwBwampzoom=1ampiact=hcampvpx=398ampvpy=128ampdur=3820amphovh=197amphovw=256amptx=206ampty=150ampsig=116867615274730240580amppage=2amptbnh=151amptbnw=196ampstart=21ampndsp=27ampved=1t429r23s20i206
PATHOPHYSIOLOGY OF
ST-ELEVATION MYOCARDIAL
INFARCTION (STEMI)
myocardial infarction
A myocardial infarction is defined as
Elevated blood levels of cardiac enzymes
(CKMB or Troponin T)
One of the following criteria are met
The patient has typical
complaints
The ECG shows ST elevation or
depression
pathological Q waves develop
on the ECG
bull PATHOPHYSIOLOGY MIA prolonged imbalance between myocardial oxygen supply and demand leads to the death of myocardial tissue Coronary
atherosclerosis is an essential part of the process in most patients
Ischemic heart disease seems to progress through stages of fatty-streak deposition in coronary arteries to development of
fibro-fatty plaque which then increases in size until it causes luminal obstruction
leading to exertional angina
any stages in this process the atherosclerotic lesion may erode
ulcerate fissure or rupture thereby exposing subendothelial
vessel wall substances to the circulating blood
Procoagulant factors (such as tissue factor) reside within the plaque itself
and in the absence of counterbalancing antithrombotic factor (eg heparin tissue-factor-
inhibitor) and fibrinolytic activities (tissues plasminogen activator [t-PA]
and single-chain urokinase-type plasminogen activator) within the endothelial cells of the coronary
artery can cause thrombosis Recent work suggests that inflammation may play a pivotal role in
the genesis of plaque rupture Total thrombotic occlusion occurs most commonly in proximal coronary
arteries its presence has been documented during the first 4 hours
after infarction in more than 85 of the patients with ST segment elevation
(Crawford MH (2009))
This potent procoagulant stimulus results in thrombus development in
this region In general acute MI occurs when this thrombosis
propagates and occludes flow within the artery resulting in ischemia of
cardiomyocytes distal to the obstruction
The ECG leads in which pathologic Q waves appear reflect the anatomical site of an infarction
TABLE 1 Localization of Myocardial Infarction Anatomical Site Leads with Abnormal ECG
Complexes Coronary Artery Most Often
Responsible Inferior IIIIIaVF RCA
Anteroseptal V1-V2 LAD Anteroapical V3-V4 LAD(distal) Anterolateral V5-V6 I aVL CFX
Posterior V1-V2 (tall R wave not Q wave) RCA
The electrocardiographic differences between these types of MI are summarized as follow
Type of Infarction Pathologic Q waves Acute ST segment Deviation
Q-wave MI Yes ST elevation Non-Q-wave MI No ST depression (and or T
wave inversion)
Angina pectoris- Neck- Shoulder- Arms
ischemic myocardial cells release mediator such as adenosine and
lactate from into local nerve endings
discomfort often refer to other region of the C7 through
dermatome
provocative substances continue to accumulate and active afferent
nerve for longer period
ischemic in acute MI persist and proceed to necrosis
HYPOTENSION
May trigger a dramatic sympathetic nervous system response
Systemic sign of subsequent catecholamine release include diaphoresis (sweating) tachycardia and cool
and clammy skin
cause of vasoconstriction
Systolic Dysfunction
Decrease lungs compliance and stimulates juxtacappilary
receptors
Left ventricle contractility can be
reduced
J receptors effects a reflex that results in rapid shallow
breathing and evokes the subjective feeling of dyspnea
Increase in LV pressure compounded by the ischemia
induced stiffness of the chamber (diastolic dysfunction) is conveyed to the left atrium and pulmonary
veins
Decreasing the stroke volume and causing the diastolic
volume and pressure within the LV to rise
Ischemia affects large amount of myocardium
SERUM MARKER OF INFARCTION
Detection of cardiac-specific troponins and creatine kinase MB isoenzyme
Intracellular macromolecules leak into the cardiac interstitium and ultimately into the bloodstream
Necrosis of myocardial tissue Cause by disruption of the sarcolemma
MYOCARDIAL INFARTION
TYPICAL SYMPTOM- Crushing chest pain
more severe and wider than usual angina
SERUM BIOMARKSCreatine kinaseTroponin
ECG initial finding- St elevation- Q Wave
STEMI
Left Ventricular Function Systolic Function
Upon interruption of antegrade flow in an epicardial coronary artery the zone of myocardium supplied by that vessel immediately loses its ability to shorten and perform contractile work Four abnormal contraction patterns develop in sequence (1) dyssynchrony that is dissociation in the time course of contraction of adjacent segments(2) hypokinesis reduction in the extent of shortening (3) akinesis cessation of shortening and (4) dyskinesis paradoxical expansion and systolic bulging
Hyperkinesis of the remaining normal myocardium initially accompanies dysfunction of the infarcting segment The early hyperkinesis of the noninfarcted zones likely results from acute compensations including increased activity of the sympathetic nervous system and the Frank-Starling mechanism A portion of this compensatory hyperkinesis is ineffective work because contraction of the noninfarcted segments of myocardium hellip
Ventricular Remodelingbull As a consequence of STEMI the changes in left ventricular size shape and
thickness involving both the infarcted and the noninfarcted segments of the ventricle described earlier occur and are collectively referred to as ventricular remodeling which can in turn influence ventricular function and prognosis
bull A combination of changes in left ventricular dilation and hypertrophy of residual noninfarcted myocardium causes remodeling
bull After the size of infarction the two most important factors driving the process of left ventricular dilation are ventricular loading conditions and infarct artery patency
bull Elevated ventricular pressure contributes to increased wall stress and the risk of infarct expansion and a patent infarct artery accelerates myocardial scar formation and increases tissue turgor in the infarct zone reducing the risk of infarct expansion and ventricular dilation
Antman EM Morrow DA McCabe CH et al Enoxaparin versus unfractionated heparin with fibrinolysis for ST-elevation myocardial infarction N Engl J Med 2006 3541477
referencesSLIDE 2 Alpert JS Thygesen K Antman E and Bassand JP Myocardial infarction redefined--a consensus document of The Joint European Society of CardiologyAmerican College of Cardiology Committee for the redefinition of myocardial infarction J Am Coll Cardiol 2000 Sep 36(3) 959-69 pmid10987628bull Book of Pathophysiology of Heart Disease fourth edition editor Leonard SLilly page 179-
184bull ILMU PENYAKIT DALAM Jilid II Edisi V Editor Aru WSudoyo Bambang Setiyohadi
Idrus Alwi page1741-1744
ST elevation MI
ST segment elevation type of acute myocardial infarction require at least 1 mm (01 mV) of ST segment elevation in the limb leads and at least 2 mm elevation in the precordial leads
The clinician must therefore be well versed in recognizing the so-called ECG mimics of acute myocardial infarction which include
These elevations must be present in anatomically contiguous leads (I aVL V5 V6 correspond to the lateral wall V1-V2 correspond to the septal wall V3-V4 correspond to the anterior wall II III aVF correspond to the inferior wall)
left ventricular hypertrophy
left bundle branch block
hyperkalemia
early repolarization
ventricular aneurysm
12-lead electrocardiogram showing ST-segment elevation (orange) in I aVL and V1-V5 with reciprocal changes (blue) in the inferior leads indicative of an anterior wall myocardial infarction
An acute STEMI involving the inferior and right ventricular wall Reciprocal changes are seen in the anterior leads
PATHOLOGIC OF Q-WAVEPathologic Q waves
Any Q-wave in leads V2ndashV3 ge 002 s or QS complex in leads V2 and V3
Q-wave ge 003 s and gt 01 mV deep or QS complex in leads I II aVL aVF or V4ndashV6 in
any two leads of a contiguous lead grouping (I aVLV6 V4ndashV6 II III and aVF)
result of absence of electrical activity
previous myocardial infarction
The evolution of an infarct on the ECG ST elevation Q wave formation T wave inversion
normalisation with a persistent Q wave
PATHOMECANISM CHEST PAINhttpemedicinemedscapecomarticle150215-overview2
ProfDrPeter Kabo Bagaimana Menggunakan Obat-obat kardiovasculer secara Rasional
AtherosclerosisProduce endothelial derived constricting
factor (EDCF)
Increase tonus artery
coronary
Ischemic myocard
Aerobic glycolysis turn
to anerobic glycolysis
Production of adenosin
Diffuse to extracellular
space
Stimulate A1 receptor in cardiac
afferent nerve ending
Bind with somatic cervico
thoracalis nerve at
ascending pathway in
medulla spinalis
Chest pain
SMOKING KILLS
These effects could potentially trigger
symptoms of ischemia in such smokers
One might also expect that the hemodynamic effects of nicotine would contribute to endothelial damage and accelerate the progression of atherosclerosis
Lipolyis - increased levels of circulating free fatty acids
and glycerol in the blood and the resulting increase in fat
metabolism drives a demand for more oxygen leading to
increased coronary blood flow and myocardial oxygen
uptake
addition to its cardiovascular effects such as elevated heart
rate blood pressure and cardiac output
nicotine has metabolic effects in particular increased lipolysis
Nicotine is a sympathomimetic chemical that promotes the release of catecholamines and other
neurotransmitters
SIGNS AND SYMPTOMS
bullChest pain (pressuretightnessheaviness and might radiate to neck arm)
bullIngestion heartburnbullNausea VomitingbullSweatingbullWeaknessbullDizziness
httpwwwcardiosmartorgManageConditionDefaultaspxid=904 httpwwwncbinlmnihgovpmcarticlesPMC2233977
ADDITIONAL EXAMINATION1 Physical examination
Gen appearance Distress Levine signbullHeart rate pulse respirrate variablebullBlood pressure variablebullLow-grade feverbullExamination of jugular venous pulsationsbullPulmonary CracklesbullS4 gallop due to reduced LV compliancebullS3 gallop if LV dysfunction presentbullMurmurs Pericardial friction rubs
2 ECG
The key to rapid diagnosis and risk stratification for the patient with chest painbullTo be obtained within 10 minutes of arrival to Emergency DepartmentbullFor STEMI 1048774ST-segment elevation gt1mm in 2+ contiguous leads OR new left bundle branch block (LBBB)bullLocation of InfarctLeadsInferior MI II III aVFAnterior MI V2-V4Lateral MI I aVL V5-V6
3 Lab studies
Cardiac Biomarkers CK CK-MB cTnbullSerum ChemistriesbullRenal FunctionbullCoagulation StudiesbullComplete Blood Count
TREATMENTAspirin
bullRapidly blocks formation of thromboxaneA2 in platelets by cyclooxygenase inhibitionbull162-325mg chewed (promotes buccalabsorption)bullISIS-2ndash23 reduction in mortality largely additive to the reduction in mortality from streptokinaseOther Adjuvant TherapiesAnalgesicsbullNitratesbullBeta-blockersbullAce InhibitorsbullOxygenbullHeparinbullIV Glycoprotein IIbIIIaInhibitorsbullClopidogrelbullStatins
Thrombolytic TherapybullCommon AgentsbullTNK-tPA30-50mg IV bolusbullReteplase10U x 2 (each over 2 minutes) IVbullAlteplaseup to 100mg in 90mins (based on weight)
bullContraindicationsndashAbsolute Prior intracranial hemorrhage known cerebral vascular lesion malignant intracranial neoplasm ischemic stroke within 3 months suspected aortic dissection active bleeding recent closed head injury or facial trauma within 3monthsndashRelative History of chronic severe HTN severeuncontrolled HTN at presentation (gt180110) history of ischemic stroke gt3 months traumaticprolonged CPR recent internal bleeding (2-4 weeks) pregnancy active peptic ulcer current anticoagulation
Primary PCI
bullPCI = Percutaneous Coronary Intervention
bullPTCA = Percutaneous Transluminal Coronary Angioplasty
bullPOBA = Plain Old Balloon Angioplasty
PROGNOSIS
bullDischarge usually 5 days after admissionbullSmoking CessationbullShort and Long-term survival depend upon resting LV function residual ischemic myocardium and susceptibility to ventricular arrhythmias
THE END
- CHEST PAIN SCENARIO 3 GROUP 10
- SCENARIO
- KEYWORD
- QUESTION
- DIFFERENTIAL DIAGNOSIS
- INTRODUCTION
- BASIC SCIENCE
- EKG
- Normal heart
- Myocardial Infarction Two to three days after an MI the myocyt
- Slide 11
- PATHOPHYSIOLOGY OF ST-ELEVATION MYOCARDIAL INFARCTION (STEMI)
- myocardial infarction
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- HYPOTENSION May trigger a dramatic sympathetic nervous system
- Slide 19
- Slide 21
- Left Ventricular Function Systolic Function
- Ventricular Remodeling
- references
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- PATHOLOGIC OF Q-WAVE
- PATHOMECANISM CHEST PAIN
- Slide 31
- SMOKING kills
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- ThE eND
-

EKG
Normal heart
Myocardial InfarctionTwo to three days after an MI the myocytes show that they are irreversibly damaged Theyve lost their nuclei PMNs
(polymorphonuclear leukocytes) are the first inflammatory cells on the scene They will begin to clear away the necrotic tissue Later the macrophages will finish the job These dying myocytes will eventually be replaced with scar tissue
httpwwwkumceduinstructionmedicineanatomyhistowebpathpath01htm
httpwwwgooglecomimgreshl=enampgl=idampbiw=1366ampbih=624amptbm=ischamptbnid=KajG2QEK1-M4mMampimgrefurl=httpwwwmedicinenetcomheart_attack_pathology_photo_essaypage3htmampdocid=CZHmHLYLNv9ueMampimgurl=httpimagesmedicinenetcomimagesillustrationsmyocardial_infarction_1jpgampw=400amph=308ampei=8_KDUK3PH8nlrAeTzYHwBwampzoom=1ampiact=hcampvpx=398ampvpy=128ampdur=3820amphovh=197amphovw=256amptx=206ampty=150ampsig=116867615274730240580amppage=2amptbnh=151amptbnw=196ampstart=21ampndsp=27ampved=1t429r23s20i206
PATHOPHYSIOLOGY OF
ST-ELEVATION MYOCARDIAL
INFARCTION (STEMI)
myocardial infarction
A myocardial infarction is defined as
Elevated blood levels of cardiac enzymes
(CKMB or Troponin T)
One of the following criteria are met
The patient has typical
complaints
The ECG shows ST elevation or
depression
pathological Q waves develop
on the ECG
bull PATHOPHYSIOLOGY MIA prolonged imbalance between myocardial oxygen supply and demand leads to the death of myocardial tissue Coronary
atherosclerosis is an essential part of the process in most patients
Ischemic heart disease seems to progress through stages of fatty-streak deposition in coronary arteries to development of
fibro-fatty plaque which then increases in size until it causes luminal obstruction
leading to exertional angina
any stages in this process the atherosclerotic lesion may erode
ulcerate fissure or rupture thereby exposing subendothelial
vessel wall substances to the circulating blood
Procoagulant factors (such as tissue factor) reside within the plaque itself
and in the absence of counterbalancing antithrombotic factor (eg heparin tissue-factor-
inhibitor) and fibrinolytic activities (tissues plasminogen activator [t-PA]
and single-chain urokinase-type plasminogen activator) within the endothelial cells of the coronary
artery can cause thrombosis Recent work suggests that inflammation may play a pivotal role in
the genesis of plaque rupture Total thrombotic occlusion occurs most commonly in proximal coronary
arteries its presence has been documented during the first 4 hours
after infarction in more than 85 of the patients with ST segment elevation
(Crawford MH (2009))
This potent procoagulant stimulus results in thrombus development in
this region In general acute MI occurs when this thrombosis
propagates and occludes flow within the artery resulting in ischemia of
cardiomyocytes distal to the obstruction
The ECG leads in which pathologic Q waves appear reflect the anatomical site of an infarction
TABLE 1 Localization of Myocardial Infarction Anatomical Site Leads with Abnormal ECG
Complexes Coronary Artery Most Often
Responsible Inferior IIIIIaVF RCA
Anteroseptal V1-V2 LAD Anteroapical V3-V4 LAD(distal) Anterolateral V5-V6 I aVL CFX
Posterior V1-V2 (tall R wave not Q wave) RCA
The electrocardiographic differences between these types of MI are summarized as follow
Type of Infarction Pathologic Q waves Acute ST segment Deviation
Q-wave MI Yes ST elevation Non-Q-wave MI No ST depression (and or T
wave inversion)
Angina pectoris- Neck- Shoulder- Arms
ischemic myocardial cells release mediator such as adenosine and
lactate from into local nerve endings
discomfort often refer to other region of the C7 through
dermatome
provocative substances continue to accumulate and active afferent
nerve for longer period
ischemic in acute MI persist and proceed to necrosis
HYPOTENSION
May trigger a dramatic sympathetic nervous system response
Systemic sign of subsequent catecholamine release include diaphoresis (sweating) tachycardia and cool
and clammy skin
cause of vasoconstriction
Systolic Dysfunction
Decrease lungs compliance and stimulates juxtacappilary
receptors
Left ventricle contractility can be
reduced
J receptors effects a reflex that results in rapid shallow
breathing and evokes the subjective feeling of dyspnea
Increase in LV pressure compounded by the ischemia
induced stiffness of the chamber (diastolic dysfunction) is conveyed to the left atrium and pulmonary
veins
Decreasing the stroke volume and causing the diastolic
volume and pressure within the LV to rise
Ischemia affects large amount of myocardium
SERUM MARKER OF INFARCTION
Detection of cardiac-specific troponins and creatine kinase MB isoenzyme
Intracellular macromolecules leak into the cardiac interstitium and ultimately into the bloodstream
Necrosis of myocardial tissue Cause by disruption of the sarcolemma
MYOCARDIAL INFARTION
TYPICAL SYMPTOM- Crushing chest pain
more severe and wider than usual angina
SERUM BIOMARKSCreatine kinaseTroponin
ECG initial finding- St elevation- Q Wave
STEMI
Left Ventricular Function Systolic Function
Upon interruption of antegrade flow in an epicardial coronary artery the zone of myocardium supplied by that vessel immediately loses its ability to shorten and perform contractile work Four abnormal contraction patterns develop in sequence (1) dyssynchrony that is dissociation in the time course of contraction of adjacent segments(2) hypokinesis reduction in the extent of shortening (3) akinesis cessation of shortening and (4) dyskinesis paradoxical expansion and systolic bulging
Hyperkinesis of the remaining normal myocardium initially accompanies dysfunction of the infarcting segment The early hyperkinesis of the noninfarcted zones likely results from acute compensations including increased activity of the sympathetic nervous system and the Frank-Starling mechanism A portion of this compensatory hyperkinesis is ineffective work because contraction of the noninfarcted segments of myocardium hellip
Ventricular Remodelingbull As a consequence of STEMI the changes in left ventricular size shape and
thickness involving both the infarcted and the noninfarcted segments of the ventricle described earlier occur and are collectively referred to as ventricular remodeling which can in turn influence ventricular function and prognosis
bull A combination of changes in left ventricular dilation and hypertrophy of residual noninfarcted myocardium causes remodeling
bull After the size of infarction the two most important factors driving the process of left ventricular dilation are ventricular loading conditions and infarct artery patency
bull Elevated ventricular pressure contributes to increased wall stress and the risk of infarct expansion and a patent infarct artery accelerates myocardial scar formation and increases tissue turgor in the infarct zone reducing the risk of infarct expansion and ventricular dilation
Antman EM Morrow DA McCabe CH et al Enoxaparin versus unfractionated heparin with fibrinolysis for ST-elevation myocardial infarction N Engl J Med 2006 3541477
referencesSLIDE 2 Alpert JS Thygesen K Antman E and Bassand JP Myocardial infarction redefined--a consensus document of The Joint European Society of CardiologyAmerican College of Cardiology Committee for the redefinition of myocardial infarction J Am Coll Cardiol 2000 Sep 36(3) 959-69 pmid10987628bull Book of Pathophysiology of Heart Disease fourth edition editor Leonard SLilly page 179-
184bull ILMU PENYAKIT DALAM Jilid II Edisi V Editor Aru WSudoyo Bambang Setiyohadi
Idrus Alwi page1741-1744
ST elevation MI
ST segment elevation type of acute myocardial infarction require at least 1 mm (01 mV) of ST segment elevation in the limb leads and at least 2 mm elevation in the precordial leads
The clinician must therefore be well versed in recognizing the so-called ECG mimics of acute myocardial infarction which include
These elevations must be present in anatomically contiguous leads (I aVL V5 V6 correspond to the lateral wall V1-V2 correspond to the septal wall V3-V4 correspond to the anterior wall II III aVF correspond to the inferior wall)
left ventricular hypertrophy
left bundle branch block
hyperkalemia
early repolarization
ventricular aneurysm
12-lead electrocardiogram showing ST-segment elevation (orange) in I aVL and V1-V5 with reciprocal changes (blue) in the inferior leads indicative of an anterior wall myocardial infarction
An acute STEMI involving the inferior and right ventricular wall Reciprocal changes are seen in the anterior leads
PATHOLOGIC OF Q-WAVEPathologic Q waves
Any Q-wave in leads V2ndashV3 ge 002 s or QS complex in leads V2 and V3
Q-wave ge 003 s and gt 01 mV deep or QS complex in leads I II aVL aVF or V4ndashV6 in
any two leads of a contiguous lead grouping (I aVLV6 V4ndashV6 II III and aVF)
result of absence of electrical activity
previous myocardial infarction
The evolution of an infarct on the ECG ST elevation Q wave formation T wave inversion
normalisation with a persistent Q wave
PATHOMECANISM CHEST PAINhttpemedicinemedscapecomarticle150215-overview2
ProfDrPeter Kabo Bagaimana Menggunakan Obat-obat kardiovasculer secara Rasional
AtherosclerosisProduce endothelial derived constricting
factor (EDCF)
Increase tonus artery
coronary
Ischemic myocard
Aerobic glycolysis turn
to anerobic glycolysis
Production of adenosin
Diffuse to extracellular
space
Stimulate A1 receptor in cardiac
afferent nerve ending
Bind with somatic cervico
thoracalis nerve at
ascending pathway in
medulla spinalis
Chest pain
SMOKING KILLS
These effects could potentially trigger
symptoms of ischemia in such smokers
One might also expect that the hemodynamic effects of nicotine would contribute to endothelial damage and accelerate the progression of atherosclerosis
Lipolyis - increased levels of circulating free fatty acids
and glycerol in the blood and the resulting increase in fat
metabolism drives a demand for more oxygen leading to
increased coronary blood flow and myocardial oxygen
uptake
addition to its cardiovascular effects such as elevated heart
rate blood pressure and cardiac output
nicotine has metabolic effects in particular increased lipolysis
Nicotine is a sympathomimetic chemical that promotes the release of catecholamines and other
neurotransmitters
SIGNS AND SYMPTOMS
bullChest pain (pressuretightnessheaviness and might radiate to neck arm)
bullIngestion heartburnbullNausea VomitingbullSweatingbullWeaknessbullDizziness
httpwwwcardiosmartorgManageConditionDefaultaspxid=904 httpwwwncbinlmnihgovpmcarticlesPMC2233977
ADDITIONAL EXAMINATION1 Physical examination
Gen appearance Distress Levine signbullHeart rate pulse respirrate variablebullBlood pressure variablebullLow-grade feverbullExamination of jugular venous pulsationsbullPulmonary CracklesbullS4 gallop due to reduced LV compliancebullS3 gallop if LV dysfunction presentbullMurmurs Pericardial friction rubs
2 ECG
The key to rapid diagnosis and risk stratification for the patient with chest painbullTo be obtained within 10 minutes of arrival to Emergency DepartmentbullFor STEMI 1048774ST-segment elevation gt1mm in 2+ contiguous leads OR new left bundle branch block (LBBB)bullLocation of InfarctLeadsInferior MI II III aVFAnterior MI V2-V4Lateral MI I aVL V5-V6
3 Lab studies
Cardiac Biomarkers CK CK-MB cTnbullSerum ChemistriesbullRenal FunctionbullCoagulation StudiesbullComplete Blood Count
TREATMENTAspirin
bullRapidly blocks formation of thromboxaneA2 in platelets by cyclooxygenase inhibitionbull162-325mg chewed (promotes buccalabsorption)bullISIS-2ndash23 reduction in mortality largely additive to the reduction in mortality from streptokinaseOther Adjuvant TherapiesAnalgesicsbullNitratesbullBeta-blockersbullAce InhibitorsbullOxygenbullHeparinbullIV Glycoprotein IIbIIIaInhibitorsbullClopidogrelbullStatins
Thrombolytic TherapybullCommon AgentsbullTNK-tPA30-50mg IV bolusbullReteplase10U x 2 (each over 2 minutes) IVbullAlteplaseup to 100mg in 90mins (based on weight)
bullContraindicationsndashAbsolute Prior intracranial hemorrhage known cerebral vascular lesion malignant intracranial neoplasm ischemic stroke within 3 months suspected aortic dissection active bleeding recent closed head injury or facial trauma within 3monthsndashRelative History of chronic severe HTN severeuncontrolled HTN at presentation (gt180110) history of ischemic stroke gt3 months traumaticprolonged CPR recent internal bleeding (2-4 weeks) pregnancy active peptic ulcer current anticoagulation
Primary PCI
bullPCI = Percutaneous Coronary Intervention
bullPTCA = Percutaneous Transluminal Coronary Angioplasty
bullPOBA = Plain Old Balloon Angioplasty
PROGNOSIS
bullDischarge usually 5 days after admissionbullSmoking CessationbullShort and Long-term survival depend upon resting LV function residual ischemic myocardium and susceptibility to ventricular arrhythmias
THE END
- CHEST PAIN SCENARIO 3 GROUP 10
- SCENARIO
- KEYWORD
- QUESTION
- DIFFERENTIAL DIAGNOSIS
- INTRODUCTION
- BASIC SCIENCE
- EKG
- Normal heart
- Myocardial Infarction Two to three days after an MI the myocyt
- Slide 11
- PATHOPHYSIOLOGY OF ST-ELEVATION MYOCARDIAL INFARCTION (STEMI)
- myocardial infarction
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- HYPOTENSION May trigger a dramatic sympathetic nervous system
- Slide 19
- Slide 21
- Left Ventricular Function Systolic Function
- Ventricular Remodeling
- references
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- PATHOLOGIC OF Q-WAVE
- PATHOMECANISM CHEST PAIN
- Slide 31
- SMOKING kills
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- ThE eND
-

