chertkow-ccnarqrv quebec oct2013 · 08/10/2013 1 ccna the canadian consortium for nd...
TRANSCRIPT

08/10/2013
1
CCNA
The Canadian Consortium forN d ti d A i
CCNA
Neurodegenerationand AgingDr. Howard Chertkow,
Professor, Dept. of Neurology, McGill University;Physician, Division of Geriatric Medicine,
Dept. of Medicine, Jewish General Hospital; Director, Bloomfield Centre for Research in Aging,
Lady Davis Institute, Jewish General Hospital.
CCNA OverOveOverviewOVOVEROverview of Presentation
CIMA-Q CCNA- General ApproachThe teamsThe PlatformsThe PlatformsThe novelty of the approachThe cross-cutting cores
-Training-Knowledge Transfer-Women and Dementia core-ELSI
International collaborationGovernanceCIMA-Q and CCNASummary

08/10/2013
2
CCNA CIMA
CIMA‐Q plan and deliverables
Creating a registry of AD, MCI, SCI (Subjective Cognitive Impairment)Clinical, neuropsychology, imagingBiosamples
CCNA PLATEFORMES ET AXES MÉTHODOLOGIQUES
1. Banques de cerveau (amélioration des critères cliniques)2. Génotypage3. Neuroimagerie4. Biomarqueurs5. Marqueurs cognitifs/comportementaux (détection et progression)6 Modèles animaux6. Modèles animaux

08/10/2013
3
CCNA PLATEFORMES ET AXES MÉTHODOLOGIQUES
7. Cohortes cliniques8 Plateforme de colonies de rongeurs et8. Plateforme de colonies de rongeurs et de phénotypage9. Transfert de connaissance (e.gCDKTN)10. Harmonisation (critères, outils utilisés, banque de données, etc.)
CCNA FRSQ AD Research pg. 2 –autresaspects-
High Risk Pilot projects P4.Biomarqueurs, qP5. Marqueurs cognitifs,P6.Modèles animauxEt les themes: 1. Mécanismes biologiques2. Prévention3. Détection précoce 4. Thérapeutiques innovantes:

08/10/2013
4
CCNA Modèle méthodologique
Expert group Expert group Expert group Expert group
Neuro-imaging
Cognitive/behavioural symptoms
Biomarkers Risk and protection
factors
Population cohort (NuAge)
Clinicalcohort
Brainbank
CCNA
Cohort:50 Mild Alzheimer’s Disease subjects150 Mild Cognitive Impairment subjects100 Subjective Cognitive Impairment subjects50 Normal subjects
Deliverables: Cognitive, neuropsychiatric markers• Identification of a psychometrically reliable and valid battery of cognitive measures.• Harmonized web-based training and quality control procedures for administration and scoring of those proceduresprocedures.• Cognitive data from 350 older individuals.• These results will establish a battery of cognitive and clinical tools for the early-stage identification of AD

08/10/2013
5
CCNA CIMA-QCIMACIMAImaging Deliverables:•7 MRI and 3 PET qualified platforms • quality control records for MRI and PET platforms • 170 MRI scans for healthy older adults, SCI, MCI and AD subjects, with accompanying pre‐processed images and medial temporal lobe volumetric information • 35 PET scans for SCI, MCI and AD subjects, with accompanying qualified reports •Advanced protocols for standardized MRI and PET acquisitions • The first worldwide platform for PET reader training
CCNA ICRSAD Goals
1Primary
1Primary
2Secondary
2Secondary
3Quality
3Quality
preventionprevention preventionprevention Of lifeOf life

08/10/2013
6
CCNA WhOur Expression of Interest (EOI) included:• 37 principal applicants 4 from B.C.,
CCNA-Who we are:
5 from Alberta, 1 from Saskatchewan, 13 from Ontario, 11 from Québec,3 from Nova Scotia.
9 are junior researchers•9 are junior researchers• 285 other researchers•Steering committee: Chertkow (PI)Theme leaders, co-leaders, (Rylett, Hogan, Black, Masellis, Rockwood) Feldman, Gauthier
CCNA The CCNA application• Work in progress- grant due Dec. 2nd
• National in scope- still in process of recruiting researchers from Manitoba, New Brunswick, Newfoundland
• Budget in flux crucial role of partners especially for• Budget in flux – crucial role of partners- especially for platforms
• About 45 million dollars for 5 years• Leveraging/harmonization with other groups to maximize
productivity and save costs- Canadian Long. Study of Aging – biobanking, normal
control group- Ontario Brain Institute – cohorts, MRI- FRQS/Pfizer CIMA-Q (Québec) – cohorts, imaging-other provincial plans and agencies.
• Interactive discussions with partners- nothing set in stone here• Addressing EOI critiques and suggestions