Normal heart
Myocardial InfarctionTwo to three days after an MI the myocytes show that they are irreversibly damaged Theyve lost their nuclei PMNs
(polymorphonuclear leukocytes) are the first inflammatory cells on the scene They will begin to clear away the necrotic tissue Later the macrophages will finish the job These dying myocytes will eventually be replaced with scar tissue
httpwwwkumceduinstructionmedicineanatomyhistowebpathpath01htm
httpwwwgooglecomimgreshl=enampgl=idampbiw=1366ampbih=624amptbm=ischamptbnid=KajG2QEK1-M4mMampimgrefurl=httpwwwmedicinenetcomheart_attack_pathology_photo_essaypage3htmampdocid=CZHmHLYLNv9ueMampimgurl=httpimagesmedicinenetcomimagesillustrationsmyocardial_infarction_1jpgampw=400amph=308ampei=8_KDUK3PH8nlrAeTzYHwBwampzoom=1ampiact=hcampvpx=398ampvpy=128ampdur=3820amphovh=197amphovw=256amptx=206ampty=150ampsig=116867615274730240580amppage=2amptbnh=151amptbnw=196ampstart=21ampndsp=27ampved=1t429r23s20i206
PATHOPHYSIOLOGY OF
ST-ELEVATION MYOCARDIAL
INFARCTION (STEMI)
myocardial infarction
A myocardial infarction is defined as
Elevated blood levels of cardiac enzymes
(CKMB or Troponin T)
One of the following criteria are met
The patient has typical
complaints
The ECG shows ST elevation or
depression
pathological Q waves develop
on the ECG
bull PATHOPHYSIOLOGY MIA prolonged imbalance between myocardial oxygen supply and demand leads to the death of myocardial tissue Coronary
atherosclerosis is an essential part of the process in most patients
Ischemic heart disease seems to progress through stages of fatty-streak deposition in coronary arteries to development of
fibro-fatty plaque which then increases in size until it causes luminal obstruction
leading to exertional angina
any stages in this process the atherosclerotic lesion may erode
ulcerate fissure or rupture thereby exposing subendothelial
vessel wall substances to the circulating blood
Procoagulant factors (such as tissue factor) reside within the plaque itself
and in the absence of counterbalancing antithrombotic factor (eg heparin tissue-factor-
inhibitor) and fibrinolytic activities (tissues plasminogen activator [t-PA]
and single-chain urokinase-type plasminogen activator) within the endothelial cells of the coronary
artery can cause thrombosis Recent work suggests that inflammation may play a pivotal role in
the genesis of plaque rupture Total thrombotic occlusion occurs most commonly in proximal coronary
arteries its presence has been documented during the first 4 hours
after infarction in more than 85 of the patients with ST segment elevation
(Crawford MH (2009))
This potent procoagulant stimulus results in thrombus development in
this region In general acute MI occurs when this thrombosis
propagates and occludes flow within the artery resulting in ischemia of
cardiomyocytes distal to the obstruction
The ECG leads in which pathologic Q waves appear reflect the anatomical site of an infarction
TABLE 1 Localization of Myocardial Infarction Anatomical Site Leads with Abnormal ECG
Complexes Coronary Artery Most Often
Responsible Inferior IIIIIaVF RCA
Anteroseptal V1-V2 LAD Anteroapical V3-V4 LAD(distal) Anterolateral V5-V6 I aVL CFX
Posterior V1-V2 (tall R wave not Q wave) RCA
The electrocardiographic differences between these types of MI are summarized as follow
Type of Infarction Pathologic Q waves Acute ST segment Deviation
Q-wave MI Yes ST elevation Non-Q-wave MI No ST depression (and or T
wave inversion)
Angina pectoris- Neck- Shoulder- Arms
ischemic myocardial cells release mediator such as adenosine and
lactate from into local nerve endings
discomfort often refer to other region of the C7 through
dermatome
provocative substances continue to accumulate and active afferent
nerve for longer period
ischemic in acute MI persist and proceed to necrosis
HYPOTENSION
May trigger a dramatic sympathetic nervous system response
Systemic sign of subsequent catecholamine release include diaphoresis (sweating) tachycardia and cool
and clammy skin
cause of vasoconstriction
Systolic Dysfunction
Decrease lungs compliance and stimulates juxtacappilary
receptors
Left ventricle contractility can be
reduced
J receptors effects a reflex that results in rapid shallow
breathing and evokes the subjective feeling of dyspnea
Increase in LV pressure compounded by the ischemia
induced stiffness of the chamber (diastolic dysfunction) is conveyed to the left atrium and pulmonary
veins
Decreasing the stroke volume and causing the diastolic
volume and pressure within the LV to rise
Ischemia affects large amount of myocardium
SERUM MARKER OF INFARCTION
Detection of cardiac-specific troponins and creatine kinase MB isoenzyme
Intracellular macromolecules leak into the cardiac interstitium and ultimately into the bloodstream
Necrosis of myocardial tissue Cause by disruption of the sarcolemma
MYOCARDIAL INFARTION
TYPICAL SYMPTOM- Crushing chest pain
more severe and wider than usual angina
SERUM BIOMARKSCreatine kinaseTroponin
ECG initial finding- St elevation- Q Wave
STEMI
Left Ventricular Function Systolic Function
Upon interruption of antegrade flow in an epicardial coronary artery the zone of myocardium supplied by that vessel immediately loses its ability to shorten and perform contractile work Four abnormal contraction patterns develop in sequence (1) dyssynchrony that is dissociation in the time course of contraction of adjacent segments(2) hypokinesis reduction in the extent of shortening (3) akinesis cessation of shortening and (4) dyskinesis paradoxical expansion and systolic bulging
Hyperkinesis of the remaining normal myocardium initially accompanies dysfunction of the infarcting segment The early hyperkinesis of the noninfarcted zones likely results from acute compensations including increased activity of the sympathetic nervous system and the Frank-Starling mechanism A portion of this compensatory hyperkinesis is ineffective work because contraction of the noninfarcted segments of myocardium hellip
Ventricular Remodelingbull As a consequence of STEMI the changes in left ventricular size shape and
thickness involving both the infarcted and the noninfarcted segments of the ventricle described earlier occur and are collectively referred to as ventricular remodeling which can in turn influence ventricular function and prognosis
bull A combination of changes in left ventricular dilation and hypertrophy of residual noninfarcted myocardium causes remodeling
bull After the size of infarction the two most important factors driving the process of left ventricular dilation are ventricular loading conditions and infarct artery patency
bull Elevated ventricular pressure contributes to increased wall stress and the risk of infarct expansion and a patent infarct artery accelerates myocardial scar formation and increases tissue turgor in the infarct zone reducing the risk of infarct expansion and ventricular dilation
Antman EM Morrow DA McCabe CH et al Enoxaparin versus unfractionated heparin with fibrinolysis for ST-elevation myocardial infarction N Engl J Med 2006 3541477
referencesSLIDE 2 Alpert JS Thygesen K Antman E and Bassand JP Myocardial infarction redefined--a consensus document of The Joint European Society of CardiologyAmerican College of Cardiology Committee for the redefinition of myocardial infarction J Am Coll Cardiol 2000 Sep 36(3) 959-69 pmid10987628bull Book of Pathophysiology of Heart Disease fourth edition editor Leonard SLilly page 179-
184bull ILMU PENYAKIT DALAM Jilid II Edisi V Editor Aru WSudoyo Bambang Setiyohadi
Idrus Alwi page1741-1744
ST elevation MI
ST segment elevation type of acute myocardial infarction require at least 1 mm (01 mV) of ST segment elevation in the limb leads and at least 2 mm elevation in the precordial leads
The clinician must therefore be well versed in recognizing the so-called ECG mimics of acute myocardial infarction which include
These elevations must be present in anatomically contiguous leads (I aVL V5 V6 correspond to the lateral wall V1-V2 correspond to the septal wall V3-V4 correspond to the anterior wall II III aVF correspond to the inferior wall)
left ventricular hypertrophy
left bundle branch block
hyperkalemia
early repolarization
ventricular aneurysm
12-lead electrocardiogram showing ST-segment elevation (orange) in I aVL and V1-V5 with reciprocal changes (blue) in the inferior leads indicative of an anterior wall myocardial infarction
An acute STEMI involving the inferior and right ventricular wall Reciprocal changes are seen in the anterior leads
PATHOLOGIC OF Q-WAVEPathologic Q waves
Any Q-wave in leads V2ndashV3 ge 002 s or QS complex in leads V2 and V3
Q-wave ge 003 s and gt 01 mV deep or QS complex in leads I II aVL aVF or V4ndashV6 in
any two leads of a contiguous lead grouping (I aVLV6 V4ndashV6 II III and aVF)
result of absence of electrical activity
previous myocardial infarction
The evolution of an infarct on the ECG ST elevation Q wave formation T wave inversion
normalisation with a persistent Q wave
PATHOMECANISM CHEST PAINhttpemedicinemedscapecomarticle150215-overview2
ProfDrPeter Kabo Bagaimana Menggunakan Obat-obat kardiovasculer secara Rasional
AtherosclerosisProduce endothelial derived constricting
factor (EDCF)
Increase tonus artery
coronary
Ischemic myocard
Aerobic glycolysis turn
to anerobic glycolysis
Production of adenosin
Diffuse to extracellular
space
Stimulate A1 receptor in cardiac
afferent nerve ending
Bind with somatic cervico
thoracalis nerve at
ascending pathway in
medulla spinalis
Chest pain
SMOKING KILLS
These effects could potentially trigger
symptoms of ischemia in such smokers
One might also expect that the hemodynamic effects of nicotine would contribute to endothelial damage and accelerate the progression of atherosclerosis
Lipolyis - increased levels of circulating free fatty acids
and glycerol in the blood and the resulting increase in fat
metabolism drives a demand for more oxygen leading to
increased coronary blood flow and myocardial oxygen
uptake
addition to its cardiovascular effects such as elevated heart
rate blood pressure and cardiac output
nicotine has metabolic effects in particular increased lipolysis
Nicotine is a sympathomimetic chemical that promotes the release of catecholamines and other
neurotransmitters
SIGNS AND SYMPTOMS
bullChest pain (pressuretightnessheaviness and might radiate to neck arm)
bullIngestion heartburnbullNausea VomitingbullSweatingbullWeaknessbullDizziness
httpwwwcardiosmartorgManageConditionDefaultaspxid=904 httpwwwncbinlmnihgovpmcarticlesPMC2233977
ADDITIONAL EXAMINATION1 Physical examination
Gen appearance Distress Levine signbullHeart rate pulse respirrate variablebullBlood pressure variablebullLow-grade feverbullExamination of jugular venous pulsationsbullPulmonary CracklesbullS4 gallop due to reduced LV compliancebullS3 gallop if LV dysfunction presentbullMurmurs Pericardial friction rubs
2 ECG
The key to rapid diagnosis and risk stratification for the patient with chest painbullTo be obtained within 10 minutes of arrival to Emergency DepartmentbullFor STEMI 1048774ST-segment elevation gt1mm in 2+ contiguous leads OR new left bundle branch block (LBBB)bullLocation of InfarctLeadsInferior MI II III aVFAnterior MI V2-V4Lateral MI I aVL V5-V6
3 Lab studies
Cardiac Biomarkers CK CK-MB cTnbullSerum ChemistriesbullRenal FunctionbullCoagulation StudiesbullComplete Blood Count
TREATMENTAspirin
bullRapidly blocks formation of thromboxaneA2 in platelets by cyclooxygenase inhibitionbull162-325mg chewed (promotes buccalabsorption)bullISIS-2ndash23 reduction in mortality largely additive to the reduction in mortality from streptokinaseOther Adjuvant TherapiesAnalgesicsbullNitratesbullBeta-blockersbullAce InhibitorsbullOxygenbullHeparinbullIV Glycoprotein IIbIIIaInhibitorsbullClopidogrelbullStatins
Thrombolytic TherapybullCommon AgentsbullTNK-tPA30-50mg IV bolusbullReteplase10U x 2 (each over 2 minutes) IVbullAlteplaseup to 100mg in 90mins (based on weight)
bullContraindicationsndashAbsolute Prior intracranial hemorrhage known cerebral vascular lesion malignant intracranial neoplasm ischemic stroke within 3 months suspected aortic dissection active bleeding recent closed head injury or facial trauma within 3monthsndashRelative History of chronic severe HTN severeuncontrolled HTN at presentation (gt180110) history of ischemic stroke gt3 months traumaticprolonged CPR recent internal bleeding (2-4 weeks) pregnancy active peptic ulcer current anticoagulation
Primary PCI
bullPCI = Percutaneous Coronary Intervention
bullPTCA = Percutaneous Transluminal Coronary Angioplasty
bullPOBA = Plain Old Balloon Angioplasty
PROGNOSIS
bullDischarge usually 5 days after admissionbullSmoking CessationbullShort and Long-term survival depend upon resting LV function residual ischemic myocardium and susceptibility to ventricular arrhythmias
THE END
- CHEST PAIN SCENARIO 3 GROUP 10
- SCENARIO
- KEYWORD
- QUESTION
- DIFFERENTIAL DIAGNOSIS
- INTRODUCTION
- BASIC SCIENCE
- EKG
- Normal heart
- Myocardial Infarction Two to three days after an MI the myocyt
- Slide 11
- PATHOPHYSIOLOGY OF ST-ELEVATION MYOCARDIAL INFARCTION (STEMI)
- myocardial infarction
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- HYPOTENSION May trigger a dramatic sympathetic nervous system
- Slide 19
- Slide 21
- Left Ventricular Function Systolic Function
- Ventricular Remodeling
- references
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- PATHOLOGIC OF Q-WAVE
- PATHOMECANISM CHEST PAIN
- Slide 31
- SMOKING kills
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- ThE eND
-

Myocardial InfarctionTwo to three days after an MI the myocytes show that they are irreversibly damaged Theyve lost their nuclei PMNs
(polymorphonuclear leukocytes) are the first inflammatory cells on the scene They will begin to clear away the necrotic tissue Later the macrophages will finish the job These dying myocytes will eventually be replaced with scar tissue
httpwwwkumceduinstructionmedicineanatomyhistowebpathpath01htm
httpwwwgooglecomimgreshl=enampgl=idampbiw=1366ampbih=624amptbm=ischamptbnid=KajG2QEK1-M4mMampimgrefurl=httpwwwmedicinenetcomheart_attack_pathology_photo_essaypage3htmampdocid=CZHmHLYLNv9ueMampimgurl=httpimagesmedicinenetcomimagesillustrationsmyocardial_infarction_1jpgampw=400amph=308ampei=8_KDUK3PH8nlrAeTzYHwBwampzoom=1ampiact=hcampvpx=398ampvpy=128ampdur=3820amphovh=197amphovw=256amptx=206ampty=150ampsig=116867615274730240580amppage=2amptbnh=151amptbnw=196ampstart=21ampndsp=27ampved=1t429r23s20i206
PATHOPHYSIOLOGY OF
ST-ELEVATION MYOCARDIAL
INFARCTION (STEMI)
myocardial infarction
A myocardial infarction is defined as
Elevated blood levels of cardiac enzymes
(CKMB or Troponin T)
One of the following criteria are met
The patient has typical
complaints
The ECG shows ST elevation or
depression
pathological Q waves develop
on the ECG
bull PATHOPHYSIOLOGY MIA prolonged imbalance between myocardial oxygen supply and demand leads to the death of myocardial tissue Coronary
atherosclerosis is an essential part of the process in most patients
Ischemic heart disease seems to progress through stages of fatty-streak deposition in coronary arteries to development of
fibro-fatty plaque which then increases in size until it causes luminal obstruction
leading to exertional angina
any stages in this process the atherosclerotic lesion may erode
ulcerate fissure or rupture thereby exposing subendothelial
vessel wall substances to the circulating blood
Procoagulant factors (such as tissue factor) reside within the plaque itself
and in the absence of counterbalancing antithrombotic factor (eg heparin tissue-factor-
inhibitor) and fibrinolytic activities (tissues plasminogen activator [t-PA]
and single-chain urokinase-type plasminogen activator) within the endothelial cells of the coronary
artery can cause thrombosis Recent work suggests that inflammation may play a pivotal role in
the genesis of plaque rupture Total thrombotic occlusion occurs most commonly in proximal coronary
arteries its presence has been documented during the first 4 hours
after infarction in more than 85 of the patients with ST segment elevation
(Crawford MH (2009))
This potent procoagulant stimulus results in thrombus development in
this region In general acute MI occurs when this thrombosis
propagates and occludes flow within the artery resulting in ischemia of
cardiomyocytes distal to the obstruction
The ECG leads in which pathologic Q waves appear reflect the anatomical site of an infarction
TABLE 1 Localization of Myocardial Infarction Anatomical Site Leads with Abnormal ECG
Complexes Coronary Artery Most Often
Responsible Inferior IIIIIaVF RCA
Anteroseptal V1-V2 LAD Anteroapical V3-V4 LAD(distal) Anterolateral V5-V6 I aVL CFX
Posterior V1-V2 (tall R wave not Q wave) RCA
The electrocardiographic differences between these types of MI are summarized as follow
Type of Infarction Pathologic Q waves Acute ST segment Deviation
Q-wave MI Yes ST elevation Non-Q-wave MI No ST depression (and or T
wave inversion)
Angina pectoris- Neck- Shoulder- Arms
ischemic myocardial cells release mediator such as adenosine and
lactate from into local nerve endings
discomfort often refer to other region of the C7 through
dermatome
provocative substances continue to accumulate and active afferent
nerve for longer period
ischemic in acute MI persist and proceed to necrosis
HYPOTENSION
May trigger a dramatic sympathetic nervous system response
Systemic sign of subsequent catecholamine release include diaphoresis (sweating) tachycardia and cool
and clammy skin
cause of vasoconstriction
Systolic Dysfunction
Decrease lungs compliance and stimulates juxtacappilary
receptors
Left ventricle contractility can be
reduced
J receptors effects a reflex that results in rapid shallow
breathing and evokes the subjective feeling of dyspnea
Increase in LV pressure compounded by the ischemia
induced stiffness of the chamber (diastolic dysfunction) is conveyed to the left atrium and pulmonary
veins
Decreasing the stroke volume and causing the diastolic
volume and pressure within the LV to rise
Ischemia affects large amount of myocardium
SERUM MARKER OF INFARCTION
Detection of cardiac-specific troponins and creatine kinase MB isoenzyme
Intracellular macromolecules leak into the cardiac interstitium and ultimately into the bloodstream
Necrosis of myocardial tissue Cause by disruption of the sarcolemma
MYOCARDIAL INFARTION
TYPICAL SYMPTOM- Crushing chest pain
more severe and wider than usual angina
SERUM BIOMARKSCreatine kinaseTroponin
ECG initial finding- St elevation- Q Wave
STEMI
Left Ventricular Function Systolic Function
Upon interruption of antegrade flow in an epicardial coronary artery the zone of myocardium supplied by that vessel immediately loses its ability to shorten and perform contractile work Four abnormal contraction patterns develop in sequence (1) dyssynchrony that is dissociation in the time course of contraction of adjacent segments(2) hypokinesis reduction in the extent of shortening (3) akinesis cessation of shortening and (4) dyskinesis paradoxical expansion and systolic bulging
Hyperkinesis of the remaining normal myocardium initially accompanies dysfunction of the infarcting segment The early hyperkinesis of the noninfarcted zones likely results from acute compensations including increased activity of the sympathetic nervous system and the Frank-Starling mechanism A portion of this compensatory hyperkinesis is ineffective work because contraction of the noninfarcted segments of myocardium hellip
Ventricular Remodelingbull As a consequence of STEMI the changes in left ventricular size shape and
thickness involving both the infarcted and the noninfarcted segments of the ventricle described earlier occur and are collectively referred to as ventricular remodeling which can in turn influence ventricular function and prognosis
bull A combination of changes in left ventricular dilation and hypertrophy of residual noninfarcted myocardium causes remodeling
bull After the size of infarction the two most important factors driving the process of left ventricular dilation are ventricular loading conditions and infarct artery patency
bull Elevated ventricular pressure contributes to increased wall stress and the risk of infarct expansion and a patent infarct artery accelerates myocardial scar formation and increases tissue turgor in the infarct zone reducing the risk of infarct expansion and ventricular dilation
Antman EM Morrow DA McCabe CH et al Enoxaparin versus unfractionated heparin with fibrinolysis for ST-elevation myocardial infarction N Engl J Med 2006 3541477
referencesSLIDE 2 Alpert JS Thygesen K Antman E and Bassand JP Myocardial infarction redefined--a consensus document of The Joint European Society of CardiologyAmerican College of Cardiology Committee for the redefinition of myocardial infarction J Am Coll Cardiol 2000 Sep 36(3) 959-69 pmid10987628bull Book of Pathophysiology of Heart Disease fourth edition editor Leonard SLilly page 179-
184bull ILMU PENYAKIT DALAM Jilid II Edisi V Editor Aru WSudoyo Bambang Setiyohadi
Idrus Alwi page1741-1744
ST elevation MI
ST segment elevation type of acute myocardial infarction require at least 1 mm (01 mV) of ST segment elevation in the limb leads and at least 2 mm elevation in the precordial leads
The clinician must therefore be well versed in recognizing the so-called ECG mimics of acute myocardial infarction which include
These elevations must be present in anatomically contiguous leads (I aVL V5 V6 correspond to the lateral wall V1-V2 correspond to the septal wall V3-V4 correspond to the anterior wall II III aVF correspond to the inferior wall)
left ventricular hypertrophy
left bundle branch block
hyperkalemia
early repolarization
ventricular aneurysm
12-lead electrocardiogram showing ST-segment elevation (orange) in I aVL and V1-V5 with reciprocal changes (blue) in the inferior leads indicative of an anterior wall myocardial infarction
An acute STEMI involving the inferior and right ventricular wall Reciprocal changes are seen in the anterior leads
PATHOLOGIC OF Q-WAVEPathologic Q waves
Any Q-wave in leads V2ndashV3 ge 002 s or QS complex in leads V2 and V3
Q-wave ge 003 s and gt 01 mV deep or QS complex in leads I II aVL aVF or V4ndashV6 in
any two leads of a contiguous lead grouping (I aVLV6 V4ndashV6 II III and aVF)
result of absence of electrical activity
previous myocardial infarction
The evolution of an infarct on the ECG ST elevation Q wave formation T wave inversion
normalisation with a persistent Q wave
PATHOMECANISM CHEST PAINhttpemedicinemedscapecomarticle150215-overview2
ProfDrPeter Kabo Bagaimana Menggunakan Obat-obat kardiovasculer secara Rasional
AtherosclerosisProduce endothelial derived constricting
factor (EDCF)
Increase tonus artery
coronary
Ischemic myocard
Aerobic glycolysis turn
to anerobic glycolysis
Production of adenosin
Diffuse to extracellular
space
Stimulate A1 receptor in cardiac
afferent nerve ending
Bind with somatic cervico
thoracalis nerve at
ascending pathway in
medulla spinalis
Chest pain
SMOKING KILLS
These effects could potentially trigger
symptoms of ischemia in such smokers
One might also expect that the hemodynamic effects of nicotine would contribute to endothelial damage and accelerate the progression of atherosclerosis
Lipolyis - increased levels of circulating free fatty acids
and glycerol in the blood and the resulting increase in fat
metabolism drives a demand for more oxygen leading to
increased coronary blood flow and myocardial oxygen
uptake
addition to its cardiovascular effects such as elevated heart
rate blood pressure and cardiac output
nicotine has metabolic effects in particular increased lipolysis
Nicotine is a sympathomimetic chemical that promotes the release of catecholamines and other
neurotransmitters
SIGNS AND SYMPTOMS
bullChest pain (pressuretightnessheaviness and might radiate to neck arm)
bullIngestion heartburnbullNausea VomitingbullSweatingbullWeaknessbullDizziness
httpwwwcardiosmartorgManageConditionDefaultaspxid=904 httpwwwncbinlmnihgovpmcarticlesPMC2233977
ADDITIONAL EXAMINATION1 Physical examination
Gen appearance Distress Levine signbullHeart rate pulse respirrate variablebullBlood pressure variablebullLow-grade feverbullExamination of jugular venous pulsationsbullPulmonary CracklesbullS4 gallop due to reduced LV compliancebullS3 gallop if LV dysfunction presentbullMurmurs Pericardial friction rubs
2 ECG
The key to rapid diagnosis and risk stratification for the patient with chest painbullTo be obtained within 10 minutes of arrival to Emergency DepartmentbullFor STEMI 1048774ST-segment elevation gt1mm in 2+ contiguous leads OR new left bundle branch block (LBBB)bullLocation of InfarctLeadsInferior MI II III aVFAnterior MI V2-V4Lateral MI I aVL V5-V6
3 Lab studies
Cardiac Biomarkers CK CK-MB cTnbullSerum ChemistriesbullRenal FunctionbullCoagulation StudiesbullComplete Blood Count
TREATMENTAspirin
bullRapidly blocks formation of thromboxaneA2 in platelets by cyclooxygenase inhibitionbull162-325mg chewed (promotes buccalabsorption)bullISIS-2ndash23 reduction in mortality largely additive to the reduction in mortality from streptokinaseOther Adjuvant TherapiesAnalgesicsbullNitratesbullBeta-blockersbullAce InhibitorsbullOxygenbullHeparinbullIV Glycoprotein IIbIIIaInhibitorsbullClopidogrelbullStatins
Thrombolytic TherapybullCommon AgentsbullTNK-tPA30-50mg IV bolusbullReteplase10U x 2 (each over 2 minutes) IVbullAlteplaseup to 100mg in 90mins (based on weight)
bullContraindicationsndashAbsolute Prior intracranial hemorrhage known cerebral vascular lesion malignant intracranial neoplasm ischemic stroke within 3 months suspected aortic dissection active bleeding recent closed head injury or facial trauma within 3monthsndashRelative History of chronic severe HTN severeuncontrolled HTN at presentation (gt180110) history of ischemic stroke gt3 months traumaticprolonged CPR recent internal bleeding (2-4 weeks) pregnancy active peptic ulcer current anticoagulation
Primary PCI
bullPCI = Percutaneous Coronary Intervention
bullPTCA = Percutaneous Transluminal Coronary Angioplasty
bullPOBA = Plain Old Balloon Angioplasty
PROGNOSIS
bullDischarge usually 5 days after admissionbullSmoking CessationbullShort and Long-term survival depend upon resting LV function residual ischemic myocardium and susceptibility to ventricular arrhythmias
THE END
- CHEST PAIN SCENARIO 3 GROUP 10
- SCENARIO
- KEYWORD
- QUESTION
- DIFFERENTIAL DIAGNOSIS
- INTRODUCTION
- BASIC SCIENCE
- EKG
- Normal heart
- Myocardial Infarction Two to three days after an MI the myocyt
- Slide 11
- PATHOPHYSIOLOGY OF ST-ELEVATION MYOCARDIAL INFARCTION (STEMI)
- myocardial infarction
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- HYPOTENSION May trigger a dramatic sympathetic nervous system
- Slide 19
- Slide 21
- Left Ventricular Function Systolic Function
- Ventricular Remodeling
- references
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- PATHOLOGIC OF Q-WAVE
- PATHOMECANISM CHEST PAIN
- Slide 31
- SMOKING kills
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- ThE eND
-

httpwwwgooglecomimgreshl=enampgl=idampbiw=1366ampbih=624amptbm=ischamptbnid=KajG2QEK1-M4mMampimgrefurl=httpwwwmedicinenetcomheart_attack_pathology_photo_essaypage3htmampdocid=CZHmHLYLNv9ueMampimgurl=httpimagesmedicinenetcomimagesillustrationsmyocardial_infarction_1jpgampw=400amph=308ampei=8_KDUK3PH8nlrAeTzYHwBwampzoom=1ampiact=hcampvpx=398ampvpy=128ampdur=3820amphovh=197amphovw=256amptx=206ampty=150ampsig=116867615274730240580amppage=2amptbnh=151amptbnw=196ampstart=21ampndsp=27ampved=1t429r23s20i206
PATHOPHYSIOLOGY OF
ST-ELEVATION MYOCARDIAL
INFARCTION (STEMI)
myocardial infarction
A myocardial infarction is defined as
Elevated blood levels of cardiac enzymes
(CKMB or Troponin T)
One of the following criteria are met
The patient has typical
complaints
The ECG shows ST elevation or
depression
pathological Q waves develop
on the ECG
bull PATHOPHYSIOLOGY MIA prolonged imbalance between myocardial oxygen supply and demand leads to the death of myocardial tissue Coronary
atherosclerosis is an essential part of the process in most patients
Ischemic heart disease seems to progress through stages of fatty-streak deposition in coronary arteries to development of
fibro-fatty plaque which then increases in size until it causes luminal obstruction
leading to exertional angina
any stages in this process the atherosclerotic lesion may erode
ulcerate fissure or rupture thereby exposing subendothelial
vessel wall substances to the circulating blood
Procoagulant factors (such as tissue factor) reside within the plaque itself
and in the absence of counterbalancing antithrombotic factor (eg heparin tissue-factor-
inhibitor) and fibrinolytic activities (tissues plasminogen activator [t-PA]
and single-chain urokinase-type plasminogen activator) within the endothelial cells of the coronary
artery can cause thrombosis Recent work suggests that inflammation may play a pivotal role in
the genesis of plaque rupture Total thrombotic occlusion occurs most commonly in proximal coronary
arteries its presence has been documented during the first 4 hours
after infarction in more than 85 of the patients with ST segment elevation
(Crawford MH (2009))
This potent procoagulant stimulus results in thrombus development in
this region In general acute MI occurs when this thrombosis
propagates and occludes flow within the artery resulting in ischemia of
cardiomyocytes distal to the obstruction
The ECG leads in which pathologic Q waves appear reflect the anatomical site of an infarction
TABLE 1 Localization of Myocardial Infarction Anatomical Site Leads with Abnormal ECG
Complexes Coronary Artery Most Often
Responsible Inferior IIIIIaVF RCA
Anteroseptal V1-V2 LAD Anteroapical V3-V4 LAD(distal) Anterolateral V5-V6 I aVL CFX
Posterior V1-V2 (tall R wave not Q wave) RCA
The electrocardiographic differences between these types of MI are summarized as follow
Type of Infarction Pathologic Q waves Acute ST segment Deviation
Q-wave MI Yes ST elevation Non-Q-wave MI No ST depression (and or T
wave inversion)
Angina pectoris- Neck- Shoulder- Arms
ischemic myocardial cells release mediator such as adenosine and
lactate from into local nerve endings
discomfort often refer to other region of the C7 through
dermatome
provocative substances continue to accumulate and active afferent
nerve for longer period
ischemic in acute MI persist and proceed to necrosis
HYPOTENSION
May trigger a dramatic sympathetic nervous system response
Systemic sign of subsequent catecholamine release include diaphoresis (sweating) tachycardia and cool
and clammy skin
cause of vasoconstriction
Systolic Dysfunction
Decrease lungs compliance and stimulates juxtacappilary
receptors
Left ventricle contractility can be
reduced
J receptors effects a reflex that results in rapid shallow
breathing and evokes the subjective feeling of dyspnea
Increase in LV pressure compounded by the ischemia
induced stiffness of the chamber (diastolic dysfunction) is conveyed to the left atrium and pulmonary
veins
Decreasing the stroke volume and causing the diastolic
volume and pressure within the LV to rise
Ischemia affects large amount of myocardium
SERUM MARKER OF INFARCTION
Detection of cardiac-specific troponins and creatine kinase MB isoenzyme
Intracellular macromolecules leak into the cardiac interstitium and ultimately into the bloodstream
Necrosis of myocardial tissue Cause by disruption of the sarcolemma
MYOCARDIAL INFARTION
TYPICAL SYMPTOM- Crushing chest pain
more severe and wider than usual angina
SERUM BIOMARKSCreatine kinaseTroponin
ECG initial finding- St elevation- Q Wave
STEMI
Left Ventricular Function Systolic Function
Upon interruption of antegrade flow in an epicardial coronary artery the zone of myocardium supplied by that vessel immediately loses its ability to shorten and perform contractile work Four abnormal contraction patterns develop in sequence (1) dyssynchrony that is dissociation in the time course of contraction of adjacent segments(2) hypokinesis reduction in the extent of shortening (3) akinesis cessation of shortening and (4) dyskinesis paradoxical expansion and systolic bulging
Hyperkinesis of the remaining normal myocardium initially accompanies dysfunction of the infarcting segment The early hyperkinesis of the noninfarcted zones likely results from acute compensations including increased activity of the sympathetic nervous system and the Frank-Starling mechanism A portion of this compensatory hyperkinesis is ineffective work because contraction of the noninfarcted segments of myocardium hellip
Ventricular Remodelingbull As a consequence of STEMI the changes in left ventricular size shape and
thickness involving both the infarcted and the noninfarcted segments of the ventricle described earlier occur and are collectively referred to as ventricular remodeling which can in turn influence ventricular function and prognosis
bull A combination of changes in left ventricular dilation and hypertrophy of residual noninfarcted myocardium causes remodeling
bull After the size of infarction the two most important factors driving the process of left ventricular dilation are ventricular loading conditions and infarct artery patency
bull Elevated ventricular pressure contributes to increased wall stress and the risk of infarct expansion and a patent infarct artery accelerates myocardial scar formation and increases tissue turgor in the infarct zone reducing the risk of infarct expansion and ventricular dilation
Antman EM Morrow DA McCabe CH et al Enoxaparin versus unfractionated heparin with fibrinolysis for ST-elevation myocardial infarction N Engl J Med 2006 3541477
referencesSLIDE 2 Alpert JS Thygesen K Antman E and Bassand JP Myocardial infarction redefined--a consensus document of The Joint European Society of CardiologyAmerican College of Cardiology Committee for the redefinition of myocardial infarction J Am Coll Cardiol 2000 Sep 36(3) 959-69 pmid10987628bull Book of Pathophysiology of Heart Disease fourth edition editor Leonard SLilly page 179-
184bull ILMU PENYAKIT DALAM Jilid II Edisi V Editor Aru WSudoyo Bambang Setiyohadi
Idrus Alwi page1741-1744
ST elevation MI
ST segment elevation type of acute myocardial infarction require at least 1 mm (01 mV) of ST segment elevation in the limb leads and at least 2 mm elevation in the precordial leads
The clinician must therefore be well versed in recognizing the so-called ECG mimics of acute myocardial infarction which include
These elevations must be present in anatomically contiguous leads (I aVL V5 V6 correspond to the lateral wall V1-V2 correspond to the septal wall V3-V4 correspond to the anterior wall II III aVF correspond to the inferior wall)
left ventricular hypertrophy
left bundle branch block
hyperkalemia
early repolarization
ventricular aneurysm
12-lead electrocardiogram showing ST-segment elevation (orange) in I aVL and V1-V5 with reciprocal changes (blue) in the inferior leads indicative of an anterior wall myocardial infarction
An acute STEMI involving the inferior and right ventricular wall Reciprocal changes are seen in the anterior leads
PATHOLOGIC OF Q-WAVEPathologic Q waves
Any Q-wave in leads V2ndashV3 ge 002 s or QS complex in leads V2 and V3
Q-wave ge 003 s and gt 01 mV deep or QS complex in leads I II aVL aVF or V4ndashV6 in
any two leads of a contiguous lead grouping (I aVLV6 V4ndashV6 II III and aVF)
result of absence of electrical activity
previous myocardial infarction
The evolution of an infarct on the ECG ST elevation Q wave formation T wave inversion
normalisation with a persistent Q wave
PATHOMECANISM CHEST PAINhttpemedicinemedscapecomarticle150215-overview2
ProfDrPeter Kabo Bagaimana Menggunakan Obat-obat kardiovasculer secara Rasional
AtherosclerosisProduce endothelial derived constricting
factor (EDCF)
Increase tonus artery
coronary
Ischemic myocard
Aerobic glycolysis turn
to anerobic glycolysis
Production of adenosin
Diffuse to extracellular
space
Stimulate A1 receptor in cardiac
afferent nerve ending
Bind with somatic cervico
thoracalis nerve at
ascending pathway in
medulla spinalis
Chest pain
SMOKING KILLS
These effects could potentially trigger
symptoms of ischemia in such smokers
One might also expect that the hemodynamic effects of nicotine would contribute to endothelial damage and accelerate the progression of atherosclerosis
Lipolyis - increased levels of circulating free fatty acids
and glycerol in the blood and the resulting increase in fat
metabolism drives a demand for more oxygen leading to
increased coronary blood flow and myocardial oxygen
uptake
addition to its cardiovascular effects such as elevated heart
rate blood pressure and cardiac output
nicotine has metabolic effects in particular increased lipolysis
Nicotine is a sympathomimetic chemical that promotes the release of catecholamines and other
neurotransmitters
SIGNS AND SYMPTOMS
bullChest pain (pressuretightnessheaviness and might radiate to neck arm)
bullIngestion heartburnbullNausea VomitingbullSweatingbullWeaknessbullDizziness
httpwwwcardiosmartorgManageConditionDefaultaspxid=904 httpwwwncbinlmnihgovpmcarticlesPMC2233977
ADDITIONAL EXAMINATION1 Physical examination
Gen appearance Distress Levine signbullHeart rate pulse respirrate variablebullBlood pressure variablebullLow-grade feverbullExamination of jugular venous pulsationsbullPulmonary CracklesbullS4 gallop due to reduced LV compliancebullS3 gallop if LV dysfunction presentbullMurmurs Pericardial friction rubs
2 ECG
The key to rapid diagnosis and risk stratification for the patient with chest painbullTo be obtained within 10 minutes of arrival to Emergency DepartmentbullFor STEMI 1048774ST-segment elevation gt1mm in 2+ contiguous leads OR new left bundle branch block (LBBB)bullLocation of InfarctLeadsInferior MI II III aVFAnterior MI V2-V4Lateral MI I aVL V5-V6
3 Lab studies
Cardiac Biomarkers CK CK-MB cTnbullSerum ChemistriesbullRenal FunctionbullCoagulation StudiesbullComplete Blood Count
TREATMENTAspirin
bullRapidly blocks formation of thromboxaneA2 in platelets by cyclooxygenase inhibitionbull162-325mg chewed (promotes buccalabsorption)bullISIS-2ndash23 reduction in mortality largely additive to the reduction in mortality from streptokinaseOther Adjuvant TherapiesAnalgesicsbullNitratesbullBeta-blockersbullAce InhibitorsbullOxygenbullHeparinbullIV Glycoprotein IIbIIIaInhibitorsbullClopidogrelbullStatins
Thrombolytic TherapybullCommon AgentsbullTNK-tPA30-50mg IV bolusbullReteplase10U x 2 (each over 2 minutes) IVbullAlteplaseup to 100mg in 90mins (based on weight)
bullContraindicationsndashAbsolute Prior intracranial hemorrhage known cerebral vascular lesion malignant intracranial neoplasm ischemic stroke within 3 months suspected aortic dissection active bleeding recent closed head injury or facial trauma within 3monthsndashRelative History of chronic severe HTN severeuncontrolled HTN at presentation (gt180110) history of ischemic stroke gt3 months traumaticprolonged CPR recent internal bleeding (2-4 weeks) pregnancy active peptic ulcer current anticoagulation
Primary PCI
bullPCI = Percutaneous Coronary Intervention
bullPTCA = Percutaneous Transluminal Coronary Angioplasty
bullPOBA = Plain Old Balloon Angioplasty
PROGNOSIS
bullDischarge usually 5 days after admissionbullSmoking CessationbullShort and Long-term survival depend upon resting LV function residual ischemic myocardium and susceptibility to ventricular arrhythmias
THE END
- CHEST PAIN SCENARIO 3 GROUP 10
- SCENARIO
- KEYWORD
- QUESTION
- DIFFERENTIAL DIAGNOSIS
- INTRODUCTION
- BASIC SCIENCE
- EKG
- Normal heart
- Myocardial Infarction Two to three days after an MI the myocyt
- Slide 11
- PATHOPHYSIOLOGY OF ST-ELEVATION MYOCARDIAL INFARCTION (STEMI)
- myocardial infarction
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- HYPOTENSION May trigger a dramatic sympathetic nervous system
- Slide 19
- Slide 21
- Left Ventricular Function Systolic Function
- Ventricular Remodeling
- references
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- PATHOLOGIC OF Q-WAVE
- PATHOMECANISM CHEST PAIN
- Slide 31
- SMOKING kills
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- ThE eND
-