08/10/2013
7
CCNACanadian Issues:• Rural service delivery•Provincial health care systems•Use of single payer system•cohesion across disciplines•cohesion across disciplines•collaborative structure
International issues:•NDD as global problems•Vascular emphasisVascular emphasis•Gender emphasis•Excellence of researchers•Need for novel molecules, new approaches, three themes
CCNA CCNA – our objectives1. To transform the Canadian NDD community into a synergistic clinical and research
network.
2. To create a novel Canadian dementia research infrastructure that will transform2. To create a novel Canadian dementia research infrastructure that will transform Canada into a single Alzheimer’s Disease Research Centre (ADRC). • clinical assessments •imaging protocols • biobanking protocols • brain banking • biomarkers: all are coordinated, shared and made available for the broadest use.
3. To address issues that are of particular importance within the Canadian landscape, including service delivery challenges, care for indigenous individuals, and addressing challenges of care within different provincial systems.
4. To include Teams focussing on neurodegenerative diseases beyond Alzheimer’s disease: LBD, VCI, FTD, PDD –
• common mechanisms • comorbidities • distinctive and shared pathologies
5. To position this Canadian network to partner globally and to move quickly.
6. Provide a critical link between basic scientists and clinical populations.

08/10/2013
8
CCNA General plan:
• General plan:• Lean administrative structure• 1/3 to ½ of funds to support 8 platforms• 2/3 of funds to 20 teams in the three themes• Roll over CDKTN to become the KT organ of
CCNA• Training program
T i l “ ”• Two special “cores” –– ELSI (Ethical, Legal, Social) consultancy program– Women and Dementia
CCNATeams- Theme 1Prevention of cognitive impairment and dementiaJane Rylett, David Hogan
Team 1 - Clinical genetics and gene discoveryg g yPeter St. George-Hyslop (U.of T.)Team 2 - Inflammation and Nerve Growth FactorsClaudio Cuello (McGill)Team 3 - Protein MisfoldingNeil Cashman (UBC)Team 4 - Synapses and metabolomicsRobert Bartha (Western)Team 5 - Lipid and Lipoprotein MetabolismCheryl Wellington (UBC)Team 6 - Nutrition, Exercise and Lifestyle in AD preventionCarol Greenwood (U. of T.)

08/10/2013
9
CCNA
Teams- Theme 2Treatments Sandra Black, Mario Masellis
Team 7 - Vascular illness and its impact on NDDEric Smith (Calgary)Eric Smith (Calgary)Team 8 - Lewy Bodies (PDD and LBD), Aging, and DementiaRichard Camicioli (Alberta)Team 9 - Developing New BiomarkersRoger Dixon (Alberta)Pierre Bellec (U. de Montréal)Team 10 - Cognitive Intervention and Brain PlasticitySylvie Belleville (U de Montréal)Sylvie Belleville (U. de Montréal)Team 11 - Prevention and Treatment of Neuropsychiatric SymptomsNathan Herrmann (U. of T.)Team 12 - Mobility, Exercise and CognitionManuel Montero-Odasso (Western)Team 13 - Frontotemporal dementiaRobin Hsiung (UBC)
CCNA
Teams- Theme 3Quality of Life Ken Rockwood
Team 14 - How multi-morbidity modifies the risk of dementia and the patterns of disease expression
M li A d (D lh i )Melissa Andrew (Dalhousie)Team 15 - Gerontechnology and dementiaAlex Mihailidis (U. of T.)Team 16 - Driving and dementiaGary Naglie (U. of T.)Team 17 - Interventions at the Sensory and Cognitive InterfaceNatalie Phillips (Concordia) Team 18 - Program to improve the effectiveness of dementia caregiversJoel Sadavoy (U. of T.)Team 19 - Integrating dementia patient care into the health care systemHoward Bergman (McGill)Team 20 - Issues in dementia care for rural and indigenous populationsDebra Morgan (U. Saskatchewan)Kristen Jacklin (U. Northern Ontario).

08/10/2013
10
CCNA
Theme 1 Theme 3
1. Genetics
2. Inflammation4. Synapse
5. Lipoprotein
6. Exercise,Lifestyle
14. Comorbidity
15. Gerontechnology
16. Driving 18. Caregivers
19. Health CareSystem
20. Rural,Indigenous
ELSI
Women
Theme 2
3. Protein Misfoldy p
7. Vascular
8. Parkinsons9. Biomarkers
10. Cognitive Therapy
11 Neuropsychiatric13. FTD
17. Sensory Interfaceg
Key - Arrows Red – one-way interactionwithin themeBlue – two-way interactionWithin themePink – one-way Interaction across themesGreen – two-way interaction across themes
Platforms: Clinical, Biomarkers, Imaging, Neuropsychology, Genetics, Brain Banks
11. Neuropsychiatric
12. Mobility
CCNA
Teams and Platforms being built together to support each other– hypothesis driven platforms