PATHOPHYSIOLOGY OF
ST-ELEVATION MYOCARDIAL
INFARCTION (STEMI)
myocardial infarction
A myocardial infarction is defined as
Elevated blood levels of cardiac enzymes
(CKMB or Troponin T)
One of the following criteria are met
The patient has typical
complaints
The ECG shows ST elevation or
depression
pathological Q waves develop
on the ECG
bull PATHOPHYSIOLOGY MIA prolonged imbalance between myocardial oxygen supply and demand leads to the death of myocardial tissue Coronary
atherosclerosis is an essential part of the process in most patients
Ischemic heart disease seems to progress through stages of fatty-streak deposition in coronary arteries to development of
fibro-fatty plaque which then increases in size until it causes luminal obstruction
leading to exertional angina
any stages in this process the atherosclerotic lesion may erode
ulcerate fissure or rupture thereby exposing subendothelial
vessel wall substances to the circulating blood
Procoagulant factors (such as tissue factor) reside within the plaque itself
and in the absence of counterbalancing antithrombotic factor (eg heparin tissue-factor-
inhibitor) and fibrinolytic activities (tissues plasminogen activator [t-PA]
and single-chain urokinase-type plasminogen activator) within the endothelial cells of the coronary
artery can cause thrombosis Recent work suggests that inflammation may play a pivotal role in
the genesis of plaque rupture Total thrombotic occlusion occurs most commonly in proximal coronary
arteries its presence has been documented during the first 4 hours
after infarction in more than 85 of the patients with ST segment elevation
(Crawford MH (2009))
This potent procoagulant stimulus results in thrombus development in
this region In general acute MI occurs when this thrombosis
propagates and occludes flow within the artery resulting in ischemia of
cardiomyocytes distal to the obstruction
The ECG leads in which pathologic Q waves appear reflect the anatomical site of an infarction
TABLE 1 Localization of Myocardial Infarction Anatomical Site Leads with Abnormal ECG
Complexes Coronary Artery Most Often
Responsible Inferior IIIIIaVF RCA
Anteroseptal V1-V2 LAD Anteroapical V3-V4 LAD(distal) Anterolateral V5-V6 I aVL CFX
Posterior V1-V2 (tall R wave not Q wave) RCA
The electrocardiographic differences between these types of MI are summarized as follow
Type of Infarction Pathologic Q waves Acute ST segment Deviation
Q-wave MI Yes ST elevation Non-Q-wave MI No ST depression (and or T
wave inversion)
Angina pectoris- Neck- Shoulder- Arms
ischemic myocardial cells release mediator such as adenosine and
lactate from into local nerve endings
discomfort often refer to other region of the C7 through
dermatome
provocative substances continue to accumulate and active afferent
nerve for longer period
ischemic in acute MI persist and proceed to necrosis
HYPOTENSION
May trigger a dramatic sympathetic nervous system response
Systemic sign of subsequent catecholamine release include diaphoresis (sweating) tachycardia and cool
and clammy skin
cause of vasoconstriction
Systolic Dysfunction
Decrease lungs compliance and stimulates juxtacappilary
receptors
Left ventricle contractility can be
reduced
J receptors effects a reflex that results in rapid shallow
breathing and evokes the subjective feeling of dyspnea
Increase in LV pressure compounded by the ischemia
induced stiffness of the chamber (diastolic dysfunction) is conveyed to the left atrium and pulmonary
veins
Decreasing the stroke volume and causing the diastolic
volume and pressure within the LV to rise
Ischemia affects large amount of myocardium
SERUM MARKER OF INFARCTION
Detection of cardiac-specific troponins and creatine kinase MB isoenzyme
Intracellular macromolecules leak into the cardiac interstitium and ultimately into the bloodstream
Necrosis of myocardial tissue Cause by disruption of the sarcolemma
MYOCARDIAL INFARTION
TYPICAL SYMPTOM- Crushing chest pain
more severe and wider than usual angina
SERUM BIOMARKSCreatine kinaseTroponin
ECG initial finding- St elevation- Q Wave
STEMI
Left Ventricular Function Systolic Function
Upon interruption of antegrade flow in an epicardial coronary artery the zone of myocardium supplied by that vessel immediately loses its ability to shorten and perform contractile work Four abnormal contraction patterns develop in sequence (1) dyssynchrony that is dissociation in the time course of contraction of adjacent segments(2) hypokinesis reduction in the extent of shortening (3) akinesis cessation of shortening and (4) dyskinesis paradoxical expansion and systolic bulging
Hyperkinesis of the remaining normal myocardium initially accompanies dysfunction of the infarcting segment The early hyperkinesis of the noninfarcted zones likely results from acute compensations including increased activity of the sympathetic nervous system and the Frank-Starling mechanism A portion of this compensatory hyperkinesis is ineffective work because contraction of the noninfarcted segments of myocardium hellip
Ventricular Remodelingbull As a consequence of STEMI the changes in left ventricular size shape and
thickness involving both the infarcted and the noninfarcted segments of the ventricle described earlier occur and are collectively referred to as ventricular remodeling which can in turn influence ventricular function and prognosis
bull A combination of changes in left ventricular dilation and hypertrophy of residual noninfarcted myocardium causes remodeling
bull After the size of infarction the two most important factors driving the process of left ventricular dilation are ventricular loading conditions and infarct artery patency
bull Elevated ventricular pressure contributes to increased wall stress and the risk of infarct expansion and a patent infarct artery accelerates myocardial scar formation and increases tissue turgor in the infarct zone reducing the risk of infarct expansion and ventricular dilation
Antman EM Morrow DA McCabe CH et al Enoxaparin versus unfractionated heparin with fibrinolysis for ST-elevation myocardial infarction N Engl J Med 2006 3541477
referencesSLIDE 2 Alpert JS Thygesen K Antman E and Bassand JP Myocardial infarction redefined--a consensus document of The Joint European Society of CardiologyAmerican College of Cardiology Committee for the redefinition of myocardial infarction J Am Coll Cardiol 2000 Sep 36(3) 959-69 pmid10987628bull Book of Pathophysiology of Heart Disease fourth edition editor Leonard SLilly page 179-
184bull ILMU PENYAKIT DALAM Jilid II Edisi V Editor Aru WSudoyo Bambang Setiyohadi
Idrus Alwi page1741-1744
ST elevation MI
ST segment elevation type of acute myocardial infarction require at least 1 mm (01 mV) of ST segment elevation in the limb leads and at least 2 mm elevation in the precordial leads
The clinician must therefore be well versed in recognizing the so-called ECG mimics of acute myocardial infarction which include
These elevations must be present in anatomically contiguous leads (I aVL V5 V6 correspond to the lateral wall V1-V2 correspond to the septal wall V3-V4 correspond to the anterior wall II III aVF correspond to the inferior wall)
left ventricular hypertrophy
left bundle branch block
hyperkalemia
early repolarization
ventricular aneurysm
12-lead electrocardiogram showing ST-segment elevation (orange) in I aVL and V1-V5 with reciprocal changes (blue) in the inferior leads indicative of an anterior wall myocardial infarction
An acute STEMI involving the inferior and right ventricular wall Reciprocal changes are seen in the anterior leads
PATHOLOGIC OF Q-WAVEPathologic Q waves
Any Q-wave in leads V2ndashV3 ge 002 s or QS complex in leads V2 and V3
Q-wave ge 003 s and gt 01 mV deep or QS complex in leads I II aVL aVF or V4ndashV6 in
any two leads of a contiguous lead grouping (I aVLV6 V4ndashV6 II III and aVF)
result of absence of electrical activity
previous myocardial infarction
The evolution of an infarct on the ECG ST elevation Q wave formation T wave inversion
normalisation with a persistent Q wave
PATHOMECANISM CHEST PAINhttpemedicinemedscapecomarticle150215-overview2
ProfDrPeter Kabo Bagaimana Menggunakan Obat-obat kardiovasculer secara Rasional
AtherosclerosisProduce endothelial derived constricting
factor (EDCF)
Increase tonus artery
coronary
Ischemic myocard
Aerobic glycolysis turn
to anerobic glycolysis
Production of adenosin
Diffuse to extracellular
space
Stimulate A1 receptor in cardiac
afferent nerve ending
Bind with somatic cervico
thoracalis nerve at
ascending pathway in
medulla spinalis
Chest pain
SMOKING KILLS
These effects could potentially trigger
symptoms of ischemia in such smokers
One might also expect that the hemodynamic effects of nicotine would contribute to endothelial damage and accelerate the progression of atherosclerosis
Lipolyis - increased levels of circulating free fatty acids
and glycerol in the blood and the resulting increase in fat
metabolism drives a demand for more oxygen leading to
increased coronary blood flow and myocardial oxygen
uptake
addition to its cardiovascular effects such as elevated heart
rate blood pressure and cardiac output
nicotine has metabolic effects in particular increased lipolysis
Nicotine is a sympathomimetic chemical that promotes the release of catecholamines and other
neurotransmitters
SIGNS AND SYMPTOMS
bullChest pain (pressuretightnessheaviness and might radiate to neck arm)
bullIngestion heartburnbullNausea VomitingbullSweatingbullWeaknessbullDizziness
httpwwwcardiosmartorgManageConditionDefaultaspxid=904 httpwwwncbinlmnihgovpmcarticlesPMC2233977
ADDITIONAL EXAMINATION1 Physical examination
Gen appearance Distress Levine signbullHeart rate pulse respirrate variablebullBlood pressure variablebullLow-grade feverbullExamination of jugular venous pulsationsbullPulmonary CracklesbullS4 gallop due to reduced LV compliancebullS3 gallop if LV dysfunction presentbullMurmurs Pericardial friction rubs
2 ECG
The key to rapid diagnosis and risk stratification for the patient with chest painbullTo be obtained within 10 minutes of arrival to Emergency DepartmentbullFor STEMI 1048774ST-segment elevation gt1mm in 2+ contiguous leads OR new left bundle branch block (LBBB)bullLocation of InfarctLeadsInferior MI II III aVFAnterior MI V2-V4Lateral MI I aVL V5-V6
3 Lab studies
Cardiac Biomarkers CK CK-MB cTnbullSerum ChemistriesbullRenal FunctionbullCoagulation StudiesbullComplete Blood Count
TREATMENTAspirin
bullRapidly blocks formation of thromboxaneA2 in platelets by cyclooxygenase inhibitionbull162-325mg chewed (promotes buccalabsorption)bullISIS-2ndash23 reduction in mortality largely additive to the reduction in mortality from streptokinaseOther Adjuvant TherapiesAnalgesicsbullNitratesbullBeta-blockersbullAce InhibitorsbullOxygenbullHeparinbullIV Glycoprotein IIbIIIaInhibitorsbullClopidogrelbullStatins
Thrombolytic TherapybullCommon AgentsbullTNK-tPA30-50mg IV bolusbullReteplase10U x 2 (each over 2 minutes) IVbullAlteplaseup to 100mg in 90mins (based on weight)
bullContraindicationsndashAbsolute Prior intracranial hemorrhage known cerebral vascular lesion malignant intracranial neoplasm ischemic stroke within 3 months suspected aortic dissection active bleeding recent closed head injury or facial trauma within 3monthsndashRelative History of chronic severe HTN severeuncontrolled HTN at presentation (gt180110) history of ischemic stroke gt3 months traumaticprolonged CPR recent internal bleeding (2-4 weeks) pregnancy active peptic ulcer current anticoagulation
Primary PCI
bullPCI = Percutaneous Coronary Intervention
bullPTCA = Percutaneous Transluminal Coronary Angioplasty
bullPOBA = Plain Old Balloon Angioplasty
PROGNOSIS
bullDischarge usually 5 days after admissionbullSmoking CessationbullShort and Long-term survival depend upon resting LV function residual ischemic myocardium and susceptibility to ventricular arrhythmias
THE END
- CHEST PAIN SCENARIO 3 GROUP 10
- SCENARIO
- KEYWORD
- QUESTION
- DIFFERENTIAL DIAGNOSIS
- INTRODUCTION
- BASIC SCIENCE
- EKG
- Normal heart
- Myocardial Infarction Two to three days after an MI the myocyt
- Slide 11
- PATHOPHYSIOLOGY OF ST-ELEVATION MYOCARDIAL INFARCTION (STEMI)
- myocardial infarction
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- HYPOTENSION May trigger a dramatic sympathetic nervous system
- Slide 19
- Slide 21
- Left Ventricular Function Systolic Function
- Ventricular Remodeling
- references
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- PATHOLOGIC OF Q-WAVE
- PATHOMECANISM CHEST PAIN
- Slide 31
- SMOKING kills
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- ThE eND
-

myocardial infarction
A myocardial infarction is defined as
Elevated blood levels of cardiac enzymes
(CKMB or Troponin T)
One of the following criteria are met
The patient has typical
complaints
The ECG shows ST elevation or
depression
pathological Q waves develop
on the ECG
bull PATHOPHYSIOLOGY MIA prolonged imbalance between myocardial oxygen supply and demand leads to the death of myocardial tissue Coronary
atherosclerosis is an essential part of the process in most patients
Ischemic heart disease seems to progress through stages of fatty-streak deposition in coronary arteries to development of
fibro-fatty plaque which then increases in size until it causes luminal obstruction
leading to exertional angina
any stages in this process the atherosclerotic lesion may erode
ulcerate fissure or rupture thereby exposing subendothelial
vessel wall substances to the circulating blood
Procoagulant factors (such as tissue factor) reside within the plaque itself
and in the absence of counterbalancing antithrombotic factor (eg heparin tissue-factor-
inhibitor) and fibrinolytic activities (tissues plasminogen activator [t-PA]
and single-chain urokinase-type plasminogen activator) within the endothelial cells of the coronary
artery can cause thrombosis Recent work suggests that inflammation may play a pivotal role in
the genesis of plaque rupture Total thrombotic occlusion occurs most commonly in proximal coronary
arteries its presence has been documented during the first 4 hours
after infarction in more than 85 of the patients with ST segment elevation
(Crawford MH (2009))
This potent procoagulant stimulus results in thrombus development in
this region In general acute MI occurs when this thrombosis
propagates and occludes flow within the artery resulting in ischemia of
cardiomyocytes distal to the obstruction
The ECG leads in which pathologic Q waves appear reflect the anatomical site of an infarction
TABLE 1 Localization of Myocardial Infarction Anatomical Site Leads with Abnormal ECG
Complexes Coronary Artery Most Often
Responsible Inferior IIIIIaVF RCA
Anteroseptal V1-V2 LAD Anteroapical V3-V4 LAD(distal) Anterolateral V5-V6 I aVL CFX
Posterior V1-V2 (tall R wave not Q wave) RCA
The electrocardiographic differences between these types of MI are summarized as follow
Type of Infarction Pathologic Q waves Acute ST segment Deviation
Q-wave MI Yes ST elevation Non-Q-wave MI No ST depression (and or T
wave inversion)
Angina pectoris- Neck- Shoulder- Arms
ischemic myocardial cells release mediator such as adenosine and
lactate from into local nerve endings
discomfort often refer to other region of the C7 through
dermatome
provocative substances continue to accumulate and active afferent
nerve for longer period
ischemic in acute MI persist and proceed to necrosis
HYPOTENSION
May trigger a dramatic sympathetic nervous system response
Systemic sign of subsequent catecholamine release include diaphoresis (sweating) tachycardia and cool
and clammy skin
cause of vasoconstriction
Systolic Dysfunction
Decrease lungs compliance and stimulates juxtacappilary
receptors
Left ventricle contractility can be
reduced
J receptors effects a reflex that results in rapid shallow
breathing and evokes the subjective feeling of dyspnea
Increase in LV pressure compounded by the ischemia
induced stiffness of the chamber (diastolic dysfunction) is conveyed to the left atrium and pulmonary
veins
Decreasing the stroke volume and causing the diastolic
volume and pressure within the LV to rise
Ischemia affects large amount of myocardium
SERUM MARKER OF INFARCTION
Detection of cardiac-specific troponins and creatine kinase MB isoenzyme
Intracellular macromolecules leak into the cardiac interstitium and ultimately into the bloodstream
Necrosis of myocardial tissue Cause by disruption of the sarcolemma
MYOCARDIAL INFARTION
TYPICAL SYMPTOM- Crushing chest pain
more severe and wider than usual angina
SERUM BIOMARKSCreatine kinaseTroponin
ECG initial finding- St elevation- Q Wave
STEMI
Left Ventricular Function Systolic Function
Upon interruption of antegrade flow in an epicardial coronary artery the zone of myocardium supplied by that vessel immediately loses its ability to shorten and perform contractile work Four abnormal contraction patterns develop in sequence (1) dyssynchrony that is dissociation in the time course of contraction of adjacent segments(2) hypokinesis reduction in the extent of shortening (3) akinesis cessation of shortening and (4) dyskinesis paradoxical expansion and systolic bulging
Hyperkinesis of the remaining normal myocardium initially accompanies dysfunction of the infarcting segment The early hyperkinesis of the noninfarcted zones likely results from acute compensations including increased activity of the sympathetic nervous system and the Frank-Starling mechanism A portion of this compensatory hyperkinesis is ineffective work because contraction of the noninfarcted segments of myocardium hellip
Ventricular Remodelingbull As a consequence of STEMI the changes in left ventricular size shape and
thickness involving both the infarcted and the noninfarcted segments of the ventricle described earlier occur and are collectively referred to as ventricular remodeling which can in turn influence ventricular function and prognosis
bull A combination of changes in left ventricular dilation and hypertrophy of residual noninfarcted myocardium causes remodeling
bull After the size of infarction the two most important factors driving the process of left ventricular dilation are ventricular loading conditions and infarct artery patency
bull Elevated ventricular pressure contributes to increased wall stress and the risk of infarct expansion and a patent infarct artery accelerates myocardial scar formation and increases tissue turgor in the infarct zone reducing the risk of infarct expansion and ventricular dilation
Antman EM Morrow DA McCabe CH et al Enoxaparin versus unfractionated heparin with fibrinolysis for ST-elevation myocardial infarction N Engl J Med 2006 3541477
referencesSLIDE 2 Alpert JS Thygesen K Antman E and Bassand JP Myocardial infarction redefined--a consensus document of The Joint European Society of CardiologyAmerican College of Cardiology Committee for the redefinition of myocardial infarction J Am Coll Cardiol 2000 Sep 36(3) 959-69 pmid10987628bull Book of Pathophysiology of Heart Disease fourth edition editor Leonard SLilly page 179-
184bull ILMU PENYAKIT DALAM Jilid II Edisi V Editor Aru WSudoyo Bambang Setiyohadi
Idrus Alwi page1741-1744
ST elevation MI
ST segment elevation type of acute myocardial infarction require at least 1 mm (01 mV) of ST segment elevation in the limb leads and at least 2 mm elevation in the precordial leads
The clinician must therefore be well versed in recognizing the so-called ECG mimics of acute myocardial infarction which include
These elevations must be present in anatomically contiguous leads (I aVL V5 V6 correspond to the lateral wall V1-V2 correspond to the septal wall V3-V4 correspond to the anterior wall II III aVF correspond to the inferior wall)
left ventricular hypertrophy
left bundle branch block
hyperkalemia
early repolarization
ventricular aneurysm
12-lead electrocardiogram showing ST-segment elevation (orange) in I aVL and V1-V5 with reciprocal changes (blue) in the inferior leads indicative of an anterior wall myocardial infarction
An acute STEMI involving the inferior and right ventricular wall Reciprocal changes are seen in the anterior leads
PATHOLOGIC OF Q-WAVEPathologic Q waves
Any Q-wave in leads V2ndashV3 ge 002 s or QS complex in leads V2 and V3
Q-wave ge 003 s and gt 01 mV deep or QS complex in leads I II aVL aVF or V4ndashV6 in
any two leads of a contiguous lead grouping (I aVLV6 V4ndashV6 II III and aVF)
result of absence of electrical activity
previous myocardial infarction
The evolution of an infarct on the ECG ST elevation Q wave formation T wave inversion
normalisation with a persistent Q wave
PATHOMECANISM CHEST PAINhttpemedicinemedscapecomarticle150215-overview2
ProfDrPeter Kabo Bagaimana Menggunakan Obat-obat kardiovasculer secara Rasional
AtherosclerosisProduce endothelial derived constricting
factor (EDCF)
Increase tonus artery
coronary
Ischemic myocard
Aerobic glycolysis turn
to anerobic glycolysis
Production of adenosin
Diffuse to extracellular
space
Stimulate A1 receptor in cardiac
afferent nerve ending
Bind with somatic cervico
thoracalis nerve at
ascending pathway in
medulla spinalis
Chest pain
SMOKING KILLS
These effects could potentially trigger
symptoms of ischemia in such smokers
One might also expect that the hemodynamic effects of nicotine would contribute to endothelial damage and accelerate the progression of atherosclerosis
Lipolyis - increased levels of circulating free fatty acids
and glycerol in the blood and the resulting increase in fat
metabolism drives a demand for more oxygen leading to
increased coronary blood flow and myocardial oxygen
uptake
addition to its cardiovascular effects such as elevated heart
rate blood pressure and cardiac output
nicotine has metabolic effects in particular increased lipolysis
Nicotine is a sympathomimetic chemical that promotes the release of catecholamines and other
neurotransmitters
SIGNS AND SYMPTOMS
bullChest pain (pressuretightnessheaviness and might radiate to neck arm)
bullIngestion heartburnbullNausea VomitingbullSweatingbullWeaknessbullDizziness
httpwwwcardiosmartorgManageConditionDefaultaspxid=904 httpwwwncbinlmnihgovpmcarticlesPMC2233977
ADDITIONAL EXAMINATION1 Physical examination
Gen appearance Distress Levine signbullHeart rate pulse respirrate variablebullBlood pressure variablebullLow-grade feverbullExamination of jugular venous pulsationsbullPulmonary CracklesbullS4 gallop due to reduced LV compliancebullS3 gallop if LV dysfunction presentbullMurmurs Pericardial friction rubs
2 ECG
The key to rapid diagnosis and risk stratification for the patient with chest painbullTo be obtained within 10 minutes of arrival to Emergency DepartmentbullFor STEMI 1048774ST-segment elevation gt1mm in 2+ contiguous leads OR new left bundle branch block (LBBB)bullLocation of InfarctLeadsInferior MI II III aVFAnterior MI V2-V4Lateral MI I aVL V5-V6
3 Lab studies
Cardiac Biomarkers CK CK-MB cTnbullSerum ChemistriesbullRenal FunctionbullCoagulation StudiesbullComplete Blood Count
TREATMENTAspirin
bullRapidly blocks formation of thromboxaneA2 in platelets by cyclooxygenase inhibitionbull162-325mg chewed (promotes buccalabsorption)bullISIS-2ndash23 reduction in mortality largely additive to the reduction in mortality from streptokinaseOther Adjuvant TherapiesAnalgesicsbullNitratesbullBeta-blockersbullAce InhibitorsbullOxygenbullHeparinbullIV Glycoprotein IIbIIIaInhibitorsbullClopidogrelbullStatins
Thrombolytic TherapybullCommon AgentsbullTNK-tPA30-50mg IV bolusbullReteplase10U x 2 (each over 2 minutes) IVbullAlteplaseup to 100mg in 90mins (based on weight)
bullContraindicationsndashAbsolute Prior intracranial hemorrhage known cerebral vascular lesion malignant intracranial neoplasm ischemic stroke within 3 months suspected aortic dissection active bleeding recent closed head injury or facial trauma within 3monthsndashRelative History of chronic severe HTN severeuncontrolled HTN at presentation (gt180110) history of ischemic stroke gt3 months traumaticprolonged CPR recent internal bleeding (2-4 weeks) pregnancy active peptic ulcer current anticoagulation
Primary PCI
bullPCI = Percutaneous Coronary Intervention
bullPTCA = Percutaneous Transluminal Coronary Angioplasty
bullPOBA = Plain Old Balloon Angioplasty
PROGNOSIS
bullDischarge usually 5 days after admissionbullSmoking CessationbullShort and Long-term survival depend upon resting LV function residual ischemic myocardium and susceptibility to ventricular arrhythmias
THE END
- CHEST PAIN SCENARIO 3 GROUP 10
- SCENARIO
- KEYWORD
- QUESTION
- DIFFERENTIAL DIAGNOSIS
- INTRODUCTION
- BASIC SCIENCE
- EKG
- Normal heart
- Myocardial Infarction Two to three days after an MI the myocyt
- Slide 11
- PATHOPHYSIOLOGY OF ST-ELEVATION MYOCARDIAL INFARCTION (STEMI)
- myocardial infarction
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- HYPOTENSION May trigger a dramatic sympathetic nervous system
- Slide 19
- Slide 21
- Left Ventricular Function Systolic Function
- Ventricular Remodeling
- references
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- PATHOLOGIC OF Q-WAVE
- PATHOMECANISM CHEST PAIN
- Slide 31
- SMOKING kills
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- ThE eND
-

bull PATHOPHYSIOLOGY MIA prolonged imbalance between myocardial oxygen supply and demand leads to the death of myocardial tissue Coronary
atherosclerosis is an essential part of the process in most patients
Ischemic heart disease seems to progress through stages of fatty-streak deposition in coronary arteries to development of
fibro-fatty plaque which then increases in size until it causes luminal obstruction
leading to exertional angina
any stages in this process the atherosclerotic lesion may erode
ulcerate fissure or rupture thereby exposing subendothelial
vessel wall substances to the circulating blood
Procoagulant factors (such as tissue factor) reside within the plaque itself
and in the absence of counterbalancing antithrombotic factor (eg heparin tissue-factor-
inhibitor) and fibrinolytic activities (tissues plasminogen activator [t-PA]
and single-chain urokinase-type plasminogen activator) within the endothelial cells of the coronary
artery can cause thrombosis Recent work suggests that inflammation may play a pivotal role in
the genesis of plaque rupture Total thrombotic occlusion occurs most commonly in proximal coronary
arteries its presence has been documented during the first 4 hours
after infarction in more than 85 of the patients with ST segment elevation
(Crawford MH (2009))
This potent procoagulant stimulus results in thrombus development in
this region In general acute MI occurs when this thrombosis
propagates and occludes flow within the artery resulting in ischemia of
cardiomyocytes distal to the obstruction
The ECG leads in which pathologic Q waves appear reflect the anatomical site of an infarction
TABLE 1 Localization of Myocardial Infarction Anatomical Site Leads with Abnormal ECG
Complexes Coronary Artery Most Often
Responsible Inferior IIIIIaVF RCA
Anteroseptal V1-V2 LAD Anteroapical V3-V4 LAD(distal) Anterolateral V5-V6 I aVL CFX
Posterior V1-V2 (tall R wave not Q wave) RCA
The electrocardiographic differences between these types of MI are summarized as follow
Type of Infarction Pathologic Q waves Acute ST segment Deviation
Q-wave MI Yes ST elevation Non-Q-wave MI No ST depression (and or T
wave inversion)
Angina pectoris- Neck- Shoulder- Arms
ischemic myocardial cells release mediator such as adenosine and
lactate from into local nerve endings
discomfort often refer to other region of the C7 through
dermatome
provocative substances continue to accumulate and active afferent
nerve for longer period
ischemic in acute MI persist and proceed to necrosis
HYPOTENSION
May trigger a dramatic sympathetic nervous system response
Systemic sign of subsequent catecholamine release include diaphoresis (sweating) tachycardia and cool
and clammy skin
cause of vasoconstriction
Systolic Dysfunction
Decrease lungs compliance and stimulates juxtacappilary
receptors
Left ventricle contractility can be
reduced
J receptors effects a reflex that results in rapid shallow
breathing and evokes the subjective feeling of dyspnea
Increase in LV pressure compounded by the ischemia
induced stiffness of the chamber (diastolic dysfunction) is conveyed to the left atrium and pulmonary
veins
Decreasing the stroke volume and causing the diastolic
volume and pressure within the LV to rise
Ischemia affects large amount of myocardium
SERUM MARKER OF INFARCTION
Detection of cardiac-specific troponins and creatine kinase MB isoenzyme
Intracellular macromolecules leak into the cardiac interstitium and ultimately into the bloodstream
Necrosis of myocardial tissue Cause by disruption of the sarcolemma
MYOCARDIAL INFARTION
TYPICAL SYMPTOM- Crushing chest pain
more severe and wider than usual angina
SERUM BIOMARKSCreatine kinaseTroponin
ECG initial finding- St elevation- Q Wave
STEMI
Left Ventricular Function Systolic Function
Upon interruption of antegrade flow in an epicardial coronary artery the zone of myocardium supplied by that vessel immediately loses its ability to shorten and perform contractile work Four abnormal contraction patterns develop in sequence (1) dyssynchrony that is dissociation in the time course of contraction of adjacent segments(2) hypokinesis reduction in the extent of shortening (3) akinesis cessation of shortening and (4) dyskinesis paradoxical expansion and systolic bulging
Hyperkinesis of the remaining normal myocardium initially accompanies dysfunction of the infarcting segment The early hyperkinesis of the noninfarcted zones likely results from acute compensations including increased activity of the sympathetic nervous system and the Frank-Starling mechanism A portion of this compensatory hyperkinesis is ineffective work because contraction of the noninfarcted segments of myocardium hellip
Ventricular Remodelingbull As a consequence of STEMI the changes in left ventricular size shape and
thickness involving both the infarcted and the noninfarcted segments of the ventricle described earlier occur and are collectively referred to as ventricular remodeling which can in turn influence ventricular function and prognosis
bull A combination of changes in left ventricular dilation and hypertrophy of residual noninfarcted myocardium causes remodeling
bull After the size of infarction the two most important factors driving the process of left ventricular dilation are ventricular loading conditions and infarct artery patency
bull Elevated ventricular pressure contributes to increased wall stress and the risk of infarct expansion and a patent infarct artery accelerates myocardial scar formation and increases tissue turgor in the infarct zone reducing the risk of infarct expansion and ventricular dilation
Antman EM Morrow DA McCabe CH et al Enoxaparin versus unfractionated heparin with fibrinolysis for ST-elevation myocardial infarction N Engl J Med 2006 3541477
referencesSLIDE 2 Alpert JS Thygesen K Antman E and Bassand JP Myocardial infarction redefined--a consensus document of The Joint European Society of CardiologyAmerican College of Cardiology Committee for the redefinition of myocardial infarction J Am Coll Cardiol 2000 Sep 36(3) 959-69 pmid10987628bull Book of Pathophysiology of Heart Disease fourth edition editor Leonard SLilly page 179-
184bull ILMU PENYAKIT DALAM Jilid II Edisi V Editor Aru WSudoyo Bambang Setiyohadi
Idrus Alwi page1741-1744
ST elevation MI
ST segment elevation type of acute myocardial infarction require at least 1 mm (01 mV) of ST segment elevation in the limb leads and at least 2 mm elevation in the precordial leads
The clinician must therefore be well versed in recognizing the so-called ECG mimics of acute myocardial infarction which include
These elevations must be present in anatomically contiguous leads (I aVL V5 V6 correspond to the lateral wall V1-V2 correspond to the septal wall V3-V4 correspond to the anterior wall II III aVF correspond to the inferior wall)
left ventricular hypertrophy
left bundle branch block
hyperkalemia
early repolarization
ventricular aneurysm
12-lead electrocardiogram showing ST-segment elevation (orange) in I aVL and V1-V5 with reciprocal changes (blue) in the inferior leads indicative of an anterior wall myocardial infarction
An acute STEMI involving the inferior and right ventricular wall Reciprocal changes are seen in the anterior leads
PATHOLOGIC OF Q-WAVEPathologic Q waves
Any Q-wave in leads V2ndashV3 ge 002 s or QS complex in leads V2 and V3
Q-wave ge 003 s and gt 01 mV deep or QS complex in leads I II aVL aVF or V4ndashV6 in
any two leads of a contiguous lead grouping (I aVLV6 V4ndashV6 II III and aVF)
result of absence of electrical activity
previous myocardial infarction
The evolution of an infarct on the ECG ST elevation Q wave formation T wave inversion
normalisation with a persistent Q wave
PATHOMECANISM CHEST PAINhttpemedicinemedscapecomarticle150215-overview2
ProfDrPeter Kabo Bagaimana Menggunakan Obat-obat kardiovasculer secara Rasional
AtherosclerosisProduce endothelial derived constricting
factor (EDCF)
Increase tonus artery
coronary
Ischemic myocard
Aerobic glycolysis turn
to anerobic glycolysis
Production of adenosin
Diffuse to extracellular
space
Stimulate A1 receptor in cardiac
afferent nerve ending
Bind with somatic cervico
thoracalis nerve at
ascending pathway in
medulla spinalis
Chest pain
SMOKING KILLS
These effects could potentially trigger
symptoms of ischemia in such smokers
One might also expect that the hemodynamic effects of nicotine would contribute to endothelial damage and accelerate the progression of atherosclerosis
Lipolyis - increased levels of circulating free fatty acids
and glycerol in the blood and the resulting increase in fat
metabolism drives a demand for more oxygen leading to
increased coronary blood flow and myocardial oxygen
uptake
addition to its cardiovascular effects such as elevated heart
rate blood pressure and cardiac output
nicotine has metabolic effects in particular increased lipolysis
Nicotine is a sympathomimetic chemical that promotes the release of catecholamines and other
neurotransmitters
SIGNS AND SYMPTOMS
bullChest pain (pressuretightnessheaviness and might radiate to neck arm)
bullIngestion heartburnbullNausea VomitingbullSweatingbullWeaknessbullDizziness
httpwwwcardiosmartorgManageConditionDefaultaspxid=904 httpwwwncbinlmnihgovpmcarticlesPMC2233977
ADDITIONAL EXAMINATION1 Physical examination
Gen appearance Distress Levine signbullHeart rate pulse respirrate variablebullBlood pressure variablebullLow-grade feverbullExamination of jugular venous pulsationsbullPulmonary CracklesbullS4 gallop due to reduced LV compliancebullS3 gallop if LV dysfunction presentbullMurmurs Pericardial friction rubs
2 ECG
The key to rapid diagnosis and risk stratification for the patient with chest painbullTo be obtained within 10 minutes of arrival to Emergency DepartmentbullFor STEMI 1048774ST-segment elevation gt1mm in 2+ contiguous leads OR new left bundle branch block (LBBB)bullLocation of InfarctLeadsInferior MI II III aVFAnterior MI V2-V4Lateral MI I aVL V5-V6
3 Lab studies
Cardiac Biomarkers CK CK-MB cTnbullSerum ChemistriesbullRenal FunctionbullCoagulation StudiesbullComplete Blood Count
TREATMENTAspirin
bullRapidly blocks formation of thromboxaneA2 in platelets by cyclooxygenase inhibitionbull162-325mg chewed (promotes buccalabsorption)bullISIS-2ndash23 reduction in mortality largely additive to the reduction in mortality from streptokinaseOther Adjuvant TherapiesAnalgesicsbullNitratesbullBeta-blockersbullAce InhibitorsbullOxygenbullHeparinbullIV Glycoprotein IIbIIIaInhibitorsbullClopidogrelbullStatins
Thrombolytic TherapybullCommon AgentsbullTNK-tPA30-50mg IV bolusbullReteplase10U x 2 (each over 2 minutes) IVbullAlteplaseup to 100mg in 90mins (based on weight)
bullContraindicationsndashAbsolute Prior intracranial hemorrhage known cerebral vascular lesion malignant intracranial neoplasm ischemic stroke within 3 months suspected aortic dissection active bleeding recent closed head injury or facial trauma within 3monthsndashRelative History of chronic severe HTN severeuncontrolled HTN at presentation (gt180110) history of ischemic stroke gt3 months traumaticprolonged CPR recent internal bleeding (2-4 weeks) pregnancy active peptic ulcer current anticoagulation
Primary PCI
bullPCI = Percutaneous Coronary Intervention
bullPTCA = Percutaneous Transluminal Coronary Angioplasty
bullPOBA = Plain Old Balloon Angioplasty
PROGNOSIS
bullDischarge usually 5 days after admissionbullSmoking CessationbullShort and Long-term survival depend upon resting LV function residual ischemic myocardium and susceptibility to ventricular arrhythmias
THE END
- CHEST PAIN SCENARIO 3 GROUP 10
- SCENARIO
- KEYWORD
- QUESTION
- DIFFERENTIAL DIAGNOSIS
- INTRODUCTION
- BASIC SCIENCE
- EKG
- Normal heart
- Myocardial Infarction Two to three days after an MI the myocyt
- Slide 11
- PATHOPHYSIOLOGY OF ST-ELEVATION MYOCARDIAL INFARCTION (STEMI)
- myocardial infarction
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- HYPOTENSION May trigger a dramatic sympathetic nervous system
- Slide 19
- Slide 21
- Left Ventricular Function Systolic Function
- Ventricular Remodeling
- references
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- PATHOLOGIC OF Q-WAVE
- PATHOMECANISM CHEST PAIN
- Slide 31
- SMOKING kills
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- ThE eND
-