08/10/2013
11
CCNA
Cohorts
AD MCI VCI/Mixed LBD FTD Normal
BiosamplesPlatform
Platform
Imaging
Genetics
Brain Banks
Platform
Platform
Platform
Team 1Genetics
Team 2Inflammatory
Team 3……. Team 20Rural, Indigenous
CCNA
Cohorts
AD MCI VCI/Mixed LBD FTD Normal200150 200 50 50 50
Biosamples Blood •CRP, IL‐1, TNF‐alphaCSF • TrK‐A,Pro‐NGF, GFAP,MMP‐9,ACT,BDNF….
Platform
Platform
Imaging MRI‐allFDG PET 30PET‐PK11195 30PET Deprenyl 30
Genetics
Brain Banks Pro‐NGF, NGF, BDNF, TrK‐A, MMP‐9, CCL2 TIMP‐1 MMP‐3 MMP‐2
Platform
Platform
PlatformCCL2, TIMP‐1, MMP‐3, MMP‐2, CX3CL1….
Team 2 – Inflammation, Growth factors
08/10/2013
12
CCNA
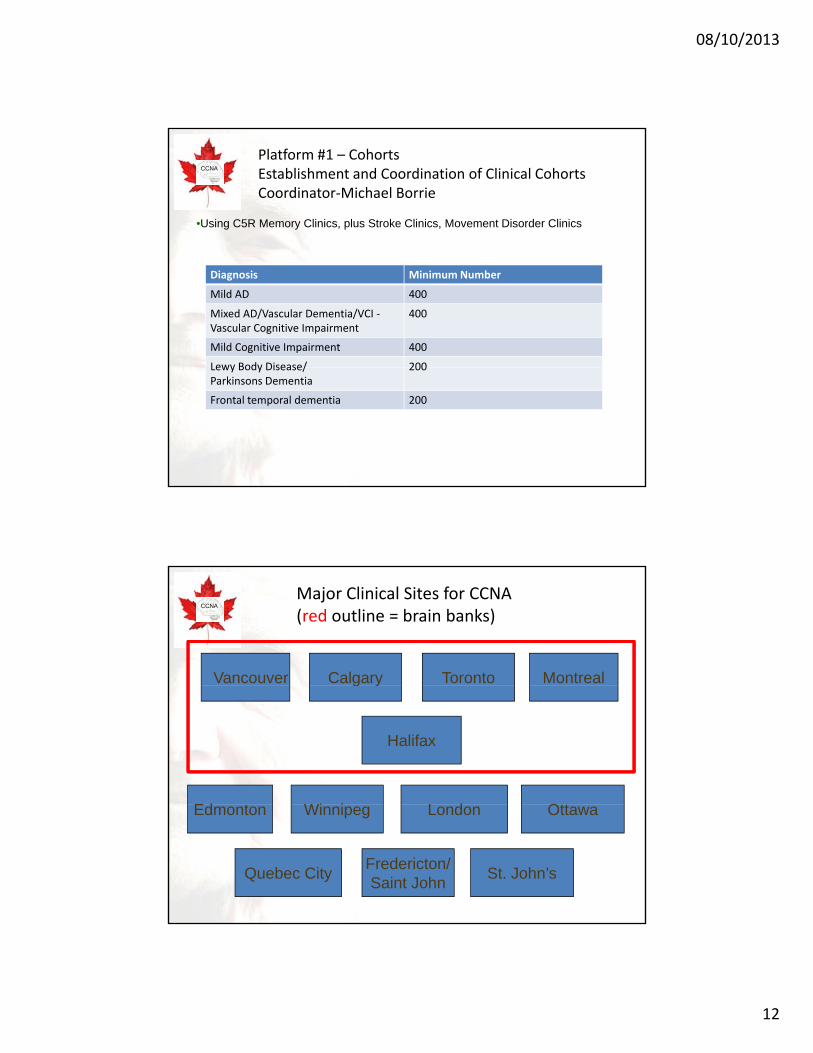
•Using C5R Memory Clinics, plus Stroke Clinics, Movement Disorder Clinics
Platform #1 – CohortsEstablishment and Coordination of Clinical Cohorts Coordinator‐Michael Borrie
Diagnosis Minimum Number
Mild AD 400
Mixed AD/Vascular Dementia/VCI ‐Vascular Cognitive Impairment
400
Mild Cognitive Impairment 400
Lewy Body Disease/ 200Lewy Body Disease/Parkinsons Dementia
200
Frontal temporal dementia 200
CCNA
MontrealCalgary TorontoVancouver
Major Clinical Sites for CCNA(red outline = brain banks)
Ed t
Halifax
g y
L dWi i OttEdmonton London
Quebec City Fredericton/Saint John
Winnipeg
St. John’s
Ottawa

08/10/2013
13
CCNAPlatform #1 – Cohorts Establishment and Coordination of Clinical Cohorts
•Subjects seen at academic (largely C5R) Memory Clinics, and Movement Disorder Clinics across the country• i d di d bj i• Rigorous standardized subject ascertainment•Shared consent procedures•iPAD/tablet clinical data (upload)•Web‐based computerized intake• Agreed on cognitive testing, MoCA, computerized testing•Detailed “deep phenotyping of each research subject”• Longitudinal follow upLongitudinal follow‐up. •Upload via C‐Brain to Montreal Neurological Institute•Coordinated with imaging, biosamples, genetics, Brain bank• Directly upload information into anonymized LORIS database • National clinical registry to support the research agenda of all teams and supply well‐ascertained volunteers for clinical trials.
CCNA
Pl tf #2 B i I iPlatform #2 – Brain ImagingAlan Evans, Louis Collins, Simon Duchesne

08/10/2013
14
CCNA
HPC Integration(8 compute installations, 80,000+ core)
CBRAIN National HPC Integration(100,000 processors)
Orcinus - Westgrid (3072 cores)
Colosse - CLUMEQ (7616 cores)
JUROPA & JUDGE – Julich, GER(30000 cores)
Kraken - SHARCNET (3774 cores)
Guillimin - CLUMEQ & Local Servers (16000 cores))GPC - SciNET
(30240 cores))
Mammouth II - RQCHP(2464 cores)
CCNA
Acquisition management Analysis pipelines
80 man‐years of developmentWeb‐based, secure data transfer of multi‐site dataGeneralized open‐source MYSQL architecture ‐ flexible, extensibleApplications in development, neurodegeneration (US, Europe, Asia)
cqu s t o a age e tProject management toolsDouble data entry/ range checkingAutomated 3D image QCJava‐based remote 3D image QC150 behavioral instrumentsMANTIS bug‐tracking
External pipelines for analysis (MNI, SPM, FSL , LONI, AFNI)Integrated with grid‐computing networks (CBRAIN, NeuGrid)
LORIS
Repository /downloadData types: behavior, clinical, imaging, geneticOn‐line remote MRI browserData querying GUI (volumes, surfaces, behavior)e.g. NIH database of normal brain development

08/10/2013
15
CCNA
CIMAQ multi-centre neuroimaging platform(Duches
Standardized acquisition/QCTrainingData bank/dissemination
CCNA
DemMETRIX platform
VolMETRIX VasoMETRIXAlzMETRIXMCIMETRIX
101 cm3 Normal subjectMCI stable
sMCI
pMCI
CN
ADVascular load
3.7 cm3
Patient with ADMCI progressor
134 cm3
Collins L.

08/10/2013
16
CCNA
• Platform #3 Biosamples• Platform #3 – Biosamples[CSF/Blood samples/Biomarker resources]. Coordinator-Judes Poirier
CCNA
1 ex
pres
sion
Temporal Cortex
Glial HO‐1 expression in AD and MCI (oxidative stress measure)
Canadian researchershave developed
Ast
rogl
ial H
O-1
Temporal Cortexand published 37 potentialnew biomarkers forNeurodegenerativeDiseases….never studied inadequate numbers.
Asr
oglia
l HO
-1 e
xpre
ssio
n
Hippocampus
Schipper et al,
NeurobiolAging, 2006

08/10/2013
17
CCNASpectrum of CCNA Biomarker Team: Breadth and
ImpactPierre Bellec
Louis Collins
Simon Duchesne
Nikolai Malykhin
NeuroImaging NeuroBiological NeuroCognitive NeuroQuantitative
Spectrum of biomarkers under development in Canadian labs
y
Eric Smith
Robert Bartha
Richard Camicioli
Howard Chertkow
Roger Dixon
Angeles Garcia
Vassilios Papadopoulos
Marc PoulinMarc Poulin
Peter Stys
Hyman Schipper
David Westaway
Esther Fujiwara
Scott Hofer
Stuart MacDonald
Doug Munoz
CCNA
Platform #3 – Biosamples[CSF/Blood samples/Biomarker resources/]. Coordinator-Judes Poirier
• CLSA model-multiple tubes of blood, bar coded, shipped for analysis
• F bi k d t t i d b th t f• Focus on biomarkers and tests required by the teams for their research program
• Coordinated acquisition of blood, csf, and (eventually) brain biomarkers from all cohort members.
• Tests carried out by relevant team experts Theme 1• CSF- Poirier/Breitner national centre for t-tau, p-tau,
csfamyloid levels.• Genetics (next slide)• Allows measurement of test sensitivity (MCI, AD),
specificity (LBD, FTD).• Allows analysis of clusters and subgroups• Allows comparative assessment of different biomarkers

08/10/2013
18
CCNAPlatform #3a -Normative Controls and Biobanking
• There are important Canadian population cohorts of elderly subjects: CLSA (Canadian Longitudinal Studyelderly subjects: CLSA (Canadian Longitudinal Study of Aging), Victoria Aging Study (Dixon), NuAge(Gaudreau).
• CCNA will partner to leverage “normal elderly subjects” – shared biosamples, cognitive testing, even MRI protocols.
• Will leverage off CLSA biosample collection andWill leverage off CLSA biosample collection and anonymizing system, and large biobank in Hamilton.
• Will supply needed normal control groups
CCNA
Platform #4 DNA Sequencing and GenotypingPlatform #4-DNA Sequencing and GenotypingPlatform/Team coordinated by Peter St. George-Hyslop