Procoagulant factors (such as tissue factor) reside within the plaque itself
and in the absence of counterbalancing antithrombotic factor (eg heparin tissue-factor-
inhibitor) and fibrinolytic activities (tissues plasminogen activator [t-PA]
and single-chain urokinase-type plasminogen activator) within the endothelial cells of the coronary
artery can cause thrombosis Recent work suggests that inflammation may play a pivotal role in
the genesis of plaque rupture Total thrombotic occlusion occurs most commonly in proximal coronary
arteries its presence has been documented during the first 4 hours
after infarction in more than 85 of the patients with ST segment elevation
(Crawford MH (2009))
This potent procoagulant stimulus results in thrombus development in
this region In general acute MI occurs when this thrombosis
propagates and occludes flow within the artery resulting in ischemia of
cardiomyocytes distal to the obstruction
The ECG leads in which pathologic Q waves appear reflect the anatomical site of an infarction
TABLE 1 Localization of Myocardial Infarction Anatomical Site Leads with Abnormal ECG
Complexes Coronary Artery Most Often
Responsible Inferior IIIIIaVF RCA
Anteroseptal V1-V2 LAD Anteroapical V3-V4 LAD(distal) Anterolateral V5-V6 I aVL CFX
Posterior V1-V2 (tall R wave not Q wave) RCA
The electrocardiographic differences between these types of MI are summarized as follow
Type of Infarction Pathologic Q waves Acute ST segment Deviation
Q-wave MI Yes ST elevation Non-Q-wave MI No ST depression (and or T
wave inversion)
Angina pectoris- Neck- Shoulder- Arms
ischemic myocardial cells release mediator such as adenosine and
lactate from into local nerve endings
discomfort often refer to other region of the C7 through
dermatome
provocative substances continue to accumulate and active afferent
nerve for longer period
ischemic in acute MI persist and proceed to necrosis
HYPOTENSION
May trigger a dramatic sympathetic nervous system response
Systemic sign of subsequent catecholamine release include diaphoresis (sweating) tachycardia and cool
and clammy skin
cause of vasoconstriction
Systolic Dysfunction
Decrease lungs compliance and stimulates juxtacappilary
receptors
Left ventricle contractility can be
reduced
J receptors effects a reflex that results in rapid shallow
breathing and evokes the subjective feeling of dyspnea
Increase in LV pressure compounded by the ischemia
induced stiffness of the chamber (diastolic dysfunction) is conveyed to the left atrium and pulmonary
veins
Decreasing the stroke volume and causing the diastolic
volume and pressure within the LV to rise
Ischemia affects large amount of myocardium
SERUM MARKER OF INFARCTION
Detection of cardiac-specific troponins and creatine kinase MB isoenzyme
Intracellular macromolecules leak into the cardiac interstitium and ultimately into the bloodstream
Necrosis of myocardial tissue Cause by disruption of the sarcolemma
MYOCARDIAL INFARTION
TYPICAL SYMPTOM- Crushing chest pain
more severe and wider than usual angina
SERUM BIOMARKSCreatine kinaseTroponin
ECG initial finding- St elevation- Q Wave
STEMI
Left Ventricular Function Systolic Function
Upon interruption of antegrade flow in an epicardial coronary artery the zone of myocardium supplied by that vessel immediately loses its ability to shorten and perform contractile work Four abnormal contraction patterns develop in sequence (1) dyssynchrony that is dissociation in the time course of contraction of adjacent segments(2) hypokinesis reduction in the extent of shortening (3) akinesis cessation of shortening and (4) dyskinesis paradoxical expansion and systolic bulging
Hyperkinesis of the remaining normal myocardium initially accompanies dysfunction of the infarcting segment The early hyperkinesis of the noninfarcted zones likely results from acute compensations including increased activity of the sympathetic nervous system and the Frank-Starling mechanism A portion of this compensatory hyperkinesis is ineffective work because contraction of the noninfarcted segments of myocardium hellip
Ventricular Remodelingbull As a consequence of STEMI the changes in left ventricular size shape and
thickness involving both the infarcted and the noninfarcted segments of the ventricle described earlier occur and are collectively referred to as ventricular remodeling which can in turn influence ventricular function and prognosis
bull A combination of changes in left ventricular dilation and hypertrophy of residual noninfarcted myocardium causes remodeling
bull After the size of infarction the two most important factors driving the process of left ventricular dilation are ventricular loading conditions and infarct artery patency
bull Elevated ventricular pressure contributes to increased wall stress and the risk of infarct expansion and a patent infarct artery accelerates myocardial scar formation and increases tissue turgor in the infarct zone reducing the risk of infarct expansion and ventricular dilation
Antman EM Morrow DA McCabe CH et al Enoxaparin versus unfractionated heparin with fibrinolysis for ST-elevation myocardial infarction N Engl J Med 2006 3541477
referencesSLIDE 2 Alpert JS Thygesen K Antman E and Bassand JP Myocardial infarction redefined--a consensus document of The Joint European Society of CardiologyAmerican College of Cardiology Committee for the redefinition of myocardial infarction J Am Coll Cardiol 2000 Sep 36(3) 959-69 pmid10987628bull Book of Pathophysiology of Heart Disease fourth edition editor Leonard SLilly page 179-
184bull ILMU PENYAKIT DALAM Jilid II Edisi V Editor Aru WSudoyo Bambang Setiyohadi
Idrus Alwi page1741-1744
ST elevation MI
ST segment elevation type of acute myocardial infarction require at least 1 mm (01 mV) of ST segment elevation in the limb leads and at least 2 mm elevation in the precordial leads
The clinician must therefore be well versed in recognizing the so-called ECG mimics of acute myocardial infarction which include
These elevations must be present in anatomically contiguous leads (I aVL V5 V6 correspond to the lateral wall V1-V2 correspond to the septal wall V3-V4 correspond to the anterior wall II III aVF correspond to the inferior wall)
left ventricular hypertrophy
left bundle branch block
hyperkalemia
early repolarization
ventricular aneurysm
12-lead electrocardiogram showing ST-segment elevation (orange) in I aVL and V1-V5 with reciprocal changes (blue) in the inferior leads indicative of an anterior wall myocardial infarction
An acute STEMI involving the inferior and right ventricular wall Reciprocal changes are seen in the anterior leads
PATHOLOGIC OF Q-WAVEPathologic Q waves
Any Q-wave in leads V2ndashV3 ge 002 s or QS complex in leads V2 and V3
Q-wave ge 003 s and gt 01 mV deep or QS complex in leads I II aVL aVF or V4ndashV6 in
any two leads of a contiguous lead grouping (I aVLV6 V4ndashV6 II III and aVF)
result of absence of electrical activity
previous myocardial infarction
The evolution of an infarct on the ECG ST elevation Q wave formation T wave inversion
normalisation with a persistent Q wave
PATHOMECANISM CHEST PAINhttpemedicinemedscapecomarticle150215-overview2
ProfDrPeter Kabo Bagaimana Menggunakan Obat-obat kardiovasculer secara Rasional
AtherosclerosisProduce endothelial derived constricting
factor (EDCF)
Increase tonus artery
coronary
Ischemic myocard
Aerobic glycolysis turn
to anerobic glycolysis
Production of adenosin
Diffuse to extracellular
space
Stimulate A1 receptor in cardiac
afferent nerve ending
Bind with somatic cervico
thoracalis nerve at
ascending pathway in
medulla spinalis
Chest pain
SMOKING KILLS
These effects could potentially trigger
symptoms of ischemia in such smokers
One might also expect that the hemodynamic effects of nicotine would contribute to endothelial damage and accelerate the progression of atherosclerosis
Lipolyis - increased levels of circulating free fatty acids
and glycerol in the blood and the resulting increase in fat
metabolism drives a demand for more oxygen leading to
increased coronary blood flow and myocardial oxygen
uptake
addition to its cardiovascular effects such as elevated heart
rate blood pressure and cardiac output
nicotine has metabolic effects in particular increased lipolysis
Nicotine is a sympathomimetic chemical that promotes the release of catecholamines and other
neurotransmitters
SIGNS AND SYMPTOMS
bullChest pain (pressuretightnessheaviness and might radiate to neck arm)
bullIngestion heartburnbullNausea VomitingbullSweatingbullWeaknessbullDizziness
httpwwwcardiosmartorgManageConditionDefaultaspxid=904 httpwwwncbinlmnihgovpmcarticlesPMC2233977
ADDITIONAL EXAMINATION1 Physical examination
Gen appearance Distress Levine signbullHeart rate pulse respirrate variablebullBlood pressure variablebullLow-grade feverbullExamination of jugular venous pulsationsbullPulmonary CracklesbullS4 gallop due to reduced LV compliancebullS3 gallop if LV dysfunction presentbullMurmurs Pericardial friction rubs
2 ECG
The key to rapid diagnosis and risk stratification for the patient with chest painbullTo be obtained within 10 minutes of arrival to Emergency DepartmentbullFor STEMI 1048774ST-segment elevation gt1mm in 2+ contiguous leads OR new left bundle branch block (LBBB)bullLocation of InfarctLeadsInferior MI II III aVFAnterior MI V2-V4Lateral MI I aVL V5-V6
3 Lab studies
Cardiac Biomarkers CK CK-MB cTnbullSerum ChemistriesbullRenal FunctionbullCoagulation StudiesbullComplete Blood Count
TREATMENTAspirin
bullRapidly blocks formation of thromboxaneA2 in platelets by cyclooxygenase inhibitionbull162-325mg chewed (promotes buccalabsorption)bullISIS-2ndash23 reduction in mortality largely additive to the reduction in mortality from streptokinaseOther Adjuvant TherapiesAnalgesicsbullNitratesbullBeta-blockersbullAce InhibitorsbullOxygenbullHeparinbullIV Glycoprotein IIbIIIaInhibitorsbullClopidogrelbullStatins
Thrombolytic TherapybullCommon AgentsbullTNK-tPA30-50mg IV bolusbullReteplase10U x 2 (each over 2 minutes) IVbullAlteplaseup to 100mg in 90mins (based on weight)
bullContraindicationsndashAbsolute Prior intracranial hemorrhage known cerebral vascular lesion malignant intracranial neoplasm ischemic stroke within 3 months suspected aortic dissection active bleeding recent closed head injury or facial trauma within 3monthsndashRelative History of chronic severe HTN severeuncontrolled HTN at presentation (gt180110) history of ischemic stroke gt3 months traumaticprolonged CPR recent internal bleeding (2-4 weeks) pregnancy active peptic ulcer current anticoagulation
Primary PCI
bullPCI = Percutaneous Coronary Intervention
bullPTCA = Percutaneous Transluminal Coronary Angioplasty
bullPOBA = Plain Old Balloon Angioplasty
PROGNOSIS
bullDischarge usually 5 days after admissionbullSmoking CessationbullShort and Long-term survival depend upon resting LV function residual ischemic myocardium and susceptibility to ventricular arrhythmias
THE END
- CHEST PAIN SCENARIO 3 GROUP 10
- SCENARIO
- KEYWORD
- QUESTION
- DIFFERENTIAL DIAGNOSIS
- INTRODUCTION
- BASIC SCIENCE
- EKG
- Normal heart
- Myocardial Infarction Two to three days after an MI the myocyt
- Slide 11
- PATHOPHYSIOLOGY OF ST-ELEVATION MYOCARDIAL INFARCTION (STEMI)
- myocardial infarction
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- HYPOTENSION May trigger a dramatic sympathetic nervous system
- Slide 19
- Slide 21
- Left Ventricular Function Systolic Function
- Ventricular Remodeling
- references
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- PATHOLOGIC OF Q-WAVE
- PATHOMECANISM CHEST PAIN
- Slide 31
- SMOKING kills
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- ThE eND
-

The ECG leads in which pathologic Q waves appear reflect the anatomical site of an infarction
TABLE 1 Localization of Myocardial Infarction Anatomical Site Leads with Abnormal ECG
Complexes Coronary Artery Most Often
Responsible Inferior IIIIIaVF RCA
Anteroseptal V1-V2 LAD Anteroapical V3-V4 LAD(distal) Anterolateral V5-V6 I aVL CFX
Posterior V1-V2 (tall R wave not Q wave) RCA
The electrocardiographic differences between these types of MI are summarized as follow
Type of Infarction Pathologic Q waves Acute ST segment Deviation
Q-wave MI Yes ST elevation Non-Q-wave MI No ST depression (and or T
wave inversion)
Angina pectoris- Neck- Shoulder- Arms
ischemic myocardial cells release mediator such as adenosine and
lactate from into local nerve endings
discomfort often refer to other region of the C7 through
dermatome
provocative substances continue to accumulate and active afferent
nerve for longer period
ischemic in acute MI persist and proceed to necrosis
HYPOTENSION
May trigger a dramatic sympathetic nervous system response
Systemic sign of subsequent catecholamine release include diaphoresis (sweating) tachycardia and cool
and clammy skin
cause of vasoconstriction
Systolic Dysfunction
Decrease lungs compliance and stimulates juxtacappilary
receptors
Left ventricle contractility can be
reduced
J receptors effects a reflex that results in rapid shallow
breathing and evokes the subjective feeling of dyspnea
Increase in LV pressure compounded by the ischemia
induced stiffness of the chamber (diastolic dysfunction) is conveyed to the left atrium and pulmonary
veins
Decreasing the stroke volume and causing the diastolic
volume and pressure within the LV to rise
Ischemia affects large amount of myocardium
SERUM MARKER OF INFARCTION
Detection of cardiac-specific troponins and creatine kinase MB isoenzyme
Intracellular macromolecules leak into the cardiac interstitium and ultimately into the bloodstream
Necrosis of myocardial tissue Cause by disruption of the sarcolemma
MYOCARDIAL INFARTION
TYPICAL SYMPTOM- Crushing chest pain
more severe and wider than usual angina
SERUM BIOMARKSCreatine kinaseTroponin
ECG initial finding- St elevation- Q Wave
STEMI
Left Ventricular Function Systolic Function
Upon interruption of antegrade flow in an epicardial coronary artery the zone of myocardium supplied by that vessel immediately loses its ability to shorten and perform contractile work Four abnormal contraction patterns develop in sequence (1) dyssynchrony that is dissociation in the time course of contraction of adjacent segments(2) hypokinesis reduction in the extent of shortening (3) akinesis cessation of shortening and (4) dyskinesis paradoxical expansion and systolic bulging
Hyperkinesis of the remaining normal myocardium initially accompanies dysfunction of the infarcting segment The early hyperkinesis of the noninfarcted zones likely results from acute compensations including increased activity of the sympathetic nervous system and the Frank-Starling mechanism A portion of this compensatory hyperkinesis is ineffective work because contraction of the noninfarcted segments of myocardium hellip
Ventricular Remodelingbull As a consequence of STEMI the changes in left ventricular size shape and
thickness involving both the infarcted and the noninfarcted segments of the ventricle described earlier occur and are collectively referred to as ventricular remodeling which can in turn influence ventricular function and prognosis
bull A combination of changes in left ventricular dilation and hypertrophy of residual noninfarcted myocardium causes remodeling
bull After the size of infarction the two most important factors driving the process of left ventricular dilation are ventricular loading conditions and infarct artery patency
bull Elevated ventricular pressure contributes to increased wall stress and the risk of infarct expansion and a patent infarct artery accelerates myocardial scar formation and increases tissue turgor in the infarct zone reducing the risk of infarct expansion and ventricular dilation
Antman EM Morrow DA McCabe CH et al Enoxaparin versus unfractionated heparin with fibrinolysis for ST-elevation myocardial infarction N Engl J Med 2006 3541477
referencesSLIDE 2 Alpert JS Thygesen K Antman E and Bassand JP Myocardial infarction redefined--a consensus document of The Joint European Society of CardiologyAmerican College of Cardiology Committee for the redefinition of myocardial infarction J Am Coll Cardiol 2000 Sep 36(3) 959-69 pmid10987628bull Book of Pathophysiology of Heart Disease fourth edition editor Leonard SLilly page 179-
184bull ILMU PENYAKIT DALAM Jilid II Edisi V Editor Aru WSudoyo Bambang Setiyohadi
Idrus Alwi page1741-1744
ST elevation MI
ST segment elevation type of acute myocardial infarction require at least 1 mm (01 mV) of ST segment elevation in the limb leads and at least 2 mm elevation in the precordial leads
The clinician must therefore be well versed in recognizing the so-called ECG mimics of acute myocardial infarction which include
These elevations must be present in anatomically contiguous leads (I aVL V5 V6 correspond to the lateral wall V1-V2 correspond to the septal wall V3-V4 correspond to the anterior wall II III aVF correspond to the inferior wall)
left ventricular hypertrophy
left bundle branch block
hyperkalemia
early repolarization
ventricular aneurysm
12-lead electrocardiogram showing ST-segment elevation (orange) in I aVL and V1-V5 with reciprocal changes (blue) in the inferior leads indicative of an anterior wall myocardial infarction
An acute STEMI involving the inferior and right ventricular wall Reciprocal changes are seen in the anterior leads
PATHOLOGIC OF Q-WAVEPathologic Q waves
Any Q-wave in leads V2ndashV3 ge 002 s or QS complex in leads V2 and V3
Q-wave ge 003 s and gt 01 mV deep or QS complex in leads I II aVL aVF or V4ndashV6 in
any two leads of a contiguous lead grouping (I aVLV6 V4ndashV6 II III and aVF)
result of absence of electrical activity
previous myocardial infarction
The evolution of an infarct on the ECG ST elevation Q wave formation T wave inversion
normalisation with a persistent Q wave
PATHOMECANISM CHEST PAINhttpemedicinemedscapecomarticle150215-overview2
ProfDrPeter Kabo Bagaimana Menggunakan Obat-obat kardiovasculer secara Rasional
AtherosclerosisProduce endothelial derived constricting
factor (EDCF)
Increase tonus artery
coronary
Ischemic myocard
Aerobic glycolysis turn
to anerobic glycolysis
Production of adenosin
Diffuse to extracellular
space
Stimulate A1 receptor in cardiac
afferent nerve ending
Bind with somatic cervico
thoracalis nerve at
ascending pathway in
medulla spinalis
Chest pain
SMOKING KILLS
These effects could potentially trigger
symptoms of ischemia in such smokers
One might also expect that the hemodynamic effects of nicotine would contribute to endothelial damage and accelerate the progression of atherosclerosis
Lipolyis - increased levels of circulating free fatty acids
and glycerol in the blood and the resulting increase in fat
metabolism drives a demand for more oxygen leading to
increased coronary blood flow and myocardial oxygen
uptake
addition to its cardiovascular effects such as elevated heart
rate blood pressure and cardiac output
nicotine has metabolic effects in particular increased lipolysis
Nicotine is a sympathomimetic chemical that promotes the release of catecholamines and other
neurotransmitters
SIGNS AND SYMPTOMS
bullChest pain (pressuretightnessheaviness and might radiate to neck arm)
bullIngestion heartburnbullNausea VomitingbullSweatingbullWeaknessbullDizziness
httpwwwcardiosmartorgManageConditionDefaultaspxid=904 httpwwwncbinlmnihgovpmcarticlesPMC2233977
ADDITIONAL EXAMINATION1 Physical examination
Gen appearance Distress Levine signbullHeart rate pulse respirrate variablebullBlood pressure variablebullLow-grade feverbullExamination of jugular venous pulsationsbullPulmonary CracklesbullS4 gallop due to reduced LV compliancebullS3 gallop if LV dysfunction presentbullMurmurs Pericardial friction rubs
2 ECG
The key to rapid diagnosis and risk stratification for the patient with chest painbullTo be obtained within 10 minutes of arrival to Emergency DepartmentbullFor STEMI 1048774ST-segment elevation gt1mm in 2+ contiguous leads OR new left bundle branch block (LBBB)bullLocation of InfarctLeadsInferior MI II III aVFAnterior MI V2-V4Lateral MI I aVL V5-V6
3 Lab studies
Cardiac Biomarkers CK CK-MB cTnbullSerum ChemistriesbullRenal FunctionbullCoagulation StudiesbullComplete Blood Count
TREATMENTAspirin
bullRapidly blocks formation of thromboxaneA2 in platelets by cyclooxygenase inhibitionbull162-325mg chewed (promotes buccalabsorption)bullISIS-2ndash23 reduction in mortality largely additive to the reduction in mortality from streptokinaseOther Adjuvant TherapiesAnalgesicsbullNitratesbullBeta-blockersbullAce InhibitorsbullOxygenbullHeparinbullIV Glycoprotein IIbIIIaInhibitorsbullClopidogrelbullStatins
Thrombolytic TherapybullCommon AgentsbullTNK-tPA30-50mg IV bolusbullReteplase10U x 2 (each over 2 minutes) IVbullAlteplaseup to 100mg in 90mins (based on weight)
bullContraindicationsndashAbsolute Prior intracranial hemorrhage known cerebral vascular lesion malignant intracranial neoplasm ischemic stroke within 3 months suspected aortic dissection active bleeding recent closed head injury or facial trauma within 3monthsndashRelative History of chronic severe HTN severeuncontrolled HTN at presentation (gt180110) history of ischemic stroke gt3 months traumaticprolonged CPR recent internal bleeding (2-4 weeks) pregnancy active peptic ulcer current anticoagulation
Primary PCI
bullPCI = Percutaneous Coronary Intervention
bullPTCA = Percutaneous Transluminal Coronary Angioplasty
bullPOBA = Plain Old Balloon Angioplasty
PROGNOSIS
bullDischarge usually 5 days after admissionbullSmoking CessationbullShort and Long-term survival depend upon resting LV function residual ischemic myocardium and susceptibility to ventricular arrhythmias
THE END
- CHEST PAIN SCENARIO 3 GROUP 10
- SCENARIO
- KEYWORD
- QUESTION
- DIFFERENTIAL DIAGNOSIS
- INTRODUCTION
- BASIC SCIENCE
- EKG
- Normal heart
- Myocardial Infarction Two to three days after an MI the myocyt
- Slide 11
- PATHOPHYSIOLOGY OF ST-ELEVATION MYOCARDIAL INFARCTION (STEMI)
- myocardial infarction
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- HYPOTENSION May trigger a dramatic sympathetic nervous system
- Slide 19
- Slide 21
- Left Ventricular Function Systolic Function
- Ventricular Remodeling
- references
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- PATHOLOGIC OF Q-WAVE
- PATHOMECANISM CHEST PAIN
- Slide 31
- SMOKING kills
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- ThE eND
-

Angina pectoris- Neck- Shoulder- Arms
ischemic myocardial cells release mediator such as adenosine and
lactate from into local nerve endings
discomfort often refer to other region of the C7 through
dermatome
provocative substances continue to accumulate and active afferent
nerve for longer period
ischemic in acute MI persist and proceed to necrosis
HYPOTENSION
May trigger a dramatic sympathetic nervous system response
Systemic sign of subsequent catecholamine release include diaphoresis (sweating) tachycardia and cool
and clammy skin
cause of vasoconstriction
Systolic Dysfunction
Decrease lungs compliance and stimulates juxtacappilary
receptors
Left ventricle contractility can be
reduced
J receptors effects a reflex that results in rapid shallow
breathing and evokes the subjective feeling of dyspnea
Increase in LV pressure compounded by the ischemia
induced stiffness of the chamber (diastolic dysfunction) is conveyed to the left atrium and pulmonary
veins
Decreasing the stroke volume and causing the diastolic
volume and pressure within the LV to rise
Ischemia affects large amount of myocardium
SERUM MARKER OF INFARCTION
Detection of cardiac-specific troponins and creatine kinase MB isoenzyme
Intracellular macromolecules leak into the cardiac interstitium and ultimately into the bloodstream
Necrosis of myocardial tissue Cause by disruption of the sarcolemma
MYOCARDIAL INFARTION
TYPICAL SYMPTOM- Crushing chest pain
more severe and wider than usual angina
SERUM BIOMARKSCreatine kinaseTroponin
ECG initial finding- St elevation- Q Wave
STEMI
Left Ventricular Function Systolic Function
Upon interruption of antegrade flow in an epicardial coronary artery the zone of myocardium supplied by that vessel immediately loses its ability to shorten and perform contractile work Four abnormal contraction patterns develop in sequence (1) dyssynchrony that is dissociation in the time course of contraction of adjacent segments(2) hypokinesis reduction in the extent of shortening (3) akinesis cessation of shortening and (4) dyskinesis paradoxical expansion and systolic bulging
Hyperkinesis of the remaining normal myocardium initially accompanies dysfunction of the infarcting segment The early hyperkinesis of the noninfarcted zones likely results from acute compensations including increased activity of the sympathetic nervous system and the Frank-Starling mechanism A portion of this compensatory hyperkinesis is ineffective work because contraction of the noninfarcted segments of myocardium hellip
Ventricular Remodelingbull As a consequence of STEMI the changes in left ventricular size shape and
thickness involving both the infarcted and the noninfarcted segments of the ventricle described earlier occur and are collectively referred to as ventricular remodeling which can in turn influence ventricular function and prognosis
bull A combination of changes in left ventricular dilation and hypertrophy of residual noninfarcted myocardium causes remodeling
bull After the size of infarction the two most important factors driving the process of left ventricular dilation are ventricular loading conditions and infarct artery patency
bull Elevated ventricular pressure contributes to increased wall stress and the risk of infarct expansion and a patent infarct artery accelerates myocardial scar formation and increases tissue turgor in the infarct zone reducing the risk of infarct expansion and ventricular dilation
Antman EM Morrow DA McCabe CH et al Enoxaparin versus unfractionated heparin with fibrinolysis for ST-elevation myocardial infarction N Engl J Med 2006 3541477
referencesSLIDE 2 Alpert JS Thygesen K Antman E and Bassand JP Myocardial infarction redefined--a consensus document of The Joint European Society of CardiologyAmerican College of Cardiology Committee for the redefinition of myocardial infarction J Am Coll Cardiol 2000 Sep 36(3) 959-69 pmid10987628bull Book of Pathophysiology of Heart Disease fourth edition editor Leonard SLilly page 179-
184bull ILMU PENYAKIT DALAM Jilid II Edisi V Editor Aru WSudoyo Bambang Setiyohadi
Idrus Alwi page1741-1744
ST elevation MI
ST segment elevation type of acute myocardial infarction require at least 1 mm (01 mV) of ST segment elevation in the limb leads and at least 2 mm elevation in the precordial leads
The clinician must therefore be well versed in recognizing the so-called ECG mimics of acute myocardial infarction which include
These elevations must be present in anatomically contiguous leads (I aVL V5 V6 correspond to the lateral wall V1-V2 correspond to the septal wall V3-V4 correspond to the anterior wall II III aVF correspond to the inferior wall)
left ventricular hypertrophy
left bundle branch block
hyperkalemia
early repolarization
ventricular aneurysm
12-lead electrocardiogram showing ST-segment elevation (orange) in I aVL and V1-V5 with reciprocal changes (blue) in the inferior leads indicative of an anterior wall myocardial infarction
An acute STEMI involving the inferior and right ventricular wall Reciprocal changes are seen in the anterior leads
PATHOLOGIC OF Q-WAVEPathologic Q waves
Any Q-wave in leads V2ndashV3 ge 002 s or QS complex in leads V2 and V3
Q-wave ge 003 s and gt 01 mV deep or QS complex in leads I II aVL aVF or V4ndashV6 in
any two leads of a contiguous lead grouping (I aVLV6 V4ndashV6 II III and aVF)
result of absence of electrical activity
previous myocardial infarction
The evolution of an infarct on the ECG ST elevation Q wave formation T wave inversion
normalisation with a persistent Q wave
PATHOMECANISM CHEST PAINhttpemedicinemedscapecomarticle150215-overview2
ProfDrPeter Kabo Bagaimana Menggunakan Obat-obat kardiovasculer secara Rasional
AtherosclerosisProduce endothelial derived constricting
factor (EDCF)
Increase tonus artery
coronary
Ischemic myocard
Aerobic glycolysis turn
to anerobic glycolysis
Production of adenosin
Diffuse to extracellular
space
Stimulate A1 receptor in cardiac
afferent nerve ending
Bind with somatic cervico
thoracalis nerve at
ascending pathway in
medulla spinalis
Chest pain
SMOKING KILLS
These effects could potentially trigger
symptoms of ischemia in such smokers
One might also expect that the hemodynamic effects of nicotine would contribute to endothelial damage and accelerate the progression of atherosclerosis
Lipolyis - increased levels of circulating free fatty acids
and glycerol in the blood and the resulting increase in fat
metabolism drives a demand for more oxygen leading to
increased coronary blood flow and myocardial oxygen
uptake
addition to its cardiovascular effects such as elevated heart
rate blood pressure and cardiac output
nicotine has metabolic effects in particular increased lipolysis
Nicotine is a sympathomimetic chemical that promotes the release of catecholamines and other
neurotransmitters
SIGNS AND SYMPTOMS
bullChest pain (pressuretightnessheaviness and might radiate to neck arm)
bullIngestion heartburnbullNausea VomitingbullSweatingbullWeaknessbullDizziness
httpwwwcardiosmartorgManageConditionDefaultaspxid=904 httpwwwncbinlmnihgovpmcarticlesPMC2233977
ADDITIONAL EXAMINATION1 Physical examination
Gen appearance Distress Levine signbullHeart rate pulse respirrate variablebullBlood pressure variablebullLow-grade feverbullExamination of jugular venous pulsationsbullPulmonary CracklesbullS4 gallop due to reduced LV compliancebullS3 gallop if LV dysfunction presentbullMurmurs Pericardial friction rubs
2 ECG
The key to rapid diagnosis and risk stratification for the patient with chest painbullTo be obtained within 10 minutes of arrival to Emergency DepartmentbullFor STEMI 1048774ST-segment elevation gt1mm in 2+ contiguous leads OR new left bundle branch block (LBBB)bullLocation of InfarctLeadsInferior MI II III aVFAnterior MI V2-V4Lateral MI I aVL V5-V6
3 Lab studies
Cardiac Biomarkers CK CK-MB cTnbullSerum ChemistriesbullRenal FunctionbullCoagulation StudiesbullComplete Blood Count
TREATMENTAspirin
bullRapidly blocks formation of thromboxaneA2 in platelets by cyclooxygenase inhibitionbull162-325mg chewed (promotes buccalabsorption)bullISIS-2ndash23 reduction in mortality largely additive to the reduction in mortality from streptokinaseOther Adjuvant TherapiesAnalgesicsbullNitratesbullBeta-blockersbullAce InhibitorsbullOxygenbullHeparinbullIV Glycoprotein IIbIIIaInhibitorsbullClopidogrelbullStatins
Thrombolytic TherapybullCommon AgentsbullTNK-tPA30-50mg IV bolusbullReteplase10U x 2 (each over 2 minutes) IVbullAlteplaseup to 100mg in 90mins (based on weight)
bullContraindicationsndashAbsolute Prior intracranial hemorrhage known cerebral vascular lesion malignant intracranial neoplasm ischemic stroke within 3 months suspected aortic dissection active bleeding recent closed head injury or facial trauma within 3monthsndashRelative History of chronic severe HTN severeuncontrolled HTN at presentation (gt180110) history of ischemic stroke gt3 months traumaticprolonged CPR recent internal bleeding (2-4 weeks) pregnancy active peptic ulcer current anticoagulation
Primary PCI
bullPCI = Percutaneous Coronary Intervention
bullPTCA = Percutaneous Transluminal Coronary Angioplasty
bullPOBA = Plain Old Balloon Angioplasty
PROGNOSIS
bullDischarge usually 5 days after admissionbullSmoking CessationbullShort and Long-term survival depend upon resting LV function residual ischemic myocardium and susceptibility to ventricular arrhythmias
THE END
- CHEST PAIN SCENARIO 3 GROUP 10
- SCENARIO
- KEYWORD
- QUESTION
- DIFFERENTIAL DIAGNOSIS
- INTRODUCTION
- BASIC SCIENCE
- EKG
- Normal heart
- Myocardial Infarction Two to three days after an MI the myocyt
- Slide 11
- PATHOPHYSIOLOGY OF ST-ELEVATION MYOCARDIAL INFARCTION (STEMI)
- myocardial infarction
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- HYPOTENSION May trigger a dramatic sympathetic nervous system
- Slide 19
- Slide 21
- Left Ventricular Function Systolic Function
- Ventricular Remodeling
- references
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- PATHOLOGIC OF Q-WAVE
- PATHOMECANISM CHEST PAIN
- Slide 31
- SMOKING kills
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- ThE eND
-

HYPOTENSION
May trigger a dramatic sympathetic nervous system response
Systemic sign of subsequent catecholamine release include diaphoresis (sweating) tachycardia and cool
and clammy skin
cause of vasoconstriction
Systolic Dysfunction
Decrease lungs compliance and stimulates juxtacappilary
receptors
Left ventricle contractility can be
reduced
J receptors effects a reflex that results in rapid shallow
breathing and evokes the subjective feeling of dyspnea
Increase in LV pressure compounded by the ischemia
induced stiffness of the chamber (diastolic dysfunction) is conveyed to the left atrium and pulmonary
veins
Decreasing the stroke volume and causing the diastolic
volume and pressure within the LV to rise
Ischemia affects large amount of myocardium
SERUM MARKER OF INFARCTION
Detection of cardiac-specific troponins and creatine kinase MB isoenzyme
Intracellular macromolecules leak into the cardiac interstitium and ultimately into the bloodstream
Necrosis of myocardial tissue Cause by disruption of the sarcolemma
MYOCARDIAL INFARTION
TYPICAL SYMPTOM- Crushing chest pain
more severe and wider than usual angina
SERUM BIOMARKSCreatine kinaseTroponin
ECG initial finding- St elevation- Q Wave
STEMI
Left Ventricular Function Systolic Function
Upon interruption of antegrade flow in an epicardial coronary artery the zone of myocardium supplied by that vessel immediately loses its ability to shorten and perform contractile work Four abnormal contraction patterns develop in sequence (1) dyssynchrony that is dissociation in the time course of contraction of adjacent segments(2) hypokinesis reduction in the extent of shortening (3) akinesis cessation of shortening and (4) dyskinesis paradoxical expansion and systolic bulging
Hyperkinesis of the remaining normal myocardium initially accompanies dysfunction of the infarcting segment The early hyperkinesis of the noninfarcted zones likely results from acute compensations including increased activity of the sympathetic nervous system and the Frank-Starling mechanism A portion of this compensatory hyperkinesis is ineffective work because contraction of the noninfarcted segments of myocardium hellip
Ventricular Remodelingbull As a consequence of STEMI the changes in left ventricular size shape and
thickness involving both the infarcted and the noninfarcted segments of the ventricle described earlier occur and are collectively referred to as ventricular remodeling which can in turn influence ventricular function and prognosis
bull A combination of changes in left ventricular dilation and hypertrophy of residual noninfarcted myocardium causes remodeling
bull After the size of infarction the two most important factors driving the process of left ventricular dilation are ventricular loading conditions and infarct artery patency
bull Elevated ventricular pressure contributes to increased wall stress and the risk of infarct expansion and a patent infarct artery accelerates myocardial scar formation and increases tissue turgor in the infarct zone reducing the risk of infarct expansion and ventricular dilation
Antman EM Morrow DA McCabe CH et al Enoxaparin versus unfractionated heparin with fibrinolysis for ST-elevation myocardial infarction N Engl J Med 2006 3541477
referencesSLIDE 2 Alpert JS Thygesen K Antman E and Bassand JP Myocardial infarction redefined--a consensus document of The Joint European Society of CardiologyAmerican College of Cardiology Committee for the redefinition of myocardial infarction J Am Coll Cardiol 2000 Sep 36(3) 959-69 pmid10987628bull Book of Pathophysiology of Heart Disease fourth edition editor Leonard SLilly page 179-
184bull ILMU PENYAKIT DALAM Jilid II Edisi V Editor Aru WSudoyo Bambang Setiyohadi
Idrus Alwi page1741-1744
ST elevation MI
ST segment elevation type of acute myocardial infarction require at least 1 mm (01 mV) of ST segment elevation in the limb leads and at least 2 mm elevation in the precordial leads
The clinician must therefore be well versed in recognizing the so-called ECG mimics of acute myocardial infarction which include
These elevations must be present in anatomically contiguous leads (I aVL V5 V6 correspond to the lateral wall V1-V2 correspond to the septal wall V3-V4 correspond to the anterior wall II III aVF correspond to the inferior wall)
left ventricular hypertrophy
left bundle branch block
hyperkalemia
early repolarization
ventricular aneurysm
12-lead electrocardiogram showing ST-segment elevation (orange) in I aVL and V1-V5 with reciprocal changes (blue) in the inferior leads indicative of an anterior wall myocardial infarction
An acute STEMI involving the inferior and right ventricular wall Reciprocal changes are seen in the anterior leads
PATHOLOGIC OF Q-WAVEPathologic Q waves
Any Q-wave in leads V2ndashV3 ge 002 s or QS complex in leads V2 and V3
Q-wave ge 003 s and gt 01 mV deep or QS complex in leads I II aVL aVF or V4ndashV6 in
any two leads of a contiguous lead grouping (I aVLV6 V4ndashV6 II III and aVF)
result of absence of electrical activity
previous myocardial infarction
The evolution of an infarct on the ECG ST elevation Q wave formation T wave inversion
normalisation with a persistent Q wave
PATHOMECANISM CHEST PAINhttpemedicinemedscapecomarticle150215-overview2
ProfDrPeter Kabo Bagaimana Menggunakan Obat-obat kardiovasculer secara Rasional
AtherosclerosisProduce endothelial derived constricting
factor (EDCF)
Increase tonus artery
coronary
Ischemic myocard
Aerobic glycolysis turn
to anerobic glycolysis
Production of adenosin
Diffuse to extracellular
space
Stimulate A1 receptor in cardiac
afferent nerve ending
Bind with somatic cervico
thoracalis nerve at
ascending pathway in
medulla spinalis
Chest pain
SMOKING KILLS
These effects could potentially trigger
symptoms of ischemia in such smokers
One might also expect that the hemodynamic effects of nicotine would contribute to endothelial damage and accelerate the progression of atherosclerosis
Lipolyis - increased levels of circulating free fatty acids
and glycerol in the blood and the resulting increase in fat
metabolism drives a demand for more oxygen leading to
increased coronary blood flow and myocardial oxygen
uptake
addition to its cardiovascular effects such as elevated heart
rate blood pressure and cardiac output
nicotine has metabolic effects in particular increased lipolysis
Nicotine is a sympathomimetic chemical that promotes the release of catecholamines and other
neurotransmitters
SIGNS AND SYMPTOMS
bullChest pain (pressuretightnessheaviness and might radiate to neck arm)
bullIngestion heartburnbullNausea VomitingbullSweatingbullWeaknessbullDizziness
httpwwwcardiosmartorgManageConditionDefaultaspxid=904 httpwwwncbinlmnihgovpmcarticlesPMC2233977
ADDITIONAL EXAMINATION1 Physical examination
Gen appearance Distress Levine signbullHeart rate pulse respirrate variablebullBlood pressure variablebullLow-grade feverbullExamination of jugular venous pulsationsbullPulmonary CracklesbullS4 gallop due to reduced LV compliancebullS3 gallop if LV dysfunction presentbullMurmurs Pericardial friction rubs
2 ECG
The key to rapid diagnosis and risk stratification for the patient with chest painbullTo be obtained within 10 minutes of arrival to Emergency DepartmentbullFor STEMI 1048774ST-segment elevation gt1mm in 2+ contiguous leads OR new left bundle branch block (LBBB)bullLocation of InfarctLeadsInferior MI II III aVFAnterior MI V2-V4Lateral MI I aVL V5-V6
3 Lab studies
Cardiac Biomarkers CK CK-MB cTnbullSerum ChemistriesbullRenal FunctionbullCoagulation StudiesbullComplete Blood Count
TREATMENTAspirin
bullRapidly blocks formation of thromboxaneA2 in platelets by cyclooxygenase inhibitionbull162-325mg chewed (promotes buccalabsorption)bullISIS-2ndash23 reduction in mortality largely additive to the reduction in mortality from streptokinaseOther Adjuvant TherapiesAnalgesicsbullNitratesbullBeta-blockersbullAce InhibitorsbullOxygenbullHeparinbullIV Glycoprotein IIbIIIaInhibitorsbullClopidogrelbullStatins
Thrombolytic TherapybullCommon AgentsbullTNK-tPA30-50mg IV bolusbullReteplase10U x 2 (each over 2 minutes) IVbullAlteplaseup to 100mg in 90mins (based on weight)
bullContraindicationsndashAbsolute Prior intracranial hemorrhage known cerebral vascular lesion malignant intracranial neoplasm ischemic stroke within 3 months suspected aortic dissection active bleeding recent closed head injury or facial trauma within 3monthsndashRelative History of chronic severe HTN severeuncontrolled HTN at presentation (gt180110) history of ischemic stroke gt3 months traumaticprolonged CPR recent internal bleeding (2-4 weeks) pregnancy active peptic ulcer current anticoagulation
Primary PCI
bullPCI = Percutaneous Coronary Intervention
bullPTCA = Percutaneous Transluminal Coronary Angioplasty
bullPOBA = Plain Old Balloon Angioplasty
PROGNOSIS
bullDischarge usually 5 days after admissionbullSmoking CessationbullShort and Long-term survival depend upon resting LV function residual ischemic myocardium and susceptibility to ventricular arrhythmias
THE END
- CHEST PAIN SCENARIO 3 GROUP 10
- SCENARIO
- KEYWORD
- QUESTION
- DIFFERENTIAL DIAGNOSIS
- INTRODUCTION
- BASIC SCIENCE
- EKG
- Normal heart
- Myocardial Infarction Two to three days after an MI the myocyt
- Slide 11
- PATHOPHYSIOLOGY OF ST-ELEVATION MYOCARDIAL INFARCTION (STEMI)
- myocardial infarction
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- HYPOTENSION May trigger a dramatic sympathetic nervous system
- Slide 19
- Slide 21
- Left Ventricular Function Systolic Function
- Ventricular Remodeling
- references
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- PATHOLOGIC OF Q-WAVE
- PATHOMECANISM CHEST PAIN
- Slide 31
- SMOKING kills
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- ThE eND
-

Systolic Dysfunction
Decrease lungs compliance and stimulates juxtacappilary
receptors
Left ventricle contractility can be
reduced
J receptors effects a reflex that results in rapid shallow
breathing and evokes the subjective feeling of dyspnea
Increase in LV pressure compounded by the ischemia
induced stiffness of the chamber (diastolic dysfunction) is conveyed to the left atrium and pulmonary
veins
Decreasing the stroke volume and causing the diastolic
volume and pressure within the LV to rise
Ischemia affects large amount of myocardium
SERUM MARKER OF INFARCTION
Detection of cardiac-specific troponins and creatine kinase MB isoenzyme
Intracellular macromolecules leak into the cardiac interstitium and ultimately into the bloodstream
Necrosis of myocardial tissue Cause by disruption of the sarcolemma
MYOCARDIAL INFARTION
TYPICAL SYMPTOM- Crushing chest pain
more severe and wider than usual angina
SERUM BIOMARKSCreatine kinaseTroponin
ECG initial finding- St elevation- Q Wave
STEMI
Left Ventricular Function Systolic Function
Upon interruption of antegrade flow in an epicardial coronary artery the zone of myocardium supplied by that vessel immediately loses its ability to shorten and perform contractile work Four abnormal contraction patterns develop in sequence (1) dyssynchrony that is dissociation in the time course of contraction of adjacent segments(2) hypokinesis reduction in the extent of shortening (3) akinesis cessation of shortening and (4) dyskinesis paradoxical expansion and systolic bulging
Hyperkinesis of the remaining normal myocardium initially accompanies dysfunction of the infarcting segment The early hyperkinesis of the noninfarcted zones likely results from acute compensations including increased activity of the sympathetic nervous system and the Frank-Starling mechanism A portion of this compensatory hyperkinesis is ineffective work because contraction of the noninfarcted segments of myocardium hellip
Ventricular Remodelingbull As a consequence of STEMI the changes in left ventricular size shape and
thickness involving both the infarcted and the noninfarcted segments of the ventricle described earlier occur and are collectively referred to as ventricular remodeling which can in turn influence ventricular function and prognosis
bull A combination of changes in left ventricular dilation and hypertrophy of residual noninfarcted myocardium causes remodeling
bull After the size of infarction the two most important factors driving the process of left ventricular dilation are ventricular loading conditions and infarct artery patency
bull Elevated ventricular pressure contributes to increased wall stress and the risk of infarct expansion and a patent infarct artery accelerates myocardial scar formation and increases tissue turgor in the infarct zone reducing the risk of infarct expansion and ventricular dilation
Antman EM Morrow DA McCabe CH et al Enoxaparin versus unfractionated heparin with fibrinolysis for ST-elevation myocardial infarction N Engl J Med 2006 3541477
referencesSLIDE 2 Alpert JS Thygesen K Antman E and Bassand JP Myocardial infarction redefined--a consensus document of The Joint European Society of CardiologyAmerican College of Cardiology Committee for the redefinition of myocardial infarction J Am Coll Cardiol 2000 Sep 36(3) 959-69 pmid10987628bull Book of Pathophysiology of Heart Disease fourth edition editor Leonard SLilly page 179-
184bull ILMU PENYAKIT DALAM Jilid II Edisi V Editor Aru WSudoyo Bambang Setiyohadi
Idrus Alwi page1741-1744
ST elevation MI
ST segment elevation type of acute myocardial infarction require at least 1 mm (01 mV) of ST segment elevation in the limb leads and at least 2 mm elevation in the precordial leads
The clinician must therefore be well versed in recognizing the so-called ECG mimics of acute myocardial infarction which include
These elevations must be present in anatomically contiguous leads (I aVL V5 V6 correspond to the lateral wall V1-V2 correspond to the septal wall V3-V4 correspond to the anterior wall II III aVF correspond to the inferior wall)
left ventricular hypertrophy
left bundle branch block
hyperkalemia
early repolarization
ventricular aneurysm
12-lead electrocardiogram showing ST-segment elevation (orange) in I aVL and V1-V5 with reciprocal changes (blue) in the inferior leads indicative of an anterior wall myocardial infarction
An acute STEMI involving the inferior and right ventricular wall Reciprocal changes are seen in the anterior leads
PATHOLOGIC OF Q-WAVEPathologic Q waves
Any Q-wave in leads V2ndashV3 ge 002 s or QS complex in leads V2 and V3
Q-wave ge 003 s and gt 01 mV deep or QS complex in leads I II aVL aVF or V4ndashV6 in
any two leads of a contiguous lead grouping (I aVLV6 V4ndashV6 II III and aVF)
result of absence of electrical activity
previous myocardial infarction
The evolution of an infarct on the ECG ST elevation Q wave formation T wave inversion
normalisation with a persistent Q wave
PATHOMECANISM CHEST PAINhttpemedicinemedscapecomarticle150215-overview2
ProfDrPeter Kabo Bagaimana Menggunakan Obat-obat kardiovasculer secara Rasional
AtherosclerosisProduce endothelial derived constricting
factor (EDCF)
Increase tonus artery
coronary
Ischemic myocard
Aerobic glycolysis turn
to anerobic glycolysis
Production of adenosin
Diffuse to extracellular
space
Stimulate A1 receptor in cardiac
afferent nerve ending
Bind with somatic cervico
thoracalis nerve at
ascending pathway in
medulla spinalis
Chest pain
SMOKING KILLS
These effects could potentially trigger
symptoms of ischemia in such smokers
One might also expect that the hemodynamic effects of nicotine would contribute to endothelial damage and accelerate the progression of atherosclerosis
Lipolyis - increased levels of circulating free fatty acids
and glycerol in the blood and the resulting increase in fat
metabolism drives a demand for more oxygen leading to
increased coronary blood flow and myocardial oxygen
uptake
addition to its cardiovascular effects such as elevated heart
rate blood pressure and cardiac output
nicotine has metabolic effects in particular increased lipolysis
Nicotine is a sympathomimetic chemical that promotes the release of catecholamines and other
neurotransmitters
SIGNS AND SYMPTOMS
bullChest pain (pressuretightnessheaviness and might radiate to neck arm)
bullIngestion heartburnbullNausea VomitingbullSweatingbullWeaknessbullDizziness
httpwwwcardiosmartorgManageConditionDefaultaspxid=904 httpwwwncbinlmnihgovpmcarticlesPMC2233977
ADDITIONAL EXAMINATION1 Physical examination
Gen appearance Distress Levine signbullHeart rate pulse respirrate variablebullBlood pressure variablebullLow-grade feverbullExamination of jugular venous pulsationsbullPulmonary CracklesbullS4 gallop due to reduced LV compliancebullS3 gallop if LV dysfunction presentbullMurmurs Pericardial friction rubs
2 ECG
The key to rapid diagnosis and risk stratification for the patient with chest painbullTo be obtained within 10 minutes of arrival to Emergency DepartmentbullFor STEMI 1048774ST-segment elevation gt1mm in 2+ contiguous leads OR new left bundle branch block (LBBB)bullLocation of InfarctLeadsInferior MI II III aVFAnterior MI V2-V4Lateral MI I aVL V5-V6
3 Lab studies
Cardiac Biomarkers CK CK-MB cTnbullSerum ChemistriesbullRenal FunctionbullCoagulation StudiesbullComplete Blood Count
TREATMENTAspirin
bullRapidly blocks formation of thromboxaneA2 in platelets by cyclooxygenase inhibitionbull162-325mg chewed (promotes buccalabsorption)bullISIS-2ndash23 reduction in mortality largely additive to the reduction in mortality from streptokinaseOther Adjuvant TherapiesAnalgesicsbullNitratesbullBeta-blockersbullAce InhibitorsbullOxygenbullHeparinbullIV Glycoprotein IIbIIIaInhibitorsbullClopidogrelbullStatins
Thrombolytic TherapybullCommon AgentsbullTNK-tPA30-50mg IV bolusbullReteplase10U x 2 (each over 2 minutes) IVbullAlteplaseup to 100mg in 90mins (based on weight)
bullContraindicationsndashAbsolute Prior intracranial hemorrhage known cerebral vascular lesion malignant intracranial neoplasm ischemic stroke within 3 months suspected aortic dissection active bleeding recent closed head injury or facial trauma within 3monthsndashRelative History of chronic severe HTN severeuncontrolled HTN at presentation (gt180110) history of ischemic stroke gt3 months traumaticprolonged CPR recent internal bleeding (2-4 weeks) pregnancy active peptic ulcer current anticoagulation
Primary PCI
bullPCI = Percutaneous Coronary Intervention
bullPTCA = Percutaneous Transluminal Coronary Angioplasty
bullPOBA = Plain Old Balloon Angioplasty
PROGNOSIS
bullDischarge usually 5 days after admissionbullSmoking CessationbullShort and Long-term survival depend upon resting LV function residual ischemic myocardium and susceptibility to ventricular arrhythmias
THE END
- CHEST PAIN SCENARIO 3 GROUP 10
- SCENARIO
- KEYWORD
- QUESTION
- DIFFERENTIAL DIAGNOSIS
- INTRODUCTION
- BASIC SCIENCE
- EKG
- Normal heart
- Myocardial Infarction Two to three days after an MI the myocyt
- Slide 11
- PATHOPHYSIOLOGY OF ST-ELEVATION MYOCARDIAL INFARCTION (STEMI)
- myocardial infarction
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- HYPOTENSION May trigger a dramatic sympathetic nervous system
- Slide 19
- Slide 21
- Left Ventricular Function Systolic Function
- Ventricular Remodeling
- references
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- PATHOLOGIC OF Q-WAVE
- PATHOMECANISM CHEST PAIN
- Slide 31
- SMOKING kills
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- ThE eND
-

SERUM MARKER OF INFARCTION
Detection of cardiac-specific troponins and creatine kinase MB isoenzyme
Intracellular macromolecules leak into the cardiac interstitium and ultimately into the bloodstream
Necrosis of myocardial tissue Cause by disruption of the sarcolemma
MYOCARDIAL INFARTION
TYPICAL SYMPTOM- Crushing chest pain
more severe and wider than usual angina
SERUM BIOMARKSCreatine kinaseTroponin
ECG initial finding- St elevation- Q Wave
STEMI
Left Ventricular Function Systolic Function
Upon interruption of antegrade flow in an epicardial coronary artery the zone of myocardium supplied by that vessel immediately loses its ability to shorten and perform contractile work Four abnormal contraction patterns develop in sequence (1) dyssynchrony that is dissociation in the time course of contraction of adjacent segments(2) hypokinesis reduction in the extent of shortening (3) akinesis cessation of shortening and (4) dyskinesis paradoxical expansion and systolic bulging
Hyperkinesis of the remaining normal myocardium initially accompanies dysfunction of the infarcting segment The early hyperkinesis of the noninfarcted zones likely results from acute compensations including increased activity of the sympathetic nervous system and the Frank-Starling mechanism A portion of this compensatory hyperkinesis is ineffective work because contraction of the noninfarcted segments of myocardium hellip
Ventricular Remodelingbull As a consequence of STEMI the changes in left ventricular size shape and
thickness involving both the infarcted and the noninfarcted segments of the ventricle described earlier occur and are collectively referred to as ventricular remodeling which can in turn influence ventricular function and prognosis
bull A combination of changes in left ventricular dilation and hypertrophy of residual noninfarcted myocardium causes remodeling
bull After the size of infarction the two most important factors driving the process of left ventricular dilation are ventricular loading conditions and infarct artery patency
bull Elevated ventricular pressure contributes to increased wall stress and the risk of infarct expansion and a patent infarct artery accelerates myocardial scar formation and increases tissue turgor in the infarct zone reducing the risk of infarct expansion and ventricular dilation
Antman EM Morrow DA McCabe CH et al Enoxaparin versus unfractionated heparin with fibrinolysis for ST-elevation myocardial infarction N Engl J Med 2006 3541477
referencesSLIDE 2 Alpert JS Thygesen K Antman E and Bassand JP Myocardial infarction redefined--a consensus document of The Joint European Society of CardiologyAmerican College of Cardiology Committee for the redefinition of myocardial infarction J Am Coll Cardiol 2000 Sep 36(3) 959-69 pmid10987628bull Book of Pathophysiology of Heart Disease fourth edition editor Leonard SLilly page 179-
184bull ILMU PENYAKIT DALAM Jilid II Edisi V Editor Aru WSudoyo Bambang Setiyohadi
Idrus Alwi page1741-1744
ST elevation MI
ST segment elevation type of acute myocardial infarction require at least 1 mm (01 mV) of ST segment elevation in the limb leads and at least 2 mm elevation in the precordial leads
The clinician must therefore be well versed in recognizing the so-called ECG mimics of acute myocardial infarction which include
These elevations must be present in anatomically contiguous leads (I aVL V5 V6 correspond to the lateral wall V1-V2 correspond to the septal wall V3-V4 correspond to the anterior wall II III aVF correspond to the inferior wall)
left ventricular hypertrophy
left bundle branch block
hyperkalemia
early repolarization
ventricular aneurysm
12-lead electrocardiogram showing ST-segment elevation (orange) in I aVL and V1-V5 with reciprocal changes (blue) in the inferior leads indicative of an anterior wall myocardial infarction
An acute STEMI involving the inferior and right ventricular wall Reciprocal changes are seen in the anterior leads
PATHOLOGIC OF Q-WAVEPathologic Q waves
Any Q-wave in leads V2ndashV3 ge 002 s or QS complex in leads V2 and V3
Q-wave ge 003 s and gt 01 mV deep or QS complex in leads I II aVL aVF or V4ndashV6 in
any two leads of a contiguous lead grouping (I aVLV6 V4ndashV6 II III and aVF)
result of absence of electrical activity
previous myocardial infarction
The evolution of an infarct on the ECG ST elevation Q wave formation T wave inversion
normalisation with a persistent Q wave
PATHOMECANISM CHEST PAINhttpemedicinemedscapecomarticle150215-overview2
ProfDrPeter Kabo Bagaimana Menggunakan Obat-obat kardiovasculer secara Rasional
AtherosclerosisProduce endothelial derived constricting
factor (EDCF)
Increase tonus artery
coronary
Ischemic myocard
Aerobic glycolysis turn
to anerobic glycolysis
Production of adenosin
Diffuse to extracellular
space
Stimulate A1 receptor in cardiac
afferent nerve ending
Bind with somatic cervico
thoracalis nerve at
ascending pathway in
medulla spinalis
Chest pain
SMOKING KILLS
These effects could potentially trigger
symptoms of ischemia in such smokers
One might also expect that the hemodynamic effects of nicotine would contribute to endothelial damage and accelerate the progression of atherosclerosis
Lipolyis - increased levels of circulating free fatty acids
and glycerol in the blood and the resulting increase in fat
metabolism drives a demand for more oxygen leading to
increased coronary blood flow and myocardial oxygen
uptake
addition to its cardiovascular effects such as elevated heart
rate blood pressure and cardiac output
nicotine has metabolic effects in particular increased lipolysis
Nicotine is a sympathomimetic chemical that promotes the release of catecholamines and other
neurotransmitters
SIGNS AND SYMPTOMS
bullChest pain (pressuretightnessheaviness and might radiate to neck arm)
bullIngestion heartburnbullNausea VomitingbullSweatingbullWeaknessbullDizziness
httpwwwcardiosmartorgManageConditionDefaultaspxid=904 httpwwwncbinlmnihgovpmcarticlesPMC2233977
ADDITIONAL EXAMINATION1 Physical examination
Gen appearance Distress Levine signbullHeart rate pulse respirrate variablebullBlood pressure variablebullLow-grade feverbullExamination of jugular venous pulsationsbullPulmonary CracklesbullS4 gallop due to reduced LV compliancebullS3 gallop if LV dysfunction presentbullMurmurs Pericardial friction rubs
2 ECG
The key to rapid diagnosis and risk stratification for the patient with chest painbullTo be obtained within 10 minutes of arrival to Emergency DepartmentbullFor STEMI 1048774ST-segment elevation gt1mm in 2+ contiguous leads OR new left bundle branch block (LBBB)bullLocation of InfarctLeadsInferior MI II III aVFAnterior MI V2-V4Lateral MI I aVL V5-V6
3 Lab studies
Cardiac Biomarkers CK CK-MB cTnbullSerum ChemistriesbullRenal FunctionbullCoagulation StudiesbullComplete Blood Count
TREATMENTAspirin
bullRapidly blocks formation of thromboxaneA2 in platelets by cyclooxygenase inhibitionbull162-325mg chewed (promotes buccalabsorption)bullISIS-2ndash23 reduction in mortality largely additive to the reduction in mortality from streptokinaseOther Adjuvant TherapiesAnalgesicsbullNitratesbullBeta-blockersbullAce InhibitorsbullOxygenbullHeparinbullIV Glycoprotein IIbIIIaInhibitorsbullClopidogrelbullStatins
Thrombolytic TherapybullCommon AgentsbullTNK-tPA30-50mg IV bolusbullReteplase10U x 2 (each over 2 minutes) IVbullAlteplaseup to 100mg in 90mins (based on weight)
bullContraindicationsndashAbsolute Prior intracranial hemorrhage known cerebral vascular lesion malignant intracranial neoplasm ischemic stroke within 3 months suspected aortic dissection active bleeding recent closed head injury or facial trauma within 3monthsndashRelative History of chronic severe HTN severeuncontrolled HTN at presentation (gt180110) history of ischemic stroke gt3 months traumaticprolonged CPR recent internal bleeding (2-4 weeks) pregnancy active peptic ulcer current anticoagulation
Primary PCI
bullPCI = Percutaneous Coronary Intervention
bullPTCA = Percutaneous Transluminal Coronary Angioplasty
bullPOBA = Plain Old Balloon Angioplasty
PROGNOSIS
bullDischarge usually 5 days after admissionbullSmoking CessationbullShort and Long-term survival depend upon resting LV function residual ischemic myocardium and susceptibility to ventricular arrhythmias
THE END
- CHEST PAIN SCENARIO 3 GROUP 10
- SCENARIO
- KEYWORD
- QUESTION
- DIFFERENTIAL DIAGNOSIS
- INTRODUCTION
- BASIC SCIENCE
- EKG
- Normal heart
- Myocardial Infarction Two to three days after an MI the myocyt
- Slide 11
- PATHOPHYSIOLOGY OF ST-ELEVATION MYOCARDIAL INFARCTION (STEMI)
- myocardial infarction
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- HYPOTENSION May trigger a dramatic sympathetic nervous system
- Slide 19
- Slide 21
- Left Ventricular Function Systolic Function
- Ventricular Remodeling
- references
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- PATHOLOGIC OF Q-WAVE
- PATHOMECANISM CHEST PAIN
- Slide 31
- SMOKING kills
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- ThE eND
-