08/10/2013
19
CCNA
AD AD UofT/UBC
FTLDFTLDUBC
DLBDLBUofT
PDPDUBC
ALSALSMcGILL
Expert nodes withexisting samples and genetic data
Genetics Platform#4– New Sample & Data Collection
•NeuroX chip SNP screen• Whole Exome/Whole Genome Sequencing• RNA‐Seq• Bioinformatics •Methylome•HistoneMark CHIP‐SEQ
• Genetic data (SNP, mutations, InDels, CNV, ROH)• Epigenetic changes
Common platformswith disease‐specificexpert curation and cross‐disease comparison
Data sharing
• Gene Expression Profile
• New Genes•Gene:Gene Interactions •Gene:Environment Interactions •Genotype:Phenotype Correlation • Genetically Specified Cohorts•Gene:Biomakrer Correlations
Output
CCNA
•IlluminaNeuroX Chip assessment providesa) all known mutations (~1 000) in genes known to cause
What the NeuroX Chip measures
a) all known mutations ( 1,000) in genes known to cause neurodegenerative diseases;
b) b) ~10,000 key tagging SNPs for all genome‐wide significant loci published in human GWAS for PD, FTLD, ALS, AD and stroke together with the top ~1,000 SNPs just below genome‐wide significance;
c) c) ~240,000 coding sequence variants with a frequency of ) ) , g q q y>1% in the human genome;
d) d) ~5,000 novel coding variants currently detected by whole exome sequencing of familial cases affected by different neurodegenerative disorders;
e) e) ~1,000 eQTL markers.

08/10/2013
20
CCNA
Platform #5-Brain Banking core of CCNA Coordinator-Sultan Darvesh
CCNA
To collect well characterized brain tissues and to make them available for researchers to understand the causes of neurodegenerative disorders
Response ‐ Establish A Canadian NDD Brain Bank Network Currently – not enough brain collection in Canada
Alzheimer’s DiseasePick’s Disease
Alzheimer’s DiseaseNormal

08/10/2013
21
CCNA Brain Banking core of CCNA Coordinator-Sultan Darvesh
Plan – establish within 12 months a “Canadian Brain Bank Network” – 4 or 5 BB’s in consortium with secondary banks as well.Standardize structure and procedures$ combination funding: Local, regional, other funders (such as Brain Canada), plus CCNA: total 300,000 /bank/yearbrain donation – national coordination structureNational brain exam protocolDatabasing of results, linked to CCNA cohortsAlso: collection of normal brains from CLSA?
CCNA Platform #6-Support for Transgenic Colonies Coordinator-David Westaway
• Basic science labs across Canada currently underfunded for support of Transgenic animal models
• CCNA will vet requests for extra support of these crucial colonies
• Will supply $15,000 /year for each TG colony used for NDD research.y

08/10/2013
22
CCNA
Platform #7-National Platform on Experimental Therapies. Coordinator-Howard Feldman Goals:
To integrate a national program for therapeutic drug development that will - develop innovative candidate therapies for AD and other- develop innovative candidate therapies for AD and other
neurodegenerative diseases- optimize preclinical and clinical development phases
Preclinical development- Inventory and coordinating role of assets and skill sets- Models of disease - Close coordination with Themes 1 and 2
Cli i l d l tClinical development- Innovative designs and advanced methodologies- Efficiencies in trial execution- National (C5R, CSC) and global networking (NYAS, ADCS, One
Mind, JPRD)
CCNA CCNA Preclinical Drug Development Development
■ Develop an inventory of resources and units across the consortium with capabilities for preclinical drug discovery
T t id tifi ti ( Th 1 d 2 th )- Target identification ( Themes 1 and 2, others) - High throughput screening with compound libraries (academic
units, pharma partners, specialized facilities CDRD, PQ- Target validation: animal models, cellular models, novel systems
pluripotent stem cells (iPSC)- Pharmacology units with ability to establish Pk, PD, dose modelling
towards phase 1 dose selection- Toxicology (GLP, outsourced, local)
Deliverables:■ Deliverables: - Preclinical package for IND and first in human phase 1 trials- Novel validated targets - Repurposed drugs with preclinical package that have potential
application to targets in neurodegeneration

08/10/2013
23
CCNA
• What is unique about the platforms?
CCNAPathological Diagnosis of Dementia
Criteria 1 Criteria 2
AD 75% 39%AD 75% 39%VaD 3% 1%LBD 9% 3%Other 13% 13%Mixed AD/VaD 20%Mixed AD/LBD 19%Mixed AD/Other 5%
44%
Source:Munoz,et al.