MYOCARDIAL INFARTION
TYPICAL SYMPTOM- Crushing chest pain
more severe and wider than usual angina
SERUM BIOMARKSCreatine kinaseTroponin
ECG initial finding- St elevation- Q Wave
STEMI
Left Ventricular Function Systolic Function
Upon interruption of antegrade flow in an epicardial coronary artery the zone of myocardium supplied by that vessel immediately loses its ability to shorten and perform contractile work Four abnormal contraction patterns develop in sequence (1) dyssynchrony that is dissociation in the time course of contraction of adjacent segments(2) hypokinesis reduction in the extent of shortening (3) akinesis cessation of shortening and (4) dyskinesis paradoxical expansion and systolic bulging
Hyperkinesis of the remaining normal myocardium initially accompanies dysfunction of the infarcting segment The early hyperkinesis of the noninfarcted zones likely results from acute compensations including increased activity of the sympathetic nervous system and the Frank-Starling mechanism A portion of this compensatory hyperkinesis is ineffective work because contraction of the noninfarcted segments of myocardium hellip
Ventricular Remodelingbull As a consequence of STEMI the changes in left ventricular size shape and
thickness involving both the infarcted and the noninfarcted segments of the ventricle described earlier occur and are collectively referred to as ventricular remodeling which can in turn influence ventricular function and prognosis
bull A combination of changes in left ventricular dilation and hypertrophy of residual noninfarcted myocardium causes remodeling
bull After the size of infarction the two most important factors driving the process of left ventricular dilation are ventricular loading conditions and infarct artery patency
bull Elevated ventricular pressure contributes to increased wall stress and the risk of infarct expansion and a patent infarct artery accelerates myocardial scar formation and increases tissue turgor in the infarct zone reducing the risk of infarct expansion and ventricular dilation
Antman EM Morrow DA McCabe CH et al Enoxaparin versus unfractionated heparin with fibrinolysis for ST-elevation myocardial infarction N Engl J Med 2006 3541477
referencesSLIDE 2 Alpert JS Thygesen K Antman E and Bassand JP Myocardial infarction redefined--a consensus document of The Joint European Society of CardiologyAmerican College of Cardiology Committee for the redefinition of myocardial infarction J Am Coll Cardiol 2000 Sep 36(3) 959-69 pmid10987628bull Book of Pathophysiology of Heart Disease fourth edition editor Leonard SLilly page 179-
184bull ILMU PENYAKIT DALAM Jilid II Edisi V Editor Aru WSudoyo Bambang Setiyohadi
Idrus Alwi page1741-1744
ST elevation MI
ST segment elevation type of acute myocardial infarction require at least 1 mm (01 mV) of ST segment elevation in the limb leads and at least 2 mm elevation in the precordial leads
The clinician must therefore be well versed in recognizing the so-called ECG mimics of acute myocardial infarction which include
These elevations must be present in anatomically contiguous leads (I aVL V5 V6 correspond to the lateral wall V1-V2 correspond to the septal wall V3-V4 correspond to the anterior wall II III aVF correspond to the inferior wall)
left ventricular hypertrophy
left bundle branch block
hyperkalemia
early repolarization
ventricular aneurysm
12-lead electrocardiogram showing ST-segment elevation (orange) in I aVL and V1-V5 with reciprocal changes (blue) in the inferior leads indicative of an anterior wall myocardial infarction
An acute STEMI involving the inferior and right ventricular wall Reciprocal changes are seen in the anterior leads
PATHOLOGIC OF Q-WAVEPathologic Q waves
Any Q-wave in leads V2ndashV3 ge 002 s or QS complex in leads V2 and V3
Q-wave ge 003 s and gt 01 mV deep or QS complex in leads I II aVL aVF or V4ndashV6 in
any two leads of a contiguous lead grouping (I aVLV6 V4ndashV6 II III and aVF)
result of absence of electrical activity
previous myocardial infarction
The evolution of an infarct on the ECG ST elevation Q wave formation T wave inversion
normalisation with a persistent Q wave
PATHOMECANISM CHEST PAINhttpemedicinemedscapecomarticle150215-overview2
ProfDrPeter Kabo Bagaimana Menggunakan Obat-obat kardiovasculer secara Rasional
AtherosclerosisProduce endothelial derived constricting
factor (EDCF)
Increase tonus artery
coronary
Ischemic myocard
Aerobic glycolysis turn
to anerobic glycolysis
Production of adenosin
Diffuse to extracellular
space
Stimulate A1 receptor in cardiac
afferent nerve ending
Bind with somatic cervico
thoracalis nerve at
ascending pathway in
medulla spinalis
Chest pain
SMOKING KILLS
These effects could potentially trigger
symptoms of ischemia in such smokers
One might also expect that the hemodynamic effects of nicotine would contribute to endothelial damage and accelerate the progression of atherosclerosis
Lipolyis - increased levels of circulating free fatty acids
and glycerol in the blood and the resulting increase in fat
metabolism drives a demand for more oxygen leading to
increased coronary blood flow and myocardial oxygen
uptake
addition to its cardiovascular effects such as elevated heart
rate blood pressure and cardiac output
nicotine has metabolic effects in particular increased lipolysis
Nicotine is a sympathomimetic chemical that promotes the release of catecholamines and other
neurotransmitters
SIGNS AND SYMPTOMS
bullChest pain (pressuretightnessheaviness and might radiate to neck arm)
bullIngestion heartburnbullNausea VomitingbullSweatingbullWeaknessbullDizziness
httpwwwcardiosmartorgManageConditionDefaultaspxid=904 httpwwwncbinlmnihgovpmcarticlesPMC2233977
ADDITIONAL EXAMINATION1 Physical examination
Gen appearance Distress Levine signbullHeart rate pulse respirrate variablebullBlood pressure variablebullLow-grade feverbullExamination of jugular venous pulsationsbullPulmonary CracklesbullS4 gallop due to reduced LV compliancebullS3 gallop if LV dysfunction presentbullMurmurs Pericardial friction rubs
2 ECG
The key to rapid diagnosis and risk stratification for the patient with chest painbullTo be obtained within 10 minutes of arrival to Emergency DepartmentbullFor STEMI 1048774ST-segment elevation gt1mm in 2+ contiguous leads OR new left bundle branch block (LBBB)bullLocation of InfarctLeadsInferior MI II III aVFAnterior MI V2-V4Lateral MI I aVL V5-V6
3 Lab studies
Cardiac Biomarkers CK CK-MB cTnbullSerum ChemistriesbullRenal FunctionbullCoagulation StudiesbullComplete Blood Count
TREATMENTAspirin
bullRapidly blocks formation of thromboxaneA2 in platelets by cyclooxygenase inhibitionbull162-325mg chewed (promotes buccalabsorption)bullISIS-2ndash23 reduction in mortality largely additive to the reduction in mortality from streptokinaseOther Adjuvant TherapiesAnalgesicsbullNitratesbullBeta-blockersbullAce InhibitorsbullOxygenbullHeparinbullIV Glycoprotein IIbIIIaInhibitorsbullClopidogrelbullStatins
Thrombolytic TherapybullCommon AgentsbullTNK-tPA30-50mg IV bolusbullReteplase10U x 2 (each over 2 minutes) IVbullAlteplaseup to 100mg in 90mins (based on weight)
bullContraindicationsndashAbsolute Prior intracranial hemorrhage known cerebral vascular lesion malignant intracranial neoplasm ischemic stroke within 3 months suspected aortic dissection active bleeding recent closed head injury or facial trauma within 3monthsndashRelative History of chronic severe HTN severeuncontrolled HTN at presentation (gt180110) history of ischemic stroke gt3 months traumaticprolonged CPR recent internal bleeding (2-4 weeks) pregnancy active peptic ulcer current anticoagulation
Primary PCI
bullPCI = Percutaneous Coronary Intervention
bullPTCA = Percutaneous Transluminal Coronary Angioplasty
bullPOBA = Plain Old Balloon Angioplasty
PROGNOSIS
bullDischarge usually 5 days after admissionbullSmoking CessationbullShort and Long-term survival depend upon resting LV function residual ischemic myocardium and susceptibility to ventricular arrhythmias
THE END
- CHEST PAIN SCENARIO 3 GROUP 10
- SCENARIO
- KEYWORD
- QUESTION
- DIFFERENTIAL DIAGNOSIS
- INTRODUCTION
- BASIC SCIENCE
- EKG
- Normal heart
- Myocardial Infarction Two to three days after an MI the myocyt
- Slide 11
- PATHOPHYSIOLOGY OF ST-ELEVATION MYOCARDIAL INFARCTION (STEMI)
- myocardial infarction
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- HYPOTENSION May trigger a dramatic sympathetic nervous system
- Slide 19
- Slide 21
- Left Ventricular Function Systolic Function
- Ventricular Remodeling
- references
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- PATHOLOGIC OF Q-WAVE
- PATHOMECANISM CHEST PAIN
- Slide 31
- SMOKING kills
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- ThE eND
-

Left Ventricular Function Systolic Function
Upon interruption of antegrade flow in an epicardial coronary artery the zone of myocardium supplied by that vessel immediately loses its ability to shorten and perform contractile work Four abnormal contraction patterns develop in sequence (1) dyssynchrony that is dissociation in the time course of contraction of adjacent segments(2) hypokinesis reduction in the extent of shortening (3) akinesis cessation of shortening and (4) dyskinesis paradoxical expansion and systolic bulging
Hyperkinesis of the remaining normal myocardium initially accompanies dysfunction of the infarcting segment The early hyperkinesis of the noninfarcted zones likely results from acute compensations including increased activity of the sympathetic nervous system and the Frank-Starling mechanism A portion of this compensatory hyperkinesis is ineffective work because contraction of the noninfarcted segments of myocardium hellip
Ventricular Remodelingbull As a consequence of STEMI the changes in left ventricular size shape and
thickness involving both the infarcted and the noninfarcted segments of the ventricle described earlier occur and are collectively referred to as ventricular remodeling which can in turn influence ventricular function and prognosis
bull A combination of changes in left ventricular dilation and hypertrophy of residual noninfarcted myocardium causes remodeling
bull After the size of infarction the two most important factors driving the process of left ventricular dilation are ventricular loading conditions and infarct artery patency
bull Elevated ventricular pressure contributes to increased wall stress and the risk of infarct expansion and a patent infarct artery accelerates myocardial scar formation and increases tissue turgor in the infarct zone reducing the risk of infarct expansion and ventricular dilation
Antman EM Morrow DA McCabe CH et al Enoxaparin versus unfractionated heparin with fibrinolysis for ST-elevation myocardial infarction N Engl J Med 2006 3541477
referencesSLIDE 2 Alpert JS Thygesen K Antman E and Bassand JP Myocardial infarction redefined--a consensus document of The Joint European Society of CardiologyAmerican College of Cardiology Committee for the redefinition of myocardial infarction J Am Coll Cardiol 2000 Sep 36(3) 959-69 pmid10987628bull Book of Pathophysiology of Heart Disease fourth edition editor Leonard SLilly page 179-
184bull ILMU PENYAKIT DALAM Jilid II Edisi V Editor Aru WSudoyo Bambang Setiyohadi
Idrus Alwi page1741-1744
ST elevation MI
ST segment elevation type of acute myocardial infarction require at least 1 mm (01 mV) of ST segment elevation in the limb leads and at least 2 mm elevation in the precordial leads
The clinician must therefore be well versed in recognizing the so-called ECG mimics of acute myocardial infarction which include
These elevations must be present in anatomically contiguous leads (I aVL V5 V6 correspond to the lateral wall V1-V2 correspond to the septal wall V3-V4 correspond to the anterior wall II III aVF correspond to the inferior wall)
left ventricular hypertrophy
left bundle branch block
hyperkalemia
early repolarization
ventricular aneurysm
12-lead electrocardiogram showing ST-segment elevation (orange) in I aVL and V1-V5 with reciprocal changes (blue) in the inferior leads indicative of an anterior wall myocardial infarction
An acute STEMI involving the inferior and right ventricular wall Reciprocal changes are seen in the anterior leads
PATHOLOGIC OF Q-WAVEPathologic Q waves
Any Q-wave in leads V2ndashV3 ge 002 s or QS complex in leads V2 and V3
Q-wave ge 003 s and gt 01 mV deep or QS complex in leads I II aVL aVF or V4ndashV6 in
any two leads of a contiguous lead grouping (I aVLV6 V4ndashV6 II III and aVF)
result of absence of electrical activity
previous myocardial infarction
The evolution of an infarct on the ECG ST elevation Q wave formation T wave inversion
normalisation with a persistent Q wave
PATHOMECANISM CHEST PAINhttpemedicinemedscapecomarticle150215-overview2
ProfDrPeter Kabo Bagaimana Menggunakan Obat-obat kardiovasculer secara Rasional
AtherosclerosisProduce endothelial derived constricting
factor (EDCF)
Increase tonus artery
coronary
Ischemic myocard
Aerobic glycolysis turn
to anerobic glycolysis
Production of adenosin
Diffuse to extracellular
space
Stimulate A1 receptor in cardiac
afferent nerve ending
Bind with somatic cervico
thoracalis nerve at
ascending pathway in
medulla spinalis
Chest pain
SMOKING KILLS
These effects could potentially trigger
symptoms of ischemia in such smokers
One might also expect that the hemodynamic effects of nicotine would contribute to endothelial damage and accelerate the progression of atherosclerosis
Lipolyis - increased levels of circulating free fatty acids
and glycerol in the blood and the resulting increase in fat
metabolism drives a demand for more oxygen leading to
increased coronary blood flow and myocardial oxygen
uptake
addition to its cardiovascular effects such as elevated heart
rate blood pressure and cardiac output
nicotine has metabolic effects in particular increased lipolysis
Nicotine is a sympathomimetic chemical that promotes the release of catecholamines and other
neurotransmitters
SIGNS AND SYMPTOMS
bullChest pain (pressuretightnessheaviness and might radiate to neck arm)
bullIngestion heartburnbullNausea VomitingbullSweatingbullWeaknessbullDizziness
httpwwwcardiosmartorgManageConditionDefaultaspxid=904 httpwwwncbinlmnihgovpmcarticlesPMC2233977
ADDITIONAL EXAMINATION1 Physical examination
Gen appearance Distress Levine signbullHeart rate pulse respirrate variablebullBlood pressure variablebullLow-grade feverbullExamination of jugular venous pulsationsbullPulmonary CracklesbullS4 gallop due to reduced LV compliancebullS3 gallop if LV dysfunction presentbullMurmurs Pericardial friction rubs
2 ECG
The key to rapid diagnosis and risk stratification for the patient with chest painbullTo be obtained within 10 minutes of arrival to Emergency DepartmentbullFor STEMI 1048774ST-segment elevation gt1mm in 2+ contiguous leads OR new left bundle branch block (LBBB)bullLocation of InfarctLeadsInferior MI II III aVFAnterior MI V2-V4Lateral MI I aVL V5-V6
3 Lab studies
Cardiac Biomarkers CK CK-MB cTnbullSerum ChemistriesbullRenal FunctionbullCoagulation StudiesbullComplete Blood Count
TREATMENTAspirin
bullRapidly blocks formation of thromboxaneA2 in platelets by cyclooxygenase inhibitionbull162-325mg chewed (promotes buccalabsorption)bullISIS-2ndash23 reduction in mortality largely additive to the reduction in mortality from streptokinaseOther Adjuvant TherapiesAnalgesicsbullNitratesbullBeta-blockersbullAce InhibitorsbullOxygenbullHeparinbullIV Glycoprotein IIbIIIaInhibitorsbullClopidogrelbullStatins
Thrombolytic TherapybullCommon AgentsbullTNK-tPA30-50mg IV bolusbullReteplase10U x 2 (each over 2 minutes) IVbullAlteplaseup to 100mg in 90mins (based on weight)
bullContraindicationsndashAbsolute Prior intracranial hemorrhage known cerebral vascular lesion malignant intracranial neoplasm ischemic stroke within 3 months suspected aortic dissection active bleeding recent closed head injury or facial trauma within 3monthsndashRelative History of chronic severe HTN severeuncontrolled HTN at presentation (gt180110) history of ischemic stroke gt3 months traumaticprolonged CPR recent internal bleeding (2-4 weeks) pregnancy active peptic ulcer current anticoagulation
Primary PCI
bullPCI = Percutaneous Coronary Intervention
bullPTCA = Percutaneous Transluminal Coronary Angioplasty
bullPOBA = Plain Old Balloon Angioplasty
PROGNOSIS
bullDischarge usually 5 days after admissionbullSmoking CessationbullShort and Long-term survival depend upon resting LV function residual ischemic myocardium and susceptibility to ventricular arrhythmias
THE END
- CHEST PAIN SCENARIO 3 GROUP 10
- SCENARIO
- KEYWORD
- QUESTION
- DIFFERENTIAL DIAGNOSIS
- INTRODUCTION
- BASIC SCIENCE
- EKG
- Normal heart
- Myocardial Infarction Two to three days after an MI the myocyt
- Slide 11
- PATHOPHYSIOLOGY OF ST-ELEVATION MYOCARDIAL INFARCTION (STEMI)
- myocardial infarction
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- HYPOTENSION May trigger a dramatic sympathetic nervous system
- Slide 19
- Slide 21
- Left Ventricular Function Systolic Function
- Ventricular Remodeling
- references
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- PATHOLOGIC OF Q-WAVE
- PATHOMECANISM CHEST PAIN
- Slide 31
- SMOKING kills
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- ThE eND
-

Ventricular Remodelingbull As a consequence of STEMI the changes in left ventricular size shape and
thickness involving both the infarcted and the noninfarcted segments of the ventricle described earlier occur and are collectively referred to as ventricular remodeling which can in turn influence ventricular function and prognosis
bull A combination of changes in left ventricular dilation and hypertrophy of residual noninfarcted myocardium causes remodeling
bull After the size of infarction the two most important factors driving the process of left ventricular dilation are ventricular loading conditions and infarct artery patency
bull Elevated ventricular pressure contributes to increased wall stress and the risk of infarct expansion and a patent infarct artery accelerates myocardial scar formation and increases tissue turgor in the infarct zone reducing the risk of infarct expansion and ventricular dilation
Antman EM Morrow DA McCabe CH et al Enoxaparin versus unfractionated heparin with fibrinolysis for ST-elevation myocardial infarction N Engl J Med 2006 3541477
referencesSLIDE 2 Alpert JS Thygesen K Antman E and Bassand JP Myocardial infarction redefined--a consensus document of The Joint European Society of CardiologyAmerican College of Cardiology Committee for the redefinition of myocardial infarction J Am Coll Cardiol 2000 Sep 36(3) 959-69 pmid10987628bull Book of Pathophysiology of Heart Disease fourth edition editor Leonard SLilly page 179-
184bull ILMU PENYAKIT DALAM Jilid II Edisi V Editor Aru WSudoyo Bambang Setiyohadi
Idrus Alwi page1741-1744
ST elevation MI
ST segment elevation type of acute myocardial infarction require at least 1 mm (01 mV) of ST segment elevation in the limb leads and at least 2 mm elevation in the precordial leads
The clinician must therefore be well versed in recognizing the so-called ECG mimics of acute myocardial infarction which include
These elevations must be present in anatomically contiguous leads (I aVL V5 V6 correspond to the lateral wall V1-V2 correspond to the septal wall V3-V4 correspond to the anterior wall II III aVF correspond to the inferior wall)
left ventricular hypertrophy
left bundle branch block
hyperkalemia
early repolarization
ventricular aneurysm
12-lead electrocardiogram showing ST-segment elevation (orange) in I aVL and V1-V5 with reciprocal changes (blue) in the inferior leads indicative of an anterior wall myocardial infarction
An acute STEMI involving the inferior and right ventricular wall Reciprocal changes are seen in the anterior leads
PATHOLOGIC OF Q-WAVEPathologic Q waves
Any Q-wave in leads V2ndashV3 ge 002 s or QS complex in leads V2 and V3
Q-wave ge 003 s and gt 01 mV deep or QS complex in leads I II aVL aVF or V4ndashV6 in
any two leads of a contiguous lead grouping (I aVLV6 V4ndashV6 II III and aVF)
result of absence of electrical activity
previous myocardial infarction
The evolution of an infarct on the ECG ST elevation Q wave formation T wave inversion
normalisation with a persistent Q wave
PATHOMECANISM CHEST PAINhttpemedicinemedscapecomarticle150215-overview2
ProfDrPeter Kabo Bagaimana Menggunakan Obat-obat kardiovasculer secara Rasional
AtherosclerosisProduce endothelial derived constricting
factor (EDCF)
Increase tonus artery
coronary
Ischemic myocard
Aerobic glycolysis turn
to anerobic glycolysis
Production of adenosin
Diffuse to extracellular
space
Stimulate A1 receptor in cardiac
afferent nerve ending
Bind with somatic cervico
thoracalis nerve at
ascending pathway in
medulla spinalis
Chest pain
SMOKING KILLS
These effects could potentially trigger
symptoms of ischemia in such smokers
One might also expect that the hemodynamic effects of nicotine would contribute to endothelial damage and accelerate the progression of atherosclerosis
Lipolyis - increased levels of circulating free fatty acids
and glycerol in the blood and the resulting increase in fat
metabolism drives a demand for more oxygen leading to
increased coronary blood flow and myocardial oxygen
uptake
addition to its cardiovascular effects such as elevated heart
rate blood pressure and cardiac output
nicotine has metabolic effects in particular increased lipolysis
Nicotine is a sympathomimetic chemical that promotes the release of catecholamines and other
neurotransmitters
SIGNS AND SYMPTOMS
bullChest pain (pressuretightnessheaviness and might radiate to neck arm)
bullIngestion heartburnbullNausea VomitingbullSweatingbullWeaknessbullDizziness
httpwwwcardiosmartorgManageConditionDefaultaspxid=904 httpwwwncbinlmnihgovpmcarticlesPMC2233977
ADDITIONAL EXAMINATION1 Physical examination
Gen appearance Distress Levine signbullHeart rate pulse respirrate variablebullBlood pressure variablebullLow-grade feverbullExamination of jugular venous pulsationsbullPulmonary CracklesbullS4 gallop due to reduced LV compliancebullS3 gallop if LV dysfunction presentbullMurmurs Pericardial friction rubs
2 ECG
The key to rapid diagnosis and risk stratification for the patient with chest painbullTo be obtained within 10 minutes of arrival to Emergency DepartmentbullFor STEMI 1048774ST-segment elevation gt1mm in 2+ contiguous leads OR new left bundle branch block (LBBB)bullLocation of InfarctLeadsInferior MI II III aVFAnterior MI V2-V4Lateral MI I aVL V5-V6
3 Lab studies
Cardiac Biomarkers CK CK-MB cTnbullSerum ChemistriesbullRenal FunctionbullCoagulation StudiesbullComplete Blood Count
TREATMENTAspirin
bullRapidly blocks formation of thromboxaneA2 in platelets by cyclooxygenase inhibitionbull162-325mg chewed (promotes buccalabsorption)bullISIS-2ndash23 reduction in mortality largely additive to the reduction in mortality from streptokinaseOther Adjuvant TherapiesAnalgesicsbullNitratesbullBeta-blockersbullAce InhibitorsbullOxygenbullHeparinbullIV Glycoprotein IIbIIIaInhibitorsbullClopidogrelbullStatins
Thrombolytic TherapybullCommon AgentsbullTNK-tPA30-50mg IV bolusbullReteplase10U x 2 (each over 2 minutes) IVbullAlteplaseup to 100mg in 90mins (based on weight)
bullContraindicationsndashAbsolute Prior intracranial hemorrhage known cerebral vascular lesion malignant intracranial neoplasm ischemic stroke within 3 months suspected aortic dissection active bleeding recent closed head injury or facial trauma within 3monthsndashRelative History of chronic severe HTN severeuncontrolled HTN at presentation (gt180110) history of ischemic stroke gt3 months traumaticprolonged CPR recent internal bleeding (2-4 weeks) pregnancy active peptic ulcer current anticoagulation
Primary PCI
bullPCI = Percutaneous Coronary Intervention
bullPTCA = Percutaneous Transluminal Coronary Angioplasty
bullPOBA = Plain Old Balloon Angioplasty
PROGNOSIS
bullDischarge usually 5 days after admissionbullSmoking CessationbullShort and Long-term survival depend upon resting LV function residual ischemic myocardium and susceptibility to ventricular arrhythmias
THE END
- CHEST PAIN SCENARIO 3 GROUP 10
- SCENARIO
- KEYWORD
- QUESTION
- DIFFERENTIAL DIAGNOSIS
- INTRODUCTION
- BASIC SCIENCE
- EKG
- Normal heart
- Myocardial Infarction Two to three days after an MI the myocyt
- Slide 11
- PATHOPHYSIOLOGY OF ST-ELEVATION MYOCARDIAL INFARCTION (STEMI)
- myocardial infarction
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- HYPOTENSION May trigger a dramatic sympathetic nervous system
- Slide 19
- Slide 21
- Left Ventricular Function Systolic Function
- Ventricular Remodeling
- references
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- PATHOLOGIC OF Q-WAVE
- PATHOMECANISM CHEST PAIN
- Slide 31
- SMOKING kills
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- ThE eND
-

referencesSLIDE 2 Alpert JS Thygesen K Antman E and Bassand JP Myocardial infarction redefined--a consensus document of The Joint European Society of CardiologyAmerican College of Cardiology Committee for the redefinition of myocardial infarction J Am Coll Cardiol 2000 Sep 36(3) 959-69 pmid10987628bull Book of Pathophysiology of Heart Disease fourth edition editor Leonard SLilly page 179-
184bull ILMU PENYAKIT DALAM Jilid II Edisi V Editor Aru WSudoyo Bambang Setiyohadi
Idrus Alwi page1741-1744
ST elevation MI
ST segment elevation type of acute myocardial infarction require at least 1 mm (01 mV) of ST segment elevation in the limb leads and at least 2 mm elevation in the precordial leads
The clinician must therefore be well versed in recognizing the so-called ECG mimics of acute myocardial infarction which include
These elevations must be present in anatomically contiguous leads (I aVL V5 V6 correspond to the lateral wall V1-V2 correspond to the septal wall V3-V4 correspond to the anterior wall II III aVF correspond to the inferior wall)
left ventricular hypertrophy
left bundle branch block
hyperkalemia
early repolarization
ventricular aneurysm
12-lead electrocardiogram showing ST-segment elevation (orange) in I aVL and V1-V5 with reciprocal changes (blue) in the inferior leads indicative of an anterior wall myocardial infarction
An acute STEMI involving the inferior and right ventricular wall Reciprocal changes are seen in the anterior leads
PATHOLOGIC OF Q-WAVEPathologic Q waves
Any Q-wave in leads V2ndashV3 ge 002 s or QS complex in leads V2 and V3
Q-wave ge 003 s and gt 01 mV deep or QS complex in leads I II aVL aVF or V4ndashV6 in
any two leads of a contiguous lead grouping (I aVLV6 V4ndashV6 II III and aVF)
result of absence of electrical activity
previous myocardial infarction
The evolution of an infarct on the ECG ST elevation Q wave formation T wave inversion
normalisation with a persistent Q wave
PATHOMECANISM CHEST PAINhttpemedicinemedscapecomarticle150215-overview2
ProfDrPeter Kabo Bagaimana Menggunakan Obat-obat kardiovasculer secara Rasional
AtherosclerosisProduce endothelial derived constricting
factor (EDCF)
Increase tonus artery
coronary
Ischemic myocard
Aerobic glycolysis turn
to anerobic glycolysis
Production of adenosin
Diffuse to extracellular
space
Stimulate A1 receptor in cardiac
afferent nerve ending
Bind with somatic cervico
thoracalis nerve at
ascending pathway in
medulla spinalis
Chest pain
SMOKING KILLS
These effects could potentially trigger
symptoms of ischemia in such smokers
One might also expect that the hemodynamic effects of nicotine would contribute to endothelial damage and accelerate the progression of atherosclerosis
Lipolyis - increased levels of circulating free fatty acids
and glycerol in the blood and the resulting increase in fat
metabolism drives a demand for more oxygen leading to
increased coronary blood flow and myocardial oxygen
uptake
addition to its cardiovascular effects such as elevated heart
rate blood pressure and cardiac output
nicotine has metabolic effects in particular increased lipolysis
Nicotine is a sympathomimetic chemical that promotes the release of catecholamines and other
neurotransmitters
SIGNS AND SYMPTOMS
bullChest pain (pressuretightnessheaviness and might radiate to neck arm)
bullIngestion heartburnbullNausea VomitingbullSweatingbullWeaknessbullDizziness
httpwwwcardiosmartorgManageConditionDefaultaspxid=904 httpwwwncbinlmnihgovpmcarticlesPMC2233977
ADDITIONAL EXAMINATION1 Physical examination
Gen appearance Distress Levine signbullHeart rate pulse respirrate variablebullBlood pressure variablebullLow-grade feverbullExamination of jugular venous pulsationsbullPulmonary CracklesbullS4 gallop due to reduced LV compliancebullS3 gallop if LV dysfunction presentbullMurmurs Pericardial friction rubs
2 ECG
The key to rapid diagnosis and risk stratification for the patient with chest painbullTo be obtained within 10 minutes of arrival to Emergency DepartmentbullFor STEMI 1048774ST-segment elevation gt1mm in 2+ contiguous leads OR new left bundle branch block (LBBB)bullLocation of InfarctLeadsInferior MI II III aVFAnterior MI V2-V4Lateral MI I aVL V5-V6
3 Lab studies
Cardiac Biomarkers CK CK-MB cTnbullSerum ChemistriesbullRenal FunctionbullCoagulation StudiesbullComplete Blood Count
TREATMENTAspirin
bullRapidly blocks formation of thromboxaneA2 in platelets by cyclooxygenase inhibitionbull162-325mg chewed (promotes buccalabsorption)bullISIS-2ndash23 reduction in mortality largely additive to the reduction in mortality from streptokinaseOther Adjuvant TherapiesAnalgesicsbullNitratesbullBeta-blockersbullAce InhibitorsbullOxygenbullHeparinbullIV Glycoprotein IIbIIIaInhibitorsbullClopidogrelbullStatins
Thrombolytic TherapybullCommon AgentsbullTNK-tPA30-50mg IV bolusbullReteplase10U x 2 (each over 2 minutes) IVbullAlteplaseup to 100mg in 90mins (based on weight)
bullContraindicationsndashAbsolute Prior intracranial hemorrhage known cerebral vascular lesion malignant intracranial neoplasm ischemic stroke within 3 months suspected aortic dissection active bleeding recent closed head injury or facial trauma within 3monthsndashRelative History of chronic severe HTN severeuncontrolled HTN at presentation (gt180110) history of ischemic stroke gt3 months traumaticprolonged CPR recent internal bleeding (2-4 weeks) pregnancy active peptic ulcer current anticoagulation
Primary PCI
bullPCI = Percutaneous Coronary Intervention
bullPTCA = Percutaneous Transluminal Coronary Angioplasty
bullPOBA = Plain Old Balloon Angioplasty
PROGNOSIS
bullDischarge usually 5 days after admissionbullSmoking CessationbullShort and Long-term survival depend upon resting LV function residual ischemic myocardium and susceptibility to ventricular arrhythmias
THE END
- CHEST PAIN SCENARIO 3 GROUP 10
- SCENARIO
- KEYWORD
- QUESTION
- DIFFERENTIAL DIAGNOSIS
- INTRODUCTION
- BASIC SCIENCE
- EKG
- Normal heart
- Myocardial Infarction Two to three days after an MI the myocyt
- Slide 11
- PATHOPHYSIOLOGY OF ST-ELEVATION MYOCARDIAL INFARCTION (STEMI)
- myocardial infarction
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- HYPOTENSION May trigger a dramatic sympathetic nervous system
- Slide 19
- Slide 21
- Left Ventricular Function Systolic Function
- Ventricular Remodeling
- references
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- PATHOLOGIC OF Q-WAVE
- PATHOMECANISM CHEST PAIN
- Slide 31
- SMOKING kills
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- ThE eND
-