08/10/2013
24
CCNA Platform- Novel approach: We will embrace the complexity of NDD
We will be both radical “lumpers” and “splitters” for the major dementias. We will entertain and test general hypotheses that are both of these in innovative fashion:both of these in innovative fashion:
– We will “lump” dementia cases together for molecular analyses, assessing AD/ Vascular/Lewy Body loads along a continuum rather than strict AD vs. Vascular dementias
– Allows us to look at risk factors, biomarkers, therapy response in real life “messy” and mixed dementia cases
– We will entertain the possibility of mixed/multiple therapy trials in years 3-5.– Brings vascular assessment VCI vascular risk factors to centre stageBrings vascular assessment, VCI, vascular risk factors to centre stage.
– We will also have the power to look at cluster analyses of AD – to assess for AD subgroups in terms of genetics, imaging, biomarkers, clinical, and eventually brain tissue, over a five year period. Data driven foray into “AD subtypes” is overdue. We will pursue novel hypotheses that significant subtypes of AD exist and can be established – we will lead as “splitters”.
CCNA
• Platform Hypotheses
Subtypes of Frontotemporal dementia

08/10/2013
25
CCNA Cross-cutting theme-training
• Building capacity is an urgent priority • Need development of front line health care professionals
with expertise in cognitive impairment and dementia. • CCNA direct support- partnering commitments for a “CCNA
training partnership program” that will fund at least 22 research fellowships across Canada on an annual basis in the area of dementia and cognitive impairment.
• These “CCNA Fellows” will carry out research projects in labs and clinics across the country as part of a CCNA team.
• Novel aspects of their training: menu-driven access to p gselected areas of interdisciplinary training (e.g. business training, use of new technologies, ethics), internships and training in industry settings, and web-based learning and virtual classroom opportunities.
• Tracking of all Fellows along with postdoctoral fellows • CCNA to catalyse their transition to independent researcher.
CCNA Knowledge transfer in the CCNA
• KT will be at the centre of CCNA. We will build on the momentum achieved by the Canadian Dementia Knowledge Transfer Network (CDKTN), whose funding is ending this year. (C ), ose u d g s e d g t s yea
• Ken Rockwood, the director of CDKTN, will sit as Theme 3 leader on the CCNA and will oversee the transition of CDKTN into the KT arm of CCNA
• On-line contact between members of the Canadian dementia research community within CCNA.
• Relevant basic and clinical research developments within CCNA, new initiatives, and collaboration opportunities will all be shared online.
• Monthly newsletters to our research community. • Organizing an annual CCNA meeting• Organizing an annual CCNA meeting. • KEY: Hosting smaller workshops/webinars to bring key members of
multiple teams together on a monthly basis.• Contact with stakeholders and partners such as the various levels of
government and the community at large will be regularly maintained. S• A dementia educational initiative targeted at physicians and care
providers will be developed. • Seek out potential new researchers in dementia annually.

08/10/2013
26
CCNA Theme 1: KT Education & TrainingThe Canadian Dementia Resource and Knowledge Exchange
(CDRAKE) is a free, virtual network for exchange in dementia
• Focus on dementia specific knowledge translation
• Learning modules to foster the development of KT skills
• KT tools and resources for researchers
© CDKTN 2012
researchers
www.DementiaKT.ca
CCNA
Theme 1 Theme 3
1. Genetics
2. Inflammation4. Synapse
5. Lipoprotein
6. Exercise,Lifestyle
14. Comorbidity
15. Gerontechnology
16. Driving 18. Caregivers
19. Health CareSystem
20. Rural,Indigenous
ELSI
Women
Theme 2
3. Protein Misfoldy p
7. Vascular
8. Parkinsons9. Biomarkers
10. Cognitive Therapy
11 Neuropsychiatric13. FTD
17. Sensory Interfaceg
Key - Arrows Red – one-way interactionwithin themeBlue – two-way interactionWithin themePink – one-way Interaction across themesGreen – two-way interaction across themes
Platforms: Clinical, Biomarkers, Imaging, Neuropsychology, Genetics, Brain Banks
11. Neuropsychiatric
12. Mobility

08/10/2013
27
CCNA Cross-cutting theme-training – KTHow the teams will communicate
• Constant web-style communication of new results and opportunitiesand opportunities
• Annual meeting of researchers• Frequent small group meetings on topics and sub-
themes• Research Webinars• Integration of new researchers• Policy role
CCNAWomen and Dementia CoreCo-leads – Dr. Gillian Einstein and Dr. Mary C. Tierney, University of TorontoMembers: Dr. Barbara Sherwin and experts across Canada
Background and Rationale– Women account for 70% of cases of dementia– Women have a higher prevalence of Alzheimer’s disease, the
most common cause of dementia– Women are the primary caregivers of people with dementia-
they are more likely to outlive their male partnersthey are more likely to outlive their male partners– Sex and gender issues must be addressed in research on
neurodegenerative diseases– Propose a Women and Dementia Core