ST elevation MI
ST segment elevation type of acute myocardial infarction require at least 1 mm (01 mV) of ST segment elevation in the limb leads and at least 2 mm elevation in the precordial leads
The clinician must therefore be well versed in recognizing the so-called ECG mimics of acute myocardial infarction which include
These elevations must be present in anatomically contiguous leads (I aVL V5 V6 correspond to the lateral wall V1-V2 correspond to the septal wall V3-V4 correspond to the anterior wall II III aVF correspond to the inferior wall)
left ventricular hypertrophy
left bundle branch block
hyperkalemia
early repolarization
ventricular aneurysm
12-lead electrocardiogram showing ST-segment elevation (orange) in I aVL and V1-V5 with reciprocal changes (blue) in the inferior leads indicative of an anterior wall myocardial infarction
An acute STEMI involving the inferior and right ventricular wall Reciprocal changes are seen in the anterior leads
PATHOLOGIC OF Q-WAVEPathologic Q waves
Any Q-wave in leads V2ndashV3 ge 002 s or QS complex in leads V2 and V3
Q-wave ge 003 s and gt 01 mV deep or QS complex in leads I II aVL aVF or V4ndashV6 in
any two leads of a contiguous lead grouping (I aVLV6 V4ndashV6 II III and aVF)
result of absence of electrical activity
previous myocardial infarction
The evolution of an infarct on the ECG ST elevation Q wave formation T wave inversion
normalisation with a persistent Q wave
PATHOMECANISM CHEST PAINhttpemedicinemedscapecomarticle150215-overview2
ProfDrPeter Kabo Bagaimana Menggunakan Obat-obat kardiovasculer secara Rasional
AtherosclerosisProduce endothelial derived constricting
factor (EDCF)
Increase tonus artery
coronary
Ischemic myocard
Aerobic glycolysis turn
to anerobic glycolysis
Production of adenosin
Diffuse to extracellular
space
Stimulate A1 receptor in cardiac
afferent nerve ending
Bind with somatic cervico
thoracalis nerve at
ascending pathway in
medulla spinalis
Chest pain
SMOKING KILLS
These effects could potentially trigger
symptoms of ischemia in such smokers
One might also expect that the hemodynamic effects of nicotine would contribute to endothelial damage and accelerate the progression of atherosclerosis
Lipolyis - increased levels of circulating free fatty acids
and glycerol in the blood and the resulting increase in fat
metabolism drives a demand for more oxygen leading to
increased coronary blood flow and myocardial oxygen
uptake
addition to its cardiovascular effects such as elevated heart
rate blood pressure and cardiac output
nicotine has metabolic effects in particular increased lipolysis
Nicotine is a sympathomimetic chemical that promotes the release of catecholamines and other
neurotransmitters
SIGNS AND SYMPTOMS
bullChest pain (pressuretightnessheaviness and might radiate to neck arm)
bullIngestion heartburnbullNausea VomitingbullSweatingbullWeaknessbullDizziness
httpwwwcardiosmartorgManageConditionDefaultaspxid=904 httpwwwncbinlmnihgovpmcarticlesPMC2233977
ADDITIONAL EXAMINATION1 Physical examination
Gen appearance Distress Levine signbullHeart rate pulse respirrate variablebullBlood pressure variablebullLow-grade feverbullExamination of jugular venous pulsationsbullPulmonary CracklesbullS4 gallop due to reduced LV compliancebullS3 gallop if LV dysfunction presentbullMurmurs Pericardial friction rubs
2 ECG
The key to rapid diagnosis and risk stratification for the patient with chest painbullTo be obtained within 10 minutes of arrival to Emergency DepartmentbullFor STEMI 1048774ST-segment elevation gt1mm in 2+ contiguous leads OR new left bundle branch block (LBBB)bullLocation of InfarctLeadsInferior MI II III aVFAnterior MI V2-V4Lateral MI I aVL V5-V6
3 Lab studies
Cardiac Biomarkers CK CK-MB cTnbullSerum ChemistriesbullRenal FunctionbullCoagulation StudiesbullComplete Blood Count
TREATMENTAspirin
bullRapidly blocks formation of thromboxaneA2 in platelets by cyclooxygenase inhibitionbull162-325mg chewed (promotes buccalabsorption)bullISIS-2ndash23 reduction in mortality largely additive to the reduction in mortality from streptokinaseOther Adjuvant TherapiesAnalgesicsbullNitratesbullBeta-blockersbullAce InhibitorsbullOxygenbullHeparinbullIV Glycoprotein IIbIIIaInhibitorsbullClopidogrelbullStatins
Thrombolytic TherapybullCommon AgentsbullTNK-tPA30-50mg IV bolusbullReteplase10U x 2 (each over 2 minutes) IVbullAlteplaseup to 100mg in 90mins (based on weight)
bullContraindicationsndashAbsolute Prior intracranial hemorrhage known cerebral vascular lesion malignant intracranial neoplasm ischemic stroke within 3 months suspected aortic dissection active bleeding recent closed head injury or facial trauma within 3monthsndashRelative History of chronic severe HTN severeuncontrolled HTN at presentation (gt180110) history of ischemic stroke gt3 months traumaticprolonged CPR recent internal bleeding (2-4 weeks) pregnancy active peptic ulcer current anticoagulation
Primary PCI
bullPCI = Percutaneous Coronary Intervention
bullPTCA = Percutaneous Transluminal Coronary Angioplasty
bullPOBA = Plain Old Balloon Angioplasty
PROGNOSIS
bullDischarge usually 5 days after admissionbullSmoking CessationbullShort and Long-term survival depend upon resting LV function residual ischemic myocardium and susceptibility to ventricular arrhythmias
THE END
- CHEST PAIN SCENARIO 3 GROUP 10
- SCENARIO
- KEYWORD
- QUESTION
- DIFFERENTIAL DIAGNOSIS
- INTRODUCTION
- BASIC SCIENCE
- EKG
- Normal heart
- Myocardial Infarction Two to three days after an MI the myocyt
- Slide 11
- PATHOPHYSIOLOGY OF ST-ELEVATION MYOCARDIAL INFARCTION (STEMI)
- myocardial infarction
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- HYPOTENSION May trigger a dramatic sympathetic nervous system
- Slide 19
- Slide 21
- Left Ventricular Function Systolic Function
- Ventricular Remodeling
- references
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- PATHOLOGIC OF Q-WAVE
- PATHOMECANISM CHEST PAIN
- Slide 31
- SMOKING kills
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- ThE eND
-

ST segment elevation type of acute myocardial infarction require at least 1 mm (01 mV) of ST segment elevation in the limb leads and at least 2 mm elevation in the precordial leads
The clinician must therefore be well versed in recognizing the so-called ECG mimics of acute myocardial infarction which include
These elevations must be present in anatomically contiguous leads (I aVL V5 V6 correspond to the lateral wall V1-V2 correspond to the septal wall V3-V4 correspond to the anterior wall II III aVF correspond to the inferior wall)
left ventricular hypertrophy
left bundle branch block
hyperkalemia
early repolarization
ventricular aneurysm
12-lead electrocardiogram showing ST-segment elevation (orange) in I aVL and V1-V5 with reciprocal changes (blue) in the inferior leads indicative of an anterior wall myocardial infarction
An acute STEMI involving the inferior and right ventricular wall Reciprocal changes are seen in the anterior leads
PATHOLOGIC OF Q-WAVEPathologic Q waves
Any Q-wave in leads V2ndashV3 ge 002 s or QS complex in leads V2 and V3
Q-wave ge 003 s and gt 01 mV deep or QS complex in leads I II aVL aVF or V4ndashV6 in
any two leads of a contiguous lead grouping (I aVLV6 V4ndashV6 II III and aVF)
result of absence of electrical activity
previous myocardial infarction
The evolution of an infarct on the ECG ST elevation Q wave formation T wave inversion
normalisation with a persistent Q wave
PATHOMECANISM CHEST PAINhttpemedicinemedscapecomarticle150215-overview2
ProfDrPeter Kabo Bagaimana Menggunakan Obat-obat kardiovasculer secara Rasional
AtherosclerosisProduce endothelial derived constricting
factor (EDCF)
Increase tonus artery
coronary
Ischemic myocard
Aerobic glycolysis turn
to anerobic glycolysis
Production of adenosin
Diffuse to extracellular
space
Stimulate A1 receptor in cardiac
afferent nerve ending
Bind with somatic cervico
thoracalis nerve at
ascending pathway in
medulla spinalis
Chest pain
SMOKING KILLS
These effects could potentially trigger
symptoms of ischemia in such smokers
One might also expect that the hemodynamic effects of nicotine would contribute to endothelial damage and accelerate the progression of atherosclerosis
Lipolyis - increased levels of circulating free fatty acids
and glycerol in the blood and the resulting increase in fat
metabolism drives a demand for more oxygen leading to
increased coronary blood flow and myocardial oxygen
uptake
addition to its cardiovascular effects such as elevated heart
rate blood pressure and cardiac output
nicotine has metabolic effects in particular increased lipolysis
Nicotine is a sympathomimetic chemical that promotes the release of catecholamines and other
neurotransmitters
SIGNS AND SYMPTOMS
bullChest pain (pressuretightnessheaviness and might radiate to neck arm)
bullIngestion heartburnbullNausea VomitingbullSweatingbullWeaknessbullDizziness
httpwwwcardiosmartorgManageConditionDefaultaspxid=904 httpwwwncbinlmnihgovpmcarticlesPMC2233977
ADDITIONAL EXAMINATION1 Physical examination
Gen appearance Distress Levine signbullHeart rate pulse respirrate variablebullBlood pressure variablebullLow-grade feverbullExamination of jugular venous pulsationsbullPulmonary CracklesbullS4 gallop due to reduced LV compliancebullS3 gallop if LV dysfunction presentbullMurmurs Pericardial friction rubs
2 ECG
The key to rapid diagnosis and risk stratification for the patient with chest painbullTo be obtained within 10 minutes of arrival to Emergency DepartmentbullFor STEMI 1048774ST-segment elevation gt1mm in 2+ contiguous leads OR new left bundle branch block (LBBB)bullLocation of InfarctLeadsInferior MI II III aVFAnterior MI V2-V4Lateral MI I aVL V5-V6
3 Lab studies
Cardiac Biomarkers CK CK-MB cTnbullSerum ChemistriesbullRenal FunctionbullCoagulation StudiesbullComplete Blood Count
TREATMENTAspirin
bullRapidly blocks formation of thromboxaneA2 in platelets by cyclooxygenase inhibitionbull162-325mg chewed (promotes buccalabsorption)bullISIS-2ndash23 reduction in mortality largely additive to the reduction in mortality from streptokinaseOther Adjuvant TherapiesAnalgesicsbullNitratesbullBeta-blockersbullAce InhibitorsbullOxygenbullHeparinbullIV Glycoprotein IIbIIIaInhibitorsbullClopidogrelbullStatins
Thrombolytic TherapybullCommon AgentsbullTNK-tPA30-50mg IV bolusbullReteplase10U x 2 (each over 2 minutes) IVbullAlteplaseup to 100mg in 90mins (based on weight)
bullContraindicationsndashAbsolute Prior intracranial hemorrhage known cerebral vascular lesion malignant intracranial neoplasm ischemic stroke within 3 months suspected aortic dissection active bleeding recent closed head injury or facial trauma within 3monthsndashRelative History of chronic severe HTN severeuncontrolled HTN at presentation (gt180110) history of ischemic stroke gt3 months traumaticprolonged CPR recent internal bleeding (2-4 weeks) pregnancy active peptic ulcer current anticoagulation
Primary PCI
bullPCI = Percutaneous Coronary Intervention
bullPTCA = Percutaneous Transluminal Coronary Angioplasty
bullPOBA = Plain Old Balloon Angioplasty
PROGNOSIS
bullDischarge usually 5 days after admissionbullSmoking CessationbullShort and Long-term survival depend upon resting LV function residual ischemic myocardium and susceptibility to ventricular arrhythmias
THE END
- CHEST PAIN SCENARIO 3 GROUP 10
- SCENARIO
- KEYWORD
- QUESTION
- DIFFERENTIAL DIAGNOSIS
- INTRODUCTION
- BASIC SCIENCE
- EKG
- Normal heart
- Myocardial Infarction Two to three days after an MI the myocyt
- Slide 11
- PATHOPHYSIOLOGY OF ST-ELEVATION MYOCARDIAL INFARCTION (STEMI)
- myocardial infarction
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- HYPOTENSION May trigger a dramatic sympathetic nervous system
- Slide 19
- Slide 21
- Left Ventricular Function Systolic Function
- Ventricular Remodeling
- references
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- PATHOLOGIC OF Q-WAVE
- PATHOMECANISM CHEST PAIN
- Slide 31
- SMOKING kills
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- ThE eND
-

12-lead electrocardiogram showing ST-segment elevation (orange) in I aVL and V1-V5 with reciprocal changes (blue) in the inferior leads indicative of an anterior wall myocardial infarction
An acute STEMI involving the inferior and right ventricular wall Reciprocal changes are seen in the anterior leads
PATHOLOGIC OF Q-WAVEPathologic Q waves
Any Q-wave in leads V2ndashV3 ge 002 s or QS complex in leads V2 and V3
Q-wave ge 003 s and gt 01 mV deep or QS complex in leads I II aVL aVF or V4ndashV6 in
any two leads of a contiguous lead grouping (I aVLV6 V4ndashV6 II III and aVF)
result of absence of electrical activity
previous myocardial infarction
The evolution of an infarct on the ECG ST elevation Q wave formation T wave inversion
normalisation with a persistent Q wave
PATHOMECANISM CHEST PAINhttpemedicinemedscapecomarticle150215-overview2
ProfDrPeter Kabo Bagaimana Menggunakan Obat-obat kardiovasculer secara Rasional
AtherosclerosisProduce endothelial derived constricting
factor (EDCF)
Increase tonus artery
coronary
Ischemic myocard
Aerobic glycolysis turn
to anerobic glycolysis
Production of adenosin
Diffuse to extracellular
space
Stimulate A1 receptor in cardiac
afferent nerve ending
Bind with somatic cervico
thoracalis nerve at
ascending pathway in
medulla spinalis
Chest pain
SMOKING KILLS
These effects could potentially trigger
symptoms of ischemia in such smokers
One might also expect that the hemodynamic effects of nicotine would contribute to endothelial damage and accelerate the progression of atherosclerosis
Lipolyis - increased levels of circulating free fatty acids
and glycerol in the blood and the resulting increase in fat
metabolism drives a demand for more oxygen leading to
increased coronary blood flow and myocardial oxygen
uptake
addition to its cardiovascular effects such as elevated heart
rate blood pressure and cardiac output
nicotine has metabolic effects in particular increased lipolysis
Nicotine is a sympathomimetic chemical that promotes the release of catecholamines and other
neurotransmitters
SIGNS AND SYMPTOMS
bullChest pain (pressuretightnessheaviness and might radiate to neck arm)
bullIngestion heartburnbullNausea VomitingbullSweatingbullWeaknessbullDizziness
httpwwwcardiosmartorgManageConditionDefaultaspxid=904 httpwwwncbinlmnihgovpmcarticlesPMC2233977
ADDITIONAL EXAMINATION1 Physical examination
Gen appearance Distress Levine signbullHeart rate pulse respirrate variablebullBlood pressure variablebullLow-grade feverbullExamination of jugular venous pulsationsbullPulmonary CracklesbullS4 gallop due to reduced LV compliancebullS3 gallop if LV dysfunction presentbullMurmurs Pericardial friction rubs
2 ECG
The key to rapid diagnosis and risk stratification for the patient with chest painbullTo be obtained within 10 minutes of arrival to Emergency DepartmentbullFor STEMI 1048774ST-segment elevation gt1mm in 2+ contiguous leads OR new left bundle branch block (LBBB)bullLocation of InfarctLeadsInferior MI II III aVFAnterior MI V2-V4Lateral MI I aVL V5-V6
3 Lab studies
Cardiac Biomarkers CK CK-MB cTnbullSerum ChemistriesbullRenal FunctionbullCoagulation StudiesbullComplete Blood Count
TREATMENTAspirin
bullRapidly blocks formation of thromboxaneA2 in platelets by cyclooxygenase inhibitionbull162-325mg chewed (promotes buccalabsorption)bullISIS-2ndash23 reduction in mortality largely additive to the reduction in mortality from streptokinaseOther Adjuvant TherapiesAnalgesicsbullNitratesbullBeta-blockersbullAce InhibitorsbullOxygenbullHeparinbullIV Glycoprotein IIbIIIaInhibitorsbullClopidogrelbullStatins
Thrombolytic TherapybullCommon AgentsbullTNK-tPA30-50mg IV bolusbullReteplase10U x 2 (each over 2 minutes) IVbullAlteplaseup to 100mg in 90mins (based on weight)
bullContraindicationsndashAbsolute Prior intracranial hemorrhage known cerebral vascular lesion malignant intracranial neoplasm ischemic stroke within 3 months suspected aortic dissection active bleeding recent closed head injury or facial trauma within 3monthsndashRelative History of chronic severe HTN severeuncontrolled HTN at presentation (gt180110) history of ischemic stroke gt3 months traumaticprolonged CPR recent internal bleeding (2-4 weeks) pregnancy active peptic ulcer current anticoagulation
Primary PCI
bullPCI = Percutaneous Coronary Intervention
bullPTCA = Percutaneous Transluminal Coronary Angioplasty
bullPOBA = Plain Old Balloon Angioplasty
PROGNOSIS
bullDischarge usually 5 days after admissionbullSmoking CessationbullShort and Long-term survival depend upon resting LV function residual ischemic myocardium and susceptibility to ventricular arrhythmias
THE END
- CHEST PAIN SCENARIO 3 GROUP 10
- SCENARIO
- KEYWORD
- QUESTION
- DIFFERENTIAL DIAGNOSIS
- INTRODUCTION
- BASIC SCIENCE
- EKG
- Normal heart
- Myocardial Infarction Two to three days after an MI the myocyt
- Slide 11
- PATHOPHYSIOLOGY OF ST-ELEVATION MYOCARDIAL INFARCTION (STEMI)
- myocardial infarction
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- HYPOTENSION May trigger a dramatic sympathetic nervous system
- Slide 19
- Slide 21
- Left Ventricular Function Systolic Function
- Ventricular Remodeling
- references
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- PATHOLOGIC OF Q-WAVE
- PATHOMECANISM CHEST PAIN
- Slide 31
- SMOKING kills
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- ThE eND
-
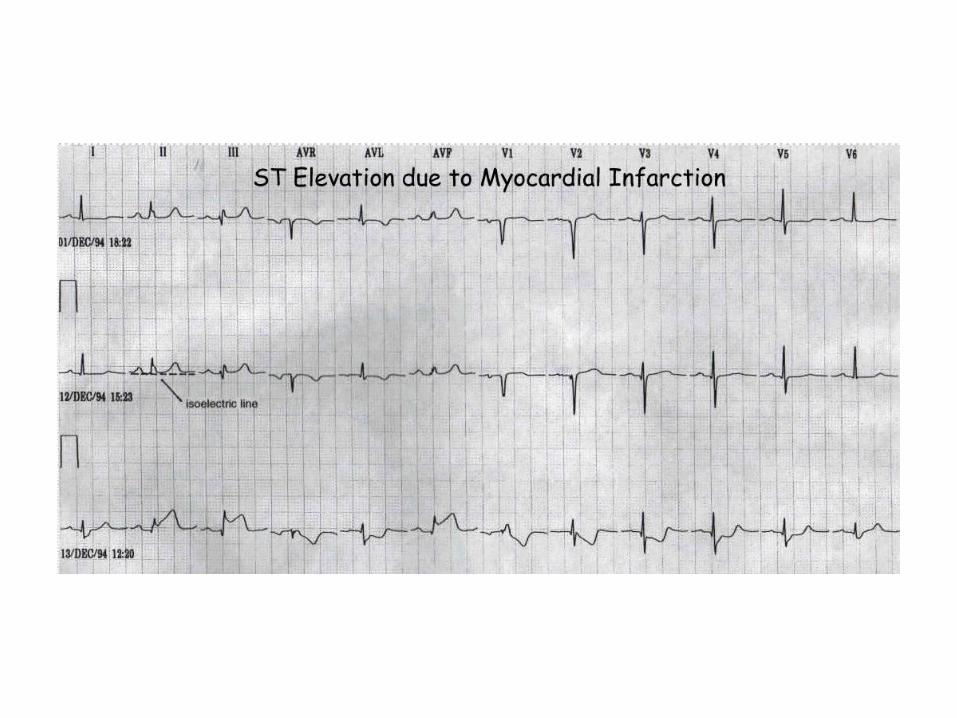
PATHOLOGIC OF Q-WAVEPathologic Q waves
Any Q-wave in leads V2ndashV3 ge 002 s or QS complex in leads V2 and V3
Q-wave ge 003 s and gt 01 mV deep or QS complex in leads I II aVL aVF or V4ndashV6 in
any two leads of a contiguous lead grouping (I aVLV6 V4ndashV6 II III and aVF)
result of absence of electrical activity
previous myocardial infarction
The evolution of an infarct on the ECG ST elevation Q wave formation T wave inversion
normalisation with a persistent Q wave
PATHOMECANISM CHEST PAINhttpemedicinemedscapecomarticle150215-overview2
ProfDrPeter Kabo Bagaimana Menggunakan Obat-obat kardiovasculer secara Rasional
AtherosclerosisProduce endothelial derived constricting
factor (EDCF)
Increase tonus artery
coronary
Ischemic myocard
Aerobic glycolysis turn
to anerobic glycolysis
Production of adenosin
Diffuse to extracellular
space
Stimulate A1 receptor in cardiac
afferent nerve ending
Bind with somatic cervico
thoracalis nerve at
ascending pathway in
medulla spinalis
Chest pain
SMOKING KILLS
These effects could potentially trigger
symptoms of ischemia in such smokers
One might also expect that the hemodynamic effects of nicotine would contribute to endothelial damage and accelerate the progression of atherosclerosis
Lipolyis - increased levels of circulating free fatty acids
and glycerol in the blood and the resulting increase in fat
metabolism drives a demand for more oxygen leading to
increased coronary blood flow and myocardial oxygen
uptake
addition to its cardiovascular effects such as elevated heart
rate blood pressure and cardiac output
nicotine has metabolic effects in particular increased lipolysis
Nicotine is a sympathomimetic chemical that promotes the release of catecholamines and other
neurotransmitters
SIGNS AND SYMPTOMS
bullChest pain (pressuretightnessheaviness and might radiate to neck arm)
bullIngestion heartburnbullNausea VomitingbullSweatingbullWeaknessbullDizziness
httpwwwcardiosmartorgManageConditionDefaultaspxid=904 httpwwwncbinlmnihgovpmcarticlesPMC2233977
ADDITIONAL EXAMINATION1 Physical examination
Gen appearance Distress Levine signbullHeart rate pulse respirrate variablebullBlood pressure variablebullLow-grade feverbullExamination of jugular venous pulsationsbullPulmonary CracklesbullS4 gallop due to reduced LV compliancebullS3 gallop if LV dysfunction presentbullMurmurs Pericardial friction rubs
2 ECG
The key to rapid diagnosis and risk stratification for the patient with chest painbullTo be obtained within 10 minutes of arrival to Emergency DepartmentbullFor STEMI 1048774ST-segment elevation gt1mm in 2+ contiguous leads OR new left bundle branch block (LBBB)bullLocation of InfarctLeadsInferior MI II III aVFAnterior MI V2-V4Lateral MI I aVL V5-V6
3 Lab studies
Cardiac Biomarkers CK CK-MB cTnbullSerum ChemistriesbullRenal FunctionbullCoagulation StudiesbullComplete Blood Count
TREATMENTAspirin
bullRapidly blocks formation of thromboxaneA2 in platelets by cyclooxygenase inhibitionbull162-325mg chewed (promotes buccalabsorption)bullISIS-2ndash23 reduction in mortality largely additive to the reduction in mortality from streptokinaseOther Adjuvant TherapiesAnalgesicsbullNitratesbullBeta-blockersbullAce InhibitorsbullOxygenbullHeparinbullIV Glycoprotein IIbIIIaInhibitorsbullClopidogrelbullStatins
Thrombolytic TherapybullCommon AgentsbullTNK-tPA30-50mg IV bolusbullReteplase10U x 2 (each over 2 minutes) IVbullAlteplaseup to 100mg in 90mins (based on weight)
bullContraindicationsndashAbsolute Prior intracranial hemorrhage known cerebral vascular lesion malignant intracranial neoplasm ischemic stroke within 3 months suspected aortic dissection active bleeding recent closed head injury or facial trauma within 3monthsndashRelative History of chronic severe HTN severeuncontrolled HTN at presentation (gt180110) history of ischemic stroke gt3 months traumaticprolonged CPR recent internal bleeding (2-4 weeks) pregnancy active peptic ulcer current anticoagulation
Primary PCI
bullPCI = Percutaneous Coronary Intervention
bullPTCA = Percutaneous Transluminal Coronary Angioplasty
bullPOBA = Plain Old Balloon Angioplasty
PROGNOSIS
bullDischarge usually 5 days after admissionbullSmoking CessationbullShort and Long-term survival depend upon resting LV function residual ischemic myocardium and susceptibility to ventricular arrhythmias
THE END
- CHEST PAIN SCENARIO 3 GROUP 10
- SCENARIO
- KEYWORD
- QUESTION
- DIFFERENTIAL DIAGNOSIS
- INTRODUCTION
- BASIC SCIENCE
- EKG
- Normal heart
- Myocardial Infarction Two to three days after an MI the myocyt
- Slide 11
- PATHOPHYSIOLOGY OF ST-ELEVATION MYOCARDIAL INFARCTION (STEMI)
- myocardial infarction
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- HYPOTENSION May trigger a dramatic sympathetic nervous system
- Slide 19
- Slide 21
- Left Ventricular Function Systolic Function
- Ventricular Remodeling
- references
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- PATHOLOGIC OF Q-WAVE
- PATHOMECANISM CHEST PAIN
- Slide 31
- SMOKING kills
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- ThE eND
-

PATHOMECANISM CHEST PAINhttpemedicinemedscapecomarticle150215-overview2
ProfDrPeter Kabo Bagaimana Menggunakan Obat-obat kardiovasculer secara Rasional
AtherosclerosisProduce endothelial derived constricting
factor (EDCF)
Increase tonus artery
coronary
Ischemic myocard
Aerobic glycolysis turn
to anerobic glycolysis
Production of adenosin
Diffuse to extracellular
space
Stimulate A1 receptor in cardiac
afferent nerve ending
Bind with somatic cervico
thoracalis nerve at
ascending pathway in
medulla spinalis
Chest pain
SMOKING KILLS
These effects could potentially trigger
symptoms of ischemia in such smokers
One might also expect that the hemodynamic effects of nicotine would contribute to endothelial damage and accelerate the progression of atherosclerosis
Lipolyis - increased levels of circulating free fatty acids
and glycerol in the blood and the resulting increase in fat
metabolism drives a demand for more oxygen leading to
increased coronary blood flow and myocardial oxygen
uptake
addition to its cardiovascular effects such as elevated heart
rate blood pressure and cardiac output
nicotine has metabolic effects in particular increased lipolysis
Nicotine is a sympathomimetic chemical that promotes the release of catecholamines and other
neurotransmitters
SIGNS AND SYMPTOMS
bullChest pain (pressuretightnessheaviness and might radiate to neck arm)
bullIngestion heartburnbullNausea VomitingbullSweatingbullWeaknessbullDizziness
httpwwwcardiosmartorgManageConditionDefaultaspxid=904 httpwwwncbinlmnihgovpmcarticlesPMC2233977
ADDITIONAL EXAMINATION1 Physical examination
Gen appearance Distress Levine signbullHeart rate pulse respirrate variablebullBlood pressure variablebullLow-grade feverbullExamination of jugular venous pulsationsbullPulmonary CracklesbullS4 gallop due to reduced LV compliancebullS3 gallop if LV dysfunction presentbullMurmurs Pericardial friction rubs
2 ECG
The key to rapid diagnosis and risk stratification for the patient with chest painbullTo be obtained within 10 minutes of arrival to Emergency DepartmentbullFor STEMI 1048774ST-segment elevation gt1mm in 2+ contiguous leads OR new left bundle branch block (LBBB)bullLocation of InfarctLeadsInferior MI II III aVFAnterior MI V2-V4Lateral MI I aVL V5-V6
3 Lab studies
Cardiac Biomarkers CK CK-MB cTnbullSerum ChemistriesbullRenal FunctionbullCoagulation StudiesbullComplete Blood Count
TREATMENTAspirin
bullRapidly blocks formation of thromboxaneA2 in platelets by cyclooxygenase inhibitionbull162-325mg chewed (promotes buccalabsorption)bullISIS-2ndash23 reduction in mortality largely additive to the reduction in mortality from streptokinaseOther Adjuvant TherapiesAnalgesicsbullNitratesbullBeta-blockersbullAce InhibitorsbullOxygenbullHeparinbullIV Glycoprotein IIbIIIaInhibitorsbullClopidogrelbullStatins
Thrombolytic TherapybullCommon AgentsbullTNK-tPA30-50mg IV bolusbullReteplase10U x 2 (each over 2 minutes) IVbullAlteplaseup to 100mg in 90mins (based on weight)
bullContraindicationsndashAbsolute Prior intracranial hemorrhage known cerebral vascular lesion malignant intracranial neoplasm ischemic stroke within 3 months suspected aortic dissection active bleeding recent closed head injury or facial trauma within 3monthsndashRelative History of chronic severe HTN severeuncontrolled HTN at presentation (gt180110) history of ischemic stroke gt3 months traumaticprolonged CPR recent internal bleeding (2-4 weeks) pregnancy active peptic ulcer current anticoagulation
Primary PCI
bullPCI = Percutaneous Coronary Intervention
bullPTCA = Percutaneous Transluminal Coronary Angioplasty
bullPOBA = Plain Old Balloon Angioplasty
PROGNOSIS
bullDischarge usually 5 days after admissionbullSmoking CessationbullShort and Long-term survival depend upon resting LV function residual ischemic myocardium and susceptibility to ventricular arrhythmias
THE END
- CHEST PAIN SCENARIO 3 GROUP 10
- SCENARIO
- KEYWORD
- QUESTION
- DIFFERENTIAL DIAGNOSIS
- INTRODUCTION
- BASIC SCIENCE
- EKG
- Normal heart
- Myocardial Infarction Two to three days after an MI the myocyt
- Slide 11
- PATHOPHYSIOLOGY OF ST-ELEVATION MYOCARDIAL INFARCTION (STEMI)
- myocardial infarction
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- HYPOTENSION May trigger a dramatic sympathetic nervous system
- Slide 19
- Slide 21
- Left Ventricular Function Systolic Function
- Ventricular Remodeling
- references
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- PATHOLOGIC OF Q-WAVE
- PATHOMECANISM CHEST PAIN
- Slide 31
- SMOKING kills
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- ThE eND
-