08/10/2013
28
CCNAWomen and Dementia Core
Objectives1. Ensure presence of a research program targeting women and
d i i d ti ll b ti ith th t tgender issues in dementia collaborating with the separate teams • Develop projects addressing critical issues in the etiology of dementia in women,
including for example, the effects of reproductive history, sex hormones, oophorectomy, postmenopausal hormone therapy (HT) use, breast cancer and its treatments, all of which intersect with issues pertaining to primary and secondary prevention and quality of life, including caregiver stress and isolation
2. Provide consultation to Teams on methodology in order to:• optimize assessment of gender and sex variables across the clinical cohorts and
other platforms• optimize studies across the 20 teams so that gender and sex variables are
adequately consideredy• optimize therapy programs (pharma and non-pharma) so that gender and sex
variables are adequately addressed 3. Allocate resources to achieve these objectives
CCNAWomen and Dementia Core
Elements to be incorporated in Shared Resources and Platforms
Clinical cohorts and normal control subjects• gender and sex issues in choice of subjects to study effects of sex hormones,
postmenopausal HT status, oophorectomy, etc.Imaging platform
• sample size affected by sex and genderBiosamples, CSF, genetic samples, biomarker resources, DNA
sequencing and genotypying• sex issues in sample collection, storage and analysis
Transgenic colonies• animal sex as a variable
Academic Clinical Trials and Drug Development• females must be studied in equal numbers as males in therapy trials.

08/10/2013
29
CCNAELSI (Ethical, Legal, and Social Implications of the research) consultation core
ELSI will be coordinated by Dr. Serge Gauthier, MD, FRCPCM Gill C t f St di i A iMcGill Centre for Studies in AgingDouglas Mental Health Research Institute
• National experts in legal, ethical, social issues surrounding dementia being recruited onto the “Consultation Core”• “Consultation Core” will consult with teams on all• Consultation Core will consult with teams on all ELSI issues• “Consultation Core” will advise Research Executive Committee on all pertinent issues arising, and draw up policy for CCNA.
CCNA International collaborations - Britain
• The Wellcome Trust/MRC/CIHR/DZNE neurodegeneration consortium is coming up forneurodegeneration consortium is coming up for renewal.
• Discussions with researchers from U.K.- Lovestone, Fox, regarding MRC “deep phenotyping” initiative and registry in Britain – coordination of clinical cohorts and genetics.
• A f th ll b ti ill b il bl• An array of other collaborations will become available.

08/10/2013
30
CCNA
ScientificDirector
Governance structureCIHR
ScientificAdvisory Group
KT Committee
Data/SamplepAccess
Committee
ELSICommitteeChair/ELSI
Management
Training
ResearchExecutiveCommittee
CommunityAdvisoryGroup
PlatformsCohorts
Women
Committee‐Manager‐ Business & Finance officer‐ Community officer
Theme 1Lead
Theme 2Lead
Theme 3
LeadTeams1‐6
Teams7‐13
Teams14‐20
CohortsBiosamplesGeneticsImagingBrainbankingMouse TG modelsClinical trials
CCNAMaintaining focus and priorities issue:
Start with all the teams (that is, all approved by CIHR)Each team – milestones, and deliverables up frontEach team milestones, and deliverables up frontTwo year end Report Carda) Deliverables (score /70) – scored for meeting milestones, and for the transformational potential of the deliverablesScoring by the International Scientific Advisory Groupb) Networking/Interchange (score/30) – scored for interchange with other groups, interaction.Scored by the theme leader
The 15 teams with lowest scores are cut by 10%.The 4 teams with the highest scores are increased by 100%
08/10/2013
31
CCNA
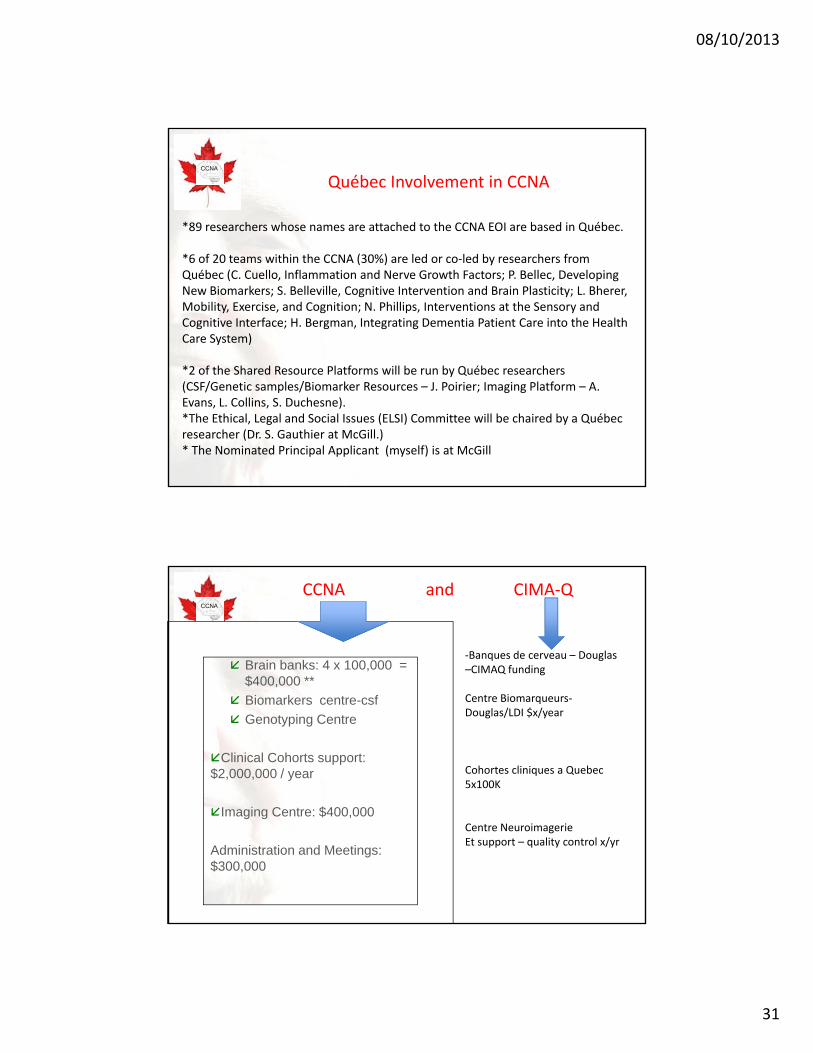
Québec Involvement in CCNA
*89 researchers whose names are attached to the CCNA EOI are based in Québec.
*6 of 20 teams within the CCNA (30%) are led or co‐led by researchers from Québec (C. Cuello, Inflammation and Nerve Growth Factors; P. Bellec, Developing New Biomarkers; S. Belleville, Cognitive Intervention and Brain Plasticity; L. Bherer, Mobility, Exercise, and Cognition; N. Phillips, Interventions at the Sensory and Cognitive Interface; H. Bergman, Integrating Dementia Patient Care into the Health Care System)
*2 f th Sh d R Pl tf ill b b Q éb h*2 of the Shared Resource Platforms will be run by Québec researchers (CSF/Genetic samples/Biomarker Resources – J. Poirier; Imaging Platform – A. Evans, L. Collins, S. Duchesne).*The Ethical, Legal and Social Issues (ELSI) Committee will be chaired by a Québec researcher (Dr. S. Gauthier at McGill.)* The Nominated Principal Applicant (myself) is at McGill
CCNA CCNAICRSAD FRSQ –1.
PlatformsBrain banks: 4 x 100,000 = $400,000 **
‐Banques de cerveau – Douglas–CIMAQ funding
CCNA and CIMA‐Q
$400,000 Biomarkers centre-csfGenotyping Centre
Clinical Cohorts support: $2,000,000 / year
Centre Biomarqueurs‐Douglas/LDI $x/year
Cohortes cliniques a Quebec5x100K
Imaging Centre: $400,000
Administration and Meetings: $300,000
Centre NeuroimagerieEt support – quality control x/yr