AtherosclerosisProduce endothelial derived constricting
factor (EDCF)
Increase tonus artery
coronary
Ischemic myocard
Aerobic glycolysis turn
to anerobic glycolysis
Production of adenosin
Diffuse to extracellular
space
Stimulate A1 receptor in cardiac
afferent nerve ending
Bind with somatic cervico
thoracalis nerve at
ascending pathway in
medulla spinalis
Chest pain
SMOKING KILLS
These effects could potentially trigger
symptoms of ischemia in such smokers
One might also expect that the hemodynamic effects of nicotine would contribute to endothelial damage and accelerate the progression of atherosclerosis
Lipolyis - increased levels of circulating free fatty acids
and glycerol in the blood and the resulting increase in fat
metabolism drives a demand for more oxygen leading to
increased coronary blood flow and myocardial oxygen
uptake
addition to its cardiovascular effects such as elevated heart
rate blood pressure and cardiac output
nicotine has metabolic effects in particular increased lipolysis
Nicotine is a sympathomimetic chemical that promotes the release of catecholamines and other
neurotransmitters
SIGNS AND SYMPTOMS
bullChest pain (pressuretightnessheaviness and might radiate to neck arm)
bullIngestion heartburnbullNausea VomitingbullSweatingbullWeaknessbullDizziness
httpwwwcardiosmartorgManageConditionDefaultaspxid=904 httpwwwncbinlmnihgovpmcarticlesPMC2233977
ADDITIONAL EXAMINATION1 Physical examination
Gen appearance Distress Levine signbullHeart rate pulse respirrate variablebullBlood pressure variablebullLow-grade feverbullExamination of jugular venous pulsationsbullPulmonary CracklesbullS4 gallop due to reduced LV compliancebullS3 gallop if LV dysfunction presentbullMurmurs Pericardial friction rubs
2 ECG
The key to rapid diagnosis and risk stratification for the patient with chest painbullTo be obtained within 10 minutes of arrival to Emergency DepartmentbullFor STEMI 1048774ST-segment elevation gt1mm in 2+ contiguous leads OR new left bundle branch block (LBBB)bullLocation of InfarctLeadsInferior MI II III aVFAnterior MI V2-V4Lateral MI I aVL V5-V6
3 Lab studies
Cardiac Biomarkers CK CK-MB cTnbullSerum ChemistriesbullRenal FunctionbullCoagulation StudiesbullComplete Blood Count
TREATMENTAspirin
bullRapidly blocks formation of thromboxaneA2 in platelets by cyclooxygenase inhibitionbull162-325mg chewed (promotes buccalabsorption)bullISIS-2ndash23 reduction in mortality largely additive to the reduction in mortality from streptokinaseOther Adjuvant TherapiesAnalgesicsbullNitratesbullBeta-blockersbullAce InhibitorsbullOxygenbullHeparinbullIV Glycoprotein IIbIIIaInhibitorsbullClopidogrelbullStatins
Thrombolytic TherapybullCommon AgentsbullTNK-tPA30-50mg IV bolusbullReteplase10U x 2 (each over 2 minutes) IVbullAlteplaseup to 100mg in 90mins (based on weight)
bullContraindicationsndashAbsolute Prior intracranial hemorrhage known cerebral vascular lesion malignant intracranial neoplasm ischemic stroke within 3 months suspected aortic dissection active bleeding recent closed head injury or facial trauma within 3monthsndashRelative History of chronic severe HTN severeuncontrolled HTN at presentation (gt180110) history of ischemic stroke gt3 months traumaticprolonged CPR recent internal bleeding (2-4 weeks) pregnancy active peptic ulcer current anticoagulation
Primary PCI
bullPCI = Percutaneous Coronary Intervention
bullPTCA = Percutaneous Transluminal Coronary Angioplasty
bullPOBA = Plain Old Balloon Angioplasty
PROGNOSIS
bullDischarge usually 5 days after admissionbullSmoking CessationbullShort and Long-term survival depend upon resting LV function residual ischemic myocardium and susceptibility to ventricular arrhythmias
THE END
- CHEST PAIN SCENARIO 3 GROUP 10
- SCENARIO
- KEYWORD
- QUESTION
- DIFFERENTIAL DIAGNOSIS
- INTRODUCTION
- BASIC SCIENCE
- EKG
- Normal heart
- Myocardial Infarction Two to three days after an MI the myocyt
- Slide 11
- PATHOPHYSIOLOGY OF ST-ELEVATION MYOCARDIAL INFARCTION (STEMI)
- myocardial infarction
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- HYPOTENSION May trigger a dramatic sympathetic nervous system
- Slide 19
- Slide 21
- Left Ventricular Function Systolic Function
- Ventricular Remodeling
- references
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- PATHOLOGIC OF Q-WAVE
- PATHOMECANISM CHEST PAIN
- Slide 31
- SMOKING kills
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- ThE eND
-

SMOKING KILLS
These effects could potentially trigger
symptoms of ischemia in such smokers
One might also expect that the hemodynamic effects of nicotine would contribute to endothelial damage and accelerate the progression of atherosclerosis
Lipolyis - increased levels of circulating free fatty acids
and glycerol in the blood and the resulting increase in fat
metabolism drives a demand for more oxygen leading to
increased coronary blood flow and myocardial oxygen
uptake
addition to its cardiovascular effects such as elevated heart
rate blood pressure and cardiac output
nicotine has metabolic effects in particular increased lipolysis
Nicotine is a sympathomimetic chemical that promotes the release of catecholamines and other
neurotransmitters
SIGNS AND SYMPTOMS
bullChest pain (pressuretightnessheaviness and might radiate to neck arm)
bullIngestion heartburnbullNausea VomitingbullSweatingbullWeaknessbullDizziness
httpwwwcardiosmartorgManageConditionDefaultaspxid=904 httpwwwncbinlmnihgovpmcarticlesPMC2233977
ADDITIONAL EXAMINATION1 Physical examination
Gen appearance Distress Levine signbullHeart rate pulse respirrate variablebullBlood pressure variablebullLow-grade feverbullExamination of jugular venous pulsationsbullPulmonary CracklesbullS4 gallop due to reduced LV compliancebullS3 gallop if LV dysfunction presentbullMurmurs Pericardial friction rubs
2 ECG
The key to rapid diagnosis and risk stratification for the patient with chest painbullTo be obtained within 10 minutes of arrival to Emergency DepartmentbullFor STEMI 1048774ST-segment elevation gt1mm in 2+ contiguous leads OR new left bundle branch block (LBBB)bullLocation of InfarctLeadsInferior MI II III aVFAnterior MI V2-V4Lateral MI I aVL V5-V6
3 Lab studies
Cardiac Biomarkers CK CK-MB cTnbullSerum ChemistriesbullRenal FunctionbullCoagulation StudiesbullComplete Blood Count
TREATMENTAspirin
bullRapidly blocks formation of thromboxaneA2 in platelets by cyclooxygenase inhibitionbull162-325mg chewed (promotes buccalabsorption)bullISIS-2ndash23 reduction in mortality largely additive to the reduction in mortality from streptokinaseOther Adjuvant TherapiesAnalgesicsbullNitratesbullBeta-blockersbullAce InhibitorsbullOxygenbullHeparinbullIV Glycoprotein IIbIIIaInhibitorsbullClopidogrelbullStatins
Thrombolytic TherapybullCommon AgentsbullTNK-tPA30-50mg IV bolusbullReteplase10U x 2 (each over 2 minutes) IVbullAlteplaseup to 100mg in 90mins (based on weight)
bullContraindicationsndashAbsolute Prior intracranial hemorrhage known cerebral vascular lesion malignant intracranial neoplasm ischemic stroke within 3 months suspected aortic dissection active bleeding recent closed head injury or facial trauma within 3monthsndashRelative History of chronic severe HTN severeuncontrolled HTN at presentation (gt180110) history of ischemic stroke gt3 months traumaticprolonged CPR recent internal bleeding (2-4 weeks) pregnancy active peptic ulcer current anticoagulation
Primary PCI
bullPCI = Percutaneous Coronary Intervention
bullPTCA = Percutaneous Transluminal Coronary Angioplasty
bullPOBA = Plain Old Balloon Angioplasty
PROGNOSIS
bullDischarge usually 5 days after admissionbullSmoking CessationbullShort and Long-term survival depend upon resting LV function residual ischemic myocardium and susceptibility to ventricular arrhythmias
THE END
- CHEST PAIN SCENARIO 3 GROUP 10
- SCENARIO
- KEYWORD
- QUESTION
- DIFFERENTIAL DIAGNOSIS
- INTRODUCTION
- BASIC SCIENCE
- EKG
- Normal heart
- Myocardial Infarction Two to three days after an MI the myocyt
- Slide 11
- PATHOPHYSIOLOGY OF ST-ELEVATION MYOCARDIAL INFARCTION (STEMI)
- myocardial infarction
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- HYPOTENSION May trigger a dramatic sympathetic nervous system
- Slide 19
- Slide 21
- Left Ventricular Function Systolic Function
- Ventricular Remodeling
- references
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- PATHOLOGIC OF Q-WAVE
- PATHOMECANISM CHEST PAIN
- Slide 31
- SMOKING kills
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- ThE eND
-

These effects could potentially trigger
symptoms of ischemia in such smokers
One might also expect that the hemodynamic effects of nicotine would contribute to endothelial damage and accelerate the progression of atherosclerosis
Lipolyis - increased levels of circulating free fatty acids
and glycerol in the blood and the resulting increase in fat
metabolism drives a demand for more oxygen leading to
increased coronary blood flow and myocardial oxygen
uptake
addition to its cardiovascular effects such as elevated heart
rate blood pressure and cardiac output
nicotine has metabolic effects in particular increased lipolysis
Nicotine is a sympathomimetic chemical that promotes the release of catecholamines and other
neurotransmitters
SIGNS AND SYMPTOMS
bullChest pain (pressuretightnessheaviness and might radiate to neck arm)
bullIngestion heartburnbullNausea VomitingbullSweatingbullWeaknessbullDizziness
httpwwwcardiosmartorgManageConditionDefaultaspxid=904 httpwwwncbinlmnihgovpmcarticlesPMC2233977
ADDITIONAL EXAMINATION1 Physical examination
Gen appearance Distress Levine signbullHeart rate pulse respirrate variablebullBlood pressure variablebullLow-grade feverbullExamination of jugular venous pulsationsbullPulmonary CracklesbullS4 gallop due to reduced LV compliancebullS3 gallop if LV dysfunction presentbullMurmurs Pericardial friction rubs
2 ECG
The key to rapid diagnosis and risk stratification for the patient with chest painbullTo be obtained within 10 minutes of arrival to Emergency DepartmentbullFor STEMI 1048774ST-segment elevation gt1mm in 2+ contiguous leads OR new left bundle branch block (LBBB)bullLocation of InfarctLeadsInferior MI II III aVFAnterior MI V2-V4Lateral MI I aVL V5-V6
3 Lab studies
Cardiac Biomarkers CK CK-MB cTnbullSerum ChemistriesbullRenal FunctionbullCoagulation StudiesbullComplete Blood Count
TREATMENTAspirin
bullRapidly blocks formation of thromboxaneA2 in platelets by cyclooxygenase inhibitionbull162-325mg chewed (promotes buccalabsorption)bullISIS-2ndash23 reduction in mortality largely additive to the reduction in mortality from streptokinaseOther Adjuvant TherapiesAnalgesicsbullNitratesbullBeta-blockersbullAce InhibitorsbullOxygenbullHeparinbullIV Glycoprotein IIbIIIaInhibitorsbullClopidogrelbullStatins
Thrombolytic TherapybullCommon AgentsbullTNK-tPA30-50mg IV bolusbullReteplase10U x 2 (each over 2 minutes) IVbullAlteplaseup to 100mg in 90mins (based on weight)
bullContraindicationsndashAbsolute Prior intracranial hemorrhage known cerebral vascular lesion malignant intracranial neoplasm ischemic stroke within 3 months suspected aortic dissection active bleeding recent closed head injury or facial trauma within 3monthsndashRelative History of chronic severe HTN severeuncontrolled HTN at presentation (gt180110) history of ischemic stroke gt3 months traumaticprolonged CPR recent internal bleeding (2-4 weeks) pregnancy active peptic ulcer current anticoagulation
Primary PCI
bullPCI = Percutaneous Coronary Intervention
bullPTCA = Percutaneous Transluminal Coronary Angioplasty
bullPOBA = Plain Old Balloon Angioplasty
PROGNOSIS
bullDischarge usually 5 days after admissionbullSmoking CessationbullShort and Long-term survival depend upon resting LV function residual ischemic myocardium and susceptibility to ventricular arrhythmias
THE END
- CHEST PAIN SCENARIO 3 GROUP 10
- SCENARIO
- KEYWORD
- QUESTION
- DIFFERENTIAL DIAGNOSIS
- INTRODUCTION
- BASIC SCIENCE
- EKG
- Normal heart
- Myocardial Infarction Two to three days after an MI the myocyt
- Slide 11
- PATHOPHYSIOLOGY OF ST-ELEVATION MYOCARDIAL INFARCTION (STEMI)
- myocardial infarction
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- HYPOTENSION May trigger a dramatic sympathetic nervous system
- Slide 19
- Slide 21
- Left Ventricular Function Systolic Function
- Ventricular Remodeling
- references
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- PATHOLOGIC OF Q-WAVE
- PATHOMECANISM CHEST PAIN
- Slide 31
- SMOKING kills
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- ThE eND
-

SIGNS AND SYMPTOMS
bullChest pain (pressuretightnessheaviness and might radiate to neck arm)
bullIngestion heartburnbullNausea VomitingbullSweatingbullWeaknessbullDizziness
httpwwwcardiosmartorgManageConditionDefaultaspxid=904 httpwwwncbinlmnihgovpmcarticlesPMC2233977
ADDITIONAL EXAMINATION1 Physical examination
Gen appearance Distress Levine signbullHeart rate pulse respirrate variablebullBlood pressure variablebullLow-grade feverbullExamination of jugular venous pulsationsbullPulmonary CracklesbullS4 gallop due to reduced LV compliancebullS3 gallop if LV dysfunction presentbullMurmurs Pericardial friction rubs
2 ECG
The key to rapid diagnosis and risk stratification for the patient with chest painbullTo be obtained within 10 minutes of arrival to Emergency DepartmentbullFor STEMI 1048774ST-segment elevation gt1mm in 2+ contiguous leads OR new left bundle branch block (LBBB)bullLocation of InfarctLeadsInferior MI II III aVFAnterior MI V2-V4Lateral MI I aVL V5-V6
3 Lab studies
Cardiac Biomarkers CK CK-MB cTnbullSerum ChemistriesbullRenal FunctionbullCoagulation StudiesbullComplete Blood Count
TREATMENTAspirin
bullRapidly blocks formation of thromboxaneA2 in platelets by cyclooxygenase inhibitionbull162-325mg chewed (promotes buccalabsorption)bullISIS-2ndash23 reduction in mortality largely additive to the reduction in mortality from streptokinaseOther Adjuvant TherapiesAnalgesicsbullNitratesbullBeta-blockersbullAce InhibitorsbullOxygenbullHeparinbullIV Glycoprotein IIbIIIaInhibitorsbullClopidogrelbullStatins
Thrombolytic TherapybullCommon AgentsbullTNK-tPA30-50mg IV bolusbullReteplase10U x 2 (each over 2 minutes) IVbullAlteplaseup to 100mg in 90mins (based on weight)
bullContraindicationsndashAbsolute Prior intracranial hemorrhage known cerebral vascular lesion malignant intracranial neoplasm ischemic stroke within 3 months suspected aortic dissection active bleeding recent closed head injury or facial trauma within 3monthsndashRelative History of chronic severe HTN severeuncontrolled HTN at presentation (gt180110) history of ischemic stroke gt3 months traumaticprolonged CPR recent internal bleeding (2-4 weeks) pregnancy active peptic ulcer current anticoagulation
Primary PCI
bullPCI = Percutaneous Coronary Intervention
bullPTCA = Percutaneous Transluminal Coronary Angioplasty
bullPOBA = Plain Old Balloon Angioplasty
PROGNOSIS
bullDischarge usually 5 days after admissionbullSmoking CessationbullShort and Long-term survival depend upon resting LV function residual ischemic myocardium and susceptibility to ventricular arrhythmias
THE END
- CHEST PAIN SCENARIO 3 GROUP 10
- SCENARIO
- KEYWORD
- QUESTION
- DIFFERENTIAL DIAGNOSIS
- INTRODUCTION
- BASIC SCIENCE
- EKG
- Normal heart
- Myocardial Infarction Two to three days after an MI the myocyt
- Slide 11
- PATHOPHYSIOLOGY OF ST-ELEVATION MYOCARDIAL INFARCTION (STEMI)
- myocardial infarction
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- HYPOTENSION May trigger a dramatic sympathetic nervous system
- Slide 19
- Slide 21
- Left Ventricular Function Systolic Function
- Ventricular Remodeling
- references
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- PATHOLOGIC OF Q-WAVE
- PATHOMECANISM CHEST PAIN
- Slide 31
- SMOKING kills
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- ThE eND
-

ADDITIONAL EXAMINATION1 Physical examination
Gen appearance Distress Levine signbullHeart rate pulse respirrate variablebullBlood pressure variablebullLow-grade feverbullExamination of jugular venous pulsationsbullPulmonary CracklesbullS4 gallop due to reduced LV compliancebullS3 gallop if LV dysfunction presentbullMurmurs Pericardial friction rubs
2 ECG
The key to rapid diagnosis and risk stratification for the patient with chest painbullTo be obtained within 10 minutes of arrival to Emergency DepartmentbullFor STEMI 1048774ST-segment elevation gt1mm in 2+ contiguous leads OR new left bundle branch block (LBBB)bullLocation of InfarctLeadsInferior MI II III aVFAnterior MI V2-V4Lateral MI I aVL V5-V6
3 Lab studies
Cardiac Biomarkers CK CK-MB cTnbullSerum ChemistriesbullRenal FunctionbullCoagulation StudiesbullComplete Blood Count
TREATMENTAspirin
bullRapidly blocks formation of thromboxaneA2 in platelets by cyclooxygenase inhibitionbull162-325mg chewed (promotes buccalabsorption)bullISIS-2ndash23 reduction in mortality largely additive to the reduction in mortality from streptokinaseOther Adjuvant TherapiesAnalgesicsbullNitratesbullBeta-blockersbullAce InhibitorsbullOxygenbullHeparinbullIV Glycoprotein IIbIIIaInhibitorsbullClopidogrelbullStatins
Thrombolytic TherapybullCommon AgentsbullTNK-tPA30-50mg IV bolusbullReteplase10U x 2 (each over 2 minutes) IVbullAlteplaseup to 100mg in 90mins (based on weight)
bullContraindicationsndashAbsolute Prior intracranial hemorrhage known cerebral vascular lesion malignant intracranial neoplasm ischemic stroke within 3 months suspected aortic dissection active bleeding recent closed head injury or facial trauma within 3monthsndashRelative History of chronic severe HTN severeuncontrolled HTN at presentation (gt180110) history of ischemic stroke gt3 months traumaticprolonged CPR recent internal bleeding (2-4 weeks) pregnancy active peptic ulcer current anticoagulation
Primary PCI
bullPCI = Percutaneous Coronary Intervention
bullPTCA = Percutaneous Transluminal Coronary Angioplasty
bullPOBA = Plain Old Balloon Angioplasty
PROGNOSIS
bullDischarge usually 5 days after admissionbullSmoking CessationbullShort and Long-term survival depend upon resting LV function residual ischemic myocardium and susceptibility to ventricular arrhythmias
THE END
- CHEST PAIN SCENARIO 3 GROUP 10
- SCENARIO
- KEYWORD
- QUESTION
- DIFFERENTIAL DIAGNOSIS
- INTRODUCTION
- BASIC SCIENCE
- EKG
- Normal heart
- Myocardial Infarction Two to three days after an MI the myocyt
- Slide 11
- PATHOPHYSIOLOGY OF ST-ELEVATION MYOCARDIAL INFARCTION (STEMI)
- myocardial infarction
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- HYPOTENSION May trigger a dramatic sympathetic nervous system
- Slide 19
- Slide 21
- Left Ventricular Function Systolic Function
- Ventricular Remodeling
- references
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- PATHOLOGIC OF Q-WAVE
- PATHOMECANISM CHEST PAIN
- Slide 31
- SMOKING kills
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- ThE eND
-

2 ECG
The key to rapid diagnosis and risk stratification for the patient with chest painbullTo be obtained within 10 minutes of arrival to Emergency DepartmentbullFor STEMI 1048774ST-segment elevation gt1mm in 2+ contiguous leads OR new left bundle branch block (LBBB)bullLocation of InfarctLeadsInferior MI II III aVFAnterior MI V2-V4Lateral MI I aVL V5-V6
3 Lab studies
Cardiac Biomarkers CK CK-MB cTnbullSerum ChemistriesbullRenal FunctionbullCoagulation StudiesbullComplete Blood Count
TREATMENTAspirin
bullRapidly blocks formation of thromboxaneA2 in platelets by cyclooxygenase inhibitionbull162-325mg chewed (promotes buccalabsorption)bullISIS-2ndash23 reduction in mortality largely additive to the reduction in mortality from streptokinaseOther Adjuvant TherapiesAnalgesicsbullNitratesbullBeta-blockersbullAce InhibitorsbullOxygenbullHeparinbullIV Glycoprotein IIbIIIaInhibitorsbullClopidogrelbullStatins
Thrombolytic TherapybullCommon AgentsbullTNK-tPA30-50mg IV bolusbullReteplase10U x 2 (each over 2 minutes) IVbullAlteplaseup to 100mg in 90mins (based on weight)
bullContraindicationsndashAbsolute Prior intracranial hemorrhage known cerebral vascular lesion malignant intracranial neoplasm ischemic stroke within 3 months suspected aortic dissection active bleeding recent closed head injury or facial trauma within 3monthsndashRelative History of chronic severe HTN severeuncontrolled HTN at presentation (gt180110) history of ischemic stroke gt3 months traumaticprolonged CPR recent internal bleeding (2-4 weeks) pregnancy active peptic ulcer current anticoagulation
Primary PCI
bullPCI = Percutaneous Coronary Intervention
bullPTCA = Percutaneous Transluminal Coronary Angioplasty
bullPOBA = Plain Old Balloon Angioplasty
PROGNOSIS
bullDischarge usually 5 days after admissionbullSmoking CessationbullShort and Long-term survival depend upon resting LV function residual ischemic myocardium and susceptibility to ventricular arrhythmias
THE END
- CHEST PAIN SCENARIO 3 GROUP 10
- SCENARIO
- KEYWORD
- QUESTION
- DIFFERENTIAL DIAGNOSIS
- INTRODUCTION
- BASIC SCIENCE
- EKG
- Normal heart
- Myocardial Infarction Two to three days after an MI the myocyt
- Slide 11
- PATHOPHYSIOLOGY OF ST-ELEVATION MYOCARDIAL INFARCTION (STEMI)
- myocardial infarction
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- HYPOTENSION May trigger a dramatic sympathetic nervous system
- Slide 19
- Slide 21
- Left Ventricular Function Systolic Function
- Ventricular Remodeling
- references
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- PATHOLOGIC OF Q-WAVE
- PATHOMECANISM CHEST PAIN
- Slide 31
- SMOKING kills
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- ThE eND
-

3 Lab studies
Cardiac Biomarkers CK CK-MB cTnbullSerum ChemistriesbullRenal FunctionbullCoagulation StudiesbullComplete Blood Count
TREATMENTAspirin
bullRapidly blocks formation of thromboxaneA2 in platelets by cyclooxygenase inhibitionbull162-325mg chewed (promotes buccalabsorption)bullISIS-2ndash23 reduction in mortality largely additive to the reduction in mortality from streptokinaseOther Adjuvant TherapiesAnalgesicsbullNitratesbullBeta-blockersbullAce InhibitorsbullOxygenbullHeparinbullIV Glycoprotein IIbIIIaInhibitorsbullClopidogrelbullStatins
Thrombolytic TherapybullCommon AgentsbullTNK-tPA30-50mg IV bolusbullReteplase10U x 2 (each over 2 minutes) IVbullAlteplaseup to 100mg in 90mins (based on weight)
bullContraindicationsndashAbsolute Prior intracranial hemorrhage known cerebral vascular lesion malignant intracranial neoplasm ischemic stroke within 3 months suspected aortic dissection active bleeding recent closed head injury or facial trauma within 3monthsndashRelative History of chronic severe HTN severeuncontrolled HTN at presentation (gt180110) history of ischemic stroke gt3 months traumaticprolonged CPR recent internal bleeding (2-4 weeks) pregnancy active peptic ulcer current anticoagulation
Primary PCI
bullPCI = Percutaneous Coronary Intervention
bullPTCA = Percutaneous Transluminal Coronary Angioplasty
bullPOBA = Plain Old Balloon Angioplasty
PROGNOSIS
bullDischarge usually 5 days after admissionbullSmoking CessationbullShort and Long-term survival depend upon resting LV function residual ischemic myocardium and susceptibility to ventricular arrhythmias
THE END
- CHEST PAIN SCENARIO 3 GROUP 10
- SCENARIO
- KEYWORD
- QUESTION
- DIFFERENTIAL DIAGNOSIS
- INTRODUCTION
- BASIC SCIENCE
- EKG
- Normal heart
- Myocardial Infarction Two to three days after an MI the myocyt
- Slide 11
- PATHOPHYSIOLOGY OF ST-ELEVATION MYOCARDIAL INFARCTION (STEMI)
- myocardial infarction
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- HYPOTENSION May trigger a dramatic sympathetic nervous system
- Slide 19
- Slide 21
- Left Ventricular Function Systolic Function
- Ventricular Remodeling
- references
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- PATHOLOGIC OF Q-WAVE
- PATHOMECANISM CHEST PAIN
- Slide 31
- SMOKING kills
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- ThE eND
-

TREATMENTAspirin
bullRapidly blocks formation of thromboxaneA2 in platelets by cyclooxygenase inhibitionbull162-325mg chewed (promotes buccalabsorption)bullISIS-2ndash23 reduction in mortality largely additive to the reduction in mortality from streptokinaseOther Adjuvant TherapiesAnalgesicsbullNitratesbullBeta-blockersbullAce InhibitorsbullOxygenbullHeparinbullIV Glycoprotein IIbIIIaInhibitorsbullClopidogrelbullStatins
Thrombolytic TherapybullCommon AgentsbullTNK-tPA30-50mg IV bolusbullReteplase10U x 2 (each over 2 minutes) IVbullAlteplaseup to 100mg in 90mins (based on weight)
bullContraindicationsndashAbsolute Prior intracranial hemorrhage known cerebral vascular lesion malignant intracranial neoplasm ischemic stroke within 3 months suspected aortic dissection active bleeding recent closed head injury or facial trauma within 3monthsndashRelative History of chronic severe HTN severeuncontrolled HTN at presentation (gt180110) history of ischemic stroke gt3 months traumaticprolonged CPR recent internal bleeding (2-4 weeks) pregnancy active peptic ulcer current anticoagulation
Primary PCI
bullPCI = Percutaneous Coronary Intervention
bullPTCA = Percutaneous Transluminal Coronary Angioplasty
bullPOBA = Plain Old Balloon Angioplasty
PROGNOSIS
bullDischarge usually 5 days after admissionbullSmoking CessationbullShort and Long-term survival depend upon resting LV function residual ischemic myocardium and susceptibility to ventricular arrhythmias
THE END
- CHEST PAIN SCENARIO 3 GROUP 10
- SCENARIO
- KEYWORD
- QUESTION
- DIFFERENTIAL DIAGNOSIS
- INTRODUCTION
- BASIC SCIENCE
- EKG
- Normal heart
- Myocardial Infarction Two to three days after an MI the myocyt
- Slide 11
- PATHOPHYSIOLOGY OF ST-ELEVATION MYOCARDIAL INFARCTION (STEMI)
- myocardial infarction
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- HYPOTENSION May trigger a dramatic sympathetic nervous system
- Slide 19
- Slide 21
- Left Ventricular Function Systolic Function
- Ventricular Remodeling
- references
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- PATHOLOGIC OF Q-WAVE
- PATHOMECANISM CHEST PAIN
- Slide 31
- SMOKING kills
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- ThE eND
-

Thrombolytic TherapybullCommon AgentsbullTNK-tPA30-50mg IV bolusbullReteplase10U x 2 (each over 2 minutes) IVbullAlteplaseup to 100mg in 90mins (based on weight)
bullContraindicationsndashAbsolute Prior intracranial hemorrhage known cerebral vascular lesion malignant intracranial neoplasm ischemic stroke within 3 months suspected aortic dissection active bleeding recent closed head injury or facial trauma within 3monthsndashRelative History of chronic severe HTN severeuncontrolled HTN at presentation (gt180110) history of ischemic stroke gt3 months traumaticprolonged CPR recent internal bleeding (2-4 weeks) pregnancy active peptic ulcer current anticoagulation
Primary PCI
bullPCI = Percutaneous Coronary Intervention
bullPTCA = Percutaneous Transluminal Coronary Angioplasty
bullPOBA = Plain Old Balloon Angioplasty
PROGNOSIS
bullDischarge usually 5 days after admissionbullSmoking CessationbullShort and Long-term survival depend upon resting LV function residual ischemic myocardium and susceptibility to ventricular arrhythmias
THE END
- CHEST PAIN SCENARIO 3 GROUP 10
- SCENARIO
- KEYWORD
- QUESTION
- DIFFERENTIAL DIAGNOSIS
- INTRODUCTION
- BASIC SCIENCE
- EKG
- Normal heart
- Myocardial Infarction Two to three days after an MI the myocyt
- Slide 11
- PATHOPHYSIOLOGY OF ST-ELEVATION MYOCARDIAL INFARCTION (STEMI)
- myocardial infarction
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- HYPOTENSION May trigger a dramatic sympathetic nervous system
- Slide 19
- Slide 21
- Left Ventricular Function Systolic Function
- Ventricular Remodeling
- references
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- PATHOLOGIC OF Q-WAVE
- PATHOMECANISM CHEST PAIN
- Slide 31
- SMOKING kills
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- ThE eND
-

Primary PCI
bullPCI = Percutaneous Coronary Intervention
bullPTCA = Percutaneous Transluminal Coronary Angioplasty
bullPOBA = Plain Old Balloon Angioplasty
PROGNOSIS
bullDischarge usually 5 days after admissionbullSmoking CessationbullShort and Long-term survival depend upon resting LV function residual ischemic myocardium and susceptibility to ventricular arrhythmias
THE END
- CHEST PAIN SCENARIO 3 GROUP 10
- SCENARIO
- KEYWORD
- QUESTION
- DIFFERENTIAL DIAGNOSIS
- INTRODUCTION
- BASIC SCIENCE
- EKG
- Normal heart
- Myocardial Infarction Two to three days after an MI the myocyt
- Slide 11
- PATHOPHYSIOLOGY OF ST-ELEVATION MYOCARDIAL INFARCTION (STEMI)
- myocardial infarction
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- HYPOTENSION May trigger a dramatic sympathetic nervous system
- Slide 19
- Slide 21
- Left Ventricular Function Systolic Function
- Ventricular Remodeling
- references
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- PATHOLOGIC OF Q-WAVE
- PATHOMECANISM CHEST PAIN
- Slide 31
- SMOKING kills
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- ThE eND
-

PROGNOSIS
bullDischarge usually 5 days after admissionbullSmoking CessationbullShort and Long-term survival depend upon resting LV function residual ischemic myocardium and susceptibility to ventricular arrhythmias
THE END
- CHEST PAIN SCENARIO 3 GROUP 10
- SCENARIO
- KEYWORD
- QUESTION
- DIFFERENTIAL DIAGNOSIS
- INTRODUCTION
- BASIC SCIENCE
- EKG
- Normal heart
- Myocardial Infarction Two to three days after an MI the myocyt
- Slide 11
- PATHOPHYSIOLOGY OF ST-ELEVATION MYOCARDIAL INFARCTION (STEMI)
- myocardial infarction
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- HYPOTENSION May trigger a dramatic sympathetic nervous system
- Slide 19
- Slide 21
- Left Ventricular Function Systolic Function
- Ventricular Remodeling
- references
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- PATHOLOGIC OF Q-WAVE
- PATHOMECANISM CHEST PAIN
- Slide 31
- SMOKING kills
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- ThE eND
-

THE END
- CHEST PAIN SCENARIO 3 GROUP 10
- SCENARIO
- KEYWORD
- QUESTION
- DIFFERENTIAL DIAGNOSIS
- INTRODUCTION
- BASIC SCIENCE
- EKG
- Normal heart
- Myocardial Infarction Two to three days after an MI the myocyt
- Slide 11
- PATHOPHYSIOLOGY OF ST-ELEVATION MYOCARDIAL INFARCTION (STEMI)
- myocardial infarction
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- HYPOTENSION May trigger a dramatic sympathetic nervous system
- Slide 19
- Slide 21
- Left Ventricular Function Systolic Function
- Ventricular Remodeling
- references
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- PATHOLOGIC OF Q-WAVE
- PATHOMECANISM CHEST PAIN
- Slide 31
- SMOKING kills
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- ThE eND
-