08/10/2013
32
CCNA
• There will be considerable synergy between CCNA and CIMA Q Imaging platform as example
Synergy between CCNA and CIMA‐Q
CIMA‐Q.‐ Imaging platform as example. • Douglas Hospital Brain Bank. CCNA will actively coordinate and co‐fund a consortium of brain banks across the country, and this will allow complementary funds for the Douglas Brain Bank to come from national as well as provincial dementia strategies.The CCNA will collaborate and build off of the clinicalThe CCNA will collaborate and build off of the clinical cohorts being established under CIMA‐Q. We hope to make the protocols comparable such that subjects enrolled into CIMA‐Q can also be at the same time included into the CCNA cohorts being established.
CCNA
Conclusion 1:This is a huge and complex construct. Will we be able to integrate it?
Response: This is the biggest and most ambitious grant ever for NDD in this country.•We will need to train on access to LORIS and data.•We will need to set up communication systems to keep researchers out of silos and bind teams together.•We will need to bring in informatics and data management experts.•We will need to communicate in ways never previously necessary.W ill d t di t d ll b t•We will need to coordinate and collaborate as never before.Leadership and management will be key.
The potential pay‐off?‐ Transformational research, break throughs, and successful deliverables never previously possible.

08/10/2013
33
CCNA
Conclusion 2-What is novel and transformative in CCNA?
• We will be constructing national platforms which are hypothesis driven and support the research program of the teams utilizing them.
• Canada is big enough and small enough:– Small enough to include the entire NDD research community- to
connect basic and clinical researchers.– Big enough to study all the Neurodegenerative Diseases- for
shared and contrasting mechanism.• We will become the first country where imaging
algorithms can be made available to clinicians and clinics in a single payer public system in real time.
• We will acknowledge and accept the “real world” dementias, embrace complexity, and study unique cohorts of mixed dementias, where multiple pathologies are at play and multiple therapies may be necessary.
CCNA Conclusion 3-What is novel and transformative in CCNA?
•We will be “lumpers”‐ studying shared mechanisms across• We will be lumpers ‐ studying shared mechanisms across NDD, as well as “splitters”‐ enunciating subtypes of AD to emerge from cluster analyses of complex data.•We will unite highly characterized cohorts across the country with a unit for Academic Clinical Trials and Drug Development – subgroups classified by pharmacogenomics, imaging, specific biomarkers will be available for pilot studies.p• We will put KT right at the centre of the research plan•First international consortium to focus on gender and women issues.

08/10/2013
34
CCNA
Thank youMerci!